Back to Journals » Journal of Pain Research » Volume 12
Cervical intradural disc herniation with Brown-Séquard syndrome: case report and literature review
Authors Rong Y, Wang J, Sui T, Liu W, Luo Y, Cai W
Received 7 January 2019
Accepted for publication 25 June 2019
Published 31 July 2019 Volume 2019:12 Pages 2403—2410
DOI https://doi.org/10.2147/JPR.S200632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Yuluo Rong,* Jiaxing Wang,* Tao Sui, Wei Liu, Yongjun Luo, Weihua Cai
Department of Orthopaedics, First Affiliated Hospital of Nanjing Medical University, Nanjing 210029, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Objective: To report a rare case of cervical intradural disc herniation (IDH) with Brown-Séquard syndrome and to review the related literature.
Methods: Pathogenesis, preoperative diagnosis, and the surgical technique are discussed, and previous literature reports are reviewed.
Results: A 44-year-old woman complained of weakness of the left upper and lower extremities and paresthesias in the right limbs after a bicycle ride 3 days earlier. She had a history of neck pain for 2 years prior. CT showed obvious ossification of the posterior longitudinal ligament (OPLL), and MRI revealed C3-7 disc herniations, with a positive “halo sign” around the herniated C4/5. We performed emergency decompression through anterior cervical corpectomy, and vertebrotomy decompression and fusion. At review 3 months after surgery, the patient’s neck pain was markedly relieved, and motor strength in the limbs had improved. At 1 year after surgery, she had recovered completely.
Conclusion: Cervical IDH is a rare condition that may be related to the traumatic inflammatory response and OPLL. Relatively rare imaging features such as the hawk-beak sign, halo sign, Y sign, and epidural gas sign could help in preoperative diagnosis. Prompt anterior cervical decompression is the preferred treatment for this condition.
Keywords: cervical intradural disc herniation, Brown-Séquard syndrome, ossification of posterior longitudinal ligament, cerebrospinal fluid leakage, surgical treatment
Introduction
Intradural disc herniation (IDH) is a rare condition that mostly occurs in the lumbar spine (92%); about 5% of cases occur in the thoracic spine, and 3% in the cervical spine.1,2 More than 100 cases of lumbar IDHs have been reported since the first description by Dandy et al in 1942.3 The first case of cervical IDH was reported in 1959.4 The pathogenetic mechanism of cervical IDH is unclear, but ossification of the posterior longitudinal ligament (OPLL) and trauma are probably involved.5
In 2010, Hsieh et al6 reported a patient with OPLL who developed cervical IDH after spinal manipulation. Wang et al and Baudracco et al have reported spontaneous cervical IDH in patients with OPLL.5,7 In this article, we report a woman with OPLL who developed cervical IDH and Brown-Séquard syndrome following minor trauma. We also briefly review all cases of cervical IDH reported to date (Table 1). Written informed consent was obtained from the patient to publish the case details and the accompanying images. Institutional approval is not required to publish anonymized patient data.
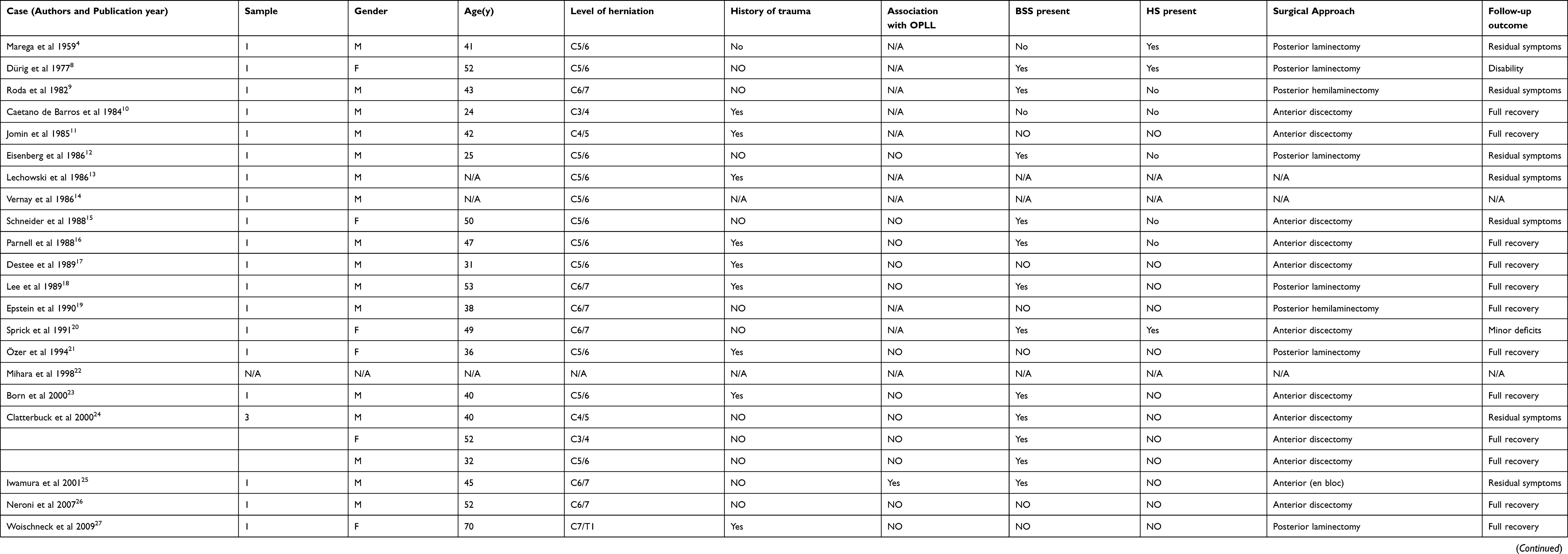 |
Table 1 Summary of reported cases with intradural cervical disc herniation |
Case report
A 44-year-old woman complained of weakness of the left upper and lower limbs and paresthesias in the right limbs after a bumpy bicycle ride 3 days earlier. She had a history of neck pain for 2 years prior. On physical examination, she had flaccid paralysis of the left limbs, with grade 0 muscle strength; sensation was normal. On the right side, she had grade 4 muscle strength, and total loss of pain and temperature sensation. There was no sphincter dysfunction. CT revealed C3-7 intervertebral disc herniations and OPLL (Figure 1). MRI showed C3-7 intervertebral disc herniations (most prominent at C3/4, C4/5, and C5/6) and marked compression of the dural sac (Figure 2). A “halo” was seen around the C4/5 level protrusion (Figure 2A). Based on the clinical features and imaging findings, our diagnosis was 1) cervical disc herniations (C3-7, with cervical IDH at C4/5); 2) Brown-Séquard syndrome (cervical myelopathy); and 3) cervical OPLL.
 |
Figure 1 Preoperative CT. (A, B) CT-scan sagittal reconstruction (bone windows). (A, D) CT-scan transverse cut at the C4-5 level. CT revealed disc herniation at C4-5 (arrow) and ossification of the posterior longitudinal ligament. Note: N/A indicates not available.Abbreviations: OPLL, ossification of posterior longitudinal ligament; BSS, Brown-Séquard syndrome; HS, Horner syndrome. |
 |
Figure 2 Preoperative MRI. (A) T2-weighted images and b: T1-weighted images. Sagittal image of the cervical spine reveals large disc herniation at C3-C7 and C4-C5 with severe spinal cord compression. A “halo” of CSF isointensity surrounds the herniated disc (arrow). (C, D) Axial T2-weighted image of the cervical spine reveals large, central disc herniation at C4-C5 (arrow) with severe spinal cord compression and surrounding edema. |
Surgery was performed under general anesthesia, with the aim of C3-6 anterior cervical discectomy and fusion (ACDF) or C4 anterior cervical corpectomy and fusion (ACCF) + C5/6 ACDF. The classic anterior cervical approach was used. C5/6 was completely decompressed and an artificial bone cage (DePuy Synthes, MA, USA) was installed and filled. The C4/5 intervertebral disc was resected. The nucleus pulposus had protruded into the dura mater, and its removal was difficult because of tight adhesions between the dura and the posterior longitudinal ligament. Therefore, subtotal resection of C4 vertebra body was performed. After the nucleus pulposus was removed, a small break in the dura mater, with exudation of cerebrospinal fluid (CSF), was apparent (Figure 3A). The posterior longitudinal ligament was dissected free of the dura and resected. The dural tear was closed. A titanium mesh (Weigao, ShanDong, China) was then installed and filled with autologous bone. The vertebral body was fixed with a titanium plate and screws (Weigao, ShanDong, China).
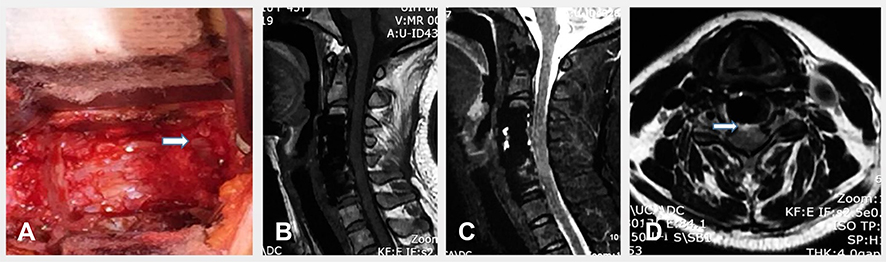 |
Figure 3 Intraoperative photograph and sagittal and axial magnetic resonance images obtained 3 months postoperatively. (A) A small breach in the dura mater (white arrow) was seen after the removal of the nucleus pulposus. There was minimal cerebral spinal fluid leakage. T1-weighted (B) and T2 weighted (C, D) MR images reveal satisfactory segmental decompression and no compression of the dural sac (whitarrow). |
Postoperatively, the patient had obvious relief of symptoms. At review 3 months after surgery, muscle strength was normal but mild sensory abnormalities persisted. The shallow feeling of the right limb skin was slightly abnormal. Imaging showed stable internal fixation, satisfactory decompression of the surgical segment, and no compression of the dural sac (Figure 3B–D). At 1 year after surgery, the patient had recovered completely, with normal muscle strength on both sides and no paresthesias. Figure 4 shows the preoperative and follow-up radiographs.
 |
Figure 4 Preoperative and postoperative follow-up radiographs; (A) lateral radiograph of the cervical spine shows absence of the physiological curvature, with degenerative changes in the cervical vertebrae. (B) Radiograph obtained 3 days after surgery shows partial restoration of the cervical curvature. (C) Radiograph obtained 3 months after surgery shows no displacement of internal fixation. (D) Radiograph obtained 1 year after surgery shows stable internal fixation. |
Discussion
Disc herniation usually occurs in the anterior epidural space; protrusion into the intradural space is unusual, especially for cervical disc herniation.34 Cervical IDH is most common at C5/6, followed by C6/7.35 Clinical manifestations include quadriplegia, paresthesias, and ataxia and, less often, radiculopathy.35,19 Brown-Séquard syndrome (hemicord syndrome) and Horner syndrome are rare presenting symptoms.6,7,36
Definitive diagnosis of IDH depends on demonstration of dural rupture during surgery. MRI may show intramedullary signals or intradural filling defects, but dural rupture is difficult to identify. However, four rare imaging signs should raise suspicion of cervical IDH: the hawk-beak sign, the halo sign, the Y sign, and the epidural gas sign. The hawk-beak sign—an abrupt termination of the posterior longitudinal ligament on MRI—was first described by Choi et al.37 The halo sign presents as a rim of isointense signal in the CSF around the herniated disc in sagittal T2-weighted images.38 The Y sign is caused by the herniated intervertebral disc peeling the arachnoid away from the dura mater, creating a “Y” shape on sagittal MR images.39 The epidural gas sign (on CT) presents as gas in the epidural space.40 According to Yang et al1 the presence of the halo sign and the Y sign in MRI is strongly suggestive of cervical IDH. In our patient the halo sign was positive (Figure 2A).
Trauma and OPLL are believed to be important factors in the pathogenesis of IDH5 Adhesions between the posterior longitudinal ligament and the dura mater are common,35 and chronic adhesion may be the result of repeated trauma. Anatomical studies have demonstrated strong adhesions between the posterior longitudinal ligament and dura, with the C5/6 and C6/7 levels being most often involved;41 this is consistent with the levels involved in our patient. OPLL, which has high prevalence in Asians (~2.4%), most commonly affects the cervical spine.42 Mechanical irritation by the OPLL may lead to chronic inflammation of the adjacent dura mater, and subsequent scarring can result in adhesions between the dura and the posterior longitudinal ligament. The fragility of the dura mater and the posterior longitudinal ligament after adhesion is increased by stimulation. When this reaches to a certain extent, the protruding intervertebral disc may penetrate the posterior longitudinal ligament and the dura mater through accidental external force into the dura.
All previously reported patients were treated with surgery (Table 1), as it is the standard treatment for cervical IDH. Anterior surgery can directly enter the area of the diseased disc and facilitate removal of the protruding disc and repair of the dura. From previous reports, anterior bone graft fusion appears to be superior to posterior decompression (Table 1). Anterior discectomy is the preferred treatment because it directly addresses the problem.43 Vertebral resection may be required depending on the size and location of the compressed disc fragments and the degree of adhesion between the dura and the posterior longitudinal ligament. Our patient had OPLL and multisegment disc herniation, along with close adhesions between the posterior longitudinal ligament and the dura. We therefore chose discectomy and decompression plus subtotal corpectomy and bone graft fusion (ACDF + ACCF).
To summarize, cervical IDH is a rare condition, with pathogenesis probably related to the traumatic inflammatory response and OPLL. Preoperative diagnosis is difficult, but imaging signs such as the hawk-beak sign, halo sign, Y sign, and epidural gas sign can be useful indicators. Prompt anterior cervical decompression is the preferred treatment. In patients with cervical spine IDH accompanied by OPLL, the possibility of dural rupture should be kept in mind, adequate preoperative preparation made, and CSF leakage carefully looked for during surgery.
Ethical approval
Ethical approval was not required for this study.
Acknowledgments
This work was sponsored by the Wu Jieping Foundation (Grant No.320-2745-16-117).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yang HS, Oh YM, Eun JP. Cervical intradural disc herniation causing progressive quadriparesis after spinal manipulation therapy: a case report and literature review. Medicine. 2016;95(6):e2797. doi:10.1097/MD.0000000000004864
2. Madhugiri VS, Gundamaneni SK, Yadav AK, Sasidharan GM, Roopesh Kumar VR, Shankar Ganesh CV. Intradural thoracic disc presenting with radiculopathy. Neurol India. 2012;60(2):257–259. doi:10.4103/0028-3886.96435
3. Dandy WE. Serious complications of ruptured intervertebral discs. JAMA. 1942;474–475. doi:10.1001/jama.1942.02830230008002
4. Marega T, Komjanc G. Injury and hernia of the disk. Minerva Ortop. 1959;10:649–652.
5. Wang D, Wang H, Shen WJ. Spontaneous cervical intradural disc herniation associated with ossification of posterior longitudinal ligament. Case Rep Orthop. 2014;2014:256207. doi:10.1155/2014/256207
6. Hsieh JH, Wu CT, Lee ST. Cervical intradural disc herniation after spinal manipulation therapy in a patient with ossification of posterior longitudinal ligament: a case report and review of the literature. Spine (Phila Pa 1976). 2010;35(5):E149–E151. doi:10.1097/BRS.0b013e3181bee8a7
7. Baudracco I, Grahovac G, Russo VM. Spontaneous cervical intradural disc herniation presenting with Brown-Sequard and Horner’s syndrome: lesson learned from a very unique case. Eur Spine J. 2017;26(Suppl 1):218–221. doi:10.1007/s00586-017-5044-4
8. Durig M. Intradurale sequestration einer cervikalen diskoshernie. ein kasuistischer beitrag[J]. Arch Orthop Unfall Chir. 1977;87:151–157.
9. Roda JM, Gonzalez C, Blazquez MG, Alvarez MP, Arguello C. Intradural herniated cervical disc. Case report. Journal of neurosurgery. 1982;57:278–280.
10. Caetano de Barros A, Caetano de Barros M. Traumatic extradural and intradural herniation of cervical disk treated surgically. Surgical neurology. 1984;21:577–580.
11. Jomin M, Lesoin F, Wavreille A, Destee A, Gozet G. [Extra- and intradural cervical disk hernia. A case]. Revue du rhumatisme et des maladies osteo-articulaires. 1985;52:593–594.
12. Eisenberg RA, Bremer AM, Northup HM. Intradural herniated cervical disk: a case report and review of the literature. AJNR American journal of neuroradiology. 1986;7:492–494.
13. Lechowski S, Urbaniak J. [Intradural herniation of the intervertebral disk of the cervical segment of the spine]. Neurologia i neurochirurgia polska. 1986;20:589–591.
14. Vernay D, Rampon S, Fraysse P, Cheminat JC, Irthum B, Clavelou P. [Extra- and intradural cervical hernia. A new case]. Revue du rhumatisme et des maladies osteo-articulaires. 1986;53:403.
15. Schneider SJ, Grossman RG, Bryan RN. Magnetic resonance imaging of transdural herniation of a cervical disk. Surgical neurology. 1988;30:216–219.
16. Parnell AP. Cervical intradural disc protrusion. Journal of Neurology, Neurosurgery , and Psychiatry. 1988;51:1007.
17. Destee A, Lesoin F, Di Paola F, Warot P. Intradural herniated cervical disc associated with chiropractic spinal manipulation. Journal of Neurology, Neurosurgery , and Psychiatry. 1989;52:1113.
18. Lee ST, Cheng SY, Lui TN. Intradural rupture of cervical intervertebral disc. Spine (Phila Pa 1976). 1989;14:1412–1414.
19. Epstein NE, Syrquin MS, Epstein JA, Decker RE. Intradural disc herniations in the cervical, thoracic, and lumbar spine: report of three cases and review of the literature. Journal of spinal disorders. 1990;3:396–403.
20. Sprick C, Fegers S. [Intradural sequestration of cervical intervertebral disk displacement]. Der Nervenarzt. 1991;62:133–135.
21. Ozer AF, Ozek MM, Pamir MN, Zirh TA, Erzen C. Intradural rupture of cervical vertebral disc. Spine (Phila Pa 1976). 1994;19:843–845.
22. Mihara H. Intradural disc herniation in the cervical spine: a case report[J]. Kanto Seikei Saigai Gekagakkai. 1998;29:27–32.
23. Borm W, Bohnstedt T. Intradural cervical disc herniation. Case report and review of the literature. Journal of neurosurgery. 2000;92:221–224.
24. Clatterbuck RE, Belzberg AJ, Ducker TB. Intradural cervical disc herniation and Brown-Sequard's syndrome. Report of three cases and review of the literature. Journal of neurosurgery. 2000;92:236–240.
25. Iwamura Y, Onari K, Kondo S, Inasaka R, Horii H. Cervical intradural disc herniation. Spine (Phila Pa 1976). 2001;26:698–702.
26. Neroni M, Gazzeri R, Galarza M, Alfieri A. Intradural cervical disc herniation in a Klippel-Feil patient. Spine (Phila Pa 1976). 2007;32:E608–610.
27. Woischneck D, Schmitz B, Kapapa T. [First description of an intradural disc herniation at the C7-T1 level]. Zeitschrift fur Orthopadie und Unfallchirurgie. 2009;147:600–602.
28. Kansal R, Mahore A, Kukreja S. Cervical intradural disc herniation and cerebrospinal fluid leak. Neurology India. 2011;59:447–450.
29. Pan J, Li L, Qian L et al. Intradural cervical disc herniation: report of two cases and review of the literature. Spine (Phila Pa 1976). 2011;36:E1033–1037.
30. Warade AG, Misra BK. Spontaneous cervical intradural disc herniation. J Clin Neurosci. 2014;21:872–873.
31. Mitchell BD, Verla T, Reddy D, Winnegan L, Omeis I. Reliable Intraoperative Repair Nuances of Cerebrospinal Fluid Leak in Anterior Cervical Spine Surgery and Review of the Literature. World neurosurgery. 2016;88:252–259.
32. Lian F J, Chang C J. Cervical intradural disc herniation and intradural gas on CT scan[J]. Fu-Jen J Med.2016;14:39–44.
33. Gunasekaran A, de Los Reyes NKM, Walters J, Kazemi N. Clinical Presentation, Diagnosis, and Surgical Treatment of Spontaneous Cervical Intradural Disc Herniations: A Review of the Literature. World neurosurgery. 2018;109:275–284.
34. Brogna C, Lavrador JP, Patel S, et al. Posterior longitudinal ligament and its implications in intradural cervical disc herniation: case report and review of the literature. Surg Neurol Int. 2018;9:119. doi:10.4103/sni.sni_32_18
35. Guan Q, Xing F, Long Y, Xiang Z. Cervical intradural disc herniation: a systematic review. J Clin Neurosci. 2018;48:1–6. doi:10.1016/j.jocn.2017.10.024
36. Ma H, Kim I. Horner syndrome associated with a herniated cervical disc: a case report. Korean J Spine. 2012;9(2):108–110. doi:10.14245/kjs.2012.9.2.108
37. Choi JY, Lee WS, Sung KH. Intradural lumbar disc herniation–is it predictable preoperatively? A report of two cases. Spine J. 2007;7(1):111–117. doi:10.1016/j.spinee.2006.02.025
38. Börm W, Bohnstedt T. Intradural cervical disc herniation. Case report and review of the literature. J Neurosurg. 2000;92(2 Suppl):221–224.
39. Sasaji T, Horaguchi K, Yamada N, Iwai K. The specific sagittal magnetic resonance imaging of intradural extra-arachnoid lumbar disc herniation. Case Rep Med. 2012;2012:383451. doi:10.1155/2012/383451
40. Hidalgo-Ovejero AM, Garcia-Mata S, Izco-Cabezon T, Garralda-Galarza G, Martinez-Grande M. Intradural disc herniation associated with epidural gas. Spine (Phila Pa 1976). 1998;23(2):281–283.
41. Yildizhan A, Pasaoglu A, Okten T, Ekinci N, Aycan K, Aral O. Intradural disc herniations pathogenesis, clinical picture, diagnosis and treatment. Acta Neurochir (Wien). 1991;110(3–4):160–165.
42. Min JH, Jang JS, Lee SH. Clinical results of ossification of the posterior longitudinal ligament (OPLL) of the thoracic spine treated by anterior decompression. J Spinal Disord Tech. 2008;21(2):116–119. doi:10.1097/BSD.0b013e318060091a
43. Rong Y, Luo Y, Liu W, Gong F, Tang P, Cai W. Clinical effects of the bridge-type ROI-C interbody fusion cage system in the treatment of cervical spondylosis with osteoporosis. Clin Interv Aging. 2018;13:2543–2551. doi:10.2147/CIA.S182969
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.