Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Cenobamate for Difficult-to-Treat Epilepsy – Selected Case Vignettes
Authors Villani F ![]() , Dono F, Operto FF, Pignatta P, Puligheddu M
, Dono F, Operto FF, Pignatta P, Puligheddu M ![]() , Stipa C, Zanoni T
, Stipa C, Zanoni T
Received 24 April 2025
Accepted for publication 22 August 2025
Published 5 November 2025 Volume 2025:21 Pages 2437—2448
DOI https://doi.org/10.2147/NDT.S529751
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Taro Kishi
Flavio Villani,1 Fedele Dono,2 Francesca Felicia Operto,3 Pietro Pignatta,4 Monica Puligheddu,5 Carlotta Stipa,6 Tiziano Zanoni7
1Division of Clinical Neurophysiology and Epilepsy Center, IRCCS Ospedale Policlinico San Martino, Genova, Italy; 2Department of Neuroscience, Imaging and Clinical Sciences, “G. d’Annunzio” University of Chieti-Pescara, Chieti, Italy; 3Department of Health Sciences, University of Catanzaro, Catanzaro, Italy; 4Neurology and Epilepsy Unit, Humanitas Gradenigo Hospital, Turin, Italy; 5Department of Medical Sciences and Public Health, University of Cagliari, Cagliari, Italy; 6Reference Center for Rare and Complex Epilepsies (EpiCARE), IRCCS Istituto Delle Scienze Neurologiche di Bologna, Bologna, Italy; 7Neurology Unit, Azienda Ospedaliera Universitaria Integrata Verona, Verona, Italy
Correspondence: Flavio Villani, Email [email protected]
Introduction: Epilepsy affects millions worldwide, presenting unique challenges in specific populations such as the elderly, children, and patients with comorbidities or drug-resistant forms. Tailored approaches addressing unmet needs in these subgroups are critical to improving outcomes.
Areas Covered: This research uniquely integrates real-world evidence and detailed case vignettes from the EPI CONNECT project to evaluate the role of cenobamate in managing these complex cases, providing practical insights beyond traditional clinical trials. The article explores the potential of cenobamate, a novel antiseizure medication with dual mechanisms of action, in improving seizure control, simplifying polytherapy, and enhancing tolerability across various subpopulations. Case-based narratives illustrate its practical use in challenging scenarios.
Expert Opinion: Cenobamate offers important advantages for underserved epilepsy populations, including seizure improvement, polypharmacy reduction, and improved adherence and quality of life. This review seeks to bridge current clinical practice with ongoing research efforts, fostering improved personalized treatment approaches and advancing understanding of cenobamate’s long-term role in managing difficult-to-treat epilepsy populations. It aims to provide practical guidance for clinicians and to highlight future research directions, encouraging ongoing investigation into long-term efficacy, safety, and personalized care strategies.
Keywords: antiseizure medication, cenobamate, cognitive comorbidities, drug-resistant epilepsy, epilepsy management, developmental and epileptic encephalopathies, DEEs, Lennox-Gastaut syndrome, pharmacoresistance, seizure control, vagus nerve stimulation
Introduction
Epilepsy is a chronic neurological disorder characterized by recurrent and unprovoked seizures which affects approximately 50 million individuals globally, posing significant personal and societal burdens.1,2 Despite recent advancements in diagnostic procedures and therapeutic options, a significant portion of patients within specific subpopulations face unique clinical challenges, hence requiring a more tailored approach.3 In particular, elderly patients, individuals with cognitive and psychiatric comorbidities, patients with severe developmental and epileptic encephalopathies (DEEs), and individuals identified as candidates for surgical interventions or neuromodulation (eg vagus nerve stimulation (VNS)) constitute some of the most challenging subpopulations.4–7
Each of these patient groups presents distinct challenges and unmet needs. The elderly often face diagnostic and therapeutic challenges due to overlapping symptoms with neurodegenerative disorders, compounded by treatment complexities arising from age-related comorbidities, age-related physiological changes (ie, altered renal and hepatic functioning), and the burdens of polypharmacy.8,9 Incidence ranges from about 2.4 to over 10 per 1000 person-years, increasing sharply with age, especially >60 years. Prevalence estimates vary from 6.4 to 19.3 per 1,000, with higher rates in older age groups.10–12 Similarly, managing epilepsy in patients with cognitive or psychiatric comorbidities is fraught with difficulties, as conventional antiseizure medications (ASMs) tend to worsen the neuropsychiatric profile or introduce additional adverse effects.13,14 Precise epidemiological data are less well defined but these comorbidities are common in epilepsy.15 In severe DEEs, such as Lennox-Gastaut syndrome (LGS) and tuberous sclerosis complex (TSC), drug-resistance is frequently observed and therapeutic options remain fairly limited. DEEs are rare but severe; epidemiology is less well quantified in general population data.16,17 Finally, individuals who fail pharmacological treatment and require surgical or neuromodulation approaches often represent some of the most refractory cases, necessitating highly individualized treatment strategies. This subgroup represents around 20–30% of those with focal epilepsy who are drug-resistant, having failed two or more antiseizure medications.18–20 Similarly, VNS — the first approved neuromodulation therapy — achieves ≥ 50% seizure reduction in 50–60% of recipients, with about 8% attaining seizure freedom.21 Data on the management of the aforementioned subpopulations are limited and often extrapolated from studies involving more general populations.15 The lack of targeted evidence hinders the development of optimized therapeutic approaches, underscoring the critical need for further research supported by real-world data.22
Adjunctive cenobamate, a novel add-on ASM indicated for focal onset seizures in adults with epilepsy who have not achieved adequate control with at least two prior antiseizure drugs, may represent a therapeutic opportunity for difficult-to-treat patient populations.23–25
Cenobamate is a tetrazole-derived carbamate whose antiseizure effect stems from a dual mechanism: (i) preferential block of the persistent voltage-gated sodium current with promotion of fast/slow channel inactivation, and (ii) positive allosteric modulation of synaptic and extrasynaptic GABA-A receptors at a benzodiazepine-insensitive site, strengthening both phasic and tonic inhibition.26,27 Exposure is dose-proportional up to ~300 mg/day but rises supra-proportionally thereafter, requiring titration. Metabolism is dominated by UGT2B7/2B4 glucuronidation with minor CYP2E1/2B6/2A6/3A4/5 and CYP2C19 contributions; at therapeutic doses cenobamate inhibits CYP2C19 while inducing CYP3A4, increasing phenytoin, phenobarbital and N-desmethyl-clobazam levels but lowering carbamazepine and lamotrigine, and reducing steroid-based contraceptive efficacy.26,27
Preliminary evidence suggests its efficacy in controlling seizures while offering potential advantages in tolerability and safety, making it an intriguing option for addressing the challenges faced by disadvantaged groups.28–32 Moreover, multiple meta-analyses—from a pooled trial review in 2020 to broader network comparisons in 2022 and 2024 —consistently rank cenobamate at the top for both ≥ 50% responder and seizure-freedom rates, without an accompanying rise in treatment discontinuations, underscoring its efficacy and favourable tolerability across modern add-on ASMs.33–35 Real-world uptake, however, lags because reimbursement controls, the 12-week slow-titration schedule and CYP-mediated interactions demand extra clinician effort, while familiarity with the drug is still limited.36
The EPI CONNECT project is a multicentre Italian initiative that compiles real-world cenobamate vignettes in four difficult-to-treat groups—older adults, patients with cognitive or psychiatric comorbidities, developmental-encephalopathy syndromes, and surgical/VNS candidates. It documents routine titration, drug interactions and polypharmacy reduction, providing clinician-driven insights to guide future studies.
Project Design
The EPICONNECT working group consists of a diverse team of Italian epileptologists (the Authors of the present article) with varying levels of clinical experience and specialized expertise in both adult and pediatric epilepsy. The project aimed to integrate real-world evidence and clinical experiences to address the challenges faced by the aforementioned epilepsy subpopulations.
The initiative was structured around two in-person expert meetings, supplemented by a dedicated online platform (www.epiconnect.it) for data sharing and collaborative discussions. The meetings provided a forum for reviewing current literature, presenting clinical cases, and discussing expert opinions on treatment strategies, with a particular focus on the role of cenobamate as a potential therapeutic option. This article presents five selected case vignettes (summarized in Table 1) to illustrate practical considerations and therapeutic outcomes in patients with difficult-to-treat epilepsy.
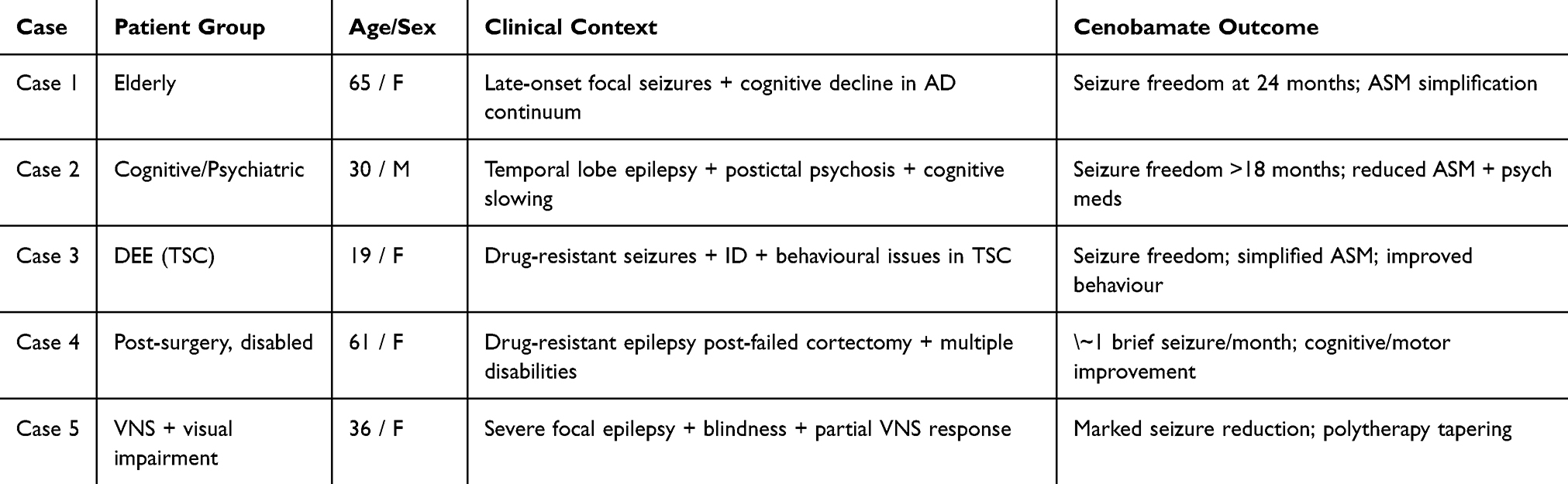 |
Table 1 Summary of the Five Clinical Vignettes Presented in the Manuscript, Illustrating the Use of Cenobamate Across Distinct Difficult-to-Treat Epilepsy Populations. Each Case Highlights Real-World Therapeutic Challenges, Clinical Context, and Observed Outcomes Following Cenobamate Introduction |
Elderly Patients with Epilepsy
In individuals over 65, epilepsy onset is predominantly attributed to cerebrovascular disorders, neurodegenerative diseases, and traumatic brain injuries.37,38 With demographic trends forecasting a substantial rise in the elderly population, addressing epilepsy in this group has become a critical public health priority.39
The elderly population poses distinct challenges compared to younger cohorts, necessitating tailored diagnostic and therapeutic strategies.8 From a clinical perspective, elderly patients often present with focal seizures predominantly characterized by non-motor features, frequently manifesting as subtle confusional states accompanied by brief automatisms.40 In contrast, focal-to-bilateral tonic-clonic seizures and primary generalized seizures are less commonly observed in this population.41 Additionally, seizures in the elderly are frequently associated with prolonged post-ictal confusion; however, such manifestations may be misinterpreted as other pathological conditions, including dysmetabolic or toxic states, or as the altered mental states and behavioral fluctuations commonly observed in neurodegenerative disorders.42,43 These seizure mimics further complicate the diagnostic process, often resulting in delays in both diagnosis and treatment.9,44
The therapeutic management of epilepsy in this demographic necessitates particular considerations, including the use of reduced doses of ASMs to minimize the risk of adverse events, as well as the careful management of drug-drug interactions due to the high burden of comorbidities.37,38,44 Furthermore, elderly patients may experience challenges with medication adherence due to polypharmacy, highlighting the potential benefit of once-daily dosing of ASMs as a more practical and effective option.38,44
Cenobamate has shown particular utility in older adults with focal epilepsy.45 Evidence reports seizure-freedom rates well above those achieved with other third-generation add-ons while simultaneously allowing tapering or discontinuation of concomitant ASMs, thereby reducing polypharmacy-related adverse effect.46,47 When appropriately managed, reducing the burden of concomitant ASMs can lead to significant clinical benefits.46,48 Nonetheless, its pharmacokinetics—near-complete absorption and a terminal half-life of ~50–60 h—support convenient once-daily dosing, an adherence advantage in this age group.49
Concerns about the effect of cenobamate on the QT interval have been minimized by data showing only a slight and clinically insignificant shortening.47,50,51 Moreover, potential pharmacokinetic interactions with oral anticoagulants seem to be negligible, based on current literature.52,53 However, the limited sample sizes in evaluation studies restrict the generalizability of these findings and underscore the need for careful monitoring, as well as further research with larger cohorts.9,33
Use of Cenobamate in Elderly Patients: A Case Vignette
A 65-year-old woman presented with weekly episodes of behavioral arrest, occasionally accompanied by mild oro-alimentary automatisms, lasting a few seconds but followed by prolonged confusion and headache. Over the previous three years, her caregiver observed progressive cognitive decline, including memory deficits and disorientation. Initial evaluation by a general neurologist attributed these episodes to cognitive fluctuations within the context of an underlying dementia. However, following a nocturnal focal-to-bilateral tonic-clonic seizure, an EEG revealed focal epileptiform abnormalities in the left temporal region, supporting a diagnosis of epilepsy. Subsequent brain MRI demonstrated mild medial temporal lobe atrophy (MTA 2), and cerebrospinal fluid (CSF) analysis showed reduced beta-amyloid 42 and elevated phosphorylated tau, indicative of a neurodegenerative disorder within the Alzheimer’s disease (AD) continuum. Neuropsychological assessment confirmed significant deficits in attention, visuospatial abilities, and executive functions, consistent with multi-domain mild cognitive impairment. Treatment was initiated with rivastigmine and levetiracetam, leading to reduced seizure frequency but resulting in behavioral side effects and insomnia. To mitigate such effects, add-on therapy with diazepam was started but poorly tolerated, exacerbating cognitive impairment, while subsequent adjunctive treatment with lacosamide yielded suboptimal seizure control. Cenobamate was introduced, titrated to 200 mg/day, resulting in a substantial reduction in both focal and focal-to-bilateral tonic-clonic seizures, and no reported cenobamate-associated side-effects. Mild dizziness and confusion (“brain fog”) at the target dose were managed by tapering and discontinuing lacosamide and by reducing diazepam dose (4 mg/day). At two years of follow-up, the patient achieved sustained seizure freedom, demonstrated no epileptiform EEG activity, and experienced improvements in neuropsychiatric symptoms and overall quality of life. At last follow up, her concomitant therapy consists of diazepam 4 mg/day.
Epilepsy with Cognitive and Psychiatric Comorbidities
Epilepsy extends beyond seizures to encompass significant cognitive and psychiatric comorbidities that profoundly impact patient outcomes and quality of life.13 Comorbidities, including memory impairment, attention deficits, depression, and anxiety, can arise due to the underlying epilepsy, its treatment, or the psychosocial stressors associated with the condition.14,54 Cognitive impairments in epilepsy are frequent and often reflect the location and extent of epileptogenic areas, with temporal lobe epilepsy frequently associated with memory deficits.13,55,56 Psychiatric comorbidities are also prevalent, with studies indicating that up to one-third of patients with epilepsy experience depression or anxiety at some point in their lives.57–59 These conditions not only impair quality of life but also worsen seizure control and reduce adherence to treatment.14
The interplay between epilepsy and its comorbidities necessitates a tailored treatment approach that balances seizure control while minimizing cognitive and psychiatric adverse effects. Older generation ASMs, although recognized for their historical role in seizure management, are often associated with significant pharmacokinetic side effects, often leading to treatment discontinuation or reduced compliance.60–62
Cenobamate represents a possible breakthrough in this context, as it has been shown to provide robust seizure control with a good general tolerability compared to older therapies.46,63 Emerging evidence suggests that cenobamate is well-tolerated, with no significant adverse effects on cognition, mood, or overall quality of life during both short- and medium-term follow-up.28,63 Notable stabilization of cognitive decline, along with improvements in seizure control and reductions in the use of concomitant ASMs, has been reported following the introduction of cenobamate in patients with drug-resistant epilepsy.31 Moreover, cenobamate pharmacological profile may require a reduction in the burden of concomitant medications.46,64 This may be due to its efficacy but also, on the other hand, to possible pharmacodynamic interactions with concomitant treatments.60,61
Use of Cenobamate in Epilepsy Patients with Cognitive and Psychiatric Comorbidities: A Case Vignette
The case concerns a 30-year-old right-handed male with no family history of epilepsy or psychiatric disorders. The patient’s epilepsy began nine years earlier, at age 21, following a year of minor episodes involving transient loss of awareness, sometimes preceded by déjà-vu, fear, and tachycardia, followed by oro-alimentary automatisms and bilateral dystonic posturing. Despite initiating lamotrigine therapy, monthly seizures persisted.
At age 28 (seven years after onset), the patient developed his first episodes of postictal psychoses, characterized by mystical delusions, psychomotor agitation, and necessity of hospitalization. Episodes emerged within 12 hours after a seizure or a seizure cluster with the intensity of psychiatric symptoms and their duration (from days to two months) directly related with the duration of the preceding seizure cluster. Interictally, he progressively exhibited cognitive slowing and persistent delusional ideation. Neuroimaging, including FDG-PET, showed bilateral temporal hypometabolism, while EEG identified bitemporal epileptiform discharges. Neuropsychological tests showed a significant visual memory impairment with milder deficit of verbal memory and word fluency.
The following year, at age 29, cenobamate was introduced and titrated gradually. At 100 mg/day, seizure frequency and intensity declined, seizure clusters were shortened. At 200 mg/day, the patient achieved seizure freedom for over 18 months, with concurrent gradual but significant improvement of psychiatric symptoms. Mild dizziness and daytime sleepiness, probably due to the interaction between cenobamate and the concomitant treatment, was controlled by tapering carbamazepine, valproate and psychiatric medications. Despite persistent memory deficits, the patient’s quality of life and functional status significantly improved.
DEEs
Epilepsy comprises a heterogeneous spectrum of disorders, many of which are represented by DEEs, characterized by severe and refractory multiple seizure types, developmental delay, neurodevelopmental disorders such as intellectual disability, disturbances of the autistic spectrum, and ADHD.16 Among DEEs, LGS arises from a highly variable etiology, including mutations in ion channels, structural brain abnormalities, or metabolic disorders.65,66 TSC, driven by TSC1 or TSC2 mutations, highlights another genetically defined epilepsy with systemic manifestations and brain structural lesions, linked to the dysregulation of the mTOR pathway.67
Despite diagnostic advances, treatment of severe DEEs remains challenging, as traditional ASMs frequently fail to achieve seizure freedom in these populations, including middle-aged patients lacking a genetic diagnosis who may need a retrospective reconsideration of the therapeutic plan.68–70 In such contexts, where refractory seizures and polytherapy are common, changing the therapeutic plan can be challenging. The application of cenobamate in DEEs remains in its early stages. While its efficacy in focal epilepsy is well-documented, data on syndromes like LGS and TSC, or Dravet are limited, and further research is needed to establish its long-term safety and efficacy in these populations. However, a possible role of cenobamate may be hypothesized, especially due to the need for polytherapy reduction which can lead to a lighter burden of concomitant drug load, if managed properly.69 The good psychiatric and cognitive tolerability profile of the drug may also be taken into account in DEE therapeutic management.71,72
Use of Cenobamate in Epilepsy Patients with DEE: A Case Vignette
A 19-year-old woman with TSC (TSC2 de novo mutation) presented with severe epilepsy and neuropsychiatric comorbidities, including moderate intellectual disability, psychosis, and behavioural disturbances. Seizures began at six months as nocturnal flexion spasms, and evolved into focal, tonic, atonic, and bilateral tonic-clonic episodes, often occurring in clusters. Imaging revealed multiple cortical tubers, subependymal nodules, and calcifications in the left caudate nucleus.
Despite trials of multiple ASMs (vigabatrin, valproate, zonisamide, clonazepam, oxcarbazepine) and adjunctive agents (cannabidiol, everolimus, risperidone), seizures persisted, and behavioural symptoms remained severe.
At the time of referral for clinical worsening (more frequent and prolonged seizures, marked aggression and irritability), her regimen comprised zonisamide 300 mg/day, clonazepam 2 mg/day, oxcarbazepine 1200 mg/day, everolimus 5 mg/day and risperidone 1.5 mL/day. Cenobamate was initiated and titrated to reach 200 mg/day. Within the first month of titration, asthenia, psychomotor slowing and poor adaptive functioning emerged, so zonisamide was reduced to 200 mg/day, oxcarbazepine to 900 mg/day and risperidone to 1 mL/day.
During the second month, seizure freedom was achieved at a cenobamate dose of 100 mg/day and maintained, but low mood, relational withdrawal and psychomotor agitation persisted. Oxcarbazepine was therefore tapered to 600 mg/day, risperidone was discontinued and clotiapine 6 drops/day was introduced. At the five-month review, the patient remained seizure-free, behavioural symptoms were stable and medication burden had been further lightened; quetiapine 25 mg three times daily was added for residual affective lability. The final maintenance regimen consisted of cenobamate 200 mg/day, zonisamide 200 mg/day, oxcarbazepine 600 mg/day, everolimus 5 mg/day, clonazepam eight drops three times daily, clotiapine six drops three times daily and quetiapine 25 mg three times daily.
Surgical and VNS Candidates
Surgical and VNS candidates represent a unique subset of patients with epilepsy, characterized by drug-resistant seizures that significantly impact their quality of life.73 For appropriately selected cases, resective surgery, laser ablation, or neuromodulation can be highly effective options, offering the potential for substantial seizure reduction or even seizure freedom.74–76 The selection of candidates for such approaches depends on detailed presurgical evaluations, including imaging, electrophysiological studies, and neuropsychological assessments, to localize the epileptogenic zone and ensure minimal impact of surgery on functional brain areas.77,78 However, many patients remain ineligible for surgery or do not achieve seizure freedom, necessitating adjunctive therapeutic options.79
While cenobamate cannot replace surgical interventions or neuromodulation in cases where these options are indicated, its integration into treatment regimens may offer a pathway to optimize seizure management. By enhancing seizure control, cenobamate can reduce the frequency of debilitating seizures, improving neuropsychological stability, and providing a bridge for patients awaiting surgical or VNS interventions.
For patients with epilepsy related to structural lesions, such as gliomas or other brain tumors, the interplay between seizure management and oncological treatments further complicates care.80,81 These patients often experience drug-resistance, and the use of enzyme-inducing ASMs warrants caution due to potential interactions with chemotherapeutic agents.73 In this context, cenobamate may represent a relatively viable option, although data on specific interactions with chemotherapeutic agents remain limited. Further studies are needed to evaluate its safety and efficacy in combination with oncological therapies.82
Moreover, surgical candidates with drug-resistant epilepsy may consider the potential of surgery to achieve seizure freedom. Cenobamate may still play a role during the preoperative phase or if surgery fails to achieve complete seizure control.73,83
Use of Cenobamate in Surgical and VNS Candidates: Two Case Vignettes
Case Vignette 1 - A 61-year-old woman with a history of developmental delays, including delayed motor milestones and speech, presented with refractory epilepsy that began at 3 years of age. Initially experiencing absence-like seizures, her condition progressed to include tonic, atonic, and generalized tonic-clonic seizures, alongside episodes characterized by speech arrest and atonia. Diagnosed with epilepsy at age 13, she underwent multiple ASMs over decades, including phenytoin, valproate, and perampanel, without achieving adequate seizure control.
In her late 30s, she underwent left frontal cortectomy due to focal cortical dysplasia, which histological analysis confirmed as architectural cortical disorganization without balloon cells. However, the surgery did not alter her seizure frequency and left her with persistent right-sided hemiparesis, expressive aphasia, and functional impairments requiring full-time caregiving.
By her early 60s, she was experiencing one to two seizures per week, occasionally in clusters. Pre-cenobamate therapy included lacosamide, levetiracetam, perampanel, and primidone, resulting in limited efficacy and significant side effects, including dizziness and worsening fatigue. Cenobamate was initiated and titrated gradually to 200 mg/day. Concurrently, perampanel and levetiracetam were discontinued, lacosamide was reduced, and clonazepam was introduced for tremor management. Ten months after starting cenobamate, seizure frequency had decreased to approximately one brief absence seizure per month, the lowest level recorded in her history. Improvements included enhanced cognition, greater environmental responsiveness, and modest motor function recovery, such as the ability to take steps with assistance.
Case Vignette 2 - A 36-years old female individual with a history of occipito-parietal hemorrhage at one month of age developed focal motor seizures early in life. Following initial recovery, she experienced episodes of nystagmus, head movements, and right homonymous hemianopsia at 18 years old, attributed to a psammomatous meningioma involving the ethmoidal-sphenoidal area, which required surgical resection. This left her with bilateral blindness and persistent focal epilepsy with a variable semiology, including psychomotor arrest, left upper limb myoclonus, and brief tonic episodes leading to falls. Nocturnal seizures were also reported.
Despite sequential exposure to carbamazepine, valproate, perampanel, lacosamide, brivaracetam, and topiramate, the patient continued to experience multiple seizures each week. Three years before referral, a VNS device was implanted, initially shortening seizures but soon failing to prevent clusters, which required diazepam rescue. At that time she was taking lacosamide 400 mg/day, brivaracetam 100 mg/day, topiramate 200 mg/day, and tapering clobazam. One year later, lacosamide was redistributed to 100 + 100 + 200 mg, brivaracetam was doubled to 200 mg/day, topiramate remained 200 mg/day, and buccal midazolam was prescribed as standby (never used); clobazam had been stopped. Nevertheless, variable semiology persisted—psychomotor arrest, left-arm myoclonus, brief tonic falls lasting 5–6 s, and occasional nocturnal events—significantly undermining quality of life and work capacity. The following spring, cenobamate was introduced and titrated over seven months to 200 mg/day. During titration seizures were confined to isolated nocturnal clusters; brivaracetam was halved and then withdrawn, and topiramate was briefly increased to 400 mg/day before gradual tapering. Three months after cenobamate initiation, only three nocturnal seizures were recorded over six weeks, allowing complete discontinuation of brivaracetam. Six months after initiation, the patient reported one to two seizures per month—some in afternoon sleep and often aborted with the VNS magnet—along with markedly improved daily functioning. Topiramate taper continued, and one year after starting cenobamate the regimen consisted of lacosamide 400 mg/day and cenobamate 200 mg/day. Seizure logs for the most recent month noted seven events (five nocturnal, grouped in two clusters), prompting consideration of increasing cenobamate to 250 mg/day.
Expert Opinion
Despite recent diagnostic and therapeutic advances, major implementation gaps remain—especially in tailoring regimens and incorporating newer agents such as cenobamate—underscoring the pressing need to better serve difficult-to-treat epilepsy subpopulations.15
In elderly patients, polypharmacy and age-related pharmacokinetic changes make seizure control particularly challenging. Cenobamate’s once-daily dosing and favourable interaction profile allow clinicians to taper or discontinue concomitant ASMs more easily, improving adherence and diminishing cumulative cognitive and systemic adverse effects that tend to weigh more heavily in this age group.84 Early observational reports describe good overall tolerability; however, the evidence base is still small, and isolated warnings of possible vision-related events counsel prudence. Further, well-designed studies in multimorbid elderly cohorts are therefore needed to confirm safety and to define best practices for dose titration and monitoring.46
Similarly, cenobamate potential to reduce polytherapy has been shown in patients with cognitive impairments, where the therapeutic aim often shifts from achieving cognitive improvement to preventing further decline. Simplifying polytherapy with cenobamate can sometimes unmask previously unnoticed adverse effects of other medications, offering an opportunity to refine treatment strategies.84 In other cases, the reduction of concomitant drug burden appears to be the primary driver of tangible improvements in cognitive function.31 However, these outcomes may depend on individual patient factors, highlighting the need for careful evaluation and monitoring, as well as for research efforts in this direction. The widespread reliance on polytherapy in difficult-to-treat cases remains a challenge, often compounding adverse effects and reducing adherence. Several of the reported cases illustrate how cenobamate may support strategies to simplify treatment regimens, aligning with growing clinical interest in minimizing polypharmacy when feasible.85–87
Patients with DEEs, such as LGS and TSC, may also benefit from cenobamate pharmacological profile. Although Dravet syndrome shares overlapping mechanisms, particularly in terms of ion channel dysfunction, no patients with Dravet were included among the present cases, and the use of sodium channel blockers in this population requires particular caution.86,87 Notably, the early clinical observation of seizure control and behavioural stabilization in other DEE cases is encouraging, especially given the high burden of drug resistance and the frequent coexistence of intellectual disability and psychiatric comorbidities.23 However, the limited inclusion of patients with encephalopathies in pivotal trials such as BLESS underscores the need for dedicated studies to confirm and extend these findings.86,88
Lastly, surgical and VNS candidates represent a unique subset of highly refractory patients requiring special management. Cenobamate has emerged as a valuable complementary therapy in such cases, providing synergic seizure control that can support and enhance surgical or neuromodulation strategies, rather than serving as an alternative.89 In some instances, cenobamate has improved seizure management during preoperative waiting periods, facilitating optimal timing and outcomes for planned surgical procedures.
Cenobamate’s dual mechanism—persistent-Na⁺ current block plus GABA-A potentiation (see Introduction)—likely underlies its efficacy in refractory cases but still requires further study.46 While broadening its therapeutic potential, its pharmacology may also increase the spectrum of potential adverse effects related to both sodium channel blockade and GABAergic modulation. Improved tolerability, where observed, may hence be more attributable to the reduction of concomitant drug burden, highlighting cenobamate overall effectiveness rather than an intrinsic advantage in tolerability. Effective use therefore hinges on meticulous titration and interaction management. The mandatory 10- to 12-week ramp-up, dictated by its ~50–60 h half-life, high protein binding and UGT/CYP metabolism, can delay benefit in urgent or frail cases. Close monitoring and timely adjustment of interacting drugs—especially phenytoin, phenobarbital, N-desmethyl-clobazam, oral contraceptives and lamotrigine—are essential to balance efficacy with safety.26,27,32,46
Epilepsy care is shifting toward precision medicine, where genetic profiling and real-world evidence guide therapy selection. Cenobamate illustrates this potential but still needs robust long-term data on quality of life, cognition, and comorbidities to secure wider adoption.15,86 Over the next decade, integrating such targeted agents with advanced diagnostics could redefine standards of care—provided we overcome access barriers and maintain close, multidisciplinary collaboration across neurology, psychiatry, and genetics to match treatments to individual patient needs.
Limitations
This work is based on a limited number of real-world case vignettes, with each scenario represented by a single illustrative example. As such, the findings should not be interpreted as generalisable evidence but rather as exploratory insights into potential clinical applications of cenobamate in complex settings. While these cases highlight consistent patterns of response and tolerability, they remain anecdotal by nature and are subject to selection and reporting biases. We explicitly acknowledge that conclusions drawn from such anecdotal observations should be interpreted with caution and cannot replace evidence generated through systematic reviews or controlled trials. Broader conclusions will require confirmation through prospective, controlled studies across larger, more diverse patient populations.
Conclusion
Cenobamate appears effective and well-tolerated in difficult-to-treat epilepsy populations—including the elderly, patients with cognitive or psychiatric comorbidities, developmental and epileptic encephalopathies, and surgical or neuromodulation candidates—but its long-term safety and optimal use still need confirmation through large, multi-centre studies with extended follow-up. Early real-world experience shows that cenobamate can deliver substantive seizure reduction while enabling meaningful simplification of polytherapy, thus addressing both seizure control and the broader management burden in these special populations. Rigorous prospective research will be essential to translate these preliminary observations into standard clinical practice and to refine personalised treatment pathways.
Ethical Approval
Ethical approval was not required for this opinion paper because no new data involving human or animal subjects were collected.
Consent for Publication
Informed consent for the publication of the clinical data and case vignettes was obtained from all patients included in this paper. Where applicable, consent was obtained from legal guardians or next of kin.
Acknowledgments
The Authors wish to acknowledge Éthos S.r.l. for providing editorial assistance and technical support.
Funding
This publication was supported by an unrestricted grant from Angelini Pharma S.p.A.. The sponsor did not play any role in the design, execution, interpretation, or writing of this article.
Disclosure
FV, FFO, PP, and TZ declare no conflicts of interest related to this manuscript. FD has served on the scientific advisory boards of Angelini, Eisai, GW/Jazz, UCB Pharma, and Livanova. She has served on speakers’ bureaus or received unrestricted grants from Angelini, Jazz, Eisai, and Livanova, and received personal fees from Angelini, Eisai and Jazz. MP has served on the scientific advisory boards of Angelini, Eisai, GW/Jazz, UCB Pharma, Idorsia, Bioproject, and Livanova. She has served on speakers’ bureaus or received unrestricted grants from Angelini, Jazz, Eisai, Pfizer, UCB Pharma, Idorsia, Livanova, Bioproject, Fidia, and Viatris. CS has received grants from Eisai, Jazz, and Angelini as a speaker.
References
1. Fiest KM, Sauro KM, Wiebe S, et al. Prevalence and incidence of epilepsy: a systematic review and meta-analysis of international studies. Neurology. 2017;88(3):296–303. doi:10.1212/WNL.0000000000003509
2. Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475–482. doi:10.1111/epi.12550
3. Ghosh S, Sinha JK, Ghosh S, Sharma H, Bhaskar R, Narayanan KB. A Comprehensive Review of Emerging Trends and Innovative Therapies in Epilepsy Management. Brain Sci. 2023;13(9):1305. doi:10.3390/brainsci13091305
4. Lezaic N, Roussy J, Masson H, Jette N, Keezer MR. Epilepsy in the elderly: unique challenges in an increasingly prevalent population. Epilepsy Behav. 2020;102:106724. doi:10.1016/j.yebeh.2019.106724
5. Lu E, Pyatka N, Burant CJ, Sajatovic M. Systematic Literature Review of Psychiatric Comorbidities in Adults with Epilepsy. J Clin Neurol. 2021;17(2):176–186. doi:10.3988/jcn.2021.17.2.176
6. Poke G, Stanley J, Scheffer IE, Sadleir LG. Epidemiology of Developmental and Epileptic Encephalopathy and of Intellectual Disability and Epilepsy in Children. Neurology. 2023;100(13):e1363–e1375. doi:10.1212/WNL.0000000000206758
7. Sheng J, Liu S, Qin H, Li B, Zhang X. Drug-Resistant Epilepsy and Surgery. Curr Neuropharmacol. 2018;16(1):17–28. doi:10.2174/1570159X15666170504123316
8. Kotloski RJ, Dowding J, Hermann BP, Sutula TP. Epilepsy and aging. Handbook Clin Neurol. 2019;167:455–475.
9. Piccenna L, O’Dwyer R, Leppik I, et al. Management of epilepsy in older adults: a critical review by the ILAE Task Force on Epilepsy in the elderly. Epilepsia. 2023;64(3):567–585. doi:10.1111/epi.17426
10. Beghi E, Giussani G. Aging and the Epidemiology of Epilepsy. Neuroepidemiology. 2018;51(3–4):216–223. doi:10.1159/000493484
11. Tang DH, Malone DC, Warholak TL, et al. Prevalence and Incidence of Epilepsy in an Elderly and Low-Income Population in the United States. J Clin Neurol. 2015;11(3):252–261. doi:10.3988/jcn.2015.11.3.252
12. Warner DF, Fein HL, Schiltz NK, et al. Incident Epilepsy Among US Medicare Beneficiaries, 2019: differences by Age, Sex, and Race/Ethnicity. Neurology. 2024;103(7):e209804. doi:10.1212/WNL.0000000000209804
13. Novak A, Vizjak K, Rakusa M. Cognitive Impairment in People with Epilepsy. J Clin Med. 2022;11(1):267. doi:10.3390/jcm11010267
14. Kanner AM. Management of psychiatric and neurological comorbidities in epilepsy. Nature reviews. Neurology. 2016;12(2):106–116. doi:10.1038/nrneurol.2015.243
15. Beghi E, Giussani G, Costa C, et al. The epidemiology of epilepsy in older adults: a narrative review by the ILAE Task Force on Epilepsy in the Elderly. Epilepsia. 2023;64(3):586–601. doi:10.1111/epi.17494
16. Noh GJ, Jane Tavyev Asher Y, Graham Jr JM. Clinical review of genetic epileptic encephalopathies. Eur J Med Genet. 2012;55(5):281–298. doi:10.1016/j.ejmg.2011.12.010
17. Strzelczyk A, Zuberi SM, Striano P, Rosenow F, Schubert-Bast S. The burden of illness in Lennox-Gastaut syndrome: a systematic literature review. Orphanet J Rare Diseases. 2023;18(1):42. doi:10.1186/s13023-023-02626-4
18. Boon P, De Cock E, Mertens A, Trinka E. Neurostimulation for drug-resistant epilepsy: a systematic review of clinical evidence for efficacy, safety, contraindications and predictors for response. Curr Opin Neurol. 2018;31(2):198–210. doi:10.1097/WCO.0000000000000534
19. Starnes K, Miller K, Wong-Kisiel L, Lundstrom BN. A Review of Neurostimulation for Epilepsy in Pediatrics. Brain Sci. 2019;9(10):283. doi:10.3390/brainsci9100283
20. Fattorusso A, Matricardi S, Mencaroni E, et al. The Pharmacoresistant Epilepsy: an Overview on Existent and New Emerging Therapies. Front Neurol. 2021;12:674483. doi:10.3389/fneur.2021.674483
21. Gonzalez HFJ, Yengo-Kahn A, Englot DJ. Vagus Nerve Stimulation for the Treatment of Epilepsy. Neurosurgery Clin North America. 2019;30(2):219–230. doi:10.1016/j.nec.2018.12.005
22. Chin RF, Mingorance A, Ruban-Fell B, et al. Treatment Guidelines for Rare, Early-Onset, Treatment-Resistant Epileptic Conditions: a Literature Review on Dravet Syndrome, Lennox-Gastaut Syndrome and CDKL5 Deficiency Disorder. Front Neurol. 2021;12:734612. doi:10.3389/fneur.2021.734612
23. Buckley CT, Waters OR, DeMaagd G. Cenobamate: a New Adjunctive Agent for Drug-Resistant Focal Onset Epilepsy. Ann Pharmacother. 2021;55(3):318–329. doi:10.1177/1060028020941113
24. Krauss GL, Klein P, Brandt C, et al. Safety and efficacy of adjunctive cenobamate (YKP3089) in patients with uncontrolled focal seizures: a multicentre, double-blind, randomised, placebo-controlled, dose-response trial. Lancet Neurol. 2020;19(1):38–48. doi:10.1016/S1474-4422(19)30399-0
25. FDA. Cenobamate. Full prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212839s000lbl.pdf. Accessed 25, June 2024.
26. Perucca E, Bialer M, White HS. New GABA-Targeting Therapies for the Treatment of Seizures and Epilepsy: i. Role of GABA as a Modulator of Seizure Activity and Recently Approved Medications Acting on the GABA System. CNS Drugs. 2023;37(9):755–779. doi:10.1007/s40263-023-01027-2
27. Schmitz B, Lattanzi S, Vonck K, Kalviainen R, Nashef L, Ben-Menachem E. Cenobamate in refractory epilepsy: overview of treatment options and practical considerations. Epilepsia Open. 2023;8(4):1241–1255. doi:10.1002/epi4.12830
28. Catalan-Aguilar J, Hampel KG, Cano-Lopez I, et al. Prospective study of cenobamate on cognition, affectivity, and quality of life in focal epilepsy. Epilepsia Open. 2024;9(1):223–235. doi:10.1002/epi4.12857
29. French JA. Cenobamate for focal seizures - a game changer? Nature reviews. Neurology. 2020;16(3):133–134. doi:10.1038/s41582-019-0309-7
30. Pietrafusa N, Falcicchio G, Russo E, et al. Cenobamate as add-on therapy for drug resistant epilepsies: effectiveness, drug to drug interactions and neuropsychological impact. What have we learned from real word evidence? Front Pharmacol. 2023;14:1239152. doi:10.3389/fphar.2023.1239152
31. Serrano-Castro PJ, Ramirez-Garcia T, Cabezudo-Garcia P, Garcia-Martin G, De La Parra J. Effect of Cenobamate on Cognition in Patients with Drug-Resistant Epilepsy with Focal Onset Seizures: an Exploratory Study. CNS Drugs. 2024;38(2):141–151. doi:10.1007/s40263-024-01063-6
32. Villani F, Cianci V, Di Bonaventura C, et al. Use of cenobamate for the treatment of focal epilepsy: an Italian expert opinion paper. Expert Rev Neurother. 2022;22(11–12):935–940. doi:10.1080/14737175.2023.2171291
33. Lattanzi S, Trinka E, Zaccara G, et al. Adjunctive Cenobamate for Focal-Onset Seizures in Adults: a Systematic Review and Meta-Analysis. CNS Drugs. 2020;34(11):1105–1120. doi:10.1007/s40263-020-00759-9
34. Lattanzi S, Trinka E, Zaccara G, et al. Third-Generation Antiseizure Medications for Adjunctive Treatment of Focal-Onset Seizures in Adults: a Systematic Review and Network Meta-analysis. Drugs. 2022;82(2):199–218. doi:10.1007/s40265-021-01661-4
35. Mulheron S, Leahy TP, McStravick M, Doran R, Delanty N. A comparison of cenobamate with other newer antiseizure medications for adjunctive treatment of focal-onset seizures: a systematic review and network meta-analysis. Seizure. 2024;118:80–90. doi:10.1016/j.seizure.2024.04.004
36. Rosenfeld WE. Epilepsy medication management: addressing common treatment barriers to adopting cenobamate and other new antiseizure medications. Epilepsia. 2025;66(1):38–48. doi:10.1111/epi.18305
37. Kramer G. Epilepsy in the elderly: some clinical and pharmacotherapeutic aspects. Epilepsia. 2001;42(3):55–59. doi:10.1046/j.1528-1157.2001.042suppl.3055.x
38. Werhahn KJ. Epilepsy in the elderly. Deutsches Arzteblatt Int. 2009;106(9):135–142. doi:10.3238/arztebl.2009.0135
39. Toniolo S, Romoli M, Sen A. Epilepsy in Older Persons. Neurol Clini. 2022;40(4):891–905. doi:10.1016/j.ncl.2022.03.014
40. Acharya JN, Acharya VJ. Epilepsy in the elderly: special considerations and challenges. Ann Indian Acad Neurol. 2014;17(Suppl 1):S18–26. doi:10.4103/0972-2327.128645
41. Baysal L, Ludolph AC, Wagner J. Clinical and paraclinical features of first unprovoked seizures in the elderly. Epilepsy Behav. 2024;158:109926. doi:10.1016/j.yebeh.2024.109926
42. Naeije G, Gaspard N, Depondt C, Pepersack T, Legros B. Acute confusional state of unknown cause in the elderly: a study with continuous EEG monitoring. Epilepsy Behav. 2012;23(3):330–334. doi:10.1016/j.yebeh.2012.01.023
43. Sambin S, Gaspard N, Legros B, Depondt C, De Breucker S, Naeije G. Role of Epileptic Activity in Older Adults With Delirium, a Prospective Continuous EEG Study. Front Neurol. 2019;10:263. doi:10.3389/fneur.2019.00263
44. Ramsay RE, Rowan AJ, Pryor FM. Special considerations in treating the elderly patient with epilepsy. Neurology. 2004;62(5 Suppl 2):S24–29. doi:10.1212/WNL.62.5_suppl_2.S24
45. O’Dwyer R, Stern S, Wade CT, Guggilam A, Rosenfeld WE. Safety and Efficacy of Cenobamate for the Treatment of Focal Seizures in Older Patients: post Hoc Analysis of a Phase III, Multicenter, Open-Label Study. Drugs Aging. 2024;41(3):251–260. doi:10.1007/s40266-024-01102-3
46. Roberti R, De Caro C, Iannone LF, Zaccara G, Lattanzi S, Russo E. Pharmacology of Cenobamate: mechanism of Action, Pharmacokinetics, Drug-Drug Interactions and Tolerability. CNS Drugs. 2021;35(6):609–618. doi:10.1007/s40263-021-00819-8
47. Darpo B, Sager PT, Xue H, Kamin M. A Phase 1 Clinical Study Evaluating the Effects of Cenobamate on the QT Interval. Clin Pharmacol Drug Dev. 2022;11(4):523–534. doi:10.1002/cpdd.1077
48. Aboumatar S, Ferrari L, Stern S, et al. Reductions in concomitant antiseizure medication drug load during adjunctive cenobamate therapy: post-hoc analysis of a subset of patients from a Phase 3, multicenter, open-label study. Epilepsy Res. 2024;200:107306. doi:10.1016/j.eplepsyres.2024.107306
49. Vernillet L, Greene SA, Kamin M. Pharmacokinetics of Cenobamate: results From Single and Multiple Oral Ascending-Dose Studies in Healthy Subjects. Clin Pharmacol Drug Dev. 2020;9(4):428–443. doi:10.1002/cpdd.769
50. Butany J, Ahn E, Luk A. Drug-related cardiac pathology. J Clin Pathol. 2009;62(12):1074–1084. doi:10.1136/jcp.2008.058255
51. Feldman AE, Gidal BE. QTc prolongation by antiepileptic drugs and the risk of torsade de pointes in patients with epilepsy. Epilepsy Behav. 2013;26(3):421–426. doi:10.1016/j.yebeh.2012.09.021
52. Candeloro M, Carlin S, Shapiro MJ, Douketis JD. Drug-drug interactions between direct oral anticoagulants and anticonvulsants and clinical outcomes: a systematic review. Research and practice in thrombosis and haemostasis. Research and Practice in Thrombosis and Haemostasis. 2023;7(3):100137. doi:10.1016/j.rpth.2023.100137
53. Steinhoff BJ, Ben-Menachem E, Klein P, et al. Therapeutic strategies during cenobamate treatment initiation: delphi panel recommendations. Ther Adv Neurol Disorders. 2024;17:17562864241256733. doi:10.1177/17562864241256733
54. Helmstaedter C, Kurthen M, Lux S, Reuber M, Elger CE. Chronic epilepsy and cognition: a longitudinal study in temporal lobe epilepsy. Ann Neurol. 2003;54(4):425–432. doi:10.1002/ana.10692
55. Ives-Deliperi V, Butler JT. Mechanisms of cognitive impairment in temporal lobe epilepsy: a systematic review of resting-state functional connectivity studies. Epilepsy Behav. 2021;115:107686. doi:10.1016/j.yebeh.2020.107686
56. Elger CE, Helmstaedter C, Kurthen M. Chronic epilepsy and cognition. Lancet. 2004;3(11):663–672. doi:10.1016/S1474-4422(04)00906-8
57. Mula M, Kanner AM, Jette N, Sander JW. Psychiatric Comorbidities in People With Epilepsy. Neurology. 2021;11(2):e112–e120. doi:10.1212/CPJ.0000000000000874
58. Kwon CS, Rafati A, Ottman R, et al. Psychiatric Comorbidities in Persons With Epilepsy Compared With Persons Without Epilepsy: a Systematic Review and Meta-Analysis. JAMA Neurol. 2024;81(6):611–618. doi:10.1001/jamaneurol.2024.0967
59. Kwon CS, Rafati A, Gandy M, Scott A, Newton CR, Jette N. Multipsychiatric Comorbidity in People With Epilepsy Compared With People Without Epilepsy: a Systematic Review and Meta-analysis. Neurology. 2024;103(3):e209622. doi:10.1212/WNL.0000000000209622
60. Eddy CM, Rickards HE, Cavanna AE. The cognitive impact of antiepileptic drugs. Ther Adv Neurol Disorders. 2011;4(6):385–407. doi:10.1177/1756285611417920
61. Iivanainen M, Savolainen H. Side effects of phenobarbital and phenytoin during long-term treatment of epilepsy. Acta Neurol Scand. 1983;97:49–67. doi:10.1111/j.1600-0404.1983.tb01535.x
62. Gunasekera CL, Sirven JI, Feyissa AM. The evolution of antiseizure medication therapy selection in adults: is artificial intelligence -assisted antiseizure medication selection ready for prime time? J Central Nervous Syst Dis. 2023;15:11795735231209209. doi:10.1177/11795735231209209
63. Krauss GL, Chung SS, Ferrari L, Stern S, Rosenfeld WE. Cognitive and psychiatric adverse events during adjunctive cenobamate treatment in Phase 2 and phase 3 clinical studies. Epilepsy Behav. 2024;151:109605. doi:10.1016/j.yebeh.2023.109605
64. Smith MC, Klein P, Krauss GL, et al. Dose Adjustment of Concomitant Antiseizure Medications During Cenobamate Treatment: expert Opinion Consensus Recommendations. Neurol ther. 2022;11(4):1705–1720. doi:10.1007/s40120-022-00400-5
65. Pal DK, Pong AW, Chung WK. Genetic evaluation and counseling for epilepsy. Nat Rev Neurol. 2010;6(8):445–453. doi:10.1038/nrneurol.2010.92
66. Striano P, Minassian BA. From Genetic Testing to Precision Medicine in Epilepsy. Neurotherapeutics. 2020;17(2):609–615. doi:10.1007/s13311-020-00835-4
67. Curatolo P. Mechanistic target of rapamycin (mTOR) in tuberous sclerosis complex-associated epilepsy. Pediatr Neurol. 2015;52(3):281–289. doi:10.1016/j.pediatrneurol.2014.10.028
68. Bayat A, Fenger CD, Techlo TR, et al. Impact of Genetic Testing on Therapeutic Decision-Making in Childhood-Onset Epilepsies-a Study in a Tertiary Epilepsy Center. Neurotherapeutics. 2022;19(4):1353–1367. doi:10.1007/s13311-022-01264-1
69. Witt JA, Elger CE, Helmstaedter C. Adverse cognitive effects of antiepileptic pharmacotherapy: each additional drug matters. Eur Neuropsychopharmacol. 2015;25(11):1954–1959. doi:10.1016/j.euroneuro.2015.07.027
70. Nabbout R, Camfield CS, Andrade DM, et al. Treatment issues for children with epilepsy transitioning to adult care. Epilepsy Behav. 2017;69:153–160. doi:10.1016/j.yebeh.2016.11.008
71. Latimer DR, Edinoff AN, Ruff RD, et al. Cenobamate, a Sodium Channel Inhibitor and Positive Allosteric Modulator of GABA(A) Ion Channels, for Partial Onset Seizures in Adults: a Comprehensive Review and Clinical Implications. Neurol Int. 2021;13(2):252–265. doi:10.3390/neurolint13020026
72. Falcicchio G, Lattanzi S, Negri F, de Tommaso M, La Neve A, Specchio N. Treatment with Cenobamate in Adult Patients with Lennox-Gastaut Syndrome: a Case Series. J Clin Med. 2022;12(1):129. doi:10.3390/jcm12010129
73. Smith KC. The management of seizures in brain tumor patients. J Neurosci Nurs. 2010;42(1):28–37;quiz38–29. doi:10.1097/JNN.0b013e3181c1fd83
74. Roa JA, Marcuse L, Fields M, et al. Long-term outcomes after responsive neurostimulation for treatment of refractory epilepsy: a single-center experience of 100 cases. J Neurosurg. 2023;139(5):1463–1470. doi:10.3171/2023.2.JNS222116
75. Cramer SW, McGovern RA, Wang SG, Chen CC, Park MC. Resective epilepsy surgery: assessment of randomized controlled trials. Neurosurgical Rev. 2021;44(4):2059–2067. doi:10.1007/s10143-020-01432-x
76. Kerezoudis P, Lundstrom BN, Meyer FB, Worrell GA, Van Gompel JJ. Surgical approaches to refractory central lobule epilepsy: a systematic review on the role of resection, ablation, and stimulation in the contemporary era. J Neurosurg. 2022;137(3):735–746. doi:10.3171/2021.10.JNS211875
77. Romanelli P, Striano P, Barbarisi M, Coppola G, Anschel DJ. Non-resective surgery and radiosurgery for treatment of drug-resistant epilepsy. Epilepsy Res. 2012;99(3):193–201. doi:10.1016/j.eplepsyres.2011.12.016
78. Kini LG, Bernabei JM, Mikhail F, et al. Virtual resection predicts surgical outcome for drug-resistant epilepsy. Brain. 2019;142(12):3892–3905. doi:10.1093/brain/awz303
79. Perucca P, Scheffer IE, Kiley M. The management of epilepsy in children and adults. Med J Australia. 2018;208(5):226–233. doi:10.5694/mja17.00951
80. Maschio M, Beghi E, Casazza MML, et al. Patterns of care of brain tumor-related epilepsy. A cohort study done in Italian Epilepsy Center. PLoS One. 2017;12(7):e0180470. doi:10.1371/journal.pone.0180470
81. Adhikari S, Walker BC, Mittal S. Pathogenesis and Management of Brain Tumor-Related Epilepsy. Debinski W, ed.. Brisbane (AU): Gliomas; 2021.
82. Weller M, Stupp R, Wick W. Epilepsy meets cancer: when, why, and what to do about it? Lancet Oncol. 2012;13(9):e375–382. doi:10.1016/S1470-2045(12)70266-8
83. Laxer KD, Elder CJ, Di Gennaro G, et al. Presurgical Use of Cenobamate for Adult and Pediatric Patients Referred for Epilepsy Surgery: expert Panel Recommendations. Neurol ther. 2024;13(5):1337–1348. doi:10.1007/s40120-024-00651-4
84. Rodriguez-Uranga JJ, Sanchez-Caro JM, Hariramani Ramchandani R. Treatment simplification to optimize cenobamate effectiveness and tolerability: a real-world retrospective study in Spain. Epilepsia Open. 2024;9(4):1345–1356. doi:10.1002/epi4.12959
85. Terman SW, Aubert CE, Hill CE, et al. Polypharmacy in patients with epilepsy: a nationally representative cross-sectional study. Epilepsy Behav. 2020;111:107261. doi:10.1016/j.yebeh.2020.107261
86. Specchio N, Pietrafusa N, Vigevano F. Is Cenobamate the Breakthrough We Have Been Wishing for? Int J Mol Sci. 2021;22(17):9339. doi:10.3390/ijms22179339
87. Brigo F, Lattanzi S. Cenobamate add-on therapy for drug-resistant focal epilepsy. Cochrane Database Syst Rev. 2024;8(8):CD014941. doi:10.1002/14651858.CD014941.pub2
88. Lattanzi S, Ranzato F, Di Bonaventura C, et al. Effectiveness and Safety of Adjunctive Cenobamate in People with Focal-Onset Epilepsy: evidence from the First Interim Analysis of the BLESS Study. Neurol ther. 2024;13(4):1203–1217. doi:10.1007/s40120-024-00634-5
89. Jobst BC, Cascino GD. Resective epilepsy surgery for drug-resistant focal epilepsy: a review. JAMA. 2015;313(3):285–293. doi:10.1001/jama.2014.17426
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.