Back to Journals » Clinical Ophthalmology » Volume 16
Changes in Noncontact Meibography and Noninvasive Tear Break-Up Time Test with Contact Lenses Usage
Authors Fattoh R ![]() , Mounir A
, Mounir A ![]() , Anbar M
, Anbar M ![]() , Mohammed OA
, Mohammed OA ![]()
Received 18 February 2022
Accepted for publication 6 April 2022
Published 5 May 2022 Volume 2022:16 Pages 1427—1437
DOI https://doi.org/10.2147/OPTH.S362307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Reham Fattoh,1 Amr Mounir,2 Mohamed Anbar,2 Osama Ali Mohammed2
1Ophthalmology Department, Sohag Ophthalmology Hospital, Sohag, Egypt; 2Ophthalmology Department, Sohag Faculty of Medicine, Sohag University, Sohag, Egypt
Correspondence: Amr Mounir, Ophthalmology Department, Sohag Faculty of Medicine, Sohag University, Almohafza Street, Mailbox: 8251, Sohag, Egypt, Tel +20 1005026170, Email [email protected]
Purpose: The study aimed to determine changes detected by noncontact meibography and noninvasive break-up time test (NIBUT) in individuals with regular use of soft contact lenses and compare these findings with irregular soft contact lenses wearers who not compliant with them and non-wearers control group.
Patients and Methods: A prospective nonrandomized case-control study in which individuals were recruited and distributed into three groups: Group A (regular contact lens wearers), group B (irregular contact lens wearers), and group C (non-wearers). Ocular Surface Disease Index (OSDI) was obtained. Noncontact meibography and noninvasive tear break-up time were measured without lenses on using Sirius® Scheimpflug Camera.
Results: One hundred sixty-six eyes of 83 individuals were included; 36 eyes in group A, 50 eyes in group B, and 80 eyes in group C. The mean total meiboscore was 1.99, 1.61, and 1.28, respectively. The mean meibograde was 3.03, 2.86, and 1.99, respectively. Noninvasive break-up time (NIF-BUT) was 8.42, 11.76, and 13.57 seconds, respectively.
Conclusion: There is a difference in OSDI score, meibomian score, and break-up time between different study groups. The study results show that there are trends in lens wearers and non-lens wearers. This is useful for the field to understand the differences between lens wearers and non-lens wearers.
Keywords: noncontact meibography, noninvasive break-up time, soft contact lenses
Introduction
Dry eye disease (DED) is an increasing public health issue and one of the most common reasons for seeking ophthalmological advice.1 Its symptoms in the young have been associated with using digital devices, contact lens wear, and refractive surgeries.2–5
Contact lens-related dry eye is a poorly understood but pervasive clinical problem. Moreover, the ability to wear contact lenses successfully is affected by the quality of the precorneal tear film.3 Therefore, a mechanical clarification can be made for contact lens-related dry eye by augmented tear film evaporation resulting in increased tear film osmolality. In a study of Kim et al,4 They showed that increased prelens tear film evaporation rate results in increased prelens and postlens tear film.
Also, in a study of Dumbleton,6 they found that dryness appears to diminish when lenses are not used and shows changes during the wearing period. Contact lens’ frequency associated with the dry eye is about 50%.7 Evidence from previous studies contributes to the consensus that contact lens discomfort is the main reason for discontinuation of wear and that the most common type of discomfort is dryness.8 In addition, it causes visual disturbance and blurred vision due to irregular tear film.
Meibography is a valuable imaging tool that allows for the direct clinical evaluation of meibomian gland dysfunction (MGD) which is widely believed to be the origin of evaporative DED. It is a specialized imaging study developed exclusively to visualize the morphology of meibomian glands in vivo directly.8 Researchers can classify MGD based on the secretion rate into low delivery (obstructive or hyposecretion) and high delivery (hypersecretory) conditions, with either primary or secondary underlying etiological explanations.9 MGD is more commonly associated with the evaporative DED than the aqueous deficient dry eye.10
The two principal meibography techniques are contact transillumination and the most recent noncontact meibography, which allows for noninvasive evaluation of the morphological abnormalities and quantification of meibomian gland loss (MGL).11
The present study aimed to determine changes detected by noncontact meibography and noninvasive break-up time test (NIBUT) in individuals with regular use of soft contact lenses and compare these findings with irregular soft contact lenses wearers who not compliant with them and non-wearers control group.
Patients and Methods
This paper presents a prospective nonrandomized case-control study conducted in Sohag Future Center for Corneal and Refractive Surgeries, Sohag, Egypt, between July 2020 and June 2021. All participants agreed to sign a written informed consent about the planned procedure, nature, and aim of the study. Additionally, the approval of the ethical committee of Sohag Faculty of Medicine was fulfilled. The study followed the tenets of the Declaration of Helsinki. One hundred sixty-six eyes of 83 subjects aged 18–35 years were recruited and distributed to three groups: Study group A (regular contact lenses wearers) included 36 eyes of 18 subjects, with regular and prolonged wear of soft contact lenses (average more than 25 hours/ week over the last six months); study group B (irregular contact lenses wearers who not compliant with them) included 50 eyes of 25 subjects with a history of contact lenses wear for hours less than 25 hours/ week or discontinuation of contact lenses for more than six months; control group C (non-wearers) included 80 eyes of 40 subjects matching the study group but without a previous history of contact lenses wear.
Individuals with one or more of the following conditions were excluded from the study: Previous refractive surgery, intraocular surgery or lid surgery, lid scarring or deformity, corneal scarring or vascularization, history of hard contact lenses wear, keratoconus compatible and other ectatic corneal conditions, evidence of rheumatoid arthritis, systemic lupus, scleroderma, diabetes mellitus, anti-glaucoma medications, and systemic medications (eg, antidepressants, diuretics, and anti-metabolites).
All individuals were subjected to the routine ophthalmic evaluation, evaluation of the eyelids, tear film, and ocular surface using slit-lamp biomicroscopy.
The 12 items of the ocular surface disease index (OSDI) questionnaire were graded on a 0–4 scale. The total OSDI score was then calculated based on the following formula: OSDI= [(sum of scores for all questions answered) × 100]/[(total number of questions answered) × 4]. The total score of OSDI ranged from 0 to 100, with higher scores representing greater disability.14
A modified Sirius® Scheimpflug Camera (C.S.O, Costruzione Strumenti Oftalmici, Florence, Italy; bon Optic VertriebsgmbH, Lübeck, Germany) with the Phoenix-Meibography Imaging software module was used to evaluate the noncontact meibography and noninvasive tear break-up time for all individuals without lenses on.
Both upper and lower eyelids were everted, and meibomian glands were visualized. First, the upper or lower eyelid was selected, then the meibomian glands were tracked in a trapezoidal area, excluding lid areas that were not completely everted. The area of MG loss was defined as the percentage of the area without visible glands concerning the total visible tarsal area. It was automatically calculated and graded once the flag icon was clicked. The partial or complete loss of meibomian glands was scored using subsequent grades (meibo-score) in each eyelid: grade 0 (no loss of meibomian glands), grade 1 (the lost area was less than or equal to 25% of the total area of meibomian glands), grade 2 (the lost area was between 26% and 50% of the total area of meibomian glands), grade 3 (the lost area was between 51% and 75% of the total area of meibomian glands), and grade 4 (the lost area was over 75% of the total area of meibomian glands). The total meiboscore was calculated by the summation of meiboscore for both upper and lower eyelids.
The meibograde system involved gland distortion with an abnormal gland to tarsus ratio, tortuous glands, gland shortening, and/or discordant patterning depending on previously studied histopathological changes. A 0–3 scale was assigned to each category according to the involvement of the eyelid: 0 means no significant eyelid involvement, 1 means involvement less than 33%, 2 means involvement ranging from 33% to 66%, and 3 means involvement over 66%.
The first and the average noninvasive break-up time (NIF-BUT and NIAvg-BUT, respectively) were measured in seconds without contact-lens wear. Each subject was requested to blink twice and then keep their eyes open as long as possible during the measurement of the NIKBUT. The first break-up was automatically detected by the device software. The corresponding time indicated the NIF-BUT, and the average time of all break-up incidents on the cornea was documented as the NIAvg-BUT. The maximum time for measurement was 17 seconds, but it could be adjusted.
The Statistical Package for the Social Sciences version 17.0 (SPSS Inc, Chicago, Illinois, USA) was utilized to analyze the data statistically. The independent t-test was used to assess the statistical significance among groups in predetermined parameters. Statistical difference was considered significant if the P value was less than 0.05 and highly significant if the P value was less than 0.01. A linear Pearson correlation coefficient was used for normally distributed values, and the linear Spearman correlation coefficient was used for non-normally distributed values.
Results
One hundred sixty-six eyes of 83 subjects (both eyes for each subject) were included. They were divided into three groups; group A (regular contact lenses wearers) included 36 eyes (21.7%), group B (irregular contact lenses wearers) included 50 eyes (30.1%), and group C (Non-wearers), as a control group, included 80 eyes (48.2%).
Demographic Characteristics
A statistically significant difference (p value 0.01) was detected in gender distribution, as shown in Table 1. Post-Hoc ANOVA multiple comparison test showed that the significant difference was between group C on the one hand and the other two groups, on the other hand. However, there was no significant difference between group A and group B. The three groups did not show any significant difference in the mean age (p value 0.07, see Table 1).
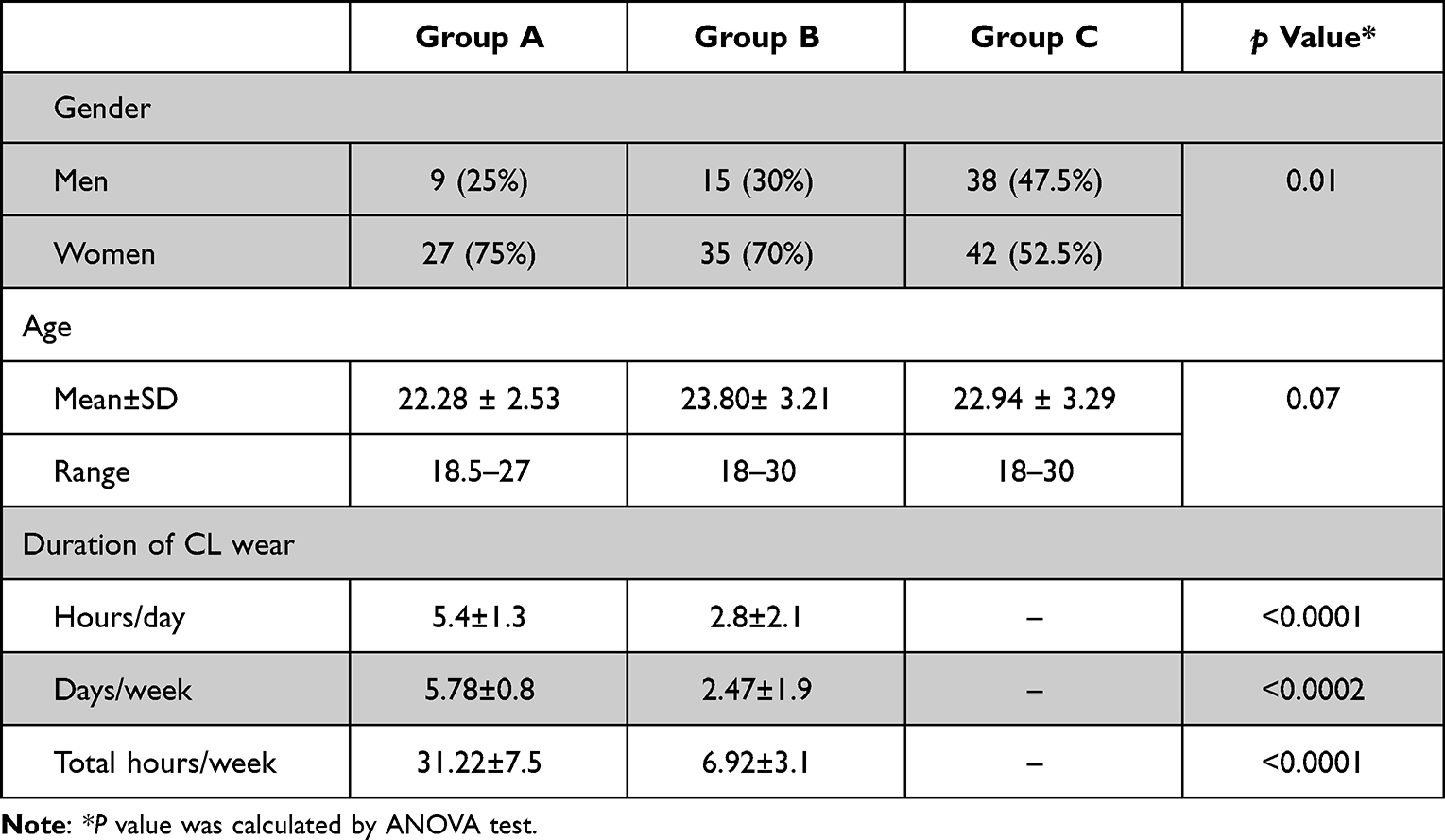 |
Table 1 Demographic Characteristics and CL Wear Duration |
Duration of Contact Lens Wear
Both groups A and B showed a high statistically significant difference (p value <0.01), regarding the duration of contact lens wear, including daily duration and total duration per week. The total duration of CL wear in group A was 31.22±7.5 hours/week compared to only 6.92±3.1 hours/week in group B (see Table 1).
OSDI
There was a statistically significant difference (p value 0.03) in the mean OSDI between the three groups. Group A recorded the highest OSDI, followed by group B, while group C had the lowest OSDI (see Table 2).
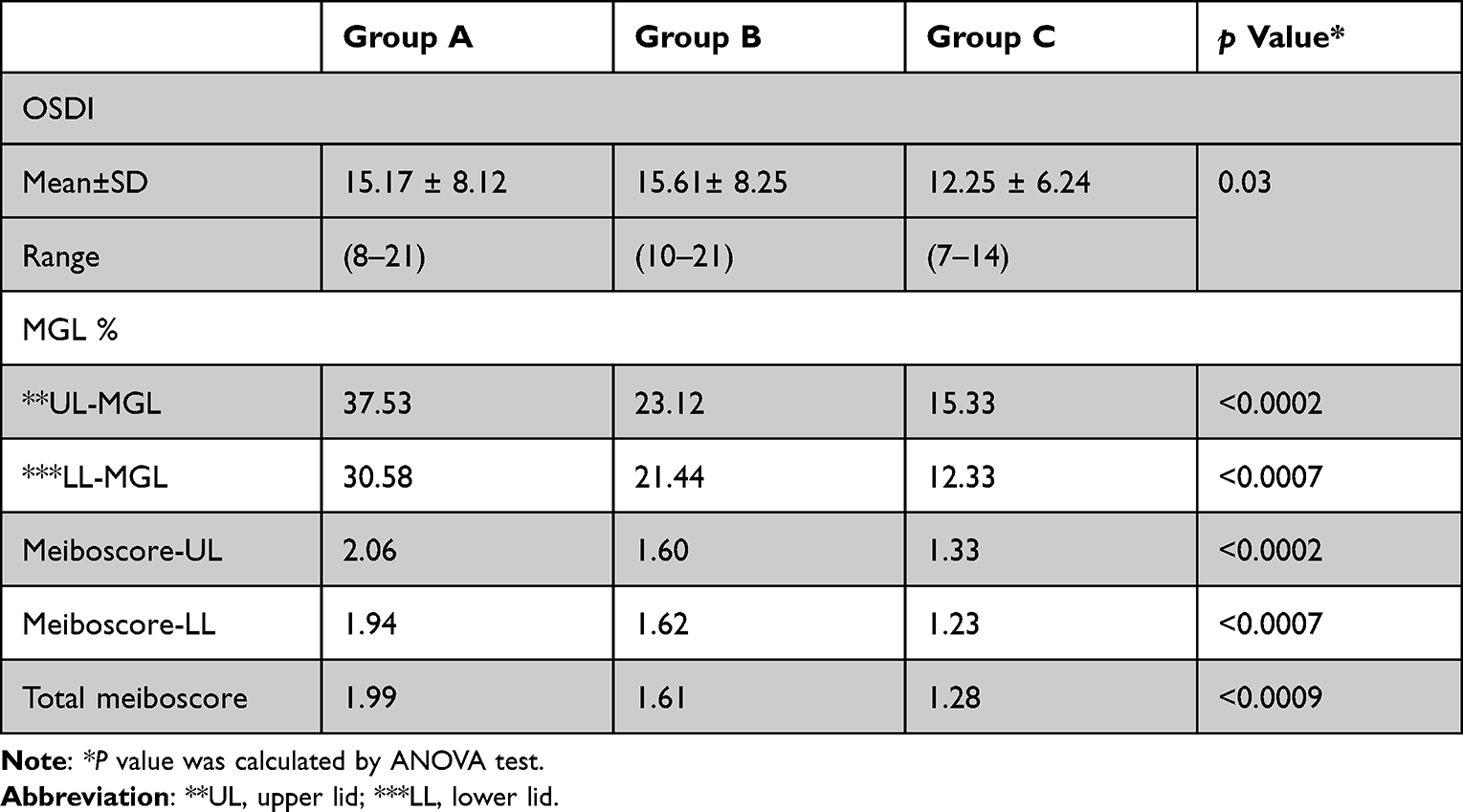 |
Table 2 The Difference Among the Three Groups Regarding the OSDI, MGL, and Meiboscore |
Meiboscore
The results showed a high statistically significant difference (p value <0.01) among the three groups in the average meiboscore of both upper and lower eyelids and also in the total meiboscore. Within each group, there was no significant difference in the mean percentage of MGL between the upper and the lower eyelids (p1 value >0.05). The mean total meiboscore was 1.99, 1.61, and 1.28 for groups A, B, and C, respectively (see Table 2).
In group A, an equal number of eyes (10 eyes, 27.7%) in both upper and lower eyelids had grade I in meiboscore. However, grade II included 50% of eyes for the lower eyelids compared to 38.9% for the upper eyelids. (Figure 1) One-third of cases had grade III for the upper lid versus only 22.2% for the lower lid. In group B, only four eyes (upper lid) and one eye (lower lid) had grade III meiboscore. (Figure 2) In group C, only three eyes (upper lid) had grade III meiboscore. In all groups, no cases with grade IV were detected (see Table 3).
 |
Table 3 Distribution According to Meiboscore Grade* |
 |
Figure 1 Red area describes the area of the lower lid examined by meibography while green area shows dilatation and tortuosity of the meibomian glands Meiboscore grade II. |
 |
Figure 2 Red area describes the area of the upper lid examined by meibography while green area shows the meibomian glands loss, distortion, and tortuosity. |
Meibograde
The following table (Table 4) shows the distribution regarding the meibograde. The cases was distributed to three levels as following: 0–3, >3-6, >6-9 for both upper and lower eye lids. There was statistaically significant difference among the three groups in all three levels of meibograde. Regarding UL-meibograde, in group A more than one third of cases (36.1%) had UL-meibograde of <6-9, and 41.7% had >3-6 UL-meibograde, while in group B only 12% had meibograde of >6-9, and compared to group C where only 3.8% had the same meibograde level. Regarding LL-meibograde, half of cases of group A and more than half of cases of group B had >3-6 meibograde. However, no cases were detected in group C with meibograde more than 6 (see Table 4). Similarly, all groups showed a high significant difference in the mean total meibograde with a p value of 0.001. It was 3.03±1.66 for group A, 2.86±1.78 for group B, and 1.99±1.07 for group C (see Table 4).
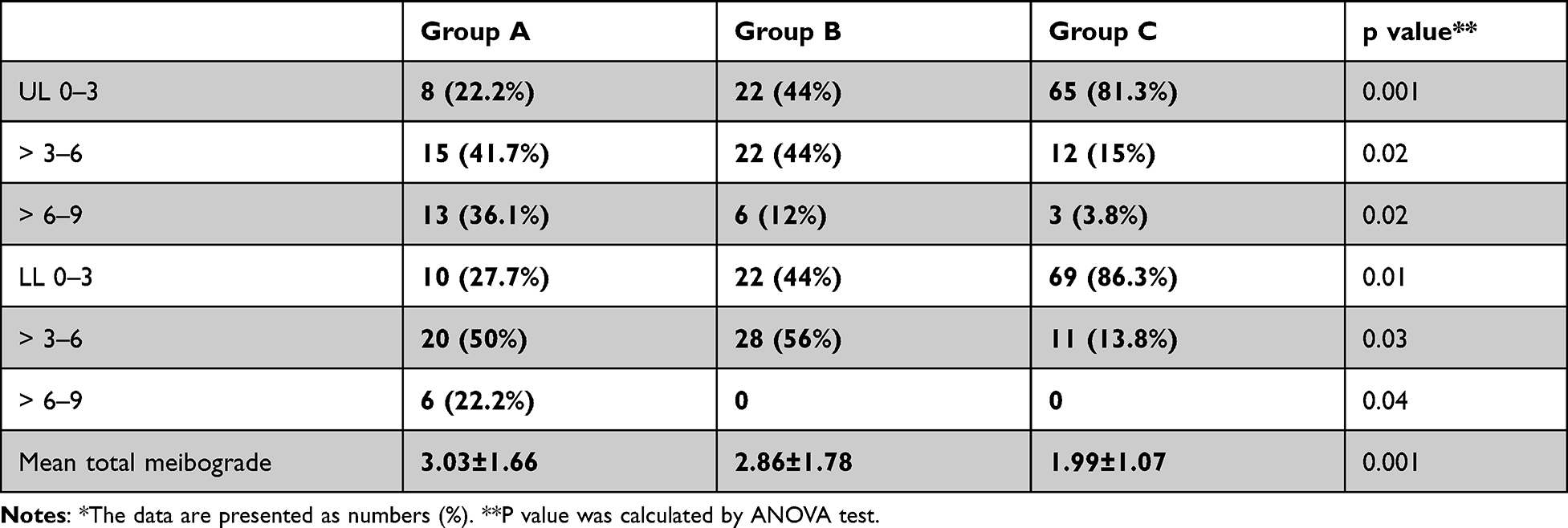 |
Table 4 Distribution According to Meibograde* |
NIF-BUT
The following table (Table 5) shows a high statistically significant difference among the three groups in the mean NIF-BUT (Figure 3A and B).
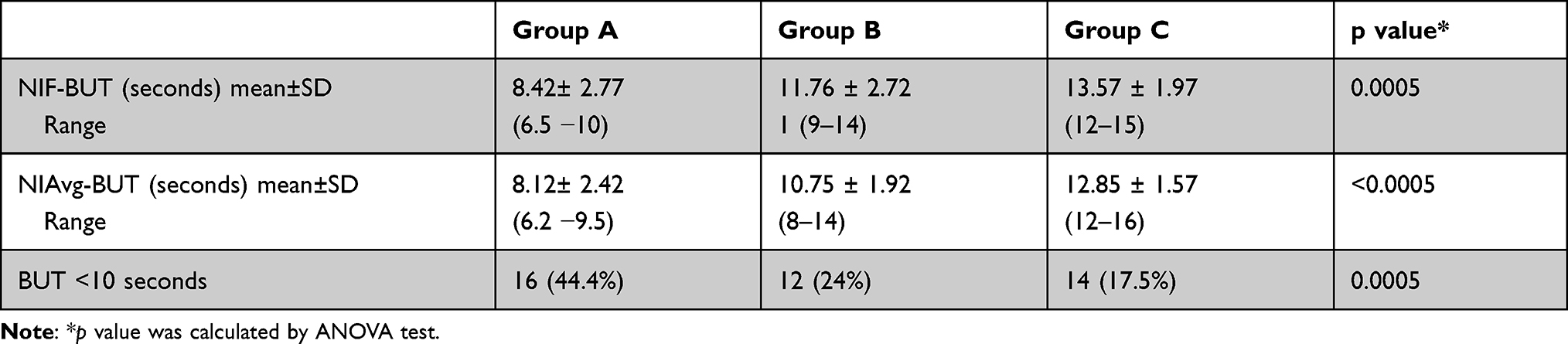 |
Table 5 The Mean NIF-BUT Among the Three Groups |
 |
Figure 3 (A) Mild affected and noninvasive break-up time test (NIF-BUT) and noninvasive average break-up time test (NIAvg-BUT) (green area shows normal break-up time of the tear film while red and orange color shows abnormal break-up time. (B) Markedly affected NIF-BUT and NIAvg-BUT |
NIAvg-BUT
The following table (Table 5) shows a high statistically significant difference among the three groups in the mean NIF-BUT (Figure 3A and B).
Table 6 shows the correlation and its significance among the different outcomes. There was a positive correlation among the duration of contact lens wear, OSDI, total meiboscore, and meibograde. In contrast, the correlation was negative between these outcomes versus both NIF-BUT and NIAvg-BUT. A significant correlation was detected between the duration of CL wear and all other outcomes except OSDI. Moreover, the total meiboscore and both NIF-BUT and NIAvg-BUT correlated significantly. Also, a high significant positive correlation was reported between NIF-BUT versus NIAvg-BUT.
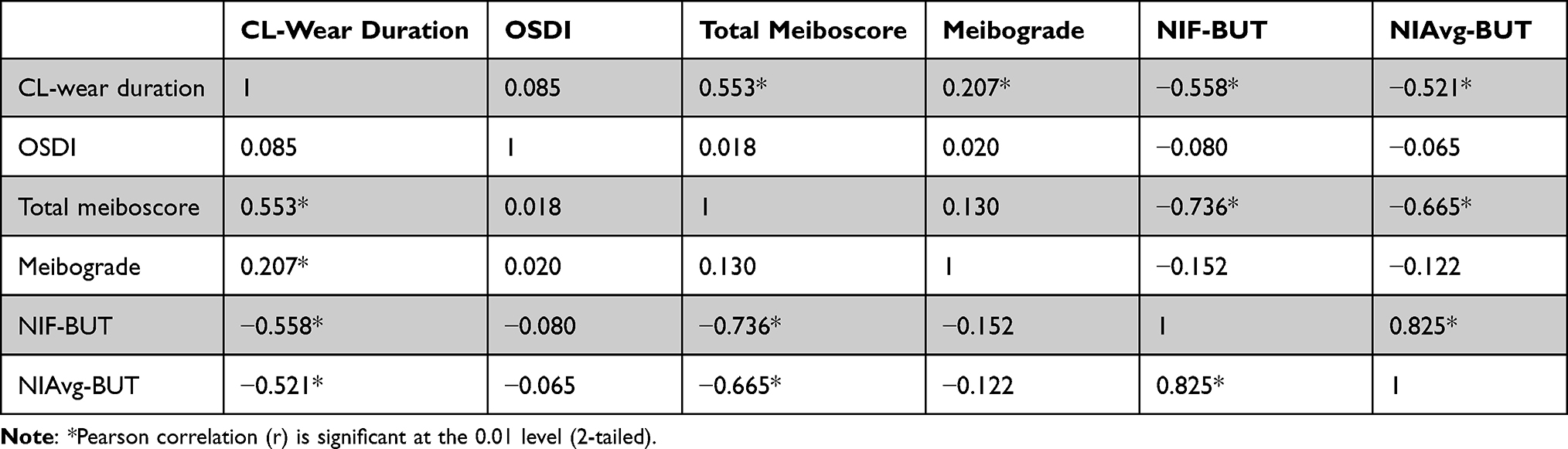 |
Table 6 Pearson Correlation Among the Studied Outcomes |
Discussion
This prospective nonrandomized case-control study aimed to determine changes detected by noncontact meibography and NIBUT in individuals with use of soft contact lenses.
Noncontact meibography detected morphological changes affecting the Meibomian glands, including dropout, shortening, dilation, and distortion. Noncontact meibography can detect detailed changes of MGs, adding a valuable tool to diagnose MGD and correctly decide the most effective management.11
The present study used a modified Sirius® Scheimpflug Camera (C.S.O, Costruzione Strumenti Oftalmici, Florence, Italy; bon Optic VertriebsgmbH, Lübeck, Germany) with the Phoenix-Meibography Imaging software module to evaluate both non-contact meibography and noninvasive tear break up-time.
Similarly, in a cross-sectional observational case series, Arita et al compared 121 contact lens wearers versus 137 non-wearers. They evaluated the meibomian glands using noncontact meibography. In addition, they measured tear production using the Schirmer I test.12
Comparatively, Pult et al evaluated the effectiveness of a near adapted infrared video security camera for noncontact meibography.13 Finis et al performed infrared meibography using Keratograph 5 M (Oculus, Wetzlar, Germany). They reported that meibography seemed insufficient as a single test for the diagnosis of MGD.14
Arita et al developed a new noninvasive mobile pen-shaped meibography system, comprising an infrared light-emitting diode as the light source and a highly sensitive complementary metal-oxide semiconductor image camera. They reported that it was a valuable tool with meibomian gland images of the same quality and quantity as the noncontact meibography system equipped with a slit lamp.15
The present study detected the correlation between contact lenses’ wear and DED. Many previous studies evaluated this correlation. For example, Llorens et al assessed the impact of daily disposable soft contact lenses on meibomian gland morphology through 12 months. They concluded that contact lens wear impacted meibomian gland morphology, and those subjects with no history of contact lens wear exhibited better meibomian gland condition than experienced wearers.16
Also, Arita et al,17 investigated the meibomian gland changes in contact lens (CL) wearers. They studied 121 eyes (39 gas permeable and 82 hydrogel lenses) compared to 137 age-matched non-CL wearers. The period of CL wear was 12.3 ± 7.2 years.18 The authors concluded that CL wearers had significantly higher MGL than age-matched non-CL-wearers.
Gu et al examined the effectiveness of using meibomian gland (MG) dropout and distortion for DED diagnosis in a young population with long-term CL wear. Seventy-three CL-wearers and 68 non-CL-wearers were enrolled. The MG dropout and distortion were calculated using noncontact meibography.18
Uçakhan et al evaluated the impact of soft CL wear on the morphology and function of the meibomian glands. One hundred seventy-three eyes of 87 soft CL wearers versus 103 eyes of 55 age-matched healthy volunteers were studied. They were classified into three groups (according to the total duration of contact lens wear): Less than three years, three to seven years, and more than seven years. OSDI, clinical findings, fluorescein staining, tear film break-up time (BUT), Schirmer I test, and meibography results were documented.19
Comparatively, Alghamdi et al investigated the effects of the duration of contact lens wear on the meibomian glands, eyelid, and tear film in CL wearers and non-wearers aged 18–35 years.20
In the present study, We found that OSDI was 15.17±8.12 and 15.61±8.25 in groups A and B, respectively, compared to only 12.25±6.24 in the control group. There was a statistically significant difference between CL wearers and non-wearers, while there was no difference related to the duration of CL wear.
Arita et al reported that CL-related allergic conjunctivitis (CLAC) was associated with increased meibomian gland distortion. Additionally, allergic reaction, rather than CL wear, appeared to be responsible for the increase in meibomian gland distortion in patients with CLAC.21
In the present study, a high significant difference was detected among the three groups for the mean meibograde. It was 3.03±1.66, 2.86±1.78, and 1.99±1.07 for groups A, B, and C, respectively.
Muhafiz et al evaluated the performance of precorneal and prelens noninvasive tear break-up time (NIBUT) measurements to determine tear instability in CL wearers. The authors concluded that precorneal NIBUT measurements might be useful in diagnosing tear instability. Pre-lens NIBUT values have not yet been capable of adequately defining the tear film dynamics in CL wearers.22
In a prospective study, Marx et al evaluated the in vivo pre-lens noninvasive drying-up time of two types of daily disposable contact lenses (DDCLs) after 12 hours of wear. They concluded that multifunctional topography allowed the objective evaluation of in vivo pre-lens tear film stability using ring mire projection.23
Molina-Martín et al evaluated the intrasession repeatability for NIBUT measurements provided by a new multi-diagnostic platform. They concluded that the new dry eye platform of the VX120+ platform evaluated provides objective automated measures of NIBUT and TMH, with an acceptable level of intrasession repeatability for clinical screening purposes.24
Pult et al analyzed the relations between meibomian gland morphology, the tear film, and the ability to predict dry eye. The authors concluded that MG scores between lids were significantly different but correlated. MG loss was significantly correlated to lipid layer thickness and stability.25
Pult evaluated the relationships between MGL and age, sex, and dry eye. Analyzing all subjects, multiple regression analyses detected that age and dry eye status (dry eye diagnosis or OSDI) but not sex were significantly related to MGL. In both non-dry eye and dry eye subjects, OSDI but not age or sex was significantly related to MGL. OSDI scores were significantly correlated with MGL, but this correlation was stronger among all subjects (r=0.536, P<0.001) and dry eye group subjects (r=0.520, P<0.001) than in the non-dry eye group subjects (r=0.275, P=0.014). Pult concluded that dry eye group subjects showed significantly increased MGL of the lower eyelid. Age and dry eye status were related to MGL of the lower eyelid, but sex was not; dry eye status was the dominant factor.26
Ozulken et al compared the outcomes of NIBUT and the other conventional dry eye tests. To evaluate the tear quality of the patients, NIBUT levels were measured by the Scheimpflug-Placido disk system (Sirius topography). The authors concluded that it is important to use a sensitive, reproducible, and noninvasive method in the evaluation of tear functions as objective and noninvasive topographic NI-BUT measurements and the minimally invasive osmolarity measurements that should be used more frequently in practice because they correlate with the measurements obtained by invasive methods.27
In a retrospective study, Lee et al evaluated the clinical symptoms of patients with dry eyes based on OSDI and analyzed the relationship between OSDI and various ocular surface parameters. The authors concluded that noninvasive examinations, such as noninvasive keratograph break-up time and interferometry of LLT, could be efficient tools for evaluating dry eye symptoms.28
The present study showed a positive correlation among the duration of contact lens wear, OSDI, total meiboscore, and meibograde. In contrast, the correlation was negative between these outcomes and both NIF-BUT and NIAvg-BUT. Additionally, a significant correlation was detected between the total meiboscore and both NIF-BUT and NIAvg-BUT. Also, a high significant positive correlation was reported between NIF-BUT versus NIAvg-BUT.
In conclusion, there is a difference in OSDI score, meibomian score, and break-up time between different study groups. The study results show that there are trends in lens wearers and non-lens wearers. This is useful for the field to understand the differences between lens wearers and non-lens wearers.
Data Sharing Statement
The Excel sheet data used to support the results of this study are available from the corresponding author upon request.
Acknowledgments
This is to certify that: the article has not been presented in a meeting. The authors did not receive any financial support from any public or private sources.
Disclosure
The authors have no financial or proprietary interest in the product, method, or material described herein. The authors declare that they have no conflicts of interest for this work.
References
1. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
2. Uchino M, Yokoi N, Uchino Y, et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: the Osaka study. Am J Ophthalmol. 2013;156(4):759–766. doi:10.1016/j.ajo.2013.05.040
3. Uchino M, Uchino Y, Dogru M, et al. Dry eye disease and work productivity loss in visual display users: the Osaka study. Am J Ophthalmol. 2014;157(2):294–300. doi:10.1016/j.ajo.2013.10.014
4. Kim YH, Nguyen T, Lin MC, et al. Protection against corneal hyperosmolarity with soft-contact-lens wear [published online ahead of print, 2021 Sep 29]. Prog Retin Eye Res. 2021;4:101012.
5. Nichols JJ, Sinnott LT. Tear film, contact lens, and patient related factors associated with contact lens-related dry eye. Invest Ophthalmol Vis Sci. 2006;47:1319–1328. doi:10.1167/iovs.05-1392
6. Dumbleton K, Caffery B, Dogru M, et al. The TFOS International workshop on contact lens discomfort: report of the subcommittee on epidemiology. Invest Ophthalmol Vis Sci. 2013;54(11):TFOS20. doi:10.1167/iovs.13-13125
7. Kaštelan S, Lukenda A, Salopek-Rabatić J, et al. Dry eye symptoms and signs in long-term contact lens wearers. Coll Antropol. 2013;37(1):199–203. PMid: 23837244.
8. Mathers WD. Ocular evaporation in meibomian gland dysfunction and dry eye. Ophthalmology. 1993;100:347–351. doi:10.1016/S0161-6420(93)31643-X
9. Tomlinson A, Bron AJ, Korb DR, et al. The international workshop on Meibomian gland dysfunction: report of the diagnosis subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4):2006–2049. doi:10.1167/iovs.10-6997f
10. Arita R. Validity of noninvasive meibography systems: noncontact meibography equipped with a slit-lamp and a mobile pen-shaped meibograph. Cornea. 2013;32(Suppl 1):S65–S70. doi:10.1097/ICO.0b013e3182a2c7c6
11. Arita R, Itoh K, Inoue K, et al. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology. 2008;115(5):911–915. doi:10.1016/j.ophtha.2007.06.031
12. Arita R, Itoh K, Inoue K, et al. Contact lens wear is associated with decrease of meibomian glands. Ophthalmology. 2009;116(3):379–384. doi:10.1016/j.ophtha.2008.10.012
13. Pult H, Riede-Pult BH. Non-contact meibography: keep it simple but effective. Cont Lens Anterior Eye. 2012;35(2):77–80. doi:10.1016/j.clae.2011.08.003
14. Finis D, Ackermann P, Pischel N, et al. Evaluation of meibomian gland dysfunction and local distribution of meibomian gland atrophy by non-contact infrared meibography. Curr Eye Res. 2015;40(10):982–989. doi:10.3109/02713683.2014.971929
15. Arita R, Itoh K, Maeda S, et al. A newly developed noninvasive and mobile pen-shaped meibography system. Cornea. 2013;32(3):242–247. doi:10.1097/ICO.0b013e31825425ef
16. Llorens-Quintana C, Garaszczuk IK, Szczesna-Iskander DH. Meibomian glands structure in daily disposable soft contact lens wearers: a one-year follow-up study. Ophthalmic Physiol Opt. 2020;40(5):607–616. doi:10.1111/opo.12720
17. Arita R, Itoh K, Lee CH. Meibomian gland changes in contact lens wearers observed by an infrared non-contact Meibography. Invest. Ophthalmol. Vis. Sci. 2008;49(13):87. doi:10.1167/iovs.07-0954
18. Gu T, Du B, Bi H, et al. Meibomian gland dropout, not distortion, can distinguish dry eyes from normal eyes in contact lens wearers. Curr Eye Res. 2020;45(8):897–903. doi:10.1080/02713683.2020.1731829
19. Uçakhan Ö, Arslanturk-Eren M. The role of soft contact lens wear on meibomian gland morphology and function. Eye Contact Lens. 2019;45(5):292–300. doi:10.1097/ICL.0000000000000572
20. Alghamdi WM, Markoulli M, Holden BA, et al. Impact of duration of contact lens wear on the structure and function of the meibomian glands. Ophthalmic Physiol Opt. 2016;36(2):120–131. doi:10.1111/opo.12278
21. Arita R, Itoh K, Maeda S, et al. Association of contact lens-related allergic conjunctivitis with changes in the morphology of meibomian glands. Jpn J Ophthalmol. 2012;56(1):14–19. doi:10.1007/s10384-011-0103-6
22. Muhafiz E, Demir MS. Ability of non-invasive tear break-up time to determine tear instability in contact lens wearers. Int Ophthalmol. 2021;42:1–0.
23. Marx S, Eckstein J, Sickenberger W. Objective analysis of pre-lens tear film stability of daily disposable contact lenses using ring mire projection. Clin Optom. 2020;20(12):203–211. doi:10.2147/OPTO.S262353
24. Molina-Martín A, de Fez D, Piñero DP. Repeatability of non-invasive break-up time measures with a new automated dry eye platform in healthy eyes. Int Ophthalmol. 2020;40(11):2855–2864. doi:10.1007/s10792-020-01470-w
25. Pult H, Riede-Pult BH, Nichols JJ. Relation between upper and lower lids’ meibomian gland morphology, tear film, and dry eye. Optom Vis Sci. 2012;89(3):E310–5. doi:10.1097/OPX.0b013e318244e487
26. Pult H. Relationships between meibomian gland loss and age, sex, and dry eye. Eye Contact Lens. 2018;44(Suppl 2):S318–S324. doi:10.1097/ICL.0000000000000467
27. Ozulken K, Aksoy Aydemir G, Tekin K, et al. Correlation of non-invasive tear break-up time with tear osmolarity and other invasive tear function tests. Semin Ophthalmol. 2020;35(1):78–85. doi:10.1080/08820538.2020.1730916
28. Lee JH, Kim CH, Choe CM, et al. Correlation analysis between ocular surface parameters with subjective symptom severity in dry eye disease. Korean J Ophthalmol. 2020;34(3):203–209. doi:10.3341/kjo.2019.0133
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.