Back to Journals » Clinical and Experimental Gastroenterology » Volume 15
Changes in Helicobacter pylori Treatment from Discovery to Nowadays: A High-Level Analysis of PubMed Publications
Authors Klang E, Soffer S ![]() , Barash Y, Shachar E
, Barash Y, Shachar E ![]() , Lahat A
, Lahat A ![]()
Received 29 September 2021
Accepted for publication 3 March 2022
Published 18 March 2022 Volume 2022:15 Pages 51—58
DOI https://doi.org/10.2147/CEG.S342048
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Koulaouzidis
Eyal Klang,1– 3,* Shelly Soffer,3– 5,* Yiftach Barash,1– 3 Eyal Shachar,2,6 Adi Lahat2,6
1Department of Diagnostic Imaging, Sheba Medical Center, Ramat Gan, Israel; 2Sackler Medical School, Tel Aviv University, Tel Aviv, Israel; 3DeepVision Lab, Sheba Medical Center, Ramat Gan, Israel; 4Internal Medicine B, Samson Assuta Ashdod University Hospital, Ashdod, Israel; 5Ben-Gurion University of the Negev, Be’er Sheva, Israel; 6Department of Gastroenterology, Sheba Medical Center, Ramat Gan, Israel
*These authors contributed equally to this work
Correspondence: Shelly Soffer, Internal Medicine B, Samson Assuta Ashdod University Hospital, Ha-Refu’a St 7, Ashdod, 7747629, Israel, Tel +973-8-300-4100, Fax +972-3-5357315, Email [email protected]
Background: Since the discovery of Helicobacter pylori (H. pylori) 40 years ago, treatment options have changed dramatically adjacent to new drugs development and the emergence of multi-drug resistance. In this study, we aimed to assess published literature on treatment regimens for H. pylori in the past four decades, with regards to specific drug resistance and geographic distribution.
Methods: We have queried PubMed for all available H. pylori-related entries published during 1987– 2020. For each entry, we retrieved the title, abstract, and keywords. Two gastrointestinal specialists decided in consensus on a list of terms to classify entries. The terms specify types of treatment and different types of regimens. Annual trends of publications were plotted for different treatment types and sub-analyses.
Results: Overall, 47,170 H. pylori-related entries were published between 1987 and 2020. Medication treatment showed the highest number of total publications 6183/47,170 (13.1%), followed by antibiotics 5493/47,170 (11.6%), and probiotic which was substantially lower (0.7%). For treatment regimens type, triple therapy had the highest number of publications 2400/47,170 (5.1%) followed by sequential therapy 342/47,170 (0.7%), and bismuth quadruple therapy 115/47,170 (0.2%). Analysis by antibiotic resistance showed that clarithromycin treatment had the highest number of publications 3537/47,170 (7.5%). Since 2013, there is a steep upward slope (5.1± 0.7 publications/year, p < 0.001) for publications originating from China.
Conclusion: Our findings reflect the changes of the commonly prescribed regimens along the years, following the occurrence and the rise of H. pylori antibiotic resistance. In recent years, there is a steep rise in publications in countries with policies of screening and eradication for gastric cancer prevention, which is currently not applied in Western countries. A text-mining analysis of H. pylori publications contributes to the understanding of treatment options and development trends worldwide.
Keywords: Helicobacter pylori, antibiotics, treatment regimens, antibiotic resistance
Introduction
Helicobacter pylori (H. pylori) is a common Gram- negative bacterium which constitutes one of the most prevalent global pathogens in humans. The bacterium infects approximately 50% of the world’s human population,1 with prevalence that varies considerably in association with geography, ethnicity, age, and socioeconomic factors.
H. pylori causes chronic active gastritis in all colonized subjects. This may lead to peptic ulcer disease (PUD), atrophic gastritis, gastric adenocarcinoma, and MALT (mucosa-associated lymphoid tissue) lymphoma.
H. pylori eradication cures gastritis and can alter the progression to long-term complications, or recurrence of disease.2,3
The bacterium was first discovered and isolated by Barry J. Marshall and Robin Warren in 1982, who revealed its role in gastritis and PUD.4 After its discovery, bacteria’s genome was fully sequenced in order to characterize the pathogenic mechanisms. The analyses have revealed new insights regarding genomic diversity, pathogenicity and mechanisms for PUD and cancer development.5
As the pathogenic role of H. pylori in PUD and gastric cancer was established, various treatment regimens were suggested with the goal of achieving complete bacterium eradication.
Along the years, as drug resistance and thereafter multi- drug resistance had emerged, more treatment regimens and rescue therapies became prevalent.6,7
The introduction of the first proton pump inhibitor (PPI), omeprazole, in 1988, followed by more PPI’s in the successive years, had revolutionized the treatment of both- PUD and H. pylori.8,9
The last international consensus was held in 2015 and included 43 experts from 24 countries-The Maastricht V/Florence consensus report. Guidelines were published in 2017.10 According to these guidelines, treatment regimen should be prescribed according to specific regional drug resistance.10
Hence, since the discovery of H. pylori 40 years ago, treatment options changed dramatically adjacent to new drugs development and the emergence of multi- drug resistance. All these changes influenced deeply treatment regimens and eradication successes worldwide.
Current computational power elicited the “text-mining” technique. This method facilitates broad-scale data extraction.11 It is used to extract data in a structured form from free-text. These data can then be used for a variety of tasks, such as database annotation or delineation of complex relationships and transferring of useful knowledge between different research domains. Text-mining may be employed to characterize trends and examine dynamics in a research field.12–14
Therefore, in our current study, we used the text mining technique in order to enlighten and clarify H. pylori’s treatment trends since its’ discovery, and to evaluate published literature on treatment regimens in the past four decades. Special attention was attributed towards drug resistance and geographic distribution.
Materials and Methods
Dataset
The US National Center for Biotechnology Information (NCBI) provides public application programming interfaces (APIs) that allow programmatic access to the PubMed database.
We have used the publicly available PyMed Python package to query the PubMed API.
The following data were extracted for each entry: PubMed unique article ID (PMID), title, publishing journal, abstract text, keywords (if any), and authors’ affiliations. Data lock was performed on June 15, 2021.
Inclusion Criteria
The entire MEDLINE/PubMed database was used as the source for this article. We retrieved all available H. pylori -related entries. The search was conducted in entries’ titles, abstracts, and keywords using the terms “Helicobacter pylori” OR “H.pylori”. We have limited the entries to entries that were published up-to December 31, 2020.
Data Processing
For text-mining, each title, study abstract, and authors’ affiliations were lowercased. Two gastrointestinal specialists (AL, ES) decided in consensus on a list of terms to classify entries (Supplementary Table 1). The terms specify three types of treatment groups: antibiotics, medications, and probiotics. Each entry was categorized by querying the title, abstract and keywords for terms belonging to the treatment groups. Entries could belong to more than one treatment group. We have also analyzed publication trends of different regimen types (Supplementary Table 2).
Also, we have sub-analyzed entries which were related to antibiotic resistance, which contained the terms “resistance” OR “eradication failure” OR “treatment failure”. These entries were divided to those containing the antibiotics “clarithromycin”, “amoxicillin”, “metronidazole”, or “levofloxacin”.
Following data extraction, all authors’ countries were retrieved from the affiliation data. Depending on the affiliations list, entries could be attributed to more than one country. Only publications with a country affiliation were utilized in the country-related sub-analysis. The publication trends of the top-five countries who belonged to the “resistance” group were analyzed.
We have also analyzed trends in publications related to antibiotic resistance and bacterial virulence genotypes (Supplementary Table 3).
Statistical Analysis
The data processing and result visualization were written on Python (Python software foundation, Version 3.6.5). Statistical significance was established at a 2-sided P < 0.05. Descriptive statistics were reported using counts with percentages for categorical variables.
Trends of the annual number of related publications were plotted for different treatment types, regimen types, antibiotic resistance, and antibiotic resistance and bacterial virulence genotypes. The slopes of publication trends were calculated by fitting linear regression to the annual number of publications in the years 2000–2020 (with X being the year of publication and Y being the number of publications per year). P-values and standard errors (SE) were calculated for the linear regression lines.
Results
Overall, out of 32 million available PubMed publications, 47,170 (0.1%) H. pylori-related entries were retrieved. Papers were published between 1987 and 2020. Figure 1 shows the study flow chart. For geographical analyses, 39,396 (83.5%) entries had a country affiliation.
 |
Figure 1 Study flow chart. |
Publication Trends
Figure 2A presents publication trends by treatment types. Medication treatment showed the highest number of total publications 6183/47,170 (13.1%), followed by antibiotics 5493/47,170 (11.6%), and probiotic which was substantially lower (0.7%). Since 2008, the number of publications for medication treatment and antibiotics was relatively similar.
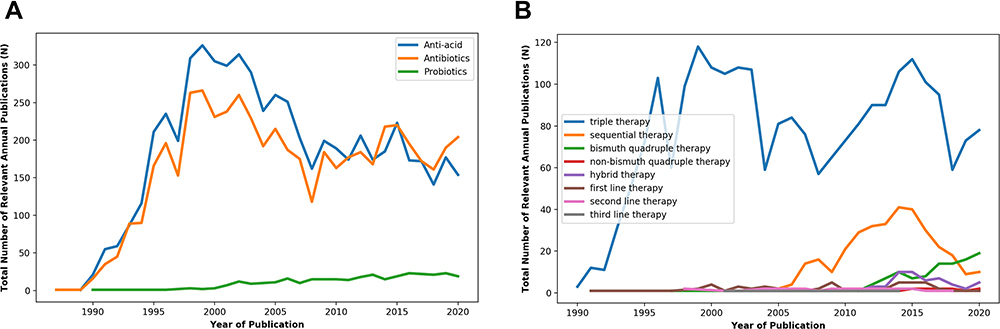 |
Figure 2 (A) Trends of Helicobacter pylori publications during 1987–2020, grouped by treatment type. (B) Trends of Helicobacter pylori publications according to treatment regimen type. |
Up until the year 2000, there was a linear upward slope of annual publications relating to medication and antibiotic treatment (31.8±2.5 publications/year p<0.001 and 23.3±2.3 publications/year p<0.001, respectively). These trends were reversed in 2000, as the annual number of publications showed a downward-slope (−7.9±1.1 publications/year, p<0.001 and −2.9±1.2 publications/year p<0.001, respectively). The publication for probiotic treatment showed a constant marginally upward trend.
For treatment regimens type, triple therapy had the highest number of publications 2400/47,170 (5.1%) followed by sequential therapy 342/47,170 (0.7%), and bismuth quadruple therapy 115/47,170 (0.2%) (Figure 2B).
Analysis by antibiotic resistance showed that clarithromycin treatment had the highest number of publications 3537/47,170 (7.5%) followed by amoxicillin 2723/47,170 (5.8%), metronidazole 2610/47,170 (5.5%), tetracycline 1029/47,170 (2.2%), and levofloxacin 652/47,170 (1.4%) (Figure 3).
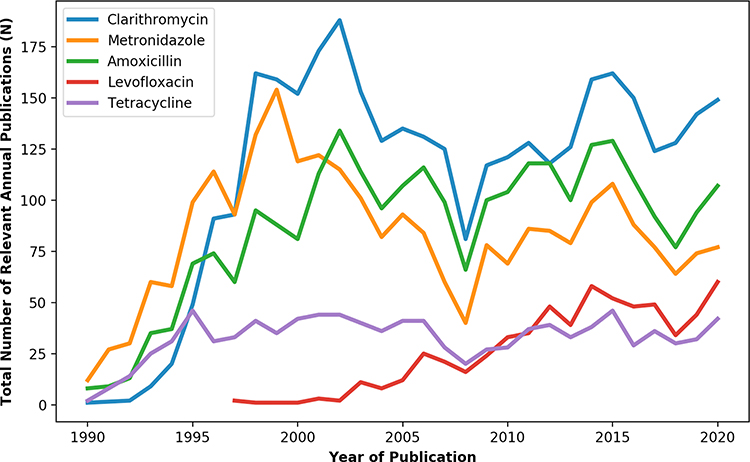 |
Figure 3 Trends of Helicobacter pylori publications according to antibiotic resistance. |
Sub-analysis of antibiotic resistance according to country of origin showed that the United States had the highest number of publications 474/3999 (11.9%). Other countries with a high number of publications relating to antibiotic resistance included China 339/3999 (8.5%, Japan 319/3999 (8.0%), Italy 269/3999 (6.7%), and South Korea 202/3999 (5.1%). Since 2013 there is a steep upward slope (5.1±0.7 publications/year, p<0.001) for publications originating from China.
Generally, a higher number of publications was evident for bacterial virulence than antibiotic resistance genotype. However, resembling trends can be evident between these two variables whereby the upward and downward slops are similar (Figure 4).
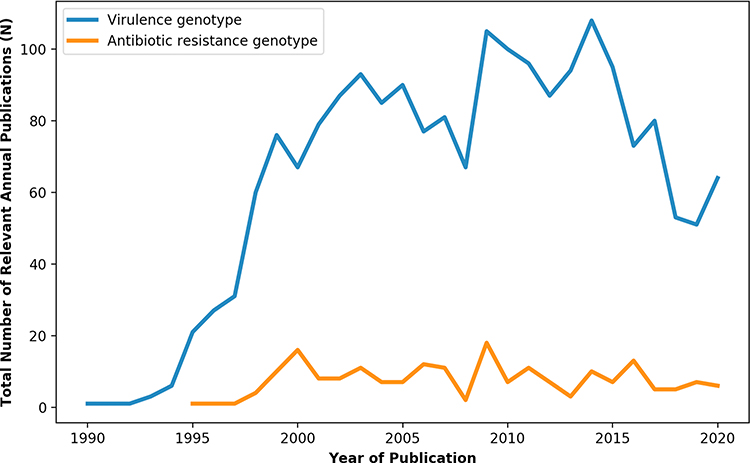 |
Figure 4 Trends of Helicobacter pylori publications according to bacterial virulence and antibiotic resistance genotype. |
Discussion
Since Barry J. Marshall and Robin Warren discovered the bacterium Helicobacter pylori 40 years ago, about 50,000 scientific publications were published worldwide. Throughout the four decades passed, high volume of scientific data regarding the bacterium role in the pathogenesis of gastric inflammation, peptic disease and gastric malignancy was accumulated. Treatment strategies were developed and changed along with emergence of antibiotic resistance, and new insights regarding different factors influencing bacterium’s transmission, virulence and drug resistance were unmasked.
In our current study, we applied a text mining approach to observe and analyze H. pylori publications in the past four decades, aiming to achieve some comprehensions about the progress attained in the understanding of the pathogenic role of this highly prevalent human infectious pathogen, and treatment strategies developed.
Since the 1990s, different national and international guidelines for the management of H. pylori-related diseases have been published and periodically updated regarding indications for treatment, diagnostic procedures, and preferred treatment regimens. These guidelines examined the outcome of different regimens of antibiotics and recommended the changes of the preferred treatment.
Reviewing treatment strategies, our analysis revealed that the most studied treatment regimen, highly outnumbers other treatments, is the triple therapy. First publications were issued as early as the beginning of the nineties, reaching a peak around 2000 and a second peak in 2015 (Figure 2). Hence, triple therapy was the preferred treatment for decades, and gained high popularity worldwide.
Only 15 years later, after the year 2005, other treatment regimens emerged, as a consequence of accumulating data observing antibiotic resistance (Figure 3). The second most studied treatment was the sequential therapy, with publication numbers that are 7 times lower than the triple therapy. Studies evaluating this treatment initiated in 2005 and reached a peak around 2015. The third in the list of studied treatments is the bismuth quadruple therapy. Publications evaluating this treatment regimen started to emerge during 2012, and in contrary to the declining publication numbers of the triple and sequential therapy in the last years, the slope of publications in this treatment regimen has an upward trend, with a constant increase in publications. These results are consistent with the last recommendations published for the management of H. pylori infection—the Maastricht V/Florence Consensus Report,10 which support this treatment regimen in most cases due to the increasing clarithromycin resistance worldwide.
Although H. pylori treatment is regimen- based, with a combination of anti- acid treatment and antibiotic for achieving improved eradication rate, we broadened our inspection and analyzed separately publications rate assessing three medications type: anti- acid medications, antibiotics and probiotics. (Figure 1). As expected, publications numbers for anti- acid treatment and antibiotics are very similar, since both treatments are essential parts of all treatment regimens, with same slopes trends. For probiotics, however, the picture is different; publication numbers are almost 20 times lower than for anti- acid medications, but there is a steady slow rise in publications slope throughout the years. This finding is in line with the growing understanding of the role of probiotics in maintaining the host gastrointestinal microbiota and the effect of probiotics on antibiotic treatment. Hence, probiotic was found to improve patient’s compliance to therapy, probably due to reducing treatments’ side effects, and to help in achieving better therapeutic results.15
H. pylori resistance to antibiotic therapy is a major concern during H. pylori treatment. In Figure 2 we analyzed publications trends regarding antibiotic resistance. As expected, the most studied antibiotic resistance is resistance to Clarithromycin. According to recent treatment guidelines,10 this resistance determines the treatment protocol of choice. Since the triple therapy, the most prevalent and studied treatment regimen contains Clarithromycin, the growing resistance to this antibiotic gradually changed the whole protocol management. As shown in Figure 2, publications slope reached the peak around the year 2000, and following the accumulating evidence for this growing resistance other treatment regimen started to emerge a few years later as shown in Figure 1B. Until the year 2000, the second most studied antibiotic resistance was Metronidazole. Thereafter, due to the growing resistance the use of this antibiotics declined, and as a result there is a parallel decline in publications rate. As publications rate for Metronidazole declined, publications regarding Amoxicillin resistance raised, and outnumbered those of Metronidazole. As reflects in our data, due to the growing resistance to Clarithromycin and Metronidazole, new treatment options emerged. One of the most popular antibiotics for second- line treatment was the quinolone levofloxacin.16–18 However, alongside the rise in this antibiotic’s usage, so did its resistance incidence. This increase in resistance rates is reflected in the publications trend, that shows a gradual increase in publications assessing levofloxacin’s resistance starting from around 2000 with a steady upward trend till nowadays. (Figure 3). Tetracycline resistance was evaluated in approximately 2% of publications (Figure 3). Publications trends remained steady since 1995, and are the lowest in the last decade. Tetracycline is part of one treatment regimen - PBMT (PPI, Bismuth, Metronidazole, Tetracycline), which also contains Metronidazole and its’ efficacy is affected by resistance to both antibiotics.19
Sub-analysis of antibiotic resistance according to country of origin showed that the United States had the highest number of publications. However, since the year 2015 until nowadays there is a steep rise in publications from China assessing antibiotics resistance, reflecting the massive H. pylori screening and eradication policy in China aiming at gastric cancer prevention summarized in the Taipei global consensus from 2020.20
Last, we analyzed publications trends for H. pylori’s genotype subtypes. As shown in Figure 3, most publications assessed the bacterium’s virulence genotype, and only a minority assessed resistance to antibiotic genotype. This finding is in line with the importance attributed to H. pylori’s virulence in the pathogenesis of carcinogenesis.21,22
Our study has a few limitations. This analysis only provides a high-level look at the field. The sheer number of publications prohibits a manual analysis of the records. A list of terms was determined based on current data in the literature and consensus between two senior Gastroenterologists. However, different terms might have achieved different results. The data was extracted from MEDLINE/PubMed. Other options as google scholar were not included Using other databases could have modified the results; however, PubMed is the most popular database source for biomedical literature.
In conclusion,
In our current study, we observed H. pylori publication trends since its discovery, four decades ago. Our findings clearly reflect the changes of the commonly prescribed regimens along the years, following the occurrence and the rise of the H. pylori antibiotic resistance. We believe our study has an historical value in order to understand the evolution along 40 years since was H. pylori discovered. In recent years there is a steep rise in publications in countries with policies of screening and eradication for gastric cancer prevention, which is currently not applied in Western countries. Intensifying treatment with probiotics is steadily rising along with the accumulating data regarding its Benefits in raising eradication rates, which, surprisingly, did not reflect yet in the international guidelines.
We believe that more treatment regimens and strategies will develop such as the development of more narrow-spectrum treatment or treatment supplements together with better anti acid drugs. These, along with the growing knowledge considering resistance prevalence and the mechanisms leading to resistance formation will change the upcoming eradication therapies. A text-mining analysis of H. pylori publications contributes to the understanding of treatment options and development trends worldwide.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest to declare.
References
1. Guarner F, Khan AG, Garisch J, et al. World gastroenterology organisation global guidelines: probiotics and prebiotics October 2011. J Clin Gastroenterol. 2012;46:468–481. doi:10.1097/MCG.0b013e3182549092
2. Sonnenberg A. historic changes of Helicobacter pylori‐associated diseases. Aliment Pharmacol Ther. 2013;38:329–342. doi:10.1111/apt.12380
3. Graham DY. History of Helicobacter pylori, duodenal ulcer, gastric ulcer and gastric cancer. World J Gastroenterol. 2014;20:5191. doi:10.3748/wjg.v20.i18.5191
4. Marshall B, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984;323:1311–1315. doi:10.1016/S0140-6736(84)91816-6
5. Ahmed N, Sechi LA. Helicobacter pylori and gastroduodenal pathology: new threats of the old friend. Ann Clin Microbiol Antimicrob. 2005;4:1–10. doi:10.1186/1476-0711-4-1
6. O’Connor A, Furuta T, Gisbert JP, O’Morain C. Review–treatment of helicobacter pylori infection 2020. Helicobacter. 2020;25:e12743. doi:10.1111/hel.12743
7. Flores-Treviño S, Mendoza-Olazarán S, Bocanegra-Ibarias P, Maldonado-Garza HJ, Garza-González E. Helicobacter pylori drug resistance: therapy changes and challenges. Expert Rev Gastroenterol Hepatol. 2018;12:819–827. doi:10.1080/17474124.2018.1496017
8. Shin JM, Munson K, Vagin O, Sachs G. The gastric HK-ATPase: structure, function, and inhibition. Pflug Arch Eur J Physiol. 2009;457:609–622. doi:10.1007/s00424-008-0495-4
9. Sachs G, Shin JM, Vagin O, et al. The gastric H, K ATPase as a drug target: past, present, and future. J Clin Gastroenterol. 2007;41:S226. doi:10.1097/MCG.0b013e31803233b7
10. Malfertheiner P, Megraud F, O’Morain CA, et al. Management of Helicobacter pylori infection—the Maastricht V/Florence consensus report. Gut. 2017;66:6–30. doi:10.1136/gutjnl-2016-312288
11. Thuraisingham B. Data Mining: Technologies, Techniques, Tools, and Trends. CRC press; 2014.
12. Soffer S, Klang E, Tau N, et al. Evolution of colorectal cancer screening research in the past 25 years: text-mining analysis of publication trends and topics. Therap Adv Gastroenterol. 2020;13:1756284820941153. doi:10.1177/1756284820941153
13. Wang S-H, Ding Y, Zhao W, et al. Text mining for identifying topics in the literatures about adolescent substance use and depression. BMC Public Health. 2016;16:279. doi:10.1186/s12889-016-2932-1
14. Zhang Y, Tao J, Wang J, et al. Trends in diatom research since 1991 based on topic modeling. Microorganisms. 2019;7:213. doi:10.3390/microorganisms7080213
15. Ji J, Yang H. Using probiotics as supplementation for Helicobacter pylori antibiotic therapy. Int J Mol Sci. 2020;21:1136. doi:10.3390/ijms21031136
16. Hu Y, Zhu Y, Lu N-H. Novel and effective therapeutic regimens for Helicobacter pylori in an era of increasing antibiotic resistance. Front Cell Infect Microbiol. 2017;7:168. doi:10.3389/fcimb.2017.00168
17. Fallone CA, Chiba N, van Zanten SV, et al. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology. 2016;151:51–69. e14. doi:10.1053/j.gastro.2016.04.006
18. Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG clinical guideline: treatment of Helicobacter pylori infection. Off j Am Coll Gastroenterol. 2017;112:212–239. doi:10.1038/ajg.2016.563
19. Savoldi A, Carrara E, Graham DY, Conti M, Tacconelli E. Prevalence of antibiotic resistance in Helicobacter pylori: a systematic review and meta-analysis in World Health Organization regions. Gastroenterology. 2018;155:1372–1382. e1317. doi:10.1053/j.gastro.2018.07.007
20. Liou J, Malfertheiner P, Lee YC, et al. Asian Pacific Alliance on Helicobacter and microbiota (APAHAM), et al. Screening and eradication of Helicobacter pylori for gastric cancer prevention: the Taipei global consensus. Gut. 2020;69:2093–2112. doi:10.1136/gutjnl-2020-322368
21. Sukri A, Hanafiah A, Mohamad Zin N, Kosai NR. Epidemiology and role of Helicobacter pylori virulence factors in gastric cancer carcinogenesis. Apmis. 2020;128:150–161. doi:10.1111/apm.13034
22. Baj J, Forma A, Sitarz M, et al. Helicobacter pylori virulence factors—mechanisms of bacterial pathogenicity in the gastric microenvironment. Cells. 2021;10:27.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.