Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Causal Associations Between Chronic Inflammatory Skin Diseases and Alzheimer’s Disease: A Bidirectional Two-Sample Mendelian Randomization Study
Authors Cai Y ![]() , Dai W, Liu F, Li Z, Liu G
, Dai W, Liu F, Li Z, Liu G
Received 15 December 2025
Accepted for publication 12 March 2026
Published 17 March 2026 Volume 2026:19 589176
DOI https://doi.org/10.2147/CCID.S589176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Yingying Cai,1– 4 Wei Dai,1,2 Fenglan Liu,1,2 Zhuorong Li,1,2 Gang Liu1,5
1School of Clinical Medicine, Chengdu Medical College, Chengdu, People’s Republic of China; 2Department of Geriatric Medicine, The First Affiliated Hospital of Chengdu Medical College, Chengdu, People’s Republic of China; 3Sichuan Clinical Research Center for Geriatrics, Chengdu, People’s Republic of China; 4Key Laboratory of Intelligent Medical Care and Elderly Health Management, Chengdu, People’s Republic of China; 5Department of Executive management, The First Affiliated Hospital of Chengdu Medical College, Chengdu, People’s Republic of China
Correspondence: Yingying Cai, Department of Geriatric Medicine, The First Affiliated Hospital of Chengdu Medical College, No. 278, Baoguang Avenue, Xindu District, Chengdu, Sichuan, 610500, People’s Republic of China, Email [email protected] Gang Liu, Department of executive management, The First Affiliated Hospital of Chengdu Medical College, No. 278, Baoguang Avenue, Xindu District, Chengdu, Sichuan, 610500, People’s Republic of China, Email [email protected]
Background: Inflammatory skin diseases (ISDs) and Alzheimer’s disease (AD) share chronic immune activation, but their causal link remains unclear.
Methods: We performed a bidirectional two-sample Mendelian randomization using GWAS summary data from Europeans. Instrumental SNPs were analyzed with inverse-variance weighted (IVW), weighted median, and MR-Egger methods, with sensitivity tests for pleiotropy and heterogeneity.
Results: Forward MR revealed significant causal effects of ISDs on AD, including lichen planus (OR 1.318, p=0.005), psoriasis vulgaris (OR 1.126, p=0.004), psoriasis with arthropathy (OR 1.032, p=0.002), psoriatic arthritis (OR 1.053, p=0.016), psoriasis (OR 1.072, p=0.008), papulosquamous conditions (OR 1.046, p=0.007), and follicular cysts (OR 1.066, p=0.047). No heterogeneity or pleiotropy was detected. Reverse analysis showed no causal effect of AD on ISDs.
Conclusion: These findings support a potential causal role of chronic skin inflammation in AD risk, though effect sizes were modest and clinical implications remain exploratory. This suggests that neuroimmune mechanisms may represent potential targets for further investigation.
Keywords: inflammatory skin diseases, alzheimer’s disease, psoriasis, lichen planus, systemic inflammation
Introduction
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder distinguished by the accumulation of amyloid-β (Aβ) plaques and the formation of intracellular neurofibrillary tangles composed of hyperphosphorylated tau protein, resulting in disrupted neuronal communication, neuroinflammation, and progressive cognitive decline.1 Clinically, AD is characterized by progressive memory impairment, language and visuospatial deficits, executive dysfunction, and neuropsychiatric symptoms that ultimately impair daily functioning and independence.2 The pathogenesis of AD is multifactorial, involving interactions between amyloid-β and tau pathology, dysregulated lipid metabolism, immune dysfunction, oxidative stress, and both genetic and environmental risk factors.3 Recent research has emphasized the critical role of immune-metabolic interactions in accelerating neurodegeneration,4 while cerebral microvascular dysfunction and other vascular or metabolic factors are increasingly recognized as important contributors to disease onset and progression.5,6 As AD continues to pose a substantial global burden, identifying modifiable risk factors remains a key public health objective.
Inflammatory skin diseases (ISDs) comprise a heterogeneous group of chronic immune-mediated disorders—including psoriasis, lichen planus, atopic dermatitis, rosacea, acne, hidradenitis suppurativa, and seborrheic dermatitis—all characterized by recurrent cutaneous inflammation.7,8 Papulosquamous diseases such as psoriasis and lichen planus typically present as scaling papules or plaques with distinctive histopathological and clinical features.9–11 Epidemiologically, oral lichen planus (OLP) has a pooled prevalence of 0.89% in the general population and 0.98% in clinical settings, while cutaneous lichen planus affects less than 1% of individuals.12,13 Psoriasis demonstrates a variable incidence, ranging from 30.3 to 321.0 per 100,000 person-years worldwide, and a prevalence from 0.14% in East Asia to 1.99% in Australasia, with peak incidence in midlife.14,15 The chronic plaque-type form accounts for the majority of psoriasis cases.16,17 Both conditions are frequently associated with comorbidities such as metabolic syndrome and systemic diseases, thereby amplifying their overall health impact.1,18
Emerging evidence suggests that ISDs and AD may share overlapping pathogenic mechanisms, providing a biological basis for their potential association. Both AD and ISDs are characterized by chronic inflammatory responses and dysregulated immune signaling. For example, pro-inflammatory cytokines such as interleukin-17 (IL-17) and tumor necrosis factor-alpha (TNF-α), which are central to the pathophysiology of psoriasis and lichen planus, also contribute to neuroinflammation and neurodegenerative cascades in AD. Furthermore, the skin and central nervous system originate from the embryonic ectoderm, supporting the concept of a “skin-brain axis” in which cutaneous immune disturbances may influence neuroinflammatory processes. This mechanistic overlap, encompassing chronic systemic inflammation, oxidative stress, and immune dysregulation, underscores a plausible biological pathway linking chronic skin inflammation to neurodegeneration and emphasizes the importance of exploring potential causal relationships between ISDs and AD.
To date, no study has definitively established a causal relationship between atopic dermatitis or other ISDs and AD. Observational research has reported an increased incidence of AD among individuals with ISDs; however, these associations are inherently limited by residual confounding from factors such as age, comorbidities, and lifestyle that may influence both conditions. Furthermore, the cross-sectional or cohort designs of these studies cannot easily exclude the possibility of reverse causation, where early, undiagnosed neuropathological processes might influence systemic inflammation or health behaviors. Earlier studies have also not fully addressed whether inflammation or metabolic disturbances act as intermediaries or are merely correlated bystanders. While available epidemiological and mechanistic studies suggest an elevated prevalence of neuropsychiatric symptoms in ISD populations,19–21 while experimental models highlight possible contributions of immune cells and mediators to cognitive decline.22 Mitochondrial dysfunction and oxidative stress, which are central to AD pathogenesis, may be amplified by neuroinflammatory activity,23,24 and the skin-brain axis is an emerging topic of interest.25 However, Mendelian randomization (MR) studies investigating cytokines such as (Interleukin-6) IL-6 and IL-18 have not found causal relationships with AD risk, leaving uncertainty about underlying pathways.26 Notably, cognitive impairment is more frequent in individuals with psoriasis and psoriatic arthritis compared to controls, with prevalence estimates of 44% and 91.9%, respectively.27,28 Despite these observations, the absence of rigorous MR research directly evaluating ISDs and AD remains a critical gap in the field. Addressing this gap is essential for clarifying causality and guiding prevention or intervention strategies.29
Mendelian randomization (MR) offers a powerful approach to address these limitations and strengthen causal inference. By using genetic variants as instrumental variables (IVs) for an exposure, MR mimics the random assignment of a randomized controlled trial. Because these genetic variants are inherited randomly and fixed at conception, their association with an outcome is generally free from confounding by environmental or lifestyle factors and is not susceptible to reverse causation. This property makes MR particularly suited to clarify whether the epidemiological associations between ISDs and AD reflect a true causal pathway.
To advance understanding in this area, the present study employs a bidirectional two-sample Mendelian randomization (TSMR) design to assess the potential causal association between ISDs—specifically psoriasis and lichen planus—and AD. These two skin diseases are selected for their well-established systemic inflammatory characteristics and higher prevalence of metabolic comorbidities, making them particularly relevant for examining shared mechanisms with AD. MR leverages the random allocation of genetic variants to minimize confounding and reverse causation, thus providing more robust causal inference compared to traditional observational studies.30 By employing genetic markers as instrumental variables (IVs), this approach seeks to clarify whether psoriasis and lichen planus contribute to AD risk. This study aims to enhance genetic epidemiological evidence regarding skin-brain interactions and to inform the development of preventive or therapeutic strategies to address the global burden of AD.
Method
Study Design
This study utilized a bidirectional TSMR design to investigate the causal relationship between ISDs (exposure) and AD (outcome) (Figure 1). The analysis employed genetic variants as IVs to infer causality. This study was conducted in strict compliance with the Strengthening the Reporting of Observational Studies in Epidemiology using Mendelian Randomization (STROBE-MR) guidelines to ensure methodological rigor and transparency.
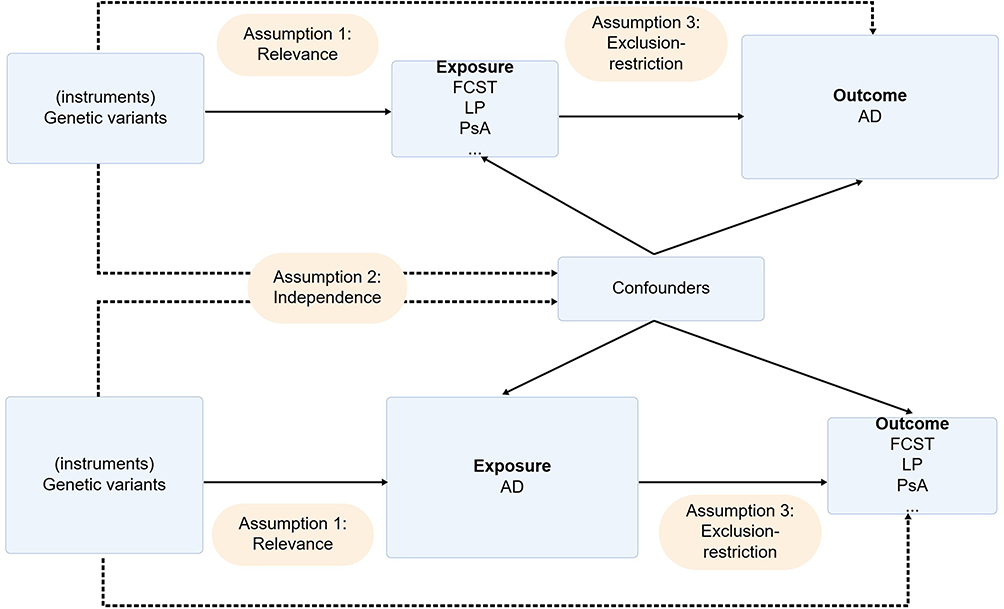 |
Figure 1 Conceptual framework of bidirectional Mendelian randomization (MR) study. Schematic overview of MR design assumptions: (1) Genetic instruments (single nucleotide polymorphisms, SNPs) strongly associate with exposures (follicular cysts of skin and subcutaneous tissue, FCST; lichen planus, LP; psoriasis with arthropathy, PsA; psoriatic arthritis, PsA) or outcome (Alzheimer’s disease, AD); (2) No confounding between instruments and exposure/outcome; (3) No direct instrument-outcome pathways excluding exposure-mediated effects. Bidirectional causality was tested between AD and multiple biomarkers/diseases using primary (inverse-variance weighted, IVW) and supplementary methods (MR-Egger, Weighted median). |
Data Sources
Data Sources of Exposure
The exposure data were sourced from genome-wide association studies (GWAS) datasets. Seven phenotypes related to ISDs were included: “Follicular Cysts of Skin and Subcutaneous Tissue”, “Lichen Planus”, “Psoriasis With Arthropathy”, “Psoriatic Arthritis”, “Psoriasis Vulgaris”, “Psoriasis”, and “Papulosquamous Conditions”. To address potential overlap among these phenotypes, particularly the psoriasis-related conditions (eg, psoriasis, psoriasis vulgaris, and psoriatic arthritis), we ensured that the GWAS data for each phenotype were derived from independent study populations, as indicated by nine distinct GWAS IDs, thereby minimizing sample overlap. Additionally, during instrumental variable selection, we applied a stringent clumping procedure (r2 < 0.001 within a 10,000 kb window) to guarantee SNP independence and avoid linkage disequilibrium. Sensitivity analyses were also performed by excluding SNPs associated with multiple phenotypes to assess the robustness of the MR estimates. The total number of single nucleotide polymorphisms (SNPs) ranged from 8,536,277 to 16,380,466 across studies. All participants in these datasets were of European ancestry, ensuring genetic homogeneity.
Data Sources of Outcome
The outcome data were also obtained from GWAS datasets, encompassing ten IDs related to AD. These IDs included finn-b-AD_EO_EXMORE, finn-b-G6_AD_WIDE, finn-b-G6_ALZHEIMER, ieu-a-297, ebi-a-GCST90027158, and ieu-b-2, among others. The number of participants for each ID ranged from 54,162 to 487,511, with case populations ranging from 587 to 39,106 and control populations from 37,154 to 468,828. All datasets were restricted to individuals of European ancestry, ensuring consistency in genetic analysis (Supplementary Table 1). The total number of SNPs included ranged from 7,055,882 to 20,921,626.
Screening of IVs
The screening of IVs was performed in accordance with the three fundamental assumptions of MR analysis: (1) IVs must be strongly associated with the exposure; (2) IVs must be independent of confounders; and (3) IVs must influence the outcome solely through the exposure pathway. The significance threshold for SNP inclusion was set at P < 5 × 10−8. To avoid linkage disequilibrium, the r2 threshold was set at < 0.001, and the genetic distance threshold at > 10,000 kb. The exposure and outcome datasets were harmonized by excluding strand-ambiguous SNPs with intermediate allele frequencies and ensuring an allele frequency (AF) greater than 10%. The F-statistic for the included SNPs was calculated, and only those with F > 10 were considered strong IVs for inclusion in the study.
Statistical Analysis
TSMR Analysis
The primary statistical method applied for the MR analysis was the inverse-variance weighted (IVW) method. This method was selected due to its ability to combine the Wald ratio estimates of the causal effects of different SNPs, thereby providing a consistent estimate of the causal effect of exposure on the outcome.31 Given the inclusion of several traits with a limited number of instrumental variables, sensitivity analyses (including weighted median and MR-Egger) were particularly emphasized to ensure robustness, as these methods provide reliable estimates under weaker instrument scenarios or in the presence of pleiotropy. Supplementary statistical methods were also applied to strengthen the accuracy and validity of the results. The weighted median method was included, which provides consistent estimates even if up to 50% of the weights originate from invalid IVs.32 Additionally, MR-Egger regression was used to account for horizontal pleiotropy, offering an unbiased estimation of causal association in the presence of horizontal pleiotropy.33 To account for the risk of false-positive findings due to multiple comparisons, a Bonferroni correction was applied. Given that seven independent skin traits were tested, the threshold for statistical significance was set at P < 0.007 (0.05/7).
Statistical analysis was conducted using R software (version 4.4.1) and the TwoSampleMR package, both of which are well-established tools for MR analysis. For power analysis, the F-statistic was used, with an F-statistic greater than 10 indicating no weak IV bias.34
Reverse TSMR Analysis
In the reverse direction, the IVW estimates provided no evidence supporting a causal effect of genetically predicted Alzheimer’s disease on arthropathic psoriasis (OR = 0.981, 95% CI: 0.864–1.115, p = 0.772), psoriatic arthritis under a broader Alzheimer’s disease definition (OR = 0.986, 95% CI: 0.895–1.085, p = 0.768), psoriasis vulgaris (OR = 0.965, 95% CI: 0.824–1.130, p = 0.660), overall psoriasis (OR = 1.012, 95% CI: 0.978–1.048, p = 0.490), papulosquamous disorders (OR = 1.054, 95% CI: 0.974–1.140, p = 0.191), or follicular cysts of the skin and subcutaneous tissue (OR = 0.977, 95% CI: 0.897–1.065, p = 0.599). Sensitivity analyses were generally consistent with the primary findings. Although heterogeneity was detected in several models, MR-Egger intercept tests did not indicate significant horizontal pleiotropy (all p > 0.05 where available), and leave-one-out analyses showed that exclusion of individual SNPs did not materially alter the IVW estimates. Overall, the reverse MR analyses did not support a causal effect of Alzheimer’s disease liability on the examined chronic inflammatory skin diseases.
Sensitivity Analysis
To test the stability of the instrumental variable effects, several sensitivity analysis methods were applied. The MR-Egger intercept was used to detect the presence of horizontal pleiotropy, with a significant intercept indicating directional pleiotropy.35 Cochran’s Q test was conducted to assess heterogeneity among the SNPs, which could indicate pleiotropy or other sources of heterogeneity.36 Leave-one-out (LOO) analysis was performed to evaluate the robustness of the results by assessing the impact of individual SNPs on the overall analysis,37 this approach is particularly valuable for traits instrumented by a small number of SNPs, as it ensures that no single variant is driving the observed association. The reverse sensitivity analysis mirrored these steps, interchanging the exposure and outcome as in the reverse TSMR analysis.
In conclusion, the statistical and sensitivity analyses were systematically designed to ensure the robustness and reliability of the findings in this MR study. These methods were selected for their strengths and relevance to the study objectives, reflecting current scientific practices in the field.
Result
Result of TSMR Analysis
This study employed a TSMR design to examine the causal association between various skin conditions and AD. A total of 110 SNPs were included in the analysis, with the distribution as follows: 3 for follicular cysts of the skin and subcutaneous tissue, 3 for lichen planus, 5 for psoriasis with arthropathy, 18 for psoriatic arthritis, 10 for psoriasis vulgaris, 59 for psoriasis, and 12 for papulosquamous conditions. The F-values ranged from 150.87 to 68,733.53, demonstrating strong instrument strength (Supplementary Tables 1–4).
Using the IVW method, we identified strong evidence supporting a causal association between follicular cysts of the skin and subcutaneous tissue and AD (OR: 1.066; 95% CI: 1.001–1.136; p = 0.047). However, after applying the Bonferroni-corrected significance threshold (P < 0.007), this association did not reach statistical significance. Sensitivity analyses indicated no heterogeneity (Q = 1.223; p = 0.542), no horizontal pleiotropy (MR-Egger p = 0.655), and robust findings in the LOO analysis. Similarly, lichen planus was causally associated with AD (OR: 1.318; 95% CI: 1.086–1.598; p = 0.005), with no evidence of heterogeneity (Q = 0.705; p = 0.703), no horizontal pleiotropy (MR-Egger p = 0.666), and consistent LOO results. For psoriasis with arthropathy, a causal association was observed (OR: 1.032; 95% CI: 1.011–1.053; p = 0.002), with no heterogeneity (Q = 1.926; p = 0.588), no horizontal pleiotropy (MR-Egger p = 0.944), and robust LOO results. Psoriatic arthritis demonstrated a causal relationship with AD (OR: 1.053; 95% CI: 1.010–1.098; p = 0.016), supported by the absence of heterogeneity (Q = 18.417; p = 0.363), no horizontal pleiotropy (MR-Egger p = 0.358), and robust LOO findings. Although the p-value for psoriatic arthritis was above the Bonferroni-corrected threshold, the consistency across sensitivity analyses supports the robustness of the finding. Psoriasis vulgaris also showed a causal association (OR: 1.126; 95% CI: 1.038–1.221; p = 0.004), with no heterogeneity (Q = 0.703; p = 0.951), no horizontal pleiotropy (MR-Egger p = 0.897), and stable LOO results. Psoriasis itself was linked to AD (OR: 1.072; 95% CI: 1.018–1.129; p = 0.008), with no evidence of heterogeneity (Q = 40.293; p = 0.709), no horizontal pleiotropy (MR-Egger p = 0.672), and robust LOO findings. Finally, papulosquamous conditions were found to have a causal association with AD (OR: 1.046; 95% CI: 1.012–1.080; p = 0.007), with no heterogeneity (Q = 8.730; p = 0.273), no horizontal pleiotropy (MR-Egger p = 0.118), and consistent LOO results (Figure 2–5). Overall, after applying multiple testing correction, associations for lichen planus, psoriasis with arthropathy, psoriasis vulgaris, and papulosquamous conditions remained statistically significant, while others showed consistent direction and robustness in sensitivity analyses.
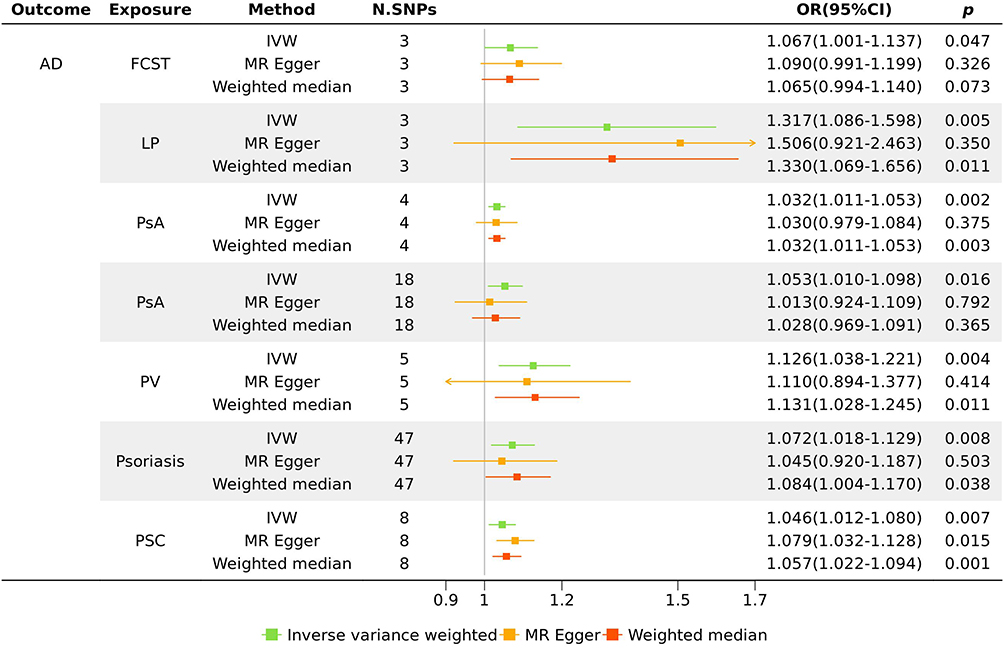 |
Figure 2 Causal associations between inflammatory skin diseases (ISDs) and Alzheimer’s disease (AD). Table summarizing Mendelian randomization (MR) results for asthma (exposure) and 6 outcomes. Effect estimates (odds ratio, OR), 95% confidence interval (CI), p-values, number of instrumental SNPs (single nucleotide polymorphisms, N.SNPs), and sensitivity analyses (inverse-variance weighted, IVW; MR-Egger; Weighted median) are shown. Significant causal effects (p < 0.05) were observed for multiple outcomes including follicular cysts of skin and subcutaneous tissue (FCST), lichen planus (LP), psoriasis with arthropathy (PsA), psoriatic arthritis (PsA), psoriasis vulgaris (PV), psoriasis, and papulosquamous conditions (PSC). |
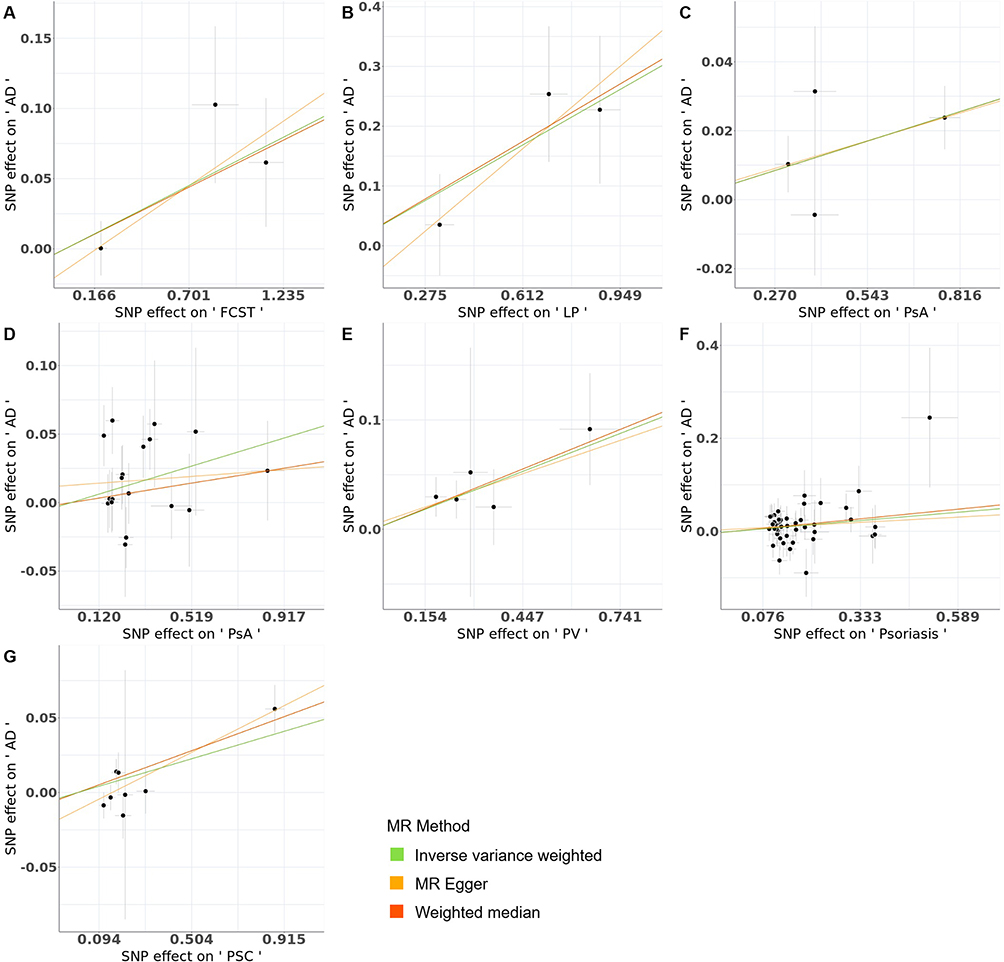 |
Figure 3 Scatter plots of single nucleotide polymorphism (SNP)-exposure effects against SNP-outcome effects. (A–G) Scatter plots showing causal estimates for: (A) follicular cysts of skin and subcutaneous tissue (FCST), (B) lichen planus (LP), (C) psoriasis with arthropathy (PsA), (D) psoriatic arthritis (PsA), (E) psoriasis vulgaris (PV), (F) psoriasis, and (G) papulosquamous conditions (PSC). Regression slopes represent causal effect size (βIV). Mendelian randomization (MR) methods (inverse-variance weighted, IVW: green line; MR-Egger: yellow line; Weighted median: Orange line) demonstrate consistent directional effects. |
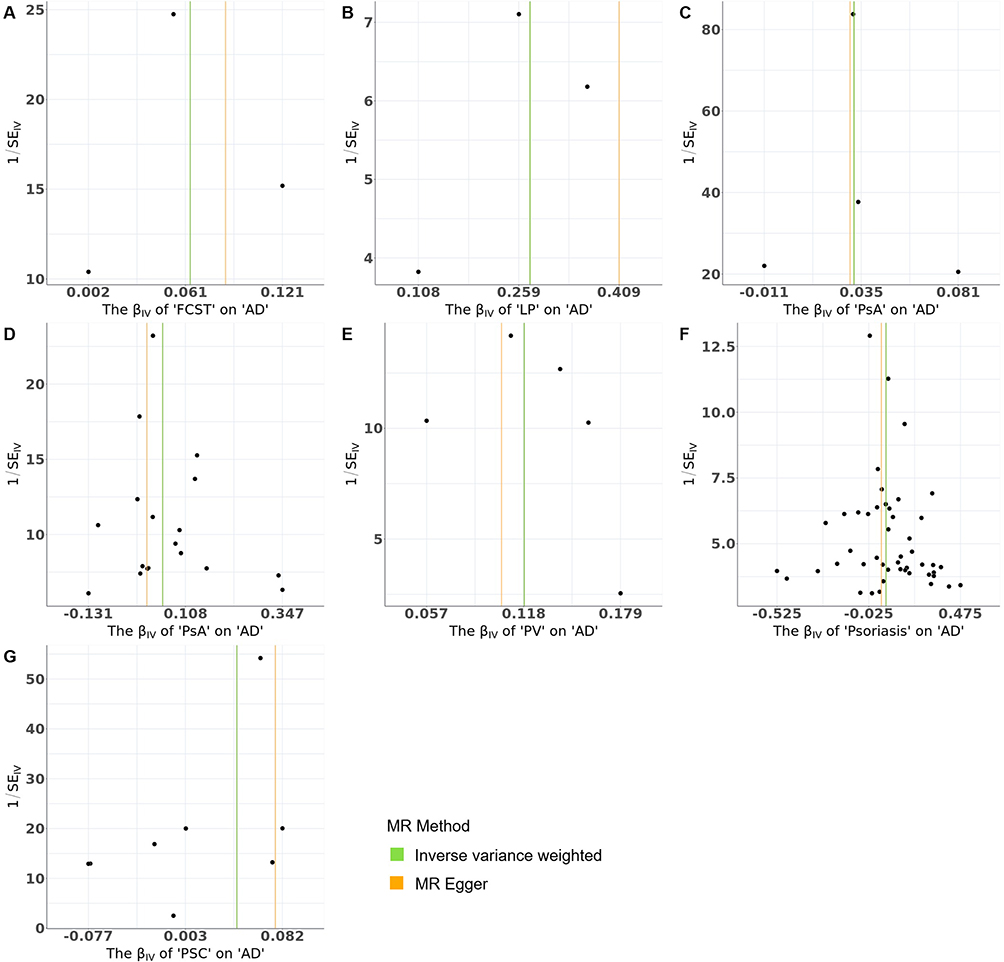 |
Figure 4 Forest plots of Mendelian randomization (MR) analyses for multiple exposures on Alzheimer’s disease (AD). Forest plots presenting causal effect estimates of multiple exposures on AD: (A) follicular cysts of skin and subcutaneous tissue (FCST), (B) lichen planus (LP), (C) psoriasis with arthropathy (PsA), (D) psoriatic arthritis (PsA), (E) psoriasis vulgaris (PV), (F) psoriasis, (G) papulosquamous conditions (PSC). Each subplot displays individual single nucleotide polymorphism (SNP) estimates (black dots) with Y-axis representing inverse of standard errors (1/SE) and X-axis showing causal effect sizes (β). Green vertical line indicates inverse-variance weighted (IVW) estimate, Orange vertical line represents MR-Egger estimate. |
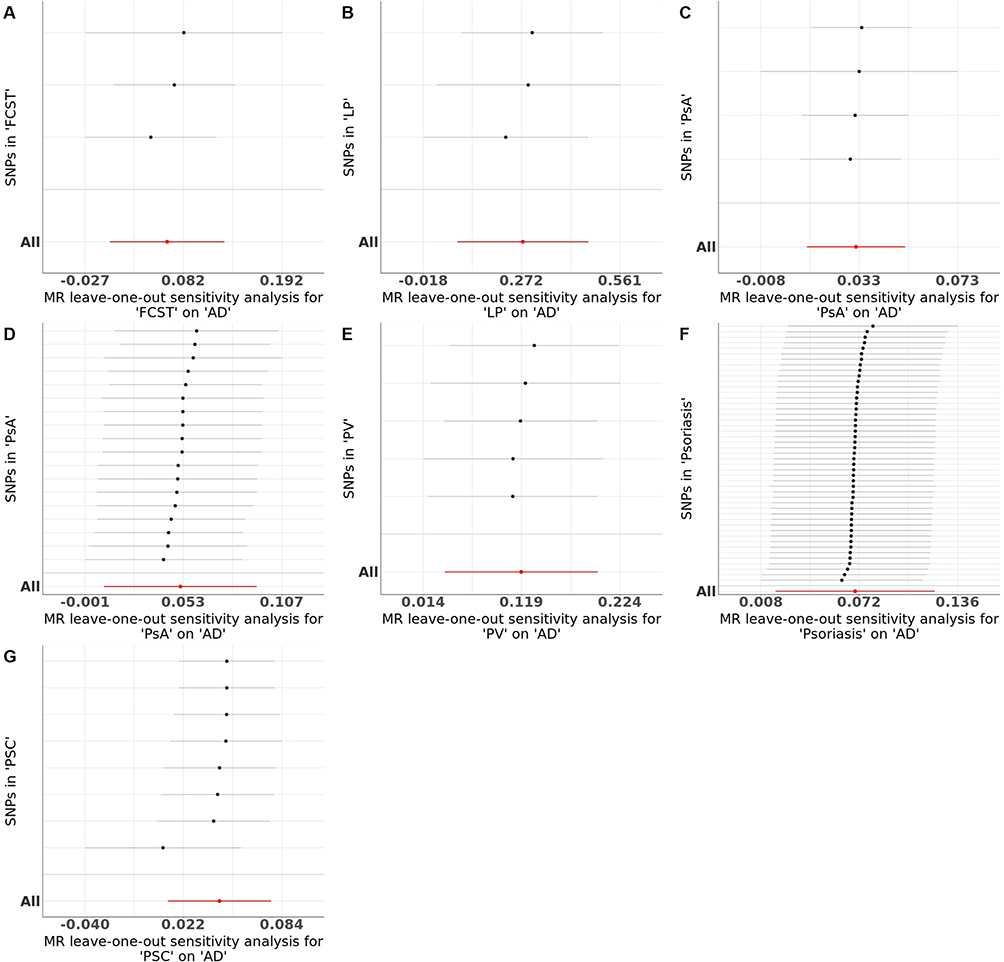 |
Figure 5 Leave-one-out (LOO) sensitivity analysis for bidirectional causal effects between inflammatory skin diseases (ISDs) and Alzheimer’s disease (AD). (A–G) Sequential exclusion of individual single nucleotide polymorphisms (SNPs) to test robustness of Mendelian randomization (MR) estimates for AD on: (A) follicular cysts of skin and subcutaneous tissue (FCST), (B) lichen planus (LP), (C) psoriasis with arthropathy (PsA), (D) psoriatic arthritis (PsA), (E) psoriasis vulgaris (PV), (F) psoriasis, (G) papulosquamous conditions (PSC). Red horizontal lines represent pooled inverse-variance weighted (IVW) estimates. Consistent effect sizes across all LOO iterations confirm that no single SNP disproportionately drove the causal associations. |
Result of Reverse TSMR Analysis
This study applied a reverse TSMR approach to evaluate potential causal associations between AD and several skin conditions, including follicular cysts of the skin and subcutaneous tissue, hypertrichosis, lichen planus, psoriasis with arthropathy, psoriatic arthritis, psoriasis vulgaris, psoriasis, papulosquamous conditions, and psoriatic and enteropathic arthropathies. The F-values were greater than 10, confirming strong instrument strength. No evidence of causal associations was identified between AD and any of the investigated skin conditions in the reverse TSMR analysis.
Discussion
This study employed MR to examine the potential causal relationships between chronic ISDs—including skin and subcutaneous follicular cysts, lichen planus, psoriasis (and its subtypes), and papulosquamous disorders—and AD, with the goal of informing treatment strategies and risk reduction approaches for susceptible populations. The importance of this research lies in addressing the complex and not yet fully understood pathogenesis of AD, in which chronic low-grade inflammation, potentially arising from localized sites such as the skin, may contribute to neurodegeneration, increased apoptosis, and brain atrophy characteristic of AD.38,39 Utilizing genetic data from public databases, MR analyses, including IVW methods and supplementary approaches, consistently demonstrated associations between these skin conditions and AD, with robust findings supported by multiple sensitivity analyses. These findings establish a foundation for investigating the interaction between systemic inflammation and neurodegenerative processes, providing context for a detailed discussion of their clinical implications and underlying mechanisms.
Evidence from MR analysis supports a possible causal association between psoriasis, psoriatic arthritis, and AD, likely mediated by shared inflammatory pathways. Mechanistically, activation of the Nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway is implicated in both neuroinflammation and neurodegeneration in AD,40,41 as well as in driving the inflammatory cascade in psoriasis.42 The S100 protein family, particularly S100 calcium-binding protein B (S100B), is upregulated in both AD and psoriasis, potentially exacerbating cerebral amyloidosis and gliosis in AD43 and amplifying inflammatory processes in psoriatic lesions.44,45 Several inflammatory cytokines, including IL-17, IL-6, Interleukin-23 receptor (IL-23R), Interleukin-12B (IL-12B), and TNF-α, are implicated in both conditions, with IL-17A in particular considered a driver of AD progression through the Toll-like receptor 4 (TLR4)/NF-κB pathway.46–48 Furthermore, the (Janus kinase/signal transducer and activator of transcription) JAK/STAT and Wnt/β-catenin pathways play pivotal roles in regulating immune responses and neuroinflammation in both AD and chronic ISDs.49–51 These findings highlight the potential of shared inflammatory mechanisms, suggesting that therapeutic interventions targeting pathways such as NF-κB, IL-17, or JAK/STAT might influence disease progression and could be further investigated for potential dual benefits in both conditions.
Oxidative stress emerges as a key contributory factor linking lichen planus, psoriasis, and AD. Elevated reactive oxygen species (ROS) can trigger mitochondrial dysfunction, including DNA mutations, impairment of the respiratory chain, and alterations in membrane permeability, all of which are believed to contribute to AD pathogenesis.52,53 In psoriasis and psoriatic arthritis, oxidative stress intensifies inflammation and tissue damage through ROS-mediated signaling.54–56 Similarly, in OLP, mitochondrial dysfunction associated with Succinate dehydrogenase complex iron sulfur subunit B (SDHB) overexpression has been linked to heightened oxidative stress.57 These findings suggest that oxidative stress may represent a shared pathogenic mechanism connecting AD with lichen planus and psoriasis. This underscores the potential of antioxidant therapies as preventive or therapeutic strategies and supports further investigation into oxidative stress modulators for reducing the burden of these diseases.
Abnormalities in glycolipid metabolism have also been identified as a possible shared mechanism among lichen planus, psoriasis, and AD. In AD, alterations in glucose metabolism and insulin resistance are recognized as early features, potentially promoting amyloidogenesis and neuroinflammation.58–60 For psoriasis, disturbances in glucose metabolism and dyslipidemia have been linked to disease activity and therapeutic response.61–63 Patients with OLP also exhibit a higher prevalence of abnormal glucose metabolism (such as diabetes mellitus and impaired glucose tolerance) and dyslipidemia, including elevated triglycerides and cholesterol, compared to controls.64–66 The recognition of abnormal glycolipid metabolism as a possible shared feature among these diseases raises the hypothesis that monitoring and managing metabolic parameters in patients with AD, lichen planus, and psoriasis could be beneficial. These findings highlight the potential value of early screening of glucose and lipid profiles and support further research into interventions targeting metabolic dysfunction in these populations.
Hormonal dysregulation may serve as another unifying risk factor for AD, lichen planus, and psoriasis. In AD, factors such as reduced estrogen signaling during menopause and decreased testosterone levels due to androgen deprivation therapy have been associated with increased risk.67,68 In psoriasis, lower estrogen levels have been associated with increased disease severity, with estrogens shown to suppress psoriasis-related cytokines.69 For OLP, higher follicle-stimulating hormone (FSH) and luteinizing hormone (LH) levels may influence disease mechanisms via estrogen and progesterone pathways, with estrogen proposed as a potential biomarker.70,71 These results indicate that hormonal dysregulation may represent a common risk factor for AD, lichen planus, and psoriasis, suggesting that hormone-based therapies or monitoring remain to be further explored as possible management strategies. This provides a rationale for additional studies on hormone-modulating treatments and their potential in slowing disease progression.
This investigation represents an early attempt to utilize MR to evaluate the potential causal association between chronic ISDs—including psoriasis, psoriatic arthritis, and lichen planus—and AD. By employing genetic variants as IVs, the study introduces a new analytical framework for causality assessment, addressing a significant gap in the current understanding of the relationship between dermatological and neurodegenerative disorders. Notably, the MR methodology adopted here seeks to overcome some of the inherent limitations observed in conventional MR approaches. In particular, this novel framework acknowledges the risk of overattributing causality to exposure factors, which may occur when broader social and biological contexts are not considered. By integrating the multifaceted roles of exposure variables within complex causal mechanisms, the study aims to provide a more nuanced interpretation of potential causal pathways, which may inform strategies for prevention. Furthermore, leveraging large-scale genetic datasets and functional genomics is expected to increase the accuracy of instrumental variable selection, reduce bias from environmentally driven variants, and enhance the robustness of the causal inferences drawn. These methodological advances may improve the validity of findings and contribute to evolving standards for MR analyses in complex disease research.
Despite these strengths, several limitations must be acknowledged. The use of summary-level data in this MR analysis restricts the capacity to investigate possible nonlinear associations between chronic ISDs and AD, potentially resulting in an incomplete characterization of the relationship. Future studies incorporating individual-level data could enable a more comprehensive exploration of nonlinear effects. Additionally, the exclusion of specific biological markers—such as cytokines including IL-17, IL-6, or TNF-α—as IVs may introduce residual confounding, given their established role in inflammatory pathways relevant to both skin diseases and neurodegeneration. Incorporating such biomarkers in future MR designs could improve the specificity and precision of causal inference.44–46 Moreover, the study’s focus on a relatively homogeneous ethnic population limits the generalizability of the results to broader and more diverse populations. Expanding future research to multi-ethnic cohorts would enhance the applicability and global relevance of these findings.
To address these limitations, several directions for future research should be considered. Employing advanced statistical approaches, such as nonlinear MR or machine learning-based analyses, may better capture the complex dynamics underlying the association between ISDs and AD. The integration of additional biomarkers, for instance, cytokines or S100 proteins, within the MR framework could provide further insights into the inflammatory mechanisms that potentially link these conditions.44–46 Broadening the scope of MR analyses to more diverse populations is likely to strengthen the external validity of observed associations and support the development of more inclusive prevention and intervention strategies. Collectively, these methodological improvements, together with a multidisciplinary focus that integrates genetic, biological, and environmental data, are anticipated to advance the understanding of the interplay between chronic ISDs and AD.
Overall, this MR analysis suggests a possible causal association between chronic ISDs—such as psoriasis, psoriatic arthritis, lichen planus, and papulosquamous disorders—and the risk of AD. The findings indicate that these conditions may share underlying pathophysiological mechanisms, including dysregulation of inflammatory pathways (for example, involving NF-κB, IL-17, and S100B), increased oxidative stress, disturbances in glycolipid metabolism, and hormonal imbalances. These mechanisms are thought to contribute to both skin inflammation and neurodegenerative processes. The IVW analyses, together with sensitivity assessments, support a potential association, with odds ratios demonstrating an elevated risk of AD among individuals with these chronic skin diseases. These results highlight the hypothesis that therapeutic strategies targeting shared inflammatory, metabolic, or hormonal pathways could be explored, although further research is needed to confirm these relationships and determine their clinical significance.
Conclusion
The MR framework used in this study enhances causal inference at the genetic level by addressing methodological challenges encountered in prior observational and genetic studies. However, several limitations should be considered, including the reliance on summary-level data, potential ethnic homogeneity of the sample, and the exclusion of certain biological markers. These factors may limit the generalizability and specificity of the conclusions. Future research incorporating individual-level data, diverse populations, and additional biomarkers may further clarify the relationship between chronic ISDs and AD. Overall, these findings may inform the development of hypotheses for integrated clinical strategies to manage shared risk factors and provide a rationale for further investigation into early diagnostic or personalized therapeutic approaches for both AD and chronic ISDs.
Abbreviations
AD, Alzheimer’s disease; AF, allele frequency; Aβ, amyloid-beta; CI, confidence interval; FCST, follicular cysts of skin and subcutaneous tissue; FSH, follicle-stimulating hormone; GWAS, genome-wide association studies; IL-17, interleukin-17; IL-6, interleukin-6; IL-12B, interleukin-12B; IL-23R, interleukin-23 receptor; ISDs, inflammatory skin diseases; IVs, instrumental variables; IVW, inverse-variance weighted; JAK/STAT, Janus kinase/signal transducer and activator of transcription; LH, luteinizing hormone; LOO, leave-one-out; LP, lichen planus; MR, Mendelian randomization; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; OLP, oral lichen planus; OR, odds ratio; PsA, psoriasis with arthropathy / psoriatic arthritis; PSC, papulosquamous conditions; Psoriasis, psoriasis; PV, psoriasis vulgaris; ROS, reactive oxygen species; S100B, S100 calcium-binding protein B; SDHB, succinate dehydrogenase complex iron sulfur subunit B; SNP, single nucleotide polymorphism; STROBE-MR, Strengthening the Reporting of Observational Studies in Epidemiology using Mendelian Randomization; TLR4, toll-like receptor 4; TNF-α, tumor necrosis factor-alpha; TSMR, two-sample Mendelian randomization.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Yingying Cai, upon reasonable request.
Ethics Approval and Consent to Participate
This study was reviewed and approved by the Medical Ethics Committee of The First Affiliated Hospital of Chengdu Medical College (Approval Letter No.: 2026CYFYIRB-BA-046). The study used publicly available summary-level data from genome-wide association studies (GWAS), which had obtained prior ethical approval and informed consent from participants in the original studies. As the data are de-identified and publicly accessible, the requirement for informed consent was waived by the ethics committee.
Acknowledgments
The authors gratefully acknowledge the technical support and professional guidance provided by Knowledge-Vision Co., Ltd. during this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Program of Health Commission of Sichuan Province [grant number 24LCYJPT07], the Sichuan Provincial Health Care Research Project [grant number 2023-2301], and the Sichuan Applied Psychology Research Center [grant number CSXL-22210].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Siddappaji KK, Gopal S. Molecular mechanisms in Alzheimer’s disease and the impact of physical exercise with advancements in therapeutic approaches. AIMS Neurosci. 2021;8(3):357–14. doi:10.3934/Neuroscience.2021020
2. Pless A, Ware D, Saggu S, et al. Understanding neuropsychiatric symptoms in Alzheimer’s disease: challenges and advances in diagnosis and treatment. Front Neurosci. 2023;17:1263771. doi:10.3389/fnins.2023.1263771
3. Wang Z, Zhang L, Qin C. Alzheimer’s disease pathogenesis: standing at the crossroad of lipid metabolism and immune response. Mol Neurodegener. 2025;20(1):67. doi:10.1186/s13024-025-00857-6
4. Rostagno AA. Pathogenesis of alzheimer’s disease. Int J Mol Sci. 2022;24(1):107. doi:10.3390/ijms24010107
5. Eisenmenger LB, Peret A, Famakin BM, et al. Vascular contributions to Alzheimer’s disease. Transl Res. 2023;254:41–53. doi:10.1016/j.trsl.2022.12.003
6. Iadecola C. Vascular and metabolic factors in alzheimer’s disease and related dementias: introduction. Cell Mol Neurobiol. 2016;36(2):151–154. doi:10.1007/s10571-015-0319-y
7. Sá DC, Festa CN. Inflammasomes and dermatology. An Bras Dermatol. 2016;91(5):566–578. doi:10.1590/abd1806-4841.20165577
8. Zhang XE, Zheng P, Ye SZ, et al. Microbiome: role in inflammatory skin diseases. J Inflamm Res. 2024;17:1057–1082. doi:10.2147/JIR.S441100
9. Sar-Pomian M, Starace MVR, Lencastre A, et al. Dermoscopic nail changes in psoriasis, lichen planus, and lichen striatus. Skin Appendage Disord. 2024;10(4):273–292. doi:10.1159/000538581
10. Abdusalamova K, Worm M, Solimani F. Hydroxychloroquine is safe and efficacious in oral lichen planus: data from a large outpatient cohort. Arch Dermatol Res. 2025;317(1):711. doi:10.1007/s00403-025-04226-7
11. Wang ZY, Fei WM, Li CX, et al. Comparison of dermoscopy and reflectance confocal microscopy accuracy for the diagnosis of psoriasis and lichen planus. Skin Res Technol. 2022;28(3):480–486. doi:10.1111/srt.13158
12. Boorghani M, Gholizadeh N, Taghavi Zenouz A, et al. Oral lichen planus: clinical features, etiology, treatment and management; a review of literature. J Dent Res Dent Clin Dent Prospects. 2010;4(1):3–9. doi:10.5681/joddd.2010.002
13. Li C, Tang X, Zheng X, et al. Global prevalence and incidence estimates of oral lichen planus: a systematic review and meta-analysis. JAMA Dermatol. 2020;156(2):172–181. doi:10.1001/jamadermatol.2019.3797
14. Parisi R, Iskandar IYK, Kontopantelis E, et al. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ. 2020;369:m1590. doi:10.1136/bmj.m1590
15. Wang K, Zhao Y, Cao X. Global burden and future trends in psoriasis epidemiology: insights from the global burden of disease study 2019 and predictions to 2030. Arch Dermatol Res. 2024;316(4):114. doi:10.1007/s00403-024-02846-z
16. Langley RG, Krueger GG, Griffiths CE. Psoriasis: epidemiology, clinical features, and quality of life. Ann Rheum Dis. 2005;64 Suppl 2(Suppl 2):
17. Dogra S, Mahajan R. Psoriasis: epidemiology, clinical features, co-morbidities, and clinical scoring. Indian Dermatol Online J. 2016;7(6):471–480. doi:10.4103/2229-5178.193906
18. Michalek IM, Loring B, John SM. A systematic review of worldwide epidemiology of psoriasis. J Eur Acad Dermatol Venereol. 2017;31(2):205–212. doi:10.1111/jdv.13854
19. Katamanin OM, Tan IJ, Barry J, et al. Role of inflammation and cytokine dysregulation in depression in patients with inflammatory skin conditions. Am J Clin Dermatol. 2025;26(1):35–43. doi:10.1007/s40257-024-00905-9
20. Jalenques I, Lauron S, Almon S, et al. Prevalence and odds of signs of depression and anxiety in patients with lichen planus: systematic review and meta-analyses. Acta Derm Venereol. 2020;100(18):adv00330. doi:10.2340/00015555-3660
21. Chen Z, Balachandran YL, Chong WP, et al. Roles of cytokines in alzheimer’s disease. Int J Mol Sci. 2024;25(11):5803. doi:10.3390/ijms25115803
22. Brigas HC, Ribeiro M, Coelho JE, et al. IL-17 triggers the onset of cognitive and synaptic deficits in early stages of Alzheimer’s disease. Cell Rep. 2021;36(9):109574. doi:10.1016/j.celrep.2021.109574
23. Simoncini C, Orsucci D, Caldarazzo Ienco E, et al. Alzheimer’s pathogenesis and its link to the mitochondrion. Oxid Med Cell Longev. 2015;2015:803942. doi:10.1155/2015/803942
24. Fang D, Zhang Z, Li H, et al. Increased electron paramagnetic resonance signal correlates with mitochondrial dysfunction and oxidative stress in an alzheimer’s disease mouse brain. J Alzheimers Dis. 2016;51(2):571–580. doi:10.3233/JAD-150917
25. Klostermeier S, Li A, Hou HX, et al. Exploring the skin brain link: biomarkers in the skin with implications for aging research and alzheimer’s disease diagnostics. Int J Mol Sci. 2023;24(17):13309. doi:10.3390/ijms241713309
26. Tsui A, Davis D. Systemic inflammation and causal risk for Alzheimer’s dementia: possibilities and limitations of a Mendelian randomization approach. Aging Med. 2018;1(3):249–253. doi:10.1002/agm2.12046
27. Garcia L, Júnior ATS, Gómez D, et al. Cognitive impairment in patients with psoriatic arthritis. Acta Neurol Belg. 2022;122(1):91–96. doi:10.1007/s13760-021-01644-y
28. Di Carlo M, Becciolini A, Incorvaia A, et al. Mild cognitive impairment in psoriatic arthritis: prevalence and associated factors. Medicine. 2021;100(11):e24833. doi:10.1097/MD.0000000000024833
29. Burgess S, Woolf B, Mason AM, et al. Addressing the credibility crisis in Mendelian randomization. BMC Med. 2024;22(1):374. doi:10.1186/s12916-024-03607-5
30. Sekula P, Del Greco MF, Pattaro C, et al. Mendelian randomization as an approach to assess causality using observational data. J Am Soc Nephrol. 2016;27(11):3253–3265. doi:10.1681/ASN.2016010098
31. Sanderson E, Glymour MM, Holmes MV, et al. Mendelian randomization. Nat Rev Meth Primers. 2022;2:6. doi:10.1038/s43586-021-00092-5
32. Bowden J, Davey Smith G, Haycock PC, et al. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
33. Bowden J. Misconceptions on the use of MR-Egger regression and the evaluation of the InSIDE assumption. Int J Epidemiol. 2017;46(6):2097–2099. doi:10.1093/ije/dyx192
34. Hemani G, Zheng J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. 2018;7:e34408. doi:10.7554/eLife.34408
35. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
36. Greco MF, Minelli C, Sheehan NA, et al. Detecting pleiotropy in Mendelian randomisation studies with summary data and a continuous outcome. Stat Med. 2015;34(21):2926–2940. doi:10.1002/sim.6522
37. Li L, Ren Q, Zheng Q, et al. Causal associations between gastroesophageal reflux disease and lung cancer risk: a Mendelian randomization study. Cancer Med. 2023;12(6):7552–7559. doi:10.1002/cam4.5498
38. Tiwari S, Atluri V, Kaushik A, et al. Alzheimer’s disease: pathogenesis, diagnostics, and therapeutics. Int J Nanomed. 2019;14:5541–5554. doi:10.2147/IJN.S200490
39. Weijie Z, Meng Z, chunxiao W, et al. Obesity-induced chronic low-grade inflammation in adipose tissue: a pathway to Alzheimer’s disease. Ageing Res Rev. 2024;99:102402. doi:10.1016/j.arr.2024.102402
40. Sivamaruthi BS, Raghani N, Chorawala M, et al. NF-κB pathway and its inhibitors: a promising frontier in the management of alzheimer’s disease. Biomedicines. 2023;11(9):2587. doi:10.3390/biomedicines11092587
41. Bhardwaj S, Grewal AK, Singh S, et al. An insight into the concept of neuroinflammation and neurodegeneration in Alzheimer’s disease: targeting molecular approach Nrf2, NF-κB, and CREB. Inflammopharmacology. 2024;32(5):2943–2960. doi:10.1007/s10787-024-01502-2
42. Irrera N, Bitto A, Vaccaro M, et al. PDRN, a bioactive natural compound, ameliorates imiquimod-induced psoriasis through NF-κB pathway inhibition and Wnt/β-Catenin signaling modulation. Int J Mol Sci. 2020;21(4):1215. doi:10.3390/ijms21041215
43. Mori T, Koyama N, W ARENDASHG, et al. Overexpression of human S100B exacerbates cerebral amyloidosis and gliosis in the Tg2576 mouse model of Alzheimer’s disease. Glia. 2010;58(3):300–314. doi:10.1002/glia.20924
44. Liang H, Li J, Zhang K. Pathogenic role of S100 proteins in psoriasis. Front Immunol. 2023;14:1191645. doi:10.3389/fimmu.2023.1191645
45. Saito-Sasaki N, Sawada Y. S100 proteins in the pathogenesis of psoriasis and atopic dermatitis. Diagnostics. 2023;13(20):3167. doi:10.3390/diagnostics13203167
46. Cao M, Liu J, Zhang X, et al. IL-17A promotes the progression of Alzheimer’s disease in APP/PS1 mice. Immun Ageing. 2023;20(1):74. doi:10.1186/s12979-023-00397-x
47. Taipa R, Das Neves SP, Sousa AL, et al. Proinflammatory and anti-inflammatory cytokines in the CSF of patients with Alzheimer’s disease and their correlation with cognitive decline. Neurobiol Aging. 2019;76:125–132. doi:10.1016/j.neurobiolaging.2018.12.019
48. Furue K, Ito T, Furue M. Differential efficacy of biologic treatments targeting the TNF-α/IL-23/IL-17 axis in psoriasis and psoriatic arthritis. Cytokine. 2018;111:182–188. doi:10.1016/j.cyto.2018.08.025
49. Rusek M, Smith J, El-Khatib K, et al. The role of the JAK/STAT signaling pathway in the pathogenesis of alzheimer’s disease: new potential treatment target. Int J Mol Sci. 2023;24(1):864. doi:10.3390/ijms24010864
50. Liu X, Wang K, Wei X, et al. Interaction of NF-κB and Wnt/β-catenin signaling pathways in alzheimer’s disease and potential active drug treatments. Neurochem Res. 2021;46(4):711–731. doi:10.1007/s11064-021-03227-y
51. Tian F, Mauro TM, Li Z. The pathological role of Wnt5a in psoriasis and psoriatic arthritis. J Cell Mol Med. 2019;23(9):5876–5883. doi:10.1111/jcmm.14531
52. Singh A, Kukreti R, Saso L, et al. Oxidative stress: a key modulator in neurodegenerative diseases. Molecules. 2019;24(8):1583. doi:10.3390/molecules24081583
53. Butterfield DA, Boyd-Kimball D. Mitochondrial oxidative and nitrosative stress and alzheimer disease. Antioxidants. 2020;9(9):818. doi:10.3390/antiox9090818
54. Bilski R, Kupczyk D, Woźniak A. Oxidative imbalance in psoriasis with an emphasis on psoriatic arthritis: therapeutic antioxidant targets. Molecules. 2024;29(22):5460. doi:10.3390/molecules29225460
55. Ahmad Jamil H, Abdul Karim N. Unraveling mitochondrial reactive oxygen species involvement in psoriasis: the promise of antioxidant therapies. Antioxidants. 2024;13(10):1222. doi:10.3390/antiox13101222
56. Gabr SA, Al-Ghadir AH. Role of cellular oxidative stress and cytochrome c in the pathogenesis of psoriasis. Arch Dermatol Res. 2012;304(6):451–457. doi:10.1007/s00403-012-1230-8
57. Zhang H, Xu B, Liu J, et al. SDHB reduction promotes oral lichen planus by impairing mitochondrial respiratory function. Ann Transl Med. 2022;10(24):1367. doi:10.21037/atm-22-5999
58. Wang Q, Duan L, Li X, et al. Glucose metabolism, neural cell senescence and alzheimer’s disease. Int J Mol Sci. 2022;23(8):4351. doi:10.3390/ijms23084351
59. Kumar V, Kim SH, Bishayee K. Dysfunctional glucose metabolism in alzheimer’s disease onset and potential pharmacological interventions. Int J Mol Sci. 2022;23(17):9540. doi:10.3390/ijms23179540
60. Yin F. Lipid metabolism and Alzheimer’s disease: clinical evidence, mechanistic link and therapeutic promise. Febs J. 2023;290(6):1420–1453. doi:10.1111/febs.16344
61. Grygiel-Górniak B, Skoczek W. Molecular background and clinical implications of glucose disorders in patients with psoriatic arthritis. J Clin Med. 2023;12(18):5814. doi:10.3390/jcm12185814
62. Nowowiejska J, Baran A, Flisiak I. Aberrations in lipid expression and metabolism in psoriasis. Int J Mol Sci. 2021;22(12):6561. doi:10.3390/ijms22126561
63. Luo L, Guo Y, Chen L, et al. Crosstalk between cholesterol metabolism and psoriatic inflammation. Front Immunol. 2023;14:1124786. doi:10.3389/fimmu.2023.1124786
64. Seyhan M, Ozcan H, Sahin I, et al. High prevalence of glucose metabolism disturbance in patients with lichen planus. Diabet Res Clin Pract. 2007;77(2):198–202. doi:10.1016/j.diabres.2006.12.016
65. Li KY, Li CL, Hua H, et al. Potential relationship of dyslipidemia with dietary patterns in oral lichen planus patients-A case-control study. J Dent Sci. 2023;18(4):1638–1644. doi:10.1016/j.jds.2023.01.006
66. Xiao X, Song Z, Liu S. Potential implication of serum lipid levels as predictive indicators for monitoring oral lichen planus. J Dent Sci. 2024;19(2):1307–1311. doi:10.1016/j.jds.2023.12.026
67. Uddin MS, Rahman MM, Jakaria M, et al. Estrogen signaling in alzheimer’s disease: molecular insights and therapeutic targets for alzheimer’s dementia. Mol Neurobiol. 2020;57(6):2654–2670. doi:10.1007/s12035-020-01911-8
68. Bianchi VE. Impact of testosterone on alzheimer’s disease. World J Mens Health. 2022;40(2):243–256. doi:10.5534/wjmh.210175
69. Adachi A, Honda T. Regulatory roles of estrogens in psoriasis. J Clin Med. 2022;11(16):4890. doi:10.3390/jcm11164890
70. Lavaee F, Bazrafkan N, Zarei F, et al. Follicular-stimulating hormone, luteinizing hormone, and prolactin serum level in patients with oral lichen planus in comparison to healthy population. Biomed Res Int. 2021;2021:8679505. doi:10.1155/2021/8679505
71. Agrawal H, Patil RK, Singh V, et al. Salivary and serum estrogen level assessment in oral lichen planus patients and its correlative analysis with OLP and stress. J Family Med Prim Care. 2024;13(5):1998–2005. doi:10.4103/jfmpc.jfmpc_1332_23
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Morin Mitigates Methamphetamine-Induced Neurotoxicity: Effects on Motor and Cognitive Function
Anyanwu GE, Umeano AV, Ojiakor VO, Katchy AU, Anyanwu CN, Fakorede S
Journal of Experimental Pharmacology 2025, 17:307-321
Published Date: 11 June 2025
L-α-GPC in Cognitive Decline: Mechanisms and Clinical Evidence in Neurodegenerative Disorders
Putri VA, Hapsari RS, Amalia R
Neuropsychiatric Disease and Treatment 2026, 22:579603
Published Date: 19 May 2026