Back to Journals » International Journal of General Medicine » Volume 19
Cerebral Ventricular Dimensions in Patients with Heart Failure with Reduced Ejection Fraction (HFrEF): A Cross-Sectional MRI Study
Authors Alan B ![]()
Received 1 April 2026
Accepted for publication 28 June 2026
Published 9 July 2026 Volume 2026:19 603749
DOI https://doi.org/10.2147/IJGM.S603749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Bircan Alan
Bolu Abant Izzet Baysal University Medical Faculty, Department of Radiology, Merkez, Bolu, 14030, Turkey
Correspondence: Bircan Alan, Bolu Abant Izzet Baysal Medical Faculty, Department of Radiology, Gölköy Yerleşkesi, Merkez, Bolu, 14030, Tel +905324421951, Fax +903742534615, Email [email protected]
Background: The aim of this cross-sectional case-control study was to measure the cerebral ventricular diameters of patients with heart failure with reduced ejection fraction (HFrEF) using magnetic resonance imaging (MRI) and to investigate their differences compared to healthy controls, as well as their relationship with left ventricular ejection fraction (LVEF).
Methods: A total of 104 healthy volunteers and 104 patients with HFrEF (New York Heart Association [NYHA] class II–IV) were included in the study (mean age: 57.2 ± 8.4 vs. 59.7 ± 10.8 years, respectively; p = 0.007). In both groups, LVEF was measured using echocardiography, and cerebral ventricular diameters—including the bifrontal diameter (BFD), bihemispheric diameter (BHD), and frontal horn ratio (FHR)—were measured using MRI. Finally, the Evans index and the anteroposterior diameter of the lateral ventricle index (ALVI) were calculated.
Results: The BFD, FHR, ALVI, and Evans index were significantly higher in the HFrEF group than in the healthy control group (BFD: 37.30 ± 3.4 vs. 31.97 ± 2.2, p < 0.001; FHR: 0.32 ± 0.03 vs. 0.28 ± 0.01, p < 0.001; ALVI: 0.44 ± 0.04 vs. 0.38 ± 0.03, p < 0.001; Evans index: 0.27 ± 0.02 vs. 0.23 ± 0.01, p < 0.001). ROC curve analysis demonstrated high diagnostic and discriminatory performance for both indices in distinguishing HFrEF patients from healthy controls (AUC = 0.901 [95% CI: 0.859– 0.943], p < 0.001 for ALVI and AUC = 0.903 [95% CI: 0.862– 0.944], p < 0.001 for Evans index). Correlation analysis revealed that LVEF was significantly and negatively correlated with both the Evans index (r = − 0.550, p < 0.001) and ALVI (r = − 0.585, p < 0.001).
Conclusion: Cranial ventricular dimensions are significantly increased in patients with HFrEF compared to healthy controls, and these indices are inversely correlated with LVEF systolic impairment.
Keywords:
ALVI, Evans index, heart failure with reduced ejection fraction, cerebral ventricular diameters
Introduction
Heart failure, which is the inability of the heart to provide adequate circulation for the body’s needs, is a serious problem with increasing incidence and prevalence. In patients with heart failure, unrecognized cognitive decline and subclinical brain structural alterations can covertly impair daily self-care, thereby reducing quality of life and potentially increasing long-term healthcare costs. Patients with heart failure with reduced ejection fraction (HFrEF) are at risk of structural brain changes due to cerebral hypoperfusion. Many patients with HFrEF develop neurological dysfunction and cognitive deficits. Approximately 25–50% of patients with heart failure have cognitive deficits, such as difficulty in concentration, attention deficit, and memory impairment. Affected patients also have higher rehospitalization and mortality rates.1–5 Cranial ventriculomegaly may develop in adulthood as a result of late-onset congenital or other idiopathic pathologies or brain atrophy. The clinical presentation may be acute or chronic. The pathophysiology of the chronic form may be due to hypoxia or blood vessel changes.6
The fundamental role of bidirectional interactions between the heart and brain is increasingly recognized.7 Cardiac impulse control is a major regulatory factor in the regulation of interactions between cerebrospinal fluid (CSF) and the cardiovascular system. Cardiac impulses play a critical role in CSF circulation by controlling blood flow in cerebral vessels, particularly via mechanisms that optimize perfusion which may be severely impaired in cardiovascular diseases that reduce cerebral blood flow,8 such as advanced heart failure.
Studies have found an increase in the incidence of chronic adult hydrocephalus in heart patients with diseases such as ischemic heart disease and valve disease.9–12 However, little is known about the incidence and prevalence of hydrocephalus-like structural alterations in patients with HFrEF. We found no studies in English that evaluate differences in brain ventricular size in patients with HFrEF and its relationship with left ventricular functions.
Hence, this study aimed to investigate the differences in brain ventricular dimensions between patients with HFrEF and healthy controls, and to evaluate their relationship with left ventricular systolic impairment.
Materials and Methods
Patients
Approval for our single-center cross-sectional case-control study was obtained from the ethics committee of our university (2021/120), and the study was conducted in strict accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study. A total of 104 patients with heart failure with reduced ejection fraction (HFrEF) and New York Heart Association (NYHA) class II–IV heart failure were included in the study as a HFrEF group, with a mean age of 59.7 ± 10.8 years. A total of 104 age- and gender-matched healthy volunteers were also included in the study as a healthy control group, with a mean age of 57.2 ± 8.4 years. All participants in the HFrEF group had a documented diagnosis of heart failure (HF) at least six months before the study.
Additionally, all patients were on a stable, optimized medication regimen for at least one month before the study. In our protocol, the medication regimen was defined as “optimized” based on individual patient tolerance, contraindications, and real-world clinical status at the time of enrollment (2021–2022), rather than the strict achievement of maximum guideline-directed medical therapy (GDMT) target doses for all four drug classes. Comorbidities such as chronic kidney disease, borderline hypotension, hyperkalemia risk, and financial reimbursement bottlenecks during the active study period limited the full uptake of SGLT2 inhibitors and MRAs in a subset of our cohort.
HF diagnosis was based on clinical assessment, and the left ventricular ejection fraction (LVEF) was measured via two-dimensional echocardiography. The clinical assessment was categorized according to the New York Heart Association (NYHA) classification system, and the LVEF was calculated using the modified Simpson’s rule.13 Patients with LVEF ≤ 40% and NYHA classes II–IV were included in the study as the HFrEF group.
Exclusion criteria included: being over 70 years of age, having neurodegenerative diseases causing brain atrophy, having a previous diagnosis of dementia, having a psychiatric or other serious or life-threatening illness, having a history of stroke associated with the development of neurological signs or symptoms, having a current diagnosis of a depressive episode (ICD-10), having a history of psychoactive drug use, alcohol dependence (> 4 units/day), or severe head trauma, having a pacemaker or other implanted metal device, having a left ventricular ejection fraction (LVEF) of 41% or greater, and being classified as NYHA class I.
Images
Brain images were obtained using a 16-channel head array coil and a Signa Explorer 1.5-T scanner (GE Healthcare) magnetic resonance imaging (MRI) system. In this study, linear ventricular diameters (BFD, BHD, FHR, TIDS, ALVI, and Evans index) were evaluated on axial T2-weighted turbo spin-echo images (T2WI) without contrast media to provide the best CSF differentiation. Acquisition parameters for the T2-weighted sequence were chosen using a flip angle of 142°, an echo time (TE) of 108.5 ms, a repetition time (TR) of 6,259 ms, a bandwidth of 50 Hz/Px, and a field of view (FoV) of 220×220 mm, a slice thickness of 5.0 mm, an interslice gap of 1.0 mm, and a reconstruction matrix of 512 × 512, which generated an in-plane resolution of 0.4×0.4 mm.
Conversely, the callosal angle was calculated using reconstructed 3D T1-weighted MPRAGE images (slice thickness = 1.0 mm, no gap, reconstruction matrix = 256×256) subjected to N3 nonuniform intensity normalization and B1 inhomogeneity correction during post-processing.
Raw DICOM data were utilized for all evaluations. In order to minimize measurement bias, head tilt was corrected by aligning the plane parallel to the anterior commissure-posterior commissure (AC-PC) line. For unilateral measurements, the larger values between the left and right sides were systematically selected as the final representative diameter. The systematic evaluation of imaging studies and all manual linear measurements were performed by a senior radiologist who was completely blinded to the clinical data and group allocations of the participants to eliminate any potential observer bias. To ensure high measurement reproducibility and minimize error margins, all metrics were obtained using strictly standardized anatomical landmarks, as detailed below.
Lateral ventricle measurements were made at the level of the bilateral caudate nucleus. Third ventricle interventricular level was evaluated at the level of the foramen of Monro and the fourth ventricle at the pontomedullary junction level. The maximum measurement of the bifrontal diameter (BFD) was obtained by measuring the transverse diameters with a line drawn to the anterior corners of the frontal horns. The bihemispheric diameter (BHD) was measured along the bifrontal diameter line. The frontal horn ratio (FHR) was calculated by dividing the BFD by the BHD. The maximum transverse inner diameter of the skull (TIDS) was measured as the maximum width of the inner table of the cranium at the level of the foramens of Monro in the frontal horns.
The Evans index was calculated by dividing the BFD by the TIDS (Figure 1). The anteroposterior diameter of the lateral ventricle index (ALVI) was defined as the ratio of this lateral ventricle diameter to the maximal width of the anteroposterior inner diameter of the skull (along the cerebral falx) in the same plane (from the base of the skull to the roof of the skull, not covered by other regions such as the thalamus). We determined the axial section in the plane of the lateral ventricular body. We then measured the anteroposterior diameter of the left and right lateral ventricles in this axial section. The lateral ventricular diameter was defined as the larger of the two measured ventricular diameters (Figure 2).14
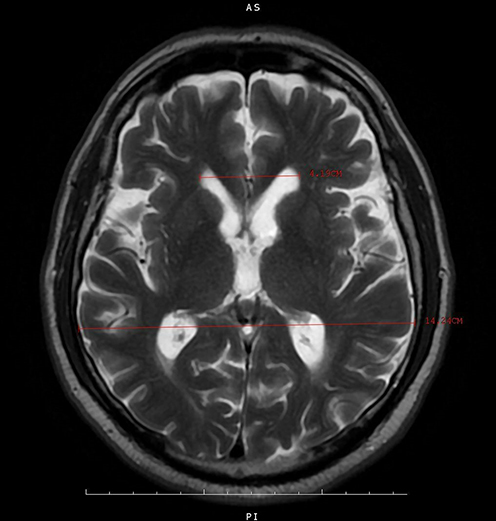 |
Figure 1 Calculation of the Evans Index. |
 |
Figure 2 Calculation of the anteroposterior diameter of the lateral ventricle index (ALVI). |
For the measurement of the callosal angle, reconstructed 3D T1-weighted MPR images were interactively reformatted to create coronal images along the anterior and posterior commissure planes perpendicular to the posterior commissure level. Two straight lines were drawn along the medial walls of the left and right lateral ventricles in the orthogonal coronal plane along the anterior and posterior commissure planes, and the angle between the lines was calculated.
Statistics
The descriptive data are presented as frequencies (percentages), or mean ± standard deviation. The normality of the continuous variables was assessed with Shapiro–Wilk tests and histogram graphs. For normally distributed variables, an independent samples t-test and one-way ANOVA were used. In case of unequal variances during the independent samples t-test, Welch’s t-test was applied. When the data did not meet the normality assumption, non-parametric Mann–Whitney U-tests and Kruskal–Wallis tests were used to compare the continuous variables between groups. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic and discriminatory performance of the Evans index and ALVI in differentiating patients with HFrEF from healthy controls, and the area under the ROC curve (AUC) was calculated. All statistical analyses were performed using the Statistical Package for Social Sciences 26.0 for Windows (SPSS Inc., Chicago, Illinois, USA). The results were considered to be significant at a level of p < 0.05.
Results
A total of 208 subjects were examined, including the HFrEF group (EF: 34.1 ± 5.3%) and the healthy control group (EF: 63.9 ± 3.6%). The mean age was 59.7 ± 10.8 years in the HFrEF group and 57.2 ± 8.4 years in the healthy control group (p = 0.007).
Comparison of demographic findings between the HFrEF and healthy control groups is summarized in Table 1. BFD, FHR, ALVI, and the Evans index were significantly higher in the HFrEF group than in the healthy control group (BFD: 37.3 ± 3.4 vs. 31.9 ± 2.2, p < 0.001; FHR: 0.32 ± 0.03 vs. 0.28 ± 0.01, p < 0.001; ALVI: 0.44 ± 0.04 vs. 0.38 ± 0.03, p < 0.001; Evans Index: 0.27 ± 0.02 vs. 0.23 ± 0.01, p < 0.001). In addition, the Callosal Angle was found to be significantly lower in the HFrEF group than in the healthy control group (91.2 ± 9.6 vs. 99.7 ± 5.0, p < 0.001; Table 2).
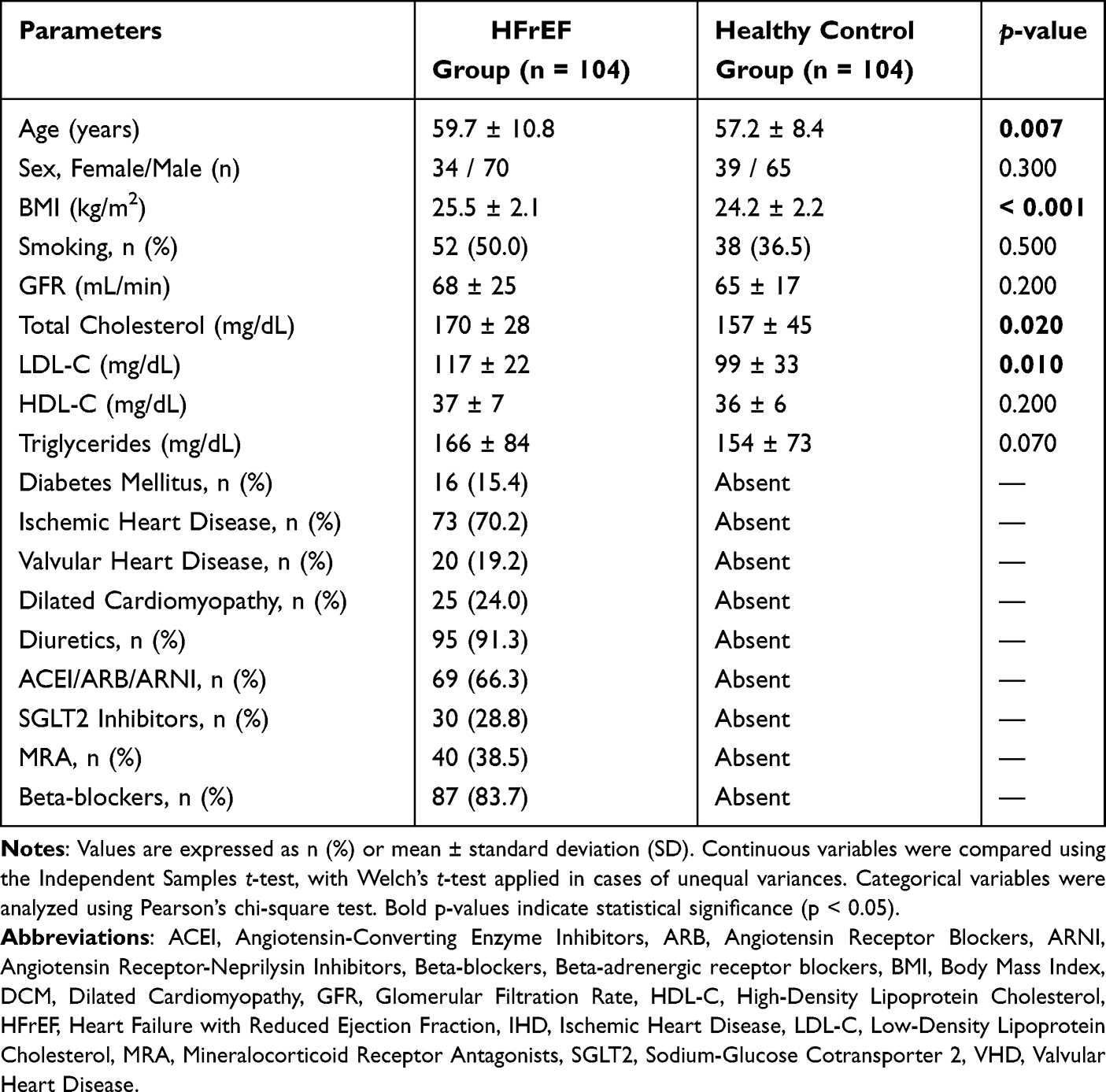 |
Table 1 Baseline Demographic, Clinical, and Laboratory Characteristics of the HFrEF and Healthy Control Groups |
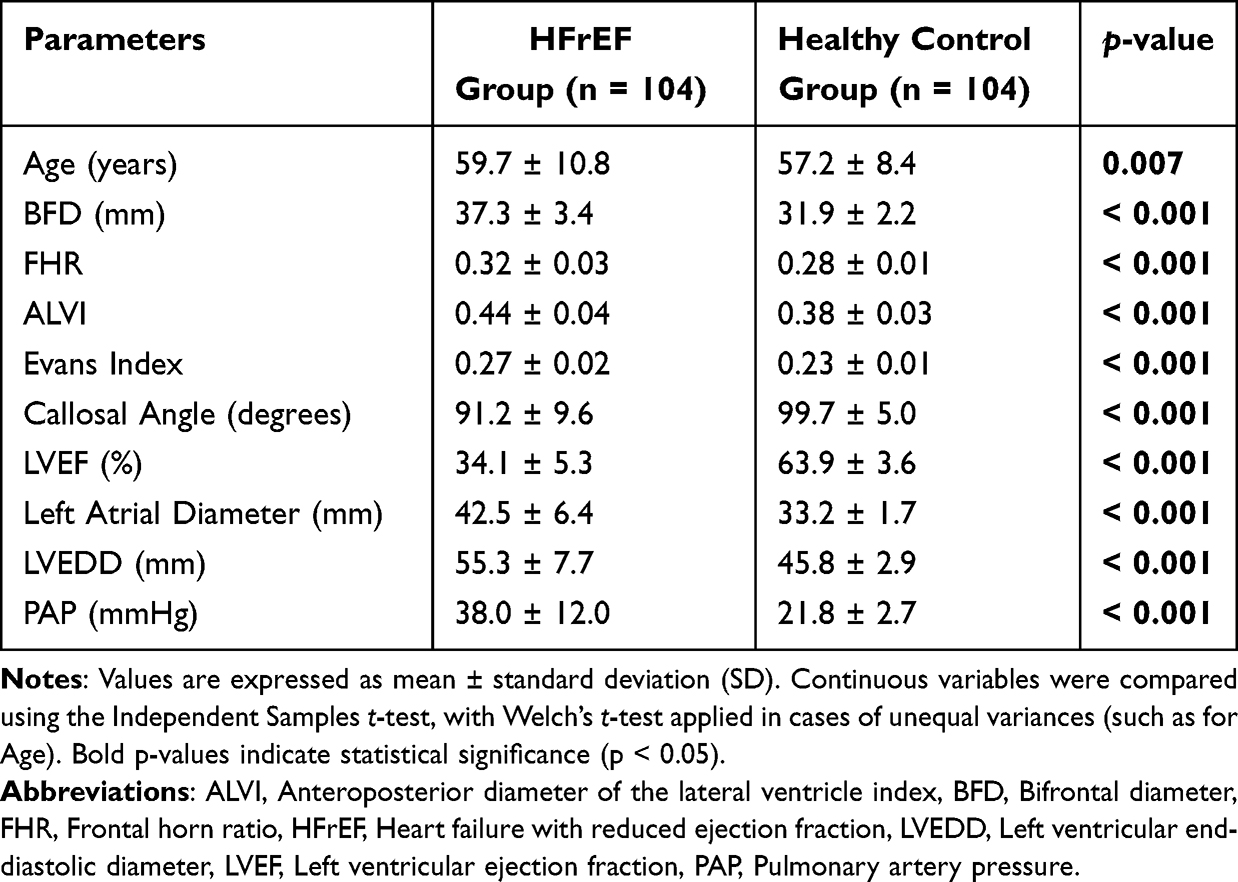 |
Table 2 Comparison of Quantitative Cranial and Echocardiographic Variables Between the HFrEF and Healthy Control Groups |
To eliminate the potential confounding effect of hyperglycemia, a subgroup analysis was performed. In heart failure patients without diabetes mellitus (non-DM HF), both the Evans Index and ALVI remained significantly higher compared to the healthy control group (p < 0.001) (Table 3).
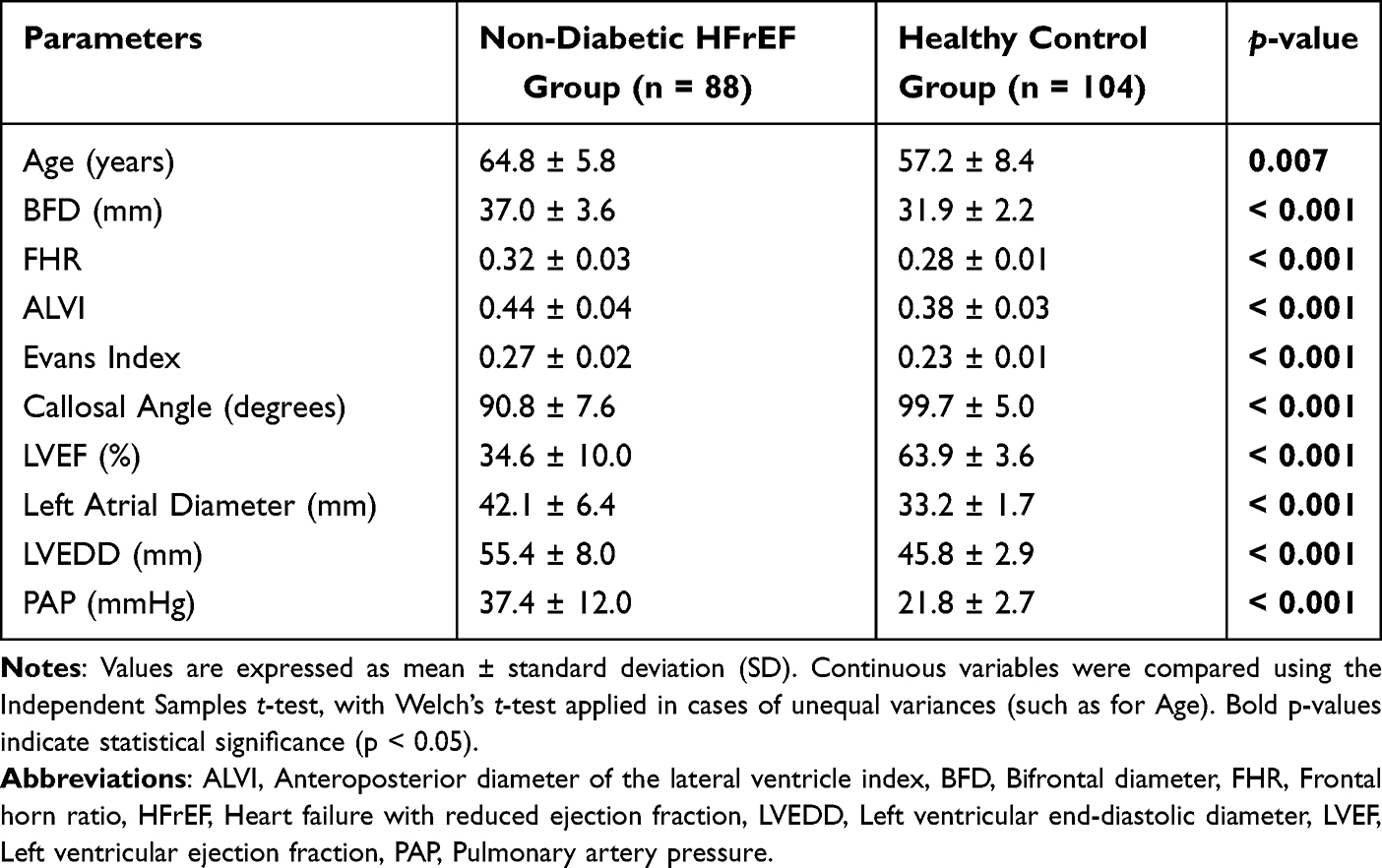 |
Table 3 Comparison of Quantitative Cranial and Echocardiographic Variables Between Non-Diabetic HFrEF Patients and Healthy Controls |
In the correlation analysis (Table 4), a significant and negative correlation was found between LVEF and cranial measurement parameters, including the Evans index (r = −0.550, p < 0.001) and ALVI (r = −0.585, p < 0.001).
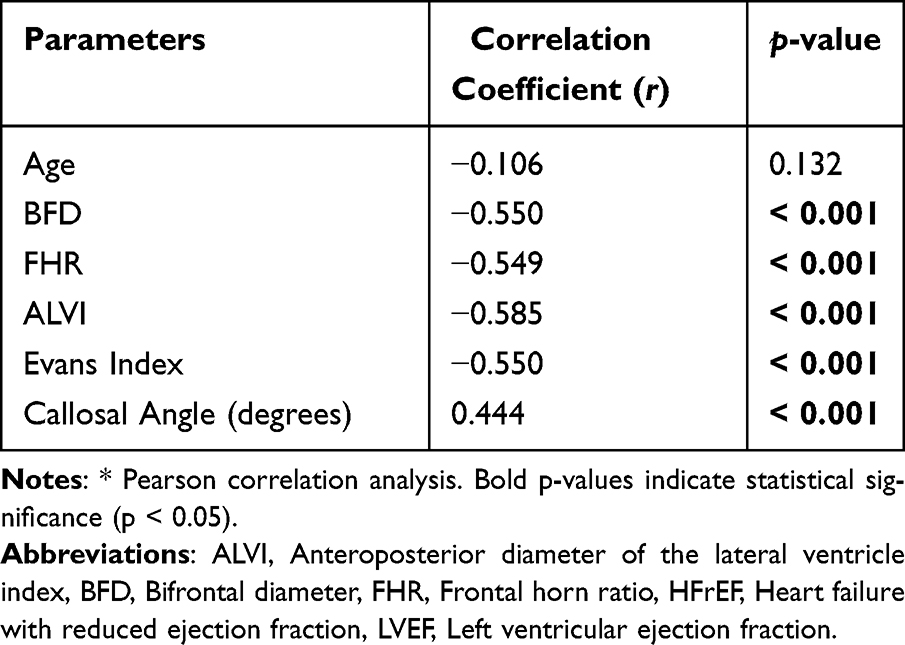 |
Table 4 Correlation Analysis of LVEF with Baseline Clinical and Cranial Measurement Parameters in Patients with HFrEF |
To evaluate the diagnostic and discriminatory performance of the indices in separating HFrEF patients from healthy controls, an ROC curve analysis was performed (with higher index values defining positivity). For ALVI, the analysis resulted in an AUC value of 0.901 (95% CI: 0.859–0.943, p < 0.001). Based on the maximum Youden index, the optimum cut-off for ALVI was determined as 0.41, which yielded a sensitivity of 78.8% and a specificity of 81.7%. For the Evans index, the AUC was 0.903 (95% CI: 0.862–0.944, p < 0.001), and the optimum cut-off was determined as 0.25, with a sensitivity of 75.0% and a specificity of 80.8% (Figure 3).
 |
Figure 3 Receiver operating characteristic (ROC) curve analysis evaluating the diagnostic and discriminatory performance of the Evans Index and the anteroposterior diameter of the lateral ventricle index (ALVI) in differentiating patients with heart failure with reduced ejection fraction (HFrEF, LVEF ≤ 40%) from healthy controls. Higher index values indicate the positive state (HFrEF cohort). Based on the maximum Youden index, the optimal cut-off threshold for ALVI was determined as 0.41, which yielded a sensitivity of 78.8% and a specificity of 81.7% (AUC = 0.901 [95% CI: 0.859–0.943], p < 0.001). For the Evans Index, the optimal cut-off threshold was determined as 0.25, providing a sensitivity of 75.0% and a specificity of 80.8% (AUC = 0.903 [95% CI: 0.862–0.944], p < 0.001). |
Discussion
In this study, we found a significant expansion in the brain ventricular systems of patients with heart failure with a reduced ejection fraction (HFrEF) compared to healthy controls. We also found a negative correlation between LVEF, which is closely related to prognosis in HF, and brain ventricular diameters. That is, as LVEF decreases, brain ventricular diameters increase.
The ALVI and Evans Index increases are objective findings indicating cranial ventricular dilatation.14 In our study, the ALVI and Evans Index were significantly increased in the HFrEF group and were negatively correlated with LVEF. To further validate these findings and evaluate the potential confounding effect of hyperglycemia, a subgroup analysis was performed. Within the HFrEF group, 16 patients (15.3%) were identified as diabetic. Even after excluding these patients, the elevations in ALVI and Evans Index remained significantly higher compared to healthy controls. However, given the baseline age difference discovered upon rigorous re-analysis, this finding should be interpreted cautiously, as age and other baseline cardiovascular risk factors may concurrently contribute to these structural alterations rather than HFrEF pathology being entirely independent.
Our ROC curve analysis demonstrated high diagnostic and discriminatory performance for case-control separation, with optimal cut-off points of 0.41 for ALVI and 0.25 for the Evans Index, determined by the maximum Youden index with higher values defining positivity. In contrast to longitudinal survival metrics, these cut-off values effectively differentiate HFrEF patients from healthy controls, reflecting the cross-sectional structural brain burden associated with lower ejection fraction. Given that an LVEF of ≤40% is a strong predictor of poor prognosis and mortality,13,15 our findings suggest that these cerebral indices covertly parallel the clinical severity profile of HFrEF patients.
The results we found in our study may support the idea that relative cranial ventricular dilatation develops in association with low EF in HFrEF patients. These changes may be related to the cognitive impairment seen in HF patients; our study is a pioneering work in this field and can be supported by further longitudinal studies. More than 40% of patients show signs and symptoms of memory impairment, difficulty concentrating, and attention deficit. This cognitive dysfunction in HF patients is associated with a poor prognosis.16,17
Although the etiology of ventricular enlargement in idiopathic normal-pressure hydrocephalus (iNPH) has not yet been fully elucidated, it is thought that various changes in CSF dynamics contribute to ventricular dilatation in iNPH. Crucially, the mean Evans Index in our HFrEF cohort was 0.27 ± 0.02, which remains below the conventional imaging threshold of 0.30 typically required for a clinical diagnosis of iNPH. Therefore, our findings represent relative ventricular enlargement rather than clinical hydrocephalus. The driving force of the pulsatile flow of CSF is the heart. CSF pulsation occurs with cardiac function, respiration, and cerebral compliance. However, restricted (systolic) cardiac motion due to various conditions leads to altered cerebral perfusion and impaired CSF pulse patterns. Chronic disturbances in CSF pulsations result in maladaptive CSF production and resorption.18,19
In the pathophysiology of HF, reduced ejection fraction, chronic changes in perfusion pressure, impaired heart–brain function, and reduced arterial pulsations may lead to reduced glymphatic function, or any mechanism by which heart–brain synchrony is altered may affect normal CSF flow dynamics and contribute to the dilatation of the cerebral ventricular system. It has been suggested that iNPH may create a vicious cycle in which restricted arterial pulsations reduce glymphatic flow, which in turn leads to reduced transport of CSF and solutes through the glymphatic pathways, further reducing intracranial compliance.7,20,21
In addition, abnormal changes in both peripheral and central chemoreflexes occur in HF patients, leading to sympathetic and parasympathetic activation. Abnormal blood pressure, heart rate, and respiratory control occur due to the decrease in baroreflex sensitivity and the accompanying increase in both peripheral and central chemosensitivity.7 All these complex mechanisms may be the pathophysiology explaining the development of dilatation in the brain ventricular system in patients with HFrEF, as we found in our study.
Limitations of the Study
The limitations of the current study are as follows:
- Due to its cross-sectional case-control design, we could not evaluate longitudinal changes over time, long-term mortality, rehospitalization rates, or clinical prognosis; hence, a definitive causal relationship between low LVEF and ventricular enlargement cannot be established.
- Although the groups were matched for age and sex, subsequent statistical re-verification revealed significant baseline differences in age (p = 0.007) and BMI (p < 0.001) between the HFrEF and control groups, introducing a potential source of residual confounding.
- Advanced volumetric brain segmentation and white matter lesion scoring (such as the Fazekas scale) were not performed. In an HFrEF population with a high burden of ischemic heart disease, it is clinically challenging to definitively differentiate whether the observed ventriculomegaly stems primarily from abnormal CSF dynamics or from ex-vacuo changes secondary to cerebral parenchymal atrophy.
- As systematic neurocognitive assessments (such as MMSE or MoCA), gait evaluation, or urinary symptoms were not performed, the neurological functional status remains unaddressed; therefore, these structural indices must be presented strictly as hypothesis-generating findings regarding the heart-brain axis. Furthermore, because all manual linear measurements were performed by a single senior radiologist, a second independent reader evaluation and formal interobserver reproducibility scoring (such as ICC or Bland-Altman analysis) were not conducted, which represents another limitation regarding measurement error margins.
- Finally, while all patients were on clinically stable medication regimens, the real-world utilization rates of SGLT2 inhibitors (28.8%) and MRAs (38.5%) during the enrollment period (2021–2022) were lower than contemporary guideline-directed medical therapy (GDMT) target thresholds due to individual tolerances, comorbidities, and institutional barriers. Consequently, the isolated effect of low EF cannot be entirely decoupled from the advanced disease burden and incomplete GDMT optimization.
Conclusion
In conclusion, cranial ventricular dimensions are significantly increased in patients with HFrEF compared to healthy controls, showing a significant inverse correlation with LVEF systolic impairment. Given the lack of longitudinal outcomes and neurocognitive data, these structural alterations serve as hypothesis-generating findings that warrant future prospective, multi-center trials with systematic neurocognitive and volumetric validation to establish their clear clinical and neurological significance.
Ethics
Ethics committee approval was given by Bolu Abant İzzet Baysal University Medical Faculty Ethics Committee 2021/120.
Acknowledgments
We extend our gratitude to Sait Alan, Mehmet İnanır, Emrah Acar, and İbrahim Dönmez for their insightful suggestions and technical assistance, which greatly improved the quality of this manuscript.
Funding
There is no funding to report.
Disclosure
The author declares no conflicts of interest with respect to this manuscript.
References
1. Li T, Bao X, Li L, Qin R, Li C, Wang X. Heart failure and cognitive impairment: a narrative review of neuroimaging mechanism from the perspective of brain MRI. Front Neurosci. 2023;17:1148400. doi:10.3389/fnins.2023.1148400
2. Kim MS, Kim JS, Kim YR, et al. Cerebral blood flow as a marker for recovery of left ventricular systolic dysfunction in patients with idiopathic dilated cardiomyopathy. J Card Fail. 2012;18(7):549–10. doi:10.1016/j.cardfail.2012.04.007
3. Agrinier N, Thilly N, Briançon S, et al. Prognostic factors associated with 15-year mortality in patients with hospitalized systolic HF: results of the observational community-based EPICAL cohort study. Int J Cardiol. 2017;228:940–947. doi:10.1016/j.ijcard.2016.11.260
4. Wedegärtner SM, Böhm M, Kindermann I. Cognitive dysfunction in heart failure—causes and sequelae. Internist. 2020;61(9):929–938. doi:10.1007/s00108-020-00835-8
5. Ovsenik A, Podbregar M, Fabjan A. Cerebral blood flow impairment and cognitive decline in heart failure. Brain Behav. 2021;11(6):e02176. doi:10.1002/brb3.2176
6. Kindermann I, Fischer D, Karbach J, et al. Cognitive function in patients with decompensated heart failure: the cognitive impairment in heart failure (CogImpair-HF) study. Eur J Heart Fail. 2012;14(4):404–413. doi:10.1093/eurjhf/hfs015
7. Doehner W, Ural D, Haeusler KG, et al. Heart and brain interaction in patients with heart failure: overview and proposal for a taxonomy. A position paper from the study group on heart and brain interaction of the heart failure association. Eur J Heart Fail. 2018;20(2):199–215. doi:10.1002/ejhf.1100
8. Luciano M, Dombrowski S. Hydrocephalus and the heart: interactions of the first and third circulations. Cleve Clin J Med. 2007;74(1):128–131. doi:10.3949/ccjm.74.Suppl_1.S128
9. Cai H, Yang F, Gao H, et al. Vascular risk factors for idiopathic normal pressure hydrocephalus: a systematic review and meta-analysis. Front Neurol. 2023;14:1220473. doi:10.3389/fneur.2023.1220473
10. Deng Z, Wang H, Huang K, et al. Association between vascular risk factors and idiopathic normal pressure hydrocephalus: a Mendelian randomization study. J Neurol. 2023;270(5):2724–2733. doi:10.1007/s00415-023-11604-6
11. Casmiro M, D’Alessandro R, Cacciatore FM, Daidone R, Calbucci F, Lugaresi E. Risk factors for the syndrome of ventricular enlargement with gait apraxia (idiopathic normal pressure hydrocephalus): a case-control study. J Neurol Neurosurg Psychiatry. 1989;52(7):847–852. doi:10.1136/jnnp.52.7.847
12. Earnest MP, Fahn S, Karp JH, Rowland LP. Normal pressure hydrocephalus and hypertensive cerebrovascular disease. Arch Neurol. 1974;31(4):262–266. doi:10.1001/archneur.1974.00490400076009
13. McDonagh TA, Metra M, Adamo M, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
14. He W, Fang X, Wang X, Gao P, Gao X, Zhou X. A new index for assessing cerebral ventricular volume in idiopathic normal-pressure hydrocephalus: a comparison with Evans’ index. Neuroradiology. 2020;62(6):661–667. doi:10.1007/s00234-020-02361-8
15. Heidenreich PA, Bozkurt B, Aguilar D, et al. AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2022;79(17):e263–e421. doi:10.1016/j.jacc.2021.12.012
16. Frey A, Sell R, Homola GA, Malsch C, Kraft P, Gunreben I. Cognitive deficits and related brain lesions in patients with chronic heart failure. JACC Heart Fail. 2018;6(7):583–592. doi:10.1016/j.jchf.2018.03.010
17. Albus C, Waller C, Fritzsche K, et al. Significance of psychosocial factors in cardiology: update 2018: position paper of the German Cardiac Society. Clin Res Cardiol. 2019;108(11):1175–1196. doi:10.1007/s00392-019-01488-w
18. Bramall AN, Anton ES, Kahle KT, Fecci PE. Navigating the ventricles: novel insights into the pathogenesis of hydrocephalus. EBioMedicine. 2022;78:103931. doi:10.1016/j.ebiom.2022.103931
19. Jacobsson J, Qvarlander S, Eklund A, Malm J. Comparison of the CSF dynamics between patients with idiopathic normal pressure hydrocephalus and healthy volunteers. J Neurosurg. 2018;131(4):1018–1023. doi:10.3171/2018.5.JNS173170
20. Ringstad G, Vatnehol SAS, Eide PK. Glymphatic MRI in idiopathic normal pressure hydrocephalus. Brain. 2017;140(10):2691–2705. doi:10.1093/brain/awx191
21. Yamada S, Ishikawa M, Nozaki K. Exploring mechanisms of ventricular enlargement in idiopathic normal pressure hydrocephalus: a role of cerebrospinal fluid dynamics and motile cilia. Fluids Barriers CNS. 2021;18(1):20. doi:10.1186/s12987-021-00243-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.