Back to Journals » International Journal of Women's Health » Volume 18
Changes in Maternal Hemoglobin Concentration and Risk of Low Birth Weight and Small-for-Gestational-Age in the United Arab Emirates: The Mutaba’ah Study
Authors Abdullahi AS ![]() , Suliman A
, Suliman A ![]() , Elhadi YAM
, Elhadi YAM ![]() , Narchi H
, Narchi H ![]() , Al Awar S
, Al Awar S ![]() , Zaręba K
, Zaręba K ![]() , Alhaj Ahmad M
, Alhaj Ahmad M ![]() , Khogali M, Ahmed LA
, Khogali M, Ahmed LA ![]()
Received 16 December 2025
Accepted for publication 4 March 2026
Published 21 March 2026 Volume 2026:18 589306
DOI https://doi.org/10.2147/IJWH.S589306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Aminu S Abdullahi,1 Abubaker Suliman,1 Yasir Ahmed Mohammed Elhadi,1 Hassib Narchi,2 Shamsa Al Awar,3 Kornelia Zaręba,3 Marwa Alhaj Ahmad,1 Mohammed Khogali,1 Luai A Ahmed1,4
1Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, Abu Dhabi, United Arab Emirates; 2Department of Pediatrics, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, Abu Dhabi, United Arab Emirates; 3Department of Obstetrics and Gynecology, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, Abu Dhabi, United Arab Emirates; 4Zayed Centre for Health Sciences, United Arab Emirates University, Al Ain, Abu Dhabi, United Arab Emirates
Correspondence: Abubaker Suliman, Email [email protected]
Background: Maternal hemoglobin (Hb) concentration and changes in Hb across trimesters have been linked to low birth weight (LBW) and small-for-gestational-age (SGA). However, these associations have shown inconsistent results and have not been investigated in pregnant women in the United Arab Emirates (UAE). We investigated the association between changes in Hb concentration during the first and second trimesters and birth weight, LBW, and SGA among pregnant women in the UAE.
Methods: We utilized data from the Mutaba’ah Study. Change in Hb was computed as the difference between the first and second trimester Hb concentrations. LBW and SGA were defined as birth weight below 2500 grams and birth weight below the 10th percentile, respectively. Multivariable regression models were used to investigate the association between changes in maternal Hb and birth weight, LBW and SGA.
Results: A total of 1500 pregnant women were included. The mean maternal age was 32 years (SD 6). Overall, Hb concentration declined from the first to the second trimesters by a median of − 9 g/L (IQR: − 14, − 3). LBW and SGA were observed among 6% and 10% of the newborns, respectively. Pregnant women who experienced the least reduction or an increase in Hb concentration had a higher risk of both LBW (adjusted odds ratio [aOR]: 3.43, 95% confidence interval [CI]: 1.77 to 6.96) and SGA (aOR: 2.08, 95% CI: 1.28 to 3.40) compared to those with the greatest reduction in Hb concentration.
Conclusion: Minimal reductions in Hb levels from the first to the second trimester were associated with LBW and SGA. The average Hb levels during the second trimester were inversely associated with birth weight and SGA. Monitoring variations in maternal Hb early in pregnancy may enhance the early identification of pregnancies at risk.
Keywords: hemoglobin, Hb change, birthweight, SGA, pregnancy
Introduction
Changes in maternal hemoglobin (Hb) concentration during pregnancy are a well‑recognized physiological adaptation to support fetal growth.1 This change is primarily driven by maternal hemodynamic adaptation, in which plasma volume expansion results in a relative reduction in Hb concentration. The relationship between maternal Hb concentration and pregnancy outcomes has been a topic of significant debate and controversy in maternal and child health research.2 Previous studies have found different links between maternal Hb levels and adverse birth outcomes, such as low birth weight (LBW) and small-for-gestational-age (SGA). Some studies showed that low Hb concentration (<110 g/L) is associated with a higher risk of LBW,3–6 while others suggest that high Hb levels (≥130 g/L) may also increase the risk.7–9 Some reports describe a U-shaped association,10–12 whereas others found no such association.13–15
Recent evidence suggests that the timing of Hb measurement during pregnancy influences the relationship with birth outcomes, with low Hb in the first trimester being more strongly linked to adverse outcomes, while high Hb poses risks throughout pregnancy.16,17 Moreover, associations between changes in maternal Hb levels – from early to late pregnancy – and the risks of adverse birth outcomes, including LBW and SGA deliveries, have also been reported linked to fetal growth outcomes. Studies from multiple countries have shown that minimal Hb reduction during pregnancy increases the likelihood of delivering LBW and SGA infants.2 Studies from multiple countries have shown that minimal Hb reduction during pregnancy increases the likelihood of delivering LBW and SGA infants.18,19
Although studies from other countries have established a link between changes in maternal Hb levels and LBW and SGA infants, it is uncertain whether similar risks are present in the United Arab Emirates (UAE) population, given the high prevalence of obesity and the swift alterations in lifestyle and nutritional habits that may affect anemia and fetal outcomes. Furthermore, there is insufficient direct evidence regarding the overall prevalence of anemia in pregnant women and LBW in the UAE. Prior research indicated that 25% of Emirati women aged 15 to 49 years are anemic, and LBW prevalence ranging from 9% to 11%.20–23 One study among pregnant women in the UAE examined trends in maternal Hb levels, but did not investigate adverse outcomes associated with these changes.24 In the present study, we assessed the association between changes in maternal Hb concentration and the risk of LBW and SGA infants in a cohort of pregnant women in the UAE.
Methods
Study Design, Setting and Participants
This analysis used data from the Mutaba’ah Study, a large ongoing prospective birth cohort in Al Ain, UAE, that investigates maternal and child health. Ethical approval for the Mutaba’ah Study was obtained from the Human Research Ethics Committee of the United Arab Emirates University (ERH-2017-5512) and the Abu Dhabi Health Research and Technology Ethics Committee (DOH/CVDC/2022/72). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, and participants enrolled voluntarily after providing informed consent.
All pregnant women from the Emirati population, aged 18 or older, living in Al Ain City who can provide informed consent are eligible to participate in the Mutaba’ah Study. Data were collected through questionnaires and medical record linkage. More detailed information about the Mutaba’ah Study can be found elsewhere.25 This analysis includes pregnant women recruited in the Mutaba’ah Study who gave birth between October 2017 and June 2024. Women with multiple pregnancies, preterm deliveries, and those with missing hemoglobin measurements in the first or second trimesters of pregnancy, birth outcome data, or gestational age were excluded from the analysis.
Variables and Measurements
Maternal educational level was categorized based on the responses to the self-administered questionnaire as “Higher than secondary” (Vocational/Diploma, Bachelors, Masters or Doctorate) or “Secondary or lower” (Illiterate, Never attended school, Primary or Secondary). Hemoglobin concentration was measured as part of routine antenatal care and recorded in the medical records of participating healthcare facilities. All available measurements of Hb concentration (g/L) during the pregnancy were extracted from the medical records. Data on maternal age (years), parity, early-pregnancy body mass index (BMI) (first available BMI recorded within the first trimester), pre-existing diabetes status (Yes/No), pre-existing hypertension status (Yes/No), delivery mode (vaginal/caesarean), fetal sex (male/female), gestational age at birth (weeks) and birth weight (grams), were also extracted from the medical records.
Hb concentration of the first 12 weeks of gestation (first trimester) and second 12 weeks of gestation (second trimester) was estimated as the average of all available Hb measurements within each trimester. Birth weight less than 2500 grams was defined as low birth weight (LBW). Small-for-gestational-age (SGA) was defined as a birth weight below the 10th percentile using the reference reported by INTERGROWTH-21st Project.26 The INTERGROWTH-21st International Standard for Newborn Weight is the most suitable available birth weight reference because it is globally representative, incorporating data from various regions and countries, including Oman, a neighboring country to the UAE.
Post-Hoc Sample Size Estimation
The minimum required sample size for developing the multivariable linear regression model with birth weight as the outcome was retrospectively estimated using the approach of Riley et al for continuous outcomes27 We used the adjusted R2=0.07; conservative estimate of anticipated model performance, from a published multivariable linear regression of birth weight on maternal hemoglobin and related predictors from the region.28 The average (SD) birth weight was approximated from the same study, and we allowed a multiplicative margin of error of 1.10 for estimation of the intercept and residual standard deviation. Specifying 10 candidate predictor parameters, yielded a recommended minimum sample size of N= 964 participants for new model development.
Data Analysis
Change in Hb concentration was computed as the difference between the average Hb concentrations during the first and second trimesters for each pregnant woman. To facilitate easy comparison, the change in Hb was further divided into tertiles – three equal cut-offs comprising those with the greatest reduction (Tertile 1), those with a moderate reduction (Tertile 2), and those with the least reduction or an increase in Hb concentration (Tertile 3).
Categorical variables were summarized using frequencies and percentages. The mean and standard deviation (SD; Range) were used to summarize continuous variables, except for the difference in Hb concentration, which was summarized as median and interquartile range (IQR; Range) due to skewed distribution.
Associations between Hb change tertiles and categorical variables were analyzed using Pearson’s chi-squared test for trends. The relationship between Hb change tertiles and quantitative variables was evaluated with Kruskal–Wallis ANOVA. Linear regression models were used to examine the relationship between Hb levels in the first and second trimesters and birth weight. Logistic regression was used to assess the associations of Hb change (both continuous and tertile measures) and first- and second-trimester Hb levels with LBW and SGA. For each analysis, a crude model and two adjusted models were constructed. In the first adjusted model (A), adjustments included maternal age, early-pregnancy BMI, and parity. Additionally, first-trimester Hb levels were controlled for when examining the association between Hb change and the three outcomes. In the second adjusted model (B), adjustments included all variables from Model A, as well as pre-existing diabetes mellitus and pre-existing hypertension. As part of a sensitivity analysis, additional models were developed to explore the potential confounding effect of first-trimester Hb on the relationship between second-trimester Hb and birth weight, LBW, and SGA.
R software (version 4.4.1) was used for data analysis. All statistical tests were performed at the 5% significance level.
Results
Hb Concentration Change
A total of 1500 pregnant women were included in the study (Table 1). The average Hb concentrations during the first and second trimesters were 115 g/L (SD: 11 g/L; range: 75 to 147) and 107 g/L (SD: 10 g/L; range: 70 to 139), respectively. Overall, the change in Hb was estimated at −9 g/L (IQR: −14 to −3; range: −34 to 31). The average Hb changes for Tertile 1, Tertile 2, and Tertile 3 were −16 g/L (IQR: −20 to −14; range: −34 to −12), −8 g/L (IQR: −10 to −7; range: −12 to −5), and 0 g/L (IQR: −3 to 4; range: −5 to 31), respectively (Table 1 and Figure 1).
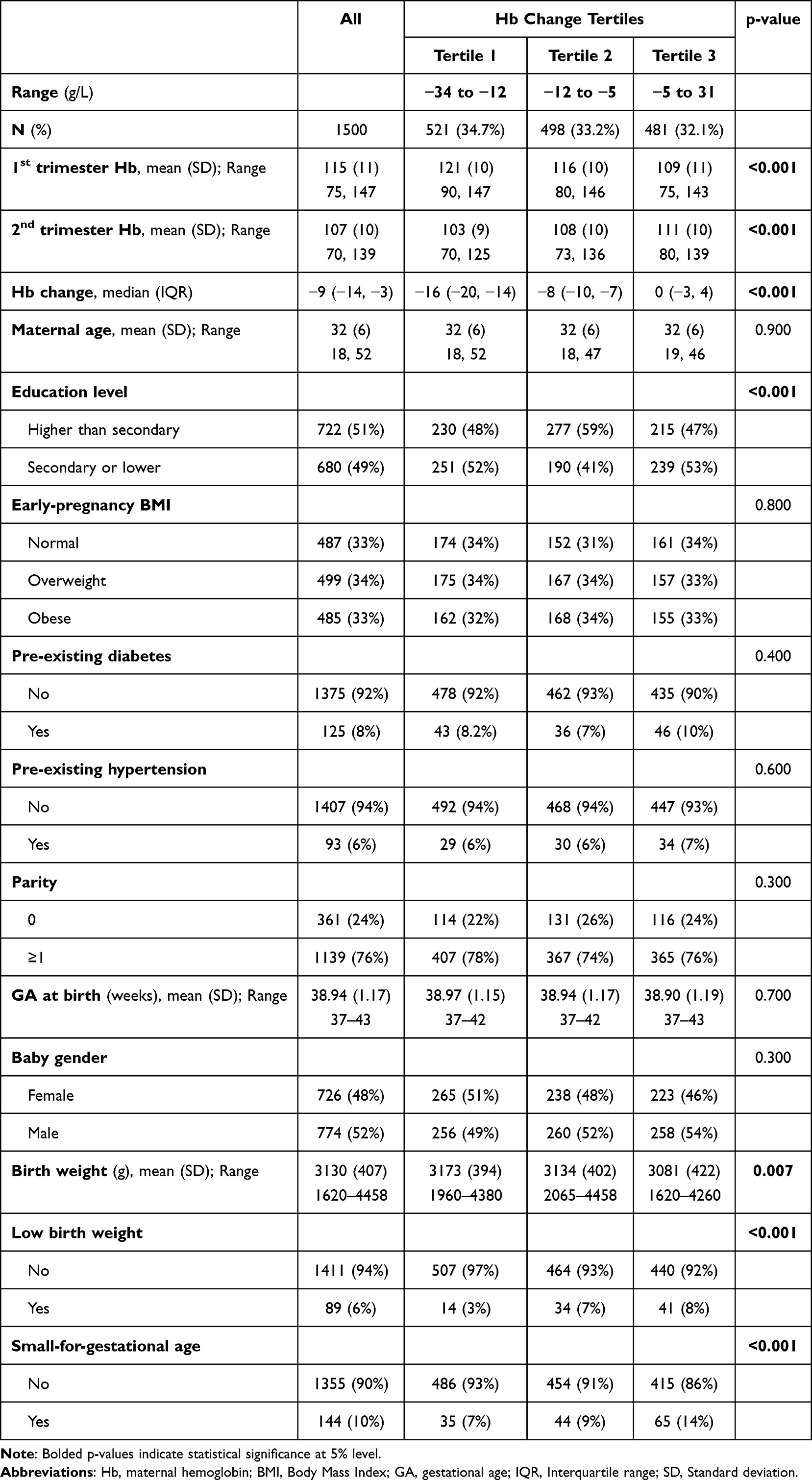 |
Table 1 Association Between Sociodemographic, Comorbidities, and Pregnancy and Neonatal Outcomes by Tertiles of Hb Concentration Changes from First to second Trimester |
 |
Figure 1 Distribution of birth weight by tertiles of Hb change from the first to the second trimester. |
Demographic, Clinical, and Obstetric Characteristics
The mean age of the women was 32 years (SD: 6; range: 18 to 52); 76% were multiparous, and about half (51%) had completed higher education. About two-thirds of the women (67%) were overweight or obese, 8% had pre-existing diabetes mellitus, and 6% had pre-existing hypertension. The overall mean gestational age was 38.9 weeks (SD: 1.17; range: 37 to 43), and just over half (52%) of the newborns were male. The change in Hb was not statistically significantly different across these characteristics, except for education levels (p<0.001) (Table 1).
The median birth weight was 3130 grams (SD: 407; range: 1620 to 4458), with 6% classified as LBW and 10% as SGA. The mean birth weight of babies born to women in Tertile 3 was significantly lower than that of babies born to women in Tertile 1 and Tertile 2 of Hb change (p=0.007). Similarly, the proportions of LBW differed significantly across the tertiles of Hb change (p<0.001), with the highest in Tertile 3 (8%), followed by Tertile 2 (7%), and Tertile 1 (3%). The proportions of SGA also varied significantly (p<0.001) across the Hb change tertiles: 14% in Tertile 3, 9% in Tertile 2, and 7% in Tertile 1 (Table 1).
Association Between Hb Changes and Birthweight-Related Outcomes
There was a significant (p<0.001) difference in the mean change in Hb between deliveries with and without LBW and SGA (Figure 2A and B; respectively). A one g/L increase in Hb from the first to the second trimester was associated with a decrease in birth weight by an average of 5.1 grams (β: −5.1, 95% confidence interval [CI]: −7.8 to −2.5) after adjusting for several potential confounders (Table 2). In terms of the relationship with the Hb change tertiles, babies born to women in Tertile 3 of Hb reduction (least reduction or an increase in Hb concentration) had, on average, 84 grams lower birth weight compared with those born to women in Tertile 1 (β: −84, 95% CI: −138 to −29). Birth weight was not significantly associated with being in Tertile 2 compared to being in Tertile 1 of Hb reduction (p=0.150).
 |
Table 2 Linear Regression Analysis for the Relationship Between Hb Concentration and Birth Weight |
 |
Figure 2 Distribution of Hb changes from the first to the second trimester by (A) low birth weight and (B) Small-for-gestational-age (SGA). |
When examining the average Hb levels separately for the first and second trimester, there was no significant association between birth weight and average Hb levels in the first trimester. However, a significant association was observed between birth weight and average Hb levels in the second trimester. For each one g/L increase in Hb in the second trimester, birth weight decreased by an average of 2.2 grams (β=−2.2, 95% CI=−4.2 to −0.17). Compared to women in Tertile 1 of the second trimester Hb, average birth weight was 51 grams lower in Tertile 3 (β: −51, 95% CI: −102 to −1.90) (Table 2).
The odds of LBW increased by an average of 5% (adjusted odds ratio [aOR]: 1.05, 95% CI: 1.02 to 1.08) for each one g/L increase in Hb (Table 3). Furthermore, being in Tertile 2 (aOR: 2.62, 95% CI: 1.39 to 5.18) and Tertile 3 (aOR: 3.43, 95% CI: 1.77 to 6.96) of Hb reduction were associated with a significant increase in the odds of LBW as compared to those in Tertile 1. Moreover, one g/L increase in average second-trimester, not first-trimester, Hb levels was significantly associated with LBW (aOR: 1.03, 95% CI: 1.01 to 1.05). Additionally, women in Tertile 3 of average second-trimester Hb had almost two times the odds of LBW compared to those in Tertile 1 (aOR: 1.86, 95% CI: 1.07 to 3.31). There was no significant difference in the odds of LBW between women in Tertile 2 and those in Tertile 1 of average second-trimester Hb.
 |
Table 3 Logistic Regression Analysis for the Association Between Hb Concentration and Low Birth Weight |
A positive association was observed between increased Hb and SGA (Table 4). A one g/L increase in Hb during the second trimester was associated with an average 4% increase in the odds of SGA (aOR: 1.04, 95% CI: 1.01 to 1.06). Similarly, women in Tertile 3 of Hb change had twice the odds of SGA compared to those in Tertile 1 (aOR: 2.08, 95% CI: 1.28 to 3.40). On the other hand, there was no significant difference in odds of SGA between women in Tertile 2 and those in Tertile 1 (p=0.290). On the other hand, second-trimester Hb was not significantly associated with SGA.
 |
Table 4 Logistic Regression Analysis for the Association Between Hb Concentration and Small-for-Gestational-Age |
In the supplementary models examining the association between second-trimester Hb and the relevant birth weight outcomes, after additionally adjusting for first-trimester Hb, the results were broadly similar in direction and statistical significance, with only three exceptions (Supplementary Table 1). Furthermore, a significant association was observed between Tertile 2 of second-trimester Hb and birth weight (β=−71, 95% CI: −124 to −19, p=0.008) when compared to women in Tertile 1. Additionally, changes in second-trimester Hb were positively associated with SGA (aOR=1.04, 95% CI: 1.01 to 1.06), and women classified within Tertile 3 of second-trimester Hb demonstrated a significantly higher likelihood of having an SGA infant than those in Tertile 1 (aOR: 1.96, 95% CI: 1.14 to 3.38).
Discussion
This study examined changes in Hb concentrations between the first and the second trimesters among pregnant women in the UAE and their association with birth weight and SGA. The findings revealed a decrease in Hb among pregnant women during the second trimester. There were inverse associations between the change in Hb concentration and birth weight and SGA. Additionally, average Hb levels during the second, rather than the first, trimester were inversely associated with birth weight and SGA.
Our finding of an overall decline in Hb concentration during the second trimester is consistent with reports from several earlier studies.2,19,29–32 This is attributed to hemodilution, a well-documented phenomenon that occurs during the second trimester as a result of significant plasma volume expansion.29,33 A meta-analysis involving 10 studies and 347 pregnancies reported a significant increase in plasma volume during pregnancy as compared to the non-pregnancy state, with the highest volume expansion happening during the second trimester.29
The findings of the present study indicate an inverse association between the change in Hb concentration and birth weight and SGA, with those who experienced a lower reduction or even an increase in Hb having a higher risk of LBW and SGA. This is in agreement with reports in other studies.2,19,34,35 Although focusing on Hb changes later in pregnancy, a study among Japanese pregnant women and their newborns found that a smaller reduction in Hb levels during the later stages of pregnancy, as compared to early pregnancy, was significantly associated with LBW.2 Similarly, Peng et al, in a more recent study among pregnant women in China, reported that the increase in maternal Hb from the second to the third trimester was positively correlated with both LBW and SGA infants.19 In 2022, a study involving two large cohorts of pregnant women in the United Kingdom reported that higher maternal Hb in late pregnancy, which may signify a lower increase from early pregnancy, was associated with LBW and SGA.36
Nonetheless, a few studies have reported contradictory associations.34,37 A study conducted in Turkey found a significant correlation between birth weight and an increase in maternal Hb from the first to the third trimester.34 Another study from the United Kingdom found no significant association between changes in Hb levels during late pregnancy and low birth weight.31 The disagreement could be due to the inclusion of changes during the third trimester in the Turkish study, whereas our study focused only on the second trimester, when plasma volume expansion is typically at its peak, or the use of pre-pregnancy Hb levels as baseline in the United Kingdom, whereas our study used first-trimester Hb levels as baseline.
The mechanisms underlying the relationship between maternal Hb change and birth weight outcomes remain unclear. The typical increase in red blood cell mass as pregnancy advances into the second trimester is concurrent with a proportionately larger increase in plasma volume, resulting in a net decrease in maternal Hb concentration.1,36–38 Such an appreciable increase in plasma volume, and in turn, a decrease in maternal Hb levels, may be essential for maintaining normal fetoplacental circulation; its absence could potentially cause problems, including those related to fetal growth.38–40 The importance of appropriate Hb reduction during the course of pregnancy was long highlighted in a large (N=153,602), multi-ethnic cohort of pregnant women in the UK.41 In that study, Steer et al concluded that failure of maternal Hb to drop below 105 g/L was associated with an increased risk of adverse outcomes, including LBW.41 More recently, Burden et al hypothesized that the decline in maternal Hb concentration during mid-trimester may reflect optimal physiologic changes, indicating the body’s ability for good plasma volume expansion.42 However, a lack of appropriate plasma expansion as pregnancy progresses may result from impaired placental function, leading to adverse outcomes and minimal decline in Hb concentration.43 Smaller declines in Hb levels during the first trimester might indicate reduced or physiologically insufficient plasma volume expansion, which could impair fetoplacental circulation, affect fetal growth, and result in LBW and SGA babies.39
Implication of the Findings
Our findings have important implications for the monitoring of changes in Hb concentration and, in turn, plasma expansion during antenatal care. They highlight the need to account for the physiological decline in Hb concentration due to plasma volume expansion when assessing anemia risks during pregnancy. A smaller decrease in Hb concentration during the second trimester may indicate inadequate plasma expansion, which is essential for optimal fetal growth. Monitoring changes in Hb concentration during the second trimester can help identify women at risk of insufficient plasma volume expansion and enable timely interventions, such as antenatal care and nutritional counseling, to prevent adverse outcomes, including low birth weight. Additionally, the overall decline in Hb concentration during the second trimester was 9 g/L, nearly double the commonly accepted threshold of 5 g/L.44 Notably, women in the lowest-risk group for adverse birth weight outcomes experienced a median Hb decrease of 17 g/L. These findings suggest that the current threshold for Hb concentration decline in the second trimester may need to be re-evaluated. Future research is warranted to explore social determinants (nutrition, access to prenatal care, cultural practices) that may affect Hb changes. Moreover, future studies should elucidate the mechanisms underlying the relationship between maternal Hb changes and birth-weight-related outcomes.
Strengths and Limitations
A key strength of our study is that it is the first, and among a few globally, to examine birthweight-related adverse pregnancy outcomes in relation to changes in Hb levels in a large cohort of pregnant women. Most studies reporting on the association between maternal Hb and birthweight-related outcomes used a single Hb measurement rather than accounting for changes in Hb throughout pregnancy.13,19,25–28 Using a single Hb measurement can limit the ability to thoroughly analyze the pattern and impact of maternal Hb changes throughout pregnancy. Additionally, we were able to properly adjust the association for multiple variables, including early-pregnancy BMI,45 that might confound the relationship between changes in maternal Hb and birth weight outcomes.
On the other hand, the interpretation of our findings may be limited, as the data are derived from women who attended antenatal care centers in one city. Hence, the generalizability of the findings to the rest of the UAE should be done with caution. Additionally, we could not adjust for placental conditions, such as placental insufficiency, which may influence the association between maternal Hb changes and birth-weight-related outcomes. Further adjustments for other socioeconomic, behavioral and clinical factors, for instance, smoking and iron supplementation before and during pregnancy, and hemoglobinopathies, should be adapted in future research to control for any potential confounding effects.
Conclusion
Pregnant women with low Hb changes between the first and second trimesters experienced increased risks of LBW and SGA. Mean Hb levels during the second trimester demonstrated an inverse relationship with birth weight and SGA. Monitoring fluctuations in maternal Hb during early- to mid-pregnancy can help pregnancies at risk of fetal growth restriction, instead of relying on a single measurement.
Generative Artificial Intelligence
We acknowledge the journal’s Artificial Intelligence policy. Generative AI tools (eg, ChatGPT) were used only to assist with language editing, grammar refinement, and formatting of the manuscript text. No AI-generated data, analysis, or references were created or modified using these tools. The authors have thoroughly reviewed all content for accuracy and originality and take full responsibility for the scientific integrity of the manuscript.
Data Sharing Statement
All relevant data are available within the manuscript. Additional requests could be submitted to the Mutaba’ah Study after ethical approval.
Ethics Approval and Informed Consent
The Mutaba’ah Study is approved by the UAE University Human Research Ethics Committee (ERH-2017-5512) and the Abu Dhabi Health Research and Technology Ethics Committee (DOH/CVDC/2022/72). Informed written consent was obtained from all participants prior to data collection.
Acknowledgment
The authors would like to acknowledge and thank all the participants of The Mutaba’ah Study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the United Arab Emirates University under grant number (12R275). The funder had no role in the design, conduct, or dissemination of the results of the current study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy: review articles. Cardiovasc J Afr. 2016;27(2):89–13. doi:10.5830/CVJA-2016-021
2. Jwa SC, Fujiwara T, Yamanobe Y, Kozuka K, Sago H. Changes in maternal hemoglobin during pregnancy and birth outcomes. BMC Pregnancy Childbirth. 2015;15:1–10. doi:10.1186/s12884-015-0516-1
3. Nair M, Churchill D, Robinson S, Nelson‐Piercy C, Stanworth SJ, Knight M. Association between maternal haemoglobin and stillbirth: a cohort study among a multi‐ethnic population in England. Br J Haematol. 2017;179(5):829–837. doi:10.1111/bjh.14961
4. Haider BA, Olofin I, Wang M, Spiegelman D, Ezzati M, Fawzi WW. Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2013;346(3):f3443–f3443. doi:10.1136/bmj.f3443
5. Alizadeh L, Raoofi A, Salehi L, Ramzi M. Impact of maternal hemoglobin concentration on fetal outcomes in adolescent pregnant women. Iran Red Crescent Med J. 2014;16(8). doi:10.5812/ircmj.19670
6. Sukrat B, Wilasrusmee C, Siribumrungwong B, et al. Hemoglobin concentration and pregnancy outcomes: a systematic review and meta‐analysis. Biomed Res Int. 2013;2013(1):769057. doi:10.1155/2013/769057
7. Ahankari A, Leonardi-Bee J. Maternal hemoglobin and birth weight: systematic review and meta-analysis. Int J Med Sci Public Health. 2015;4(4):435–445. doi:10.5455/ijmsph.2015.2212201489
8. Sekhavat L, Davar R, Hosseinidezoki S. Relationship between maternal hemoglobin concentration and neonatal birth weight. Hematology. 2011;16(6):373–376. doi:10.1179/102453311X13085644680186
9. Ali SA, Tikmani SS, Saleem S, et al. Hemoglobin concentrations and adverse birth outcomes in South Asian pregnant women: findings from a prospective Maternal and Neonatal Health Registry. Reproductive Health. 2020;17(S2):1–13. doi:10.1186/s12978-020-01006-6
10. Gaillard R, Eilers PH, Yassine S, Hofman A, Steegers EA, Jaddoe VW. Risk factors and consequences of maternal anaemia and elevated haemoglobin levels during pregnancy: a population‐based prospective cohort study. Paediatric Perinatal Epidemiol. 2014;28(3):213–226. doi:10.1111/ppe.12112
11. Scanlon KS, Yip R, Schieve LA, Cogswell ME. High and low hemoglobin levels during pregnancy: differential risks for preterm birth and small for gestational age. Obstetrics Gynecol. 2000;96(5):741–748.
12. Dewey KG, Oaks BM. U-shaped curve for risk associated with maternal hemoglobin, iron status, or iron supplementation. Am J Clin Nutr. 2017;106:1694S–702S. doi:10.3945/ajcn.117.156075
13. Abeysena C, Jayawardana P, De A. Seneviratne R. Maternal haemoglobin level at booking visit and its effect on adverse pregnancy outcome. Aust N Z J Obstetrics Gynaecol. 2010;50(5):423–427. doi:10.1111/j.1479-828X.2010.01220.x
14. Mathews F, Youngman L, Neil A. Maternal circulating nutrient concentrations in pregnancy: implications for birth and placental weights of term infants. Am J Clin Nutr. 2004;79(1):103–110. doi:10.1093/ajcn/79.1.103
15. Lu ZM, Goldenberg RL, Cliver SP, Cutter G, Blankson M. The relationship between maternal hematocrit and pregnancy outcome. Obstetrics Gynecol. 1991;77(2):190–194. doi:10.1097/00006250-199102000-00005
16. Young MF, Oaks BM, Tandon S, Martorell R, Dewey KG, Wendt AS. Maternal hemoglobin concentrations across pregnancy and maternal and child health: a systematic review and meta‐analysis. Ann N Y Acad Sci. 2019;1450(1):47–68. doi:10.1111/nyas.14093
17. Jung J, Rahman MM, Rahman MS, et al. Effects of hemoglobin levels during pregnancy on adverse maternal and infant outcomes: a systematic review and meta‐analysis. Ann N Y Acad Sci. 2019;1450(1):69–82. doi:10.1111/nyas.14112
18. Adjei-Gyamfi S, Zakaria MS, Asirifi A, Issahaku S, Ibrahim MA, Aryee PA. Maternal anaemia and polycythaemia during pregnancy and risk of inappropriate birth weight for gestational age babies: a retrospective cohort study in the northern belt of Ghana. BMJ open. 2024;14(8):e082298. doi:10.1136/bmjopen-2023-082298
19. Peng Z, Si S, Cheng H, et al. The associations of maternal hemoglobin concentration in different time points and its changes during pregnancy with birth weight outcomes. Nutrients. 2022;14(12):2542. doi:10.3390/nu14122542
20. Taha Z, Ali Hassan A, Wikkeling-Scott L, Papandreou D. Factors associated with preterm birth and low birth weight in Abu Dhabi, the United Arab Emirates. Int J Environ Res Public Health. 2020;17(4):1382. doi:10.3390/ijerph17041382
21. Al Sabbah H, Assaf EA, Al-Jawaldeh A, et al. Nutrition situation analysis in the UAE: a review study. Nutrients. 2023;15(2):363. doi:10.3390/nu15020363
22. Al Sabbah H. Prevalence of overweight/obesity, anaemia and their associations among female university students in Dubai, United Arab Emirates: a cross-sectional study. J Nutr Sci. 2020;9:e26. doi:10.1017/jns.2020.23
23. Khan W, Zaki N, Ahmad A, et al. Infant low birth weight prediction using graph embedding features. Int J Environ Res Public Health. 2023;20(2):1317. doi:10.3390/ijerph20021317
24. Abdullahi AS, Suliman A, Khan MA, et al. Temporal trends of hemoglobin among pregnant women: the Mutaba’ah study. PLoS One. 2023;18(12):e0295549. doi:10.1371/journal.pone.0295549
25. Al Haddad A, Ali N, Elbarazi I, et al. Mutaba’ah—mother and child health study: protocol for a prospective cohort study investigating the maternal and early life determinants of infant, child, adolescent and maternal health in the United Arab Emirates. BMJ open. 2019;9(8):e030937. doi:10.1136/bmjopen-2019-030937
26. Villar J, Ismail LC, Victora CG, et al. International standards for newborn weight, length, and head circumference by gestational age and sex: the Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet. 2014;384(9946):857–868. doi:10.1016/S0140-6736(14)60932-6
27. Riley RD, Snell KI, Ensor J, et al. Minimum sample size for developing a multivariable prediction model: part I–continuous outcomes. Stat Med. 2019;38(7):1262–1275. doi:10.1002/sim.7993
28. Samimi M, Asemi Z, Taghizadeh M, Azarbad Z, Rahimi-Foroushani A, Sarahroodi S. Concentrations of serum zinc, hemoglobin and ferritin among pregnant women and their effects on birth outcomes in Kashan, Iran. Oman Med J. 2012;27(1):40. doi:10.5001/omj.2012.08
29. Aguree S, Gernand AD. Plasma volume expansion across healthy pregnancy: a systematic review and meta-analysis of longitudinal studies. BMC Pregnancy Childbirth. 2019;19(1):508. doi:10.1186/s12884-019-2619-6
30. Sun M, Gu T, Wu T, et al. Variation patterns of hemoglobin levels by gestational age during pregnancy: a cross-sectional analysis of a multi-center retrospective cohort study in China. Nutrients. 2023;15(6):1383. doi:10.3390/nu15061383
31. Sulhariza HZ, Zalilah MS, Geeta A. Maternal hemoglobin change from early pregnancy to second trimester is associated with risk of gestational diabetes mellitus: a retrospective cohort study. Front Nutr. 2023;10:1197485. doi:10.3389/fnut.2023.1197485
32. Churchill D, Nair M, Stanworth SJ, Knight M. The change in haemoglobin concentration between the first and third trimesters of pregnancy: a population study. BMC Pregnancy Childbirth. 2019;19(1):359. doi:10.1186/s12884-019-2495-0
33. de Haas S, Ghossein‐Doha C, van Kuijk SM, van Drongelen J, Spaanderman M. Physiological adaptation of maternal plasma volume during pregnancy: a systematic review and meta‐analysis. Ultrasound Obstet Gynecol. 2017;49(2):177–187. doi:10.1002/uog.17360
34. Bakacak M, Avci F, Ercan O, et al. The effect of maternal hemoglobin concentration on fetal birth weight according to trimesters. J Matern Fetal Neonatal Med. 2015;28(17):2106–2110. doi:10.3109/14767058.2014.979149
35. Chen J, Guo X, Liu S, et al. Impact and changes of maternal hemoglobin on birth weight in pregnant women of Zhuang Nationality, in Guangxi. Zhonghua liu Xing Bing xue za zhi. 2017;38(2):154–157. doi:10.3760/cma.j.issn.0254-6450.2017.02.004
36. Young MF. Unpacking perplexing findings on maternal hemoglobin and pregnancy outcomes: call for further research to understand underlying etiology and mechanisms. Am J Clin Nutr. 2023;117(3):447–448. doi:10.1016/j.ajcnut.2022.11.025
37. Whittaker PG, Macphail S, Lind T. Serial hematologic changes and pregnancy outcome. Obstetrics Gynecol. 1996;88(1):33–39. doi:10.1016/0029-7844(96)00095-6
38. Vricella LK. Emerging understanding and measurement of plasma volume expansion in pregnancy. Am J Clin Nutr. 2017;106:1620S–5S. doi:10.3945/ajcn.117.155903
39. Steer PJ. Maternal hemoglobin concentration and birth weight. Am J Clin Nutr. 2000;71(5):1285S–7S. doi:10.1093/ajcn/71.5.1285s
40. Scholl TO. Maternal iron status: relation to fetal growth, length of gestation, and iron endowment of the neonate. Nutr Rev. 2011;69(suppl_1):S23–S9. doi:10.1111/j.1753-4887.2011.00429.x
41. Steer P, Alam MA, Wadsworth J, Welch A. Relation between maternal haemoglobin concentration and birth weight in different ethnic groups. BMJ. 1995;310(6978):489–491. doi:10.1136/bmj.310.6978.489
42. Burden CA, Smith GC, Sovio U, Clayton GL, Fraser A. Maternal hemoglobin levels and adverse pregnancy outcomes: individual patient data analysis from 2 prospective UK pregnancy cohorts. Am J Clin Nutr. 2023;117(3):616–624. doi:10.1016/j.ajcnut.2022.10.011
43. Ng S-W, Norwitz SG, Norwitz ER. The impact of iron overload and ferroptosis on reproductive disorders in humans: implications for preeclampsia. Int J Mol Sci. 2019;20(13):3283. doi:10.3390/ijms20133283
44. Control CfD. CDC criteria for anemia in children and childbearing-aged women. MMWR Morb Mortal Wkly Rep. 1989;38(22):400–404.
45. Wang Y, Ma H, Feng Y, et al. Association among pre-pregnancy body mass index, gestational weight gain and neonatal birth weight: a prospective cohort study in China. BMC Pregnancy Childbirth. 2020;20(1):690. doi:10.1186/s12884-020-03323-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.