")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 15
Cefepime-Induced Neutropenia: A Case Report and Literature Review
Authors Koraysh S , Koleri J, Ali M
Received 27 February 2023
Accepted for publication 13 April 2023
Published 19 April 2023 Volume 2023:15 Pages 33—40
DOI https://doi.org/10.2147/CPAA.S406139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Somaya Koraysh,1 Junais Koleri,2 Maisa Ali2
1Department of Pharmacy, Hamad Bin Khalifa Medical City, Hamad Medical Corporation, Doha, Qatar; 2Department of Infectious Disease, Communicable Disease Center, Hamad Medical Corporation, Doha, Qatar
Correspondence: Somaya Koraysh, Tel +974 5546 5857, Email [email protected]
Abstract: Cefepime is a fourth-generation cephalosporin utilized in treatment of multiple Gram-negative and -positive infections. The current report presents a case of 50-year-old man admitted with epidural abscess who developed neutropenia after prolonged use of cefepime. The neutropenia developed after 24 days of cefepime treatment and resolved 4 days after cessation of cefepime. Assessment of the patient’s profile indicated no other possible cause for neutropenia. A literature review was done, and is presented herein to compare and identify the pattern of cefepime-induced neutropenia in 15 patients. The data presented in this article highlight that despite its rarity, cefepime-induced neutropenia should be considered by clinicians when planning a prolonged course of cefepime.
Keywords: neutropenia, cefepime, cephalosporin, adverse event, epidural abscess
Introduction
Neutrophils are an integral part of host defense mechanisms. They constitute the largest amount of white blood cells (WBCs), reaching up to 60% in the adult body.1 Neutropenia is defined as a reduction in absolute neutrophil count (ANC; product of WBC and percentages of segmented and banded neutrophils) to <1500 cell/mm3. Neutropenia can be categorized as mild (1000–1500 cell/mm3), moderate (500–1000 cells/mm3), or severe (<500 cells/mm3).2 Severer forms of neutropenia (ANC <100 cells/mm3) are simultaneously termed agranulocytosis, a life-threatening condition that usually manifests with severe infectious presentation.3 Mechanisms behind neutropenia include reduced production or differentiation in the bone marrow and peripheral destruction by immunological or cytotoxic mechanisms.2,4
Neutropenia can be the product of a primary (congenital) or secondary (acquired) causes. Drug-induced neutropenia (DIN) is believed to be one of the main causes of acquired neutropenia and was first described in 1931.1 In 1991, an incidence of four cases/million population/year was reported in a nationwide study.1 With the expansion in the production of medical agents, the incidence of DIN has noticeably increased. Drugs implicated in >50% of the DIN reports include carbimazole, clozapine, dapsone, dipyrone, methimazole, penicillin G, procainamide, propylthiouracil, rituximab, sulfasalazine, and ticlopidine.4,5
Cefepime, a fourth-generation cephalosporin and β-lactam, is used in the treatment of Gram-positive and -negative bacteria that are susceptible to its activity. It is commonly used in the treatment of pneumonia, urinary tract infections, skin infections, and intra-abdominal infections, as well as an empirical antibiotic in management of febrile neutropenia.6 Common adverse reactions associated with cefepime use are gastrointestinal reactions, including Clostridioides difficile infection and neurotoxicity, including encephalopathy, aphasia, and seizure activities.7 One suspected DIN was encountered in the Qatar Rehabilitation Institute (QRI) and attributed to cefepime use. This report aims to document an encountered case of cefepime-induced neutropenia (CIN), describe the management approach, and review the available literature on CIN.
Case Presentation
A 50-year-old Filipino gentleman with a medical history of stroke, hypertension, diabetes, and diabetes-related kidney disease (baseline serum creatinine 150–200 µmol/L) presented to the emergency department with a history of fever of 5 days and low-back pain of 10 days. Low-back pain was worse with movement. On examination, he was afebrile, with tenderness in the lumbar area and no features of spinal cord or root compression.
Routine laboratory tests showed Hgb 12.8 g/dL, WBC count 26×103/µL, ALP 356 U/L, serum creatinine 211 µmol/L, CRP 189.3 mg/L, and sterile blood cultures. Medications administered regularly during his hospital stay were amlodipine 10 mg daily, atorvastatin 20 mg daily, carvedilol 6.25 mg twice daily, enoxaparin 40 mg daily, esomeprazole 40 mg daily, linagliptin 5 mg daily, sodium bicarbonate 1200 mg three times daily, paracetamol–orphenadrine 450/35 mg and tramadol 50 mg as needed for pain. His spine MRI showed an epidural collection at L5–S1 that measured approximately 40×10×8 mm maximum, meningeal thickening, and edematous changes involving L5 and S1 vertebrae, along with L4/5 paraspinal and psoas abscess. He was started on ceftriaxone 2 g once daily, which was continued for 6 days, and then escalated to piperacillin–tazobactam as fever persisted. He underwent L1/2 and L5/S1 right-side laminotomy and drainage of epidural abscess. Pus and tissue were sent for culture, which turned out to be sterile and negative for TB.
Four days after the surgery, antibiotics were optimized to cefepime 2 g every 12 hours in view of the meningeal involvement seen on MRI and operation. Dosage was calculated based on adjusted body weight and creatinine clearance (48 mL/min). The plan was to continue cefepime for 6 weeks and then repeat imaging studies. His fever subsided after the surgery. CRP decreased to a quarter of the peak value and WBC count normalized in 1 week postsurgery (Table 1). After 4 weeks on cefepime, his WBC count started to decrease, reaching a nadir of 1400 cells/mm3 with ANC of 200 cells/mm3 (14%). These were accidental findings during routine blood tests, and the patient reported no symptoms associated with the marked changes in his WBC count. No changes in red blood cell count, Hgb, or platelet count were noted (Table 1). A diagnosis of CIN was considered, cefepime discontinued, and meropenem 2 g every 8 hours initiated. Dosage was calculated based on creatinine clearance (53 mL/min). Withdrawal of cefepime showed an immediate effect on lab results: WBC count increased to 2000 cells/mm3 and normalized to 4200 cells/mm3 within 4 days, with a similar response from neutrophils (Table 1, Figure 1). His treatment course was completed with meropenem, with no further adverse events.
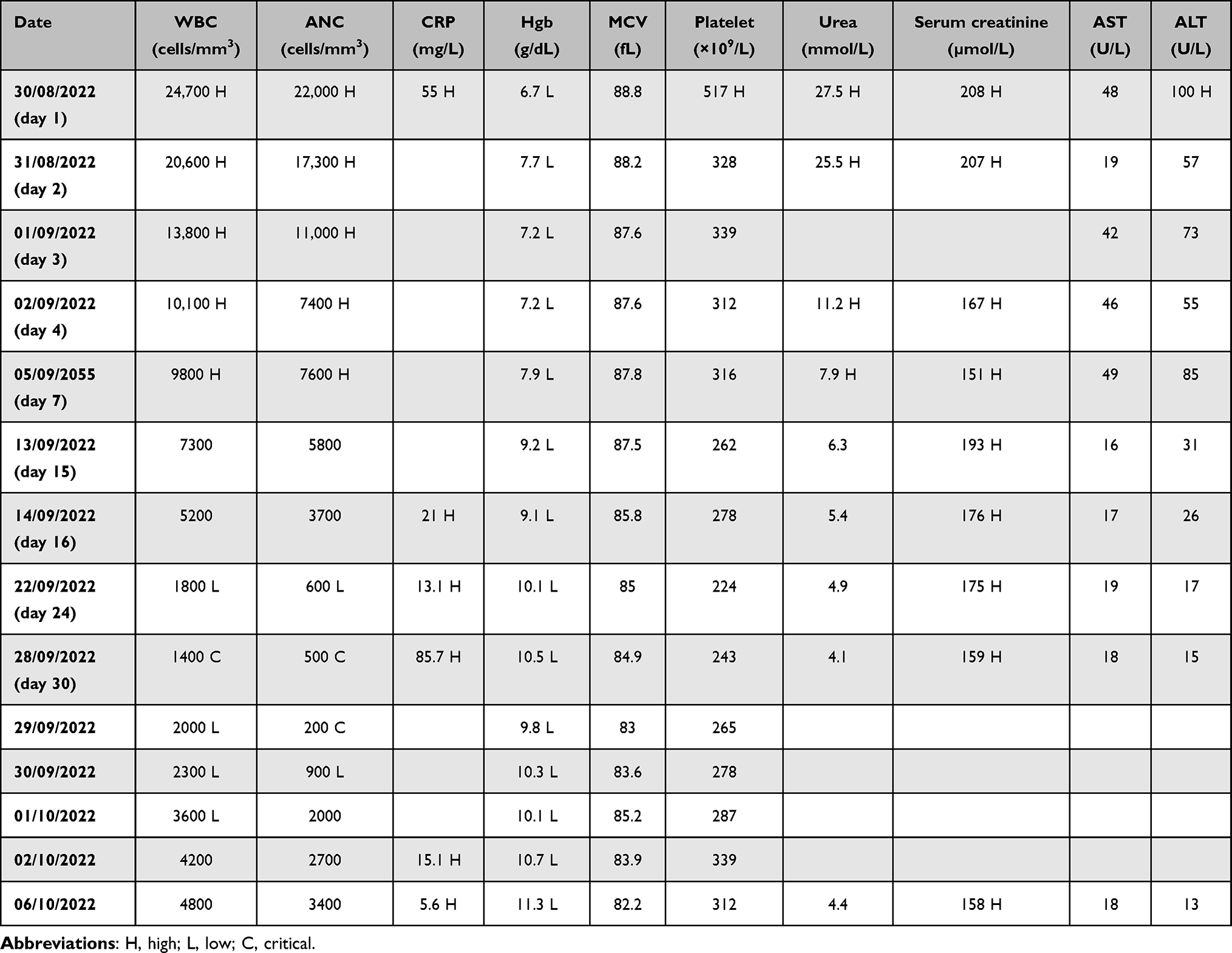 |
Table 1 Lab results during cefepime therapy |
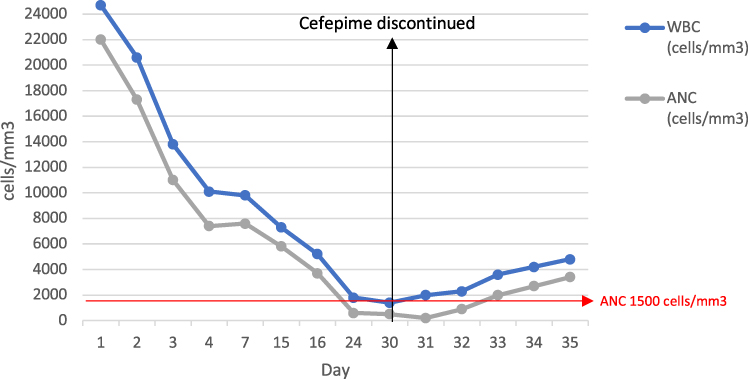 |
Figure 1 Patient's lab results during cefepime therapy. Cefepime was discontinued on day 30. |
Discussion
CIN is a rare side effect (<1%) that has been reported in postmarketing surveillance studies.8–13 In the presented case, culture results did not yield any bacterial colonies; however, the antimicrobial regimen was switched to cefepime for better distribution of medicine to the infected site. The patient had experienced a significant improvement on subsequent lab work (WBC and CRP) and spinal CT, which showed a marked reduction in abscess size. As noted in Figure 1, during the 30 days of treatment, there was a gradual decrease in WBC and ANC until they reached critical levels. The patient reported no complaints or symptoms accompanying the drop in WBC levels. After discontinuation of cefepime, there was a marked elevation in WBC and ANC levels within 4 days. The Naranjo Adverse Drug Reaction Probability Scale yielded a score of 7 for the suspected incident, indicating a probable adverse drug event.14
DIN induced by antibiotics is considered an uncommon side effect, but is well-documented in the literature. A recent systematic review of 83 reports on antibiotically induced neutropenia reported penicillin to be the most common class associated with the development of DIN (32%), followed by glycopeptides (28%), and non-penicillin β-lactams (19%). Among the antibiotics, vancomycin (n=24) and ceftaroline (n=12) were the most commonly reported to induce neutropenia. Only four cases of CIN were documented.15
DIN can be categorized into two categories based on the triggering agent. First, neutropenia can develop with the use of cytotoxic agents, immunosuppressants, or radiotherapy. This detrimental effect is dose-dependent and can be predicted by their pharmacological actions, which involve DNA damage and myelosuppression.3 Alternatively, noncytotoxic drugs have been observed to lead to idiosyncratic neutropenic reactions (also termed “bizarre” reactions), as they occur only rarely. As opposed to the former agents, no clear dose dependence has been observed.3 Despite the lack of clearly defined mechanisms for idiosyncratic DIN, research suggests that it is highly consistent with an immunomediated reaction.3,16,17 The immunoresponse can be triggered by the drug acting as an antigen or more probably by its active metabolite acting as a hapten (a small molecule incapable of eliciting an immunoresponse unless it binds covalently with an endogenous protein), the resultant structural change in the protein — hypothesized to be neutrophil glycoprotein-drug complex — can lead to T-cell activation and formation of antibodies that lead to neutrophil destruction. Another hypothesized immunomediated reaction involves generating “danger signals” that lead to upregulation of inflammasomes, which activates a second signal for T-cell activation.17
Complications related to neutropenia include opportunistic infections, sepsis, and increased risk of mortality.1,2,4 A systematic review evaluating case reports of non-chemotherapy drug-induced neutropenia concluded that patients who had a nadir of <100 cells/mm3 had a significantly higher risk of local infections (59% vs 39%), sepsis (20% vs 6%), and fatal complications (10% vs 3%) than patients with a nadir of >100 cells/mm3 (p<0.001).4 In the presented case, the nadir reached 200 cells/mm3 with no reported signs or symptoms of local or systemic infections. Compared to available case reports in the literature (Table 2), five of 14 cases reported fever or flulike symptoms, one reported back pain, while eight were reported as asymptomatic.9–13
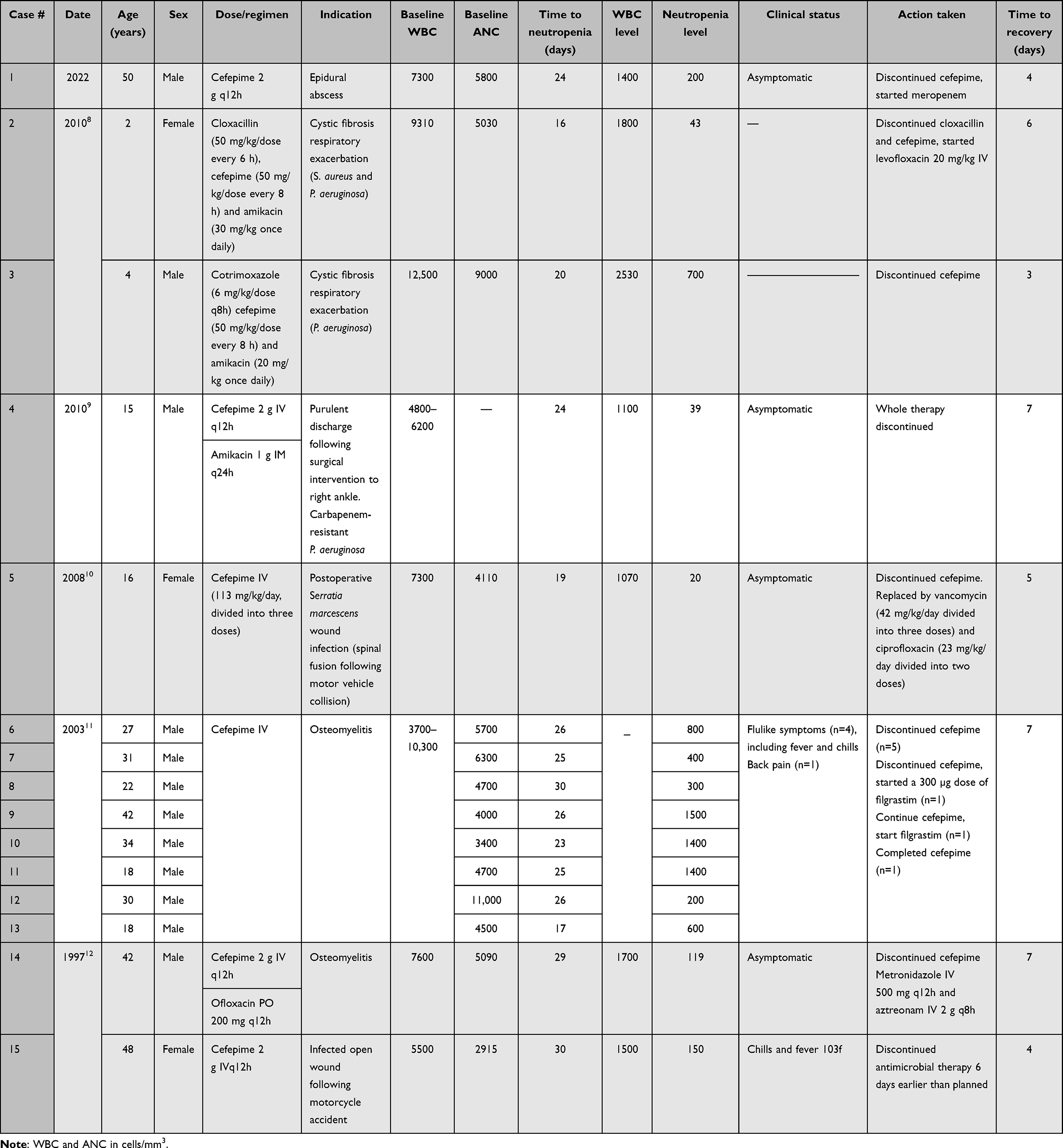 |
Table 2 Summary of case reports on cefepime-induced neutropenia |
Considering other potential causes of neutropenia, the patient’s medical record dids not raise suspicion of other medications that would lead to an adverse event of neutropenia. Additionally, at the time of switching to cefepime, no other medicine was initiated concurrently, as all other medications were started since admission, so it is unlikely that neutropenia was induced by an alternative agent. Only three of the identified case reports mentioned the use of concurrent medications (Table 2), which included amikacin,9,10 cloxacillin,9 trimethoprim–sulfamethoxazole,9 ofloxacin, and hydrocodone–acetaminophen.13 Both cloxacillin and co-trimoxazole have been reported as potentially inducing neutropenia;5,18,19 therefore, whether cefepime or the concomitant use of these antibiotics were the potential lead to neutropenia cannot be ruled out.9 Our patient received piperacillin–tazobactam for 4 days and then switched to cefepime for optimization of bioavailability due to meningeal involvement. While there are ample studies associating piperacillin–tazobactam with DIN,15 the hypothesized immunomediated mechanism of action for DIN indicates a delayed onset of reaction after initiation (ie, 1–6 months, a necessary period for the expansion in number of pathological T-cells).3 Available literature reports a median of 20 days of treatment until neutropenia develops with piperacillin–tazobactam,15 and the patient received his doses for 4 days before switching to cefepime.
Some studies have associated the rapid IV infusion of β-lactams with the development of neutropenia.8,20 In a retrospective study, a cluster of CIN during outpatient parenteral therapy was studied.8 Of the 168 who took cefepime, nine satisfied the CIN definition and all of them received cefepime for ≥2 weeks. It was noticed that patients who received cefepime as IV push were 7.42 times as likely to develop CIN. In the current report, the patient received cefepime in a standard infusion over 30 minutes. Further research is needed to evaluate a plausible physiological basis for the effect of infusion rate on development of neutropenia.
Available reports include patients who had osteomyelitis (n=9),12,13 surgery-related infections (n=3),10,11,13 or cystic fibrosis (n=2).9 Of the 14 cases, only three reported susceptible Pseudomonas aeruginosa9,10 and one susceptible Serratia marcescens;11 however, the other nine cases were diagnosed with osteomyelitis,12,13 and cefepime is a mainstay of empiric therapy in the management of osteomyelitis.21 In the collated reports, the average time to neutropenia was 24 days (16–30) and the average time to recovery 6 (3–7) days, similar to what is described in this report (Table 1).
Emerging cross-reactivity studies support the substitution to an alternative β-lactam from a different group in cases of adverse events; however, this strategy in the setting of DIN is still under scrutiny, given the noted recurrence of neutropenia in 15%–30% of cases who are reintroduced to antibiotics.22 These data mainly include reintroducing the same agent (ie, rechallenging) or substituting to an agent with a structural similarity, which does not contradict the use of alternative antibiotics with different side chains or structure, as they are believed to be the main contributors to cross reactivity amongst β-lactams.23 One case report of ceftriaxone-induced neutropenia reported complete resolution after substituting with cefepime. Despite them sharing R1 side chain and core structure, they differed in the R2 side chain, which was used to justify the absence of DIN recurrence.24 In the present case, meropenem was initiated as an alternative antibiotic agent, and neutropenia resolved without any medical intervention or noted recurrence, similar to 12 of the cases presented in Table 2.
Interestingly, filgrastim (a colony-stimulating factor) was initiated in two cases to aid the resolution of neutropenia.12 The reports mentioned no difference in duration to recovery, as opposed to the available literature. A systematic review of case reports with acute antibiotically induced neutropenia conducted a subgroup analysis of 50 cases after 1991, reporting a statistically significant reduction in the median duration of neutropenia when using a colony-stimulating factor compared to no treatment (median 7.0 vs 3.5 days, p=0.017).15
Recommendations
The results of this case and the other reports summarized in this work indicate the need for including complete blood count and differentials in the routine workup (eg, twice weekly) for patients starting a long course of cefepime. In terms of case reporting, several gaps have been identified that led to challenges in assessing and collating the data, eg, none of the case reports assessed causality. Authors utilizing the Adverse Drug Reaction Probability Scale would aid in standardizing the assessment of causality.14 Additionally, a comprehensive presentation of patients’ laboratory data would be a great asset in identifying patterns of deterioration or resolution, as well as concurrent effect on other blood cells. Clear description of concurrent medications (ie, agents, start time, frequency, and duration) is essential to assess the certainty and probability of the hypothesized agent being the true culprit. Future research may be aimed at studying the prevalence of CIN in Qatar and potential risk factors of the development of CIN, including an ethnicity-based epidemiological study, which could shed light on the possibility of DIN risk being attributed to patients’ ethnicity and genetic differences.
Conclusion
The presented case report signifies potential adverse reactions associated with prolonged use of cefepime. Available literature highlights its rarity as a side effect; however, clinicians must exercise caution and be aware of CIN as a possibility with prolonged use of cefepime to prevent complications associated with neutropenia.
Ethics
This report was approved by the Medical Research Center (MRC) at Hamad Medical Corporation (HMC) in 2022 (MRC-04-22-688). Informed consent for publication of the patient’s deidentified case details was obtained from the patient before submission.
Acknowledgment
Open Access Funding provided by Qatar National Library.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bhatt V, Saleem A. Review: drug-induced neutropenia--pathophysiology, clinical features, and management. Ann Clin Lab Sci. 2004;34(2):131–137.
2. Justiz Vaillant AA, Zito PM. Neutropenia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
3. Rattay B, Benndorf RA. Drug-induced idiosyncratic agranulocytosis - infrequent but dangerous. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.727717
4. Andersohn F, Konzen C, Garbe E. Systematic review: agranulocytosis induced by nonchemotherapy drugs. Ann Intern Med. 2007;146(9):657. doi:10.7326/0003-4819-146-9-200705010-00009
5. Coates TD. Drug-induced neutropenia and agranulocytosis. In: UpToDate. Waltham, MA: UpToDate; 2023.
6. O’Connor A, Lopez MJ, Eranki AP. Cefepime. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
7. Post TW. Cefepime. In: UpToDate. Waltham, MA: UpTodate; 2023.
8. Foong KS, Hsueh K, Bailey TC, et al. A cluster of cefepime-induced neutropenia during outpatient parenteral antimicrobial therapy. Clin Infect Dis. 2019;69(3):534–537. doi:10.1093/cid/ciy1112
9. Hernández R, Delpiano L, Amador J, Arias M, Carrasco Delgado J. Neutropenia asociada al uso de cefepime en pacientes pediátricos con fibrosis quística. Rev Chil Infectol. 2019;36(1):112–114. doi:10.4067/S0716-10182019000100112
10. Malincarne L, Francisci D, Martinelli L, Masini G, Baldelli F. A case of severe cefepime-related neutropenia in a 15-year-old patient. Scand J Infect Dis. 2010;42(2):156–157. doi:10.3109/00365540903380503
11. Hettmer S, Heeney MM. Cefepime-induced neutropenia in a teenager. Pediatr Blood Cancer. 2008;51(5):715–716. doi:10.1002/pbc.21664
12. Wong BB, Ko GJ. Neutropenia in patients receiving long-term cefepime therapy for osteomyelitis. Am J Health Syst Pharm. 2003;60(21):2229–2232. doi:10.1093/ajhp/60.21.2229
13. Dahlgren AF. Two cases of possible cefepime-induced neutropenia. Am J Health Syst Pharm. 1997;54(22):2621–2622. doi:10.1093/ajhp/54.22.2621
14. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. doi:10.1038/clpt.1981.154
15. Holz JM, Chevtchenko AV, Aitullina A. Acute antibiotically induced neutropenia: a systematic review of case reports. Br J Clin Pharmacol. 2022;88(5):1978–1984. doi:10.1111/bcp.15170
16. Johnston A, Uetrecht J. Current understanding of the mechanisms of idiosyncratic drug-induced agranulocytosis. Expert Opin Drug Metab Toxicol. 2015;11(2):243–257. doi:10.1517/17425255.2015.985649
17. Curtis BR. Non–chemotherapy drug–induced neutropenia: key points to manage the challenges. Hematol Am Soc Hematol Educ Program. 2017;2017(1):187–193. doi:10.1182/asheducation-2017.1.187
18. Gatell JM, Rello J, Miro JM, Martinez JA, Soriano E, SanMiguel Garcia J. Cloxacillin-induced neutropenia. J Infect Dis. 1986;154(2):372. doi:10.1093/infdis/154.2.372
19. Jayaweera JAAS, Abeydeera WPH, Ranasinghe GR. Intravenously administered cloxacillin-induced neutropenia with eosinophilia in a patient with infective endocarditis: a case report. J Med Case Rep. 2018;12(1):384. doi:10.1186/s13256-018-1933-3
20. Briggs S, Smith S, Ritchie S, Fitzharris P, Ellis-Pegler R. Late-onset bolus intravenous beta-lactam antibiotic adverse reaction: short-lived symptoms during drug administration and associated laboratory abnormalities. Scand J Infect Dis. 2014;46(1):14–20. doi:10.3109/00365548.2013.849815
21. Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis. 2015;61(6):e26–e46. doi:10.1093/cid/civ482
22. Cimino C, Allos BM, Phillips EJ. A review of β-Lactam–associated neutropenia and implications for cross-reactivity. Ann Pharmacother. 2021;55(8):1037–1049. doi:10.1177/1060028020975646
23. Chaudhry SB, Veve MP, Wagner JL. Cephalosporins: a focus on side chains and β-Lactam cross-reactivity. Pharm J Pharm Educ Pract. 2019;7(3):103.
24. Uy N, Thiagarajan P, Musher DM. Cephalosporin side chain idiosyncrasies: a case report of ceftriaxone-induced agranulocytosis and review of literature. Open Forum Infect Dis. 2015;2(1). doi:10.1093/ofid/ofv007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.