Back to Journals » Infection and Drug Resistance » Volume 12
Central nervous system Listeria monocytogenes infection mimicking central nervous system idiopathic inflammatory demyelinating disease
Authors Xu R, Bai Y, Duan C, Zhao S, Chen X, Yang Q
Received 6 October 2018
Accepted for publication 18 December 2018
Published 22 January 2019 Volume 2019:12 Pages 255—259
DOI https://doi.org/10.2147/IDR.S189930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Rui Xu,1,* Yang Bai,2,* Chunmei Duan,1 Shifu Zhao,1 Xiaoyan Chen,1 Qingwu Yang1
1Department of Neurology, Xinqiao Hospital and The Second Affiliated Hospital, Army Medical University (Third Military Medical University), Chongqing 400037, China; 2Department of Otolaryngology, Southwest Hospital, Army Medical University (Third Military Medical University), Chongqing 400038, China
*These authors contributed equally to this work
Abstract: Listeria monocytogenes (Lm) is an opportunistic pathogen that causes life-threatening infections, especially when the central nervous system (CNS) is involved. Here, we report a patient who was admitted to the hospital with headache, dizziness, right side facial numbness, and hoarseness. The individual was initially diagnosed with central nervous system idiopathic inflammatory demyelinating disease (CNS IIDD), which was then found to be CNS Lm infection (brainstem and cervical cord infection). CNS Lm infection mimicking CNS IIDD is rare but must be considered because the treatment is totally different and therapeutic error may be life-threatening.
Keywords: Listeria monocytogenes, CNS infection, CNS IIDD
Introduction
The Gram-positive bacterium Listeria monocytogenes (Lm) was first isolated in a human patient with meningitis in 1921.1 Among listeriosis patients, central nervous system (CNS) Lm infection is a serious and fatal disease; early and appropriate antimicrobial therapy is the most important treatment to reduce mortality and disability.2,3 In humans, CNS Lm infection often occurs in the brainstem. It was reported that Lm rhombencephalitis occurred in up to 24% of listeriosis patients.1,4 This characteristic of Lm causing CNS infection may lead to a misdiagnosis for central nervous system idiopathic inflammatory demyelinating disease (CNS IIDD), such as isolated brain stem syndrome (IBSS), multiple sclerosis (MS), neuromyelitis optica (NMO), or clinical isolated syndrome (CIS). For example, IBSS usually shows an extensive high signal intensity lesion involving the midbrain and the pons in T2-weighted magnetic resonance imaging (MRI) images, which is similar to the MRI findings of Lm rhombencephalitis at the early stage of infection.
Intravenous methylprednisolone (IVMP) pulse therapy is the standard therapy for CNS IIDD, which is totally different from the therapy for CNS Lm infection. Therefore, differential diagnosis between CNS Lm infection (especially for brainstem and cervical cord infection) and CNS IIDD must be seriously considered, as misdiagnosis of CNS Lm infection for CNS IIDD may be life-threatening.
Case report
A 25-year-old previously healthy man was admitted to the hospital with a history of headache (a mild prickling pain of the right occipital), dizziness, right side facial numbness for the last 8 days, and hoarseness for the last 4 days. At the time of admission, neurological examination showed hypoesthesia on the right side of the face and tenderness of exit of the greater occipital nerve. The pharynx reflex was impaired. The meningeal irritation sign was negative, and body temperature was 36.5°C. The blood tests, inflammatory markers, TORCH, and EB virus antibody were all normal. Lumbar puncture was performed, and the pressure was 175 mmH2O. Cerebrospinal fluid (CSF) analysis revealed only a WBC count of 86×106/L (99% monocytes), and culture was negative after a 48-hour incubation. The NMO, MBP, and MOG antibodies were negative both in the CSF and serum. However, an oligoclonal band (OB) was found in the CSF (Figure 1E). MRI of the brain revealed nodular regions of abnormal signal in the medulla oblongata and cervical cord, characterized by hyper-intensity on T2-weighted and fluid attenuated inversion recovery (flair) sequences (Figure 1A and B). After gadolinium injection, nodular enhancing lesions were also detected in the medulla oblongata and cervical cord (Figure 1C and D).
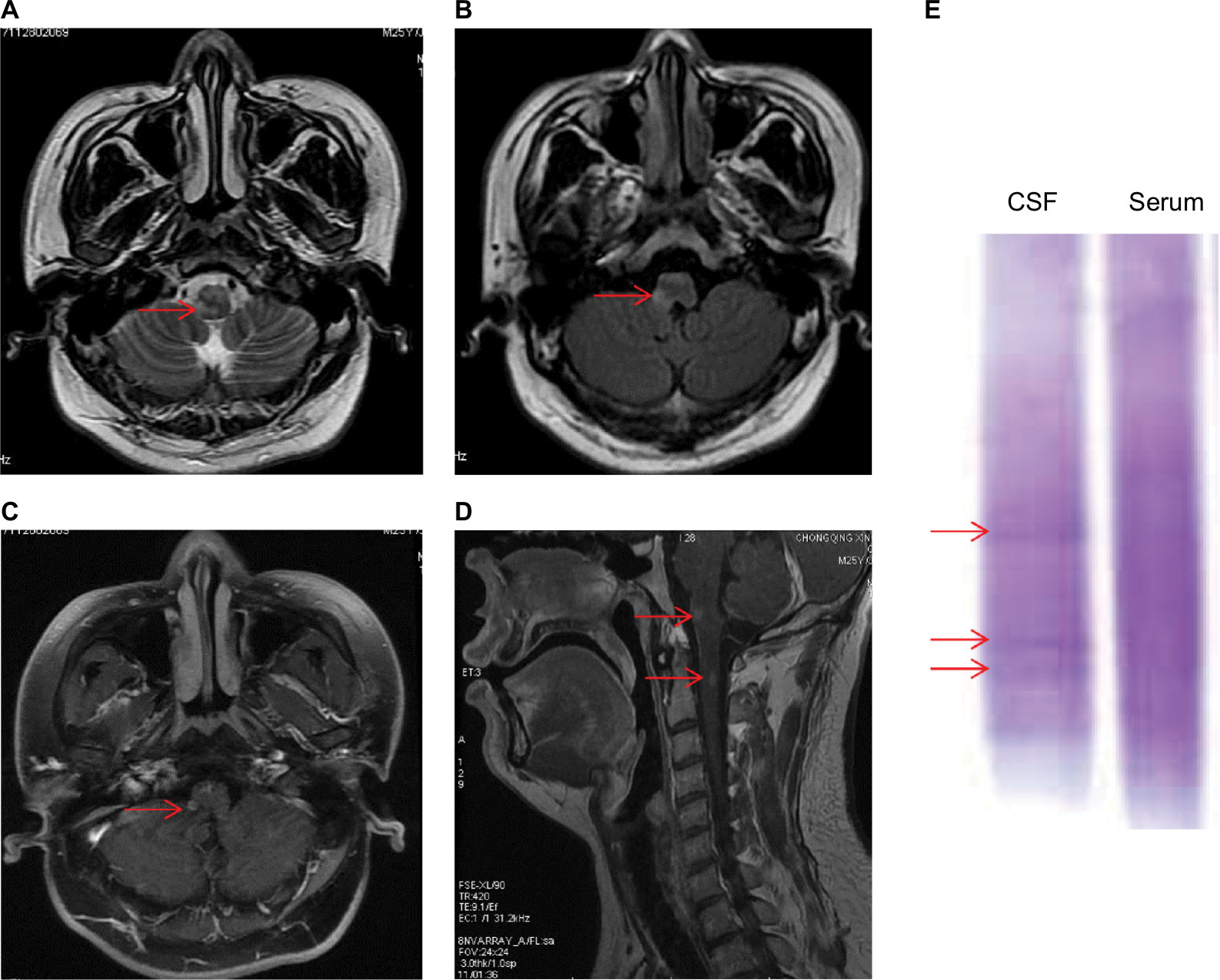 | Figure 1 MRI findings and OB found in the CSF on admission. Notes: MRI of the brain revealed nodular regions of abnormal signal in the medulla oblongata and cervical cord, characterized by hyper-intensity on (A) T2-weighted and (B) flair sequences (arrow). (C and D) Nodular enhancing lesions were detected in the medulla oblongata and cervical cord (arrow). (E) OB found in the CSF (arrow). Abbreviations: CSF, cerebrospinal fluid; MRI, magnetic resonance imaging; OB, oligoclonal band. |
The patient had no clinical symptoms of infection such as fever, cough, sneezing, and so on. The meningeal irritation sign was negative, and the serial laboratory tests were normal. CSF analysis revealed that the number of cells increased slightly and that OB was found in the CSF. MRI examination showed only nodular lesions in the medulla oblongata and cervical cord. Therefore, the patient was considered as CNS IIDD and treated with IVMP pulse therapy (methylprednisolone, 1,000 mg/day). After the first day of IVMP, the patient felt that the hoarseness was improved significantly. However, on the seventh to ninth days, the patient complained of worsened dizziness, vertigo, headache, and balance difficulty. The body temperature increased to 39.9°C, and nystagmus and neck stiffness were observed. His Kernig sign was also positive. A lumbar puncture was immediately performed based on the suspicion of CNS infection. The CSF became turbid, and the pressure increased to 330 mmH2O. CSF analysis showed an elevated WBC count of 635×106/L and a predominance of polymorphonuclear cells (62%). The protein level was mildly elevated (0.45 g/L), while the CSF glucose was slightly decreased (2.68 mmol/L, blood glucose 7.4 mmol/L). Blood tests also showed an elevated WBC count of 24.7×109/L with 87.7% neutrophils, and inflammatory markers including C-reactive protein, IL-6, IL-8, and tumor necrosis factor-α all increased. Repeat MRI was performed, and the lesions were found not only in the brainstem but also in the cerebellum with a hyper-intensity on T2-weighted and flair sequences (Figure 2A and B). The lesions were also found to be patched or ring gadolinium-enhanced with abscess-like appearances (Figure 2D and E). Finally, the blood or CSF sample was cultured on the blood agar plates (Figure 2C), isolates were subjected to Gram staining (Figure 2F), then species identification and drug susceptibility were analyzed by VITEK2 compact (bioMerieux, Craponne, France), and Lm was identified in both blood and CSF. Meanwhile the presence of Lm was further confirmed by PCR assay, and inlA gene primers were used for Lm species-specific recognition as previously reported.5
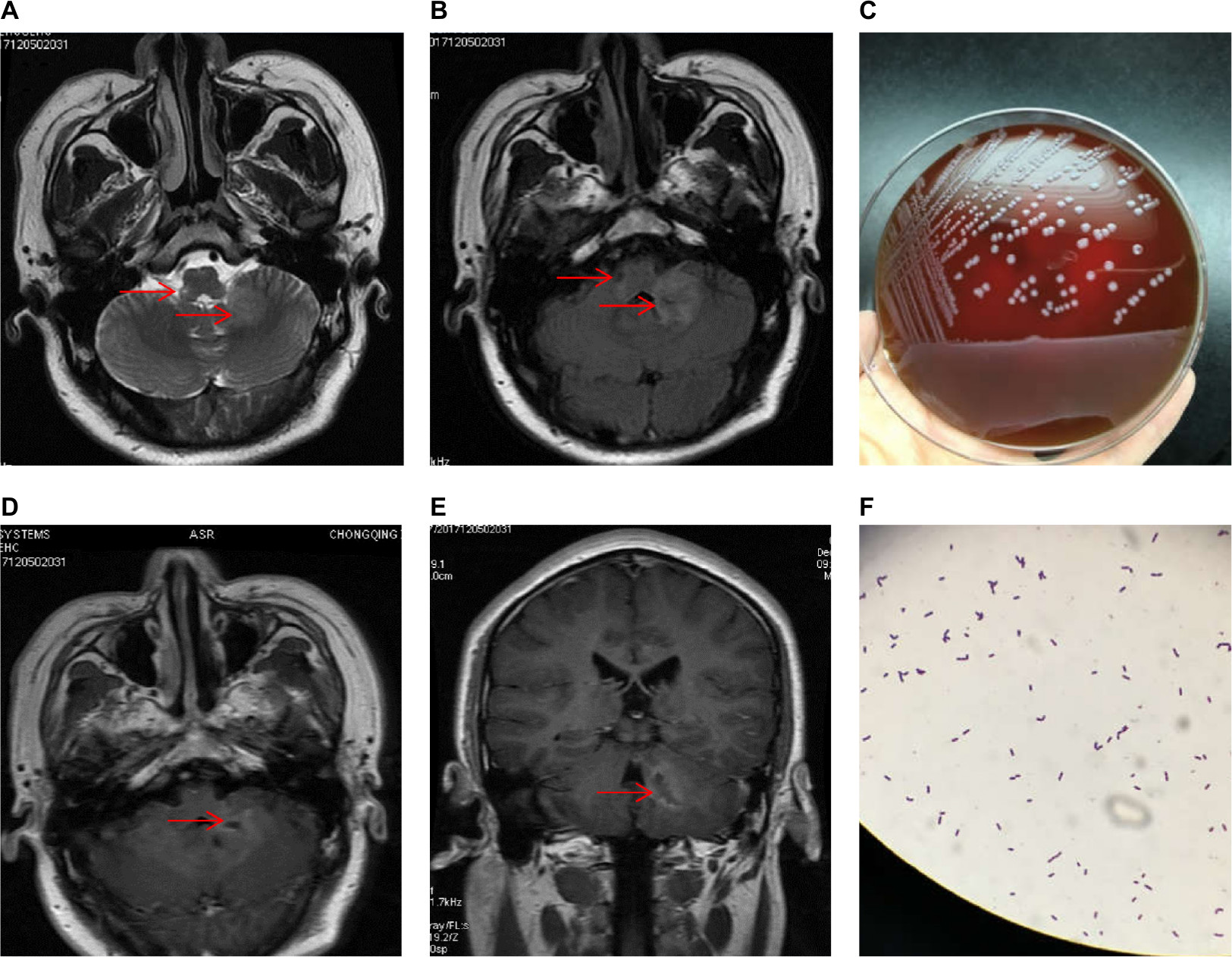 | Figure 2 MRI findings and bacterial cultures when the patient’s condition worsened. Notes: Repeat MRI was performed and the lesions were found not only in the brainstem but also in the cerebellum with a hyper-intensity on (A) T2-weighted and (B) flair sequences (arrow). (C) Bacterial cultures were taken and Lm was identified. (D and E) The lesions were found patched or ring gadolinium-enhanced with abscess-like appearances (arrow). (F) Gram staining of the bacteria. Abbreviations: Lm, Listeria monocytogenes; MRI, magnetic resonance imaging. |
The patient was treated with intravenous penicillin for 4 weeks and meropenem for 2 weeks, followed by a further 2-week course of oral co-trimoxazole monotherapy. The patient was reviewed after 2 months post-admission and had only a left-sided dysmetria.
We confirm that a written informed consent has been provided by the patient to have the case details and any accompanying images published, and institutional approval was required to publish the case details.
Discussion
Lm belongs to the bacterial genus Listeria, which are Gram-positive, facultatively anaerobic, and intracellular coccobacilli.1 Ready-to-eat foods and undercooked and inadequately reheated meats are among the most common modes of transmission to humans.3 Predisposing factors of invasive listeriosis were immunosuppression (eg, HIV infection or chemotherapy), age >50 years, and underlying conditions such as malignancy or diabetes.6,7 However, in this 25-year-old patient, immunosuppressive conditions such as HIV infection or chemotherapy was ruled out, meanwhile underlying conditions such as malignancy or diabetes also did not exist. One of the possible predisposing factor in the presented case was that the patient was a cook and he had raw food before he got sick.
Neurolisteriosis may manifest in humans in many forms such as meningitis, meningoencephalitis, and rhombencephalitis.8 Compared with other pathogens, Lm has a “brainstem predilection”, which means that brain abscesses are always located in subcortical areas (such as the pons or medulla).9 The pathogenesis and the mechanisms are still not clear, but studies have shown that Lm might invade the brainstem by axonal migration along various cranial nerves.1,10 Therefore, Lm-induced rhombencephalitis may be misdiagnosed as CNS IIDD such as IBSS, MS, NMO, or CIS based on MRI examination, especially at the early stage of the Lm infection.
In the presented case, our patient did not present any of the typical characteristics of CNS bacterial infection. The patient had no nonspecific symptoms such as fever, nausea, vomiting, and headache (he had a mild prickling pain of the right occipital lobe, which was considered as occipital neuralgia). And he did not show meningeal signs, cerebellar signs, hemiparesis, or hemisensory defects. Laboratory tests also revealed that the blood tests and inflammatory markers were all normal. CSF bacterial culture was negative and CSF analysis showed that only white cells were slightly elevated. Meanwhile, OB was found in the CSF. MRI examination showed only nodular lesions found in the medulla oblongata and cervical cord, and the patient did have cranial nerve deficits. Above all, based on the symptoms, signs, laboratory tests, and MRI examination, the patient was misdiagnosed as CNS IIDD.
In this present case, the patient did not show any characteristics of CNS Lm infection, and we also discussed the possible reasons. The most likely reason is that the patient may have been in the early stages of bacterial infection. Meanwhile, the patient sought medical treatment in different hospitals repeatedly before he received a regular and systemic hospitalization in our hospital, and he might have received antibiotic therapy (although he denied the history of antibiotic therapy). In addition, OB was found in the CSF, which played a key role in the misdiagnosis of CNS IIDD in this case. It is known that OB is considered an important factor for the diagnosis of CNS IIDD such as MS. The sensitivity for detecting OBs in MS patients with the isoelectric focusing method is ~95% and the specificity is >86%,11 but it should be noted that in addition to MS, many other neurologic diseases generate CSF-specific OBs as a humoral immune response (including infection). OBs can also be found in other conditions such as HIV,12 and it can even be found in up to 8% of healthy subjects.13
To our knowledge, Décard et al had once reported Listeria rhombencephalitis mimicking a demyelinating event in an immunocompetent young patient.14 However, the CSF analysis of the patient in their report showed negative OBs, which might raise the awareness of clinicians for alternative diagnoses.14 Compared with their case, the patient in this case showed more typical and misleading characteristics of CNS IIDD from symptoms, signs, laboratory tests, CSF analyses, and MRI examinations. Therefore, although it is rare, we propose that differential diagnosis of CNS IIDD and CNS Lm infection should be noted, especially for patients presenting with typical brainstem defects.
Acknowledgment
This work was supported by the Miao Pu project of Army Medical University (2017R016) and SWH2016JCYB-29.
Author contributions
RX, YB, CD, SZ, XC, and QY were involved in the neurological patient care, analysis, and interpretation of clinical results and data. RX and YB drafted the manuscript. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Oevermann A, Zurbriggen A, Vandevelde M. Rhombencephalitis caused by Listeria monocytogenes in humans and ruminants: a zoonosis on the rise? Interdiscip Perspect Infect Dis. 2010;2010:632513. | ||
Yılmaz PÖ, Mutlu NM, Sertçelik A, Baştuğ A, Doğu C, Kışlak S. Linezolid and dexamethasone experience in a serious case of listeria rhombencephalitis. J Infect Public Health. 2016;9(5):670–674. | ||
Mansbridge CT, Grecu I, Li Voon Chong JS, Vandervelde C, Saeed K. Two cases of Listeria rhombencephalitis. IDCases. 2018;11:22–25. | ||
Bartt R. Listeria and atypical presentations of Listeria in the central nervous system. Semin Neurol. 2000;20(3):361–374. | ||
Liu D, Lawrence ML, Austin FW, Ainsworth AJ. A multiplex PCR for species- and virulence-specific determination of Listeria monocytogenes. J Microbiol Methods. 2007;71(2):133–140. | ||
Kales CP, Holzman RS. Listeriosis in patients with HIV infection: clinical manifestations and response to therapy. J Acquir Immune Defic Syndr. 1990;3(2):139–143. | ||
Mylonakis E, Hohmann EL, Calderwood SB. Central nervous system infection with Listeria monocytogenes. 33 years’ experience at a general hospital and review of 776 episodes from the literature. Medicine (Baltimore). 1998;77(5):313–336. | ||
Clauss HE, Lorber B. Central nervous system infection with Listeria monocytogenes. Curr Infect Dis Rep. 2008;10(4):300–306. | ||
Eckburg PB, Montoya JG, Vosti KL. Brain abscess due to Listeria monocytogenes: five cases and a review of the literature. Medicine (Baltimore). 2001;80(4):223–235. | ||
Oevermann A, Di Palma S, Doherr MG, Abril C, Zurbriggen A, Vandevelde M. Neuropathogenesis of naturally occurring encephalitis caused by Listeria monocytogenes in ruminants. Brain Pathol. 2010;20(2):378–390. | ||
Domingues RB, Fernandes GBP, Leite F, et al. The cerebrospinal fluid in multiple sclerosis: far beyond the bands. Einstein (Sao Paulo). 2017;15(1):100–104. | ||
Soong J, Riley R, Mcpherson R. Oligoclonal bands of immunoglobulins in serum leading to diagnosis of human immunodeficiency virus 1 infection. Am J Clin Pathol. 2016;145(2):277–281. | ||
Gurtner KM, Shosha E, Bryant SC, et al. CSF free light chain identification of demyelinating disease: comparison with oligoclonal banding and other CSF indexes. Clin Chem Lab Med. 2018;56(7):1071–1080. | ||
Décard BF, Thöne J, Haghikia A, et al. Listeria rhombencephalitis mimicking a demyelinating event in an immunocompetent young patient. Mult Scler. 2017;23(1):123–125. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.