Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Certain Metabolic Syndrome Component Combinations are Linked to Increased Risk of Hypogonadism in Taiwanese Men
Authors Hong YH, Hung KC ![]() , Lin CL
, Lin CL ![]() , Hung CL
, Hung CL ![]() , Tu SK, Yang DH
, Tu SK, Yang DH ![]() , Liao CC
, Liao CC ![]()
Received 9 August 2024
Accepted for publication 7 June 2025
Published 18 June 2025 Volume 2025:18 Pages 1977—1984
DOI https://doi.org/10.2147/DMSO.S483344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Yu-Han Hong,1 Kuang-Chen Hung,2– 5 Chih-Li Lin,6 Chia-Lien Hung,7 Shih-Kai Tu,1 Deng-Ho Yang,5,7– 9 Chun-Cheng Liao1,5– 7
1Department of Family Medicine, Taichung Armed Forces General Hospital, Taichung, Taiwan; 2Department of Surgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 3School of Medicine, National Sun Yat-sen University, Kaohsiung, Taiwan; 4College of Health Sciences, Central Taiwan University of Science and Technology, Taichung, Taiwan; 5School of Medicine, National Defense Medical Center, Taipei, Taiwan; 6Institute of Medicine, Chung Shan Medical University, Taichung, Taiwan; 7Department of Medical Education and Research, Taichung Armed Forces General Hospital, Taichung, Taiwan; 8Department of Medical Laboratory Science and Biotechnology, Central Taiwan University of Science and Technology, Taichung, Taiwan; 9Division of Rheumatology/Immunology/Allergy, Department of Internal Medicine, Taichung Armed Forces General Hospital, Taichung, Taiwan
Correspondence: Chun-Cheng Liao, Family Medicine Department, Taichung Armed Forces General Hospital, 348, Sec. 2, Zhongshan Road, Taiping Dist, Taichung, 411228, Taiwan, Tel +886423934191#525239 ; +886970703499, Fax +88623934191, Email [email protected]
Purpose: This study examined the association between specific combinations of metabolic syndrome (MS) components and the risk of hypogonadism in Taiwanese men.
Patients and Methods: We retrospectively analyzed 6,986 men who underwent health screening from 2009 to 2017. MS was defined as meeting at least three of five criteria: waist circumference (W), triglycerides (T), high-density lipoprotein cholesterol (H), fasting glucose (F), and blood pressure (B). Hypogonadism was defined as total testosterone < 300 ng/dL. Differences in MS component prevalence between men with and without hypogonadism were compared. Logistic regression adjusted for age and body mass index was used to assess associations.
Results: Among all participants, 6,221 (89.0%) had hypogonadism. The prevalence of MS components was significantly higher in this group (p < 0.001). The risk of hypogonadism increased with the number of MS compon ents. Notably, the combinations F-H-W, F-H-B-W, and F-T-H-B-W were associated with significantly higher odds of hypogonadism.
Conclusion: Specific MS component combinations are strongly associated with increased hypogonadism risk in Taiwanese men. These findings suggest that MS composition, not just its presence, should be considered in evaluating testosterone deficiency.
Keywords: metabolic syndrome, hypogonadism, blood pressure, fasting blood glucose, high-density lipoprotein
Introduction
Metabolic syndrome (MS) is a cluster of disorders that includes hypertension, dyslipidemia, and insulin resistance, which are often accompanied by abdominal (visceral) obesity. MS poses significant public health challenges in noncommunicable disease management, especially because global obesity has become increasingly prevalent.1,2 According to the reports of Nutrition and Health Surveys in Taiwan (NAHSIT) in 1993–1996 and 2005–2008, MS prevalence markedly increased from 13.6% to 25.5%.3 Thus, the risk of developing serious health problems, such as nonalcoholic fatty liver disease, chronic kidney disease, erectile dysfunction, cardiovascular diseases (CVD), stroke, and type 2 diabetes mellitus (T2DM), could also significantly increase.4–14 In addition, MS increases the risk of mental disorders, such as depression.15
Male hypogonadism is a condition in which the testes do not produce sufficient testosterone due to a deficiency in the pituitary/hypothalamus or testicular function. Testosterone is a vital hormone for sexual, cognitive, and physical functions and growth. Male hypogonadism can lead to various issues, including sexually related (for example, infertility and erectile dysfunction) and even physiologically related (eg, obesity, osteoporosis, and muscle loss) issues. Thus, this condition can also increase the risk of T2DM, CVD, and MS.10,11,16–18
The correlation between male hypogonadism and MS has been widely reported.6,18–20 However, few studies have focused on the potential relationship between various combinations of MS components and the different levels of risk they pose for hypogonadism. In previous study, high triglycerides combined with high waist circumference (HTGW) may be a risk factor for hypogonadism. This suggests that abdominal or subcutaneous fat may contribute to the occurrence of hypogonadism in men.21 Inspired by the findings of a previous investigation that analyzed the association between diverse combinations of metabolic syndrome (MS) and both cardiovascular disease (CVD) and overall mortality in a cohort of older adults in Taiwan, we adopted a similar methodology in our current study to explore the impact of various MS components on hypogonadism.9
This study aimed to investigate variations in the relationship between hypogonadism and the number and different combinations of MS components.
Subjects and Methods
Study Population
This retrospective cohort study used data collected from the MJ Health Screening Center, a large private health examination institute in Taiwan, spanning from 2009 to 2017. Considering that the institute offers self-paid health examination services in the major districts of the country, with a general cost of 200–730 USD (17 USD for the specific measurement of serum testosterone), the demographic characteristics of the included patients were considered representative of the general population in Taiwan.22
We included a total of 6986 male participants regardless of whether they had underlying medical conditions. Individuals who did not have enough data to assess MS status or testosterone levels, female individuals, or male individuals aged >65 years were excluded from this study.
Participants were classified into two groups: those with and without hypogonadism. All data used in this research were obtained through authorization from the MJ Health Research Foundation (authorization code: MJHRF2019016A) and were approved by the Tri-Service General Hospital Institutional Review Board (approval number: A202005160). This study was performed in accordance with the principles of the Declaration of Helsinki. Any conclusions or interpretations presented in this paper do not reflect the views of the MJ Health Research Foundation. Written informed consent was obtained from all study participants prior to their health examination, allowing the use of their data in the analysis. The MJ Health Research Foundation removed all personal identification information to maintain anonymity throughout the research process.
Definition of MS and Hypogonadism
Hypogonadism, as defined by the 2018 American Urological Association guideline, is characterized by total testosterone levels < 300 ng/dL.23
According to the 2005 American Heart Association/National Heart Lung Blood Institute guideline, male MS is confirmed when a patient has at least three of the following five criteria: 1) obesity with a waist circumference (WC) ≥ 90 cm, 2) triglyceride (TG) ≥ 150 mg/dL, 3) high-density lipoprotein (HDL) < 40 mg/dL, 4) systolic blood pressure (BP) ≥ 130 mmHg or diastolic BP ≥ 85 mmHg, and 5) fasting blood glucose (FG) ≥ 100 mg/dL.24
Clinical data and baseline parameters such as body mass index (BMI), BP, WC, HDL, TG, and FG were collected. The center used the chemiluminescent microparticle immunoassay (ARCHITECT i2000) for measuring testosterone, the Homogeneous Direct method (TOSHIBA C8000) for HDL cholesterol, the GPO-POD-ESPT method (TOSHIBA C8000) for TG, and the HK.G-6-PD.NADP method (TOSHIBA C8000) for FG.
The waistline was measured at the midpoint between the top of the hip bone and the bottom of the ribs, without clothing that could interfere with the measurement. The patient should be fasting, standing in a relaxed position with arms naturally hanging down, and the waistline should be measured at the end of exhalation.
Statistical Analysis
Independent samples t-tests were conducted to compare age, BMI, and MS criteria (WC, TG, HDL, FG, and BP) between participants with and without hypogonadism. We also used chi-square test to conduct correlation analysis for the MS criteria between the two groups. While evaluating the relationships between the MS criteria and hypogonadism, we calculated unadjusted and adjusted odds ratios (OR) through logistic regression. The logistic regression model adjusted for age and BMI. All statistical data were analyzed using the SPSS version 22.0 (IBM, Armonk, NY, USA) software, and a p-value of <0.05 was considered statistically significant.
Results
Baseline Characteristics of the Participants
Table 1 summarizes basic patient characteristics. Of the 6986 participants recruited in this study, 6221 had hypogonadism and 765 had no hypogonadism. According to the mean values of each parameter, BMI, MS criteria (WC, TG, HDL, FG, and BP), and testosterone were significantly different between the groups with and without hypogonadism.
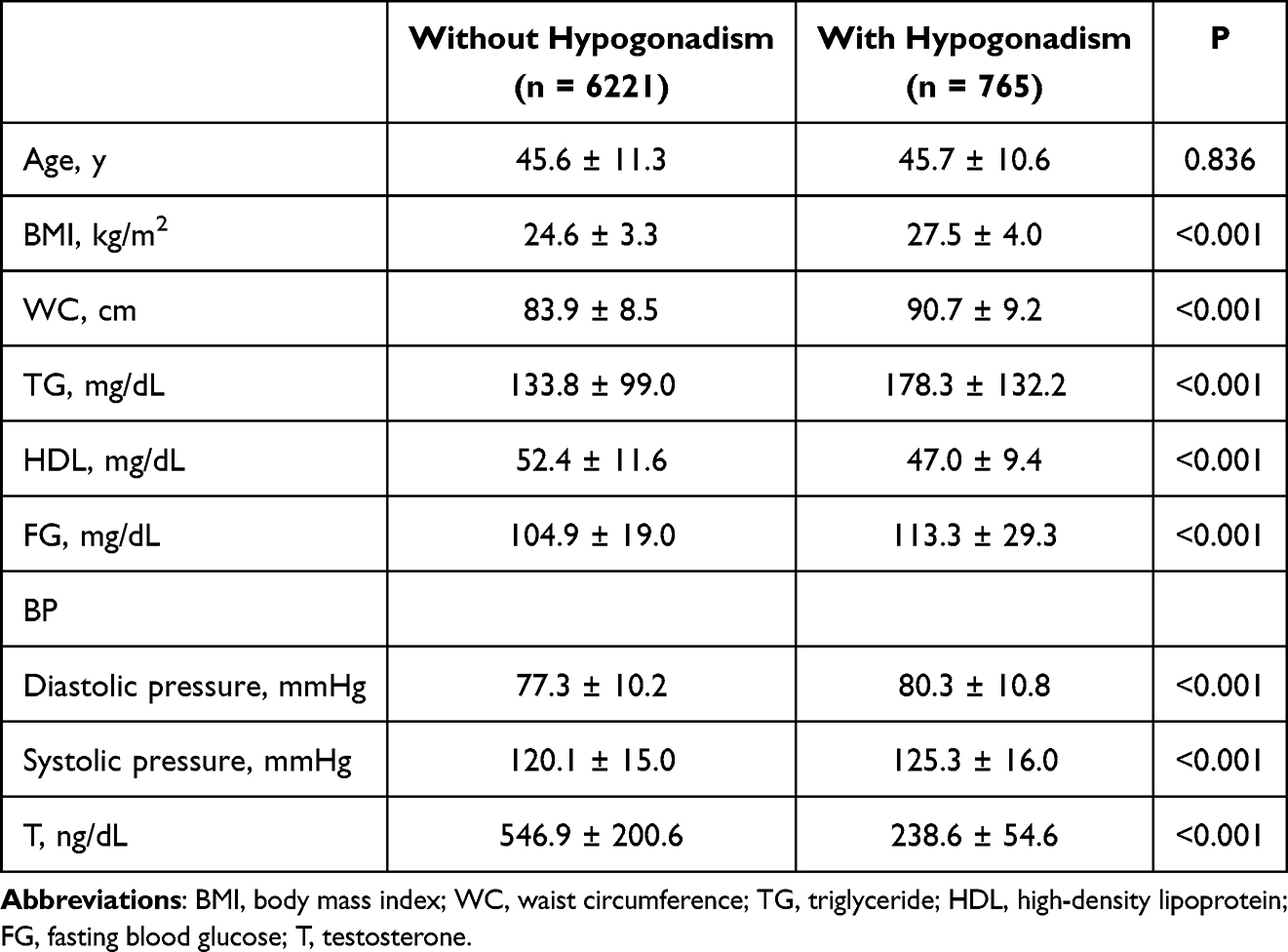 |
Table 1 Characteristics of Participants with and without Hypogonadism |
Correlations Between MS Criteria and Hypogonadism
As shown in Table 2, the distribution of MS criteria (WC, TG, HDL, FG, and BP) was significantly different between participants with and without hypogonadism (p < 0.001). Participants with hypogonadism were more likely to have FG (73.8%), WC (50.6%), TG (50.4%), BP (47.2%), or HDL (20.8%) compared to those without hypogonadism.
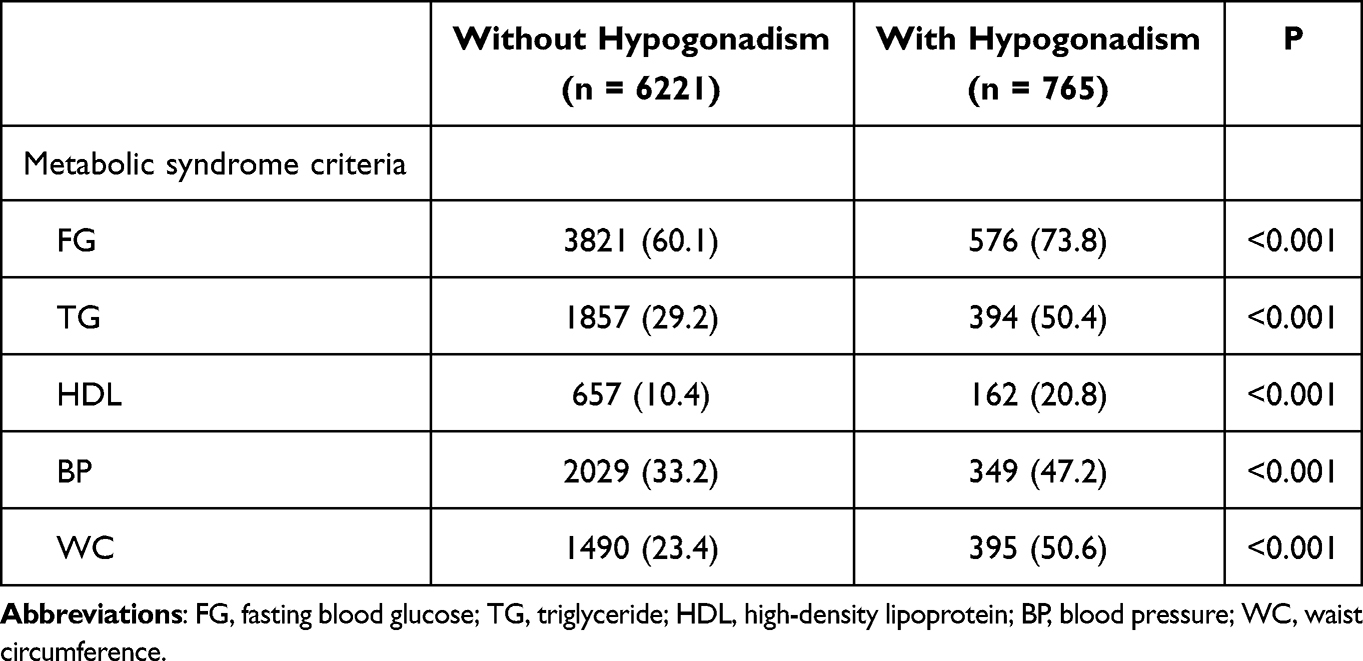 |
Table 2 Incidence of Hypogonadism in Each Metabolic Syndrome (MS) Criteria |
Risk of Hypogonadism According to the MS Criteria
Table 3 presents the association of each of the MS criteria and the items consisting of combined MS criteria as well as without MS, with the risk of hypogonadism according to the unadjusted logistic regression analysis. Among all MS criteria, WC had the highest correlation with the risk of hypogonadism, followed by TG, HDL, FG, and BP. Regarding the combined MS criteria, participants with 3, 4, and 5 MS criteria had higher risk of hypogonadism than those without MS.
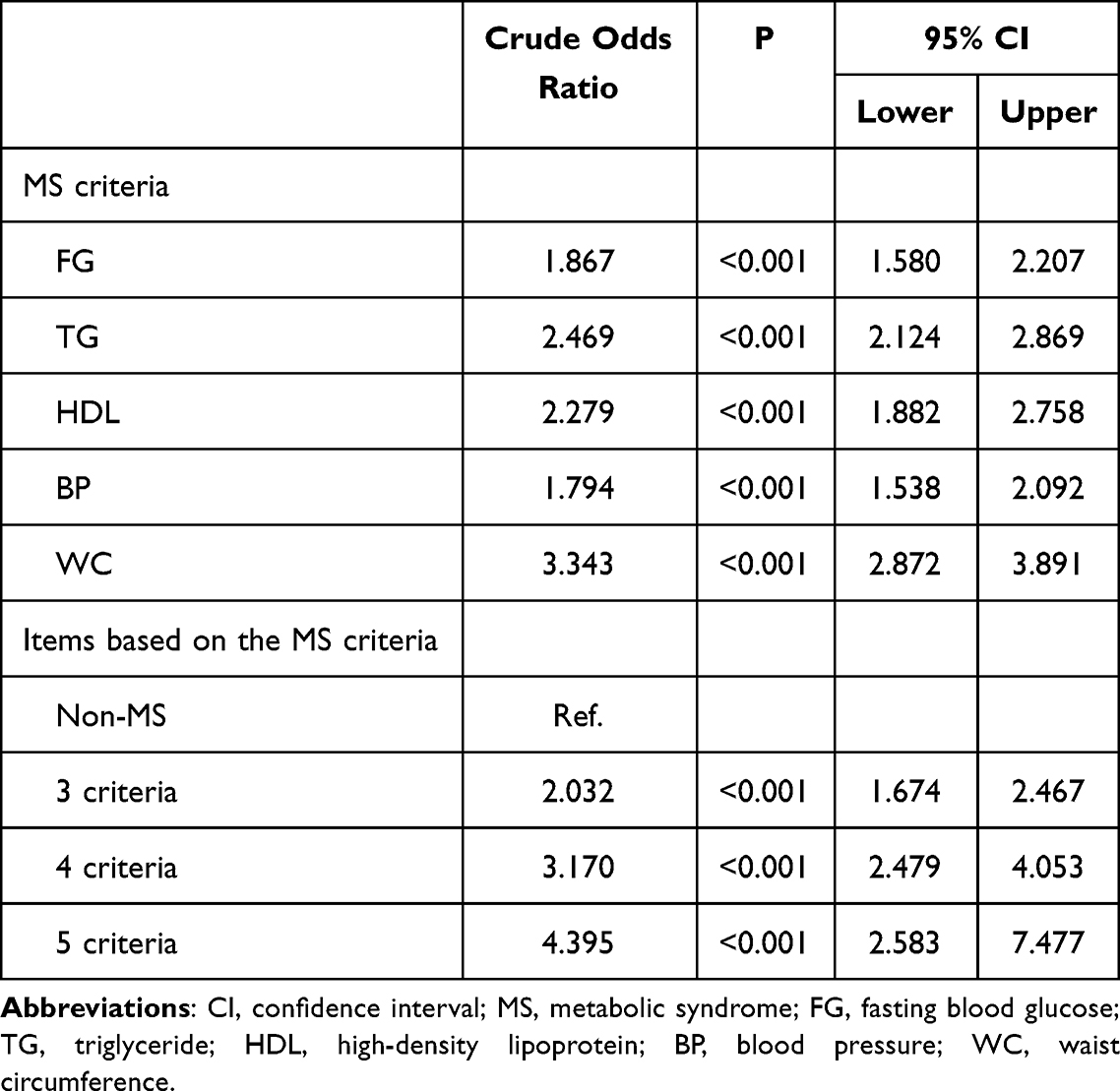 |
Table 3 Crude Odds Ratio for Hypogonadism of Each MS Criteria and Based on MS Criteria |
Table 4 shows the association of each of the MS criteria and the items consisting of combined MS criteria, as well as without MS, with the risk of hypogonadism after adjustment for age and BMI. The results revealed that WC showed the highest risk of hypogonadism, followed by TG, HDL, FG and BP. In combined MS criteria, compared with those without MS, patients with 5 MS criteria had the highest risk for hypogonadism, followed by those with 4 and 3 MS criteria sequentially. Thus, the risk of hypogonadism increased as the MS criteria increased.
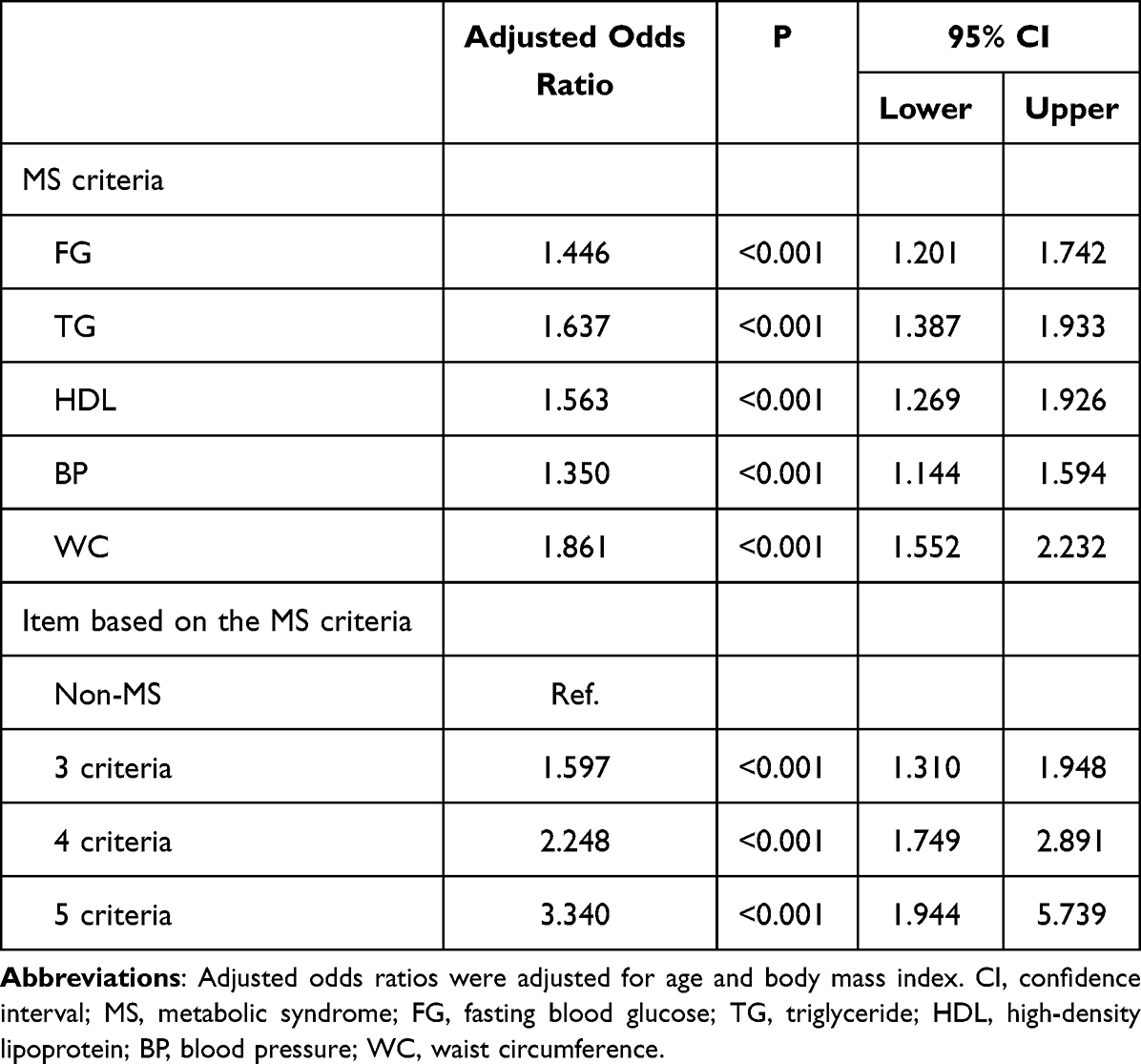 |
Table 4 Adjusted Odds Ratio for Hypogonadism of Each MS Criteria and Based on MS Criteria |
Finally, we analyzed the correlation between the MS criteria in a multiple logistic regression model after adjustment for age and BMI, as shown in Figure 1, wherein FG, WC, BP, HDL, and TG stand for F, W, B, H, and T, respectively. Model 1 reveals that participants with F-H-W had the highest risk for hypogonadism, followed by those with T-B-W, F-B-W, and F-T-B consecutively (p < 0.05). In model 2, participants with F-H-B-W, F-T-H-B, and F-T-B-W had higher risks for hypogonadism than those without MS. In model 3, participants with F-T-H-B-W also had a higher risk for hypogonadism than those without MS.
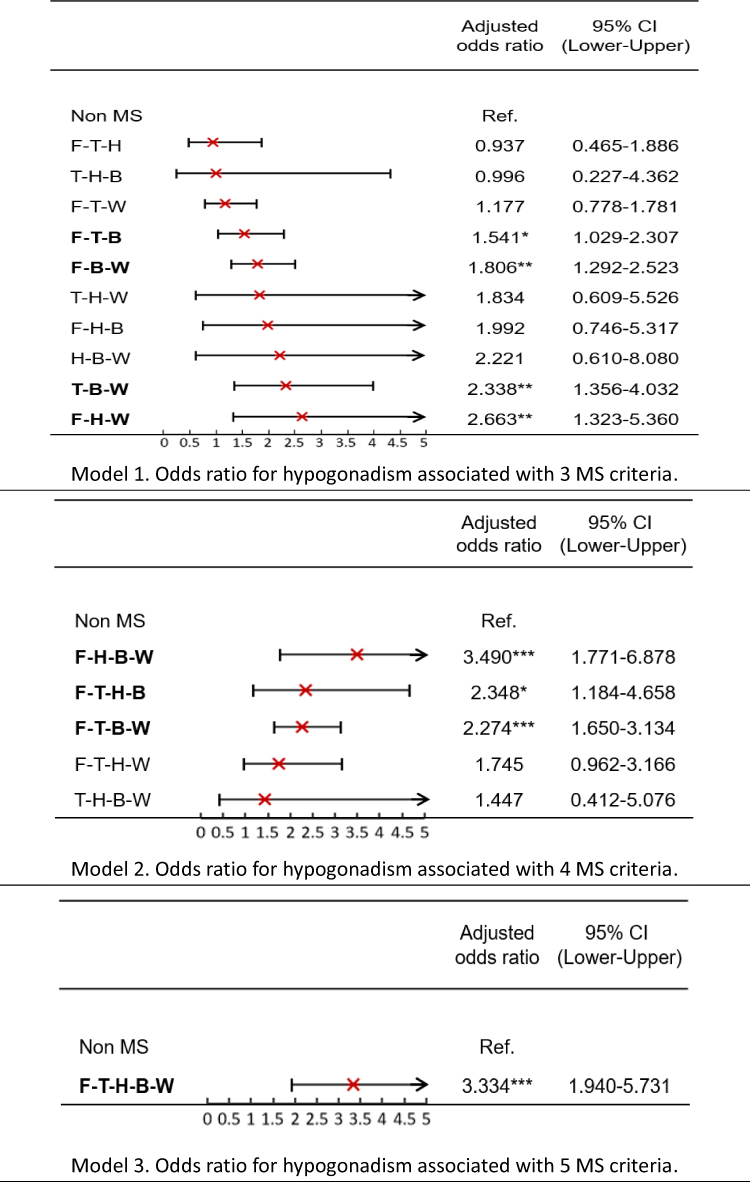 |
Figure 1 Odds ratio for hypogonadism associated with 3, 4, or 5 MS criteria. Abbreviations: CI, confidence interval; MS, metabolic syndrome; F, fasting blood gluose; T, triglyceride; H, high-density lipoprotein; B, blood pressure; W, waist circumference. Notes: Adjusted odds ratios (ORs) were adjusted for age and body mass index. *p < 0.05, **p < 0.01, ***p < 0.001. |
Discussion
Our study contributes to the growing body of literature exploring the complex relationship between metabolic syndrome (MS) components and testosterone levels. Rather than examining MS as a binary condition, we investigated how specific combinations of MS components relate to the likelihood of biochemical hypogonadism (defined as total testosterone <300 ng/dL). This approach provides a more nuanced perspective that may better inform clinical risk stratification. Wen et al9 were the first to propose that different component factors of MS show varying risks of CVD. The presence of specific combinations of MS factors influenced the level of risk of mortality in patients with MS.9 In line with these findings, we explored whether different MS factors lead to the same risk of hypogonadism.
In Figure 1, model 1 shows that MS with F-H-W had the highest OR for the development of hypogonadism compared to other combined MS components. However, F-T-H, T-H-B, F-T-W, T-H-W, F-H-B, and H-B-W did not show significant differences in hypogonadism risk when compared with participants without Ms. In model 2, participants with F-H-B-W were more susceptible to hypogonadism than those without Ms, whereas those with F-T-H-W and T-H-B-W did not show significant differences in hypogonadism when compared with those without Ms. In Model 3, the F-T-H-B-W phenotype was associated with a significantly increased risk of biochemical hypogonadism relative to individuals without metabolic syndrome (adjusted OR: 3.334, p < 0.05). Intriguingly, as depicted in Figure 1, the adjusted OR for F-H-B-W (OR: 3.490) astonishingly surpassed that for F-T-H-B-W (OR: 3.334).
These findings are consistent with previous reports. A meta-analysis by Corona et al19 and data from Brand et al20 both demonstrated that men with MS tend to have lower total testosterone levels, and that testosterone declines with increasing MS burden. Our results reinforce this association and further identify abdominal obesity (waist circumference) as the most strongly correlated individual component (adjusted OR: 1.861). This is consistent with previous Taiwanese data25 and the broader literature indicating that visceral adiposity is inversely associated with testosterone and sex hormone–binding globulin (SHBG) levels.26 Mechanistically, low testosterone contributes to increased lipoprotein lipase activity and fatty acid uptake in adipocytes, which promotes further visceral fat accumulation and perpetuates MS features such as hypertriglyceridemia and insulin resistance.18 Excessive adiposity also increases aromatase activity—leading to peripheral conversion of testosterone to estradiol—and stimulates the release of pro-inflammatory cytokines (eg, IL-1β, TNF-α, IL-6), which suppress the hypothalamic–pituitary–gonadal axis and reduce testosterone production.27–29 While our study showed significant associations between specific MS patterns and low testosterone, we note several differences from prior studies, such as Brand et al.20 These differences may be attributable to population variation (ours being exclusively Taiwanese), differences in inclusion criteria (we excluded men over 65 years old and those with extreme outliers), and differing definitions of hypogonadism (Brand et al used 250–300 ng/dL, whereas we used <300 ng/dL).
Several limitations should be acknowledged. First, the retrospective and cross-sectional nature of this study limits our ability to draw causal inferences. However, we recognize that previous research has established plausible biological mechanisms for the bidirectional relationship between MS and low testosterone. Second, the use of self-paid health screening data may limit generalizability due to socioeconomic selection bias. Third, although we used a widely accepted biochemical cutoff (<300 ng/dL), the absence of clinical symptom data (eg, libido, erectile function) limits our ability to diagnose true clinical hypogonadism. Fourth, some participants may have been on testosterone replacement therapy or lipid-lowering agents, which could not be accounted for due to dataset limitations. Finally, although our laboratory used validated assays, the variability across immunoassay platforms underscores the need for standardized testosterone measurement protocols.30
Conclusion
In Taiwanese men, the presence of metabolic syndrome is associated with an increased risk of low testosterone. However, not all combinations of MS components confer the same risk. Specific patterns—particularly those involving F, W, low HDL, and T—were significantly associated with higher odds of hypogonadism. These findings suggest that assessing the composition of MS components, rather than simply counting their number, may improve risk stratification and early identification of men at higher risk for testosterone deficiency.
Acknowledgments
This study received assistance from the Department of Medical Education and Research, Taichung Armed Forces General Hospital. This research received no external TCAFGH-D-111011. All or part of the data used in this research were authorized by and received from the MJ Health Research Foundation (Authorization Code: MJHRF2021003A). Any interpretation or conclusion described in this paper does not represent the views of MJ Health Research Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):12. doi:10.1007/s11906-018-0812-z
2. Afshin A, et al. Health effects of overweight and obesity in 195 Countries over 25 Years. N Engl J Med. 2017;377(1):13–27.
3. Yeh CJ, Chang HY, Pan WH. Time trend of obesity, the metabolic syndrome and related dietary pattern in Taiwan: from NAHSIT 1993-1996 to NAHSIT 2005-2008. Asia Pac J Clin Nutr. 2011;20(2):292–300.
4. Lakka HM, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA. 2002;288(21):2709–2716. doi:10.1001/jama.288.21.2709
5. Kaur J. A comprehensive review on metabolic syndrome. Cardiol Res Pract. 2014;2014:943162. doi:10.1155/2014/943162
6. Wang C, Jackson G, Jones TH, et al. Low testosterone associated with obesity and the metabolic syndrome contributes to sexual dysfunction and cardiovascular disease risk in men with type 2 diabetes. Diabetes Care. 2011;34(7):1669–1675. doi:10.2337/dc10-2339
7. Hong Y, Jin X, Mo J, et al. Metabolic syndrome, its preeminent clusters, incident coronary heart disease and all-cause mortality--results of prospective analysis for the atherosclerosis risk in communities study. J Intern Med. 2007;262(1):113–122. doi:10.1111/j.1365-2796.2007.01781.x
8. Guize L, Thomas F, Pannier B, et al. All-cause mortality associated with specific combinations of the metabolic syndrome according to recent definitions. Diabetes Care. 2007;30(9):2381–2387. doi:10.2337/dc07-0186
9. Wen CJ, Lee YS, Lin WY, et al. The metabolic syndrome increases cardiovascular mortality in Taiwanese elderly. Eur J Clin Invest. 2008;38(7):469–475. doi:10.1111/j.1365-2362.2008.01965.x
10. Saad F. The role of testosterone in type 2 diabetes and metabolic syndrome in men. Arq Bras Endocrinol Metabol. 2009;53(8):901–907. doi:10.1590/S0004-27302009000800002
11. Corona G, Bianchini S, Sforza A, et al. Hypogonadism as a possible link between metabolic diseases and erectile dysfunction in aging men. Hormones. 2015;14(4):569–578. doi:10.14310/horm.2002.1635
12. Kupelian V, Shabsigh R, Araujo AB, et al. Erectile dysfunction as a predictor of the metabolic syndrome in aging men: results from the Massachusetts male aging study. J Urol. 2006;176(1):222–226. doi:10.1016/S0022-5347(06)00503-9
13. Paschos P, Paletas K. Non alcoholic fatty liver disease and metabolic syndrome. Hippokratia. 2009;13(1):9–19.
14. Prasad GV. Metabolic syndrome and chronic kidney disease: current status and future directions. World J Nephrol. 2014;3(4):210–219. doi:10.5527/wjn.v3.i4.210
15. Al-Khatib Y, Akhtar MA, Kanawati MA, et al. Depression and metabolic syndrome: a narrative review. Cureus. 2022;14(2):e22153. doi:10.7759/cureus.22153
16. Kumar P, Kumar N, Thakur D, et al. Male hypogonadism: symptoms and treatment. J Adv Pharm Technol Res. 2010;1(3):297–301. doi:10.4103/0110-5558.72420
17. Huhtaniemi I. Late-onset hypogonadism: current concepts and controversies of pathogenesis, diagnosis and treatment. Asian J Androl. 2014;16(2):192–202. doi:10.4103/1008-682X.122336
18. Pivonello R, Menafra D, Riccio E, et al. Metabolic disorders and male hypogonadotropic hypogonadism. Front Endocrinol. 2019;10:345. doi:10.3389/fendo.2019.00345
19. Corona G, Monami M, Rastrelli G, et al. Testosterone and metabolic syndrome: a meta-analysis study. J Sex Med. 2011;8(1):272–283. doi:10.1111/j.1743-6109.2010.01991.x
20. Brand JS, Rovers MM, Yeap BB, et al. Testosterone, sex hormone-binding globulin and the metabolic syndrome in men: an individual participant data meta-analysis of observational studies. PLoS One. 2014;9(7):e100409. doi:10.1371/journal.pone.0100409
21. Wang SK, Lee M-C, Hung C-L, et al. Association between hypertriglyceridemic waist phenotype and hypogonadism in Taiwanese adult men. PLoS One. 2022;17(3):e0265629. doi:10.1371/journal.pone.0265629
22. Zhong SR, Yang -H-H, Liao C-H, et al. Association between low serum testosterone and the development of metabolic syndrome in elderly Taiwanese men. Diabetes Metab Syndr Obes. 2021;14:99–106. doi:10.2147/DMSO.S282832
23. Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200(2):423–432. doi:10.1016/j.juro.2018.03.115
24. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and blood institute scientific statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
25. Hsu PS, Hung C-L, Tu S-K, et al. Waist circumference is more closely associated with hypogonadism than is hyperglycemia, independent of BMI in middle-aged men. J Diabetes Res. 2021;2021:1347588. doi:10.1155/2021/1347588
26. Gyawali P, Martin SA, Heilbronn LK, et al. Cross-sectional and longitudinal determinants of serum sex hormone binding globulin (SHBG) in a cohort of community-dwelling men. PLoS One. 2018;13(7):e0200078. doi:10.1371/journal.pone.0200078
27. Norata GD, Tibolla G, Seccomandi PM, et al. Dihydrotestosterone decreases tumor necrosis factor-alpha and lipopolysaccharide-induced inflammatory response in human endothelial cells. J Clin Endocrinol Metab. 2006;91(2):546–554. doi:10.1210/jc.2005-1664
28. Mohamad NV, Wong SK, Wan Hasan WN, et al. The relationship between circulating testosterone and inflammatory cytokines in men. Aging Male. 2019;22(2):129–140. doi:10.1080/13685538.2018.1482487
29. Malkin CJ, Pugh PJ, Jones RD, et al. The effect of testosterone replacement on endogenous inflammatory cytokines and lipid profiles in hypogonadal men. J Clin Endocrinol Metab. 2004;89(7):3313–3318. doi:10.1210/jc.2003-031069
30. Livingston M, Downie P, Hackett G, et al. An audit of the measurement and reporting of male testosterone levels in UK clinical biochemistry laboratories. Int J Clin Pract. 2020;74(11):e13607. doi:10.1111/ijcp.13607
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Clinically Related Factors of Hypertriglyceridemia in Patients with Bipolar Disorder in Anhui Province, China
Li J, Lei W, Wang Y, Wu Q
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2695-2705
Published Date: 7 August 2025
Longitudinal Associations Between Metabolic Risk Burden and the Cardio–Ankle Vascular Index (CAVI) in Japan Using Health-Check Cohort
Horibuchi Y, Aluariachy L, Yamaura R, Kasahara H, Tsugane S, Yamazaki T
Vascular Health and Risk Management 2026, 22:601750
Published Date: 8 May 2026