Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Challenging and Successful Therapy Decision-Making for AML Post Cytotoxic Therapy and Concomitant Active Breast Cancer – A Case Report and Experience-Driven Strategy
Authors Wichtowski M ![]() , Adamska M
, Adamska M ![]() , Łojko-Dankowska A, Gil L
, Łojko-Dankowska A, Gil L
Received 15 May 2025
Accepted for publication 20 December 2025
Published 30 January 2026 Volume 2026:18 536327
DOI https://doi.org/10.2147/BCTT.S536327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pranela Rameshwar
Mateusz Wichtowski,1 Monika Adamska,2 Anna Łojko-Dankowska,2 Lidia Gil2
1Department of Surgical Oncology, Institute of Oncology; Poznan University of Medical Sciences, Poznan, Poland; 2Department of Hematology, Transplantation and Cellular Therapies; Poznan University of Medical Sciences, Poznan, Poland
Correspondence: Monika Adamska, Department of Hematology, Transplantation and Cellular Therapies; Poznan University of Medical Sciences, Szamarzewskiego 84 St, Poznań, 60-569, Poland, Email [email protected]
Background: Breast cancer (BC) represents the most frequent female malignancy worldwide, and one of the rare, however life-threatening, complications after oncological treatment is acute myeloid leukemia post cytotoxic therapy (AML-pCT). Moreover, most AML-pCT cases have contributed to previous BC cytotoxic therapies. The treatment approach for AML-pCT in BC survivors with an active second BC represents the challenging decision-making process that is described in this report.
Results: A 48-year-old woman was diagnosed with invasive lobular carcinoma of the right breast (T2N0M0, BRCA1 negative) and successfully treated with breast-conserving therapy, adjuvant radiotherapy, and hormone therapy. Seven years later, she was diagnosed with ductal carcinoma in situ in the left breast, and unexpectedly, directly before the surgery, with leukocytosis, anemia, and thrombocytopenia. Hematological investigation revealed a diagnosis of AML-pCT (intermediate ELN2022 risk group). After a management conference involving both oncologists and haematologists, conserving surgery of the left breast (pTis, pNX) was performed. Seven days later the patient started intensive antileukemic treatment with “ 3+7” induction chemotherapy, followed by two consolidation chemotherapies, which resulted in complete remission (CR) of leukemia with negative measurable residual disease. Despite a high hematopoietic cell transplantation comorbidity index score (due to a previous neoplasm), the patient qualified for allogeneic hematopoietic cell transplantation (alloHCT). The procedure was performed using myeloablative conditioning with a matched unrelated donor. Currently, 3 years post-alloHCT, the patient remains in CR for all three neoplasms.
Conclusion: In this case report, we describe the therapeutic success of intensive alloHCT in AML-pCT patient with active BC. The presented treatment approach for active BC and AML-pCT requires collaboration between oncologists and hematologists to ensure fast decision-making.
Keywords: breast cancer, acute myeloid leukemia post cytotoxic therapy, case report
Introduction
Breast cancer (BC) represents the most frequent female malignancy worldwide, with the highest oncological mortality.1 Approximately one in eight woman will develop BC in the duration of her life.2 One of the rare, however life-threatening, unintended complications of BC treatment is acute myeloid leukemia post cytotoxic therapy (AML-pCT), which can occur after the use of successful primary cancer radiotherapy, chemotherapy or poly-ADP-ribose polymerase1 (PARP1) inhibitors.3,4
AML-pCT constitutes 20% of all acute myeloid leukemias and represents a subtype with a poor prognosis, with an estimated overall survival of 7–10 months and a complete response rate of 30%.5–7 The disease is characterized by adverse genetic abnormalities and a complex karyotype. Genes involved in the pathogenesis of AML-pCT can be grouped into functional classes: epigenetic regulators (ASXL1, DNMT3A, EZH2, IDH1/IDH2, TET2), transcription regulators (RUNX1, TP53), signaling pathway regulators (FLT3) and RNA spliceosome machinery regulators (SRSF2, SF3B1, U2AF1).8 Genomic instability may lead to emergence of aggressive subclones and treatment resistance.9 The only curative treatment option for AML-pCT is allogeneic hematopoietic cell transplantation (alloHCT).
BC represents the most frequent solid tumor contributing to AML-pCT.10 About 5% of all BC patients possess germline BRCA1 mutations.11,12 Of note, among AML-pCT after BC, germline mutations were noted in 21% and most commonly detected within BRCA1, TP53 and BRCA2 genes.13 In one study, myeloid neoplasms were diagnosed in 0.6–1.8% of BC survivors, occurring 5–10 years after BC diagnosis.14 Within BC survivors, the most common second neoplasm is the subsequent contralateral breast cancer (CBC).15
On the grounds that the occurrence of AML-pCT post BC is estimated to grow worldwide, we propose and discuss a challenging and successful therapeutic strategy for AML-pCT with concomitant active BC, as illustrated by the history.
Case Report
A 48-year-old caucasian woman with hypothyroidism (family history of BC in mother) was diagnosed with invasive lobular carcinoma (ILC) (T2 N0 M0) of the right breast in 2014 (positive for estrogen and progesterone receptors, negative for HER2 receptors). She was treated surgically with breast-conserving therapy (BCT) and sentinel node biopsy (SNB), with subsequent adjuvant radiotherapy (52.5 Gy, 6 MV photons) and hormonotherapy. Genetic testing of germline BRCA1 mutations yielded negative results. After treatment, the ILC BC remained in remission, and the patient was under the care of an outpatient oncological surgical clinic (Figure 1).
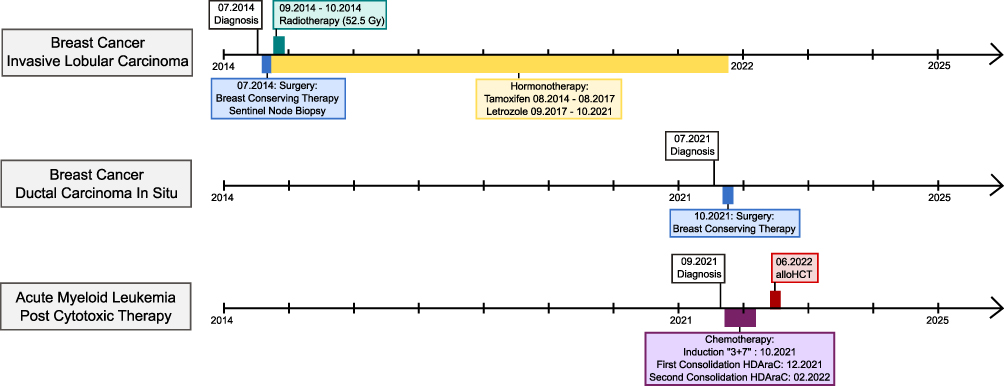 |
Figure 1 Time axis with the treatment of three neoplasms. |
Seven years later (07.2021), routine mammography revealed microcalcifications in the left breast (BI-RADS: 4B). Physical examination of the breast and axillary region revealed no clinical findings. A biopsy of the suspected area (08.2021) revealed ductal carcinoma in situ (DCIS) with comedo necrosis and high nuclear atypia (negative for both estrogen and progesterone receptors, positive for androgen receptors). Based on the aforementioned results, the patient was primarily qualified for oncological treatment with surgery and adjuvant radiotherapy of the left breast.
Unexpectedly, a peripheral blood count performed on the day of admission to the surgical ward (09.2021) revealed high leukocytosis (> 163 × 109/L), anemia (4.4 mmol/L), and thrombocytopenia (39 × 109/L) (Table 1). The patient was in a good general condition without any symptoms or complaints. Therefore, she was transferred to the hematology department, where bone marrow aspiration revealed AML-pCT diagnosis with the presence of 80% myeloblasts. Molecular biology results revealed negative results for the following markers: CBFB::MYH11 and RUNX1::RUNX1T1 fusion genes, FLT3-TKD, FLT3-ITD, NPM1, BCR-ABL and TP53 mutations (in classical karyotyping, metaphases were not analyzable). Considering the above-mentioned results, the disease was classified as an intermediate genetic risk subgroup (European LeukemiaNet 2022 stratification), and the patient’s Charlson Comorbidity Index (CCI) score of 3 points (due to the presence of a previous neoplasm).
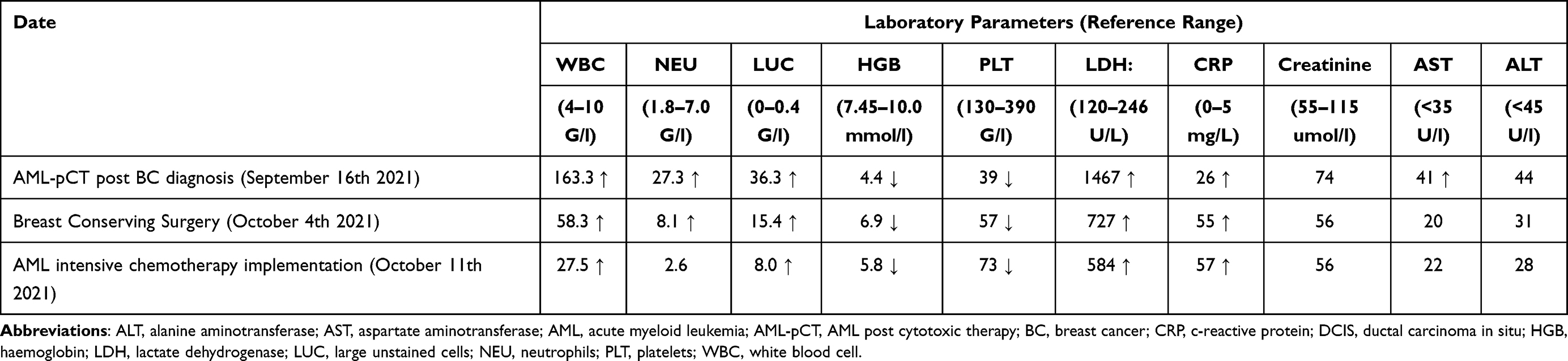 |
Table 1 Laboratory Parameters in Different Moments |
At this point, during a management conference between hematologists, oncologists, and surgical oncologists, intensive treatment with subsequent alloHCT versus palliative treatment for AML was discussed. For a DCIS, surgery was the most reasonable option. This was mainly due to the small tumor size (limited to a cluster of microcalcifications) and negative receptor status, which translated into a lack of justification for changing hormonal treatment (the patient was already receiving hormonal treatment because of a previous BC).
AML-pCT represents a life-threatening condition requiring urgent treatment. Importantly, at this moment, the only curative treatment option, alloHCT, was not possible because of active secondary BC. However, the abandonment of BC treatment may lead to rapid BC progression, which significantly worsens prognosis. On the other hand, early BC that has not spread beyond the breast or axillary lymph nodes can be completely cured with the rapid implementation of surgical treatment.
Finally, conserving surgery for BC was performed (10.2021), without sentinel node biopsy (low risk of DCIS progression according to imaging results). Importantly, as part of the preparation for BC surgery, the AML-pCT patient received hydroxycarbamide and required platelet and red blood cell transfusions (Table 1). Microscopic examination of the removed breast tissue did not reveal any further cancer cells; therefore, the diagnosis of DCIS was confirmed (pTis, pNx). At this stage, the patient did not require adjuvant BC therapy (Figure 1). When the platelet count reached >30 G/l the wound healed properly, without complications.
The patient was transferred to the hematology ward, and 7 days after surgery, intensive treatment with induction “3+7” chemotherapy consisting of daunorubicin and cytarabine (10.2021) was initiated (Table 1). The neutropenic period was complicated by probable invasive fungal disease (suggestive of chest CT scans); thus, voriconazole was implemented and resulted in improvement. Bone marrow examination after induction chemotherapy revealed complete remission (CR) of AML-pCT, with negative minimal residual disease (MRD), as measured by flow cytometry. Two consolidation therapies with high doses of cytarabine were implemented (12.2021, 01.2022) (Figure 1). The post-treatment bone marrow MRD remained at 0.000%.
Since the patient did not have a matched sibling donor, she qualified for alloHCT from an unrelated donor and was admitted to the transplantation unit (05.2022). Her age-adjusted hematopoietic cell transplantation comorbidity index (HCT-CI) score was 4. Myeloablative chemotherapy, consisting of busulfan and fludarabine, was introduced as a conditioning regimen before alloHCT. A stem cells infusion from 10/10 HLA-matched unrelated donor was performed (06.2022) (Figure 1). ATG, methotrexate, and cyclosporine were administered for the graft-versus-host disease (GvHD) prophylaxis. Neutrophil recovery (>0.5 G/l ANC) occurred on day +14 after infusion. A neutropenic period was complicated by Escherichia coli sepsis and oral mucositis. The patient’s condition improved after a standard empirical antibiotic therapy consisting of meropenem and colistin. She was discharged from the transplant unit (July 2022) in good general condition, without any symptoms or complaints. Three years after alloHCT, she remains under outpatient care in CR of AML-pCT, with 0.000% MRD and no symptoms of GvHD. Genetic testing of germline BRCA1, PALB2 and CHEK2 mutations yielded negative results. Importantly, the patient was also in the remission for both BCs (ILC in the right breast and DCIS in the left breast).
Discussion
We have described a successful therapeutic approach in the case of AML-pCT following primary BC with an active second CBC based on surgical CBC excision with subsequent rapid implementation of intensive AML-pCT treatment with alloHCT.
The presented case highlights the importance of close collaboration between hematologists, oncology surgeons, and oncologists in order to engage in proper individualized therapeutic decision-making.16
In this report, already existing indexes to evaluate the patient’s condition (eg CCI, HCT-CI) were not supportive, as they do not have regard for the presence of two active neoplasms but only for the history of treatment of any neoplasm.
Notably, the AML-pCT diagnosis did not disqualify the patient from surgical treatment; however, appropriate patient preparation before surgery was required. As AML-pCT represents a life-threatening condition that should be treated immediately, minimally invasive surgery ensuring fast recovery and wound healing for patients is recommended.
Patients with multiple neoplasms and BC in both breasts should be considered for genetic testing for inherited cancer risk.17 Among BC survivors with harmful BRCA1 and BRCA2 variants, the risk of CBC is increased.18 Importantly, BRCA1, BRCA2, and TP53 cancer susceptibility mutations were found in 17% of patients with myeloid neoplasms post cytotoxic therapy (including AML-pCT), contributing to leukaemogensis.19 In a study with AML-pCT following BC cytotoxic therapy, 20% of patients had BRCA1, BRCA2, or TP53 mutations.13
The CBC risk for BC survivors was elevated when lobular morphology of primary BC, with a tumor size >2 cm and negative estrogen HER2 receptors, was present.15 Myeloid leukemia was observed more frequently when BC was treated with chemotherapy, and the risk of CBC was lower for patients undergoing hormonotherapy.15 Thus, according to the above study, our patient exhibited risk factors for CBC. Importantly, there is growing need for early BC detection and for BC treatment tailored based on molecular profiling, because it may prevent cytotoxic treatment for early-stage BC20 and further lower the risk for developing AML-pCT post BC.
Among BC survivors who received cytotoxic therapy and with the occurrence of cytopenias who were referred for hematological check-up, every third patient was diagnosed with AML-pCT.21 In another study, Caucasian BC survivors had an increased risk of developing AML-pCT.22 Thus, BC survivors after cytotoxic therapy, particularly BC patients with germline cancer susceptibility mutations, should undergo regular hematological screening.
Nowadays, first-line intensive treatment of AML-pCT relies on CPX-351 chemotherapy, which significantly improves OS when compared to “3+7” chemotherapy: 5.96 versus 9.33 months.23 Importantly, three-year OS among alloHCT recipients after CPX-351 versus “3+7” chemotherapy was 56% versus 23% respectively.24 Emerging treatment for AML patients eligible for intensive therapies seems to be venetoclax combined with intensive chemotherapy as a frontline therapy, which is evaluated in ongoing clinical trials (NCT05177731, NCT04628026).25
The patient signed written informed consent to participate in a study (approval no. 1040/19, Bioethics Committee of Poznan University of Medical Science) conducted in accordance with the Declaration of Helsinki. Limitations: (1) for cancer susceptibility only BRCA1, PALB2 and CHEK2 gene mutations were tested.
Conclusion
To conclude, with increasing numbers of AML-pCT and active secondary neoplasms, we encourage hematologists and oncologists to have close collaboration in order to make fast and proper decisions. Patients with multiple neoplasms should undergo expanded genetic testing. AML-pCT post BC with active second CBC can be successfully treated with surgical excision of the CBC and rapid implementation of intensive leukemia treatment with subsequent alloHCT as the only curative modality. Decision-making frameworks for multiple neoplasms treatment approaches should be developed.
Abbreviations
alloHCT, allogeneic hematopoietic cell transplantation; AML-pCT, acute myeloid leukemia post cytotoxic therapy; ANC, absolute neutrophil count; BC, breast cancer; BCT, breast-conserving therapy; CBC, contralateral breast cancer; CCI, Charlson Comorbidity Index; CR, complete remission; DCIS, ductal carcinoma in situ; ELN2022, European LeukemiaNet 2022 stratification; GvHD, graft versus host disease; HCT-CI, hematopoietic cell transplantation comorbidity index; ILC, invasive lobular carcinoma; MRD, minimal residual disease; SNB, sentinel node biopsy.
Patient Consent
Written informed consent was obtained from the patient, and she agreed to publication of the details of her case. This study and the publication of the case report were approved by the Bioethics Committee of Poznan University of Medical Science (approval no.1040/19).
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–7. doi:10.3322/caac.21834
2. Jahangiri L. The impact of extracellular vesicles on breast cancer metastasis and therapeutics: genetic considerations. Cancer Genet. 2025;298–299:1–9. doi:10.1016/j.cancergen.2025.08.003
3. Khoury JD, Solary E, Abla O, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: myeloid and Histiocytic/Dendritic Neoplasms. Leukemia. 2022;36(7):1703–1719. doi:10.1038/s41375-022-01613-1
4. Sonkin D, Thomas A, Teicher BA. Cancer treatments: past, present, and future. Cancer Genet. 2024;286–287:18–24. doi:10.1016/j.cancergen.2024.06.002
5. Chantadisai M, Kulkarni HR, Baum RP. Therapy-related myeloid neoplasm after peptide receptor radionuclide therapy (PRRT) in 1631 patients from our 20 years of experiences: prognostic parameters and overall survival. Eur J Nucl Med Mol Imaging. 2021;48(5):1390–1398. doi:10.1007/s00259-020-05127-9
6. Morton LM, Dores GM, Schonfeld SJ, et al. Association of Chemotherapy for Solid Tumors With Development of Therapy-Related Myelodysplastic Syndrome or Acute Myeloid Leukemia in the Modern Era. JAMA Oncol. 2019;5(3):318–325. doi:10.1001/jamaoncol.2018.5625
7. Döhner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140(12):1345–1377. doi:10.1182/blood.2022016867
8. Martignoles JA, Delhommeau F, Hirsch P. Genetic Hierarchy of Acute Myeloid Leukemia: from Clonal Hematopoiesis to Molecular Residual Disease. Int J Mol Sci. 2018;19(12):3850. doi:10.3390/ijms19123850
9. Liu H, Dilger JP. Different strategies for cancer treatment: targeting cancer cells or their neighbors? Chin J Cancer Res. 2025;37(2):289–292. doi:10.21147/j.issn.1000-9604.2025.02.12
10. Adamska M, Kowal-Wiśniewska E, Barańska M, et al. Acute Myeloid Leukemia Post Cytotoxic Therapy in Breast Cancer Survivors-Over 23 Years of Single Center Analysis. J Clin Med. 2024;13(4):989. doi:10.3390/jcm13040989
11. Malone KE, Daling JR, Doody DR, et al. Prevalence and predictors of BRCA1 and BRCA2 mutations in a population-based study of breast cancer in white and black American women ages 35 to 64 years. Cancer Res. 2006;66(16):8297–8308. doi:10.1158/0008-5472.CAN-06-0503
12. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: breast Cancer (Version 4.2025). 2025. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419.
13. Churpek J, Marquez R, Neistadt B, et al. Inherited mutations in cancer susceptibility genes are common among breast cancer survivors who develop therapy-related leukemia. Cancer. 2016;122(2):304–311. doi:10.1002/cncr.29615
14. Wolff AC, Blackford AL, Visvanathan K, et al. Risk of Marrow Neoplasms After Adjuvant Breast Cancer Therapy: the National Comprehensive Cancer Network Experience. J Clin Oncol. 2015;33(4):340–348. doi:10.1200/JCO.2013.54.6119
15. Allen I, Hassan H, Joko-Fru WY, et al. Risks of second primary cancers among 584,965 female and male breast cancer survivors in England: a 25-year retrospective cohort study. Lancet Regional Health. 2024;40:100903. doi:10.1016/j.lanepe.2024.100903
16. Joshi RM, Telang B, Soni G, Khalife A. Overview of perspectives on cancer, newer therapies, and future directions. Oncol Transl Med. 2024;10(3):105–109.
17. NCI. Cancer Genetics Risk Assessment and Counseling (PDQ®). 2024. Available from: https://www.cancer.gov/publications/pdq/information-summaries/genetics/risk-assessment-hp-pdq.
18. Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA. 2017;317(23):2402–2416. doi:10.1001/jama.2017.7112
19. Schulz E, Valentin A, Ulz P, et al. Germline mutations in the DNA damage response genes BRCA1, BRCA2, BARD1 and TP53 in patients with therapy related myeloid neoplasms. J Med Genet. 2012;49(7):422–428. doi:10.1136/jmedgenet-2011-100674
20. Gonzalez T, Nie Q, Chaudhary LN, et al. Methylation signatures as biomarkers for non-invasive early detection of breast cancer: a systematic review of the literature. Cancer Genet. 2024;282–283:1–8. doi:10.1016/j.cancergen.2023.12.003
21. Petrone G, Gaulin C, Derkach A, et al. Routine clinical parameters and laboratory testing predict therapy-related myeloid neoplasms after treatment for breast cancer. Haematologica. 2022;108(1):161–170. doi:10.3324/haematol.2021.280437
22. Wei JL, Jiang YZ, Shao ZM. Survival and chemotherapy-related risk of second primary malignancy in breast cancer patients: a SEER-based study. Int J Clin Oncol. 2019;24(8):934–940. doi:10.1007/s10147-019-01430-0
23. Lancet JE, Uy GL, Newell LF, et al. CPX-351 versus 7+3 cytarabine and daunorubicin chemotherapy in older adults with newly diagnosed high-risk or secondary acute myeloid leukaemia: 5-year results of a randomised, open-label, multicentre, Phase 3 trial. Lancet Haematol. 2021;8(7):e481–91. doi:10.1016/S2352-3026(21)00134-4
24. Uy GL, Newell LF, Lin TL, et al. Transplant outcomes after CPX-351 vs 7 + 3 in older adults with newly diagnosed high-risk and/or secondary AML. Blood Adv. 2022;6(17):4989–4993. doi:10.1182/bloodadvances.2021006468
25. Lu J, Xue SL, Wang Y, et al. Venetoclax and decitabine vs intensive chemotherapy as induction for young patients with newly diagnosed AML. Blood. 2025;145(22):2645–2655. doi:10.1182/blood.2024027217
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.