Back to Journals » Journal of Inflammation Research » Volume 19
Challenges in Differentiating Chronic Inducible Urticaria from Chronic Spontaneous Urticaria
Authors Bendayan E, Ton That A, Zhu CK, Netchiporouk E, Ben-Shoshan M
Received 12 August 2025
Accepted for publication 21 January 2026
Published 31 January 2026 Volume 2026:19 546302
DOI https://doi.org/10.2147/JIR.S546302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anish R. Maskey
Ethan Bendayan,1 Alexandre Ton That,1 Catherine Keying Zhu,2 Elena Netchiporouk,2,3,* Moshe Ben-Shoshan4,*
1Faculty of Medicine and Health Sciences, McGill University, Montreal, QC, Canada; 2Division of Dermatology, Department of Medicine, McGill University Health Centre, Montreal, QC, Canada; 3Division of Experimental Medicine, Department of Medicine, McGill University, Montreal, QC, Canada; 4Division of Pediatric Allergy and Clinical Immunology, Department of Pediatrics, McGill University, Montreal, QC, Canada
*These authors contributed equally to this work
Correspondence: Ethan Bendayan, Faculty of Medicine and Health Sciences, McGill University, 1001 Decarie Boulevard, Montreal, Quebec, H4A 3J1, Canada, Email [email protected]
Abstract: Chronic urticaria (CU) is a mast cell-driven condition presenting with recurrent wheals (hives), angioedema, or both for over 6 weeks. It encompasses chronic spontaneous urticaria (CSU), in which hives occur without specific external triggers, and chronic inducible urticaria (CIndU), in which stimuli, such as physical factors, reliably induce hives. Differentiating CIndU from CSU may be challenging yet crucial. Patients may have unrecognized triggers or may have both CSU and CIndU, rendering diagnosis and management challenging. Drawing on current guidelines, randomized control trials, observational studies, and other recent studies, this narrative review discusses the subtypes of CSU and CIndU, emphasizing clinical distinctions, diagnosis, and treatment implications. Key diagnostic clues to identify CIndU include the reproducibility of symptoms followed by defined stimuli and a positive response to provocation testing. In contrast, CSU diagnosis should be centered on clinical history. Biomarkers may be helpful to establish a diagnosis of autoimmune CSU but are rarely ordered in routine practice. Treatment is outlined according to current guidelines and evidence, noting that while second-generation H1-antihistamines are first-line for all CU patients, patients with CIndU often require trigger avoidance and occasionally off-label therapies (eg, omalizumab) for adequate control. In addition, this review discusses emerging treatments for CU, such as dupilumab, Bruton’s tyrosine kinase (BTK) inhibitors, and barzolvolimab, which reflect the rapidly evolving therapeutic landscape. This review provides a practical guide for clinicians to differentiate and manage CSU and CIndU, by identifying key differences between CSU and CIndU based on current evidence.
Keywords: chronic urticaria, chronic inducible urticaria, chronic spontaneous urticaria, provocation testing
Introduction
Chronic urticaria (CU) refers to recurring urticaria (hives) and/or angioedema for >6 weeks.1 It is broadly divided into chronic spontaneous urticaria (CSU) and chronic inducible urticaria (CIndU).1 CSU, previously known as chronic “idiopathic” urticaria, is defined by recurrent wheals/angioedema that occur unpredictably and without identifiable triggers, whereas a reproducible external trigger can be identified in CIndU.1 This distinction is clinically important for diagnosis and management: identifying a trigger can direct avoidance strategies and specific interventions in CIndU, while CSU diagnosis typically involves ruling out underlying causes, assessing aggravating factors, and evaluating biomarkers predicting response to treatment instead.1
CU significantly impairs quality of life and productivity.1 It is a common condition, with an estimated lifetime prevalence of approximately 1–4%.2,3 At any time, CSU is more prevalent than CIndU, with reported point prevalences of up to 2.7% and 1.5%, respectively.1 Notably, both subtypes of CU can coexist in the same patient.1 In fact, up to 30% of patients with CSU have an inducible trigger as well.4 For example, a patient with daily spontaneous hives who also develops wheals upon cold exposure will be considered to have both CIndU (ie, cold-induced urticaria) and CSU.5 Studies suggest that patients with concomitant CSU and CIndU tend to have more severe disease, with more frequent angioedema, emergency visits, and a need for systemic steroids compared to those with isolated CIndU.5 These patients represent a particularly challenging endotype with a more refractory course.5
Differentiating CIndU from CSU can be challenging for several reasons. Patients may not recognize or report subtle triggers, making CIndU appear like CSU. Some physical urticaria subtypes like delayed pressure urticaria (DPU) have a delayed onset of symptoms after the stimulus, obscuring the association.3 Additionally, baseline disease activity in CSU may be modulated by non-specific exacerbating factors, like psychological stress, that are not considered true CIndU triggers, but can make differentiation more challenging.1 This review will discuss CSU and the spectrum of CIndU triggers, focusing on practical clinical features that aid in distinguishing them, the use of provocation testing for diagnosis, and implications for treatment. Key diagnostic clues and management considerations are highlighted (Tables 1 and 2). For this narrative review, a non-systematic literature search of clinical guidelines, randomized control trials, observational studies, and other relevant studies was conducted using PubMed.
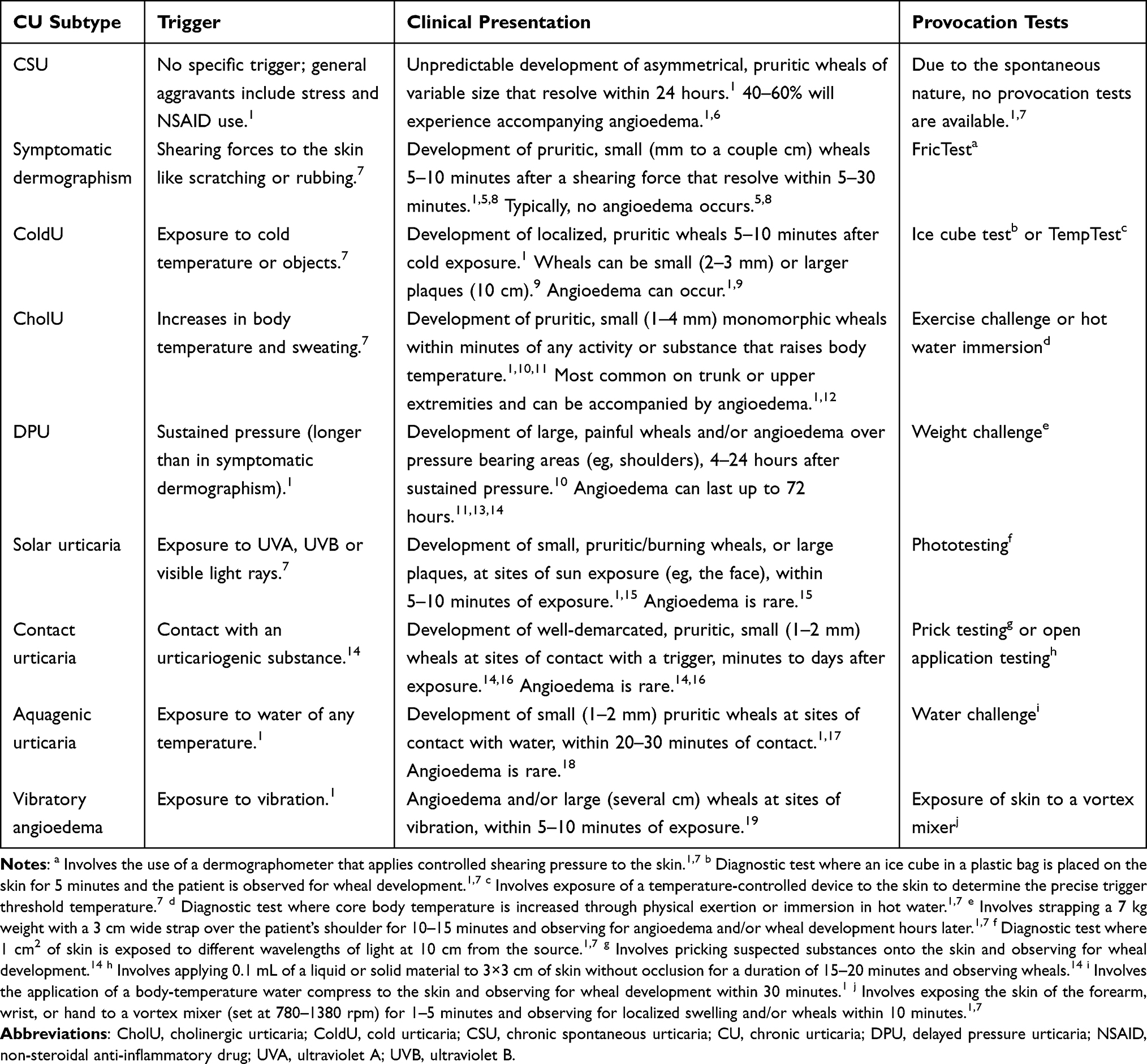 |
Table 1 Diagnostic Differences in CU Subtypes |
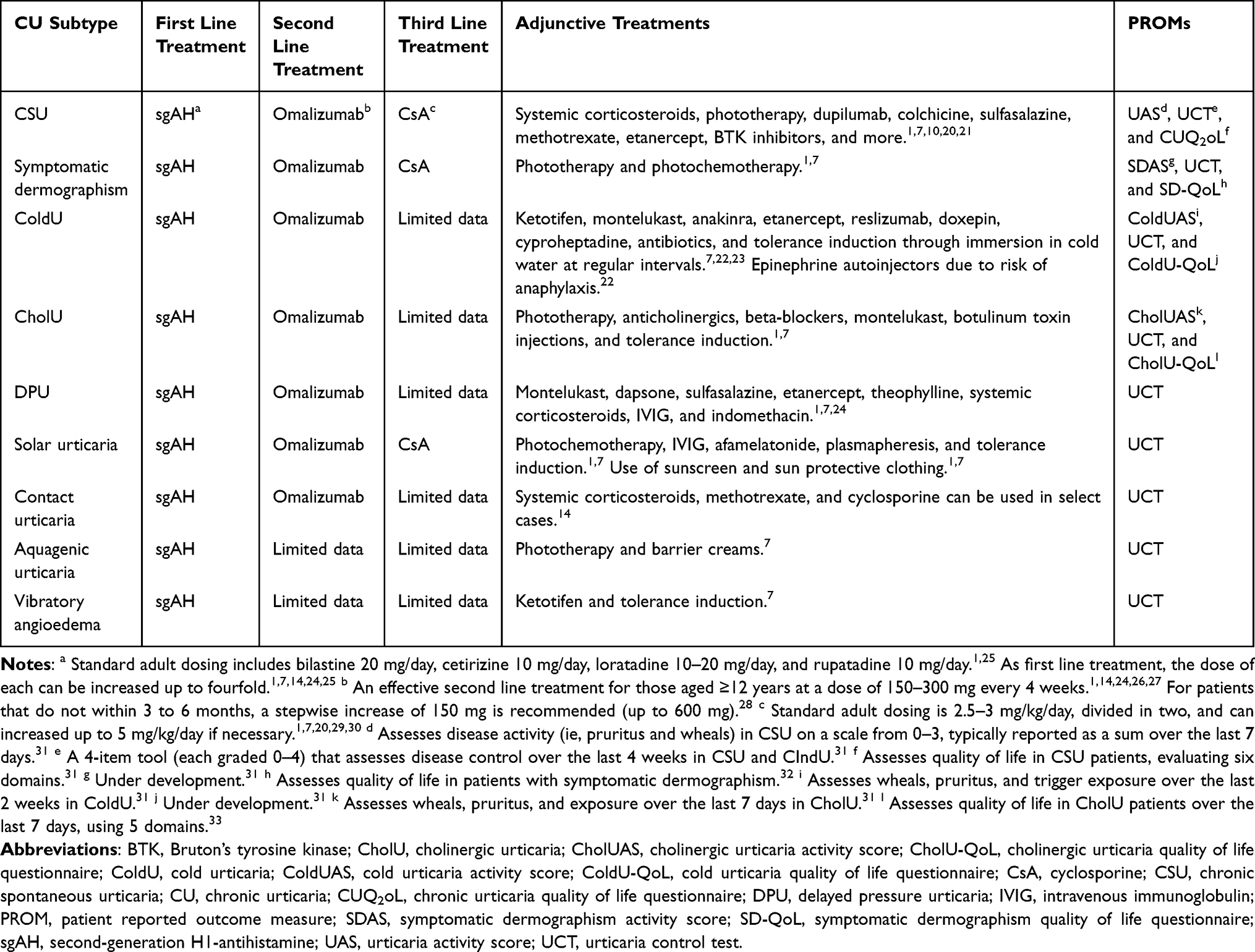 |
Table 2 Treatment Approaches and PROMs in CU Subtypes |
Chronic Spontaneous Urticaria
CSU is characterized by the spontaneous appearance of wheals, angioedema, or both, on a near-daily basis without a consistent provoking factor (Figure 1).1 By definition, hives in CSU occur without a trigger and it is a diagnosis of exclusion after inducible causes have been considered.1 CSU episodes can often exhibit unpredictable frequency and duration.1 Individual hives characteristically last less than 24 hours by definition, often lasting just a few hours.1 Angioedema affects up to 40–60% of CSU patients and may last for days.1,12,34 Patients describe intense pruritus, and the chronic itching and disfigurement lead to poor quality of life, sleep disturbance, and anxiety.35
 |
Figure 1 Characteristic wheals in a child with chronic spontaneous urticaria. |
CSU can affect all ages but is considered most common in adults, especially in those older than 30 years.1 In adults, there is a female predominance, with up to 70% of patients being female.1,2,36 The average duration of CSU in adults is 11.5 years.37 Spontaneous remission occurs in approximately 17% of patients at one-year post-onset, but those with more severe disease may have a more protracted course.38 It was reported that resolution of CSU is similarly low in children (10% natural resolution rate) and even lower in inducible forms (eg, 5% resolution per year in ColdU).39,40
Unlike CIndU, which has exogenous triggers, CSU is thought to result from endogenous pathophysiologic triggers, of which 30–50% are autoimmune-mediated.41 Two forms of autoimmunity are described: type I autoallergy, in which IgE antibodies target self-antigens (autoallergens) leading to mast cell degranulation, and type IIb autoimmunity, in which IgG antibodies target IgE or the high-affinity IgE receptor (FcεRI) on mast cells.2 Type IIb CSU (also termed autoimmune CSU) is associated with biomarkers such as low total IgE levels, positive autologous serum skin test (ASST), and other autoimmune thyroid antibodies such as anti-thyroid peroxidase (anti-TPO).2 Clinically, patients with type IIb autoimmune CSU tend to have more severe urticaria that responds poorly to second-generation H1-antihistamines (sgAHs) and can be refractory to omalizumab (anti-IgE therapy).2 Chronic infections, stress, and pseudoallergens (ie, dietary components) have been proposed as contributors in some CSU cases, but routine screening for these is often low-yield and not broadly recommended.42
Clinical Evaluation of Chronic Spontaneous Urticaria
The cornerstone of CSU diagnosis is a thorough history and physical exam to exclude inducible causes, which define CIndU.1 Clinicians should inquire about any patterns or exposures, like cold or water, that precede hives to ensure their symptoms are not attributable to CIndU.1 In CSU, by definition, patients will not have a consistent trigger and hives develop without explanation.1 Certain non-specific factors may exacerbate CSU, like stress and use of non-steroidal anti-inflammatory drugs (NSAIDs), but these are not considered specific inducible subtypes.1
To date, no clear biomarker can define CSU and guidelines recommend minimal routine testing, often limited to a complete blood count and C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) to assess for underlying inflammation.1,2 If clinical suspicion is high, tests for autoimmune markers may be done (eg, anti-TPO antibodies, ASST, total serum IgE, basophil activation test [BAT], basophil histamine release assay [BHRA]) to identify an autoimmune CSU endotype.2,43,44
More specifically, thyroid autoimmunity is commonly associated with CSU, and anti-TPO antibodies can be found in 21–26% of CSU patients—especially type IIb CSU patients.43,44 Similarly, patients with type IIb CSU typically have low total serum IgE levels (<40 IU/L), whereas levels are normal-to-high in type I CSU and in CIndU.43 While total IgE levels are not diagnostic, higher levels predict better response to omalizumab and, therefore, may have clinical significance in some cases.43
The ASST is an in vivo clinical test where a patient’s own serum is injected intradermally to detect the presence of circulating histamine release factors.1,45 Other basophil-based biomarkers, such as the BAT and BHRA, are also non-specific biomarkers: BAT measures basophil activation markers (CD63 or CD203c) in the serum; the BHRA measures serum-induced histamine release.43 The BAT and BHRA are seldom used clinically and are usually reserved for specialized or research settings.45 Positive immunoassays for IgG-anti-FcεRI or IgG-anti-IgE are also important biomarkers to establish a diagnosis of type IIb CSU.43
Basopenia and eosinopenia may be suggestive of an autoimmune phenotype.43 Recently, T-cell cytokines, such as IL-17 and IL-33, have emerged as potential CSU biomarkers; however, more research on their specificity and sensitivity is needed.45
According to some, the diagnosis of type IIb CSU requires a positive ASST, a positive immunoassay for IgG-anti-FcεRI or IgG-anti-IgE, and a positive BHRA or BAT; however, some studies define it as the presence of one autoimmune biomarker (eg, positive ASST, positive anti-TPO, or low total IgE).43,46
Overall, most biomarkers are non-specific and reserved for type IIb CSU—they are generally absent or non-informative in type I CSU and CIndU.43 Importantly, there is a lack of validated biomarkers for CIndU and diagnosis relies on history and provocation testing. Even in CSU, diagnosis is generally not biomarker-based and should be primarily guided by clinical history (ie, pattern and timing of flares).45
Furthermore, extensive allergy testing is not routinely indicated in CSU, as food and environmental allergies rarely cause CU.26 Likewise, screening for chronic infections or other internal diseases should be guided by history.42
To clinically distinguish CSU from CIndU, it is crucial to establish the pattern of flares. A patient with CSU might report that they develop hives randomly throughout the day, in an irreproducible manner.1,42 In contrast, CIndU manifests in relation to specific activities or environmental exposures.1 Recognizing CSU is important because it directs the clinician to focus on internal causes or comorbidities, and to inform patients that trigger avoidance is usually not possible, aside from general provoking factors (ie, stresss or NSAIDs).1 Accurate identification of CSU also allows the clinician to investigate for autoimmune urticaria, which is more likely to fail the standard therapeutic approach.43
Chronic Inducible Urticaria
CIndU is the subtype of CU in which hives and/or angioedema are consistently provoked by specific stimuli.1 By definition, a patient with CIndU remains symptom-free unless exposed to the precipitating factor, or after a threshold of exposure is exceeded.1 The triggers can be physical forces (eg, cold, heat, vibration, or sunlight) or other environmental/chemical exposures (eg, water, increase in body temperature, or contact with certain substances).3,10 The exact pathophysiological mechanisms by which physical, chemical, or environmental triggers induce mast cell degranulation in CIndU remain incompletely understood. The key feature is that the patient can often identify certain activities that trigger their hives, which their clinician can confirm by provocation testing.
CIndU is less common than CSU, but within specialty urticaria clinics it is frequently encountered.2 Some patients have isolated CIndU with no spontaneous hives at all, while others may have inducible triggers alongside spontaneous flares (ie, concomitant CSU and CIndU).2 The most frequent subtypes of CIndU are physical urticarias, especially symptomatic dermographism, cold urticaria (ColdU), and cholinergic urticaria (CholU).1,2,5 Less common forms include DPU, solar urticaria, vibratory urticaria, aquagenic urticaria, and contact urticaria.1 Each subtype displays characteristic clinical features and diagnostic considerations (Table 1).
Symptomatic Dermographism
Symptomatic dermographism (dermographic urticaria) is the most common subtype of CIndU and is triggered by mechanical shearing forces on the skin like scratching.5,10 Patients develop linear wheals, which can resemble writing, at sites of scratching, rubbing, or friction; it is often prominent along scratch lines or under clothing seams.13 The reaction is typically pruritic and occurs within minutes (typically within 5–10 minutes after stroking the skin), and each wheal usually resolves within 30 minutes.1,10,11 Unlike CSU, these patients do not develop hives spontaneously; lesions strictly arise after physical forces to the skin.1 Angioedema is typically absent in isolated dermographism.5 While mild forms of dermographism can be seen in the general population, the response is exaggerated and bothersome in those with dermographic urticaria.11 Diagnostic clues include being able to elicit a raised pruritic wheal by firmly stroking the patient’s skin with a dermographometer or ball-point pen.7,47
Cold Urticaria
ColdU is provoked by exposure to cold temperatures (eg, cold air, cold water, or contact with cold objects).10 Patients notice hives and angioedema in cold-exposed areas of skin, within minutes of cooling or rewarming.1,5,10 For example, upon touching ice, affected individuals develop localized itchy welts, or generalized urticaria and anaphylaxis in severe cases.11 ColdU lesions typically develop rapidly (within 5–10 minutes of exposure) and resolve within 30 minutes if rewarming is prompt.1,48 This condition often affects young adults, and both genders are affected, with some studies suggesting a slight female predominance.5 ColdU is particularly important to recognize because it is the main CIndU subtype clearly associated with anaphylaxis, with up 21% of patients experiencing anaphylaxis with normal activities (eg, swimming in cold water).5,10,22,34 Differentiating ColdU from CSU can be lifesaving as a CSU patient might take a cold shower with no issue, whereas a ColdU patient could have a dangerous reaction.22 A simple in-office diagnostic test is the ice cube test, where an ice cube is placed on the forearm for 5 minutes; a positive test is the formation of a typical wheal at the site during rewarming (Figure 2).10
 |
Figure 2 Positive ice cube test in a child with cold urticaria. |
Cholinergic Urticaria
CholU is triggered by increased core body temperature and sweating.10 Common provoking scenarios include exercise, hot baths or showers, saunas, emotional stress, and spicy food.10,11 Within minutes of such activities, patients develop numerous tiny itchy wheals on a background of diffuse erythema, typically on the upper trunk, neck, and arms (Figure 3).1,10,11 The hives in CholU tend to resolve quickly, often fading within an hour.10,12 CholU predominantly affects adolescents and young adults, with no specific sex predominance.2,5,10 One survey found that up to 20% of college students reported CholU symptoms with exercise, suggesting that mild forms may be common.10,12 It is crucial to distinguish CholU from exercise-induced anaphylaxis, a separate condition where exercise (often in combination with food ingestion) leads to anaphylactic reactions.11,42 In CholU, the lesions are typically small, and the reaction, while uncomfortable, usually remains limited to hives.11 If a patient only experiences pinpoint hives with overheating and no systemic symptoms, CholU is likely the diagnosis instead of exercise-induced anaphylaxis.11 An exercise challenge (eg, running in place or on a treadmill until an increase in heart rate and perspiration occurs) can serve as a provocation test, reproducing the hives.10 Less common forms of CholU also exist.12 A classification based on clinical characteristics was proposed to include four subtypes of CholU:12
- Conventional sweat allergy-type CholU
- Follicular-type CholU with a positive ASST
- CholU with palpebral angioedema, which is more predominant in females and associated with anaphylaxis and a predisposition to atopy
- CholU with acquired anhidrosis and/or hypohidrosis.
 |
Figure 3 Truncal distribution of wheals in a patient with cholinergic urticaria. |
Delayed Pressure Urticaria
In DPU, the trigger is sustained pressure on the skin, but unlike dermographism, the reaction is delayed by several hours.1,3,10 Patients develop deep, painful swelling or urticarial plaques at sites of prolonged pressure, such as under tight belts, on the soles of the feet after walking, on the buttocks after sitting, or under the straps of a backpack.13 The wheals and angioedema of DPU typically appear 4–8 hours after the pressure stimulus and can appear up to 12–24 hours later in some, making this a difficult diagnosis to establish.1,3,10,11,13 The angioedema can last >24 hours and tends to be more painful or burning rather than pruritic.11,13,14 DPU often coexists with CSU, with up to 36% of all CU patients having concomitant CSU and DPU.1,2 In fact, purely isolated DPU without CSU is relatively uncommon.2 This subtype can significantly impact quality of life because routine activities such as standing and carrying objects can precipitate symptoms.10 Provocation testing for DPU involves applying a known pressure to the skin for a fixed duration (eg, strapping a 7–10 kg weight to the patient’s thigh) and observing for a wheal 6–8 hours later.10,11 DPU is one of the most difficult subtypes to diagnose and to manage.
Solar Urticaria
Solar urticaria is triggered by sunlight (ultraviolet [UV] or visible light) exposure.10 Affected patients develop hives on sun-exposed skin within 5–10 minutes of sun exposure.1,10 The reaction can occur with various wavelengths of light; some patients react mainly to UVA, while others react to UVB or visible light.13 Solar urticaria is rare and patients must be differentiated from photosensitive dermatoses (ie, polymorphic light eruption or systemic lupus erythematosus), which are not usually immediate in onset and/or last >24 hours.7,49 Phototesting in specialized centers can confirm the specific wavelengths that trigger the reaction.49 Like ColdU, solar urticaria can occasionally cause systemic reactions; however, there is no clear association with anaphylaxis.34,49,50 This is supported by a recent systematic review which found that angioedema (2.4%), systemic symptoms (4.4%), and anaphylaxis (0.9%) are rare amongst patients with solar urticaria.51
Contact Urticaria
Contact urticaria results from direct skin contact with an urticariogenic substance.10 It can be non-immunologic, usually caused by low molecular weight chemicals like benzoic acid, or IgE-mediated, in which case an allergen is the trigger.10,14 Wheals can be immediate or delayed, developing within minutes to days after exposure.1,10,14 In IgE-mediated contact urticaria, lesions may spread beyond the contact area and can be accompanied by anaphylaxis if the allergen is potent.14 For example, in highly allergic individuals, skin contact with a peanut protein can cause a systemic reaction. Non-immunologic triggers are usually accompanied by a burning or stinging sensation, while immunologic triggers cause pruritus.14 A careful history of topical exposures, such as cosmetic products, foods or occupational exposures, can point to contact urticaria.14 Skin prick testing or open application testing with the suspected substance can be diagnostic if done cautiously.11,14 Patch testing can be used to exclude contact dermatitis, but is not used to diagnose contact urticaria itself.14
Aquagenic Urticaria
Aquagenic urticaria is exceedingly rare and is triggered by contact with water of any temperature, unlike ColdU which is only triggered by cold water.5,10 Patients develop small pruritic wheals in areas that contact water, usually within 20–30 minutes of exposure, that last about 30–60 minutes.1,10,11 Angioedema is rare in aquagenic urticaria.18 Interestingly, in some cases, only certain water sources, such as sea water, elicit the response, while other sources, like tap water, do not.10 Importantly, pruritus after water contact can also occur with polycythemia vera and other internal diseases, but these cases are not accompanied by wheals.10 Aquagenic urticaria is diagnosed clinically and by water challenge, in which a body-temperature water compress is applied to skin, and the patient is observed for hives.10,11
Vibratory Angioedema
Vibratory angioedema (vibratory urticaria) is a rare form of CIndU which can be hereditary or acquired, and is triggered by vibrational stimuli, such as using a lawn mower or jogging on a hard surface.10 Angioedema and/or hives develop within 5–10 minutes of exposure at the site of vibration and resolve within 24 hours.1,10,11 Vibratory urticaria can be particularly burdensome for construction workers, or patients who operate machinery like power tools and jackhammers.11 It can be clinically diagnosed by placing a vibrating device, such as a lab vortex mixer, on the skin for a fixed time and watching for a reaction.10
Provocation Testing in Urticaria
Provocation testing is a critical tool for diagnosing CIndU.1 A detailed history should guide appropriate tests (Figure 4).1 For example, as noted, a simple ice cube test, in which an ice cube is applied to the skin for five minutes, is used to diagnose ColdU, with a wheal within a few minutes of exposure indicating a positive result (Figure 2).10 For dermographism, a tongue depressor or specialized dermographometer drawn across the skin can reproduce linear hives within minutes.10,47 Exercise challenge (treadmill or step climbing) or a hot bath test (immersing in warm water) can provoke CholU in a controlled setting.10 Pressure testing can be done by applying weights or a tourniquet and evaluating hours later for swelling.10 Phototesting with various wavelengths confirms solar urticaria.10 These tests have standardized protocols (eg, different size ice cubes or durations to measure the threshold that causes reaction).
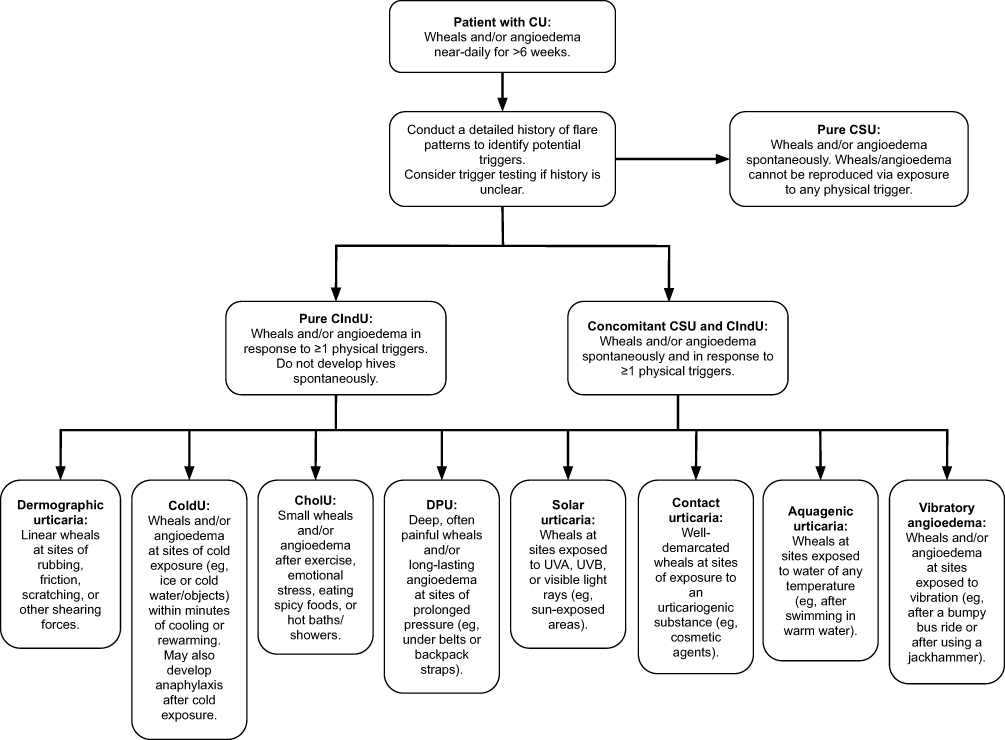 |
Figure 4 Diagnostic algorithm to differentiate the subtypes of chronic urticaria. Abbreviations: CholU, cholinergic urticaria; CIndU, chronic inducible urticaria; ColdU, cold urticaria; CSU, chronic spontaneous urticaria; CU, chronic urticaria; DPU, delayed pressure urticaria; UVA, ultraviolet A; UVB, ultraviolet B. |
The goals of provocation testing include: confirming the diagnosis of a suspected CIndU subtype, determining the threshold of stimulus needed to cause hives, and establishing a baseline disease activity to monitor treatment response over time.10 For instance, if a patient with ColdU only reacts if ice is applied for >3 minutes, that threshold can be tracked for improvement with therapy.
Provocation tests should be done in a supervised setting where a physician is present with a working epinephrine injector on hand.10 This is because certain subtypes of CIndU, like ColdU, can occasionally lead to systemic reactions during testing.10 Additionally, patients should typically be off antihistamines or other mast cell-suppressing medications for a few days prior to provocation testing to avoid false-negative results.10
Provocation testing is only indicated for the subtype suggested on history and CU patients should not undergo provocation testing for all CIndU subtypes.2 For example, a patient whose history is only consistent with solar urticaria, should not undergo the ice cube test for ColdU. In atypical cases where initial standard tests are negative, but suspicion remains high, more specialized testing can be pursued.10 For example, a patient with suspected ColdU and a negative ice cube test might undergo a whole-body cold challenge or cool water immersion test to rule out an unusual presentation of ColdU.10
Provocation testing is not only for diagnosis, but also for patient counseling because it can help patients understand which activities to avoid and which not to. In summary, provocation tests are crucial for confirming the CIndU subtype and distinguishing CIndU from CSU. By contrast, CSU is a diagnosis of exclusion when no specific trigger can explain all episodes of hives and/or angioedema.1
Treatment Implications
Management of CU aims for complete symptom control with minimal side effects.1 Both CSU and CIndU are treated with a similar stepwise approach as outlined in current EAACI/GA2LEN/EuroGuiDerm/APAAACI guidelines, but there are important differences in treating subtypes of CIndU (Table 2).1,26
First-line therapy for any subtype of CU is daily sgAHs, such as cetirizine, loratadine, and bilastine.10,26 SgAHs prevent histamine from binding the H1 receptor by binding as an inverse agonist.25 Unlike first-generation H1-antihistamines, sgAHs are non-sedating because they have limited penetration of the blood-brain barrier, making them the preferred option.25,26,29 Daily sgAH use can reduce itch and wheal formation in both CSU and CIndU.1 If standard dosing of sgAHs is inadequate, international guidelines recommend increasing the dose up to fourfold, in a stepwise manner.1,23,26 In both CSU and CIndU, up-dosing has been shown to be effective to control disease in those not controlled on standard doses.23 This approach appears to be well tolerated, as a systematic review found that up-dosed sgAHs increase minor adverse events (eg, headache, upper respiratory tract infection, and somnolence), but not major adverse events.52
Despite the effectiveness of sgAHs up-dosing, symptoms will persist in 45–60% of adult CU patients, especially in those with CSU, dermographic urticaria, and CholU.10,25,42 While a systematic review showed that sgAHs were more effective than placebo in CIndU, many patients still did not reach full control.23 This highlights the need for additional therapies in refractory cases, termed antihistamine-refractory CU.
Omalizumab, a monoclonal anti-IgE antibody, has revolutionized CSU management and is now an established second-line therapy for CSU that is antihistamine-refractory.1 Omalizumab binds free IgE, which down-regulates cell-surface IgE receptors (FcεRIs), leading to decreased mast cell activation and histamine release.3 In antihistamine-refractory CSU, 150–300 mg of subcutaneous omalizumab monthly has demonstrated high symptom control rates in those aged ≥12 years, both in clinical trials and real-world practice.1,26 Moreover, a recent meta-analysis suggests possible safety and efficacy in CSU patients <12 years.53 Up-dosing to 450–600 mg monthly can be attempted for those who do not respond to standard dosing after 3–6 months.28 While omalizumab is not FDA- and EMA-approved for CIndU, it has been used off-label in all major subtypes of CIndU subtypes with promising outcomes.1,10 Studies have shown that omalizumab can help manage resistant cases of ColdU, dermographism, contact urticaria, solar urticaria, DPU, and CholU.1,10,14 For example, one study of patients with severe antihistamine-refractory dermographic urticaria found that omalizumab therapy led to marked reduction in whealing and improved quality of life.23 Similar findings were reported in a study on DPU.10 Thus, for antihistamine-refractory CIndU, off-label use of omalizumab can be considered. In fact, many CU specialists routinely prescribe omalizumab for severe CIndU, given the high response rates across subtypes.10
Despite the efficacy of omalizumab in CU, up to 30% of patients will require third-line treatments, particularly older patients, females, those with type IIb CSU, and those with low serum IgE levels.2,20,41 In these cases, the use of cyclosporine, a calcineurin inhibitor immunosuppressant, is often recommended in order to suppress mast cell activation.1 Cyclosporine, combined with sgAHs, can induce remission in many omalizumab-resistant CSU patients, but side effects must be monitored.1 Cyclosporine treatment is usually started at a dose of 2.5–3 mg/kg divided into two daily doses and then titrated down to the lowest effective dose.20,29,30 Once a patient has been on cyclosporine for more than 12 months, they should be transitioned to a safer off-label medication given its nephrotoxicity and effect on blood pressure.26,30 Cyclosporine is also contraindicated in patients with chronic kidney disease and previous malignancy.30 In addition to CSU, cyclosporine has also been used successfully in some cases of CIndU, but data is limited.54
Short courses of systemic corticosteroids can be given to manage flares, but long-term use is not recommended to manage CU.1,55 Many CU patients have received a course of systemic corticosteroids to manage an acute CU exacerbation, with the number exceeding 73% in those with mixed CSU and CIndU.5
Beyond pharmacologic treatments, management must be individualized to the CU subtype as well. This is where differentiating CSU from CIndU, and identifying the subtype of CIndU, impacts clinical decisions.
Trigger Avoidance
In CIndU, unlike CSU, avoidance of the offending stimulus can significantly reduce symptoms.1 Patients should be educated about their triggers and how to minimize exposure. For example, patients with ColdU should avoid sudden total-body cold exposure, especially swimming in cold water.34 Epinephrine autoinjectors should be prescribed for patients with ColdU, especially those with any history of systemic reactions, but they are under-prescribed in practice, potentially leading to life threatening complications.22 For solar urticaria, sun protection is critical.49,50 Some patients with solar urticaria benefit from phototherapy desensitization under medical supervision.10,26 Patients with DPU should be advised to avoid sustained pressure, like tight clothing and prolonged standing; however, trigger avoidance is very challenging for these patients.24,26 Body-warming activities should be avoided in CholU, but complete trigger avoidance is a challenge in CholU much like in DPU.47 Those with vibratory urticaria should avoid tasks involving intense vibration, such as the use of jackhammers.11 Aquagenic urticaria patients can be advised to apply a barrier oil before exposure to water.17
Subtype-Specific Assessment
Patient reported outcomes measures (PROMs) are patient perceptions of their health status.56 Such perceptions are the only currently available tool to assess response to treatment among patients with CU and are critical for decision-making.56
Many PROMs have been developed and validated to assess CSU, angioedema, and CIndU for this purpose (Table 2).56 There are two main PROMs for CU patients: the urticaria activity score (UAS) and the urticaria control test (UCT).56 The UAS is the recommended gold standard in guidelines to assess CSU activity which is supported its documented usefulness in many clinical trials as a primary or secondary endpoint.56 The UAS reports the number of hives and the severity of itch, which are the two important component symptoms of CSU.56 Each component is rated on a scale 0–3, and the scores are summed to derive the UAS.56
The UCT is often more suitable for use in the clinical setting and is also suitable for CIndU.31,56,57 This is a four-item questionnaire which queries about physical symptoms, impact on quality of life, treatment effectiveness, and symptom control over the past four weeks.56
Subtype-Specific Therapies
Additional treatments are available for certain CU subtypes (Table 2). For CholU, anticholinergic agents, in addition to sgAHs, have been used off-label with varying success.12,23 Anecdotally, beta-blockers like propranolol have been reported to help CholU in some cases, but are not standard therapy.12 For severe antihistamine-refractory CholU, omalizumab has shown benefit, but more studies are needed.12,23 Montelukast, a leukotriene receptor antagonist, can be considered as an adjunctive therapy in CSU or CIndU for an additive improvement; however, evidence for benefit is low.26,42,58 In refractory DPU, some studies support the use of anti-inflammatory agents such as dapsone or colchicine, but evidence is also anecdotal.23,24 Cyclosporine, as mentioned, can be effective for DPU and other physical subtypes of refractory CU.1,54
While avoidance of triggers is not possible in those with CSU, known general aggravants should be avoided, such as NSAIDs, which can exacerbate urticaria in 30% of CSU patients.1 Moreover, if CSU is associated with an underlying autoimmune disease, such as thyroid disease, treating that condition might result in some improvement.37 For patients with refractory CSU and demonstrated autoantibodies, adding immunosuppressants like cyclosporine can be considered earlier, given the immune-driven nature.43 However, biologic therapies targeting IgE and mast cells, such as omalizumab, should be considered first.3 Three hundred mg of subcutaneous dupilumab, a monoclonal IL-4Rα antibody, every 2 weeks has been suggested to be an effective off-label treatment for CSU that fails first-, second-, and third-line therapies.20 Efficacy of dupilumab was demonstrated in a randomized controlled trial (LIBERTY-CSU CUPID Study A) mainly for omalizumab-naïve patients.59 Dupilumab may be particularly beneficial for those with autoallergic CSU and/or comorbid type 2 diseases (eg, atopic dermatitis).60 Efficacy in CIndU subtypes, such as ColdU and CholU, is currently being evaluated in clinical trials (NCT04681729, NCT03749148).60 Selective Bruton’s tyrosine kinase (BTK) inhibitors, such as fenebrutinib, remibrutinib, and rilzabrutinib, selectively block mast cell signalling by targeting BTK, downstream of the FcεRI.60 Clinical trial data (NCT03137069, REMIX-1/REMIX-2, RILECSU) suggest efficacy in CSU, and they may have a role in all CSU endotypes and in those with autoimmune comorbidities.21,60–62 According to a systematic review, omalizumab, dupilumab, remibrutinib, and cyclosporine are most effective to treat CU amongst immunomodulators.63 Dupilumab and remibrutinib have recently been FDA-approved for management of antihistamine-refractory CSU.64,65
Emerging Therapies
The treatment landscape for CU is evolving and several new treatments are being developed, especially for CSU.1 Potential treatments in development include: barzolvolimab and biologics targeting IL-17 and IL-23.60
Barzolvolimab decreases the number of mast cells via inhibition of the tyrosine kinase receptor KIT and may be effective for CSU and/or CIndU.60,66 In fact, a single 3 mg/kg dose was shown to rapidly reduce disease burden in those with antihistamine-refractory ColdU or symptomatic dermographism in a phase 1b clinical trial (NCT04538794).60,66 Barzolvolimab has also been shown to be effective for antihistamine-refractory CSU at ≥1.5 mg/kg every 4 weeks (NCT04538794).60,66 In case series studies, secukinumab (anti-IL-17) and tildrakizumab (anti-IL-23) reduced UAS scores in patients with omalizumab-refractory CSU.60,67,68 These therapies are not yet standard, but they herald a future where treatment can be personalized based on CU endotype.
Conclusion
Distinguishing CIndU from CSU is a fundamental step in the evaluation of patients with CU. While a CSU diagnosis requires ruling out all triggers, CIndU requires the identification of specific triggers through history and provocation testing.1 Clinical patterns, such as the timing of wheals, presence of physical stimuli, and duration of lesions, provide critical clues to the specific diagnosis.1 Correct classification guides management because, while patients with CIndU benefit from targeted trigger avoidance counseling and adjustments in therapy around anticipated exposures, CSU management focuses more on systemic control of mast cell activity and addressing underlying autoimmunity.1 In practice, up to 30% of CSU patients have concomitant CIndU and require a combination of approaches.1,4,5,10 In these cases, diagnosis may be particularly challenging and should be guided by history and provocation testing for suspected triggers. It is important to keep in mind that the presence of one inducible trigger on history does not exclude concomitant CSU or the presence of other triggers. Patients with CIndU who remain symptomatic despite guideline-based therapy and trigger avoidance should be re-evaluated for the presence of CSU and/or other triggers.
Treatment principles overlap, and EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline-based therapies, such as sgAHs and omalizumab, can be applied to achieve complete symptom control in most patients, regardless of the CU subtype.1,26,54 Careful observation, a detailed history, and personalized testing help optimize care. Recognition of an inducible trigger allows patients to practice avoidance, which can dramatically improve quality of life and disease control.22 Meanwhile, CSU often requires earlier initiation of immunomodulatory therapy, especially for type IIb CSU.43 While CU can be managed by sgAHs or omalizumab in most patients, amongst those with CSU, 45–60% are refractory to sgAHs and 30% are refractory to omalizumab.2,20,25,41,42 Emerging therapies, such as dupilumab, BTK inhibitors, and KIT inhibitors, may provide additional options for patients with antihistamine- or omalizumab-refractory disease.60 Moreover, the therapeutic landscape is rapidly evolving and phenotype differentiation will likely play an even larger role in the future, with the introduction of endotype-specific therapies. In summary, disease control can be achieved in most CU patients through a detailed history, focused provocation tests, and guideline-driven therapy.
Consent for Publication
Written consent was obtained from patients, or their legal guardians if applicable, for publication of all images included in this manuscript.
Acknowledgments
The authors thank the Canadian Dermatology Foundation and the Fonds de recherche du Québec for funding this research.
Funding
This work is funded by the Canadian Dermatology Foundation and the Fonds de recherche du Québec.
Disclosure
EN has been a speaker or consultant, or has received investigator-initiated research funding from AbbVie, Arcutis, Bausch Health, Boehringer Ingelheim International, Bristol Myers Squibb, Galderma, Janssen, LEO Pharma, Medexus, Novartis Pharmaceuticals, Pfizer, Sanofi Genzyme, Sun Pharmaceuticals, Eli Lilly, and UCB. EN is the founder of Montreal Derm FilEZ website, which is a non-profit educational resource. M.B.-S. is a consultant for Novartis and Sanofi. The other authors declare no conflicts of interest.
References
1. Kolkhir P, Gimenez-Arnau AM, Kulthanan K, Peter J, Metz M, Maurer M. Urticaria. Nat Rev Dis Primers. 2022;8(1):61. doi:10.1038/s41572-022-00389-z
2. Bizjak M, Kosnik M. Key differences between chronic inducible and spontaneous urticaria. Front Allergy. 2024;5:1487831. doi:10.3389/falgy.2024.1487831
3. Kaplan AP, Gimenez-Arnau AM, Saini SS. Mechanisms of action that contribute to efficacy of omalizumab in chronic spontaneous urticaria. Allergy. 2017;72(4):519–15. doi:10.1111/all.13083
4. Goncalo M, Gimenez-Arnau A, Al-Ahmad M, et al. The global burden of chronic urticaria for the patient and society. Br J Dermatol. 2021;184(2):226–236. doi:10.1111/bjd.19561
5. Ornek Ozdemir S, Kuteyla Can P, Degirmentepe EN, Cure K, Singer R, Kocaturk E. A comparative analysis of chronic inducible urticaria in 423 patients: clinical and laboratory features and comorbid conditions. J Eur Acad Dermatol Venereol. 2024;38(3):513–520. doi:10.1111/jdv.19637
6. Schettini N, Corazza M, Schenetti C, Pacetti L, Borghi A. Urticaria: a Narrative Overview of Differential Diagnosis. Biomedicines. 2023;11(4):1096. doi:10.3390/biomedicines11041096
7. Sanchez-Borges M, Gonzalez-Aveledo L, Caballero-Fonseca F, Capriles-Hulett A. Review of Physical Urticarias and Testing Methods. Curr Allergy Asthma Rep. 2017;17(8):51. doi:10.1007/s11882-017-0722-1
8. Nobles T, Muse ME, Schmieder GJ. Dermatographism. StatPearls. 2025;2025:1.
9. Stepaniuk P, Vostretsova K, Kanani A. Review of cold-induced urticaria characteristics, diagnosis and management in a Western Canadian allergy practice. Allergy Asthma Clin Immunol. 2018;14:85. doi:10.1186/s13223-018-0310-5
10. Munoz M, Kiefer LA, Pereira MP, Bizjak M, Maurer M. New insights into chronic inducible urticaria. Curr Allergy Asthma Rep. 2024;24(8):457–469. doi:10.1007/s11882-024-01160-y
11. Pozderac I, Lugovic-Mihic L, Artukovic M, Stipic-Markovic A, Kuna M, Fercek I. Chronic inducible urticaria: classification and prominent features of physical and non-physical types. Acta Dermatovenerol Alp Pannonica Adriat. 2020;29(3):141–148.
12. Fukunaga A, Oda Y, Imamura S, Mizuno M, Fukumoto T, Washio K. Cholinergic Urticaria: subtype Classification and Clinical Approach. Am J Clin Dermatol. 2023;24(1):41–54. doi:10.1007/s40257-022-00728-6
13. Radonjic-Hoesli S, Hofmeier KS, Micaletto S, Schmid-Grendelmeier P, Bircher A, Simon D. Urticaria and Angioedema: an Update on Classification and Pathogenesis. Clin Rev Allergy Immunol. 2018;54(1):88–101. doi:10.1007/s12016-017-8628-1
14. Bizjak M, Aerts O, Pesque D, et al. Contact Urticaria and Related Conditions: clinical Review. Contact Dermatitis. 2025;93(2):87–107. doi:10.1111/cod.14794
15. Imamura S, Oda Y, Fukumoto T, et al. Solar urticaria: clinical characteristics, treatment effectiveness, long-term prognosis, and QOL status in 29 patients. Front Med Lausanne. 2024;11:1328765. doi:10.3389/fmed.2024.1328765
16. Vethachalam S, Persaud Y. Contact Urticaria. StatPearls. 2025;2025:1.
17. Rothbaum R, McGee JS. Aquagenic urticaria: diagnostic and management challenges. J Asthma Allergy. 2016;9:209–213. doi:10.2147/JAA.S91505
18. Rujitharanawong C, Kulthanan K, Tuchinda P, Chularojanamontri L, Metz M, Maurer M. A Systematic Review of Aquagenic Urticaria-Subgroups and Treatment Options. J Allergy Clin Immunol Pract. 2022;10(8):2154–2162. doi:10.1016/j.jaip.2022.04.033
19. Kaplan AP. Angioedema. World Allergy Organ J. 2008;1(6):103–113. doi:10.1097/WOX.0b013e31817aecbe
20. Zhu C, BinJadeed H, Gabrielli S, et al. Prevalence of omalizumab-resistant chronic urticaria and real-world effectiveness of dupilumab in patients with omalizumab-refractory chronic urticaria: a single-centre experience. Clin Exp Dermatol. 2024;49(10):1227–1231. doi:10.1093/ced/llae145
21. Gimenez-Arnau A, Ferrucci S, Ben-Shoshan M, et al. Rilzabrutinib in Antihistamine-Refractory Chronic Spontaneous Urticaria: the RILECSU Phase 2 Randomized Clinical Trial. JAMA Dermatol. 2025;161(7):679–687. doi:10.1001/jamadermatol.2025.0733
22. Bizjak M, Kosnik M, Dinevski D, et al. Adrenaline autoinjector is under-prescribed in typical cold urticaria patients living in tropical climate countries. Qatar Med J. 2022;2022(2):19. doi:10.5339/qmj.2022.fqac.19
23. Dressler C, Werner RN, Eisert L, Zuberbier T, Nast A, Maurer M. Chronic inducible urticaria: a systematic review of treatment options. J Allergy Clin Immunol. 2018;141(5):1726–1734. doi:10.1016/j.jaci.2018.01.031
24. Kulthanan K, Ungprasert P, Tuchinda P, Chularojanamontri L, Charoenpipatsin N, Maurer M. Delayed Pressure Urticaria: a Systematic Review of Treatment Options. J Allergy Clin Immunol Pract. 2020;8(6):2035–2049e5. doi:10.1016/j.jaip.2020.03.004
25. Sanchez-Borges M, Ansotegui IJ. Second generation antihistamines: an update. Curr Opin Allergy Clin Immunol. 2019;19(4):358–364. doi:10.1097/ACI.0000000000000556
26. Zuberbier T, Abdul Latiff AH, Abuzakouk M, et al. The international EAACI/GA(2)LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy. 2022;77(3):734–766. doi:10.1111/all.15090
27. Agache I, Akdis CA, Akdis M, et al. EAACI Biologicals Guidelines-Omalizumab for the treatment of chronic spontaneous urticaria in adults and in the paediatric population 12-17 years old. Allergy. 2022;77(1):17–38. doi:10.1111/all.15030
28. Kocaturk E, Deza G, Kiziltac K, Gimenez-Arnau AM. Omalizumab Updosing for Better Disease Control in Chronic Spontaneous Urticaria Patients. Int Arch Allergy Immunol. 2018;177(4):360–364. doi:10.1159/000491530
29. Bernstein JA, Lang DM, Khan DA, et al. The diagnosis and management of acute and chronic urticaria: 2014 update. J Allergy Clin Immunol. 2014;133(5):1270–1277. doi:10.1016/j.jaci.2014.02.036
30. Kulthanan K, Chaweekulrat P, Komoltri C, et al. Cyclosporine for Chronic Spontaneous Urticaria: a Meta-Analysis and Systematic Review. J Allergy Clin Immunol Pract. 2018;6(2):586–599. doi:10.1016/j.jaip.2017.07.017
31. Weller K, Podder I, Salman A, Gimenez-Arnau AM, Neisinger S, Altrichter S. Clinical Evaluation and Outcome Measures of Chronic Spontaneous Urticaria and Chronic Inducible Urticaria. J Allergy Clin Immunol Pract. 2025. doi:10.1016/j.jaip.2025.07.008
32. Munoz M, Schoepke N, Altrichter S, et al. Development of the symptomatic dermographism quality of life questionnaire. Clin Transl Allergy. 2025;15(2):e70038. doi:10.1002/clt2.70038
33. Ruft J, Asady A, Staubach P, et al. Development and validation of the Cholinergic Urticaria Quality-of-Life Questionnaire (CholU-QoL). Clin Exp Allergy. 2018;48(4):433–444. doi:10.1111/cea.13102
34. Prosty C, Gabrielli S, Le M, et al. Prevalence, Management, and Anaphylaxis Risk of Cold Urticaria: a Systematic Review and Meta-Analysis. J Allergy Clin Immunol Pract. 2022;10(2):586–596e4. doi:10.1016/j.jaip.2021.10.012
35. Berberi G, Maazi M, Prosty C, et al. Health-Related Quality of Life in Chronic Urticaria: a Systematic Review and Meta-Analysis. J Allergy Clin Immunol Pract. 2025. doi:10.1016/j.jaip.2025.03.049
36. Kolkhir P, Bonnekoh H, Metz M, Maurer M. Chronic Spontaneous Urticaria: a Review. JAMA. 2024;332(17):1464–1477. doi:10.1001/jama.2024.15568
37. Kolkhir P, Metz M, Altrichter S, Maurer M. Comorbidity of chronic spontaneous urticaria and autoimmune thyroid diseases: a systematic review. Allergy. 2017;72(10):1440–1460. doi:10.1111/all.13182
38. Balp MM, Halliday AC, Severin T, et al. Clinical Remission of Chronic Spontaneous Urticaria (CSU): a Targeted Literature Review. Dermatol Ther. 2022;12(1):15–27. doi:10.1007/s13555-021-00641-6
39. Netchiporouk E, Sasseville D, Moreau L, Habel Y, Rahme E, Ben-Shoshan M. Evaluating Comorbidities, Natural History, and Predictors of Early Resolution in a Cohort of Children With Chronic Urticaria. JAMA Dermatol. 2017;153(12):1236–1242. doi:10.1001/jamadermatol.2017.3182
40. Prosty C, Gabrielli S, Mule P, et al. Cold urticaria in a pediatric cohort: clinical characteristics, management, and natural history. Pediatr Allergy Immunol. 2022;33(3):e13751. doi:10.1111/pai.13751
41. Bracken SJ, Abraham S, MacLeod AS. Autoimmune Theories of Chronic Spontaneous Urticaria. Front Immunol. 2019;10:627. doi:10.3389/fimmu.2019.00627
42. Lang DM. Chronic Urticaria. N Engl J Med. 2022;387(9):824–831. doi:10.1056/NEJMra2120166
43. Kolkhir P, Munoz M, Asero R, et al. Autoimmune chronic spontaneous urticaria. J Allergy Clin Immunol. 2022;149(6):1819–1831. doi:10.1016/j.jaci.2022.04.010
44. Kolkhir P, Kovalkova E, Chernov A, et al. Autoimmune Chronic Spontaneous Urticaria Detection with IgG Anti-TPO and Total IgE. J Allergy Clin Immunol Pract. 2021;9(11):4138–4146e8. doi:10.1016/j.jaip.2021.07.043
45. Bernstein JA, Ansotegui I, Asero R, et al. Diagnostic testing for chronic spontaneous urticaria with or without angioedema: the do’s, don’t and maybe’s. World Allergy Organ J. 2025;18(7):101068. doi:10.1016/j.waojou.2025.101068
46. Sella JA, Ferriani MPL, Melo JML, et al. Type I and type IIb autoimmune chronic spontaneous urticaria: using common clinical tools for endotyping patients with CSU. J Allergy Clin Immunol Glob. 2023;2(4):100159. doi:10.1016/j.jacig.2023.100159
47. Maurer M, Fluhr JW, Khan DA. How to Approach Chronic Inducible Urticaria. J Allergy Clin Immunol Pract. 2018;6(4):1119–1130. doi:10.1016/j.jaip.2018.03.007
48. Diaz VL, Gribbons KB, Yazdi-Nejad K, et al. Cold Urticaria Syndromes: diagnosis and Management. J Allergy Clin Immunol Pract. 2023;11(8):2275–2285. doi:10.1016/j.jaip.2023.05.040
49. Botto NC, Warshaw EM. Solar urticaria. J Am Acad Dermatol. 2008;59(6):909–20;quiz921–2. doi:10.1016/j.jaad.2008.08.020
50. Syed HA, Crane JS, Harris BW, Schlessinger J. Solar Urticaria. StatPearls. 2025;2025:1.
51. McSweeney SM, Kloczko E, Chadha M, et al. Systematic review of the clinical characteristics and natural history of solar urticaria. J Am Acad Dermatol. 2023;89(1):138–140. doi:10.1016/j.jaad.2023.01.039
52. Xiao X, Xue P, Shi Y, et al. The efficacy and safety of high-dose nonsedating antihistamines in chronic spontaneous urticaria: a systematic review and meta-analysis of randomized clinical trials. BMC Pharmacol Toxicol. 2023;24(1):23. doi:10.1186/s40360-023-00665-y
53. Alomari O, Ozceker D, Mokresh ME, et al. Omalizumab in pediatric chronic spontaneous urticaria: a systematic review and meta-analysis of efficacy and safety. Pediatr Allergy Immunol. 2025;36(6):e70132. doi:10.1111/pai.70132
54. Matos AL, Figueiredo C, Goncalo M. Differential Diagnosis of Urticarial Lesions. Front Allergy. 2022;3:808543. doi:10.3389/falgy.2022.808543
55. Chu X, Wang J, Ologundudu L, et al. Efficacy and Safety of Systemic Corticosteroids for Urticaria: a Systematic Review and Meta-Analysis of Randomized Clinical Trials. J Allergy Clin Immunol Pract. 2024;12(7):1879–1889e8. doi:10.1016/j.jaip.2024.04.016
56. Bernstein JA, Apfelbacher C, Chu DK, Schneider L, Saini SS, Ben Shoshan M. Patient-Reported Outcome Measures in Chronic Spontaneous Urticaria, Angioedema, and Atopic Dermatitis. J Allergy Clin Immunol Pract. 2024;12(10):2583–2590. doi:10.1016/j.jaip.2024.08.021
57. Kocaturk E, Can PK, Akbas PE, et al. Management of chronic inducible urticaria according to the guidelines: a prospective controlled study. J Dermatol Sci. 2017;87(1):60–69. doi:10.1016/j.jdermsci.2017.02.283
58. Rayner DG, Liu M, Chu AWL, et al. Leukotriene receptor antagonists as add-on therapy to antihistamines for urticaria: systematic review and meta-analysis of randomized clinical trials. J Allergy Clin Immunol. 2024;154(4):996–1007. doi:10.1016/j.jaci.2024.05.026
59. Maurer M, Casale TB, Saini SS, et al. Dupilumab Reduces Urticaria Activity, Itch, and Hives in Patients with Chronic Spontaneous Urticaria Regardless of Baseline Serum Immunoglobulin E Levels. Dermatol Ther. 2024;14(9):2427–2441. doi:10.1007/s13555-024-01231-y
60. Zuberbier T, Ensina LF, Gimenez-Arnau A, et al. Chronic urticaria: unmet needs, emerging drugs, and new perspectives on personalised treatment. Lancet. 2024;404(10450):393–404. doi:10.1016/S0140-6736(24)00852-3
61. Metz M, Gimenez-Arnau A, Hide M, et al. Remibrutinib in Chronic Spontaneous Urticaria. N Engl J Med. 2025;392(10):984–994. doi:10.1056/NEJMoa2408792
62. Metz M, Sussman G, Gagnon R, et al. Fenebrutinib in H(1) antihistamine-refractory chronic spontaneous urticaria: a randomized phase 2 trial. Nat Med. 2021;27(11):1961–1969. doi:10.1038/s41591-021-01537-w
63. Chu AWL, Oykhman P, Chu X, et al. Comparative efficacy and safety of biologics and systemic immunomodulatory treatments for chronic urticaria: systematic review and network meta-analysis. J Allergy Clin Immunol. 2025;156(4):1008–1023. doi:10.1016/j.jaci.2025.06.004
64. Mullard A. FDA approves BTK inhibitor for chronic hives. Nat Rev Drug Discov. 2025;24(11):815. doi:10.1038/d41573-025-00165-0
65. Wedi B. Biologic and small molecule therapies in chronic spontaneous urticaria: an update. Curr Opin Allergy Clin Immunol. 2025;25(5):418–425. doi:10.1097/ACI.0000000000001095
66. Maurer M, Metz M, Anderson J, et al. Anti-KIT Barzolvolimab for Chronic Spontaneous Urticaria. Allergy. 2025;80(8):2178–2186. doi:10.1111/all.16598
67. Sabag DA, Matanes L, Bejar J, et al. Interleukin-17 is a potential player and treatment target in severe chronic spontaneous urticaria. Clin Exp Allergy. 2020;50(7):799–804. doi:10.1111/cea.13616
68. Bonnekoh H, Kiefer L, Buttgereit T, et al. Anti-IL-23 treatment with tildrakizumab can be effective in omalizumab-refractory chronic spontaneous urticaria: a case series. J Allergy Clin Immunol Pract. 2023;11(8):2578–2580e1. doi:10.1016/j.jaip.2023.05.019
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.