Back to Journals » Infection and Drug Resistance » Volume 15
Ceftolozane/Tazobactam Activity Against Drug-Resistant Pseudomonas aeruginosa and Enterobacterales Causing Healthcare-Associated Infections in Eight Asian Countries: Report from an Antimicrobial Surveillance Program (2016–2018)
Authors Pfaller M, Shortridge D, Chen WT, Sader H, Castanheira M
Received 30 August 2022
Accepted for publication 14 November 2022
Published 22 November 2022 Volume 2022:15 Pages 6739—6753
DOI https://doi.org/10.2147/IDR.S387097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Michael Pfaller,1,2 Dee Shortridge,1 Wei-Ting Chen,3 Helio Sader,1 Mariana Castanheira1
1JMI Laboratories, North Liberty, IA, USA; 2University of Iowa College of Medicine, Iowa City, IA, USA; 3Merck & Co., Inc, Kenilworth, NJ, USA
Correspondence: Dee Shortridge, JMI Laboratories, 345 Beaver Kreek Centre, Suite A, North Liberty, IA, 52317, USA, Tel +1 319-665-3370, Fax +1319-665-3371, Email [email protected]
Purpose: To evaluate the in vitro activity of ceftolozane/tazobactam and comparator agents tested against Pseudomonas aeruginosa and Enterobacterales isolates from hospitalised patients in Asia. Ceftolozane/tazobactam is an antipseudomonal cephalosporin combined with a well-established β-lactamase inhibitor.
Methods: A total of 2038 Gram-negative organisms (376 P. aeruginosa and 1662 Enterobacterales) were collected consecutively using a prevalence-based approach from 11 medical centres. Organisms were susceptibility tested by broth microdilution according to CLSI guidelines. CLSI and EUCAST breakpoint criteria were used.
Results: Ceftolozane/tazobactam was the most potent (MIC50/90, 0.5/4 mg/L) β-lactam agent tested against P. aeruginosa isolates, inhibiting 91.0% of the isolates at an MIC of ≤ 4 mg/L. P. aeruginosa exhibited high rates of susceptibility to amikacin (92.0/92.0% [CLSI/EUCAST]) and colistin by EUCAST criteria only (99.2% intermediate [CLSI]/99.2% susceptible [EUCAST]). Ceftolozane/tazobactam (MIC50/90, 0.25/16 mg/L; 86.8/86.8% susceptible [CLSI/EUCAST]) and meropenem (MIC50/90, 0.03/0.12 mg/L; 93.0/93.3% susceptible [CLSI/EUCAST]) were the most active compounds tested against Enterobacterales. Isolates displayed susceptibility rates to other β-lactam agents, ranging from 81.5/77.7% for piperacillin/tazobactam, 66.0/64.5% for cefepime, and 65.3/60.9% for ceftazidime using CLSI/EUCAST breakpoints. Among the Enterobacterales isolates, 6.8% were carbapenem-resistant Enterobacterales (CRE) and 29.6% exhibited an extended-spectrum β-lactamase (ESBL) non-CRE phenotype. Ceftolozane/tazobactam showed good activity against ESBL non-CRE phenotype strains of Enterobacterales (MIC50/90, 0.5/8 mg/L; 84.8/84.8% susceptible), but not against isolates with a CRE phenotype (MIC50/90, > 32/> 32 mg/L).
Conclusion: Ceftolozane/tazobactam was the most active β-lactam agent tested against P. aeruginosa and demonstrated higher in vitro activity than the available cephalosporins when tested against Enterobacterales from Asian countries.
Keywords: Asia, ceftolozane/tazobactam, drug resistance, Enterobacterales, P. aeruginosa, surveillance
Introduction
Antimicrobial resistance (AMR) is a grave threat to the global healthcare system.1–5 Whereas Gram-positive cocci remain a concern due to methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci, recent years have seen the emergence of multidrug-resistant (MDR; resistant to 3 or more classes of antimicrobial agents) strains of Gram-negative bacilli (GNB).1–5 MDR GNBs are especially prominent in Asian countries compared to the United States (US) and western Europe.1,4,6–16 Regional variation in antimicrobial susceptibility is considerable in Asia1,7,8,10,11 due in part to the lack of diagnostic laboratory facilities outside of major cities, varying standards of antimicrobial usage, self-medication, poor adherence to complete antimicrobial regimens, low quality and often counterfeit antimicrobials, and differing standards of public hygiene between countries.6,12
Enterobacterales and Pseudomonas aeruginosa constitute the greatest source of AMR in hospitalised individuals.1–5 These GNBs account for 70% of hospital-associated infections (HAIs) acquired in the intensive care unit (ICU) and respond to the pressure of antimicrobial exposure with the development of resistance to various classes of agents, often resulting in an MDR phenotype.1–5 The MDR nature of these pathogens is associated with delays in appropriate therapy and corresponding increases in morbidity and mortality.5,17–19 Therapeutic options for treating infections caused by MDR GNBs are extremely limited, with only a few agents, such as the carbapenems, providing sufficient coverage.2,3,5,17,20
Ceftolozane/tazobactam is a β-lactam/ β-lactamase inhibitor combination that represents a potential carbapenem-sparing treatment option for extended-spectrum β-lactamase (ESBL)-producing Enterobacterales and MDR P. aeruginosa.13,20–22 Ceftolozane/tazobactam has potent activity against P. aeruginosa, including antibiotic-resistant strains, as well as Enterobacterales, including most ESBL-producing strains.13,20,23–26 Ceftolozane/tazobactam has limited activity against Acinetobacter spp., Stenotrophomonas maltophilia, and GPC or against organisms producing carbapenemases, metallo-β-lactamases, and a small number of AmpC β-lactamases found in Enterobacterales strains.13,20–22 Ceftolozane/tazobactam has been approved by the US and Europe for the treatment of complicated intra-abdominal infections (cIAI) and complicated urinary tract infections (cUTI) with a dose of 1.5 grams of ceftolozane/tazobactam every 8 hrs, and hospital-acquired bacterial pneumonia/ventilator-associated bacterial pneumonia with a higher dose of 3.0 grams of ceftolozane/tazobactam q 8 hrs.20,22
In the present study, we examined the activity of ceftolozane/tazobactam and comparators against 2038 isolates of P. aeruginosa and Enterobacterales from hospitalised patients at 11 medical centres in 8 countries in Asia from 2016 to 2018 collected in the SENTRY Antimicrobial Surveillance Program. Our analysis includes the activity of ceftolozane/tazobactam against specific resistant phenotypes (ESBL non-CRE phenotype and MDR strains of Enterobacterales and P. aeruginosa) and the frequency of resistance patterns in each of these 8 Asian countries.
Materials and Methods
Sampling Sites and Organisms
A total of 2038 non-duplicate isolates of GNB, including 1662 Enterobacterales and 376 P. aeruginosa, were collected consecutively across 4 infection types from 11 medical centres located in 8 countries in Asia from 2016 to 2018. These centres were participants in the SENTRY Antimicrobial Surveillance Program. All centres followed a common protocol for isolate collection, which was previously described.27 Only 1 isolate per patient per infection type was submitted (1 infection per patient). All organisms were isolated from hospitalised patients with bloodstream infection (554 isolates), pneumonia in hospitalised patients (521 isolates), skin and skin structure infection (370 isolates), intra-abdominal infection (185 isolates), and other sites (32 isolates). Species identification was performed at each participating medical centre and confirmed by the monitoring laboratory (JMI Laboratories, North Liberty, Iowa, USA) using matrix-assisted laser desorption ionization-time of flight mass spectrometry (Bruker, Billerica, Massachusetts, USA) or standard biochemicals when necessary.
Antimicrobial Susceptibility Testing
Minimal inhibitory concentrations (MICs) were determined using the frozen broth microdilution method as described by the Clinical and Laboratory Standards Institute (CLSI).28 Ceftolozane/tazobactam and piperacillin/tazobactam were both tested with a fixed tazobactam concentration of 4 mg/L. Quality control and the interpretation of results were performed according to CLSI M100-S31 and European Committee on Antimicrobial Susceptibility Testing (EUCAST) 2021 guidelines.29,30 Escherichia coli, Klebsiella pneumoniae, Klebsiella oxytoca, and Proteus mirabilis were grouped as an ESBL screen-positive phenotype based on the CLSI screening criteria for presumptive ESBL production, i.e., ceftazidime, ceftriaxone, or aztreonam MICs ≥2 mg/L.29 CRE isolates were defined as those displaying MIC values ≥4 mg/L for imipenem (P. mirabilis and indole-positive Proteae were not included due to intrinsically elevated MIC values), meropenem, and/or doripenem.29 Results for doripenem and imipenem were used, along with meropenem, to determine the presumptive CRE phenotype and are not reported individually. In version 10.0 of the EUCAST breakpoints, the Enterobacterales and P. aeruginosa breakpoints of several antimicrobial agents (aztreonam, ciprofloxacin, cefepime, ceftazidime, imipenem, and piperacillin/tazobactam) were changed to recategorize all isolates in the wild-type population as “susceptible, increased exposure”. The arbitrary susceptible breakpoint of ≤0.001 mg/L was chosen by EUCAST to ensure that no isolates were labeled susceptible to these agents. As a result, P. aeruginosa isolates previously susceptible to aztreonam, cefepime, ceftazidime, ciprofloxacin, imipenem, and piperacillin/tazobactam as well as previously imipenem-susceptible isolates of Morganella morganii, Proteus spp., and Providencia spp. are shown in parentheses in the table as susceptible, increased exposure. In addition, CLSI removed the susceptible category for colistin, reporting only intermediate or resistant categories for Enterobacterales and P. aeruginosa.
P. aeruginosa isolates were classified as ceftazidime-nonsusceptible (NS; MIC, >8 mg/L), levofloxacin-NS (MIC, >1 mg/L), meropenem-NS (MIC, >2 mg/L), or piperacillin/tazobactam-NS (MIC, >16 mg/L). Multidrug-resistant (MDR; nonsusceptible to at least 3 antimicrobial classes) and extensively drug resistant (XDR; susceptible to 2 or fewer antimicrobial classes) P. aeruginosa isolates were classified according to Magiorakos et al and used the following antimicrobial class representative agents: ceftazidime, doripenem, gentamicin, levofloxacin, meropenem, piperacillin/tazobactam, tigecycline (for species with breakpoints), and colistin (7 classes).31 Results for doripenem and tigecycline were used to determine the MDR phenotype and are not reported individually.
Results
Among the 2038 isolates tested, there were 1662 Enterobacterales isolates (including 716 E. coli, 610 Klebsiella spp., 152 Enterobacter spp., 50 Citrobacter spp., 48 P. mirabilis, 25 indole-positive Proteae, and 53 Serratia marcescens) and 376 P. aeruginosa isolates (Table 1). Countries that provided the isolates for this survey included Japan (85 isolates), Korea (496), Malaysia (279), Philippines (430), Singapore (60), Taiwan (241), Thailand (346), and Vietnam (101).
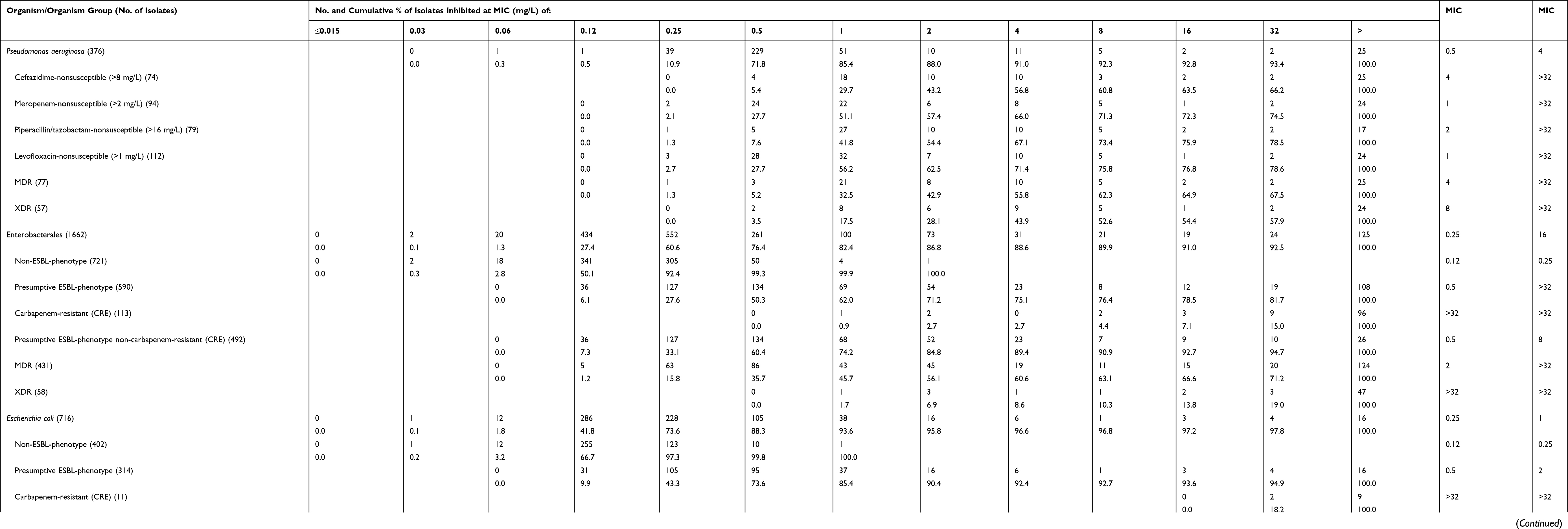 |
Table 1 Antimicrobial Activity of Ceftolozane/Tazobactam Tested Against the Main Organisms and Organism Groups |
Overall Activity of Ceftolozane/Tazobactam
During the years 2016 to 2018, ceftolozane/tazobactam maintained a consistent and potent level of activity against the target pathogens from the study sites in Asia (Table 1). Ceftolozane/tazobactam MIC values ranged from 0.06 mg/L to >32 mg/L against isolates of P. aeruginosa, and 91.0% of the tested isolates were susceptible at the CLSI/EUCAST breakpoint of ≤4 mg/L. Among the resistant phenotypes, 56.8% (ceftazidime-NS), 71.4% (levofloxacin-NS), 66.0% (meropenem-NS), 67.1% (piperacillin/tazobactam-NS), 55.8% (MDR), and 43.9% (XDR) isolates were susceptible to ceftolozane/tazobactam (Table 1).
Among the Enterobacterales isolates tested, 6.8% were CRE (range 0.0% [Japan and Singapore] to 26.6% [Vietnam]) and 29.6% exhibited a presumptive ESBL non-CRE phenotype (range 7.3% [Singapore] to 40.4% [Vietnam]) (Table 2). A presumptive ESBL non-CRE phenotype was observed in 42.3% of E. coli (range 30.0% [Singapore] to 65.4% [Vietnam]) and 32.0% of K. pneumoniae (range 0.0% [Singapore] to 40.7% [Korea]) isolates. Important resistant phenotypes among the P. aeruginosa isolates included ceftazidime-NS (19.7%; range 10.8% [Taiwan] to 28.6% [Vietnam]), meropenem-NS (25.0%; range 10.3% [Philippines] to 35.6% [Thailand]), piperacillin/tazobactam-NS (21.0%; range 8.3% [Malaysia] to 32.1% [Korea]), MDR (20.5%; range 10.3% [Philippines] to 32.1% [Korea]) and XDR (15.2%; range 8.3% [Malaysia] to 28.6% [Vietnam]) (Table 2).
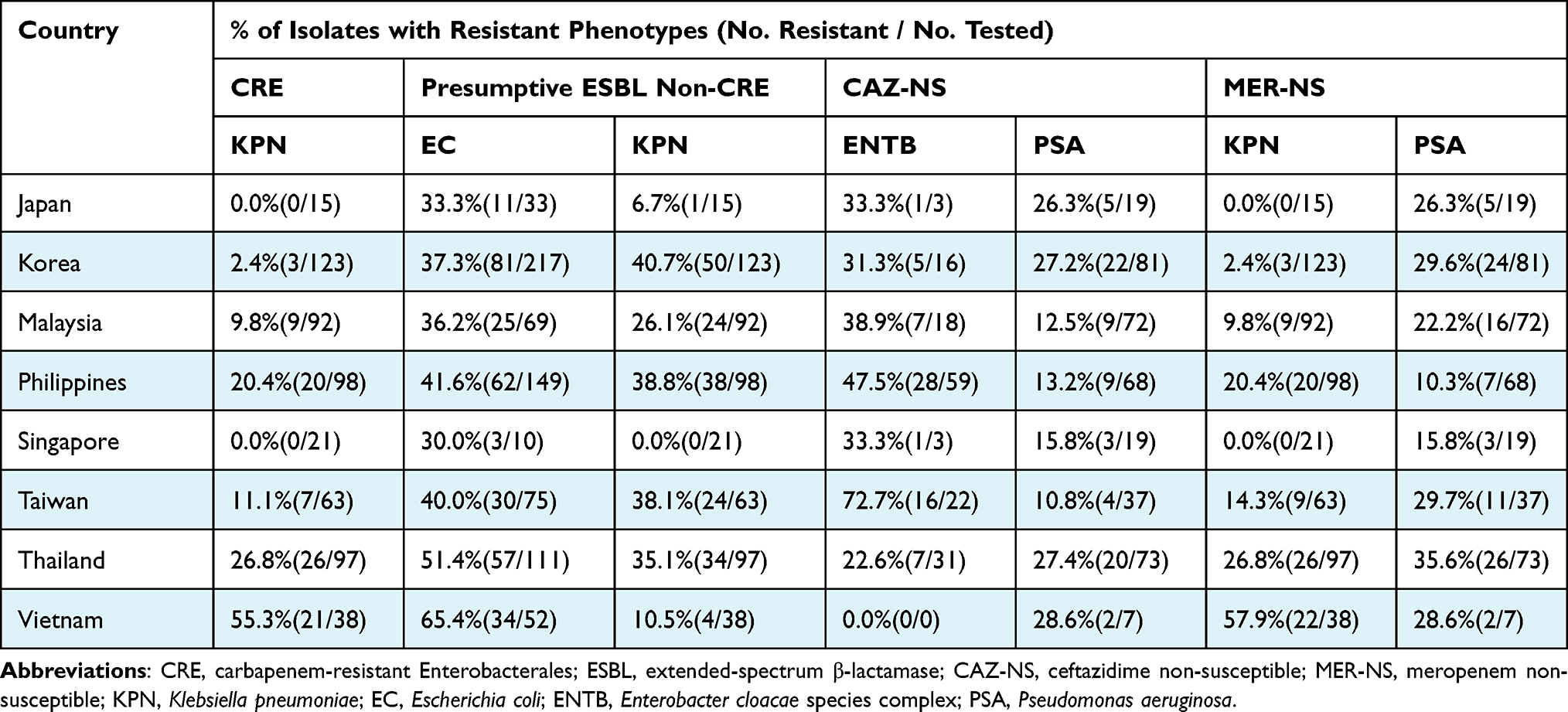 |
Table 2 Geographical Distribution of Phenotypically Resistant Isolates |
Ceftolozane/tazobactam MIC values ranged from 0.03 to >32 mg/L, and 86.8% of the tested Enterobacterales isolates were inhibited at an MIC value of ≤2 mg/L (88.6% at ≤4 mg/L) (Table 1). Whereas ceftolozane/tazobactam showed good activity against presumptive ESBL non-CRE phenotype strains of Enterobacterales (MIC50/90, 0.5/8 mg/L; 84.8/84.8% susceptible [CLSI/EUCAST]), it lacked useful activity (MIC50/90, >32/>32 mg/L) against isolates with a presumptive CRE phenotype.
Activities of Ceftolozane/Tazobactam and Comparators Against P. aeruginosa
Ceftolozane/tazobactam was the most active (MIC50//90, 0.5/4 mg/L) β-lactam agent tested against 376 P. aeruginosa isolates, inhibiting 91.0% of the isolates at a MIC of ≤4 mg/L (Tables 1 and 3). Overall susceptibility rates (Table 3) for cefepime (83.5% susceptible [CLSI] and 83.5% susceptible-increased exposure [EUCAST]), ceftazidime (80.3% susceptible [CLSI] and 80.3% susceptible-increased exposure [EUCAST]), meropenem (75.0/75.0% susceptible [CLSI/EUCAST]) and piperacillin/tazobactam (79.0% susceptible [CLSI] and 79.0% susceptible-increased exposure [EUCAST]), were all below that of ceftolozane/tazobactam at ≤4 mg/L (91.0/91.0% susceptible [CLSI/EUCAST]; Table 3). Both amikacin (MIC50/90, 4/16 mg/L; 92.0/92.0% susceptible [CLSI/EUCAST]) and colistin (MIC50/90, 1/1 mg/L; 99.2% intermediate [CLSI] and 99.2% susceptible [EUCAST]) showed good activity against P. aeruginosa (Table 3).
 |
Table 3 Activity of Ceftolozane/Tazobactam and Comparator Agents Tested Against the Main Organisms and Organism Groups |
Ceftolozane/tazobactam retained activity against isolates of P. aeruginosa that were NS to the other antipseudomonal β-lactam agents (Table 3): ceftazidime-NS (56.8/56.8% susceptible [CLSI/EUCAST]), meropenem-NS (66.0% susceptible [CLSI/EUCAST]), and piperacillin/tazobactam-NS (67.1/67.1% susceptible [CLSI/EUCAST]). Ceftolozane/tazobactam was also active against MDR strains of P. aeruginosa (55.8/55.8% susceptible [CLSI/EUCAST]) and levofloxacin-NS isolates (71.4/71.4% [CLSI/EUCAST]). None of the other β-lactam agents inhibited more than 48% of these resistant phenotypes. Notably, colistin was highly active against ceftazidime-NS (MIC50/90, 1/1 mg/L; 97.3% intermediate [CLSI] and 97.3% susceptible [EUCAST]), meropenem-NS (MIC50/90, 1/1 mg/L; 97.9% intermediate [CLSI] and 97.9% susceptible [EUCAST]), piperacillin/tazobactam-NS (MIC50/90, 1/1 mg/L; 97.5% intermediate [CLSI] and 97.5% susceptible [EUCAST]), and MDR (MIC50/90, 1/1 mg/L; 96.1% intermediate [CLSI] and 96.1% susceptible [EUCAST]) strains of P. aeruginosa (Table 3). Compared to colistin, amikacin was less active against ceftazidime-NS (MIC50/90, 8/>32 mg/L; 64.9/64.9% susceptible [CLSI/EUCAST]), meropenem-NS isolates (MIC50/90, 8/>32 mg/L; 71.3/71.3% susceptible [CLSI/EUCAST]), piperacillin/tazobactam-NS isolates (MIC50/90, 8/>32 mg/L; 73.4/73.4% susceptible [CLSI/EUCAST]), and MDR (MIC50/90, 16/>32 mg/L; 61.0/61.0% susceptible [CLSI/EUCAST]) strains of P. aeruginosa.
The susceptibility of P. aeruginosa to antipseudomonal β-lactams varied markedly among the Asian nations that participated in the survey (Tables 2 and 4). The lowest susceptibility rates for ceftazidime, meropenem, and piperacillin/tazobactam were observed in Korea (72.8%, 70.4%, and 67.9%, respectively), Thailand (72.6%, 64.4%, and 78.1%, respectively), and Vietnam (71.4%, 71.4%, and 71.4%, respectively) and the highest were in the Philippines (86.8%, 89.7%, and 82.4%, respectively). Ceftolozane/tazobactam activity provided greater than 80% coverage against isolates from the 7 countries submitting 10 or more isolates (Table 4).
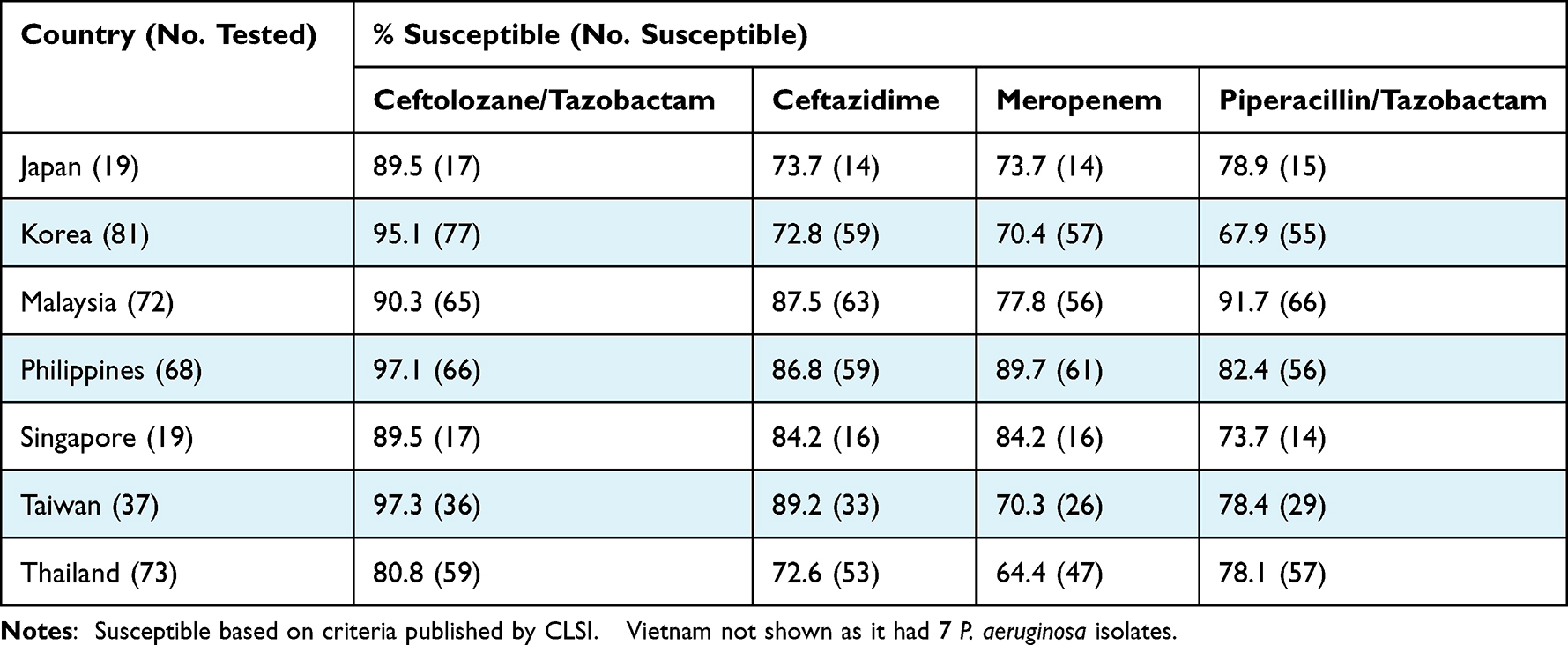 |
Table 4 Antimicrobial Activity of Ceftolozane/Tazobactam, Ceftazidime, Meropenem, and Piperacillin/Tazobactam Against Isolates of P. aeruginosa stratified by Country for Countries with 10 or More Isolates |
Activities of Ceftolozane/Tazobactam and Comparators Against Enterobacterales
Ceftolozane/tazobactam (MIC50/90, 0.25/16 mg/L) inhibited 86.8/86.8% of the 1662 Enterobacterales isolates tested at the CLSI/EUCAST susceptible breakpoints of ≤2/≤2 mg/L, respectively (Tables 1 and 3). Enterobacterales isolates displayed susceptibility rates to other β-lactam agents ranging from 93.0/93.3% for meropenem, 81.5/77.7% for piperacillin/tazobactam, 66.0/64.5% for cefepime, and 65.3/60.9% for ceftazidime using CLSI/EUCAST breakpoints. Among the non-β-lactam agents, amikacin (MIC50/90, 2/8 mg/L; 97.7/94.9% susceptible [CLSI/EUCAST]) was more active than colistin (MIC50/90, 0.12/>8 mg/L; 87.6% susceptible [EUCAST]), gentamicin (MIC50/90, 0.5/>8 mg/L; 76.7/75.9% susceptible [CLSI/EUCAST]), and levofloxacin (MIC50/90, 0.5/>4 mg/L; 58.7/58.7% susceptible [CLSI/EUCAST]). Against 492 presumptive ESBL non-CRE phenotype Enterobacterales isolates, ceftolozane/tazobactam (MIC50/90, 0.5/8 mg/L; 84.8/84.8% susceptible [CLSI/EUCAST]), meropenem (MIC50/90, 0.03/0.12 mg/L; 99.2/100.0% susceptible [CLSI/EUCAST]), colistin (MIC50/90, 0.12/0.25 mg/L; 94.3% susceptible [EUCAST]), amikacin (MIC50/90, 2/8 mg/L; 96.7/91.5% susceptible [CLSI/EUCAST]), and piperacillin/tazobactam (MIC50/90, 4/> 64 mg/L; 75.1/66.1% susceptible [CLSI/EUCAST]) were the only agents to retain clinically useful activity (Table 3).
A total of 716 E. coli isolates were evaluated, 95.8/95.8% of which were susceptible to ceftolozane/tazobactam (MIC50/90, 0.25/1 mg/L) by CLSI/EUCAST interpretive guidelines. Meropenem (MIC50/90, ≤0.015/0.03 mg/L; 98.6/98.6% susceptible [CLSI/EUCAST]), amikacin (MIC50/90, 2/8 mg/L; 99.0/96.8% susceptible [CLSI/EUCAST]), colistin (MIC50/90, 0.12/0.25 mg/L; 99.3% susceptible [EUCAST]), and piperacillin/tazobactam (MIC50/90, 2/16 mg/L; 91.6/88.2% susceptible [CLSI/EUCAST]) showed good activity against E. coli (Table 3). Cefepime (MIC50/90, ≤0.12/>16 mg/L; 63.1/62.0% susceptible [CLSI/EUCAST]), ceftazidime (MIC50/90, 0.25/> 32 mg/L; 67.3/60.1% susceptible [CLSI/EUCAST]), gentamicin (MIC50/90, 1/>8 mg/L; 70.5/69.8% susceptible [CLSI/EUCAST]), and levofloxacin (MIC50/90, 1/>4 mg/L; 49.6/49.6% susceptible [CLSI/EUCAST]) showed decreased activity against E. coli isolates. Among presumptive ESBL non-CRE phenotype E. coli isolates, resistance rates to cefepime, ceftazidime, gentamicin, and levofloxacin were elevated (Table 3). Meropenem (MIC50/90, 0.03/0.06 mg/L; 100.0/100.0% susceptible [CLSI/EUCAST]) and amikacin (MIC50/90, 4/8 mg/L; 99.0/94.7% susceptible [CLSI/EUCAST]) retained potent activity against presumptive ESBL non-CRE phenotype strains of E. coli. Ceftolozane/tazobactam inhibited 93.7% of the presumptive ESBL non-CRE phenotype isolates of E. coli at ≤2 mg/L (Tables 1 and 3). Piperacillin/tazobactam was slightly less active (MIC50/90, 4/32 mg/L; 88.0/80.1% susceptible [CLSI/EUCAST]) than ceftolozane/tazobactam against these strains of E. coli.
Ceftolozane/tazobactam showed moderate activity against isolates of K. pneumoniae (MIC50/90, 0.25/>32 mg/L; 74.8/74.8% susceptible [CLSI/EUCAST]) and was slightly less active against presumptive ESBL non-CRE phenotype isolates (MIC50/90, 2/>32 mg/L; 69.1/69.1% susceptible [CLSI/EUCAST]) (Tables 1 and 3). Among the β-lactam comparator agents tested, only meropenem was more active than ceftolozane/tazobactam against Klebsiella species, irrespective of the resistant phenotype (Table 3). Ceftolozane/tazobactam was also active against other frequently isolated Enterobacterales, including Klebsiella oxytoca (MIC50/90, 0.25/>32 mg/L; 84.6/84.6% susceptible [CLSI/EUCAST]), Klebsiella aerogenes (MIC50/90, 0.25/8 mg/L; 84.0/84.0% susceptible [CLSI/EUCAST]), Enterobacter cloacae species complex (MIC50/90, 0.25/32 mg/L; 77.0/77.0% susceptible [CLSI/EUCAST]), Citrobacter spp. (MIC50/90, 0.25/0.5 mg/L; 92.0/92.0% susceptible [CLSI/EUCAST]), P. mirabilis (MIC50/90, 0.5/1 mg/L; 95.8/95.8% susceptible [CLSI/EUCAST]), indole-positive Proteae (MIC50/90, 0.25/0.5 mg/L; 100.0/100.0% susceptible [CLSI/EUCAST]), and Serratia marcescens (MIC50/90, 0.5/1 mg/L; 98.1/98.1% susceptible [CLSI/EUCAST]) (Tables 1 and 3). Ceftolozane/tazobactam (MIC50/90, 4/>32 mg/L; 46.2/46.2% susceptible [CLSI/EUCAST]), cefepime (MIC50/90, 16/>16 mg/L; 32.3/24.6% susceptible [CLSI/EUCAST]), and piperacillin/tazobactam (MIC50/90, 64/>64 mg/L; 30.8/23.1% susceptible [CLSI/EUCAST]) all showed decreased activity against ceftazidime-nonsusceptible E. cloacae species complex (Table 3).
Previously in 1998–2010 and 2013–2015, we showed that, among isolates of E. coli and K. pneumoniae, the rates of presumptive ESBL and CRE phenotypes varied markedly among Asian countries.7,10,11,13,14,16 As seen in Table 2, resistance rates among these 2 species from 2016 to 2018 show continued variability among the Asian countries evaluated. The occurrence of K. pneumoniae isolates with a presumptive CRE phenotype ranged from 0.0% in Japan and Singapore to 55.3% in Vietnam and was 15.7% overall. The highest rates of presumptive ESBL non-CRE phenotype E. coli were identified in isolates from Vietnam (65.4%) followed by Thailand (51.4%) and the lowest rates were in isolates from Singapore (30.0%). In contrast, the highest rates of presumptive ESBL non-CRE phenotype K. pneumoniae were associated with isolates from Korea (40.7%) while the lowest rates were in isolates from Vietnam (10.5%), Japan (6.7%), and Singapore (0.0%). Similar variability in resistance profiles was seen for ceftazidime-NS isolates of Enterobacter spp. and meropenem-NS isolates of K. pneumoniae (Table 2). These resistance rates are considerably higher than rates reported in 1998 to 2002,7,11 2008,10 and 2013 to 2015.13
Discussion
Our study results extend those previously reported concerning the in vitro activity of ceftolozane/tazobactam against strains of Enterobacterales and P. aeruginosa in Asia.13 Ceftolozane/tazobactam was the most active of the tested β-lactam agents against P. aeruginosa and was second to meropenem against Enterobacterales. Ceftolozane/tazobactam retained activity against most presumptive ESBL non-CRE phenotype strains, second only to meropenem. Likewise, ceftolozane/tazobactam was more active than the other antipseudomonal β-lactam agents tested against strains of P. aeruginosa that were NS to ceftazidime, meropenem, and piperacillin/tazobactam as well as MDR strains. Among the non-β-lactam comparator agents, colistin and amikacin were the most active against Enterobacterales and P. aeruginosa, including the various resistant phenotypes. It should be noted that colistin and amikacin are nephrotoxic.32 In addition, colistin efficacy has been found to be poor when given systemically to patients with pneumonia.33
Previously, Castanheira et al demonstrated a steady increase in the E. coli and K. pneumoniae ESBL prevalence rate in Asian countries from 1997 to 2016.1 Notably, the resistance patterns for commonly used antimicrobials against Enterobacterales varied by geographical location and species characteristics.1,10,11,13 Our findings support and extend those observations. The rates of presumptive ESBL non-CRE phenotype E. coli and K. pneumoniae in the present study (42.3% and 28.7%, respectively) were comparable to or slightly higher than those reported by Pfaller et al for 2013 to 2015 (34.9% and 30.4%, respectively) and were higher than the presumptive ESBL non-CRE rates seen in the US and western Europe.1,7,8,10,11 Carbapenem resistance attributable to acquired carbapenemases remains relatively uncommon in Asia, comprising only 2% to 5% of Enterobacterales in 2004–2009,8,9 3.6% in 2013–2015,13 and 6.8% in the present survey (2016–2018; Table 1). The majority of presumptive CRE phenotype isolates were accounted for by K. pneumoniae, with CRE rates of greater than 9% in 5 of the 8 Asian countries (range 0.0–55.3%; 15.7% overall) (Table 2). As previously noted, ceftolozane/tazobactam did not have activity against CRE.13
There are some limitations to this work that must be acknowledged. First, patient-level data is not collected in SENTRY Program. Second, no confirmatory testing was performed for either ESBL or CRE production. This is consistent with our previous publication concerning the activity of ceftolozane-tazobactam against Enterobacterales isolates from Asia.13 As such, we described these results as presumptive ESBL non-CRE phenotype and presumptive CRE phenotype strains. Third, we did not link the isolation of bacterial species and associated resistance profiles with patient presentation, treatment, or outcome. Fourth, susceptibility to ceftazidime/avibactam was not determined in this study. Fifth and finally, the SENTRY Program depends on the classification of isolates as originating from clinically significant healthcare-associated infections of specific body sites (e.g., bloodstream, respiratory specimens, urinary tract, skin and soft tissue specimens, and intra-abdominal abscesses) based on the judgement of the submitting laboratory.
In summary, these data for ceftolozane/tazobactam collected from 2016 to 2018 from 11 Asian medical centres demonstrate its sustained potency and spectrum against P. aeruginosa and Enterobacterales when compared to previous studies.13,23–26 These data suggest that ceftolozane/tazobactam may be an important treatment option for HAIs caused by wild-type and MDR strains of P. aeruginosa, including those resistant to ceftazidime or piperacillin/tazobactam as well as ESBL non-CR Enterobacterales.20 Resistance rates among GNB from Asia are relatively high and have been increasing in recent years, emphasizing the need for resistance surveillance and antimicrobial stewardship in those countries.6,12
Ethical Statement
Isolates were collected as part of the routine hospital laboratory procedure. No patient information was collected that could identify specific patients, only limited patient demographics were collected. Ethical approval not required.
Acknowledgments
JMI Laboratories contracted to perform services in 2020 for Affinity Biosensors, Allergan, Amicrobe, Inc., Amplyx Pharma, Artugen Therapeutics USA, Inc., Astellas, Basilea, Beth Israel Deaconess Medical Center, bioMerieux, Inc., BioVersys Ag, Bugworks, Cidara, Cipla, Contrafect, Cormedix, Crestone, Inc., Curza, CXC7, Entasis, Fedora Pharmaceutical, Fimbrion Therapeutics, Fox Chase, GlaxoSmithKline, Guardian Therapeutics, Hardy Diagnostics, IHMA, Janssen Research & Development, Johnson & Johnson, Kaleido Biosciences, KBP Biosciences, Luminex, Matrivax, Mayo Clinic, Medpace, Meiji Seika Pharma Co., Ltd., Melinta, Menarini, Merck, Meridian Bioscience Inc., Micromyx, MicuRx, N8 Medical, Nabriva, National Institutes of Health, National University of Singapore, North Bristol NHS Trust, Novome Biotechnologies, Paratek, Pfizer, Prokaryotics Inc., QPEX Biopharma, Rhode Island Hospital, RIHML, Roche, Roivant, Salvat, Scynexis, SeLux Diagnostics, Shionogi, Specific Diagnostics, Spero, SuperTrans Medical LT, T2 Biosystems, The University of Queensland, Thermo Fisher Scientific, Tufts Medical Center, Universite de Sherbrooke, University of Iowa, University of Iowa Hospitals and Clinics, University of Wisconsin, UNT System College of Pharmacy, URMC, UT Southwestern, VenatoRx, Viosera Therapeutics, and Wayne State University.
Funding
This study was performed by JMI Laboratories and supported by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, which included funding for services related to preparing this manuscript.
Disclosure
W-T Chen is an employee of Merck & Co., Inc., Kenilworth, NJ, USA. MP, DS, HS and MC are affiliated with JMI Laboratories. The authors report no other conflicts of interest in this work.
References
1. Castanheira M, Deshpande LM, Mendes RE, Canton R, Sader HS, Jones RN. Variations in the occurrence of resistance phenotypes and carbapenemase genes among Enterobacteriaceae isolates in 20 years of the SENTRY Antimicrobial Surveillance Program. Open Forum Infect Dis. 2019;6:S23–S33. doi:10.1093/ofid/ofy347
2. Jernigan JA, Hatfield KM, Wolford H, et al. Multidrug-resistant bacterial infections in U.S. hospitalized patients, 2012–2017. N Engl J Med. 2020;382:1309–1319. doi:10.1056/NEJMoa1914433
3. Magill SS, O’Leary E, Ray SM, et al. Antimicrobial use in US hospitals: comparison of results from emerging infections program prevalence surveys, 2015 and 2011. Clin Infect Dis. 2021;72:1784–1792. doi:10.1093/cid/ciaa373
4. Shortridge D, Gales AC, Streit JM, Huband MD, Tsakris A, Jones RN. Geographic and temporal patterns of antimicrobial resistance in Pseudomonas aeruginosa over 20 years from the SENTRY Antimicrobial Surveillance Program, 1997–2016. Open Forum Infect Dis. 2019;6:S63–S68. doi:10.1093/ofid/ofy343
5. Weiner-Lastinger LM, Abner S, Edwards JR, et al. Antimicrobial-resistant pathogens associated with adult healthcare-associated infections: summary of data reported to the National Healthcare Safety Network, 2015–2017. Infect Control Hosp Epidemiol. 2020;41:1–18. doi:10.1017/ice.2019.296
6. Ashley EA, Lubell Y, White NJ, Turner P. Antimicrobial susceptibility of bacterial isolates from community acquired infections in Sub-Saharan Africa and Asian low and middle income countries. Trop Med Int Health. 2011;16:1167–1179. doi:10.1111/j.1365-3156.2011.02822.x
7. Bell JM, Turnidge JD, Gales AC, Pfaller MA, Jones RN, Sentry ASG. Prevalence of extended spectrum beta-lactamase (ESBL)-producing clinical isolates in the Asia-Pacific region and South Africa: regional results from SENTRY Antimicrobial Surveillance Program (1998–1999). Diagn Microbiol Infect Dis. 2002;42:193–198. doi:10.1016/S0732-8893(01)00353-4
8. Bertrand X, Dowzicky MJ. Antimicrobial susceptibility among Gram-negative isolates collected from intensive care units in North America, Europe, the Asia-Pacific Rim, Latin America, the Middle East, and Africa between 2004 and 2009 as part of the tigecycline evaluation and surveillance trial. Clin Ther. 2012;34:124–137. doi:10.1016/j.clinthera.2011.11.023
9. Chen YH, Hsueh PR, Badal RE, et al. Antimicrobial susceptibility profiles of aerobic and facultative Gram-negative bacilli isolated from patients with intra-abdominal infections in the Asia-Pacific region according to currently established susceptibility interpretive criteria. J Infect. 2011;62:280–291. doi:10.1016/j.jinf.2011.02.009
10. Farrell DJ, Turnidge JD, Bell J, Sader HS, Jones RN. The in vitro evaluation of tigecycline tested against pathogens isolated in eight countries in the Asia-Western Pacific region (2008). J Infect. 2010;60:440–451. doi:10.1016/j.jinf.2010.03.024
11. Hirakata Y, Matsuda J, Miyazaki Y, et al. Regional variation in the prevalence of extended-spectrum beta-lactamase-producing clinical isolates in the Asia-Pacific region (SENTRY 1998–2002). Diagn Microbiol Infect Dis. 2005;52:323–329. doi:10.1016/j.diagmicrobio.2005.04.004
12. Jean SS, Hsueh PR. High burden of antimicrobial resistance in Asia. Int J Antimicrob Agents. 2011;37:291–295. doi:10.1016/j.ijantimicag.2011.01.009
13. Pfaller MA, Shortridge D, Sader HS, Castanheira M, Flamm RK. Ceftolozane-tazobactam activity against drug-resistant Enterobacteriaceae and Pseudomonas aeruginosa causing health care-associated infections in the Asia-Pacific region (APAC; minus China, Australia and New Zealand): report from an antimicrobial surveillance program (2013–2015). Int J Antimicrob Agents. 2018;51:181–189. doi:10.1016/j.ijantimicag.2017.09.016
14. Sader HS, Flamm RK, Jones RN. Antimicrobial activity of ceftaroline and comparator agents tested against bacterial isolates causing skin and soft tissue infections and community-acquired respiratory tract infections isolated from the Asia-Pacific region and South Africa (2010). Diagn Microbiol Infect Dis. 2013;76:61–68. doi:10.1016/j.diagmicrobio.2013.01.005
15. Sheng WH, Badal RE, Hsueh PR, Program S. Distribution of extended-spectrum beta-lactamases, AmpC beta-lactamases, and carbapenemases among Enterobacteriaceae isolates causing intra-abdominal infections in the Asia-Pacific region: results of the study for Monitoring Antimicrobial Resistance Trends (SMART). Antimicrob Agents Chemother. 2013;57:2981–2988. doi:10.1128/AAC.00971-12
16. Turnidge J, Bell J, Biedenbach DJ, Jones RN. Pathogen occurrence and antimicrobial resistance trends among urinary tract infection isolates in the Asia-Western Pacific Region: report from the SENTRY antimicrobial surveillance program, 1998–1999. Int J Antimicrob Agents. 2002;20:10–17. doi:10.1016/S0924-8579(02)00050-X
17. Kollef MH, Golan Y, Micek ST, Shorr AF, Restrepo MI. Appraising contemporary strategies to combat multidrug resistant gram-negative bacterial infections--proceedings and data from the Gram-Negative Resistance Summit. Clin Infect Dis. 2011;53(Suppl 2):S33–S55. doi:10.1093/cid/cir475
18. Cosgrove SE. The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs. Clin Infect Dis. 2006;42:S82–S89. doi:10.1086/499406
19. Zhang D, Micek ST, Kollef MH. Time to appropriate antibiotic therapy is an independent determinant of postinfection ICU and hospital lengths of stay in patients with sepsis. Crit Care Med. 2015;43:2133–2140. doi:10.1097/CCM.0000000000001140
20. Lizza BD, Betthauser KD, Ritchie DJ, Micek ST, Kollef MH. New perspectives on antimicrobial agents: ceftolozane-tazobactam. Antimicrob Agents Chemother. 2021;65:e0231820. doi:10.1128/AAC.02318-20
21. Munita JM, Aitken SL, Miller WR, et al. Multicenter evaluation of ceftolozane/tazobactam for serious infections caused by carbapenem-resistant Pseudomonas aeruginosa. Clin Infect Dis. 2017;65:158–161. doi:10.1093/cid/cix014
22. Puzniak L, Dillon R, Palmer T, Collings H, Enstone A. Real-world use of ceftolozane/tazobactam: a systematic literature review. Antimicrob Resist Infect Control. 2021;10:68. doi:10.1186/s13756-021-00933-8
23. Farrell DJ, Flamm RK, Sader HS, Jones RN. Antimicrobial activity of ceftolozane-tazobactam tested against Enterobacteriaceae and Pseudomonas aeruginosa with various resistance patterns isolated in U.S. Hospitals (2011–2012). Antimicrob Agents Chemother. 2013;57:6305–6310. doi:10.1128/AAC.01802-13
24. Farrell DJ, Sader HS, Flamm RK, Jones RN. Ceftolozane/tazobactam activity tested against gram-negative bacterial isolates from hospitalized patients with pneumonia in United States and European medical centres (2012). Int J Antimicrob Agents. 2014;43:533–539. doi:10.1016/j.ijantimicag.2014.01.032
25. Sader HS, Farrell DJ, Castanheira M, Flamm RK, Jones RN. Antimicrobial activity of ceftolozane/tazobactam tested against Pseudomonas aeruginosa and Enterobacteriaceae with various resistance patterns isolated in European hospitals (2011–2012). J Antimicrob Chemother. 2014;69:2713–2722. doi:10.1093/jac/dku184
26. Sader HS, Farrell DJ, Flamm RK, Jones RN. Ceftolozane/tazobactam activity tested against aerobic Gram-negative organisms isolated from intra-abdominal and urinary tract infections in European and United States hospitals (2012). J Infect. 2014;69:266–277. doi:10.1016/j.jinf.2014.04.004
27. Fuhrmeister AS, Jones RN. The importance of antimicrobial resistance monitoring worldwide and the origins of SENTRY antimicrobial surveillance program. Open Forum Infect Dis. 2019;6:S1–S4. doi:10.1093/ofid/ofy346
28. CLSI. M07ED11 Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically: eleventh edition. Wayne, PA: Clinical and Laboratory Standards Institute; 2018.
29. CLSI. M100Ed31. Performance standards for antimicrobial susceptibility testing: 31st informational supplement. Wayne, PA: Clinical and Laboratory Standards Institute; 2021.
30. EUCAST. Breakpoint tables for interpretation of MICs and zone diameters. Version 11.0, January 2021. European Committee on Antimicrobial Susceptibility Testing; 2021.
31. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18:268–281. doi:10.1111/j.1469-0691.2011.03570.x
32. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious diseases society of America guidance on the treatment of Extended-Spectrum Beta-Lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin Infect Dis. 2021;72:e169–e183. doi:10.1093/cid/ciaa1478
33. Satlin MJ, Lewis JS, Weinstein MP, et al. Clinical and Laboratory Standards Institute (CLSI) and European Committee on Antimicrobial Susceptibility Testing (EUCAST) position statements on polymyxin B and colistin clinical breakpoints. Clin Infect Dis. 2020;71:e523–e529. doi:10.1093/cid/ciaa121
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.