Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Cerebral, Psychosocial, Family Functioning and Disability of Persons with Schizophrenia
Authors Valencia M, Medina R, Calixto E, Rodríguez N
Received 12 April 2022
Accepted for publication 30 July 2022
Published 15 September 2022 Volume 2022:18 Pages 2069—2082
DOI https://doi.org/10.2147/NDT.S370449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Marcelo Valencia,1 Rafael Medina,2 Eduardo Calixto,3 Noemí Rodríguez2
1Department of Innovation and Global Health, Epidemiologic and Psychosocial Research Direction; National Institute of Psychiatry Ramón de la Fuente, Mexico City, Mexico; 2Institute Jaliscience of Mental Health, Guadalajara, Jalisco, Mexico; 3Neurobiology Department, Neurosciences Direction, National Institute of Psychiatry Ramon de la Fuente, Mexico City, Mexico
Correspondence: Marcelo Valencia, Department of Innovation and Global Health, Epidemiologic and Psychosocial Research Direction, National Institute of Psychiatry Ramón de la Fuente, Calzada México-Xochimilco 101, Colonia San Lorenzo Huipulco, Alcaldía Tlalpan, Mexico City, 14370, Mexico, Tel +52 1 55 4160 5164, Email [email protected]
Abstract: The human brain is the most cognitively capable of mammalian brains, endowed as it is with an overdeveloped cerebral cortex that, in parallel, renders it vulnerable to mental disorders. Schizophrenia is the expression of the dysregulation of the neuronal activity of cortical and subcortical regions due to modifications in the levels of the various neurotransmitters, especially of dopamine, with a reciprocal, intimate relationship among genes with environmental and psychosocial factors. If the dopaminergic system increases the function prefrontal cortex will be reduced: this is the main reason of social, occupational and familiar disruption. The present article describes the function of the brain in schizophrenia and its relation with anatomical, physiological, and genetic changes, in addition to identifying, psychosocial and family factors that can be determinant in the functionality of the patient. A review of national and international bibliography was conducted bearing in mind the following variables: functioning at the cerebral level; psychosocial functioning, familial functioning, disability, and functionality in persons with schizophrenia. Due to the variety of the issues included in this review, it can be concluded that schizophrenia is the product of a complex array of symptoms, deficits and disabilities. It was identified that there is a reciprocal confluence of diverse genetic, psychosocial, familial, environmental, educative, and social factors which affect the functionality of persons with this disorder. The latter makes it necessary to study the patient taking into consideration all of these components in an integral manner.
Keywords: cerebral functioning, psychosocial and family functioning, disability and functionality, schizophrenia
Introduction
The brain represents a mere 2% of the weight of our body, but the entirety of the genetic material; between approximately 55% and 60% of our genes are for neuronal function, organization, and metabolism. The adult human brain possesses on average 86 billion neurons; among these cells, between 21 and 26 billion are situated in the cerebral cortex.1,2 The brain is the sole organ that studies itself and that is capable of generating 5000 thoughts per hour or of consciously making more than 2100 decisions daily.3 The cerebral neurons situated in various anatomical centers of the cerebral cortex and the subcorticals are organs that engage in diverse physiological activities and the control of vital activities, among these, sleep, cardiorespiratory activity, complex activities such as the will, decision-making, the labeling of emotions, behavior, and social impediments, as well as the cognitive functions.4
Three dynamic factors harbor an important interdependence in the manifestations of the diverse mental disorders, that is, biological, psychological, and social. These three factors are responsible for the stimulation, perception, and adaptation that the brain carries out. The groups of neurons of the cerebral cortex integrate their information in a regulated manner, in a controlled biophysical activity, anatomy, and physiology. Evidence indicates great importance in interaction gene-environments on patients with schizophrenia (methylations, mutations, modify regions of regulatory or promoter of genes, etc.), four times greater concordance in monozygotic twins than in dizygotic twins. The previous findings in twins’ study of schizophrenia show genes and proteins involved in changes of neurotransmitter pathway, in special whit dopamine system (biosynthesis, receptors or modulators, alteration in the short arm of chromosome 5, 6, 8, 9, 20 and the long arm of chromosome 22, specific alterations of the genes WKL1, 22q13.33, Leu309Met that represents anatomical alterations in the amygdala, the caudate nucleus and in the hippocampus) clearly designate connection of environmental factors as a key determinant in disease development. Our mental health comprises an integration of anatomy and physiology with a genetic component in a dynamic biofeedback of the social surroundings of each individual.5
The main aim of this review was relational the changes in system dopaminergic (molecular, physiological and neuro anatomical), in the brain of a person with schizophrenia associate at psychosocial, family factors, disabilities and functionality and his possible bidirectional interaction.
Method
Publications on schizophrenia were searched considering key words referring to the following areas of functioning such as cerebral, psychosocial, familial, disability, and functionality. Search was limited to peer-reviewed studies in English and Spanish published between 1 January 1950 and 1 December 2020 that matched the MeSH using the following electronic databases: Medline; EBM Reviews; PsychINFO; Base Salud en Español; Medic Latina; Ciencias de la Salud-BIREME. Exclusion criteria included: 1) publications prior to 1950; 2) editorials, letters, comments, personal communications, conference notes and congress abstracts. In addition, the research team broadened the search by reviewing and incorporating publications included in the reference lists from the identified articles.
In the search, we encounter other definitions such as: remission, symptomatic remission, functional remission, functional recovery, recovery, positive symptoms, negative symptoms, cognitive symptoms, cognitive dysfunctions, cognitive impairments, cognitive functioning, functional impairment, neuropsychological, psychotic symptomatology, psychotic crises, antipsychotic medication, treatment resistant, medication adherence, non-adherence, therapeutic adherence, non-compliance, psychosocial treatment, rehabilitation, psychosocial rehabilitation, relapse, rehospitalizations, stigma, clinical studies, and evidence-based practices. All these variables have been included in their corresponding section of this manuscript. Terms referring to quality of life were excluded of the review because we consider that these definitions would be the subject of another manuscript.
The Functioning of the Brain
The mental processes are the physiological expression of the neuronal activity within a framework of a neurochemistry in equilibrium: neurotransmitters such as dopamine, adrenalin, serotonin, and modulators such as the cytokines, peptides such as the endorphins associated with an adequate mitochondrial energy balance between oxygen consumption and glucose metabolism. In this manner, the perception of each sense, logical reasoning, the motivations, the emotions, the learning of social impediments, or the higher brain functions are the result of brain activity that could be measured through magnetic resonance images, electroencephalographic activity, evoked potentials, etc.6 Schizophrenia is a chronic disease of the brain, its first manifestations can be assessed at the end of adolescence or at the beginning of the adult age, and it is frequently accompanied by disability.7 Schizophrenia has the following clinical characteristics: unusual thought content; disequilibrium in the expression of the emotions, it is a syndrome with a reference of brusque mood changes of the will, with a disparity in the manifestation of symptoms; therefore, the severity of symptomatology should be considered and assessed case-by-case. Changes in the neuronal activity of various brain areas are directly associated with changes in the concentrations of the neuronal activity of transmitters in the synaptic space, principally of catecholamines, primordially dopamine, which are responsible for the positive symptoms, such as those found in delusions and hallucinations, which appear abruptly. These symptoms are most frequently controlled with antipsychotic medications. In contrast, the negative symptoms last longer and are concerned with apathy, disinterest in life, lack of motivation associated with affective poverty, and modifications in sleep patterns, with consequences in neuronal plastic changes in the long term and which are difficult to manage with pharmacotherapy,8 and finally, the cognitive symptoms, which indicate difficulties in or the impossibility of maintaining attention, memory, and concentration, which can cause permanent deterioration in the cognitive functioning of the patient.
The neuronal circuits that underlie the psychosis of a crisis of schizophrenia are characterized by an important increase, and without regulation, of the following neurons: a) thalamo-cortical; b) limbic, and c) those of the basal ganglia. These stimuli, which emerge from the subcortical glutaminergic afferent neurons, significantly change the levels of dopamine in the synergic space (activated by the basal ganglia), give rise to an increase in opioid activity (increase of the function of the kappa receptor), favoring the release of serotonin (increase of the function of the Raphe nuclei) and of noradrenaline, allowing for an even greater activation of the Locus coeruleus.9 The increase of dopamine is related with an increase of the limbic neuronal activity with a diminution in parallel of the prefrontal neuronal function. This is the process of anomalous cerebral laterality and of the loss of contact with reality, a disequilibrium that can begin from early neurodevelopment with an altered connectivity in various regions of the brain. The result comprises a cortical functional disorganization, the social limits, or social filters gradually diminish and change the form of relevant evaluation of the triggers of the behavioral responses. There could be a favored appearance of euphoric states, diminishing the function of the hippocampus and the cerebral amygdala, in addition to an increase of the activity of the thalamus.10
Defining with complete certainty the physiopathology and the neuronal mechanisms of the cerebral disorganization of schizophrenia continues to be one of the most significant challenges of Psychiatry since the XIX century. Even during the anatomopathological fervor based on findings through tomography, functional magnetic resonance, and tractographies associated with the poor results of patients with a diagnosis of schizophrenia, it fell to the Neurosurgeon Fred Plum11 to emit the lapidary statement that this disorder was the graveyard of the Neuropathologists.
The great majority of patients with a diagnosis of schizophrenia have a brain with some anatomical variations that, on the other hand, have been constantly questioned by distinct groups of Anatomists, in that the anatomical variation does not in itself indicate the severity of the illness nor as a predictor of crises or relapses of the disease. Throughout decades, schizophrenia came to be considered as a disease that is more “functional” than “structural”, despite that the history of abnormal findings in the anatomy of the brain dates from the Victorian era, from those years with the predomination of the ventricular alterations and the abnormal displacement of the cerebrospinal fluid in comparison with the controls, without this being consistent and with a great number of positive cases without apparent abnormalities. The Dark Ages of the psychodynamic period had to transpire, as well as the development of the technology in neuroimaging tests, such as Positron Emission Tomography (PET) and Single-Photon Emission Computed Tomography (SPECT), for there to be novel contributions to the understanding of the brain dysfunction of schizophrenia.
Through the Enhancing NeuroImaging Genetics through Meta-Analysis (ENIGMA) Consortium,12 frequent anatomical changes have been identified in patients with schizophrenia compared with healthy individuals of the same age. Examples of these changes are the following: diminution in the volume of structures such as the frontal cortex (responsible for the regulation of the higher cerebral functions and movements); the hippocampus (related with the cognitive processes); the cerebral amygdala (anatomical site of the emotional process), and the hypothalamus (origin of hormonal regulation; life cycles; metabolic control, and temperature control, among many other functions) associated with the diminution of the cerebellar cortex (control of movements). In contrast, we observe the increase in size presented in structures such as the globus pallidus (regulator of movements and obsessive ideas), the lateral ventricles, and the third ventricle (regulators of intracranial pressure).12
Box 1 summarizes the principal findings on the structural abnormalities in the brain of persons with schizophrenia.
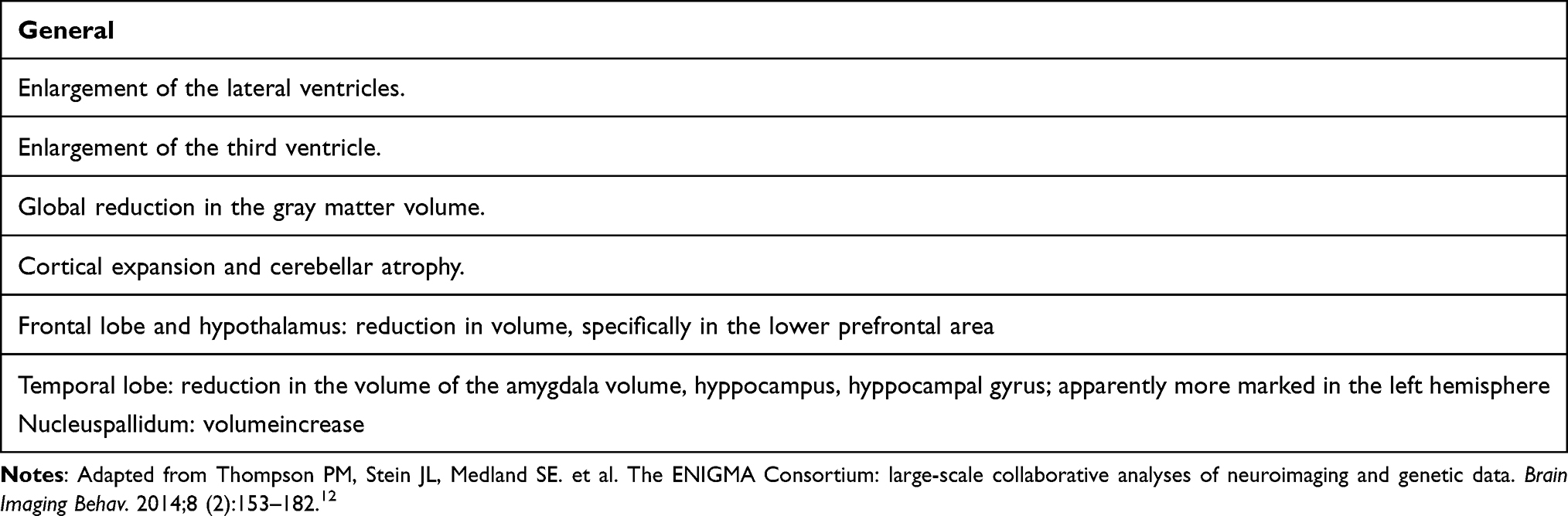 |
Box 1 Structural Abnormalities in the Brain of People with Schizophrenia |
Different techniques of anatomical study, but that are complementary among themselves, such as tractography or magnetic resonance by means of diffusion tensor imaging, have also been demonstrated in patients with schizophrenia, especially in the uncinate fasciculus, the cingulate gyrus, and the arcuate nucleus. In the same manner, studies with evoked potentials and the registration of ocular movements have contributed new evidence in the study of neuronal abnormalities in schizophrenia. The models of neurodevelopment and epigenetics are at the forefront of the general understanding of the pathologic processes of schizophrenia; the most recent structural and functional findings allow us to understand their relation with the cognitive functioning and the characteristic symptoms of the disease.
The genes are involved in the development and in the maintenance of the signs and symptoms of schizophrenia in an important fashion, calculated in a range of 20–50%; this genetic component of schizophrenia is found directly influenced by environmental factors.13 It is known that four chromosomes are intimately related with the disease: for example, chromosome 8 (responsible for the expression of the neuroregulin-1 protein, which intervenes in neuronal migration); chromosomes 1 and 11 (responsible for the genes Disrupted in Schizophrenia 1 (DISC1) and DISC2); their expression is linked to the maturation of the neuronal network of the hippocampus, and chromosome 22 (related with the expression of the enzyme that catabolizes the catecholamines (Catechol-O-MethylTransferase [COMT])). Additionally, schizophrenia is directly related with anomalies in the expression of genes of the D2 receptor of dopamine (with great inhibitory activity of the neuronal activity of the cerebral cortex), intimately associated with modifications in the DNA through methylation generated by stress or after the initiation of certain addictions. Likewise, schizophrenia has also come to show alterations in the expression of the DDR1protein involved in the formation of myelin in the brain. While a unique schizophrenia gene does not exist, the environment, stressor factors, pharmacological factors, or factors of wear-and-tear can induce the changes, whether these be the expression of the triggers or of the facilitators of the mutation of the previously mentioned genes.14
In relation dopaminergic hypothesis between schizophrenia with drugs abuse, many studies show evidences bi-directional drugs dose dependence in induction or aggravate of positive and negative symptoms of the schizophrenia. This indicates an intimate relationship between pharmacological and neurophysiological changes induced by dopamine release drugs generate negative impact in social and epidemiological events. The relationship between schizophrenia with comorbid with substance use (alcohol, amphetamine, cocaine or cannabis) is associated with high rates of hospitalization and mortality. The increases of dopamine in the mesolimbic system are the principal characteristic of schizophrenia and can be associated directly with antisocial behavior, psychotic symptoms, tolerance, dependence, craving and withdrawal. While the exact molecular and pharmacological mechanisms contributing to substance abuse in patients with schizophrenia are not known, different hypothesis have been put forward to explain the basis of the co-occurrence of these disorders; the dopamine and his receptors are the principal target of future research: epidemiological, pharmacological and genetic association with brain anatomic studies to provide an updated formulation regarding the basis of substance use in patients with schizophrenia and this disorder can be increase by drug abuse.
Psychosocial Functioning
Schizophrenia is a disabling psychiatric disorder characterized by symptoms that include hallucinations, delusions and cognitive deficits. In addition, there are a great variety of symptoms such as: emotional and social withdrawal, anxiety, mannerism and posturing, disorientation, blunted affect, active social avoidance and behavioral dysfunction. Patients experience repeated relapses because of exacerbation of the psychotic symptoms even when taking antipsychotic medication that could lead to rehospitalizations. In this century, we are in the process of clarifying the relationship between schizophrenia, disabilities and the psychosocial consequences of the disease.
In order to be able to understand schizophrenia, one must venture beyond knowledge of the psychotic symptomatology, including positive; negative, and cognitive symptoms. There are also other components, such as psychosocial functioning, as well as cognitive functioning, which are present along the entire course of the disease. Symptoms associated with marked social or occupational dysfunction were included as diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders- DSM-IV.15 Psychosocial functioning entertains such relevance that in the 5th edition of the DSM-V,16 it is aptly indicated that the diagnosis of schizophrenia requires considering psychosocial functioning as an important element in the initiation and development of the disease. That is, the symptoms of schizophrenia are importantly associated with the deterioration of psychosocial functioning, which is a fundamental aspect in the diagnosis, course, and management of the disease.
The study of psychosocial functioning has evolved over time from what was initially considered as problems in social adjustment/maladjustment, adaptation, social behavior, difficulties in role performance, role impairment and social dysfunction,17–22 to what at present is determined as social or psychosocial functioning.23–31 Role theory approach32 to study role performance can be considered as the best way to conceptualize and evaluate psychosocial functioning. The word “role” derives from the Latin “rotula”, which refers to the conducts, behaviors, or activities in which persons can engage, considering the interactions that they can have with other persons, within the social ambience in which they behave, while the concept of “functioning” refers to the abilities that the person possesses for performing or functioning in their social roles.22,33
Due to the amplitude, diversity, and complexity of the concept, a consensus has not yet been reached with respect to a definition of social/psychosocial functioning. The Handbook of Social Functioning in schizophrenia defines this impairment as
the inability of individuals to meet societal defined roles, such as homemaker, worker, student, spouse, family member, or friend. In addition, individuals´ satisfaction with their ability to meet these roles, their ability to care for themselves and the extent of their leisure and recreational activities are often subsumed under the rubric of social functioning.34
Psychosocial functioning refers to role performance of individuals in their relationship with other individuals and within a determined environment, thus defining it as: “the actions that individuals carry out in relation to the conditions under which they behave in the social group to which they belong”.35 It also includes diverse activities that individuals carry out in their daily life, with respect to their self-care, self-control autonomy, leisure time, and their interpersonal relationships.36 It refers to the manner in which a person functions according to social expectations, difficulties in getting along with others, and the ability to live according to interpersonal, social, or cultural norms.
Difficulties or a deterioration in psychosocial functioning are considered important characteristics in schizophrenia.37 Patients on occasion can encounter difficulties in establishing social interactions with people, with friends, or difficulties in maintaining relations with the family, refusing to collaborate in household activities, or engaging in an inadequate role performance in some occupational activity.38 It has been estimated that at least one-third of patients with schizophrenia encounter difficulties in complying with their psychosocial roles, even when their psychotic symptomatology is in remission.39–41 In recent decades, in addition to the treatment of the symptoms of the disease, using antipsychotic medication, psychosocial factors have come to be considered for assessing the functioning of the patient in the community; due to this, psychosocial treatment and rehabilitation models have been developed and emerged as complements to antipsychotic drugs. Therefore, pharmacological and psychosocial advances have changed the therapeutic goals for this illness searching for the beneficial effects of integrating pharmacological and psychosocial treatment for these patients.42–53 In a study in which Psychiatrists were questioned with regard to which strategies they would prefer for improving the psychosocial functioning of their patients with schizophrenia, they indicated, psychosocial treatment (46%), pharmacotherapy (26%), no specific strategy (6%), or (10%) did not respond, 70% of these patients had poor psychosocial functioning.40 In schizophrenia, psychosocial functioning can be conceptualized as an early and chronic indicator of a disorder of neurodevelopment. Therefore, it is possible that, for some patients, poor psychosocial functioning could be the result of neurological changes. But also, alternatively, difficulties in psychosocial functioning can be the result of social and environmental factors associated with the initiation of the disease related to the secondary consequences of having a psychotic disorder.54
Various challenging issues schizophrenia patients have to face such as symptomatic remission, functioning and recovery as the ultimate goal. It has been demonstrated that remission can be a reachable goal.47,55,56 Parallel to this, significant efforts have been made for improving functioning. However, this has been a complicated goal because there is a limited consensus about its definition,57 and neither agreement has been reached about a tool for evaluating functioning. We still do not know what constitutes, good functioning, appropriate functioning or normal functioning which indicates the complexities of assessing functioning in schizophrenia.
Considering psychosocial functioning scales as an outcome measure in schizophrenia studies, three scales have been reported as the most frequently used: The Global Assessment of Functioning (GAF),15 The Global Assessment Scale (GAS),23 and The Social Functioning Scale (SFS).58 Two additional reviews29,59 indicate that new scales have been designed for assessing psychosocial functioning: The Personal and Social Performance60 (PSP) and The Social Occupational Functioning Scale (SOFS).61
We cite one example only, considering the GAF as the most frequently used instrument. It is a well-known internationally and widely used scale for scoring a combination of symptoms and functioning with a range score from 1 to 100 with intervals or section, each with 10 points. Lower scores describe the most severely ill while higher scores indicate better improvements on symptoms and functioning. Good functioning or functioning within a normal range should be of >50;62 >6029,57,60,61,63–68 >71;69 >80;70 >8171. These results demonstrate the lack of consensus about the assessment of psychosocial functioning in schizophrenia patients.
With respect to scales for assessing psychosocial functioning in schizophrenia, factorial analyses with Varimax rotation have yielded five factors of functioning: occupational; social; economic; sexual/partner, and familiar,35 l or alternatively, six factors, including social isolation, occupational difficulties, familial frictions, familial dependence, sexual dissatisfaction, and extra-familial frictions.19
While there are instruments to measure remission of psychotic symptomatology as well as functional recovery in schizophrenia, there have also been developed a great variety of scales to evaluate psychosocial functioning, some of which are included in Table 1.
 |
Table 1 Instruments for the Assessment of Psychosocial Functioning in Schizophrenia |
Family Functioning
The moment a person receives the diagnosis of schizophrenia can be the beginning of a series of events and situations with which this person will have to deal that can change his/her life and that can consequently affect and alter the family system. A series of questions will arise regarding the need to obtain immediate responses, due to the fact that relatives do not have the knowledge about the disease, as it has been found in diverse studies that relatives are not found to be prepared to provide the care and support that the patient needs.72,73 Questions such as, Why does the disease occur?, What are the disease’s causes?, and What are the possible explanations for the disorder?, inquiring whether it could be something genetic? or whether it could be the result of communication difficulties or problems in the family ambit in which the patient lives?. The possible association between family problems and schizophrenia dates from some time back; however, the nature of this association has not yet been elucidated.74 While this is being resolved, patients will come to understand that their life is changing and that they will have to make a series of adjustments, preferably with the support of their family. In Mexico, nearly 95% of patients with schizophrenia live with their families.75 Relatives will seek explanations concerning the diagnosis, answers with regard to the impact, the duration and management of the disease, and being a chronic disease, if it will last for a long time, and whether there is a cure for it. Additionally, the patient will have to deal with the following: assistance and payment of medical consultations, acquisition of antipsychotic medication, economic changes and adjustments in terms of whether to seek resources to defray these expenses, compliance with medication, participation in therapies, facing relapses, hospitalizations, and other alterations that can affect the patient’s life. In any case, the family will have to make decisions with respect to continuing the care the patient needs, providing emotional and economic support, as well as managing the emotional burden. Relatives will come to note that the disease definitively alters the familial functioning, and they will decide the manner in which to support the patient, whether by allocating responsibilities, in a balanced manner, among all of the family members, or by considering one or two family members who will thenceforth be the designated relatives for the management of the patient, known as “primary caregivers.” But there can also occur, in the worst of cases, the desire not to participate, in and neglecting the patient’s care during the latter’s recovery process, which can generate a familial crisis, above all when relatives see that not all of the family members collaborate equally, altruistically, and without arriving at a consensus on how to support and help the patient. These induce an unfavorable ambience for the patient’s recovery, and that preferably this would be the beginning of conflicts, and gradually the loss of communication among family members.
In an attempt to understand the experiences that these families undergo, diverse factors have been studied with regard to the patient’s compromise in aspects such as adherence to the indicated dose and schedule of medication compliance. Non-compliance can expose the patients to relapse, which generally occur within the familial environment and which can give rise to recurring crises and hospitalizations, leading to what is known as the “Revolving Door Syndrome”.76 Non-compliance with antipsychotic medication can be one of the main causes of relapse and hospital re-admissions. A retrospective study with a 5-year follow-up quantified that 82% of patients underwent a psychotic relapse and that 78% experienced up to two relapses.77 It was also identified that, during a 10-month period, patients with schizophrenia receiving pharmacological treatment had a probability of relapse of 16% and, in contrast, of 53% in those in who stopped taking.78 It has been estimated that the most important risk factor related to relapse was poor medication compliance due to the fact of negative attitudes of patients towards.79 Non-compliance with the use of medication according to the CATIE (Clinical Antipsychotic Trials of Intervention) showed a media of 4.6 months of discontinuation reaching up to 74% of discontinuation at 18 months.80,81 In response to these inconveniences, there is a great variety of psychoeducative programs to prevent and manage relapse. Participating in these programs, patients and family members can understand the importance of taking antipsychotic medication, which is considered as a protective factor that can help to avoid psychotic crises. The inadequate management of a relapse could initiate a family crisis. Algorithms for the treatment of schizophrenia, set forth as the first-line strategy, we find the use of antipsychotics for the patient, associated with a psychoeducative process for patients and their family, National Institute for clinical excellence.82–85 In another type of intervention, known as from “family-to-family”, relatives who had been previously trained in the illness, teach other relatives to learn diverse aspects about the management of the disease.86 An efficient training of family members will help considerably in terms of better functioning of the patient’s ambit, which in turn could aid in the patient’s functional recovery. Schizophrenia and the familial environment, relapses and recurrent hospitalizations, have been the object of diverse studies. For this purpose, these authors87–89 developed the construct denominated “Expressed Emotion” (EE), which includes two important aspects of the family environment: 1) critical attitudes, and 2) emotional over-involvement of the relatives with the patient. It has been identified that in families with high EE, relapse rate reaches up to 76%, in contrast with families with Low EE, with 28% of these patients relapsing. Similarly, patients most exposed to presenting relapse were those living with families with high EE, who were not taking antipsychotics, and spent more time with the family, relapse for these patients was 92%. Therefore, a greater proportion of relapse can be predicted in families with EE, indicating the importance and the need for including the family in the integral treatment of patient with schizophrenia. The participation of the family is essential and can be a determinant factor for making the difference between functional or dysfunctional patients. With regard to schizophrenia, what is needed are families who are informed with respect to the disease, who can recognize the early warning signs of a relapse,90 who understand the importance and need for their ill family member to take their antipsychotics, and who can additionally receive psychoeducation that permits them to carry out the convenient management of the patient, as indicated in diverse treatment guides for this disorder.45,48,91,92
Disability and Functionality
The evaluation of diverse diseases through the disease burden measured in terms of disability has allowed the mental disorders to position themselves in their true place in the epidemiological panoramas. From the past decade, neuropsychiatric pathologies have been considered the principal cause of disability in global terms, significantly surpassing the majority of the other groups of medical pathologies.93 Schizophrenia, despite its low prevalence, itself contributes to nearly 1–2% of the disability of all non-transmissible diseases and is considered among the ten top leading causes of disease relating disability in the world.94 When the formulation of disability or functional impairment entered the complex equation of mental disorders, the Disability adjusted life years (DALYs) was considered. Disability ranked as high as cardiovascular and respiratory diseases,95 revealing the true magnitude of the impact of disability of mental disorders.96 Few psychiatric illnesses exert such a devastating impact as schizophrenia does on the persons affected.93 Today, schizophrenia is considered a disease, or a group of diseases, that affects the greater part of mental functions, far beyond the simplistic stereotype of considering it a psychiatric entity characterized by hallucinations and delusions. Its impact on the processes and content of thought, the sensorial, the higher mental functions, emotional expression, and volition ends up being catastrophic for the general functioning of the majority of persons with this illness.97
In addition to the clinical factors, other significant elements that contribute importantly for schizophrenia to be considered as one of the diseases that cause more disability at the global level, for example, are early age of the appearance of the disease and the inexistence of curative treatments for this entity. Thus, if we were to consider that the greater part of cases begins at between 20 and 30 years of age. Current life expectancies are found at around 80 years; we have patients who tend to live for around 50 years of age with symptomatology that importantly shrinks a substantial part of the functional capacity of their lives. On the other hand, it should be considered that, in up to 75% of cases of schizophrenia, there is a problem related with treatment adherence,80 or with the patients’ access to treatment, which logically impacts the prognosis in each of these cases. It is noteworthy that, in a significant number of these persons, schizophrenia is not the sole existing diagnosis, but instead, there is a high concurrence of other psychiatric and non-psychiatric illnesses that directly have repercussions on morbimortality and, logically, on the functional level of the subjects affected98 (see Box 2).
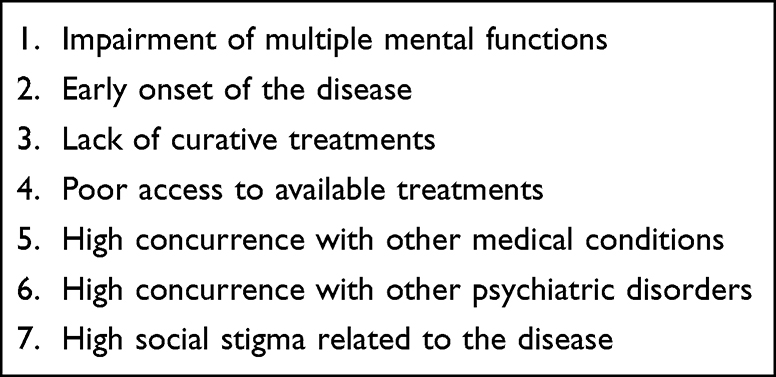 |
Box 2 Factors That Contribute to High Disability in Schizophrenia |
Another important factor to consider is the social stigma associated with the patient with schizophrenia. This stigma is a phenomenon that is narrowly linked with mental disease with multiple negative repercussions, such as discrimination, as well as deficiencies in the treatment received, little economic investment, and limited public policies, associated with normalization of the mistreatment, unjustified fear in patients, and violation of their rights. This is more frequent and serious in relation to the severity of the psychiatric illness. Studies demonstrate the perception of the population with respect to persons with schizophrenia, conceiving of them as unpredictable and aggressive individuals without arguments that sustain this fact.99 It has also been demonstrated that there are few medical evaluations –not psychiatric- to which these patients are submitted, and that when these evaluations are provided, they tend to be incomplete or poor in quality. As if this were trivial, the population with severe mental disorders tends to be the most vulnerable to humiliating and discriminatory treatment, as well as frequent victims of systemic violations of their most basic human rights. A good example of all of the latter is the number of patients who end up in indigence or who are committed to institutions for the rest of their lives.98
Recently, attention has been centered on the contribution of the cognitive dysfunctions of schizophrenia. Mohamed et al100 identified that functional recovery depends less on the acute recuperation from the psychotic symptoms than on neurocognition. In 2018,101 it was reported that the more the cognitive impact, the less the functional and social recuperation and autonomy, and consequently, dysfunctionality. Working memory, executive functioning, verbal fluidity, visuomotor skills, and attention are some of the cognitive functions that most frequently cause disability in these patients. The cognitive factor is recognized as that with the most predictive weight for objectives as significant as that of functional recovery. Therefore, the neuropsychological evaluation is indispensable in all of these patients in order to determine a more precise prognosis and, above all, to present much more specific interventional strategies, in which the most adequate interventions are taken into account, such as cognitive remediation and psychosocial rehabilitation, to reduce the impact of these problems and to entertain greater expectations for the success of the rest of the interventions.
Functionality in People with Schizophrenia
It is possible to suggest links between neurocognition and social function, due to a decrease in the activity or subsequent apoptosis of neurons in the prefrontal cortex, especially in the orbitofrontal region, a site where it is possible to suggest the neurobiological decision-making process, social limits or understanding of the social bond, decreased attention, cognitive biases or loss of selective attention, the social impact of the patient with schizophrenia is immediate: the patient suffers isolation, violence and commonly violation of their human rights.
The patient with schizophrenia has a brain physiology tending to the development of ideas, sometimes creativity or interpretation of reality with loss of limits. This can commonly cause a dysfunction in their social environment, since many of the people in their environment do not coincide with the creative goal of the patient. The social function of the patient with schizophrenia is gradually transformed, increasingly irreversibly if there is the absence of the adequate diagnosis and appropriate treatment are not carried out.
The symptomatology of schizophrenia (positive or negative signs) usually generates fear, estrangement and denial from the family. This passage of the disease develops an environment that increasingly emotionally wears down the family, which moves away from the understanding of the patient. One of the main non-assessable or quantifiable aspects in the management of schizophrenia is the breakdown of family ties, estrangement and loss of the family economy.
Discussion
Schizophrenia is a disease only termed in humans, whose functional characteristic is the increase of dopamine, adrenalin, and endorphins associated with modifications of receptors, immunological modulators that tend to induce anatomical changes in cerebral nuclei. The capacity that the brain possesses for adapting to new risks, learning, analyzing, and avoiding errors is modified throughout life;5 in schizophrenia, the functions of the brain can change due to genetic, anatomic, functional or traumatic alterations.9 An environment of negative stimuli can induce modifications in neuronal communication and in the neurochemistry of the brain.10,13 Factors such as alterations in fetal development, obstetric complications during pregnancy, chronic inflammations, sustained psychosocial stress and drug consumption are involved in the manifestations of symptoms of psychiatric disorders, as is the case of schizophrenia.10
The appearance of delusions, hallucinations, and thought disorders (positive symptoms) associated with poor affect, lack of energy, apathy, demotivation (negative symptoms), as well as difficulties, especially in maintaining attention, concentration, and memory (cognitive symptoms) this is the result of an over-activation of the limbic neuronal networks, basal ganglia associated with a diminution in the activity of the prefrontal cortex. This tends to comprise a behavioral dysregulation that socially stigmatizes the patient. Environmental factors, social relations, as well as family members, can provide an even greater amount of feedback in this process, in recognizing it and avoiding it and that can prevent relapses or that can change the stigma attached to this disease.14 But is not only the stigma relatives have to face, but their inner feelings about the illness, such as: guilt, shame, anger and other negative emotions. In addition, families have to struggle with a disease they know little about it. The family-to-family program is a good example of a psychoeducational intervention designed to help relatives to cope better with a loved one with a mental illness.102 This is of relevance since it has been estimated that one out of four families have at least one relative suffering from a mental illness.103
Schizophrenia is one of the world’s most disabling illness.104 It is ranked among the ten leading causes of disease related to disability in the world.94 These patients function in the community at a much lower level than the general population.105 The level of stress their relatives experience is the double of the general population.106 Many years ago, these patients were confined to asylums or mental institutions, they were institutionalized until the deinstitutionalization process allowed them to live in the community. Since then, the great majority of schizophrenia patients are living in the community,107 this is a new reality. Invariably, they will need antipsychotic medication to achieve symptomatic remission and psychosocial treatment to improve functioning in the community with the support of their relatives that would need psychoeducation considering recovery as the ultimate goal. Research indicates that symptomatic remission can be achieved by 20–97% of patients and functional recovery by 10–68%53,108–111 Outcome for a person with schizophrenia should be based on medicine-based practices that should include: 1) optimal dose of antipsychotic medication to attain remission of symptoms, 2) Psychosocial and Psychoeducational strategies for patients and relatives to have a real knowledge about the illness that will allow them to cope more efficiently with environmental stresses and learn the corresponding skills for survival in the community, and 3) patients and relatives should have the necessary skills for an assertive home-based management to resolve social problems and needs that would help to prevent crises such as symptom exacerbation.112 It has been reported that schizophrenia patients satisfied with their life in general had less severe symptoms as well as better functioning than patients who were not satisfied with their lives.113 These patients experience disability in multiple areas of functioning such as occupational, social and self-care, finance, marriage or an equivalent.24,114 Cognitive impairments and negative symptoms are the most consistent predictors of disability.115 Treatment resistant schizophrenia has been associated with the worst community functioning.116 If we pursue for the well-being of these patients; therefore, treatment of schizophrenia should be an issue of big concern. It has been summarized as follows: 1) It has been estimated that in epidemiological surveys, approximately 40% of people diagnosed with schizophrenia indicated that they had not received any mental treatment in the preceding 6–12 months, 2) According to clinical epidemiological studies, most patients virtually drop out of after their first contact with clinical services receiving practically little mental health care in the subsequent years. 3) In addition, clinical studies indicate that routine treatment do not comply with evidence-based practices.117 There is a science-to-service gap in the real world of schizophrenia treatment, the problem is that approximately 95% of patients living with schizophrenia are not currently receiving all forms of evidence-based treatments.118
A review is needed to provide a comprehensive perspective on the totally of the brain, psychosocial and family functioning, disability and functionality as important domains for understanding a complex illness such as schizophrenia. Adequate information on the biological and psychosocial process as well as familial feedback can be of vital importance in the management of the treatment and the adequate biopsychosocial rehabilitation of the patient with schizophrenia in order to allow for better intervention targeting and to suggest guidance for future research. Learning from outcome studies could lead us toward a comprehensive biological and psychosocial understanding of schizophrenia.
Conclusions
Schizophrenia is the result of various alterations in different neurotransmissions of the brain; however, the increase in the activity of mesolimbic dopaminergic activity is the main neuronal factor that influences the decrease in the function of the prefrontal cortex, these changes are inherent to measurable pharmacological, physiological and anatomical variations in schizophrenia.
The neurochemical change of the brain with schizophrenia has a direct manifestation in psychosocial area; this makes schizophrenia a disease that can be diagnosed early, analyzed in different areas and specifically evaluated in its treatment. However, the family aspect and social projection are fundamental for a better medical understanding and biopsychosocial integration. Genes and the social environment, drugs and the stressful impact are factors that contribute to the manifestation and pharmacological resistance in some cases of schizophrenia, and the understanding of these new evidence will improve decision-making in the diagnosis, management and decision of the environment social involvement in the patient with schizophrenia.
Since schizophrenia represents a low epidemiological impact in relation to numbers in a country, better knowledge of this disease will have a direct impact on recognizing populations at risk and identifying biological markers as well as psychosocial components that would help for a better diagnosis and contribute to better treatment of the disease.
Acknowledgments
This publication was supported by the project “Symptomatic, psychosocial remission and functional recovery in patients with schizophrenia”. Project code and number: CF 41041. Direction of Epidemiological and Psychosocial Research. National Institute of Psychiatry Ramon de la Fuente, Mexico City, Mexico.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article, gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Herculano-Houzel S. The human brain in numbers: a linearly scaled-up primate brain. Front Hum Neurosci. 2009;3(31):1–11. doi:10.3389/neuro.09.031.2009
2. von Bartheld CS, Bahney J, Herculano-Houzel S. The search for true numbers of neurons and glial cells in the human brain: a review of 150 years of cell counting. J Comp Neurol. 2016;524(18):3865–3895. doi:10.1002/cne.24040
3. Helfrich RF, Fiebelkorn IC, Szczepanski SM, et al. Neural mechanisms of sustained attention are rhythmic. Neuron. 2018;99(4):854–865. doi:10.1016/j.neuron.2018.07.032
4. Berlucchi G, Vallar G. The history of the neurophysiology and neurology of the parietal lobe. Handb Clin Neurol. 2018;151:3–30.
5. Stiles J, Jernigan TL. The basics of brain development. Neuropsychol Rev. 2010;20(4):327–348. doi:10.1007/s11065-010-9148-4
6. Kandel E. La Era Del Inconsciente: La Exploración Del Inconsciente En El Arte, la Mente y El Cerebro. Barcelona: Ediciones Paidós; 2013. Spanish.
7. Insel TR. Rethinking schizophrenia. Nature. 2010;468(7321):187–193. doi:10.1038/nature09552
8. Rajasekaran A, Venkatasubramanian G, Berk M, et al. Mitochondrial dysfunction in schizophrenia: pathways, mechanisms and implications. Neurosci Biobehav Rev. 2015;48:10–21. doi:10.1016/j.neubiorev.2014.11.005
9. Stahl SM. Beyond the dopamine hypothesis of schizophrenia to three neural networks of psychosis: dopamine, serotonin, and glutamate. CNS Spectr. 2018;23(3):187–191. doi:10.1017/S1092852918001013
10. Ross CA, Margolis RL, Reading SA, et al. Neurobiology of schizophrenia. Neuron. 2006;52(1):139–153. doi:10.1016/j.neuron.2006.09.015
11. Plum F. Prospects for research on schizophrenia. Neuropathological findings. Neurosci Res Prog Bull. 1972;10:384–388.
12. Thompson PM, Stein JL, Medland SE, et al. The ENIGMA Consortium: large-scale collaborative analyses of neuroimaging and genetic data. Brain Imaging Behav. 2014;8(2):153–182. doi:10.1007/s11682-013-9269-5
13. Zhuo C, Hou W, Li G, et al. The genomics of schizophrenia: shortcomings and solutions. Prog Neuropsychopharmacol Biol Psychiatry. 2019;93:71–76. doi:10.1016/j.pnpbp.2019.03.009
14. Kotlar AV, Mercer KB, Zwick ME, et al. New discoveries in schizophrenia genetics reveal neurobiological pathways: a review of recent findings. Eur J Med Genet. 2015;58(12):704–714. doi:10.1016/j.ejmg.2015.10.008
15. American Psychiatric Association (APA). Diagnostic and Statistical Manual for Mental Disorders.
16. Asociación Estadounidense de Psiquiatría (APA). Manual Estadístico de los Trastornos Mentales V. [DSM-5. Diagnostic and Statistical Manual of Mental Disorders]. Arlington, VA: Editorial Médica Panamericana; 2013. Spanish.
17. Neiman LJ, Hugues JW. The problem of the concept of role. A resurvey of the literature. Soc Forces. 1954;30:141–149. doi:10.2307/2571625
18. Videbeck R. Dynamic properties of the concept role. Midwest Soc. 1958;20(2):104–108.
19. Gurland BJ, Yorkston NJ, Stone AR, et al. The Structured and Scaled Interview to Assess Maladjustment (SSIAM)I. Description, rationale, and development. Arch Gen Psychiatry. 1972;27(2):259–264. doi:10.1001/archpsyc.1972.01750260101017
20. Jablensky A, Schwarz R, Tomov T. WHO collaborative study on impairments and disabilities associated with schizophrenic disorders. A preliminary communication: objectives and methods. Acta Psychiatr Scand. 1980;62:152–163. doi:10.1111/j.1600-0447.1980.tb07687.x
21. Platt S. Social adjustment as a criterion of treatment success: just what are we measuring ? Psychiatry. 1981;44:95–112. doi:10.1080/00332747.1981.11024096
22. Weissman M, Sholomskas D, John K. The assessment of social adjustment. An update. Archiv Gen Psychiatry. 1981;38:1250–1258. doi:10.1001/archpsyc.1981.01780360066006
23. Endicott J, Spitzer RL, Fleiss JL, et al. The global assessment scale. A procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry. 1976;33(6):766–771. doi:10.1001/archpsyc.1976.01770060086012
24. Valencia M, Rascón ML, Juárez F, et al. A psychosocial skills training approach in Mexican out-patients with schizophrenia. Psychol Med. 2007;37:1393–1402. doi:10.1017/S0033291707000657
25. Aas IHM. Global Assessment of Functioning (GAF): properties and frontier of current knowledge. Ann Gen Psychiatry. 2010;9:20. doi:10.1186/1744-859X-9-20
26. Aas IHM. Towards a better Global Assessment of Functioning (GAF): improving scale properties. Int J Emerg Ment Health. 2014;17(1):197–202.
27. Brissos S, Molodynski A, Figueira ML. The importance of measuring psychosocial functioning in schizophrenia. Ann Gen Psychiatry. 2011;10(1):18–25. doi:10.1186/1744-859X-10-18
28. Stefanopoulou E, Lafuente AR, Fonseca AS. Global assessment of psychosocial functioning and predictors of outcome in schizophrenia. Int J Psychiatry Clin Pract. 2011;15(1):62–68. doi:10.3109/13651501.2010.519035
29. Figueira ML, Brissos S. Measuring psychosocial outcomes in schizophrenia patients. Curr Opin Psychiatry. 2011;24:91–99. doi:10.1097/YCO.0b013e3283438119
30. Gorwood P. Psychosocial functioning (PSF)- definition and measurement. Eur Psychiatry. 2012;27:1. doi:10.1016/S0924-9338(12)75679-1
31. Suttajit S, Suwanna A, Srisurapanont L, et al. Psychosocial functioning in schizophrenia: are some symptoms or demographic characteristics predictors across the functioning domains? Neuropsychiatr Dis Treat. 2015;11:2471–2477. doi:10.2147/NDT.S88085
32. Sarbin T, Allen V. Role Theory. The Handbook of Social Psychology.
33. Clare AW, Cairns VE. Designs development and the use of a standardized interview to assess maladjustment and dysfunction in the community studies. Psychol Med. 1978;8:589–604. doi:10.1017/S0033291700018808
34. Mueser K, Tarrier N. Handbook of Social Functioning in Schizophrenia. Boston, MA: Alland&Bacon; 1998.
35. Valencia M, Rojas E, González C, Ramos L. Evaluación del funcionamiento psicosocial en pacientes de un centro de salud. Revista Salud Pública de México. 1989;31(5):674–687. Spanish.
36. Casas E, Escandell MJ, Ribas M, et al. Instrumentos de evaluación en rehabilitación psicosocial. [Assessment in psychosocial rehabilitation]. Revista de la Asociación Española de Neuropsiquiatría. 2010;105:25–47. Spanish.
37. Brissos S, Dias VV, Balanza-Martinez V, et al. Symptomatic remission in schizophrenia patients: relationship with social functioning, quality of life, and neurocognitive performance. Schizophr Res. 2011;129(2–3):133–136. doi:10.1016/j.schres.2011.04.001
38. Green MF, Kern RS. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “right stuff”? Schizophrenia Bull. 2000;26(1):119–136. doi:10.1093/oxfordjournals.schbul.a033430
39. Bellack A, Green M, Cook JA, et al. Assessment of community functioning in people with schizophrenia and other severe mental illnesses: a white paper based on an NIMH-sponsored workshop. Schiz Bull. 2007;33(3):805–822. doi:10.1093/schbul/sbl035
40. Gorwood P, Burns T, Juckel G, et al. Psychiatrists’ perceptions of the clinical importance, assessment and management of patient functioning in schizophrenia in Europe, the Middle East and Africa. Ann Gen Psychiatry. 2013;12(8):1–8. doi:10.1186/1744-859X-12-8
41. Valencia M, Fresán A, Barak Y, et al. Predicting functional remission in patients with Schizophrenia: a cross-sectional study of symptomatic remission, psychosocial remission, functioning, and clinical outcome. Neuropsychiatr Dis Treat. 2015;11:2339–2348. doi:10.2147/NDT.S87335
42. Penn DL, Mueser KT. Research update on the psychosocial treatment of schizophrenia. Am J Psychiatry. 1996;153:607–617.
43. Marder SR, Integrating pharmacological and psychosocial treatments for schizophrenia. Acta Psychiatr Scand. 2000;Suppl 407:87–90. doi:10.1034/j.1600-0447.2000.00017.x
44. Kopelowicz A, Liberman RP. Integrating treatment with rehabilitation for persons with major mental illnesses. Psychiatr Serv. 2003;54(11):1491–1498. doi:10.1176/appi.ps.54.11.1491
45. Lehman AF, Kreyenbuhl J, Buchanan RW, et al. The Schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations 2003. Schizophr Bull. 2004;30(2):193–217. doi:10.1093/oxfordjournals.schbul.a007071
46. Pfammatter M, Junghan UM, Brenner HD. Efficacy of psychological therapy in schizophrenia: conclusions from meta-analyses. Schizophr Bull. 2006;32(Suppl1):S64–S80. doi:10.1093/schbul/sbl030
47. Liberman RP. Recovery from Disability. Manual of Psychiatric Rehabilitation. American Psychiatric Publishing, Inc; 2008.
48. Dixon LB, Dickerson F, Bellack AS, et al.; Schizophrenia Patient Outcomes Research Team (PORT). The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements. Schizophr Bull. 2010;36(1):48–70. doi:10.1093/schbul/sbp115
49. Valencia M, Rascón ML, Juárez F, et al. Application in Mexico of psychosocial rehabilitation with schizophrenia patients. Psychiatry. 2010;73(3):248–326. doi:10.1521/psyc.2010.73.3.248
50. Valencia M, Diaz A, Juarez F. Integration of pharmacological and psychosocial treatment in Mexico: the case of a developing country proposal. Pharmacotherapy. 2012;3:41–68.
51. Valencia M, Fresan A, Juárez F, et al. The beneficial effects of combining pharmacological and psychosocial treatment on remission and functional outcome in outpatients with schizophrenia. J Psychiatr Res. 2013;47:1886–1892. doi:10.1016/j.jpsychires.2013.09.006
52. Valencia M, Moriana JA, Kopelowicz A, et al. Social skills training for Spanish-speaking persons with schizophrenia: experiences from Latin America, Spain and the USA. Am J Psychiatr Rehabil. 2015;18(3):209–246. doi:10.1080/15487768.2014.954161
53. Valencia M, Fresán A, Kopelowicz A, et al. Symptomatic remission and functional recovery in outpatients with schizophrenia. Adv Schizophr Res. 2018;47:1–20.
54. Lin A, Wood SJ, Yung AR. Measuring psychosocial outcome is good. Curr Opin Psychiatry. 2013;26:0951–7367. doi:10.1097/YCO.0b013e32835d82aa
55. Andreasen NC, Carpenter WT, Kane J, et al. Remission in schizophrenia: proposed criteria and rationale for consensus. Am J Psychiatry. 2005;162(3):441–449. doi:10.1176/appi.ajp.162.3.441
56. Leucht S, Lasser R. The concepts of remission and recovery in schizophrenia. Pharmacopsychiatry. 2006;39(5):161–170. doi:10.1055/s-2006-949513
57. Burns T, Patrick D. Social functioning as an outcome measure in schizophrenia studies. Acta Psychiatr Scand. 2007;116(6):403–418. doi:10.1111/j.1600-0447.2007.01108.x
58. Birchwood M, Smith J, Cochrane R, et al. The Social Functioning Scale. The development and validation of a new scale of social adjustment for use in family intervention programmes with schizophrenic patients. Br J Psychiatry. 1990;157:853–859. doi:10.1192/bjp.157.6.853
59. Peuskens J, Gorwood P. How are we assessing functioning in schizophrenia ? A need for a consensus approach. Eur Psychiatry. 2012;27:391–395. doi:10.1016/j.eurpsy.2011.02.013
60. Morosini P, Magliano L, Brambilla LO, et al. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. 2000;101:323–329. doi:10.1111/j.1600-0447.2000.tb10933.x
61. Saraswat N, Rao K, Subbakrishna DK, et al. The Social Occupational Functioning Scale (SOFS): a brief measure of functional status in persons with schizophrenia. Schizophr Res. 2006;81:301–309.
62. Whitehorn D, Brown J, Richard J, et al. Multiple dimensions of recovery in early psychosis. Int Rev Psychiatry. 2002;14:273–283. doi:10.1080/0954026021000016914
63. Harding CM, Brooks GW, Ashicaga T, et al. The Vermont longitudinal study of persons with severe mental illness: II. Long term outcome of subjects who retrospectively met DSM-III criteria for schizophrenia. Am J Psychiatry. 1987;144:727–735.
64. Goldman HH, Skodol AE. Revising axis V for DSM-IV: a review of measures of social functioning. Am J Psychiatry. 1992;149:9. doi:10.1176/ajp.149.1.9
65. Menezes NM, Arenovich T, Zipursky RB. A systematic review of longitudinal outcome studies of first-episode psychosis. Psychol Med. 2006;36(10):1349–1362. doi:10.1017/S0033291706007951
66. Torgalsbøen AK, Rishov Rund B. Maintenance of recovery from schizophrenia at 20-year follow-up: what happened? Psychiatry. 2010;73(1):70. doi:10.1521/psyc.2010.73.1.70
67. Lambert M, De Marinis T, Pfeil J, et al. Establishing remission and Good clinical functioning in schizophrenia: predictors of best outcome with long-term risperidone long-acting injectable treatment. Eur Psychiatry. 2010;25:220–229. doi:10.1016/j.eurpsy.2009.09.001
68. Henry LP, Amminger GP, Harris M, et al. The EPPIC follow-up study of first-episode psychosis:longer-term clinical and functional outcome 7 years after index admissions. J Clin Psychiatry. 2010;71(6):716–728. doi:10.4088/JCP.08m04846yel
69. Hopper K, Harrison G, Wanderling JA. An overview of course and outcome in ISoS. In Recovery from schizophrenia. An international perspective. A report from the WHO collaborative project. In: Hopper K, Harrison G, Janca A, Sartorios N, editors. The International Study of Schizophrenia. Oxford University Press; 2007:23–38.
70. Bobes J, Ciudad A, Alvarez E, et al. Recovery from schizophrenia: results from a 1-year follow-up observational study of patients in symptomatic remission. Schizophr Res. 2009;115(1):58–66. doi:10.1016/j.schres.2009.07.003
71. San L, Ciudad A, Alvarez E, et al. Symptomatic remission and social/vocational functioning in outpatients with schizophrenia: prevalence and associations in a cross-sectional study. Eur Psychiatry. 2007;22(8):490–498. doi:10.1016/j.eurpsy.2007.06.005
72. Doornbos MM. Predicting family health in families of young adults with severe mental Illness. J Fam Nurs. 2002;8(3):241–263. doi:10.1177/107484070200800306
73. Magliano L, Fiorillo A, De Rosa C, et al. National mental health project working group. Family burden in long-term diseases: a comparative study in schizophrenia vs. physical disorders. Soc Sci Med. 2005;61(2):313–322. doi:10.1016/j.socscimed.2004.11.064
74. Falloon RH, Boyd J, McGill CW. Family Care of Schizophrenia: A Problem Solving Approach to the Treatment of Mental Illness. The Guildford Press; 1984.
75. Valencia M, Rascón ML, Quiroga H. Aportaciones de la investigación respecto al tratamiento psicosocial y familiar de pacientes con esquizofrenia. Salud Ment. 2003;26(5):1–18.
76. Goffman E. Essays on the Social Situation of Mental Patients and Other Inmates. Anchor Books Edit; 1961.
77. Kane JM. Review of treatments that can ameliorate adherence in patients with schizophrenia. J ClinPsychiatry. 2006;67(Suppl 5):9–14.
78. Gilbert PL, Harris J, McAdams LA, et al. Neuroleptic withdrawal in schizophrenia patients: a review of the literature. Arch Gen Psychiatry. 1995;52:173–188. doi:10.1001/archpsyc.1995.03950150005001
79. Xiao J, Mi W, L. L, et al. High relapse rate and poor medication adherence in the Chinese population with schizophrenia: results from an observational survey in the People’s Republic of China. Neuropsychiatr Dis Treat. 2015;11:1161–1167. doi:10.2147/NDT.S72367
80. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Eng J Med. 2005;353:1209–1223.
81. Perkins DO. Predictors of nonadherence in patients with schizophrenia. J Clin Psychiatry. 2002;63:12–16. doi:10.4088/JCP.v63n1206
82. American Psychiatric Association. Practice guideline for the treatment of patients with schizophrenia, Second Edition. Am J Psychiatry. 2004;161(2):1–56.
83. National Institute for Clinical Excellence. Core Interventions in the Treatment and Management of Schizophrenia in Primary and Secondary Care. London: NICE; 2002.
84. Castle D, Copolov DL, Wykes T, et al. Pharmacological and Psychosocial Treatments in Schizophrenia. Informa Health Care; 2008.
85. Verduzco W. Guía basada en la evidencia de la Asociación Psiquiátrica de América Latina y de la Asociación Psiquiátrica Mexicana para el tratamiento del paciente con esquizofrenia. [Evidence-based guideline of the Latin American Psychiatric Association and the Mexican Psychiatric Association for the treatment of patients with schizophrenia]. Salud Ment. 2014;37:S1–S118. Spanish.
86. Dixon L, Stewart B, Burland J, et al. Pilot study of the effectiveness of the family-to-family education program. Psychiatric Servi. 2001;52(7):965–967. doi:10.1176/appi.ps.52.7.965
87. Brown GW. The mental hospital as an institution. BrJ Psychiatry. 1977;130:1–18. doi:10.1192/bjp.130.1.1
88. Leff J, Vaughn C. Expressed Emotion in Families. New York: Guildford Press; 1985.
89. Kuipers E, Leff J, Lam DE. Guía práctica de trabajo con las familias. [Esquizofrenia/ Family Work for Schizophrenia]. In: Published by Arrangements with the Royal College of Psychiatrists. London: Ediciones Paidos Iberica; 2004. Spanish.
90. Birchwood M, Spencer E. Schizophrenia: early warning signs. Adv Psychiatr Treat. 2000;6:93–101. doi:10.1192/apt.6.2.93
91. Mari J, Streiner D. Family intervention for those with schizophrenia. In: Cochrane Library. London: BMJ Publications; 1996.
92. Kreyenbuhl J, Buchanan RW, Dickerson FB, et al. The schizophrenia patient outcomes research team (PORT): updated treatment recommendations 2009. Schizophr Bull. 2010;36(1):94–103. doi:10.1093/schbul/sbp130
93. Prince M, Patel V, Saxena. S. No health without mental health. Lancet. 2007;370:859–877. doi:10.1016/S0140-6736(07)61238-0
94. Tandon R, Keshavan MS, Nasrallah HA, Schizophrenia A. “just the facts”: what we know in 2008 part 1: overview. Schizophr Res. 2008;100:4–19. doi:10.1016/j.schres.2008.01.022
95. Murray CJL, Lopez AD. Global Health Statistics; a Compendium of Incidence, Prevalence and Mortality Estimates for Over 200 Conditions. Cambridge: Harvard School of Public Health on behalf of the World Health Organization and the World Bank; 1996.
96. Ustun B, Kennedy C. What is “functionally impairment”? Disentangling disability from clinical significance. World Psychiatry. 2009;8:82–85. doi:10.1002/j.2051-5545.2009.tb00219.x
97. MacDonald A, Schultz C. What we know: finds that every theory of schizophrenia should explain. Schizophr Bull. 2009;35(3):493–508. doi:10.1093/schbul/sbp017
98. Barbato A. Schizophrenia and public health/Angelo Barbato. In: WHO Nations for Mental Health Initiative & World Health Organization. Division of Mental Health and Prevention of Substance Abuse. World Health Organization; 1997.
99. Fresán A, Robles-García R, Cota M, et al. Actitudes de mujeres estudiantes de psicología hacia las personas con trastornos mentales graves: relación con la percepción de agresividad y peligrosidad. Salud Ment. 2012;35:215–223.
100. Mohamed S, Rosenheck R, Swartz M, et al. Relationship of cognition and psychopathology to functional impairment in schizophrenia. AmJ Psychiatry. 2008;165(8):978–987. doi:10.1176/appi.ajp.2008.07111713
101. Bowie CR, Best MW, Depp C, et al. Cognitive and functional deficits in bipolar disorder and schizophrenia as a function of the presence and history of psychosis. Bipolar Disord. 2018;20(7):604–613. doi:10.1111/bdi.12654
102. Dixon L. Educating and Empowering Families. Harvard Mental Health Letter; 2011.
103. World Health Ornization. Informe sobre la salud en el mundo 2001. Salud mental: Nuevos conocimientos, nuevas esperanzas. [The World health report: 2001: Mental health: new understanding, new hope]. Ginebra, Suiza: World Health Organization; 2001. Spanish.
104. Murray CJL, Lopez AD. Global mortality, disability, and the contributions of risk factors: global burden of disease study. Lancet. 1979;349:1436–1442. doi:10.1016/S0140-6736(96)07495-8
105. Jobe TH, Harrow M. Long-term outcome of patients with schizophrenia: a review. Can J Psychiatry. 2005;50:892–900. doi:10.1177/070674370505001403
106. Oldridge ML, Hugues ICT. Psychological well-being in families with a member with a member suffering from schizophrenia: an investigation into long-standing problems. Br J Psychiatry. 1992;161:249–251. doi:10.1192/bjp.161.2.249
107. Shrivastava AK, Stitt L, Thakar M, et al. The abilities of improved schizophrenia patients to work and live independently in the community: a 10-year Long-term Outcome Study from Mumbai, India. Ann Gen Psychiatry. 2009;8:24. doi:10.1186/1744-859X-8-2
108. Valencia M, Caraveo J, Colin R, Verduzco W, Corona F. Remisión sintomática y recuperación funcional en pacientes que padecen esquizofrenia. Salud Ment. 2014;31(1):59–74. doi:10.17711/SM.0185-3325.2014.008
109. Emsley R, Chiliza B, Asmal L, et al. The concepts of remission and recovery in schizophrenia. Curr Opin Psychiatry. 2011;24(2):114–121. doi:10.1097/YCO.0b013e3283436ea3
110. AlAqueel B, Margolese HC. Remission in schizophrenia: critical and systematical review. Harv Rev Psychiatry. 2012;20:281–297. doi:10.3109/10673229.2012.747804
111. Schennach-Wolff R, Jäger M, Seemüller F, et al. Defining and predicting functional outcome in schizophrenia and schizophrenia spectrum disorders. Schizophr Res. 2009;113(2–3):216–217. doi:10.1016/j.schres.2009.05.032
112. Falloon IRH, Montero I, Zihni Sungur M, et al. Implementation of evidence-based treatment for schizophrenic disorders: two-year outcome of an international field trial of optimal treatment. World Psychiatry. 2014;3(2):104–109.
113. Fervaha G, Agid O, Takeuchi H. Life satisfaction among individuals with schizophrenia in the clinical antipsychotic trial of Intervention effectiveness (CATIE) study. Am J Psychiatry. 2013;170:1061–1062. doi:10.1176/appi.ajp.2013.13010060
114. Harvey PD. Disability in schizophrenia: contributing factors and validated assessments. J Clin Psychiatry. 2014;75(Suppl 1):15–20. doi:10.4088/JCP.13049su1c.03
115. Robinson DG, Woerner MG, McMeniman M, et al. Symptomatic and functional recovery from a first episode of schizophrenia or schizoaffective disorder. Am J Psych. 2004;161(3):473–479. doi:10.1176/appi.ajp.161.3.473
116. Iasevoli F, Giordano S, Balletta R, et al. Treatment resistant schizophrenia is associated with the worst community functioning among severely-ill high-disabling psychiatric conditions and its most relevant predictor of poorer achievements in functional milestones. Prog Neuropsychopharmacol Biol Psychiatry. 2016;65:34–48. doi:10.1016/j.pnpbp.2015.08.010
117. Mojtabai R, Fochtmann L, Chang SW, et al. Unmet need for mental health care in schizophrenia: an overview of literature and new data from a first-admission study. Schizophr Bull. 2009;53(4):679–695. doi:10.1093/schbul/sbp045
118. Drake RE, Essock SM. The science-to-service gap in real-world schizophrenia treatment: the 95% problem. Schizophr Bull. 2009;35(4):677–678.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.