Back to Journals » Clinical Ophthalmology » Volume 20
Changes in Corneal Biomechanics and Epithelial Thickness in High Myopia Over −8.00D with/without Myopic Regression After Femtosecond Laser-Assisted in Situ Keratomileusis
Authors Shao T, Li H, Peng Y, Zhang J, Wang H, Long K
Received 3 December 2025
Accepted for publication 5 March 2026
Published 27 March 2026 Volume 2026:20 586339
DOI https://doi.org/10.2147/OPTH.S586339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Sotiria Palioura
Ting Shao,1– 3 Hua Li,1– 3 Yusu Peng,1– 3 Jiafan Zhang,1– 3 Huifeng Wang,1– 3 Keli Long1– 3
1Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University, Qingdao, Shandong, People’s Republic of China; 2State Key Laboratory Cultivation Base, Shandong Key Laboratory of Eye Diseases, Qingdao, Shandong, People’s Republic of China; 3School of Ophthalmology, Shandong First Medical University, Qingdao, Shandong, People’s Republic of China
Correspondence: Keli Long, Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University, No. 5. Yanerdao Road, Shi-Nan District, Qingdao, Shandong, 266000, People’s Republic of China, Email [email protected]
Purpose: To compare the changes in corneal biomechanics and epithelial thickness after femtosecond laser-assisted in situ keratomileusis (FS-LASIK) in high myopia over − 8.00D patients with and without myopia regression.
Methods: This retrospective case-control study included thirty-nine patients. Based on refractive status at one year after surgery, patients with a myopic shift ≥ 1.00 D were classified as the myopic regression group (R group, 33 eyes), while the remaining patients were classified as the normal group (N group, 42 eyes). Preoperative and postoperative visual outcomes, refraction, topography, corneal epithelial thickness, and corneal biomechanics were compared.
Results: Ambrosio relational thickness to the horizontal profile (ARTh) at 3, 6, and 12 months postoperatively was significantly smaller in the R than in the N group, with mean differences of − 9.75 (95% confidence interval (CI): − 18.44 to − 1.04), p= 0.029; − 12.23 (95% CI: − 20.02 to − 4.42), p= 0.003; and − 9.47 (95% CI: − 16.86 to − 2.08), p= 0.013, respectively. Meanwhile, the stiffness parameter A1 (SP-A1) at 6 and 12 months after surgery was smaller in the R than in the N group, with mean differences of − 6.62 (95% CI: − 12.85 to − 0.37), p= 0.038 and − 7.26 (95% CI: − 13.79 to − 0.71), p= 0.030, respectively. The postoperative changes in SP-A1 at 6 and 12 months were significantly larger in the R group than in the N group (6.47, 95% CI: 1.04 to 11.91, p= 0.020; and 5.96, 95% CI: 0.37 to 11.52, p= 0.037, respectively). In addition, corneal epithelial thickness (CET) in different zones showed a significant negative correlation with refractive error at 12 months after surgery, with correlation coefficients ranging from − 0.55 to − 0.32 (all p< 0.05, with the central zone showing p< 0.001).
Conclusion: Ultra-high myopic patients with post-FS-LASIK regression have poorer corneal biomechanics and greater central epithelial thickening, highlighting these factors as key susceptibility features for refractive instability. Early assessment of these parameters may help identify at-risk patients and guide personalized management to improve long-term outcomes.
Keywords: myopic regression, FS-LASIK, biomechanics, epithelial thickness, ultra-high myopia
Introduction
Refractive regression can significantly impact the long-term stability and predictability of corneal refractive surgery, thereby impairing visual performance and quality of life.1 This complication is particularly concerning in patients with ultra-high myopia (typically spherical equivalent > −8.00 D), as the deeper laser ablation required in these cases leaves a thinner residual stromal bed, increasing the risk of biomechanical instability and subsequent myopic shift.1,2 It is well-documented that myopic regression increases with higher corrections,1 and the reduction in corneal biomechanical strength correlates with the percentage of tissue altered (PTA) and residual stromal bed thickness.2
Current corneal refractive surgeries include photorefractive keratectomy (PRK), which ablates stroma after epithelial removal; laser in situ keratomileusis (LASIK), which creates a corneal flap followed by stromal ablation; and small incision lenticule extraction (SMILE), a flapless technique that removes an intrastromal lenticule through a small incision. Each technique carries specific complications: PRK may cause postoperative pain and corneal haze;1 LASIK involves flap-related risks such as dislocation and epithelial ingrowth, and significantly alters corneal biomechanics due to flap creation;1,2 SMILE better preserves biomechanical strength but is technically demanding.2 Among these, femtosecond LASIK (FS-LASIK) is particularly relevant for ultra-high myopia correction, yet its impact on biomechanical stability warrants further investigation.
Myopic regression after refractive surgery for correcting high myopia is not uncommon,3,4 and the increased epithelial thickness is one of the major causes of this complication.5 The −8.00 D threshold for ultra-high myopia was selected based on our previous finding that most patients with significant regression after FS-LASIK had preoperative spherical equivalent exceeding −8.00 D, with greater epithelial thickening and biomechanical compromise.5 Clinically, patients between −8.00 D and −10.00 D are the primary FS-LASIK candidates for high myopia, while those exceeding −10.00 D increasingly choose implantable collamer lens (ICL) surgery. More specifically, myopic regression can occur when the epithelial thickness in the central zone becomes greater than that in the paracentral and mid-periphery zone.6 Previous studies showed that typical procedures such as PRK, LASIK, and SMILE can increase epithelial thickness.7,8 In theory, refractive regression can be a surgical retreatment procedure; however, the likelihood of postoperative corneal ectasia is markedly increased, and many patients are no longer suitable for retreatment due to the thin corneal thickness after the first surgery. In such a case, the preferred approach to treat myopic regression is to use steroids and antiglaucoma medications to temporarily improve visual acuity.5,9
Currently, it is believed that changes in the corneal curvature gradient and the decrease in corneal biomechanics are the main reasons for epithelial remodeling and thickening during regression.10,11 The combination of corneal laser with collagen cross-linking can improve postoperative corneal biomechanics, significantly reducing epithelial thickness.11–13 However, whether this method can improve postoperative refractive status and vision remains inconclusive.14 In addition, epithelial thickness has also been considered to be influenced by additional parameters such as corneal wound healing, nerve injury, and regeneration.15
Our previous study (Li et al, 2022) prospectively investigated steroid treatment response in patients with established regression after FS-LASIK or TPRK.5 In contrast, the present retrospective case-control study investigates early biomechanical and epithelial predictors of regression in a consecutive ultra-high myopia cohort followed from surgery through 12 months. While the prior work examined epithelial changes after regression occurred, the current study focuses on pre-regression characteristics that may identify at-risk patients. Early identification of biomechanical predictors in ultra-high myopia enables proactive management—such as counseling, prophylactic corneal cross-linking (CXL), or intensified monitoring—thereby improving surgical safety and long-term stability. Therefore, the purpose of this study was to investigate the epithelial thickness increase and corneal biomechanical changes after FS-LASIK in ultra-high-myopic patients with and without postoperative myopia regression.
Patients And Methods
Patients and Measurements
This retrospective case-control study consecutively enrolled 39 patients (75 eyes) who underwent FS-LASIK for ultra-high myopia (SE > −8.00 D) at Qingdao Eye Hospital between May 2021 and July 2023 and completed the 12-month follow-up. Table 1 summarizes the inclusion and exclusion criteria.16 All surgeries were uneventful, and no eyes were excluded due to postoperative complications.
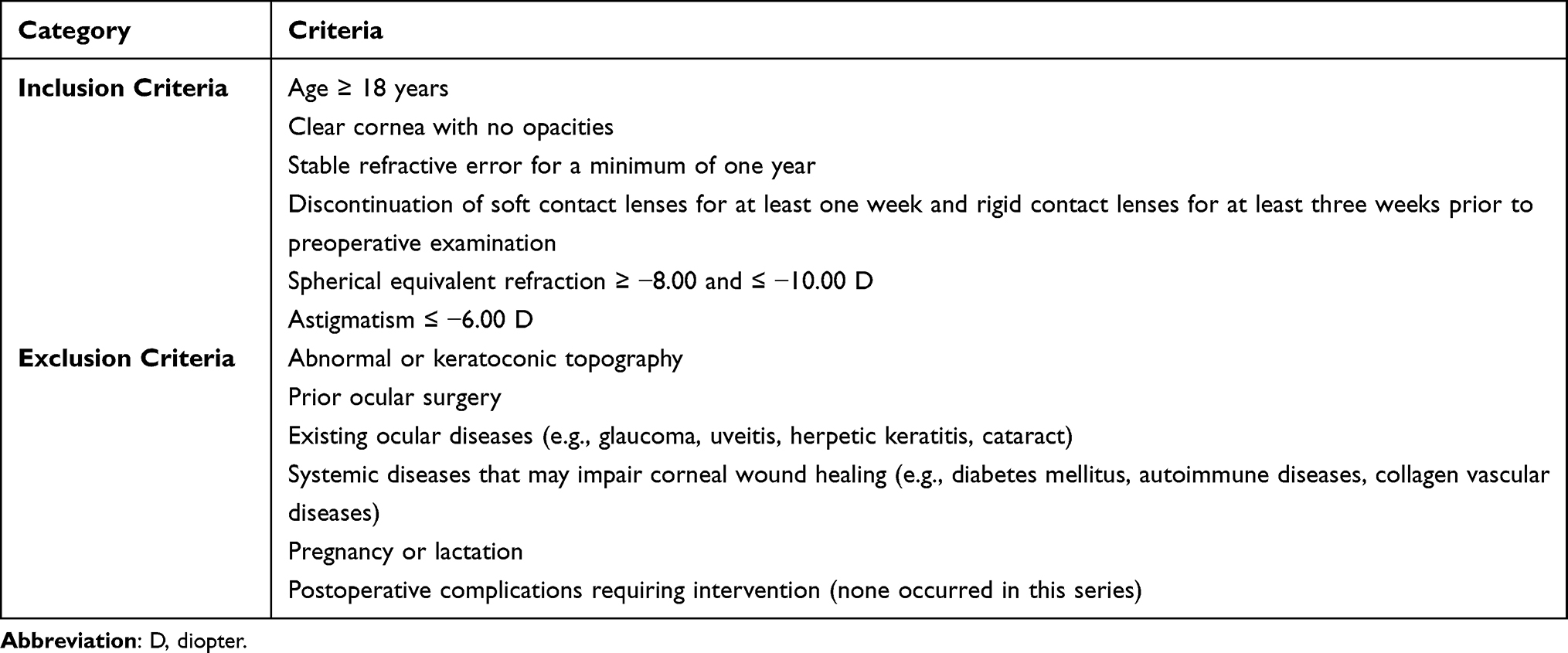 |
Table 1 Inclusion and Exclusion Criteria |
Based on refractive status at 12 months postoperatively, eyes with a myopic shift ≥ 1.00 D were classified as the regression group (R group, 33 eyes), and those with shift < 1.00 D as the normal group (N group, 42 eyes). This classification was determined solely by the objective refractive outcomes at 12 months postoperatively, rather than by any preoperative patient characteristics or investigator assignment.
The patients were thoroughly briefed on the objectives of our research, including the potential advantages and disadvantages associated with FS-LASIK surgery. Each patient signed an informed consent form to take part in the study. The study protocol adhered to the principles outlined in the Declaration of Helsinki and received approval from the Ethics Committee of Qingdao Eye Hospital of Shandong First Medical University [2021]02.
Standard ophthalmic examinations were performed on all patients, including axial length, corneal curvature and thickness, cycloplegic and manifest refraction, slit-lamp evaluation of the anterior and posterior segment, uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), and intraocular pressure (IOP). The Pentacam analysis system (Oculus, Pentacam HR, Wetzlar, Hesse, Germany), dynamic Scheimpflug analyzer (Oculus, Corvis ST, Wetzlar, Hesse, Germany), and anterior segment optical coherence tomography (Optovue Inc., RTVue-100, Fremont, CA, USA) were used to perform the measurements before and after the surgery. The epithelial thickness map, which encompasses a 7-mm diameter area, was separated into 17 sectors. This included a central 2-mm zone and eight octants equally distributed within the paracentral (2–5 mm), and midperipheral (5–7 mm) zones. The same skilled doctor performed all examinations. This standardized protocol is automatically generated by the RTVue OCT system and is widely used in corneal refractive surgery research because it provides comprehensive spatial distribution of epithelial thickness.5 The central zone is of particular interest as epithelial thickening in this region has been associated with myopic regression, while the paracentral and mid-peripheral zones allow assessment of the epithelial remodeling pattern across the cornea.6
Surgical Methods
A skilled surgeon (KL) performed all FS-LASIK surgeries under topical anesthesia. A WaveLight FS200 femtosecond laser (WaveLight GmbH, FS200, Erlangen, Germany) was used to create each flap, with a thickness of 110 µm and a diameter of 8.3 mm. The hinge position was superior, and the pulse energy was 0.80 µJ.17 The Amaris 750S excimer laser (Schwind Eye-Tech-Solutions, Amaris 750S, Kleinostheim, Germany) with an optical zone of 6.0–6.3 mm was utilized for laser ablation. All surgical operations went smoothly, with emmetropia as the targeted postoperative refraction. The standard postoperative regimen included one drop each of 0.3% levofloxacin qid for one week and 0.1% fluorometholone qid for the first two weeks, and then reduced once every two weeks. Following surgery, all patients were followed up 1 day, 1 week, 1 month, 3 months, 6 months, and 1 year. Uncorrected and corrected distance visual acuity (UDVA and CDVA, respectively), subjective refraction, IOP, topography, corneal biomechanics, and CET were evaluated in the patients.
Statistical Analysis
All data were analyzed using IBM SPSS version 27.0. Continuous variables are presented as mean ± standard deviation. Normality was assessed using the Kolmogorov–Smirnov test. To compare the two groups across multiple time points, a two-way repeated measures ANOVA was performed. Comparisons at each time point were conducted using estimated marginal means with Bonferroni adjustment. Statistical significance was set at p < 0.05. Pearson correlation was used to examine the relationship between corneal epithelial thickness (CET) and refractive error at 12 months. Linear regression quantified these relationships, reporting slopes (β) with 95% confidence intervals.
Sensitivity Analysis
As both eyes from some patients were included, a sensitivity analysis was performed by randomly selecting one eye per patient (39 eyes) and re-analyzing ARTh at 12 months using an independent samples t-test.
Post-Hoc Power Analysis
A post-hoc power analysis was performed based on the primary outcome (ARTh at 12 months). With observed means (R group: 114.19 ± 14.57; N group: 123.66 ± 16.92), the effect size was 0.60 (Cohen’s d). Using G*Power 3.1 (α = 0.05, power = 80%), the estimated minimum sample size was approximately 36 eyes per group. Our study (33 R group, 42 N group) is adequately powered.
Results
Baseline
Based on their refractive status one year after surgery, patients with a myopic shift of 1.00 D or greater were classified as the myopic regression group (R group), while the remaining patients were classified as the normal group (N group). A total of 33 eyes from 17 patients and 42 eyes from 22 patients were included in the R group and N group, respectively. No significant differences were observed in preoperative parameters, including sphere, cylinder, SE, central corneal thickness, mean corneal curvature, optical zone, and ablation depth (p > 0.05), between the two groups (Table 2).
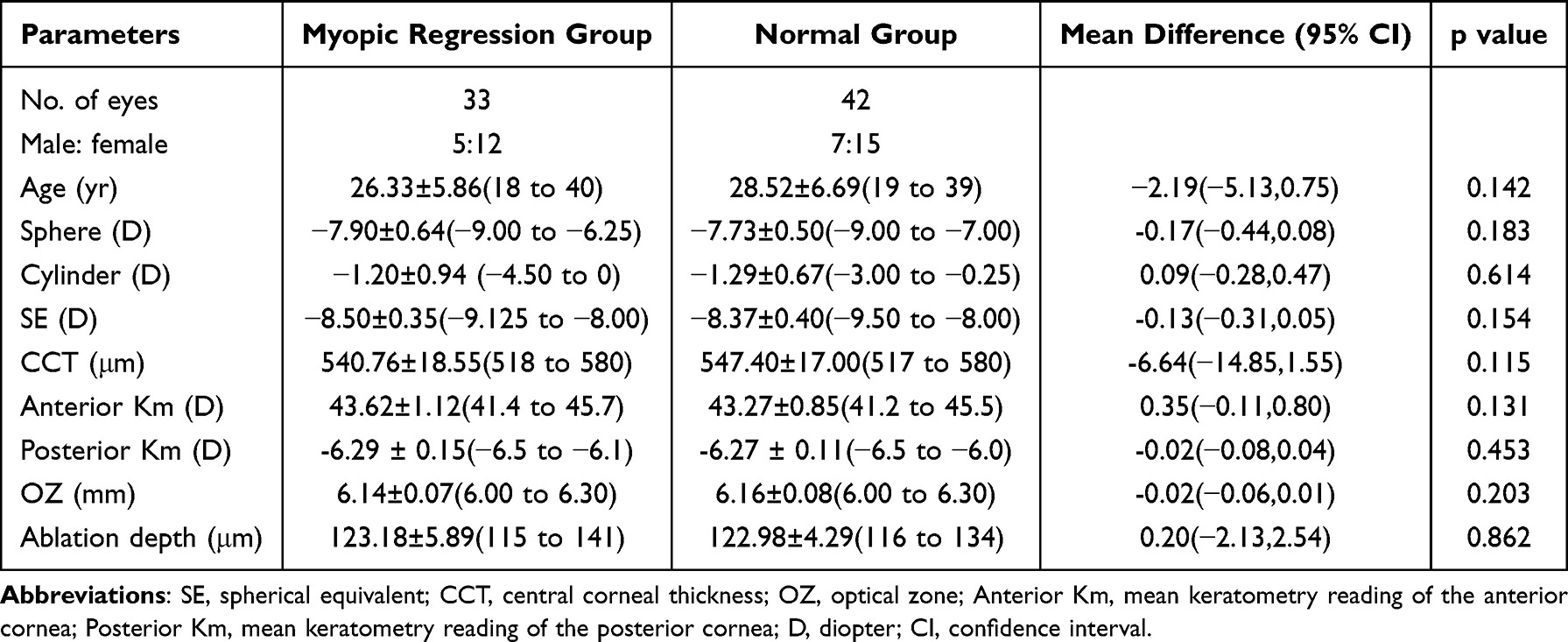 |
Table 2 Baseline Characteristics of the Patients in Both Groups |
Visual Acuity and Refractive Status
Visual acuities were converted to the logarithm of the minimum angle of resolution (logMAR) for analysis. A statistically significant difference was observed in UDVA, sphere, and SE of the myopic regression group and normal group at 3, 6, and 12 months after surgery (all p < 0.05), as shown in Table 3. In contrast, no differences were observed in CDVA and cylinder between both groups at 3, 6, and 12 months postoperatively (all p > 0.05).
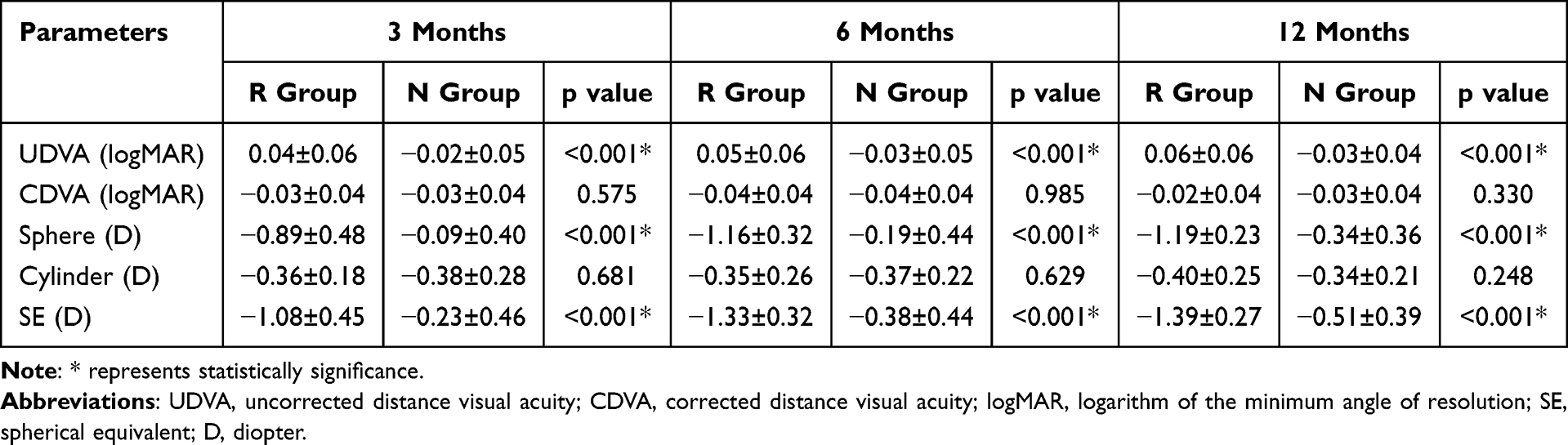 |
Table 3 Comparison of Visual Acuity and Refractive Status Between the Two Groups |
Posterior Corneal Surface Parameters
The flat K reading (K1) of posterior corneal curvature in the R group was −6.11±0.14D, −6.07±0.14D, −6.07±0.14D, and −6.08±0.15D prior to and 3, 6, and 12 months post-surgery, respectively. The steep K reading (K2) of posterior corneal curvature was −6.50±0.19D, −6.44±0.19D, −6.47±0.18D, and −6.48±0.19D preoperatively and 3, 6, and 12 months postoperatively, respectively. The mean K reading (Km) of posterior corneal curvature was −6.29±0.15D, −6.26±0.14D, −6.29±0.15D, and −6.29±0.15D before and 3, 6, and 12 months after surgery, respectively. In the N group, the K1 was −6.08±0.11D, −6.05±0.12D, −6.06±0.12D, and −6.06±0.11D prior to and 3, 6, and 12 months post-surgery, respectively. The K2 was −6.46±0.16D, −6.43±0.16D, −6.46±0.17D, and −6.46±0.15D before and 3, 6, and 12 months after surgery, respectively. The Km was −6.27±0.11D, −6.24±0.11D, −6.26±0.11D, and −6.26±0.12D prior to and 3, 6, and 12 months post-surgery, respectively. No significant differences were observed between the two groups for any posterior corneal surface parameter (K1, K2, or Km) at any time point (preoperative: all p≥0.379; 3 months: all p≥0.458; 6 months: all p≥0.411; 12 months: all p≥0.264).
Corneal Biomechanical Parameters
The corneal biomechanical parameters of the regression group and the normal group both pre and postoperatively are shown in Table 4. Our findings revealed that the Ambrosio relational thickness to the horizontal profile (ARTh) was significantly smaller in the regression group than in the normal group at all follow-up visits (p =0.029; p =0.003; p =0.013). Meanwhile, the stiffness parameter A1 (SP-A1) was smaller in the regression group than in the normal group at 6 and 12 months after surgery (p =0.038; p =0.030). No significant differences in other biomechanical parameters were observed between the two groups (all p > 0.05).
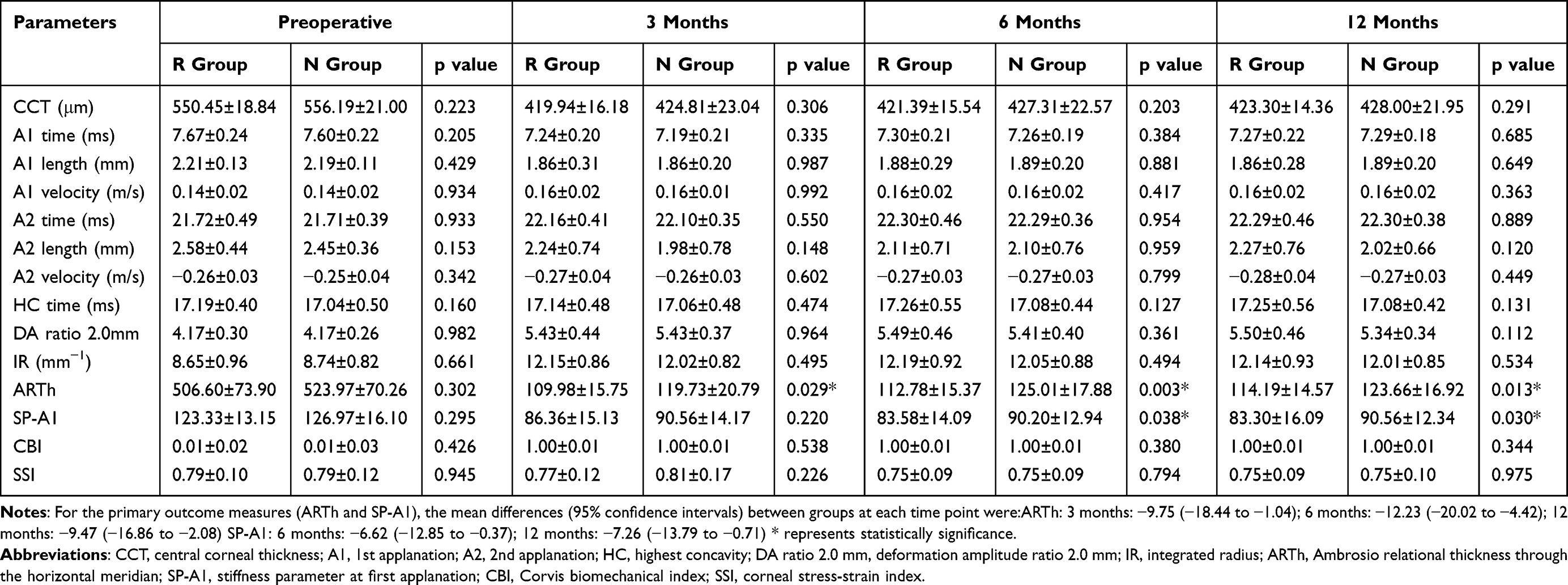 |
Table 4 Corneal Biomechanics Parameters Preoperatively and Postoperatively |
Changes in the Corneal Biomechanical Parameters
Changes in the corneal biomechanical parameters before and after surgery between the two groups are shown in Table 5. SP-A1 changes at 3, 6, and 12 months after surgery were greater in the regression group than in the normal group; however, this change was statistically significant at 6 and 12 months (p =0.020 and 0.037), but not at 3 months (p =0.312). No differences in other biomechanical parameters were observed.
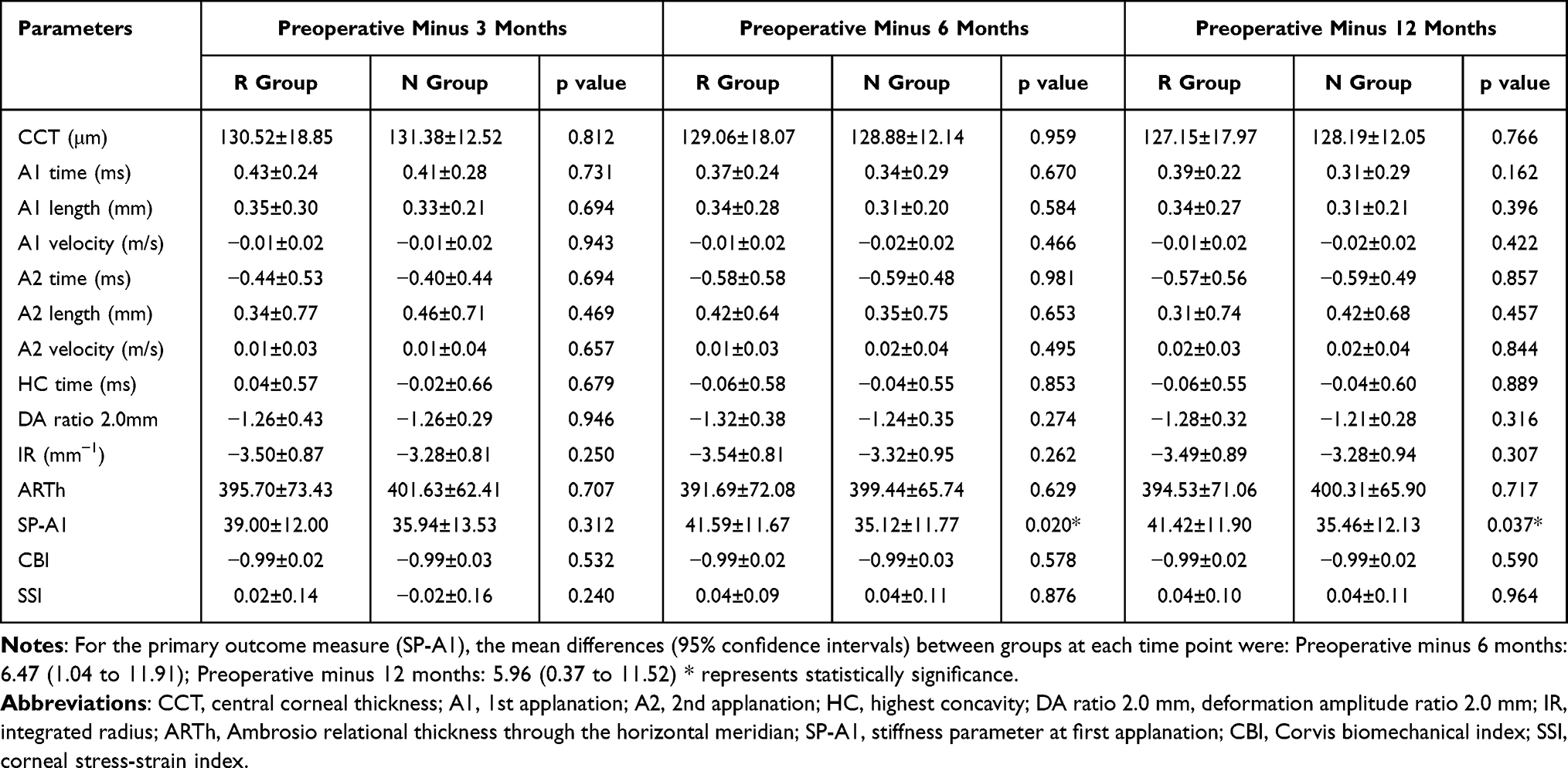 |
Table 5 Change in Corneal Biomechanics Parameters |
Corneal Epithelial Thickness
CET was divided into 17 different zones in the 7-mm diameter area, as shown in Figure 1A–C) demonstrates the corneal schematic diagram in different zones, which displays the mean and standard deviation of CET in both groups before and 12 months after surgery. CET between the two groups did not show any statistically significant difference before surgery. In contrast, at 12 months postoperatively, CET in the regression group was significantly thicker than that in the normal group in 15 of the 17 zones, with p values ranging from <0.001 to 0.042. The exceptions were the T7 and ST7 zones, where the differences did not reach statistical significance (T7: p = 0.617; ST7: p = 0.085).
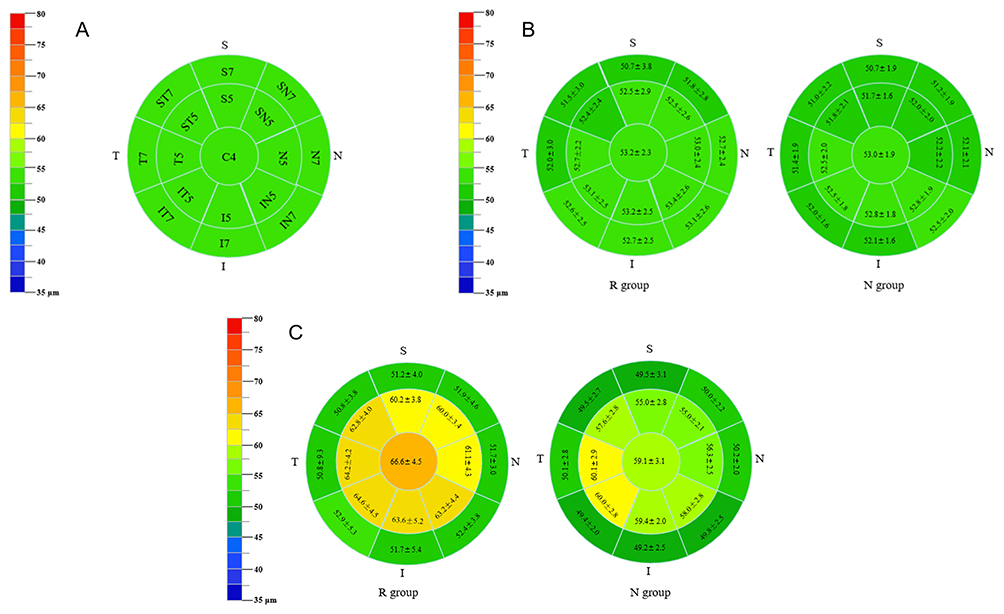 |
Figure 1 Comparison of the preoperative and postoperative corneal epithelial thickness between the two groups (A): Seventeen different zones in the 7-mm diameter area of corneal epithelial thickness, C= central, S= superior, T= temporal, I= inferior, N= nasal; (B) Pre-operative; (C) 12 months after surgery. |
Correlations Between Corneal Epithelial Thickness and the Refractive Error
Correlation and regression analyses were performed to evaluate the relationship between corneal epithelial thickness (CET) and refractive error at 12 months after surgery.
Pearson correlation analysis revealed that CET in nine zones (the central 2-mm zone and eight paracentral 2–5 mm zones) showed a significant negative correlation with refractive error (all p < 0.05, Figure 2). The correlation coefficients ranged from −0.55 to −0.32 across these zones, indicating a moderate to strong negative relationship.
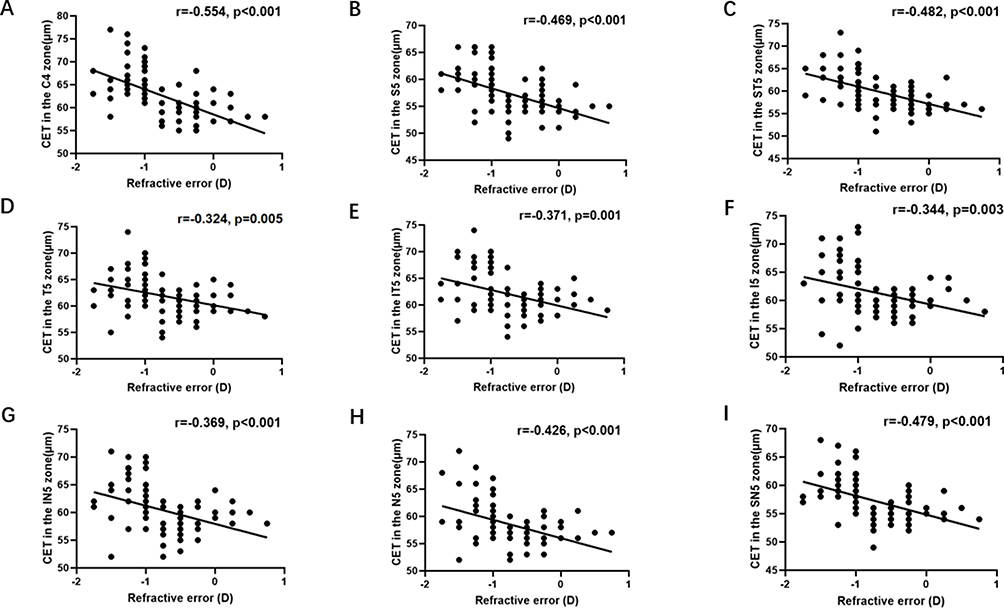 |
Figure 2 Correlation between corneal epithelial thickness in nine different zones and refractive error at 12 months after surgery (A): C4 zone, (B) S5 zone, (C) ST5 zone, (D) T5 zone, (E) IT5 zone, (F) I5 zone, (G) IN5 zone, (H) N5 zone, (I) SN5 zone; CET: corneal epithelial thickness. |
Linear regression analysis further quantified these relationships. In the central zone (C4), each 1-μm increase in CET was associated with a 0.056 D decrease in refractive error (β = −0.056, 95% confidence interval (CI): −0.076 to −0.036, p < 0.001). Across the paracentral zones, the slopes ranged from −0.060 to −0.043, with all p values < 0.05. The corresponding scatterplots and correlation coefficients are shown in Figure 2.
Sensitivity Analysis
To assess the potential impact of inter-eye correlation, a sensitivity analysis using one randomly selected eye per patient was performed. The results were consistent with the main analysis: ARTh at 12 months remained significantly lower in the regression group (111.68 ± 11.91 vs. 123.76 ± 16.17, mean difference: −12.08, 95% CI: −21.56 to −2.61, p = 0.014).
Discussion
In this study, we found that ultra-high myopic patients who developed postoperative regression after FS-LASIK exhibited significantly lower ARTh and SP-A1 values at 3, 6, and 12 months compared to those with stable refraction (Table 4). These parameters, reflecting corneal stiffness and thickness progression,18,19 are known to decrease after refractive surgery.2 Few studies have investigated whether this decrease differs between eyes with and without subsequent regression. Our findings suggest that such differences may exist, indicating that early postoperative biomechanical measurements could potentially help identify patients at higher risk for refractive instability. Furthermore, the regression group showed significantly greater central epithelial thickening at 12 months, with a strong negative correlation between epithelial thickness and refractive error (Figure 2), implicating epithelial remodeling as a key contributor to the myopic shift. These findings extend the current understanding of post-FS-LASIK regression by linking it to both biomechanical compromise and regional epithelial hyperplasia in the vulnerable ultra-high myopia population.
Our data showed that both ARTh and SP-A1 after FS-LASIK were smaller in the R group than that in the N group at all follow-up times. SP-A1 is regarded as an important parameter for assessing corneal stiffness at the time of first applanation,18 and larger SP-A1 values indicate stiffer corneas. ARTh is the quotient of corneal thickness at the thinnest point of the horizontal meridian and thickness progression.19 Therefore, a lower ARTh value is suggestive of a thinner cornea and a faster thickness progression toward the periphery. In the present study, it indicated the thicker and stiffer corneas in N group than that in R group after surgery.
While SP-A1 and ARTh were significantly lower in the regression group, the stress-strain index (SSI) —a parameter reflecting intrinsic material stiffness independent of thickness—showed no significant difference between groups. This dissociation suggests that regression-prone corneas are not materially softer, but rather structurally disadvantaged: they are thinner with steeper thickness progression (lower ARTh). Biomechanical measurements reflect not only tissue hardness but also thickness, structure, and hydration. Even with comparable intrinsic material properties (SSI), differences in corneal geometry lead to distinct stress distribution under intraocular pressure. This differential stress may be perceived differently by epithelial cells, influencing their proliferative response and contributing to epithelial remodeling and regression. Thus, susceptibility to regression in ultra-high myopic eyes appears driven primarily by structural reserve rather than material weakness.
Anterior surfaces flattened by laser ablation are commonly compensated by epithelial remodeling and thickening to maintain good optical quality of the cornea after refractive surgery.5,10,20 In our study, CET in different zones showed a significant negative correlation with refractive error at 12 months after surgery. However, epithelial thickening patterns matter: lenticular-shaped central thickening increases optical power and promotes regression, while negative meniscus-like peripheral thickening does not.21 Reinstein et al22 showed an approximate 6-µm increase in epithelial thickness over the central 7-mm corneal zone at 1 year after LASIK for myopia. After the first month, the authors observed that the epithelium thickened by 5 µm and correlated with a −0.38 D shift in refraction. In contrast, our findings revealed a significantly greater degree of epithelial thickening at one year after surgery, because we included patients with ultra-high myopia, as opposed to Reinstein et al which included patients with moderate to low myopia.
In our previous study, the postoperative refractive status of patients undergoing FS-LASIK was more likely to drift to myopia than TPRK when correcting high myopia, which may be related to the more decreased biomechanical stability and more obvious epithelial thickening after FS-LASIK.23 Kanellopoulos and Asimellis believe that postoperative epithelial thickness is not only influenced by the corneal curvature gradient, but also by corneal biomechanics.24,25 One factor is that the amount of epithelial thickening is determined by the rate of change of the curvature of the stromal surface.26 Another possible factor is that a thinned cornea, hereby inducing epithelial hyperplasia.25,27 Beyond biomechanics, wound healing plays a crucial role: experimental studies demonstrate that inflammation, oxidative stress, and growth factors affect epithelial regeneration.28–30 This highlights the multifactorial nature of epithelial remodeling.
The combination of FS-LASIK and TPRK with prophylactic high-fluence cross-linking has been shown to strengthen corneal rigidity and decrease the degree of epithelial thickening, reducing the probability of refractive regression.11,12 In our study, ARTh and SP-A1 of the refractive regression group were lower than those of the normal group, accompanied by an increase in corneal epithelial thickness. Previous studies revealed superior postoperative biomechanical outcomes following SMILE than after FS-LASIK,31–34 and that the degree of epithelial hyperplasia is greater after FS-LASIK than after SMILE in both central and paracentral regions.7 This in turn suggests that biomechanical changes are closely related to the degree of epithelial hyperplasia, and the greater they are, the more obvious the corneal epithelial hyperplasia can be. In addition to the thickening of the corneal epithelium, other studies suggested that refractive regression is related to the protrusion of the posterior corneal surface.35–37 As shown in the results, we also analyzed the postoperative corneal posterior surface parameters of the two groups and did not find any differences.
This study has several limitations. First, we could not confirm the exact starting point of refractive regression. Although the epithelial thickness profile has been reported to be stable between 3 and 12 months after surgery,22 the absence of epithelial measurements at earlier postoperative time points precludes analysis of the temporal relationship between epithelial remodeling and the onset of regression. Second, as a retrospective case-control study, our findings are subject to potential selection bias. This bias may not fully account for preoperative differences or confounding factors such as individual wound healing responses, preoperative biomechanical variations, or medication adherence. Although patients were enrolled consecutively to minimize bias, unmeasured confounding factors could not be fully controlled. Third, although both eyes from some patients were included, we did not explicitly account for inter-eye correlation in the primary analysis. However, a sensitivity analysis using one randomly selected eye per patient yielded consistent results for the primary outcome, suggesting that this potential bias is unlikely to have substantially influenced our main conclusions. Nevertheless, future prospective studies should employ appropriate statistical methods (eg., mixed-effects models or generalized estimating equations) to account for inter-eye correlation. Fourth, causative relationships cannot be established. Fifth, patient-reported outcomes such as subjective satisfaction were not assessed, limiting our ability to evaluate the full clinical impact of regression. Finally, the regression group (33 eyes) was slightly below the estimated ideal sample size (36 eyes). Larger prospective studies are warranted.
In conclusion, this study provides novel insights into the biomechanical and epithelial characteristics associated with regression after FS-LASIK. Our findings demonstrate that ultra-high myopic patients who develop regression exhibit poorer postoperative corneal biomechanics (lower ARTh and SP-A1) and greater central epithelial thickening. The negative correlation between epithelial thickness and refractive error further underscores the role of epithelial remodeling in refractive outcomes. These results highlight that compromised biomechanical integrity and regional epithelial hyperplasia are key features of eyes susceptible to regression. Early assessment of these parameters may help identify at-risk patients, enabling personalized management and improving long-term refractive stability.
Funding
The authors have no funding to declare for this study.
Disclosure
The authors do not have any conflict of interest and have no commercial or proprietary interest in this work.
References
1. Yan MK, Chang JS, Chan TC. Refractive regression after laser in situ keratomileusis. Clin Exp Ophthalmol. 2018;46(8):934–11. doi:10.1111/ceo.13315
2. Pniakowska Z, Jurowski P, Wierzbowska J. Clinical evaluation of corneal biomechanics following laser refractive surgery in myopic eyes: a review of the literature. J Clin Med. 2022;12(1):243. doi:10.3390/jcm12010243
3. Fu D, Zhang ZY, Wang L, Zhou XT, Yu ZQ. Refractive regression and changes in central corneal thickness three years after laser-assisted subepithelial keratectomy for high myopia in eyes with thin corneas: a retrospective study. Semin Ophthalmol. 2017;32(5):631–641. doi:10.3109/08820538.2016.1142579
4. Chen YI, Chien KL, Wang IJ, et al. An interval-censored model for predicting myopic regression after laser in situ keratomileusis. Invest Ophthalmol Vis Sci. 2007;48(8):3516–3523. doi:10.1167/iovs.06-1044
5. Li H, Han Q, Zhang J, Shao T, Wang H, Long K. Role of corneal epithelial thickness during myopic regression in femtosecond laser-assisted in situ keratomileusis and transepithelial photorefractive keratectomy. BMC Ophthalmol. 2022;22(1):481. doi:10.1186/s12886-022-02727-x
6. Cho Y, Hieda O, Wakimasu K, et al. Multiple linear regression analysis of the impact of corneal epithelial thickness on refractive error post corneal refractive surgery. Am J Ophthalmol. 2019;207:326–332. doi:10.1016/j.ajo.2019.05.016
7. Ryu IH, Kim BJ, Lee JH, Kim SW. Comparison of corneal epithelial remodeling after femtosecond laser-assisted LASIK and small incision lenticule extraction (SMILE). J Refract Surg. 2017;33(4):250–256. doi:10.3928/1081597X-20170111-01
8. Gauthier CA, Holden BA, Epstein D, Tengroth B, Fagerholm P, HambergNyström H. Role of epithelial hyperplasia in regression following photorefractive keratectomy. Br J Ophthalmol. 1996;80(6):545–548. doi:10.1136/bjo.80.6.545
9. Kamiya K, Aizawa D, Igarashi A, Komatsu M, Shimizu K. Effects of antiglaucoma drugs on refractive outcomes in eyes with myopic regression after laser in situ keratomileusis. Am J Ophthalmol. 2008;145(2):233–238. doi:10.1016/j.ajo.2007.09.036
10. Reinstein DZ, Archer TJ, Gobbe M. Rate of change of curvature of the corneal stromal surface drives epithelial compensatory changes and remodeling. J Refract Surg. 2014;30(12):799–802. doi:10.3928/1081597X-20141113-02
11. Kanellopoulos AJ, Asimellis G. Epithelial remodeling after femtosecond laser-assisted high myopic LASIK: comparison of stand-alone with LASIK combined with prophylactic high-fluence cross-linking. Cornea. 2014;33(5):463–469. doi:10.1097/ICO.0000000000000087
12. Kang DSY, Kim SW. Effect of corneal cross-linking on epithelial hyperplasia and myopia regression after transepithelial photorefractive keratectomy. J Refract Surg. 2019;35(6):354–361. doi:10.3928/1081597X-20190422-01
13. Lee H, Yong Kang DS, Ha BJ, et al. Comparison of outcomes between combined transepithelial photorefractive keratectomy with and without accelerated corneal collagen cross-linking: a 1-year study. Cornea. 2017;36(10):1213–1220. doi:10.1097/ICO.0000000000001308
14. Kohnen T, Lwowski C, Hemkeppler E, et al. Comparison of femto-LASIK with combined accelerated cross-linking to femto-lasik in high myopic eyes: a prospective randomized trial. Am J Ophthalmol. 2020;211:42–55. doi:10.1016/j.ajo.2019.10.024
15. Wilson SE, Mohan RR, Hong JW, Lee JS, Choi R, Mohan RR. The wound healing response after laser in situ keratomileusis and photorefractive keratectomy: elusive control of biological variability and effect on custom laser vision correction. Arch Ophthalmol. 2001;119(6):889–896. doi:10.1001/archopht.119.6.889
16. Shao T, Li H, Zhang J, Wang H, Liu S, Long K. Comparison of wavefront-optimized and corneal wavefront-guided transPRK for high-order aberrations (>0.35 μm) in myopia. J Cataract Refract Surg. 2022;48(12):1413–1418. doi:10.1097/j.jcrs.0000000000001012
17. Liu Y, Ma B, Zhao L, et al. Influence of dendritic cells on corneal nerve morphological analysis and clinical relevance in chronic dry eye disease after femtosecond laser-assisted laser in situ keratomileusis. Front Med. 2025;12:1568787. doi:10.3389/fmed.2025.1568787
18. Roberts CJ, Mahmoud AM, Bons JP, et al. Introduction of two novel stiffness parameters and interpretation of air puff-induced biomechanical deformation parameters with a dynamic scheimpflug analyzer. J Refract Surg. 2017;33(4):266–273. doi:10.3928/1081597X-20161221-03
19. Teixeira LB, Carvalho RID, Quaresma SM, Caiado CAL, Ambrósio Jr R. Horizontal pachymetric profile for the detection of keratoconus. Rev Bras Oftalmol. 2015;74:382–385. doi:10.5935/0034-7280.20150080
20. Reinstein DZ, Srivannaboon S, Gobbe M, et al. Epithelial thickness profile changes induced by myopic LASIK as measured by Artemis very highfrequency digital ultrasound. J Refract Surg. 2009;25(5):444–450. doi:10.3928/1081597X-20090422-07
21. Moshirfar M, Desautels JD, Walker BD, Murri MS, Birdsong OC, Hoopes PCS. Mechanisms of optical regression following corneal laser refractive surgery: epithelial and stromal responses. Med Hypothesis Discov Innov Ophthalmol. 2018;7(1):1–9.
22. Reinstein DZ, Archer TJ, Gobbe M. Change in epithelial thickness profile 24 hours and longitudinally for 1 year after myopic LASIK: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg. 2012;28(3):195–201. doi:10.3928/1081597X-20120127-02
23. Zhang J, Feng Q, Ding W, Peng Y, Long K. Comparison of clinical results between trans-PRK and femtosecond LASIK for correction of high myopia. BMC Ophthalmol. 2020;20(1):243. doi:10.1186/s12886-020-01515-9
24. Vinciguerra P, Roberts CJ, Albé E, et al. Corneal curvature gradient map: a new corneal topography map to predict the corneal healing process. J Refract Surg. 2014;30(3):202–207. doi:10.3928/1081597X-20140218-02
25. Kanellopoulos AJ, Aslanides IM, Asimellis G. Correlation between epithelial thickness in normal corneas, untreated ectatic corneas, and ectatic corneas previously treated with CXL: is overall epithelial thickness a very early ectasia prognostic factor? Clin Ophthalmol. 2012;6:789–800. doi:10.2147/OPTH.S31524
26. Reinstein DZ, Archer TJ, Gobbe M. Refractive and topographic errors in topography-guided ablation produced by epithelial compensation predicted by 3D Artemis VHF digital ultrasound stromal and epithelial thickness mapping. J Refract Surg. 2012;28(9):657–663. doi:10.3928/1081597X-20120815-02
27. Kanellopoulos AJ, Asimellis G. Introduction of quantitative and qualitative cornea optical coherence tomography findings induced by collagen cross-linking for keratoconus: a novel effect measurement benchmark. Clin Ophthalmol. 2013;7:329–335. doi:10.2147/OPTH.S40455
28. Meduri A, Scorolli L, Scalinci SZ, et al. Effect of the combination of basic fibroblast growth factor and cysteine on corneal epithelial healing after photorefractive keratectomy in patients affected by myopia. Indian J Ophthalmol. 2014;62(4):424–428. doi:10.4103/0301-4738.119420
29. Meduri A, Grenga PL, Scorolli L, Ceruti P, Ferreri G. Role of cysteine in corneal wound healing after photorefractive keratectomy. Ophthalmic Res. 2009;41(2):76–82. doi:10.1159/000187623
30. Meduri A, Scalinci SZ, Morara M, et al. Effect of basic fibroblast growth factor in transgenic mice: corneal epithelial healing process after excimer laser photoablation. Ophthalmologica. 2009;223(2):139–144. doi:10.1159/000187686
31. Xin Y, Lopes BT, Wang J, et al. Biomechanical Effects of tPRK, FS-LASIK, and SMILE on the Cornea. Front Bioeng Biotechnol. 2022;10:834270. doi:10.3389/fbioe.2022.834270
32. Wu D, Wang Y, Zhang L, Wei S, Tang X. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2014;40(6):954–962. doi:10.1016/j.jcrs.2013.07.056
33. Elmohamady MN, Abdelghaffar W, Daifalla A, Salem T. Evaluation of femtosecond laser in flap and cap creation in corneal refractive surgery for myopia: a 3-year follow-up. Clin Ophthalmol. 2018;12:935–942. doi:10.2147/OPTH.S164570
34. He S, Luo Y, Ye Y, et al. A comparative and prospective study of corneal biomechanics after SMILE and FS-LASIK performed on the contralateral eyes of high myopia patients. Ann Transl Med. 2022;10(13):730. doi:10.21037/atm-22-330
35. Chan TC, Liu D, Yu M, Jhanji V. Longitudinal evaluation of posterior corneal elevation after laser refractive surgery using swept-source optical coherence tomography. Ophthalmol. 2015;122(4):687–692. doi:10.1016/j.ophtha.2014.10.011
36. Nemet A, Mimouni M, Vainer I, Sela T, Kaiserman I. Factors associated with changes in posterior corneal surface following photorefractive. Graefes Arch Clin Exp Ophthalmol. 2021;259(11):3477–3483. doi:10.1007/s00417-021-05237-6
37. Qi H, Hao Y, Xia Y, Chen Y. Regression-related factors before and after laser in situ keratomileusis. Ophthalmologica. 2006;220(4):272–276. doi:10.1159/000093083
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.