")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 14
Challenges of Medical Error Reporting in Mizan-Tepi University Teaching Hospital: A Qualitative Exploratory Study
Authors Derese M , Agegnehu W
Received 15 November 2021
Accepted for publication 20 April 2022
Published 26 April 2022 Volume 2022:14 Pages 51—59
DOI https://doi.org/10.2147/DHPS.S347738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajender R Aparasu
Msganaw Derese,1 Wubetu Agegnehu2
1Department of Nursing, College of Medicine and Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia; 2Department of Public Health, College of Medicine and Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia
Correspondence: Msganaw Derese, Department of Nursing, College of Medicine and Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia, Tel +251937935644, Email [email protected]
Background: Medical error is defined as “an act of omission or commission in planning or execution that contributes or could contribute to an unintended result”. It is a serious public health problem that can pose a threat to patient safety and if managed it can be an opportunity to an organizational learning. This study aimed to assess the challenges of error reporting.
Methods: Explorative qualitative cross-sectional study was conducted. The study was conducted among healthcare providers in Mizan-Tepi University Teaching Hospital. The study participants were selected purposely based on the patient contact hour and had served in this hospital for long period of time. Twenty-one in-depth interviews were undertaken. From each wards, three in-depth interviews were held. Case team leaders and other healthcare providers were identified and interviewed. The data were analyzed thematically.
Results: Twenty-one healthcare providers were recruited for this study. Majority of the participants, 12 (57.1%) were nurses and midwives and as to marital status, 18 (85.7%) were married. Challenges for reporting medical errors were identified as perceived lack of confidentiality of the medical errors, perceived punitive measures, lack of good reporting system, perceived fear of losing acceptance, lack of learning culture from errors, information asymmetry, mass-media publication of medical errors, avoidance of conflict and attitude of health professionals.
Conclusion: There were system and individual related challenges for reporting of medical errors. Healthcare managers should enhance medical error reporting for organizational learning by addressing these system and individual factors.
Keywords: medical error, reporting, organizational learning
Introduction
An error is defined as the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim. Errors can include problems in practice, products, procedures, and systems.1,2
Medical error is defined as “an act of omission or commission in planning or execution that contributes or could contribute to an unintended result”.3 It is a serious public health problem that can pose a threat to patient safety. Currently reducing medical errors has become an international concern.4
Morbidity and mortality conferences and autopsies, case analysis or root cause analysis, claims analysis, error reporting systems, administrative data analysis, record review or chart review, review of electronic medical record, observation of patient care, and active clinical surveillance are some of the methods for studying and measuring medical errors.2
Reporting errors is fundamental to error prevention. Studies showed that many errors go unreported by health care workers.5,6 Providers’ emotional responses to errors inhibit reporting. Self-reporting errors can be thwarted by several factors like fear of career-threatening disciplinary actions, a culture of blame and punishment do not report all errors. Fear of reprisal and punishment has led to a norm of silence. Healthcare workers need to have conversations about their concerns at work, including errors and dangerous behavior of coworkers.6
Several factors have contributed to the rise in medical errors, including the complexity of the health-care system, doctors’ reluctance to admit mistakes, a lack of leadership, and an insurance reimbursement system that rewards errors because hospitals can still bill for additional services when patients are injured but often will not pay for practices that reduce those errors.7
Globally medical errors are a common challenge in various fields of medicine, diagnostics, surgery, and care, leading to more deaths and imposing greater economic burden on health systems.8 It’s also a common occurrence that constitutes a significant public health issue that posing a serious threat to patient safety.
Medical error, after heart disease and cancer, is the third leading cause of death in the United States, according to a 2016 study.9
Even if there were a large number of medical errors in health-care settings, data in middle and low income countries are limited and varies widely since reporting error is still quite low. The factual burden of medication errors is totally underestimated. The annual cost of medical errors is estimated to be 42 billion US dollars worldwide, accounting for about 1% of total global health expenditures.6
The systematic study done in Canada indicates that the tangible sanctions facing physicians in the current medico-legal environment, norms of behavior and attitudes toward error exhibited by physicians and patients alike, causal uncertainty surrounding the error trajectory and the potential for a diffusion of responsibility, and physician weighing of harms and benefits of disclosure for patients were existing barriers to disclosure of medical errors.10
In Ethiopian medication errors were very common; whereby at least one out of two medications was wrongly prescribed and administered.11 It was caused not merely by human error, but also by the health-care systems in which people work and interact. As a result, any progress in decreasing medical errors must be made by considering the systems and processes as a whole, rather than merely at the individual level.12
In Ethiopia, as part of health system reform, many healthcare quality improvement initiatives has been tried and one of them is reporting of safety events according to the Ethiopian Hospitals Reform Implementation Guideline (EHRIG). Under the umbrella of safety event, medical error is one of patient safety event that should be reported. Although there is national guideline for reporting medical errors and safety events (EHRIG), health professionals and patients were not reporting medical errors. Therefore the aim of this study was to identify the challenges of medical error reporting for organizational learning and quality improvement in Mizan-Tepi University Teaching Hospital.
Methods
Study Area and Period
The Mizan-Tepi University Teaching Hospital was located in Mizan-Aman town which is administrative center of Bench-Sheko Zone. The hospital was established in 1986. Now it has outpatient department (OPD), medical ward, surgical ward, gynecology ward, labor ward, pediatrics ward and psychiatry ward. It has total of 521 beds and it runs multidisciplinary health care system with total of 602 staffs. So this study was conducted in Mizan-Tepi University Teaching Hospital from 01–30/01/2021.
Study Design
Explorative qualitative cross-sectional study was conducted among healthcare professionals in Mizan-Tepi University Teaching Hospital.
Population and Sampling Technique
The research was carried out among healthcare providers in Mizan-Tepi University Teaching Hospital. The healthcare providers were selected purposely based on the patient contact hour and had served in this hospital for long period of time. Twenty-one in-depth interviews were undertaken. From each wards, three in-depth interviews were held. Case team leaders and other healthcare providers were identified and interviewed. As an inclusion criterion, more than six months of service in the hospital was used.
Data Collection Tool and Procedure
After reviewing several literatures, the data collection tool was self-developed. Three public health experts with prior qualitative research experience gathered data. The data collectors were trained for three days about the purpose of the study, the ethical considerations, and the use of in-depth interview and how to facilitate the data collection procedure objectively. Semi-structured interview guide was developed in English and translated to Amharic language.
To check the consistency of the translated guide with the original interview guide, back translation was done by an independent research assistant who has been able to speak and write both English and Amharic language. The interview guide was pretested at Bachuma primary hospital. Modification was made where needed. Each day, during data collection period, debriefing sessions were held to discuss key findings, refine questions, identify data saturation and support the quality of the research process. The interview was carried out by phone call and face to face interview based on the participant’s convenience. The study participants were asked six questions: 1) what do you understand about medication error reporting? 2) What factors or challenges prevent you from reporting medical errors? 3) Is there any reporting mechanism in your organization? Could you tell us about the error reporting in your work place? 4) If you happen to make medical error, what would you do? 5) What makes you decide to report or not to report? 6) What do you understand about medical error reporting?. The hospital manager and case team leaders were interviewed by phone call due to the time constraints to hold interview meetings during the data collection period. The duration of the interview was 30–40 minutes. Thirteen (62%) of the in-depth interviews were tape recorded and the remaining 38% were recorded on papers. All the in-depth interviews were translated and transcribed to text verbatim from the language in which they were conducted into English. The paper based verbatim transcriptions were typed into Microsoft office word and reviewed by the research team to ensure that issues and questions of interest were discussed and captured. A total of 3859 word transcripts underwent thematic analysis.
Data Processing and Analysis
Using Open Code 4.0 software, which is developed by University of Umea, the data was analyzed thematically. The interviews were verbatim transcribed from the audio recordings.
Audio recorded data and the transcribed verbatim were compared to ensure accuracy of the transcription. The authors immersed in to the verbatim transcription to gather an initial impression of the data. The main points were underlined, and first impression notes were collected. These were assigned semantic codes and categorized into themes and sub-themes based on how dissimilar they were. Two of the writers worked independently on the analysis. This was followed by a series of discussions between the two authors, during which the authors’ agreed-upon themes and sub-themes were utilized.
Trustworthiness/Methodological Rigor
The degree to which the identified meanings accurately depict the participants’ opinions is measured by trustworthiness. Trustworthiness was checked using the four criteria: credibility, transferability, dependability and confirmability. To guarantee credibility prolonged engagement and peer debriefing and member checking were used. To enhance transferability, purposive sampling of the participants and thick description of the study procedure and study setting were used. The data collection, analysis, and interpretation methods are all documented in the report for dependability. The data’s dependability was ensured by the use of a stepwise replication peer assessment and a code-recode approach. An audit trail was also established for confirmability, consisting of field notes, analytical notes, and coding details.13,14
Ethical Consideration
Ethical clearance was obtained from the internal ethical review board of Mizan-Tepi University. Official permission letter was also obtained from Mizan-Tepi University teaching Hospital administration office. After explaining the purpose of the study written consent was obtained from each of the study participant. Those who gave the consent to participate in the study were then enlisted. Participants were assigned identity codes such as participant 1, 2, 3, etc. depending on their chronological participation into the study, ensuring anonymity and confidentiality. Here also it is compiled with the declaration of Helsinki-ethical principles for medical research involving human subjects.
Results
Socio-Demographic Characteristics
Twenty-one healthcare providers were recruited for this study. Majority of the participants, 12 (57.1%) were nurses and midwives and as to marital status, 18 (85.7%) were married. The majority of the participants were between the age group of 31–35. (Table 1)
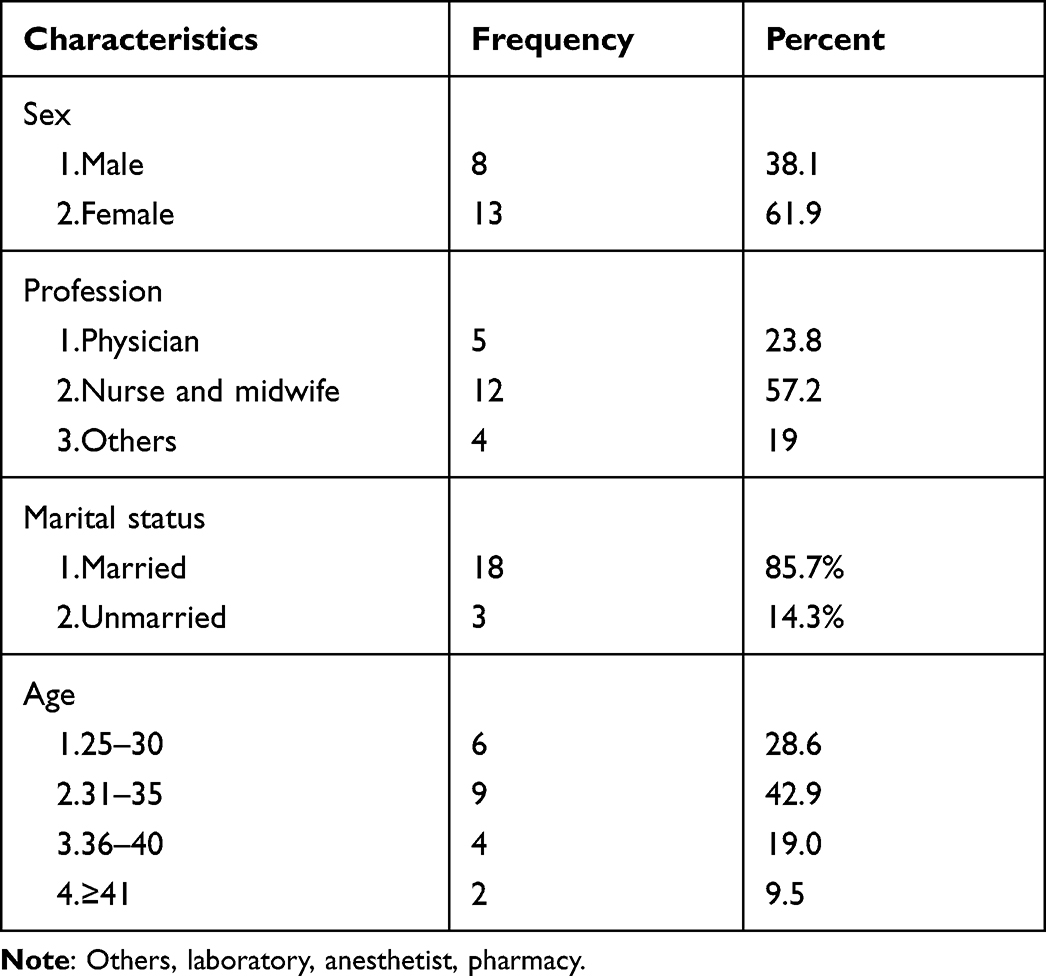 |
Table 1 Socio-Demographic Characteristics of Study Participants, 2021 |
Perceived Lack of Confidentiality of the Medical Errors
The client expects that health care providers to be perfect and they would not tolerate any kind of errors. The lack of confidentiality of the errors would damage the healthcare organizations and it would in turn, affect the health service uptake of the community.
The patients expect that the health professionals are perfect. If they hear some kind of errors, whether it would be a commission or omission, they don’t tolerate. Fearing this consequence, I think no one will disclose medical errors. (participant 1, nurse)
Imagine, if the community hears about hospital mortality due to medical error, it would our fame. It is good to learn from errors, but, for one, considering the possible consequence, I choose not to disclose. (Participant 5, nurse)
Perceived Punitive Measures
Participants mentioned that the fear of potential punishment, fear of disciplinary measure and fear of legal liability were some of the challenges of error reporting. They chose to be silent when they encounter with some kind of medical error and safety events.
In my personal experience, it is customary to punish someone who commits error and this is, I think, a bad culture. Health care providers will refrain to report mistakes to avoid such punishments rather than reporting and learning from the mistakes. (participant 2, physician)
Lack of Good Reporting System
Lack of reporting system was mentioned as one of the challenge of error reporting and organizational learning. The lack of confidential and anonymous error reporting mechanism was mentioned by the participants as the challenge of error reporting. According to the participants, there was no medical error reporting format. The participants mentioned that, the availability of medical reporting format would have helped the healthcare provider and health workers to report medical errors anonymously and it would have helped the health care organizations learn from their experiences.
If there is a secretive error reporting mechanism, the errors can be discussed without mentioning the person associated with the error. There is a meeting every two week and we can discuss the errors. The errors might not be directly attributed to the care provider. But, there are many institutional problems that might expose the care provider to commit errors. If they (medical errors) are not reported and mitigated timely, they will result in a great damage to the institution and the public at large. (participant 19, midwife)
Hmm … I think, it is good to discuss medical errors and learn from our mistakes. If we discuss our mistakes, they won’t happen again. The problem, I think, is there is no way of reporting system and format in our health center. (participant 7, nurse)
Where and, who to report to … hmm … there has to be a focal person or structural element for error reporting and organizational from experience. (participant 8, nurse)
Perceived Fear of Losing Acceptance by the Community
There was name calling and healthcare providers fear that they would lose their acceptance by the community. The healthcare provider associated with the errors, in the long run, would be communicated.
You know, we are living and working in the community. There is name calling and if you report your errors, the community will talk about you and the community will lose trust in your health care. (Participant 3, nurse)
You know what … it is annoying if a customer calls your name and they tell that they don’t want to be treated by you. … [Laughing] … we all as a human being we are prone to error but we have to be careful not lose our reputation” (Participant 12, pharmacy)
Lack of Learning Culture from Errors: “Focusing on the Sinner Rather Than the Sin” Problem
The study found that the objective of error reporting was not clearly established and it is not the error that is discussed, it is the healthcare provider that is discussed and the objective of error reporting is missing. Most of the time, quality initiatives were there and they were not translated into practice. Error reporting and organizational learning was one of the quality initiatives that were introduced by FMoH. But it was not practiced yet in the study area.
As a human being, we may do an error due to different reasons ….like shortage of times, work overload, equipment and other supplies problems. But, in our culture, I think, these factors would not be discussed and they directly point their finger on the individual. (Participant 4, nurse)
“... everybody will point at you and it is no use to report mine and my colleague’s errors.” (Participant 6, midwife)
Information Asymmetry Between the Care Provider and the Patients
Customer feedback about the service was mentioned as one of the service improvement mechanism. But, there was the problem of the information asymmetry (the service provider acts as an agent for the patients and the patients do not know about their care processes) between the care provider and the client was mentioned as a challenge of error reporting. According to the study participants, patients were not fully informed about their treatment and they could not be the source of information for medical error reporting. The patients were not actively engaged in their care and they passively took what was prescribed for them.
The clients don’t know the services they are taking. They don’t know whether they get the right treatment or not and they will not file a complaint. The only way to improve ourselves is to learn from our errors by reporting them and discussing their root causes and alternative solutions to halt them. (Participant 12, pharmacy)
“... the problem is that patients are innocent about their healthcare and we have to advocate for them. We [healthcare providers] have the professional responsibility to act on behalf of them. Because they usually are not fully informed, they cannot be a source of feedback.” (Participant 8, nurse)
Mass-Media Publication of Medical Errors
The publication of medical errors without concrete evidence and analysis through mass-media, social medias and public rumors were found to be the challenge of organizational learning from medical error reporting. The care providers abstain from reporting of medical errors in order not to defame their hospital.
The medical errors often get published by mass-media and social media. Doing this has no use rather than destroying the name of the health facility and erodes the trust of the clients up on our hospital. For that matter, the source of the medical errors could be patients themselves and Medias usually rush to judge the care providers competency and the institutions, and that is wrong I think. (Participant 9, Midwife)
Team Dynamics and Avoidance of Conflict
As healthcare is teamwork, this study highlighted that individual preference of avoidance of conflict in a team was one of the challenge for medical error reporting. Participants mentioned that, if someone discloses medical errors, it would result in conflict and their by erodes the team dynamics.
To tell the truth, if I witness a medical error, I will not report to the third party. Why would I make trouble with my coworkers? It is not good. (Participant 21, midwife)
We usually cover up each other’s errors in order to maintain our relationships. One way or another, if we don’t do so, we cannot work together. As you might know it, healthcare is teamwork and it [teamwork] is worthy taking care of. (Participant 1, nurse)
“We are the Best” Attitude of Health Professionals
The study found that some healthcare providers consider themselves as if they were perfect and they would not own up their mistakes and they do not take shared responsibility and they usually condemn others. They [healthcare providers] did not acknowledge errors and they were not prepared to learn from errors.
All errors are attributed to middle level and lower level healthcare providers. General practitioners and physicians don’t want to make themselves free from any kind of errors. According to them, it is us [nurses] that commit errors not them. (Participant 15, physician)
We [Nurses] are the scapegoats for many omissions and commissions that occur in health care facilities. (Participant 5, laboratory)
Absence of Malpractice Insurance
The participants mentioned the absence of malpractice insurance was another challenge for error reporting. “Who is going to pay the compensation for those who are victims of errors? They need to be paid compensation.”
Discussion
This study was conducted among nurses, general practitioners and physicians. There were system related factors and individual related factors that hindered organizational learning from error through error reporting. Among the system related factors, the absence of error reporting format, absence of confidential error reporting system, and the lack of organizational learning from past experiences in the hospitals were sought to be the barriers. Studies also showed that these systems related factors were the barriers for error reporting and organizational learning from errors.15 According to the Ethiopian hospitals reform guideline, different initiates were introduced to improve quality of healthcare and one of them was voluntary error reporting.16
The punitive culture of the healthcare organizations for errors was found to be one of the challenges for error reporting. Studies showed that, the main cause of medical errors is because of the healthcare systems complexity rather than individual negligence and misconduct.17 Legal liability for medical errors was also found to be the barrier for error reporting. According to studies, the disciplinary measures by the healthcare organizations combined with legal liability hindered the disclosure of medical errors.18
Many healthcare organizations (HCOs) had punitive policies against healthcare providers who commit medical errors. Even though these disciplinary measures and policies against the healthcare providers are meant to reduce the commission of medical errors, fear of potential liability for disciplinary measures and legal liability are more likely to hinder them from reporting errors and thereby the HCOs lost the opportunity to learn from errors. Chances are the same mistakes will occur repeatedly.19–21
Mass media publication of the errors due to the lack of systematic and confidential reporting system was found to be the barriers for organizational learning from past experience. Study conducted in USA showed that the disclosure of errors to the community at large resulted in the erosion of trust by the community and this in turn increases institutional betrayal.22 Communities may lack confidence in health care organizations when the errors are published by mass media and other media outlets. On the other hand, the introduction of different systematic error reporting ways resulted in the reduction of medical errors. Studies showed that the introduction of barcode system and bundle system resulted in the reduction of medical errors.23 Another study sheds light on the importance of diligence to follow the due processes of clinical care and concludes that careful labeling of drugs and patients is paramount for medical error reduction24 and this approach is very important where there is lack of open communication about misshapen.
Errors were attributed to middle and lower level health care providers especially nurses and when discussing about errors, the focus of the discussion was on the healthcare provider not on the root cause of errors. According to the study conducted in Iran, physicians were not involved in medical error reporting even if serious medical errors were done by them.25
The other factor for medical error disclosures was the information asymmetry between the care provider and the patients. Patients are expected to inform errors up on them and they would contribute to the reduction of preventable medical errors given that they are informed about the clinical procedures. The EHRG states that patients can file a complement to their healthcare provider,16 but, in healthcare marketing, there is problem of information asymmetry between the care provider and the patient and they would not be fully informed about their care and the potential side effects.26,27 In addition to the nature of healthcare market, low level of health literacy in developing countries one way or another might contribute to hide the medical errors.28
The study showed that healthcare providers want to maintain the team dynamics and they will not report the medical errors of their colleagues. Healthcare providers in the climate of fear are reluctant to report medical errors in order to avoid conflict.29 One study highlighted that medical error is a systemic problem and it has many contributing factors. According to the study, focusing on individuals cannot capture the complete picture of the problem and it has to be viewed as a systemic problem.30 In the contrary, our study showed that errors are attributable for individuals and this will not help improve quality of healthcare.
On the other hand, the study conducted in Korea among nursing professionals showed that team work was positively associated with medical error reporting performance. In a healthcare organization where there is poor team communication, the medical error reporting performance would be low.31
Limitation of the Study
This study, as it is a qualitative study in its entirety, should be understood in view of the following limitations. It was difficult to quantitate the extent of the problem the effect size of the influence of each factor for error reporting.
Conclusion
The challenges of medical error reporting can be categorized as health system related factors (lack of organizational learning culture from experiences, lack of anonymous error reporting system, team dynamics), external environment related factors (mass-media publication of medical errors, information asymmetry), individual factors (perceived lack of confidentiality of reported medical errors, “we are the best attitude of healthcare providers).
Abbreviations
EHRIG, Ethiopia Hospital Reform Implementation Guideline); OPD, out patients department; DEC, department executive committee; FMoH, Federal Minister of Health; HCOs, Health care organization.
Data Sharing Statement
The datasets used in this study are available from the corresponding author and can be obtained with a reasonable request.
Consent for Publication
Not applicable.
Acknowledgments
The authors appreciate Mizan-Tepi University’s technical assistance and ethical permission, as well as the study participants and data collectors.
Funding
No organization has provided funding for this project.
Disclosure
There are no conflicts of interest declared by the authors.
References
1. Eisenberg JM, Foster NE, Meyer G, Holland H. Federal efforts to improve quality of care: the quality interagency coordination task force (QuIC). Jt Comm J Qual Improv. 2001;27(2):93–100. doi:10.1016/S1070-3241(01)27009-6
2. Vozikis A, Rig M. Patterns of medical errors: a challenge for quality assurance in the Greek health system. Qual Assur Manag. 2012. doi:10.5772/31417
3. Grober ED, Bohnen JMA. Defining medical error. Can J Surg. 2005;48(1):39–44.
4. World Helath Organization. Draft Guidelines for Adverse Event Reporting and Learning Systems. Geneva, Switz: World Health Organization; 2005:80.
5. Leape L. Error in medicine. JAMA. 2019;272:1851–1857. doi:10.1001/jama.1994.03520230061039
6. Wolf ZR, Hughes RG. Error reporting and disclosure; 2015:2–333.
7. Bates DW, Leape LL, Cullen DJ, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. J Am Med Assoc. 1998;280(15):1311–1316. doi:10.1001/jama.280.15.1311
8. Slawomirski L, Auraaen AKN. The economics of patient safety - strengthening a value-based approach to reducing patient harm at national level: organisation for economic co-operation and development - OECD. OECD Heal Work Pap; 2018. Available from: https://www.oecd-ilibrary.org/social-issues-migration-health/the-economics-of-patient-safety_5a9858cd-en.
9. Makary MA, Daniel M. Medical error-the third leading cause of death in the US. BMJ. 2016;353:1–5.
10. Entwistle M, Kalra J. Barriers to medical error disclosure: an organizing framework and themes for future research. Austin J Pathol Lab Med. 2014;1(2):1–6.
11. Endalamaw A, Dessie G, Netsere HB, Belachew A. Medication errors in Ethiopia: systematic review and meta-analysis. Res Gate. 2020;2020. doi:10.21203/rs.3.rs-35808/v1
12. Wamisho BL, Teklemariam E. Surgical and medical error claims in Ethiopia: trends observed from 125 decisions made by the federal ethics committee for health professionals ethics review. Medicolegal Bioeth. 2019;9:23–31. doi:10.2147/MB.S219778
13. Anney VN, Dar POB, Salaam E. Ensuring the quality of the findings of qualitative research: looking at trustworthiness criteria. JETERAPS. 2014;5(2):272–281.
14. Graneheim UH, Lundman B. Qualitative Content Analysis in Nursing Research: concepts, Procedures and Measures to Achieve Trustworthiness Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2015;24:105–112.
15. Poorolajal J, Rezaie S, Aghighi N. Barriers to medical error reporting. Int J Prev Med. 2015;6(97). doi:10.4103/2008-7802.166680
16. Ethiopian Minnister of Health (EMoH). Ethiopian Hospital Reform Implementation Guidelines. Federal Democratic Republic of Ethiopia Ministry of Health; 2010.
17. Institute of Medicine. To Err is Human: Building a Safer Health System. National Academies Press; 1999.
18. Kapp MB. Medical error versus malpractice. DePaul J Health Care Law. 2015;1(4):751.
19. Kalra J, Kalra N, Baniak N. Medical error, disclosure and patient safety: a global view of quality care. Clin Chem. 2013;46(13–14):1161–1169. doi:10.1016/j.clinbiochem.2013.03.025
20. Rathert C, Phillips W. Medical error disclosure training: evidence for values-based ethical environments. J Bus Ethics. 2010;97:491–503. doi:10.1007/s10551-010-0520-3
21. Scheirton LS. Proportionality and the view from below: analysis of error disclosure. HEC Forum. 2008;20(3):215–241. doi:10.1007/s10730-008-9073-6
22. Smith CP. First, do no harm: institutional betrayal and trust in health care organizations. J Multidiscip Healthc. 2017;10:133–144. doi:10.2147/JMDH.S125885
23. Bowdle TA, Jelacic S, Nair B, et al. Facilitated self-reported anaesthetic medication errors before and after implementation of a safety bundle and barcode-based safety system. Br J Anaesth. 2018;121(6):1338–1345. doi:10.1016/j.bja.2018.09.004
24. Meena SC, Dulara SC, Meena S, Tripathi A. Case report preventable critical incidents in anaesthesia: a retrospective analysis of two anaesthetic mishaps after inadvertent drug administration. JSAN. 2016;3(2):2015–2017.
25. Ranaei A, Gorji HA, Aryankhesal A. error ‑ reporting system and reporting. J Edu Heal Promot. 2020;9:272.
26. Cruz MJD, Kini RB. The effect of information asymmetry on consumer driven health plans. Integr Innov Orient to E-Society. 2007;251:353–362.
27. Major I. Two-sided information asymmetry in the healthcare industry. Int Adv Econ Res. 2019;25:177–193. doi:10.1007/s11294-019-09732-9
28. Osborne RH, Beauchamp A, Batterham R. International journal of infectious diseases health literacy: a concept with potential to greatly impact the infectious diseases field. Int Soc J Infect Dis. 2016;43:101–102. doi:10.1016/j.ijid.2015.12.012
29. Etchells E, Lester R, Morgan B, et al. Healthcare quarterly; 2005.
30. Anderson DJ, Dipnurs R, Anderson D. Nursing and health care management issues a systems approach to the reduction of medication error on the hospital ward. J Adv Nurs. 2001;35(1):34–41. doi:10.1046/j.1365-2648.2001.01820.x
31. Hwang J, Ahn J. Teamwork and clinical error reporting among nurses in Korean hospitals. Asian Nurs Res. 2015;9(1):14–20. doi:10.1016/j.anr.2014.09.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.