Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Changes In Plasma NPY, IL-1β And Hypocretin In People Who Died By Suicide
Authors Lu J, Li S ![]() , Li H, Mou T, Zhou L, Huang B, Huang M, Xu Y
, Li H, Mou T, Zhou L, Huang B, Huang M, Xu Y ![]()
Received 19 June 2019
Accepted for publication 12 September 2019
Published 10 October 2019 Volume 2019:15 Pages 2893—2900
DOI https://doi.org/10.2147/NDT.S219962
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Jing Lu,1 Shangda Li,1 Haimei Li,1 Tingting Mou,1 Lihong Zhou,2 Bochao Huang,1 Manli Huang,1 Yi Xu1
1The Key Laboratory of Mental Disorder Management in Zhejiang Province, Department of Psychiatry, First Affiliated Hospital, College of Medicine, Zhejiang University, Zhejiang University Brain Research Institute, Hangzhou, Zhejiang Province, People’s Republic of China; 2Institute of Criminal Science and Technology, Hangzhou Public Security Bureau, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Yi Xu; Manli Huang
The Key Laboratory of Mental Disorder Management in Zhejiang Province, Department of Psychiatry, The First Affiliated Hospital, Zhejiang University School of Medicine, 79 Qing Chun Road, Hangzhou 310003, People’s Republic of China
Tel/fax +86-571-8723-5995
Email [email protected]; [email protected]
Purpose: There is growing evidence showing that inflammatory cytokines and neuropeptides may be involved in the pathophysiology of suicidal behavior. However, studies have yielded contradictory data, and no biological markers that help predict suicide have been identified. This study aimed to identify biological patterns, such as NPY, IL-1β and hypocretin plasma levels, in people who died by suicide.
Patients and methods: Twenty-two people who died by suicide compared with 22 controls matched for age and sex were studied. In suicide and control subjects, we estimated the levels of NPY, IL-1β and hypocretin in plasma using enzyme-linked immunosorbent assay. The data are presented as the median (25th–75th percentile).
Results: We found (1) a significant elevation in plasma NPY levels in suicide subjects versus control subjects (suicide: 11.38 (9.380–16.55); controls: 8.95 (7.590–10.93); P=0.013), and plasma NPY concentrations were approximately 62% higher in suicide subjects than those in control subjects; (2) a significant decrease in plasma IL-1β concentrations between suicide and control subjects (suicide: 121.1 (82.97–143.0); controls: 425.9 (233.1–835.3); P<0.001) as well as a decrease in IL-1β concentrations by almost 80%; and (3) no significant difference in plasma hypocretin levels between suicide and control subjects (suicide: 16.62 (13.62–25.77); controls: 21.63 (14.97–29.72); P=0.356).
Conclusion: Our results suggest that plasma NPY and IL-1β were related with suicide behavior rather than to suicide causes or suicide method. Specific combinations of plasma biomarkers may discriminate between types of suicidal behaviors and indicate increased risk for future suicide attempts.
Keywords: plasma biomarkers, suicide behavior, suicide causes, suicide method
Introduction
More than 800 thousand people die from suicide every year, representing a suicide rate of 11.4 per 100 million in the population, according to WHO’s first global report on suicide prevention. For sex differences, 15 males and 8 females in a population of 100 thousand died by suicide. With regard to age, globally, suicide rates are the highest in elderly persons.1 The risk factors related to suicide include war, disaster, discrimination, abuse, violence, mental disorders, poor physical health and financial loss. Psychiatric disorders are the most common factors that are present in suicide cases.1,2 Neurotransmitters, the hypothalamic–pituitary–adrenal axis, genetic factors and inflammatory cytokines may account for the pathophysiology of suicide.2,3
Although several non-biological measures used to evaluate suicide risk, like Nurses’ Global Assessment of Suicide Risk Scale, Beck Scale for Suicide Ideation, self-report and structured interview, these methods are relatively subjective. The lack of robust biomarker for clinical suicide risk assessment has led researchers to investigate the neurobiological mechanisms behind suicidal behavior, in search for potential biomarkers.
Increasing evidence has suggested that neuropeptide Y (NPY) may act as a key modulator of the crosstalk between the brain and the immune system in health and disease. Neuropeptide Y (NPY) is a highly conserved 36-amino-acid peptide.4 It is involved in a variety of physiological functions such as emotion, cognition and stress responses5 as well as many mental disorders such as major depressive disorder, schizophrenia and bipolar disorder. The study results on NPY are conflicted. Some studies reported that NPY levels were decreased in suicide subjects both in the CSF and postmortem cortex,6,7 while other studies showed that CSF NPY levels were increased in those who attempted suicide.8
Interleukin-1β (IL-1β) is an inflammatory cytokine that belongs to the IL-1 family. It is secreted by monocytes, macrophages and dendritic cells as well as B-lymphocytes and NK cells. IL-1β has been described to modulate neurons and functions of the central nervous system in a direct or mediated way.9 The aberrant level of IL-1β may affect memory and cognitive function as well as synaptic plasticity.10 We supposed that IL-1β may play an important role in patients who died by suicide. Recently, studies have indicated that IL-1β may be associated with some psychiatric disease states such as major depressive disorder and bipolar disorder.11 Studies have shown the mRNA and protein expression levels of IL-1β and IL-6 were abnormal in postmortem brain samples of suicide who died by suicide.12 Even those who attempted suicide had higher levels of inflammatory cytokines IL-6 and IL-1β, which were associated with significantly lower mean levels of vitamin D than depressed nonsuicidal patients and healthy controls.13 However, there are no data on IL-1β changes in postmortem suicidal plasma.
Hypocretin, also known as orexin, is a pair of excitatory neuropeptide hormones called hypocretin-1 (HCRT-1) and hypocretin-2 (HCRT-2). They are known to play a role in many neurophysiological and behavioral processes, such as the sleep–wake cycle, food intake, sexual behavior and stress responses, and they are severely affected in depression.14 Moreover, hypocretin is thought to be involved in suicidal behaviors. A study indicated that hypocretin was increased after a suicide attempt, while another study showed that a low hypocretin level was correlated with a more severe mental condition in those who attempted suicide.15,16
Previous studies have shown interactions among NPY, IL-1β and hypocretin. There is a neuronal relationship between the NPY and hypocretin systems, and the hypocretigenic action of NPY is mediated by hypocretin-1-induced hypocretigenic action.17 NPY may inhibit hypocretin neuronal activity, while hypocretin may possibly increase NPY release in hypothalamic nuclei.18 Furthermore, inflammatory factors such as IL-1β induced lethargy, and this was mediated by the suppression of hypocretin neuron activity.19
In the current study, we measured plasma IL-1β, NPY and hypocretin-1 in suicide subjects and in age- and sex-matched healthy control subjects. In addition, we also analyzed NPY, IL-1β and hypocretin-1 in suicide subjects with psychiatric illness (PI) and those with life events (LE). We hypothesized that plasma IL-1β, NPY and hypocretin-1 could be potential biomarkers of suicidal behavior.
Significance
The lack of robust biomarker for clinical suicide risk assessment has led researchers to investigate the neurobiological mechanisms behind suicidal behavior, in search for potential biomarkers. Previous studies have shown interactions among inflammatory cytokines and neuropeptides with suicide behavior, such as NPY, IL-1β and hypocretin. In the current study, we measured plasma NPY, IL-1β and hypocretin-1 in suicide subjects and in age- and sex-matched healthy control subjects. We hypothesized that plasma IL-1β, NPY might be potential biomarkers of suicidal behavior.
Materials And Methods
Characteristics Of Suicide And Control Subjects
Suicidal plasma samples were obtained from 22 suicide subjects (11 men and 11 women) in the Hangzhou Criminal Investigation Detachment of Public Security Bureau, and they were matched for age and sex with 22 healthy controls (HCs). After description for research purposes, written informed consent was obtained from the suicide subject’s next of kin and healthy controls.
The suicide subjects and their controls were well matched for age and sex (see Table 1, all P>0.358). The inducements of death were divided into psychiatric illness (PI) and life events (LE). Suicides with PI included schizophrenia and major depressive disorders, while those with LE were always related to health problems, family problems and social factors20 (see Table 2). Eleven suicide subjects with PI were always associated with irregular medication, while 11 suicide subjects with LE had various cultural backgrounds, such as religion, quarrels and organic disease.
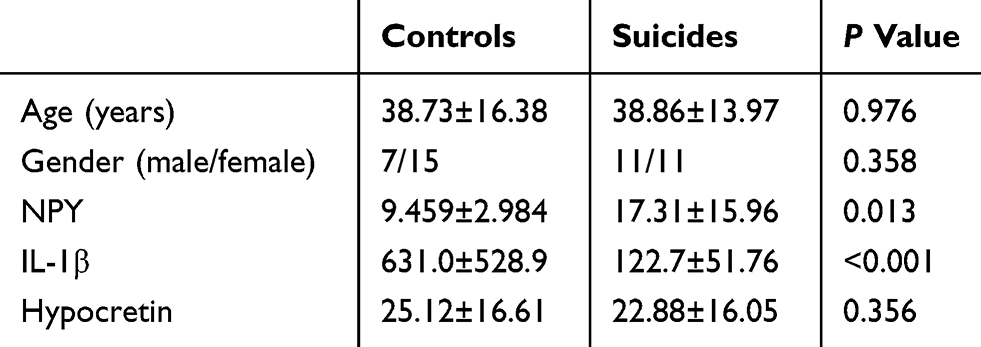 |
Table 1 General Information And Parameters Measured Of Controls And Suicides |
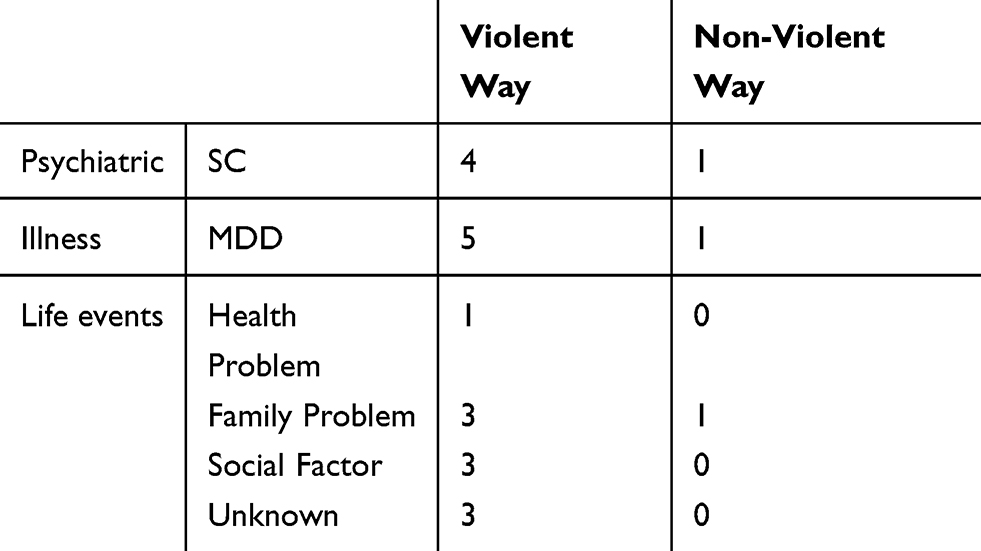 |
Table 2 The Distribution Of Suicide Methods And Suicide Causes |
Moreover, suicide death was also divided into violent or nonviolent suicide attempts.21,22 A nonviolent suicide attempt was defined as a drug overdose (3, 13.6%) or a single wrist cut. The violent attempts included jumping (8, 36.4%), hanging (6, 27.3%), drowning (3, 13.6%) and carbon monoxide poisoning (2, 9.1%).
Acquisition Of Suicidal Plasma Samples
Controls met the following criteria: 1. The age and sex were matched with suicide subjects; 2. No subjects had any lifetime histories of serious physical disorders, organic brain disease or cerebral trauma; 3. No subjects had any serious mental retardation; 4. MRI examination showed no brain structure abnormality; and 5. No subjects had metal in the body, such as a cardiac pacemaker, insulin pump or artificial heart valve. Twenty-two HCs met the inclusion criteria. The present study was approved by the ethics committee of the First Affiliated Hospital of Medical School of Zhejiang University and was already registered in China Clinical Trial Registry and registration number is ChiCTR1800015937.
Blood Collection
Venous blood samples were collected with anticoagulant tubes. Then, the blood samples were centrifuged at 3000 rpm at 4°C for 20 mins and stored at −80°C until assay.
Measurement Of Serum Peptide Concentrations
Plasma concentrations of NPY, IL-1β and hypocretin were measured by enzyme-linked immunosorbent assay (ELISA). Plasma concentrations of NPY (EZHNPY-25K, Millipore, USA), IL-1β (ab214025, Abcam, UK) and hypocretin (HU9788, TSZ, USA) were measured with an ELISA kit, following the manufacturer’s instructions. All the experiments were performed in duplicate.
Statistical Analysis
The data are expressed as the median (25th–75th percentile) and were analyzed with SPSS version 19.0 (IBM, Chicago, IL, USA). As the biological data were not always normally distributed, nonparametric tests were applied. Differences between the 2 groups were tested using a Mann–Whitney U-test. Differences among the 3 groups were first tested with a Kruskal-Wallis (K-W) test, and if a significant difference was identified, the difference between the 2 groups was checked with a Mann–Whitney U-test. Correlations were examined with Spearman’s test. All tests were 2-tailed, and P-values ≤0.05 were considered significant, while P-values <0.1 and >0.05 were considered a trend. A series of hierarchical regression analyses tested for specific and interactional effects of hypocretin, NPY and IL-1β on suicide risk.
Results
Changes In Plasma Levels Of NPY Between Suicide And Control Subjects
The present data showed that NPY concentrations in the plasma of suicide subjects were significantly higher than those in the plasma of control subjects (P=0.013, see Figure 1A). In addition, we observed a significant difference in NPY among controls and suicide subjects with PI and LE (K-W: P=0.043). Moreover, NPY concentrations in the plasma of suicide subjects with PI were significantly higher than those in the plasma of control subjects (P=0.039, see Figure 2A). Similarly, NPY concentrations in suicide subjects with LE were significantly elevated compared with those in control subjects (P=0.047, see Figure 2A). However, no significant difference was found between suicide subjects with PI and those with LE (P=0.606, see Figure 2C). There was no difference in NPY concentration between suicide subjects who died of violent behavioral causes and those who died of nonviolent behavioral causes (P=0.414).
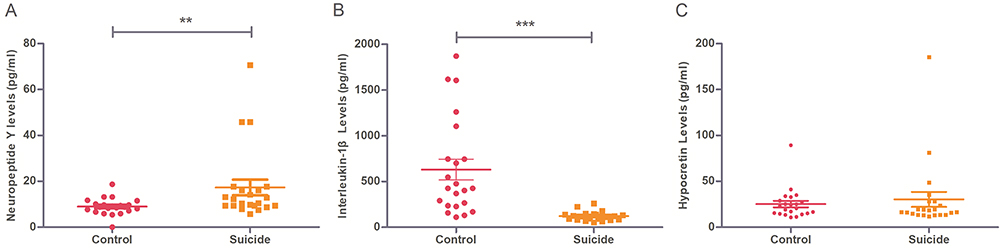 |
Figure 1 Scatter dot plots showing plasma levels of NPY, IL-1β and hypocretin between suicide (n=22) and controls (n=22). Changes in plasma levels of Neuropeptide Y (A) and Interleukin-1β (B) and hypocretin (C) from suicides (right) and controls (left). Red plots represent controls, yellow boxes represent suicides. Significance levels are indicated as **P<0.01, ***P<0.001. |
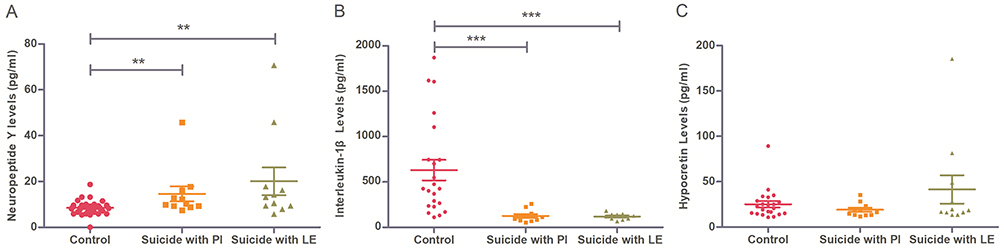 |
Figure 2 Scatter dot plots showing plasma levels of NPY, IL-1β and hypocretin between suicides with life events (LE) (n=11), suicides with psychiatric illness (PI)(n=11) and controls (n=22). Changes in plasma levels of Neuropeptide Y (A) and Interleukin-1β (B) and hypocretin (C) form suicides with life events (LE) (right), suicides with psychiatric illness (PI) (medial) and controls (left). Red plots represent controls, yellow boxes represent suicides with psychiatric illness (PI), green triangles represent suicides with life events (LE). Significance levels are indicated as **P<0.01, ***P<0.001. |
Changes In Plasma Levels Of IL-1β Between Suicide And Control Subjects
IL-1β levels in the plasma of suicide subjects were significantly lower than those in the plasma of control subjects (P<0.001, see Figure 1B). We observed a significant difference in IL-1β levels among control and suicide subjects with PI and those with LE (K-W: P<0.001). Furthermore, IL-1β concentrations in the plasma of suicide subjects with PI (P<0.001) or suicide subjects with LE (P<0.001) were significantly lower than those of control subjects, while there was no significant difference in IL-1β concentrations between suicide subjects with PI and those with LE (P=0.756, see Figure 2B). In addition, there was no difference in IL-1β concentrations between suicide subjects who died of violent behavioral causes and those who died of nonviolent behavioral causes (P=1.000).
Changes In Plasma Levels Of Hypocretin Between Suicide And Control Subjects
There was no significant difference in hypocretin concentration between control and suicide subjects (P=0.526, see Figure 1C). There was no significant difference in hypocretin levels between controls and suicide subjects with PI and those with LE (K-W: P=0.449, see Figure 2C). Moreover, no difference was found in hypocretin-1 between suicide subjects who died of violent behavioral causes and those who died of nonviolent behavioral causes (P=0.841).
Correlations Between Different Serum Peptide Levels And General Information
We found significant positive correlations between hypocretin and NPY in control subjects (P=0.014, rho=0.555), while there was no relation between age, NPY or IL-1β and hypocretin in suicide subjects (all P>0.274). In addition, there were no significant correlations among age, NPY and IL-1β in control subjects (all P>0.446).
There was no significant correlation between age, NPY or IL-1β levels and hypocretin in suicide subjects with PI (all P>0.21). Furthermore, we did not observe a significant correlation between age, NPY or IL-1β and hypocretin in suicide subjects with LE (all P>0.162)
Discussion
In the present study, we documented and compared the plasma concentrations of biological patterns in human suicide death cases. In this study, we showed that plasma NPY and IL-1β levels were correlated with suicidal behavior. Plasma NPY concentrations were significantly higher in suicide subjects than those in control subjects. Furthermore, higher NPY level concentrations were found both in suicide subjects with PI and in suicide subjects with LE than those in control subjects. In contrast, IL-1β concentrations were decreased in suicide subjects compared with those in control subjects, and there were lower IL-1β concentrations both in suicide subjects with PI and in suicide subjects with LE than those in control subjects. Our results suggested that NPY and IL-1β were related to suicidal behavior rather than suicide causes or suicide methods.
The present study showed increased levels of NPY concentrations in the plasma of suicide subjects, which may indicate that NPY affects neurobehavioral processes relevant to suicide.
Previous studies have shown that dysregulation of the NPY system plays a role in psychiatric diseases such as depression, anxiety and posttraumatic stress disorder (PTSD).7,23,24 Irwin et al found that plasma NPY was elevated in depressed patients.25 This finding indicated that NPY may play a role not only in depression but also in suicidal behavior.26 In a study of personality disorder, CSF-NPY level was positively correlated with a higher degree of impulsive aggression in personality, which may ultimately lead to suicide attempts.8 Schizophrenia patients showed an increase in CSF-NPY concentrations compared with controls,27 which may be related to higher impulsivity and aggression scores.28,29
There were several possible explanations for higher NPY levels in people who died by suicide. Most studies showed elevated NPY levels in depressive patients instead of other psychiatric illnesses. Only 7 of 22 people who died by suicide were depressed in the present study. In addition, impulsivity is thought to be positively correlated with suicidal behavior,30,31 which can explain our findings. Since NPY levels increased during activity as a result of enhanced sympathetic nerve stimulation,32 it is reasonable that the plasma NPY level in suicide subjects was elevated at the time they were committing suicide.
The present study investigated the IL-1β plasma levels in people who died by suicide, and we found that they were decreased in people who died by suicide and that this result may have been resulted from elevated NPY levels. A rodent study showed that if NPY was intraperitoneally injected into rats, it could lead to a decrease in IL-1β levels in the serum.33 A cell study also reported that NPY inhibited the IL-1β signaling pathway via nitric oxide production in microglia,34 which indicated that NPY may inhibit the release of IL-1β. A previous study showed conflicting data on IL-1β in people who attempted suicide. IL-1β levels were increased in those who attempted suicide with or without psychiatric illness compared to those in controls. IL-1β levels in BD patients with suicide risk were elevated compared to those in control patients.11 This finding is consistent with postmortem studies that showed that IL-1β protein and mRNA expression levels were significantly higher in several brain areas of people who died by suicide with a history of major depressive disorder (MDD) or bipolar disorder (BPD) than in brain areas of controls.12,35 However, Gabbay et al claimed that plasma IL-1β levels among suicidal teenagers with MDD, suicidal adolescents with MDD, nonsuicidal adolescents with MDD and healthy controls showed no difference.36 In addition, studies reported that psychiatric patients with suicide attempts and controls were found to have no significant difference in plasma IL-1β.37 A postmortem study showed no changes in IL-1β-mRNA in Brodmann’s area 11 of suicide subjects compared with controls.38 The studies mentioned above indicate that plasma IL-β levels are different in those who attempt suicide and people who died by suicide.
The hypocretinergic system has been linked to depression, schizophrenia and suicide.15,16,39,40 The relationship between hypocretin and suicide is still controversial. The present study showed no significant difference in plasma hypocretin between control and suicide subjects as well as between control and suicide subjects with PI and those with LE. A study reported that CSF-hypocretin-1 levels in patients with MDD did not differ compared to those in healthy control patients.41 Our previous postmortem study demonstrated a sex difference in that male depressive patients who had died by suicide showed significantly increased anterior cingulate cortex Hcrt-receptor-2-mRNA expression compared to male control.39
In the present study, there was no significant correlation between the plasma level of NPY and hypocretin. Both the appetite-stimulating peptides Hypocretin-1 and neuropeptide Y (NPY) are known to play a critical role in food intake.42 A previous study has provided evidence that, in goldfish, NPY-induced appetite is mediated by hypocretin-1, suggesting that the two peptides share a functional relationship for regulation of feeding.43 However Hypocretin-1 is involved in activation of the HPA axis, and that these effects could be mediated via the release of NPY in rats.44 And the mediation of hypocretin-1 play a role in thermoregulation, and its hypothermic effect seems to be mediated at least partially by NPY.45 While in clinical study, there was rarely plasma or CSF level of both NPY and hypocretin study, the plasma level of NPY and hypocretin showed different changes in obese women.46 Even the effect of hypocretin-1 might be mediated by NPY but the plasma level does not show consist changes.
We did not find a sex difference in the present study, although a final conclusion on this phenomenon should be based upon a larger sample size. Mental patients with suicide attempts showed a negative correlation between CSF-hypocretin-1 and some negative symptoms.15 However, another study showed that CSF-hypocretin-1 levels in mental patients were significantly increased at 6 and 12 months after a suicide attempt.16 Interestingly, CSF-hypocretin levels in depressed patients were significantly lower than those in adjustment disorder and dysthymia patients.21
Some concerns regarding the present postmortem study should be mentioned. The suicide subject data in the present study involved postmortem plasma, which raises the question of whether a postmortem delay might have confounded our results. All samples were collected by professional forensic personnel and then quickly treated using a standardized protocol and immediately frozen in −80°C. There were no significant correlations between storage time and any of the factor scores. However, we cannot completely rule out the possibility that postmortem delay could have influenced the biomarkers, although we believe that we took appropriate measures to minimize this risk.
Secondly, one of the inherent potential confounding factors in a postmortem study is medication use. The general information and use of antipsychotics and antidepressants in suicide subjects were provided by family members and policemen. Olanzapine was negatively correlated with serum NPY levels in schizophrenia patients.47 Duloxetine decreased serum IL-1β levels in depressed patients who responded to duloxetine, while increased IL-1β levels were found in those who did not respond to duloxetine.48 Venlafaxine increased serum NPY levels24 and reduced IL-1β in depressed patients;49 chlorpromazine may not have influenced plasma IL-1β levels in healthy volunteers,50 and animal experiments indicated that chlorpromazine reduced NPY-like immunoreactivity in the nucleus accumbens.51 In the present study, 4 of 22 suicide subjects had used medicine, including olanzapine, duloxetine, venlafaxine and chlorpromazine, in the past. However, significant differences remained (NPY P=0.004; IL-1β P<0.001; hypocretin P=0.362) when we excluded the data of the four suicide subjects who took these medications.
Thirdly, if we consider suicide methods such as hanging, jumping, drowning, poisoning and CO poisoning as different groups, the suicide method may influence the blood levels of who died by suicide. There was no significant difference in NPY, IL-1β and hypocretin levels among these groups (NPY P=0.513; IL-1β P=154; hypocretin P=0.480). Carbon monoxide may act as an independent factor to influence NPY and IL-1β. Studies have demonstrated that CO is a negative regulator of the secretion of IL-1β in vitro and in vivo, and it is consistent with our results. IL-1β levels of suicide subjects who died of CO were lower than average levels. When we excluded the two data points, the significant difference between suicide and control subjects remained.
Limitation
The controls were healthy people rather than healthy individuals who accidentally died. Given the heterogeneity of cause of death, sample size is relatively small. Verification experiment such as Western blot on brain tissue is needed in the future. Study of Hypocretin, Plasma of NPY and IL-1β level from people who have suicide idea or suicide attempt are also needed in the future. And more advanced techniques to compare the relative contributions of each biomarker to suicide risk within the suicide group.
Conclusion
Our results suggest that plasma NPY and IL-1β were related with suicide behavior rather than to suicide causes or suicide method. Specific combinations of plasma biomarkers may discriminate between types of suicidal behaviors and indicate increased risk for future suicide attempts.
Acknowledgments
Jing Lu and Shangda Li are co-first authors. We would like to thank the families of the deceased for the donations of plasma and their time and effort devoted to the consent process and interviews, and the staff in Institute of Criminal Science and Technology for their assistance.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Preventing Suicide: A Global Imperative; 2014. Available from: http://www.who.int/mental_health/suicide-prevention/world_report_2014/en/.
2. Hawton K, van Heeringen K. Suicide. Lancet. 2009;373(9672):1372–1381. doi:10.1016/S0140-6736(09)60372-X
3. Gananca L, Oquendo MA, Tyrka AR, Cisneros-Trujillo S, Mann JJ, Sublette ME. The role of cytokines in the pathophysiology of suicidal behavior. Psychoneuroendocrinology. 2016;63:296–310. doi:10.1016/j.psyneuen.2015.10.008
4. Harro J. CCK and NPY as anti-anxiety treatment targets: promises, pitfalls, and strategies. Amino Acids. 2006;31(3):215–230. doi:10.1007/s00726-006-0334-x
5. Serafini G, Pompili M, Lindqvist D, Dwivedi Y, Girardi P. The role of neuropeptides in suicidal behavior: a systematic review. Biomed Res Int. 2013;2013:687575. doi:10.1155/2013/687575
6. Widdowson PS, Ordway GA, Halaris AE. Reduced neuropeptide Y concentrations in suicide brain. J Neurochem. 1992;59(1):73–80. doi:10.1111/j.1471-4159.1992.tb08877.x
7. Heilig M, Zachrisson O, Thorsell A, et al. Decreased cerebrospinal fluid neuropeptide Y (NPY) in patients with treatment refractory unipolar major depression: preliminary evidence for association with preproNPY gene polymorphism. J Psychiatr Res. 2004;38(2):113–121.
8. Coccaro EF, Lee R, Liu T, Mathe AA. Cerebrospinal fluid neuropeptide Y-like immunoreactivity correlates with impulsive aggression in human subjects. Biol Psychiatry. 2012;72(12):997–1003. doi:10.1016/j.biopsych.2012.07.029
9. van de Veerdonk FL, Netea MG. New insights in the immunobiology of IL-1 family members. Front Immunol. 2013;4:167. doi:10.3389/fimmu.2013.00167
10. Patterson SL. Immune dysregulation and cognitive vulnerability in the aging brain: interactions of microglia, IL-1beta, BDNF and synaptic plasticity. Neuropharmacology. 2015;96(Pt A):11–18. doi:10.1016/j.neuropharm.2014.12.020
11. Monfrim X, Gazal M, De Leon PB, et al. Immune dysfunction in bipolar disorder and suicide risk: is there an association between peripheral corticotropin-releasing hormone and interleukin-1beta? Bipolar Disord. 2014;16(7):741–747. doi:10.1111/bdi.12214
12. Pandey GN, Rizavi HS, Ren X, et al. Proinflammatory cytokines in the prefrontal cortex of teenage suicide victims. J Psychiatr Res. 2012;46(1):57–63. doi:10.1016/j.jpsychires.2011.08.006
13. Grudet C, Malm J, Westrin A, Brundin L. Suicidal patients are deficient in vitamin D, associated with a pro-inflammatory status in the blood. Psychoneuroendocrinology. 2014;50:210–219. doi:10.1016/j.psyneuen.2014.08.016
14. Nollet M, Leman S. Role of orexin in the pathophysiology of depression: potential for pharmacological intervention. CNS Drugs. 2013;27(6):411–422. doi:10.1007/s40263-013-0064-z
15. Brundin L, Petersen A, Bjorkqvist M, Traskman-Bendz L. Orexin and psychiatric symptoms in suicide attempters. J Affect Disord. 2007;100(1–3):259–263. doi:10.1016/j.jad.2006.10.019
16. Brundin L, Bjorkqvist M, Traskman-Bendz L, Petersen A. Increased orexin levels in the cerebrospinal fluid the first year after a suicide attempt. J Affect Disord. 2009;113(1–2):179–182. doi:10.1016/j.jad.2008.04.011
17. Matsuda K, Matsumura K, Shimizu SS, Nakamachi T, Konno N. Neuropeptide Y-induced orexigenic action is attenuated by the orexin receptor antagonist in bullfrog larvae. Front Neurosci. 2017;11:176. doi:10.3389/fnins.2017.00176
18. Fu LY, Acuna-Goycolea C, van den Pol AN. Neuropeptide Y inhibits hypocretin/orexin neurons by multiple presynaptic and postsynaptic mechanisms: tonic depression of the hypothalamic arousal system. J Neurosci. 2004;24(40):8741–8751. doi:10.1523/JNEUROSCI.2268-04.2004
19. Grossberg AJ, Zhu X, Leinninger GM, et al. Inflammation-induced lethargy is mediated by suppression of orexin neuron activity. J Neurosci. 2011;31(31):11376–11386. doi:10.1523/JNEUROSCI.2311-11.2011
20. Oquendo MA, Perez-Rodriguez MM, Poh E, et al. Life events: a complex role in the timing of suicidal behavior among depressed patients. Mol Psychiatry. 2014;19(8):902–909. doi:10.1038/mp.2013.128
21. Brundin L, Bjorkqvist M, Petersen A, Traskman-Bendz L. Reduced orexin levels in the cerebrospinal fluid of suicidal patients with major depressive disorder. Eur Neuropsychopharmacol. 2007;17(9):573–579. doi:10.1016/j.euroneuro.2007.01.005
22. Traskman L, Asberg M, Bertilsson L, Sjostrand L. Monoamine metabolites in CSF and suicidal behavior. Arch Gen Psychiatry. 1981;38(6):631–636. doi:10.1001/archpsyc.1981.01780310031002
23. Schmeltzer SN, Herman JP, Sah R. Neuropeptide Y (NPY) and posttraumatic stress disorder (PTSD): a translational update. Exp Neurol. 2016;284(Pt B):196–210. doi:10.1016/j.expneurol.2016.06.020
24. Ozsoy S, Olguner Eker O, Abdulrezzak U. The effects of antidepressants on neuropeptide Y in patients with depression and anxiety. Pharmacopsychiatry. 2016;49(1):26–31. doi:10.1055/s-0035-1565241
25. Irwin M, Brown M, Patterson T, Hauger R, Mascovich A, Grant I. Neuropeptide Y and natural killer cell activity: findings in depression and alzheimer caregiver stress. Faseb J. 1991;5(15):3100–3107. doi:10.1096/fasebj.5.15.1743441
26. Roy A. Neuropeptides in relation to suicidal behavior in depression. Neuropsychobiology. 1993;28(4):184–186. doi:10.1159/000119021
27. Peters J, Van Kammen DP, Gelernter J, Yao J, Shaw D. Neuropeptide Y-like immunoreactivity in schizophrenia. Relationships with clinical measures. Schizophr Res. 1990;3(5–6):287–294. doi:10.1016/0920-9964(90)90012-v
28. Nolan KA, D’Angelo D, Hoptman MJ. Self-report and laboratory measures of impulsivity in patients with schizophrenia or schizoaffective disorder and healthy controls. Psychiatry Res. 2011;187(1–2):301–303. doi:10.1016/j.psychres.2010.10.032
29. Harrison A, Genders R, Davies H, Treasure J, Tchanturia K. Experimental measurement of the regulation of anger and aggression in women with anorexia nervosa. Clin Psychol Psychother. 2011;18(6):445–452. doi:10.1002/cpp.726
30. Liu ZZ, Chen H, Bo QG, et al. Psychological and behavioral characteristics of suicide attempts and non-suicidal self-injury in Chinese adolescents. J Affect Disord. 2018;226:287–293. doi:10.1016/j.jad.2017.10.010
31. Alasaarela L, Hakko H, Riala K, Riipinen P. Association of self-reported impulsivity to nonsuicidal self-injury, suicidality, and mortality in adolescent psychiatric inpatients. J Nerv Ment Dis. 2017;205(5):340–345. doi:10.1097/NMD.0000000000000655
32. Zukowska-Grojec Z, Wahlestedt C. Origin and actions of neuropeptide Y in the cardiovascular system. In: Colmers WF, Wahlestedt C, editors. The Biology of Neuropeptide Y and Related Peptides. Totowa, NJ: Humana Press; 1993:315–388.
33. Oztas B, Sahin D, Kir H, et al. The effect of leptin, ghrelin, and neuropeptide-Y on serum Tnf-alpha, Il-1beta, Il-6, Fgf-2, galanin levels and oxidative stress in an experimental generalized convulsive seizure model. Neuropeptides. 2017;61:31–37. doi:10.1016/j.npep.2016.08.002
34. Ferreira R, Santos T, Viegas M, et al. Neuropeptide Y inhibits interleukin-1beta-induced phagocytosis by microglial cells. J Neuroinflammation. 2011;8:169. doi:10.1186/1742-2094-8-72
35. Pandey GN. Inflammatory and innate immune markers of neuroprogression in depressed and teenage suicide brain. Mod Trends Pharmacopsychiatry. 2017;31:79–95. doi:10.1159/000470809
36. Gabbay V, Klein RG, Guttman LE, et al. A preliminary study of cytokines in suicidal and nonsuicidal adolescents with major depression. J Child Adolesc Psychopharmacol. 2009;19(4):423–430. doi:10.1089/cap.2008.0140
37. Melhem NM, Munroe S, Marsland A, et al. Blunted HPA axis activity prior to suicide attempt and increased inflammation in attempters. Psychoneuroendocrinology. 2017;77:284–294. doi:10.1016/j.psyneuen.2017.01.001
38. Tonelli LH, Stiller J, Rujescu D, et al. Elevated cytokine expression in the orbitofrontal cortex of victims of suicide. Acta Psychiatr Scand. 2008;117(3):198–206. doi:10.1111/j.1600-0447.2007.01128.x
39. Lu J, Zhao J, Balesar R, et al. Sexually dimorphic changes of hypocretin (orexin) in depression. EBioMedicine. 2017;18:311–319. doi:10.1016/j.ebiom.2017.03.043
40. Chien YL, Liu CM, Shan JC, et al. Elevated plasma orexin A levels in a subgroup of patients with schizophrenia associated with fewer negative and disorganized symptoms. Psychoneuroendocrinology. 2015;53:1–9. doi:10.1016/j.psyneuen.2014.12.012
41. Schmidt FM, Arendt E, Steinmetzer A, et al. CSF-hypocretin-1 levels in patients with major depressive disorder compared to healthy controls. Psychiatry Res. 2011;190(2–3):240–243. doi:10.1016/j.psychres.2011.06.004
42. Akimoto-Takano S, Sakurai C, Kanai S, Hosoya H, Ohta M, Miyasaka K. Differences in the appetite-stimulating effect of orexin, neuropeptide Y and ghrelin among young, adult and old rats. Neuroendocrinology. 2005;82(5–6):256–263. doi:10.1159/000092754
43. Volkoff H, Peter RE. Interactions between orexin A, NPY and galanin in the control of food intake of the goldfish, carassius auratus. Regul Pept. 2001;101(1–3):59–72. doi:10.1016/s0167-0115(01)00261-0
44. Russell SH, Small CJ, Dakin CL, et al. The central effects of orexin-A in the hypothalamic-pituitary-adrenal axis in vivo and in vitro in male rats. J Neuroendocrinol. 2001;13(6):561–566.
45. Jaszberenyi M, Bujdoso E, Kiss E, Pataki I, Telegdy G. The role of NPY in the mediation of orexin-induced hypothermia. Regul Pept. 2002;104(1–3):55–59. doi:10.1016/s0167-0115(01)00339-1
46. Baranowska B, Wolinska-Witort E, Martynska L, Chmielowska M, Baranowska-Bik A. Plasma orexin A, orexin B, leptin, neuropeptide Y (NPY) and insulin in obese women. Neuro Endocrinol Lett. 2005;26(4):293–296.
47. Raposo NR, Ferreira AS, Gattaz WF. Body mass index increase, serum leptin, adiponectin, neuropeptide Y and lipid levels during treatment with olanzapine and haloperidol. Pharmacopsychiatry. 2011;44(5):169–172. doi:10.1055/s-0031-1280793
48. Fornaro M, Rocchi G, Escelsior A, Contini P, Martino M. Might different cytokine trends in depressed patients receiving duloxetine indicate differential biological backgrounds. J Affect Disord. 2013;145(3):300–307. doi:10.1016/j.jad.2012.08.007
49. Chen CY, Yeh YW, Kuo SC, et al. Differences in immunomodulatory properties between venlafaxine and paroxetine in patients with major depressive disorder. Psychoneuroendocrinology. 2018;87:108–118. doi:10.1016/j.psyneuen.2017.10.009
50. Bleeker MW, Netea MG, Kullberg BJ, Van der Ven-Jongekrijg J, Van der Meer JW. The effects of dexamethasone and chlorpromazine on tumour necrosis factor-alpha, interleukin-1 beta, interleukin-1 receptor antagonist and interleukin-10 in human volunteers. Immunology. 1997;91(4):548–552. doi:10.1046/j.1365-2567.1997.00285.x
51. Obuchowicz E, Turchan J. Effects of acute or long-term treatment with chlorpromazine, haloperidol or sulpiride on neuropeptide Y-like immunoreactivity concentrations in the nucleus accumbens of rat. Eur Neuropsychopharmacol. 1999;9(1–2):51–59.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.