Back to Journals » Patient Preference and Adherence » Volume 17
“Challenges to Normalcy”- Perceived Barriers to Adherence to Home-Based Cardiac Rehabilitation Exercise in Patients with Chronic Heart Failure
Authors Yang Z ![]() , Zheng X
, Zheng X ![]() , Hu N
, Hu N ![]() , Zhang F, Wang A
, Zhang F, Wang A
Received 19 September 2023
Accepted for publication 18 December 2023
Published 21 December 2023 Volume 2023:17 Pages 3515—3524
DOI https://doi.org/10.2147/PPA.S440984
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zhen Yang, Xutong Zheng, Na Hu, Fengpei Zhang, Aiping Wang
Department of Public Services, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning Province, People’s Republic of China
Correspondence: Aiping Wang, Department of Public Services, The First Affiliated Hospital of China Medical University, No. 155, Nanjing North Street, Heping District, Shenyang, Liaoning Province, People’s Republic of China, Email [email protected]
Purpose: The aim of this study was to explore perceived barriers to adherence to home-based cardiac rehabilitation exercise in patients with chronic heart failure.
Patients and Methods: A qualitative descriptive study was conducted in this study from May to July 2023. A purposive sampling approach was adopted to select patients with chronic heart failure. Semi-structured interviews were completed to collect qualitative data for exploring the perceived barriers. In addition, information saturation and validation strategies were adopted to prove the adequacy of qualitative data. Transcripts were analysed using thematic analysis.
Results: A total of 16 patients with chronic heart failure were included in this study. Analysis of the data revealed five main barriers to adherence to home-based cardiac rehabilitation in patients with chronic heart failure. These include (1) lack of knowledge, (2) activity intolerance, (3) exercise fear, (4) role conflict, and (5) lower exercise self-efficacy.
Conclusion: This study delved deeper into understanding the challenges faced by chronic heart failure patients in adhering to home-based cardiac rehabilitation exercise. The development of precise and effective management and intervention strategies based on these barriers is necessary to improve patient compliance with home-based cardiac rehabilitation exercise.
Keywords: cardiac rehabilitation, exercise, influencing factors, qualitative research, thematic analysis
Introduction
Chronic heart failure, the terminal stage of various cardiovascular diseases, is characterized by high rates of hospitalization and mortality, imposing a significant burden on patients.1 Despite some advancements in the prevention and treatment of this condition, its clinical outlook and associated disease burden remain grave.2 As such, there is an utmost need for effective interventions that can enhance clinical prognosis, improve quality of life, mitigate disease recurrence, and reduce mortality among patients from chronic heart failure.
Cardiac rehabilitation refers to the integration of all methods to ensure that patients with chronic heart disease achieve optimal physical, mental, and social function, so that patients can regain normal function as much as possible in society through their own efforts and lead an active life.3 As recommended by the highest level of evidence in the relevant guidelines, cardiac rehabilitation is an effective measure to strengthen the standardized management of patients with chronic heart failure, which can significantly improve clinical outcomes and quality of life.4,5 As the core of cardiac rehabilitation, exercise plays an irreplaceable role in improving the cardiorespiratory performance of patients with chronic heart failure.6 However, due to the chronic nature of the disease and transportation limitations, exercise-based institutional cardiac rehabilitation places a heavy financial burden and time cost on patients.7,8 As an alternative model, exercise-based home cardiac rehabilitation offers a more cost-effective alternative to ameliorate this situation.9,10 Compared with institutional cardiac rehabilitation exercise, home-based cardiac rehabilitation exercise has the same effect on reducing cardiovascular risk, promoting psychological and spiritual health, enhancing cardiac function and prognosis, and improving quality of life in patients with chronic heart failure.11,12 In addition, home-based cardiac rehabilitation exercise provides professionals with systematic and appropriate medical care for patients with chronic heart failure outside of medical institutions (eg community, home, workplace, etc.).13 Also, home-based cardiac rehabilitation can help patients with chronic heart failure to overcome travel difficulties, flexible choice of rehabilitation locations, can increase the freedom of patient education, consultation time choice, and reduce the medical cost of patients with chronic heart failure has a positive significance.11,14,15 Importantly, mobile health (mhealth)-based home cardiac rehabilitation programs offer a viable solution to overcome numerous barriers, significantly enhancing telehealth options for individuals in rural areas.16,17 Especially during a pandemic, these mhealth interventions are appropriate and effective alternative strategies for cardiac rehabilitation, ensuring continuity of care in situations where traditional in-person sessions are not feasible.18,19
Despite their numerous benefits, the efficacy of home-based cardiac rehabilitation programs ultimately relies on long-term adherence by patients with chronic heart failure’ . Regrettably, viewed globally, the proportion of chronic heart failure patients adhering to home-based cardiac rehabilitation remains suboptimal.20–22 It was reported that less than 50% of patients attend exercise-based home cardiac rehabilitation after completing the institutional cardiac rehabilitation.23 In addition, between 40% to 91% of patients expressed reluctance towards home-based cardiac rehabilitation due to limited exercise endurance.13,24 Even with rigorous interventions, long-term adherence to home cardiac rehabilitation exercises stays relatively low at 34%.25 Moreover, research revealed a close relationship exercise adherence in cardiac rehabilitation and lower hospitalization rates and higher quality of life.11 Chronic heart failure patients who actively followed exercise-based cardiac rehabilitation reported a 34% reduction in readmissions compared to non-adherents, as well as significant improvements in exercise endurance, heart function, and quality of life.26,27 Therefore, regarding the importance and necessity of adherence to home-based cardiac rehabilitation exercise, a range of barriers to adherence to home-based cardiac rehabilitation exercise are required to be confirmed to explore precise intervention targets, so as to improve home-based cardiac rehabilitation exercise adherence for patients.
Qualitative research offers comprehensive insights into the barriers affecting adherence to home-based cardiac rehabilitation exercises by providing an individual perspective in real-life environments. Therefore, this study, as part of a larger project, aims to explore the obstacle factors affecting the adherence of patients with chronic heart failure in home-based cardiac rehabilitation exercise, hoping to provide precise intervention targets for the design of intervention programs, and thereby improve adherence to home-based cardiac rehabilitation in patients with chronic heart failure.
Methods
Study Design and Participants
A qualitative descriptive study was conducted from May to July 2023 with a focus on identifying barriers to adherence to home-based cardiac rehabilitation exercise for chronic heart failure patients. In this study, participants were selected using purposive sampling with maximum variation strategies at a large cardiac rehabilitation centre in Liaoning Province, China. The centre followed international guidelines for cardiac rehabilitation procedures and management. The inclusion criteria for participants included (1) patients with chronic heart failure who were 18 years of age or older, (2) currently participating in home cardiac rehabilitation (Phase III cardiac rehabilitation), and (3) who had voluntarily given informed consent to participate in the study. The exclusion criteria for participants included patients who had previously been diagnosed with cognitive impairment or a serious organic disease that would have prevented collaboration with the interviewer. The sample size was guided by the principle of data saturation - The interview stopped when no new information emerged after three consecutive interviews.28
Instruments
General Demographic Characteristics Questionnaire
Based on a literature review and group discussion, the general sociodemographic questionnaire was developed to collect relevant sociodemographic information about the participants. The questionnaire covered age, gender, education, marital status, duration of disease (years), location, and self-reported health status.
Research Team
Researchers are regarded as key research tools in this study. The research team consists of a professor with extensive experience in qualitative research (responsible for research design and quality control) and four doctoral students with qualitative training (responsible for collecting and analyzing qualitative data, negotiating and determining coding themes).
Interview Outline
Interview outlines were developed based on the adequate literature review and research purposes. The interview outline includes the following main questions: (a) What do you think of home-based cardiac rehabilitation exercise? (b) How do you feel or experience participating in the home-based cardiac rehabilitation exercise? (c) What factors do you think would influence your participation in home-based cardiac rehabilitation exercise? (d) How specifically did the above obstacles cause you to give up or avoid doing home cardiac rehabilitation exercises? (e) Is there anything you would like to add about the barriers to home cardiac rehabilitation exercise?
Data Collection
The researchers fostered positive relationships with the study participants, serving in roles as health educators and counselors. Participant preferences determined the selection of a quiet and comfortable location for the study. Two researchers conducted semi-structured face-to-face interviews with participants. A recording license was approved by the participant to accurately capture the relevant information. After informing the purpose and significance of the study, an informed consent form was signed. This was subsequently followed by the formal semi-structured interview. A formal semi-structured interview was conducted. After the interview, a reflection diary was filled out to record the most vivid and emotional thoughts.
Data Analysis
Two researchers transcribed the audio recordings into text within a 24-hour timeframe. The thematic analysis approach was adopted to extract meaningful themes in this study.29 First, the two researchers familiarize themselves with textual data to conduct preliminary coding. A unique set of codes were then constructed to identify meaningful sentences. The code was examined and integrated by the two researchers, and new themes were extracted. These extracted themes were reviewed meticulously before finalizing their potential implications. Each theme was subsequently defined and labeled to best represent its essence. The final step involved incorporating these findings into a cohesive analytical narrative to form the report. In this procedure, none of the participants were involved in the analysis process, but the themes identified by the researchers were checked by the participants to ensure that they captured the participants’ experiences. In addition, three specialists with a profound understanding of qualitative analysis examined and approved the extracted themes and textual data, thereby validating the findings’ adequacy. NVivo 12.0 software was adopted in this study.
Rigour
This study strictly followed qualitative reporting guidelines. A triangulated data analysis procedure was conducted to enhance the reliability of the study. To establish the transferability of the study, we developed a robust description of participants’ perceived barriers to adherence to home-based cardiac rehabilitation exercises. In relation to the audit trail, the research team thoroughly documented and elucidated the various actions executed during the research, including the data collection and analytical processes, thereby fostering transparency and consistency throughout the study. The ample sample size and data saturation secured thorough exploration of perceived barriers to home-based cardiac rehabilitation exercise adherence. Interviews were conducted in a fashion to minimize the possibility of participants providing socially desirable responses.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki. After being informed of the purpose, significance, and voluntary nature of the study, participants signed informed consent forms. The participants informed consent included publication of anonymized responses. This study protocol was approved by the First Affiliated Hospital of China Medical University on January 27, 2023 (No. 2023. 66).
Results
Sociodemographic Data of the Participants
A total of 16 patients with chronic heart failure were included in the study. There were 7 male and 9 female. They are between 42 and 84 years old. Educational background is evenly distributed. As for marital status, there are 3 unmarried, 7 married and 6 divorced/widowed. The course of the disease ranges from 2 to 12 years. As for home addresses, there are 8 rural and 8 urban. In addition, 5 reported poor, 6 moderate, and 5 good (Table 1).
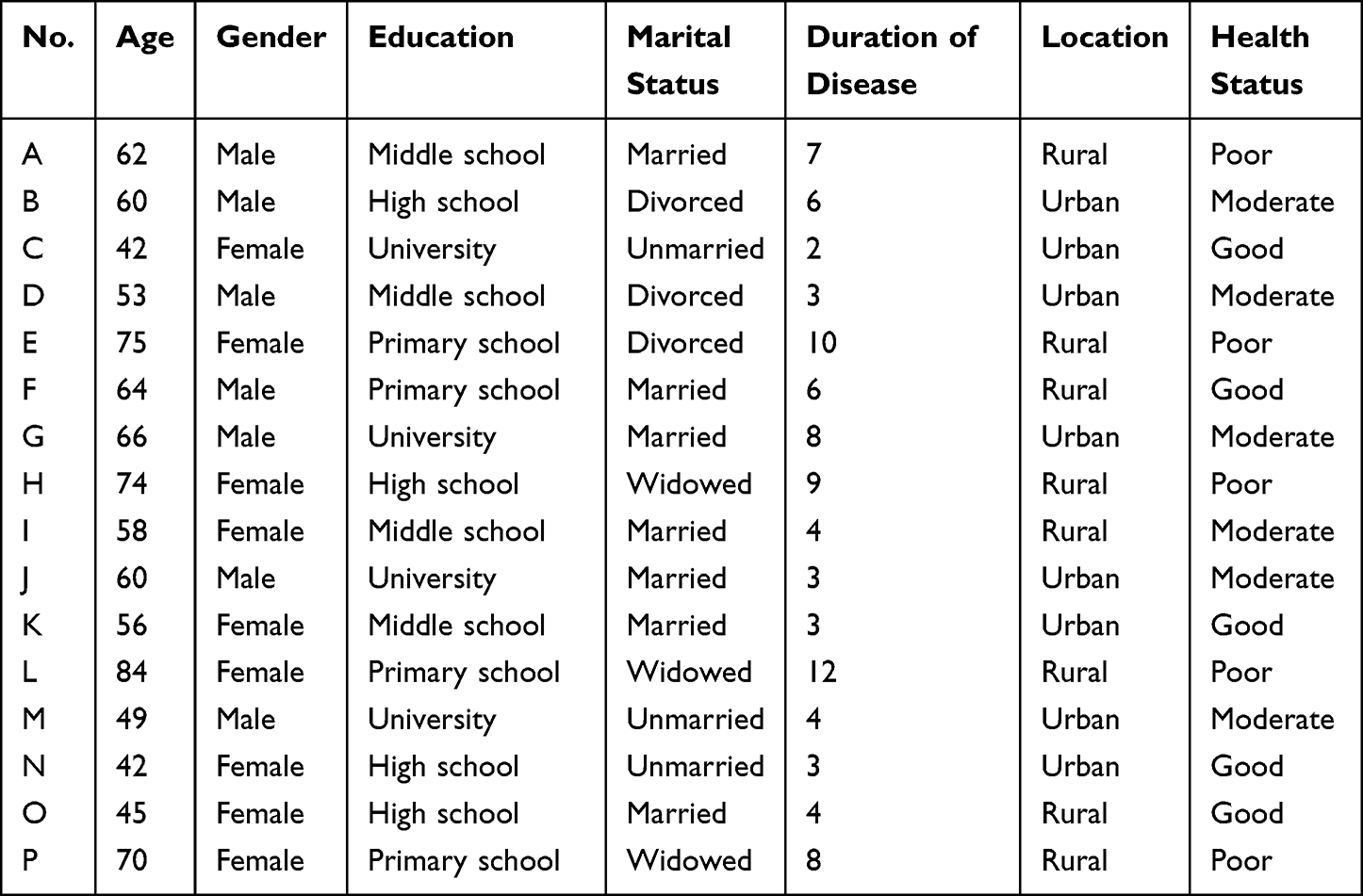 |
Table 1 General Demographic Characteristics of the Participants |
Barriers to Exercise Adherence of the Participants
In this study, a total of 5 themes were generated, covering lack of knowledge, activity intolerance, exercise fear, role conflict, and lower exercise self-efficacy (Table 2).
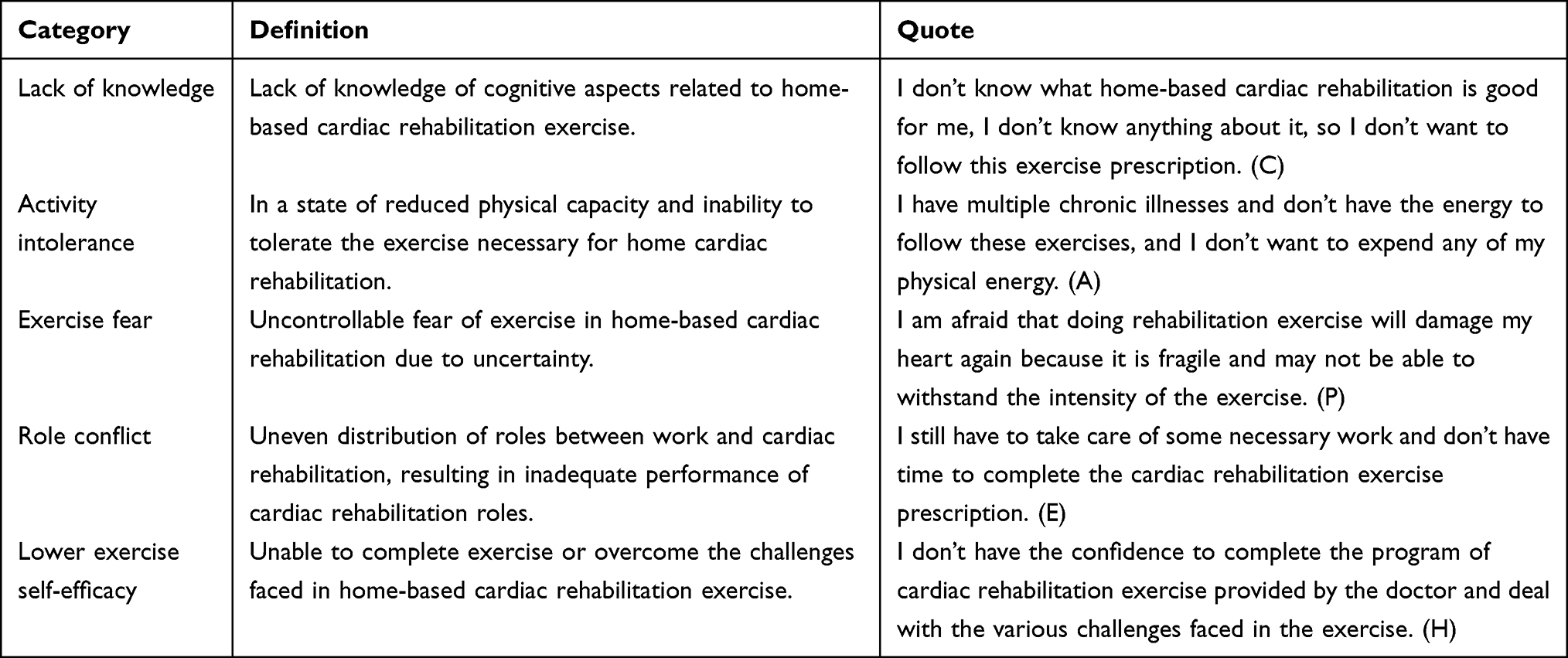 |
Table 2 Categories, Definitions and Exemplar Quotes |
Lack of Knowledge
The importance and necessity of cardiac rehabilitation in patients with chronic heart failure are underestimated due to the lack of knowledge about home-based cardiac rehabilitation. They are not clear about the purpose and significance of such exercises and do not fully recognize their personal needs this regard. Consequently, they display low adherence to home-based cardiac rehabilitation exercise programs recommended by medical professionals.
Interviewee C:I do not know the relevant knowledge of home cardiac rehabilitation, and I am not sure whether it is necessary to exercise in home cardiac rehabilitation.
Interviewee F:Because of the uncertainty about its efficacy, I did not start a home cardiac rehabilitation exercise.
Interviewee M:I do not understand the benefits of home cardiac rehabilitation exercise and I may not need to do it at home.
Activity Intolerance
With the increase of age and the emergence of other chronic diseases, it is more difficult for patients to adhere to home-based cardiac rehabilitation exercises, mainly reflected in the lack of activity endurance. They reported that the prolonged nature of the disease leads to reduced activity endurance, and exercise may further cause physical exertion. To avoid discomfort symptoms prompted by this exertion, many patients typically opt out of following home cardiac rehabilitation exercise programs.
Interviewee G:I have a lot of diseases, I simply do not have the strength to complete the home cardiac rehabilitation exercise prescription, I feel very tired.
Interviewee J:The home cardiac rehabilitation exercise greatly consumes my physical strength, and my endurance is not enough to support it.
Interviewee K:I have been sick for six years and have low activity endurance, so I am reluctant to follow the home cardiac rehabilitation exercise prescription.
Exercise Fear
In this study, patients with chronic heart failure are afraid of home-based cardiac rehabilitation exercises, mainly concerned about cardiovascular risks and possible unknown events. Although medical professionals are clearly informed of the benefits of exercise, they are still concerned about the potential for secondary cardiovascular injuries and remain conservative in their willingness to subscribe to such exercises.
Interviewee D:I am afraid to do cardiac rehabilitation at home because I am afraid it will damage my heart.
Interviewee P:Although cardiac rehabilitation professionals describe its benefits, I am still afraid of exercise, which may greatly increase the occurrence of adverse cardiovascular events.
Interviewee A:The key factor in my reluctance to follow home cardiac rehabilitation is my fear of exercise.
Role Conflict
Many chronic heart failure patients who are not yet retired must continue fulfilling their respective job roles. This often leads to a conflict between their responsibilities at work and their personal need for cardiac rehabilitation. Consequently, struggling to find enough time for at-home cardiac rehabilitation becomes a common issue among these patients. They claim that due to their commitment to their work, find it challenging to dedicate ample time for their cardiac rehabilitation at home. This results in lower adherence rates to their home cardiac rehabilitation regimens.
Interviewee B:I still need to finish some of my trivial work and have no time to follow the prescription of home cardiac rehabilitation exercise issued by the doctor.
Interviewee H:It is difficult for me to take full time to complete the agreed exercise prescription, because I have some other things.
Interviewee N:I need to finish my work before I consider completing a prescription for home cardiac rehabilitation exercise. I seldom go to exercise.
Lower Exercise Self-Efficacy
The low exercise self-efficacy of patients with chronic heart failure is an important factor in their non-adherence to home cardiac rehabilitation exercise. They reported a lack of confidence to overcome the challenges of home-based cardiac rehabilitation exercises or felt unable to complete them. Lower exercise self-efficacy reduced their confidence in completing home-based cardiac rehabilitation exercises, thereby affecting their adherence to these exercises.
Interviewee I:I am not confident in home cardiac rehabilitation and I may not be able to cope with the challenges I face in home cardiac rehabilitation.
Interviewee E:I would not like to follow the home cardiac rehabilitation exercise, it is too difficult for me, I may not be able to complete it.
Interviewee O:I have difficulty completing cardiac rehabilitation at home and I have no confidence in doing it at all.
Discussion
In this study, we examined the perceived barriers to adherence to home-based cardiac rehabilitation exercises among patients with chronic heart failure. These mainly include a lack of knowledge, activity intolerance, exercise fear, role conflict, and lower exercise self-efficacy. Despite the obvious benefits of exercise-based home cardiac rehabilitation, the proportion of patients who adhere to this form remains insufficient. This study acknowledges the diverse nature of individuals, hence, we explored the hindrance factors affecting this low adherence from the patients’ point of view. The findings provide references for precise management and control strategies taking into account these hindrance factors that can be addressed.
This study found that lack of knowledge is an obstacle for patients with chronic heart failure to comply with home cardiac rehabilitation exercise, consistent with the results obtained by Ghisi et al in the female population.19 Patients with chronic heart failure who lack relevant knowledge have a vague understanding of the benefits of home-based cardiac rehabilitation exercises, which may greatly undermine their motivation to adhere to such exercises.30,31 In addition, based on the knowledge-belief-behavior theory, knowledge is the basis of individual behavior, and belief is the driving force of individual behavior.32 Lacking of relevant knowledge may weaken the belief of patients with chronic heart failure in home-based cardiac rehabilitation exercise, and then lead to a decrease in their self-perceived needs and reluctance to comply with home cardiac rehabilitation exercise.33,34 Therefore, cardiac rehabilitation professionals should fully carry out distance education based on mobile health technology to significantly improve the home-based cardiac rehabilitation exercise adherence of chronic heart failure patients.
In this study, exercise fear was explored as a key factor in non-adherence to home-based cardiac rehabilitation in patients with chronic heart failure, consistent with the results of Keessen et al.35 Because of the uncertainty about cardiovascular risks and adverse events, patients with chronic heart failure are afraid of home-based cardiac rehabilitation exercise and are reluctant to perform home-based cardiac rehabilitation.35 Quantitative studies have also shown that chronic heart failure patients in home cardiac rehabilitation have poorer levels of physical activity.12,36 In this population, the benefits of home-based cardiac rehabilitation exercise are well known. However, the fear and concern that physical activity may cause secondary cardiovascular damage may far outweigh the findings of their benefits, leading to a reluctance to comply with home-based cardiac rehabilitation exercise.37,38 Therefore, professional guidance from professionals and psychological support from families are very necessary to reduce the fear of exercise in patients with chronic heart failure and improve exercise adherence.
The interview results showed that activity intolerance is an obstacle for patients with chronic heart failure to comply with home-based cardiac rehabilitation exercises, and relevant quantitative studies have also confirmed this view.39,40 Chronic heart failure is a kind of heart dysfunction disease, patients often have symptoms of reduced activity tolerance in daily life.41 Cardiac rehabilitation exercise is a treatment to improve heart function and increase activity endurance by gradually increasing physical activity. If patients lack activity tolerance, they may not be able to carry out a cardiac rehabilitation exercise program due to physical exhaustion.37 In addition, patients with chronic heart failure expressed resistance to some conventional rehabilitation exercises because some exercises exceeded their activity tolerance. For them, engaging in externally forced exercise may actually worsen their symptoms and anxiety.37 Therefore, the patients with chronic heart failure should follow the exercise prescription gradually according to their own preferences to improve the prognosis of the disease during the period of home cardiac rehabilitation. Also, cardiac rehabilitation professionals should develop appropriate and personalized home-based cardiac rehabilitation exercise prescriptions based on a comprehensive assessment of the patient.
The interview results of this study revealed that time-based role conflict is a barrier affecting the adherence to home-based cardiac rehabilitation exercise of patients with chronic heart failure. Specifically, this conflict refers to the uneven distribution of patients’ roles between work and cardiac rehabilitation, resulting in inadequate performance of cardiac rehabilitation roles.42 Young and middle-aged people with chronic heart failure have multiple roles in their families and society, so returning to work quickly can have a significant impact on themselves and their families.43,44 Related research suggests that a majority of patients expect to be able to return to work, which may cause additional time conflicts that reduce their ability to follow home-based cardiac rehabilitation exercise prescriptions.45,46 To address this issue, consider effectively managing time and role conflict by changing the way exercise is prescribed or adjusting work hours. It is important to understand that the home cardiac rehabilitation exercise program should maintain some flexibility so that appropriate adjustments can be made according to the individual situation of the patient.
The results of this study suggested that low exercise self-efficacy is a key barrier to non-adherence to home-based cardiac rehabilitation exercise in patients with chronic heart failure. This result has also been confirmed in related quantitative studies.17,19,47–49 Patients with low exercise self-efficacy may be reluctant to participate in the formulation of cardiac rehabilitation exercise prescriptions, and may not be willing to expend energy to develop cardiac rehabilitation exercise skills and address the challenges of exercise.49,50 Therefore, improving exercise self-efficacy in patients with chronic heart failure may be a key component in overcoming barriers to exercise adherence in home-based cardiac rehabilitation. In addition, patients with low exercise self-efficacy may lack understanding of the impact of exercise, be reluctant to seek relevant support and feedback information, and may have doubts about the effect of exercise, so they are naturally reluctant to actively participate.47,51 Therefore, in addition to the professional knowledge and careful guidance of medical staff, the active participation of patients themselves, the support of family members, and the understanding and acceptance of the public are all critical to the successful improvement of patients’ exercise self-efficacy.
In future research and practice, mhealth-based home-based cardiac rehabilitation procedures will be the mainstream. Its effectiveness has been well documented in terms of reducing cardiovascular risk, improving clinical outcomes and quality of life.12 Also, related studies have found that the risk of adverse events during home-based cardiac rehabilitation with mhealth appears to be low.52 The findings on the safety of home-based cardiac rehabilitation should lead heart patients to be more active in their environment and to engage in regular physical activity.
Limitations
The themes described in this study lacks empirical evidence and needs to be continuously revised and improved through quantitative design in future studies. Theoretical saturation is a relative concept, and with further interviews, the density and dimension of this category of interpretative understanding may be enriched. Although the data has reached saturation, transferability is limited due to the small sample size and the fact that younger participants are not included. In future studies, young patients with chronic heart failure with disease classification and prognostic indicators should be included to complement the outcome study of this study.
Implications for Research, Policy and Practice
In the context of clinical practice, spotting and comprehending perceived barriers faced by patients suffering from chronic heart failure becomes of crucial importance for fostering patients’ adherence to home-based cardiac rehabilitation exercise routines. These barriers can come in various forms, including a lack of knowledge about the exercise regimen, intolerance to physical activities, fear of exercising due in part to the misconceptions surrounding the effects of exercise on their condition, conflict with their regular roles or duties, and a lack of confidence about their own ability to carry out the recommended exercises (lower exercise self-efficacy).
Recognizing these hurdles allows healthcare practitioners to develop tailored clinical interventions with a targeted approach to surmount these challenges faced by the patients. Such clinical interventions could focus on patient education, aiming to boost the patients’ knowledge and understanding about execution of cardiac rehabilitation exercises; psychological support to curb any fear or anxiety related to exercise and its effects on their condition; or creating personalized rehabilitation routines that take into consideration the patients’ physical capacity, lifestyle, and daily roles or responsibilities.
These are expected to dramatically enhance patient compliance, thus facilitating such patients to take full advantage of the established benefits associated with home-based rehabilitation exercises. With better compliance to such exercises, they should experience an improvement in their cardiovascular health, symptom management, and overall quality of life. The insights gained from understanding these barriers are of immense clinical relevance. They may hold the potential to transform the management of chronic heart disease, to patient outcomes. Such valuable understanding puts healthcare practitioners in a stronger position to devise strategies that would greatly improve patient engagement, exercise adherence, and subsequently, their health.
Conclusion
This study delved deeper into understanding the challenges faced by chronic heart failure patients in adhering to home-based cardiac rehabilitation exercises. These challenges were explored from an individual perspective in a realistic home-setting and encompassed numerous factors including lack of knowledge, activity intolerance, exercise fear, role conflict, and lower exercise self-efficacy. Identifying these barriers could pave way for targeted interventions aimed at enhancing adherence to home-based cardiac rehabilitation among patients with chronic heart failure.
Data Sharing Statement
Research data will be shared with reasonable requests.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki. After being informed of the purpose, significance, and voluntary nature of the study, participants signed informed consent forms. The participants informed consent included publication of anonymized responses. This study protocol was approved by the First Affiliated Hospital of China Medical University on January 27, 2023 (No. 2023. 66).
Acknowledgments
The authors are grateful to patients with chronic heart failure who participated in this study, and also to the nursing directors for their strong support during the interview process.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Crea F. Epidemiology and treatment of acute and chronic heart failure. Eur Heart J. 2023;44(5):329–332. doi:10.1093/eurheartj/ehad022
2. Slavin SD, Khera R, Zafar SY, Nasir K, Warraich HJ. Financial burden, distress, and toxicity in cardiovascular disease. Am Heart J. 2021;238:75–84. doi:10.1016/j.ahj.2021.04.011
3. Josephson RA. Cardiac rehabilitation 2022. Prog Cardiovasc Dis. 2022;70:1. doi:10.1016/j.pcad.2022.01.010
4. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e876–e894. doi:10.1161/CIR.0000000000001062
5. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
6. Patti A, Merlo L, Ambrosetti M, Sarto P. Exercise-based cardiac rehabilitation programs in heart failure patients. Heart Fail Clin. 2021;17(2):263–271. doi:10.1016/j.hfc.2021.01.007
7. Bourke A, Niranjan V, O’Connor R, Woods C. Barriers to and motives for engagement in an exercise-based cardiac rehabilitation program in Ireland: a qualitative study. BMC Prim Care. 2022;23(1):28. doi:10.1186/s12875-022-01637-7
8. Moghei M, Turk-Adawi K, Isaranuwatchai W, et al. Cardiac rehabilitation costs. Int J Cardiol. 2017;244:322–328. doi:10.1016/j.ijcard.2017.06.030
9. Batalik L, Filakova K, Sladeckova M, Dosbaba F, Su J, Pepera G. The cost-effectiveness of exercise-based cardiac telerehabilitation intervention: a systematic review. Eur J Phys Rehabil Med. 2023;59(2):248–258. doi:10.23736/S1973-9087.23.07773-0
10. Clark RA, Conway A, Poulsen V, Keech W, Tirimacco R, Tideman P. Alternative models of cardiac rehabilitation: a systematic review. Eur J Prev Cardiol. 2015;22(1):35–74. doi:10.1177/2047487313501093
11. Chen YW, Wang CY, Lai YH, et al. Home-based cardiac rehabilitation improves quality of life, aerobic capacity, and readmission rates in patients with chronic heart failure. Medicine (Baltimore). 2018;97(4):e9629. doi:10.1097/MD.0000000000009629
12. Antoniou V, Davos CH, Kapreli E, Batalik L, Panagiotakos DB, Pepera G. Effectiveness of home-based cardiac rehabilitation, using wearable sensors, as a multicomponent, cutting-edge intervention: a systematic review and meta-analysis. J Clin Med. 2022;11(13):3772. doi:10.3390/jcm11133772
13. Kulnik ST, Sareban M, Höppchen I, et al. Outpatient cardiac rehabilitation closure and home-based exercise training during the first COVID-19 lockdown in Austria: a mixed-methods study. Front Psychol. 2022;13:817912. doi:10.3389/fpsyg.2022.817912
14. Shields GE, Rowlandson A, Dalal G, et al. Cost-effectiveness of home-based cardiac rehabilitation: a systematic review. Heart. 2023;109(12):913–920. doi:10.1136/heartjnl-2021-320459
15. Yang Z, Sun L, Sun Y, Dong Y, Wang A. A conceptual model of home-based cardiac rehabilitation exercise adherence in patients with chronic heart failure: a constructivist grounded theory study. Patient Prefer Adherence. 2023;17:851–860. doi:10.2147/PPA.S404287
16. Nagatomi Y, Ide T, Higuchi T, et al. Home-based cardiac rehabilitation using information and communication technology for heart failure patients with frailty. ESC Heart Fail. 2022;9(4):2407–2418. doi:10.1002/ehf2.13934
17. Antoniou V, Pasias K, Loukidis N, et al. Translation, cross-cultural adaptation and psychometric validation of the Greek version of the Cardiac Rehabilitation Barriers Scale (CRBS-GR): what are the barriers in South-East Europe? Int J Environ Res Public Health. 2023;20(5):4064. doi:10.3390/ijerph20054064
18. Thomas RJ, Beatty AL, Beckie TM, et al. Home-based cardiac rehabilitation: a scientific statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation. 2019;140(1):e69–e89. doi:10.1161/CIR.0000000000000663
19. Ghisi GLM, Kim WS, Cha S, et al. Women’s cardiac rehabilitation barriers: results of the international council of cardiovascular prevention and rehabilitation’s first global assessment. Can J Cardiol. 2023;39:S0828-282X(23)01552–0. doi:10.1016/j.cjca.2023.07.016
20. Ruano-Ravina A, Pena-Gil C, Abu-Assi E, et al. Participation and adherence to cardiac rehabilitation programs. A systematic review. Int J Cardiol. 2016;223:436–443. doi:10.1016/j.ijcard.2016.08.120
21. Nielsen J, Duncan K, Pozehl B. Patient-selected strategies for post cardiac rehabilitation exercise adherence in heart failure. Rehabil Nurs. 2019;44(3):181–185. doi:10.1097/rnj.0000000000000127
22. Ge C, Ma J, Xu Y, et al. Predictors of adherence to home-based cardiac rehabilitation program among coronary artery disease outpatients in China. J Geriatr Cardiol. 2019;16(10):749–755. doi:10.11909/j.issn.1671-5411.2019.10.003
23. Schopfer DW, Nicosia FM, Ottoboni L, Whooley MA. Patient perspectives on declining to participate in home-based cardiac rehabilitation: a mixed-methods study. J Cardiopulm Rehabil Prev. 2020;40(5):335–340. doi:10.1097/HCR.0000000000000493
24. Krishnamurthi N, Schopfer DW, Ahi T, et al. Predictors of patient participation and completion of home-based cardiac rehabilitation in the veterans health administration for patients with coronary heart disease. Am J Cardiol. 2019;123(1):19–24. doi:10.1016/j.amjcard.2018.09.024
25. Whellan DJ, O’Connor CM, Lee KL, et al. HF-ACTION Trial Investigators. Heart failure and a controlled trial investigating outcomes of exercise training (HF-ACTION): design and rationale. Am Heart J. 2007;153(2):201–211. doi:10.1016/j.ahj.2006.11.007
26. Long L, Mordi IR, Bridges C, et al. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst Rev. 2019;1(1):CD003331. doi:10.1002/14651858.CD003331.pub5
27. Fukuta H, Goto T, Wakami K, Kamiya T, Ohte N. Effects of exercise training on cardiac function, exercise capacity, and quality of life in heart failure with preserved ejection fraction: a meta-analysis of randomized controlled trials. Heart Fail Rev. 2019;24(4):535–547. doi:10.1007/s10741-019-09774-5
28. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
29. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
30. Siegmund LA, Ahmed HM, Crawford MT, Bena JF. Feasibility of a Facebook intervention for exercise motivation and cardiac rehabilitation adherence: study protocol. JMIR Res Protoc. 2017;6(8):e162. doi:10.2196/resprot.7554
31. Jasmine TJ, Wai-Chi SC, Hegney DG. The impact of knowledge and beliefs on adherence to cardiac rehabilitation programs in patients with heart failure: a systematic review. JBI Libr Syst Rev. 2012;10(7):399–470. doi:10.11124/jbisrir-2012-53
32. Teo CJH, Burns SF, Kawabata M. Developing nutrition knowledge and attitude measures for athletes with the knowledge-attitude-behavior model. Res Q Exerc Sport. 2023;94(1):110–117. doi:10.1080/02701367.2021.1942771
33. Vanzella LM, Oh P, Pakosh M, Ghisi GLM. Barriers and facilitators to virtual education in cardiac rehabilitation: a systematic review of qualitative studies. Eur J Cardiovasc Nurs. 2022;21(5):414–429. doi:10.1093/eurjcn/zvab114
34. Frohmader TJ, Lin F, Chaboyer W. Patient perceptions of nurse mentors facilitating the Aussie Heart Guide: a home-based cardiac rehabilitation programme for rural patients. Nurs Open. 2015;3(1):41–50. doi:10.1002/nop2.34
35. Keessen P, den Uijl I, Visser B, et al. Fear of movement in patients attending cardiac rehabilitation: a validation study. J Rehabil Med. 2020;52(2):jrm00021. doi:10.2340/16501977-2749
36. Ter Hoeve N, Keessen P, Den Uijl I, et al. Assessing changes in fear of movement in patients attending cardiac rehabilitation: responsiveness of the TSK-NL heart questionnaire. J Rehabil Med. 2022;54:jrm00328. doi:10.2340/jrm.v54.2519
37. Dibben GO, Dalal HM, Taylor RS, et al. Cardiac rehabilitation and physical activity: systematic review and meta-analysis. Heart. 2018;104(17):1394–1402. doi:10.1136/heartjnl-2017-312832
38. Bermudez T, Bolger N, Bierbauer W, et al. Physical activity after cardiac rehabilitation: explicit and implicit attitudinal components and ambivalence. Health Psychol. 2021;40(8):491–501. doi:10.1037/hea0001109
39. Li J, Yang P, Fu D, et al. Effects of home-based cardiac exercise rehabilitation with remote electrocardiogram monitoring in patients with chronic heart failure: a study protocol for a randomised controlled trial. BMJ Open. 2019;9(3):e023923. doi:10.1136/bmjopen-2018-023923
40. Shoemaker MJ, Dias KJ, Lefebvre KM, Heick JD, Collins SM. Physical therapist clinical practice guideline for the management of individuals with heart failure. Phys Ther. 2020;100(1):14–43. doi:10.1093/ptj/pzz127
41. Wheat HL, Fedson S, Bozkurt B, Josephson RA. Cardiac rehabilitation in heart failure: indications for exercise training based on heart failure phenotype. Prog Cardiovasc Dis. 2022;70:16–21. doi:10.1016/j.pcad.2021.10.003
42. Sumner J, Harrison A, Doherty P. The effectiveness of modern cardiac rehabilitation: a systematic review of recent observational studies in non-attenders versus attenders. PLoS One. 2017;12(5):e0177658. doi:10.1371/journal.pone.0177658
43. McHorney CA, Mansukhani SG, Anatchkova M, et al. The impact of heart failure on patients and caregivers: a qualitative study. PLoS One. 2021;16(3):e0248240. doi:10.1371/journal.pone.0248240
44. Emmons-Bell S, Johnson C, Roth G. Prevalence, incidence and survival of heart failure: a systematic review. Heart. 2022;108(17):1351–1360. doi:10.1136/heartjnl-2021-320131
45. Sagar VA, Davies EJ, Briscoe S, et al. Exercise-based rehabilitation for heart failure: systematic review and meta-analysis. Open Heart. 2015;2(1):e000163. doi:10.1136/openhrt-2014-000163
46. Hegewald J, Romero Starke K, Garthus-Niegel S, et al. Work-life conflict and cardiovascular health: 5-year follow-up of the Gutenberg health study. PLoS One. 2021;16(5):e0251260. doi:10.1371/journal.pone.0251260
47. Heidari M, Harandi PN, Moghaddasi J, Kheiri S, Azhari A. Effect of home-based cardiac rehabilitation program on self-efficacy of patients with implantable cardioverter defibrillator. Sage Open Nurs. 2023;9:23779608231166473. doi:10.1177/23779608231166473
48. Rodgers WM, Murray TC, Selzler AM, Norman P. Development and impact of exercise self-efficacy types during and after cardiac rehabilitation. Rehabil Psychol. 2013;58(2):178–184. doi:10.1037/a0032018
49. Howarter AD, Bennett KK, Barber CE, Gessner SN, Clark JM. Exercise self-efficacy and symptoms of depression after cardiac rehabilitation: predicting changes over time using a piecewise growth curve analysis. J Cardiovasc Nurs. 2014;29(2):168–177. doi:10.1097/JCN.0b013e318282c8d6
50. Candelaria D, Kirkness A, Bruntsch C, et al. Exercise self-efficacy improvements during cardiac rehabilitation: impact of social disparities. J Cardiopulm Rehabil Prev. 2023;43(3):179–185. doi:10.1097/HCR.0000000000000742
51. Shea MG, Farris SG, Hutchinson J, Headley S, Schilling P, Pack QR. Effects of exercise testing and cardiac rehabilitation in patients with coronary heart disease on fear and self-efficacy of exercise: a pilot study. Int J Behav Med. 2023. doi:10.1007/s12529-023-10207-9
52. Stefanakis M, Batalik L, Antoniou V, Pepera G. Safety of home-based cardiac rehabilitation: a systematic review. Heart Lung. 2022;55:117–126. doi:10.1016/j.hrtlng.2022.04.016
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
“I Still Suffer Every Second of Every Day”: A Qualitative Analysis of the Challenges of Living with Chronic Orofacial Pain
Lovette BC, Bannon SM, Spyropoulos DC, Vranceanu AM, Greenberg J
Journal of Pain Research 2022, 15:2139-2148
Published Date: 29 July 2022
Physical Restraint Experience of Patients with Mental Disorders in Mainland China: A Qualitative Study
Chong Y, Wang C, Min H, Zhang L, Zhi T, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2024, 17:431-444
Published Date: 31 January 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Exploring the Willingness of Young and Middle-Aged CHD Patients to Participate in Home-Based Cardiac Rehabilitation: A Qualitative Study
Liu T, Yang S, Rong S, Liu M, Wang X, Ji Y
Patient Preference and Adherence 2025, 19:1011-1027
Published Date: 11 April 2025
Factors Influencing Adherence to Dietary Interventions Among Patients with Gestational Diabetes Mellitus in China: A Qualitative Study Based on the COM-B Model
Jia CL, Wang LJ, Li LH, Lu YJ, Yang Y
Journal of Multidisciplinary Healthcare 2025, 18:4653-4663
Published Date: 5 August 2025