Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Categorization of COPD patients in Turkey via GOLD 2013 strategy document: ALPHABET study
Authors Gunen H, Yilmaz M, Aktas O, Ergun P, Ortakoylu MG, Demir A, Cetinkaya P, Gurgun A, Otlu M, Cilli A, Yilmaz U, Kokturk N, Candemir I, Yakar H ![]() , Ar I, Konya A
, Ar I, Konya A
Received 28 April 2015
Accepted for publication 26 August 2015
Published 13 November 2015 Volume 2015:10(1) Pages 2485—2494
DOI https://doi.org/10.2147/COPD.S87464
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Hakan Gunen,1 Mehmet Yilmaz,2 Oguz Aktas,1 Pinar Ergun,3 Mediha Gonenc Ortakoylu,4 Atike Demir,5 Pelin Cetinkaya,6 Alev Gurgun,7 Muge Otlu,8 Aykut Cilli,9 Ufuk Yilmaz,5 Nurdan Kokturk,10 Ipek Candemir,3 Halil Ibrahim Yakar,1 Idilhan Ar,11 Aylin Konya11
1Department of Chest Diseases, Sureyyapasa Chest Diseases and Thoracic Surgery Training and Research Hospital, Istanbul, Turkey; 2Department of Chest Diseases, Safranbolu State Hospital, Karabuk, Turkey; 3Department of Chest Diseases, Ataturk Chest Diseases and Thoracic Surgery Training and Research Hospital, Ankara, Turkey; 4Department of Chest Diseases, Yedikule Chest Diseases and Thoracic Surgery Training and Research Hospital, Istanbul, Turkey; 5Department of Chest Diseases, Dr Suat Seren Chest Diseases and Thoracic Surgery Training and Research Hospital, Izmir, Turkey; 6Department of Chest Diseases, Cukurova Dr Askim Tufekci State Hospital, Adana, Turkey; 7Department of Chest Diseases, Ege University Faculty of Medicine, Izmir, Turkey; 8Department of Chest Diseases, Bingol State Hospital, Bingol, Turkey; 9Department of Chest Diseases, Akdeniz University, Faculty of Medicine, Antalya, Turkey; 10Department of Chest Diseases, Gazi University Faculty of Medicine, Ankara, Turkey; 11Medical Department, Novartis Pharmaceuticals, Istanbul, Turkey
Objective: To determine distribution of COPD assessment categories and physicians’ adherence to Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2013 strategy in Turkish COPD patients.
Methods: A total of 1,610 COPD patients (mean [standard deviation] age: 62.6 [9.9] years, 85.7% were males) were included in this multicenter, non-interventional, cross-sectional study. Patients were categorized via GOLD 2013 strategy document. Consistency between reported and re-classified GOLD categories, and measures used for symptom evaluation and exacerbation was analyzed.
Results: Overall, 41.1% of patients were assigned to GOLD A, while 13.2% were assigned to GOLD C categories. Long-acting beta-2 agonist + long-acting muscarinic antagonist + inhaled corticosteroid regimen was the most common treatment (62.0%). Over-treatment was noted in >70% of GOLD A, B, and C patients. A high consistency between measures of symptom evaluation (Kappa coefficient =0.993, P<0.0001) and a low-moderate consistency between exacerbation risk measures (Kappa coefficient =0.237, P<0.0001) were noted.
Conclusion: Our findings revealed GOLD A as the most prevalent category in Turkish cohort of COPD patients. Group assignment was altered depending on the chosen measure for symptom and risk assessment. Physician non-adherence to treatment recommendations in GOLD 2013 document leading to over-treatment in patients assigned to GOLD A, B, and C categories was also detected.
Keywords: combined COPD assessment, symptoms, exacerbation risk, physician adherence, Turkey
Introduction
COPD is one of the leading causes of morbidity and mortality worldwide.1 COPD prevalence in the population aged over 40 years was reported to range from 9.1% to 19.1% in Turkey,2–4 while the national disease burden report revealed that COPD was the third leading cause of mortality and eighth leading cause of disability.5
On the basis of recent recognition of the multidimensional nature of COPD and consequent emphasis placed on symptoms and exacerbations, airflow limitation alone has been considered not sufficient to reflect the true burden of the disease and to entirely reflect the heterogeneity of the COPD patient population.1,6–9 Accordingly, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) committee published a revised “combined COPD assessment” classification. A multidimensional approach has been proposed in the GOLD 2013 update.1
In Turkey, recommendations in local guidelines for COPD are consistent with the GOLD strategy. However, to the best of our knowledge, no study has been published in Turkey, or in worldwide medical literature, on the distribution of patients with COPD according to the GOLD 2013 strategy as the primary objective. Therefore the present non-interventional cross-sectional single-visit study was designed to determine distribution of combined COPD assessment categories described in GOLD 2013 strategy document among Turkish COPD patients. This study was also aimed to determine physicians’ adherence to 2013 update of the multidimensional GOLD strategy in the daily clinical practice and to compare physician subjective vs risk/symptom objective criteria assignment of patients to GOLD categories.
Methods
Study population
This multicenter, non-interventional, cross-sectional study was conducted at 12 secondary/tertiary care hospitals across Turkey between June and December 2013. To represent the distribution of COPD outpatient clinics in Turkey, the centers were selected according to the model of distribution to include six training and research hospitals, three university hospitals, three multidisciplinary state hospitals, and a pulmonary diseases hospital.
In Turkey, patients’ pathway in COPD care usually starts in secondary or tertiary care hospitals by specialists, mostly pulmonologists. Specialists can initiate COPD treatment according to regulations. Diagnosis, treatment, and follow-up of COPD patients are managed by specialists, especially pulmonologists. General practitioners and family practitioners are rarely involved in the diagnosis, treatment, and follow-up of COPD patients. All patients can apply to all clinics and hospitals, a referral system is not operated in Turkey.
Male and female patients aged ≥40 years, previously diagnosed with COPD by a pulmonologist with stable COPD at the time of enrollment, with smoking history (≥10 pack/years), and who were being followed-up as outpatients were included in the study. Patients with COPD exacerbations necessitating hospitalization due to worsening of COPD symptoms, or need for systemic corticosteroid and/or additional bronchodilator treatment, or change in COPD maintenance treatment for exacerbation within the last month or at the study enrollment, as well as pregnant/lactating women were excluded.
The study was approved by the Ethics Committee of Yeditepe University Hospital. Written informed consent was obtained from each subject following a detailed explanation of the protocol of the study. All study procedures were conducted in accordance with the ethical principles stated in the Declaration of Helsinki.
Study parameters
Data on patient demographics, COPD duration, co-morbidities, hospitalization associated with COPD, smoking status, spirometry findings, combined COPD assessment methods and related COPD categories, and selected treatment protocols were recorded. Consistent with non-interventional design, selection of treatment protocols, and diagnostic/therapeutic methods were at physicians’ discretion according to the local prescribing information and routine medical practices.
GOLD categories reported by physicians were compared with the re-classified GOLD categories in terms of consistency. If more than one method was reported for symptom evaluation or exacerbation risk, the one with worst findings was used for re-classification. Additionally, selected treatments for each GOLD category were grouped as first-line, alternative, other possible alternative, over-, or under-treatment as recommended by GOLD 2013 (Table S1 in the Supplementary material).1 Re-classification was based on calculations made using data previously collected by physicians. Physician assigned rather than re-classified GOLD was considered in analysis to reflect real-life bedside data regarding physicians’ assessments in COPD categorization.
Combined COPD assessment according to GOLD 2013 document
Evaluation of symptoms was based on Medical Research Council dyspnea scale (mMRC)10 or COPD assessment test (CAT)11 scores to indicate whether the patient has less symptoms (mMRC score 0–1 or CAT score <10) or more symptoms (mMRC score ≥2 or CAT ≥10). Exacerbation risk was determined using both GOLD spirometry classification of airflow limitation based on post-bronchodilator forced expiratory volume in 1 second (FEV1) values and by evaluating the number of exacerbations within the past 12 months. The worse of the two evaluations was considered in the classification. In addition, at least one hospitalization for a COPD exacerbation during the past 12 months was considered as high risk. In case of an inconsistency between spirometry and exacerbation history, the assessment indicating the highest risk was used.1 Accordingly, patients were classified in categories of A (low risk, less symptoms), B (low risk, more symptoms), C (high risk, less symptoms), and D (high risk, more symptoms).1
Statistical analysis
The sample size calculation was based on the estimated COPD prevalence of 20% in Turkey in the light of previous publications.2–4,12 For a single proportion, a sample size of 1,022 was estimated to yield a COPD prevalence of 20% (with a 5% error margin) at 95% confidence interval using the two-way confidence intervals formula13 with targeted proportion ranged from 17.5% to 22.5%. This sample size was considered to be sufficient also to demonstrate a prevalence lower than 20% with a 5% error margin. Since a higher rate of missing data was expected in line with the study design, the calculated sample size was increased by 50% leading to at least 1,500 patients being included in the study. With the total of 1,610 patients included, the margin of error was reduced to 4%.
Statistical analysis was made using computer software SPSS version 22.0 (IBM Corporation, Armonk, NY, USA). Consistency for dichotomous variable was evaluated with Kappa test, whereas association for ordinal variable was evaluated via Gamma test. Coefficient value of Kappa or Gamma test ranges from −1 to 1 and −1 and 1 represent high consistency or association whereas 0 represents none. Data were expressed as mean (standard deviation [SD]), median, interquartile range, minimum–maximum and percent (%) where appropriate. P<0.05 was considered statistically significant.
Results
Patient characteristics
COPD patients (n=1,610) with a mean (SD) age of 62.6 (9.9) years (85.7% males) were enrolled. Mean (SD) duration of COPD was determined to be 6.4 (6.0) years, 31.5% of patients were active smokers and cardiovascular disease was the leading co-morbid disorder (40%) (Table 1).
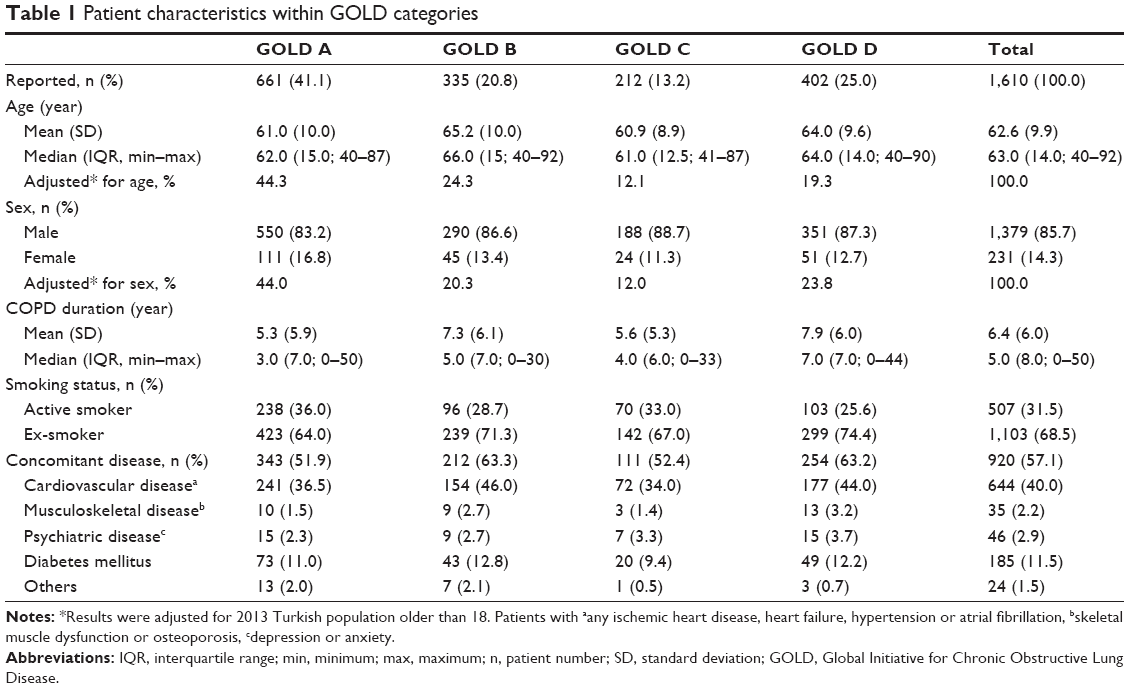 | Table 1 Patient characteristics within GOLD categories |
Based on pulmonary function test findings available in 1,414 (87.8%) patients, mean (SD)/median (min–max) values for predicted forced vital capacity was 69.4 (20.8)%/69.0 (16.0–139.0)%, for predicted FEV1 was 55.9 (20.9)%/55.0 (11.0–142.0)%, and for FEV1/forced vital capacity was 65.7 (14.6)%/66.0 (29.0–125.0)%.
GOLD categories with respect to patient characteristics
According to combined COPD evaluation by physicians, GOLD A category was the most commonly identified category (41.1%), while GOLD C was identified only in 13.2% of patients (Table 1). Demographics and disease characteristics according to GOLD categories are presented in Table 1.
Selected treatment regimens
Long-acting beta-2 agonist (LABA) + long-acting muscarinic antagonist (LAMA) + inhaled corticosteroid (ICS) regimen was the most commonly selected treatment (62.0% of all patients; with an increase as the category worsens, from 49.5% in GOLD A to 78.9% in GOLD D category).
Qualitative assessment of patient treatment (first-line, over, and under) with respect to GOLD 2013 document
Overall the selected treatment protocol was the first-line treatment according to GOLD 2013 in 26.5% of the patients, while over-treatment was noted in 56.6%. The rate of first-line treatment increased, while over-treatment was determined to decrease, as the GOLD category worsens (Table 2).
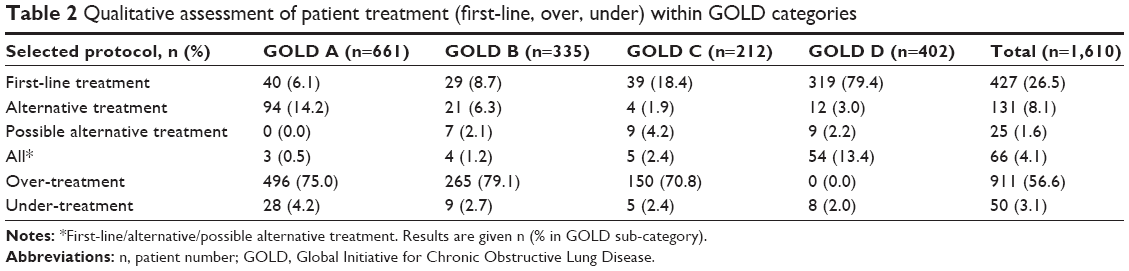 | Table 2 Qualitative assessment of patient treatment (first-line, over, under) within GOLD categories |
Treatment specifics within GOLD categories LABA + ICS and LABA + LAMA + ICS regimens were the leading treatments selected inappropriately for the patients in GOLD A (21% and 49.5%, respectively) and GOLD B categories (17.6% and 61.2%, respectively), despite not being recommended for this group according to the GOLD 2013 document. LABA + LAMA + ICS treatment was also noted to be selected in 70.3% of patients in GOLD C category despite not being recommended for this group (Table 3).
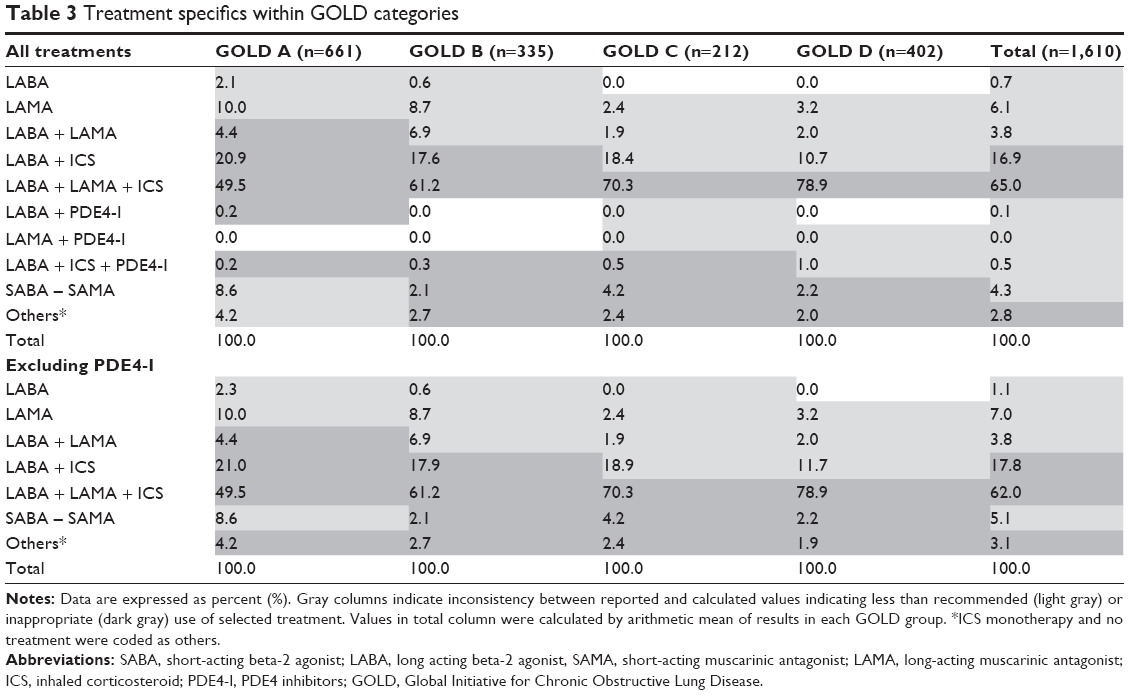 | Table 3 Treatment specifics within GOLD categories |
Risk and symptom determinations by GOLD categories symptom evaluation was based on mMRC alone in 80.1% of patients, CAT alone in 1.3%, and both methods in 18.6% of patients. Both methods (n=299) showed high consistency in classifying the patients according to symptom severity (Kappa coefficient =0.993, P<0.0001) (Table 4).
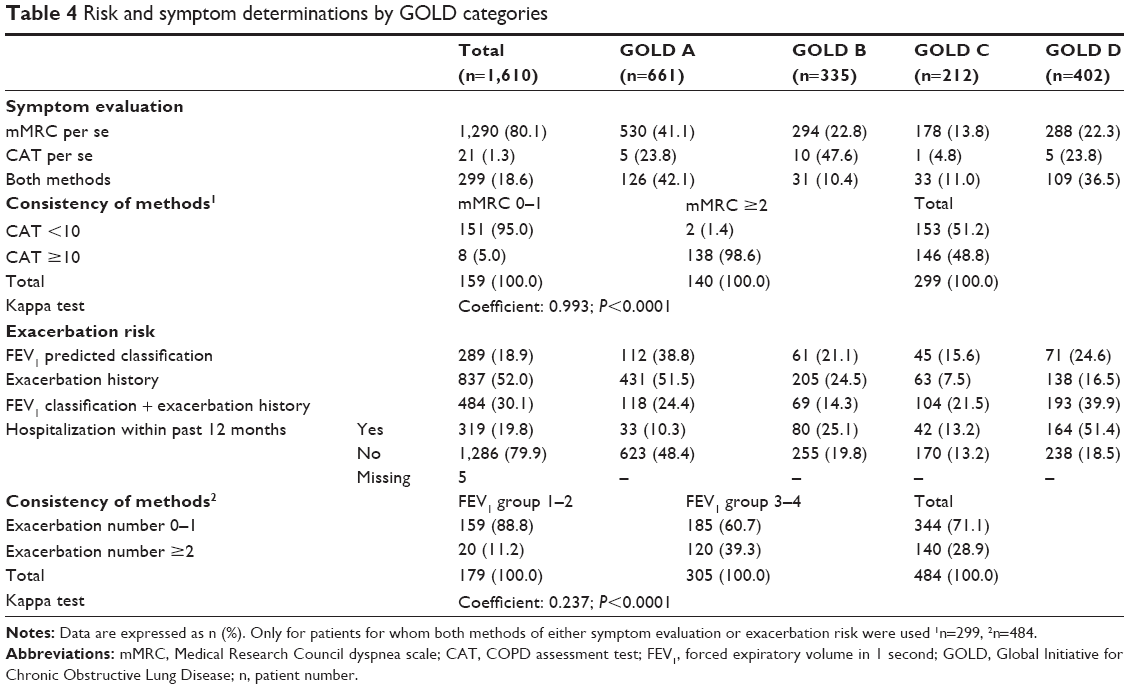 | Table 4 Risk and symptom determinations by GOLD categories |
Exacerbation risk evaluation was based on exacerbation history alone in 52.0% of patients (yielded GOLD A in 51.5% of patients), FEV1 predicted classification alone in 18.9% (yielded GOLD A in 38.8%), while both methods were used in 30.1% of patients (yielded GOLD D in 39.9%), showing low-moderate consistency in classifying patients according to exacerbation risk (Kappa coefficient =0.237, P<0.0001) (Table 4).
At least one former hospitalization due to COPD exacerbation within the past 12 months was noted in 19.8% (n=319) of patients and revealed GOLD D in 51.4% (Table 4).
Consistency between re-classified and reported GOLD categories
When compared with the re-classified categories, GOLD categories were determined to be correctly reported by physicians in 92.1% of patients. Correct reporting was determined to decrease as GOLD category worsens, from 97.1% in GOLD A category to 85.9% in GOLD D category. GOLD D category was reported as a milder category than it should be (14.1%), more commonly than other categories (Table 5).
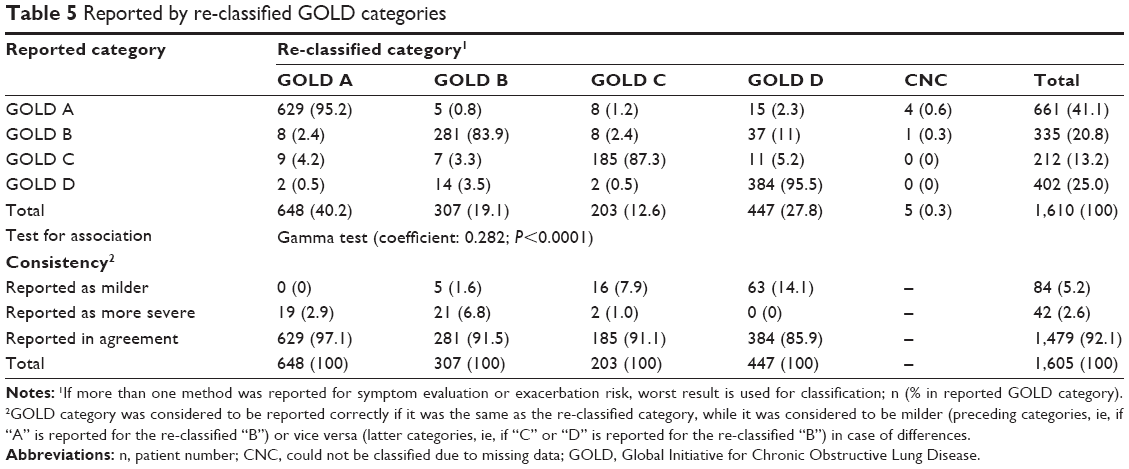 | Table 5 Reported by re-classified GOLD categories |
Among patients whose GOLD category could be re-classified (n=1,605), GOLD A was considered in 40.2%, GOLD B in 19.1%, GOLD C in 12.6%, and GOLD D in 27.8%. Reported by physicians and re-classified GOLD categories showed moderate–weak association (Gamma coefficient =0.282, P<0.0001) (Table 5).
Discussion
The present cross-sectional study revealed that COPD patients were most commonly assigned to GOLD A category (41.1%) according to the combined COPD assessment categories of GOLD 2013 strategy document. LABA + LAMA + ICS regimen was the most commonly (62.0%) selected treatment by physicians, while over-treatment was noted in >70% of patients in GOLD A, B, and C categories. When compared with GOLD A category, the rate of first-line treatment (from 6.1% to 79.4%, respectively) and reporting a milder category than it should be (from 0.0% to 14.1%, respectively) increased in GOLD D category. A decrease in the correct reporting of GOLD category (from 97.1% to 85.9%, respectively) and the rate of over-treatment (from 75.0% to 0.0%, respectively) was noted as the GOLD category worsens. mMRC was used more often (80.1%) than CAT (1.3%) in symptom evaluation, while exacerbation history (52.0%) was used more frequently in comparison with FEV1 predicted classification (18.9%) in evaluation of exacerbation risk in combined COPD assessment.
Data from COPDGene cohort,9 eleven retrospective study cohorts,14 the CHAIN study in Spain,15 and a large database of primary-care patients across the United Kingdom16 indicated assignment of 34% to 38.2% of patients to the GOLD A category. Identification of GOLD A category in 41.1% of our patients seems in line with these findings.
Lowest numbers of patients being assigned to GOLD C category in our cohort seems in agreement with the recently published comparative analysis of four different cohorts by Agusti et al17 indicating GOLD C as the less prevalent category.
Similarly, combined COPD assessment in COPDGene cohort by Han et al9 revealed GOLD C category as the least prevalent category, while GOLD D and A categories were the two most common categories.
Progression of disease has been stated to be associated with higher symptomatic burden and the consequent increase in exacerbation incidence.8 Accordingly, longer duration of disease, higher percentage of ex-smokers, and higher rate for comorbid diseases were evident in “more symptoms” (B and D) than in “less symptoms” (A and C) groups in our cohort.
Comorbidities, cardiovascular diseases in particular, were highly prevalent in all GOLD categories in our cohort. Notably, identification of even higher levels of co-morbidities in “more symptoms” (B and D) than in less symptoms (A and C) groups seems consistent with published data on the presence of comorbidities not only in the most severe disease category (group D) but also in the less severe disease category (group B) in patients with COPD.8,18,19 Also, our findings emphasize the likelihood of consequent alteration in the prognosis of these patients given the impact of comorbidities on the management and survival of patients.18,19
Considering symptom evaluation, mMRC was used in the majority of patients (81.0%) and revealed “less symptoms” consistent with GOLD A category in 41.0% of patients. CAT per se on the other hand, was used in 1.3% of patients, revealed “more symptoms” consistent with GOLD B category in 47.6% of patients. This is in agreement with the reported increase in the number of patients in “more symptomatic” groups (B and D) when CAT was used in conjunction with single or combined risk criteria compared to mMRC.8
Indeed the two methods showed high consistency (Kappa coefficient =0.993, P<0.0001) in our cohort which supports GOLD 2013 strategy recommendation that it is unnecessary to use more than one scale for symptom evaluation.1 However, one must remain prudent when comparing these results, given the likelihood of bias since CAT per se was applied only in a minority of our patients as well as the differences expected in distribution of GOLD categories depending on the specific population studied.17,18
Considering exacerbation risk, use of exacerbation history per se (52.0%) and FEV1 predicted classification (18.9%) per se or both methods (30.1%) revealed different assignment grades in our cohort. Higher prevalence of GOLD A (51.5% vs 38.8%) and lower prevalence of GOLD C (7.5% vs 15.6%) with use of exacerbation history alone was noted compared with use of FEV1 predicted classification alone. Additionally, a higher percentage of patients designated to GOLD D category via combined use of both methods (39.9%) vs either exacerbation history (16.5%) or FEV1% (24.6%) predicted classification alone. Similarly, combined use of exacerbation history and lung function in the evaluation of exacerbation risk was reported to be associated with an increase in the number of patients in high risk groups in COPD patients9 as well as in the general population.19 Consistent with the statement that exacerbation history and FEV1 do not behave identically in predicting risk,9 two methods used for exacerbation risk evaluation in our cohort showed low–moderate consistency (Kappa coefficient =0.237, P<0.0001).
Choice of symptom or risk measure has a substantial modifying impact on grade assignment in combined COPD assessment.9,14,15,20 This has been considered to have implications in the practical application of combined GOLD classification in terms of identification of homogeneous groups of patients, while limiting the symptom and risk assessment to one metric has also been suggested to improve feasibility.9
Despite being recommended as the first-line therapy only in GOLD D category of patients in the GOLD 2013 strategy, LABA + LAMA + ICS regimen was selected in a substantial number of our patients regardless of the category (62.0%). The excessive use of this combination led to over-treatment in a considerable number of patients assigned to GOLD A, B, and C categories (75.0%, 79.1%, and 70.8%, respectively).
Similarly, analysis of data from the Adelphi Respiratory Disease Specific Programme in 3,813 COPD patients by Vestbo et al8 revealed that the highest proportion of patients receiving ICS was in group D, while a considerable proportion of patients in low risk groups (A and B) were receiving ICS + LABA.
Also, data from a study by Han et al9 revealed that not only exacerbation risk but also rate of ICS + LABA and LAMA treatment was higher in patients assigned to GOLD D category when evaluation was based on both lung function and exacerbation history than on lung function or exacerbation history solely. Our findings also support that clinicians are already more aggressive in treating this category of patients.9 Moderate–weak consistency (Gamma coefficient =0.282, P<0.0001) was noted between re-classified and reported rates for GOLD categories in the present study. Accordingly, reporting a category “better than it should be” was determined to be more common among physicians as the category worsens, leading to 14.1% of GOLD D category patients in our cohort to be categorized inappropriately as A, B, or C categories.
In this regard our findings support the demonstrated conflict between the current real-life practice and the GOLD treatment recommendations in terms of low referral to COPD management guidelines by physicians, proving that adherence to the GOLD treatment strategy is far from optimal.8,21–23
Certain limitations of this study should be considered. Implementation of CAT and mMRC assessments by the same physician seems to be the major limitation which may account for the two methods revealing almost identical findings. There may be a bias risk regarding center selection despite all efforts, but since no previous similar studies were available, it was impossible to validate the results using an external reference at the time of this report. Participating physicians were expected to enroll all eligible patients during the enrollment period; therefore patient selection bias risk was negligible. However, sample size of the study is rather high and study centers were selected to represent hospital models in Turkey allowing assessment of geographical variability and thereby enabling the results of the study to be projected to the overall patient population in Turkey. Despite these limitations, given the paucity of the solid information available on this area, our findings represent a valuable contribution to the literature.
Conclusion
Providing data on distribution of combined COPD assessment categories based on GOLD 2013 strategy for the first time in the literature, our findings revealed GOLD A and GOLD C as the most and the least prevalent categories in Turkish cohort of COPD patients, respectively. Non-adherence to treatment recommendations was noted with pronounced selection of LABA + LAMA + ICS regimen regardless of GOLD category by physicians, and the consequent high rates of over-treatment. Our findings seem to indicate that choice of symptom or risk measure can substantially alter group assignment. Since this is the first study with a primary objective of determining the distribution of combined COPD assessment categories described in GOLD 2013 strategy document among COPD patients, our results should be supported by further studies.
Acknowledgments
The study is funded by Novartis Pharmaceuticals Turkey. We thank Cagla Ayhan, MD and Prof Sule Oktay, MD, PhD from KAPPA Consultancy Training Research Ltd, Istanbul who provided editorial support and Mehmet Berktas, MD, MICR from KAPPA Consultancy Training Research Ltd, Istanbul who performed statistical analysis funded by Novartis Pharmaceuticals Turkey.
Disclosure
AK and IA are Novartis Pharmaceuticals Turkey employees. The authors report no other conflicts of interest in this work.
References
Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. | ||
Kocabas A, Hancioglu A, Turkyilmaz S, et al. Prevalence of COPD in Adana, Turkey (BOLD-Turkey Study). Proc Am Thorac Soc. 2006;3(suppl):A543. | ||
Gunen H, Hacievliyagil SS, Yetkin O, Gulbas G, Mutlu LC, Pehlivan E. Prevalence of COPD: First epidemiological study of a large region in Turkey. Eur J Intern Med. 2008;19(7):499–504. | ||
Deveci F, Deveci SE, Turkoglu S, et al. The prevalence of chronic obstructive pulmonary disease in Elazig, Eastern Turkey. Eur J Intern Med. 2011;22(2):172–176. | ||
Ministry of Health Turkey, Institute of Public Health [homepage on the Internet]. Chronic diseases and risk factors survey in Turkey; 2013. Available from: http://sbu.saglik.gov.tr/Ekutuphane/kitaplar/khrfai.pdf. Accessed August 8, 2014. | ||
Schlecht NF, Schwartzman K, Bourbeau J. Dyspnea as clinical indicator in patients with chronic obstructive pulmonary disease. Chron Respir Dis. 2005;2(4):183–191. | ||
Vestbo J, Hurd SS, Rodriguez-Roisin R. The 2011 revision of the global strategy for the diagnosis, management and prevention of COPD (GOLD)-why and what? Clin Respir J. 2012;6(4):208–214. | ||
Vestbo J, Vogelmeier C, Small M, Higgins V. Understanding the GOLD 2011 Strategy as applied to a real-world COPD population. Respir Med. 2014;108(5):729–736. | ||
Han MK, Mullerova H, Curran-Everett D, et al. GOLD 2011 disease severity classification in COPDGene: a prospective cohort study. Lancet Respir Med. 2013;1(1):43–50. | ||
Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. | ||
Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline LN. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. | ||
Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. | ||
Newcombe RG. Two-sided confidence intervals for the single proportion: comparison of seven methods. Stat Med. 1998;17(8):857–872. | ||
Soriano JB, Alfageme I, Almagro P, et al. Distribution and prognostic validity of the new Global Initiative for Chronic Obstructive Lung Disease grading classification. Chest. 2013;143(3):694–702. | ||
Casanova C, Marin JM, Martinez-Gonzalez C, et al. New GOLD classification: longitudinal data on group assignment. Respir Res. 2014;15:3. | ||
Haughney J, Gruffydd-Jones K, Roberts J, Lee AJ, Hardwell A, McGarvey L. The distribution of COPD in UK general practice using the new GOLD classification. Eur Respir J. 2014;43(4):993–1002. | ||
Agusti A, Hurd S, Jones P, et al. FAQs about the GOLD 2011 assessment proposal of COPD: a comparative analysis of four different cohorts. Eur Respir J. 2013;42(5):1391–1401. | ||
Jones PW, Nadeau G, Small M, Adamek L. Characteristics of a COPD population categorised using the GOLD framework by health status and exacerbations. Respir Med. 2014;108(1):129–135. | ||
Lange P, Marott JL, Vestbo J, et al. Prediction of the clinical course of chronic obstructive pulmonary disease, using the new GOLD classification: a study of the general population. Am J Respir Crit Care Med. 2012;186(10):975–981. | ||
Nishimura K, Oga T, Tsukino M, Hajiro T, Ikeda A, Jones PW. Reanalysis of the Japanese experience using the combined COPD assessment of the 2011 GOLD classification. Respir Investig. 2014;52(2):129–135. | ||
Jochmann A, Neubauer F, Miedinger D, Schafroth S, Tamm M, Leuppi JD. General practitioner’s adherence to the COPD GOLD guidelines: baseline data of the Swiss COPD Cohort Study. Swiss Med Wkly. Epub 2010 Apr 21. | ||
Seaman J, Leonard AC, Panos RJ. Health care utilization history, GOLD guidelines, and respiratory medication prescriptions in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2010;5:89–97. | ||
Fitch K, Iwasaki K, Pyenson B, Plauschinat C, Zhang J. Variation in adherence with Global Initiative for Chronic Obstructive Lung Disease (GOLD) drug therapy guidelines: a retrospective actuarial claims data analysis. Curr Med Res Opin. 2011;27(7):1425–1429. |
Supplementary material
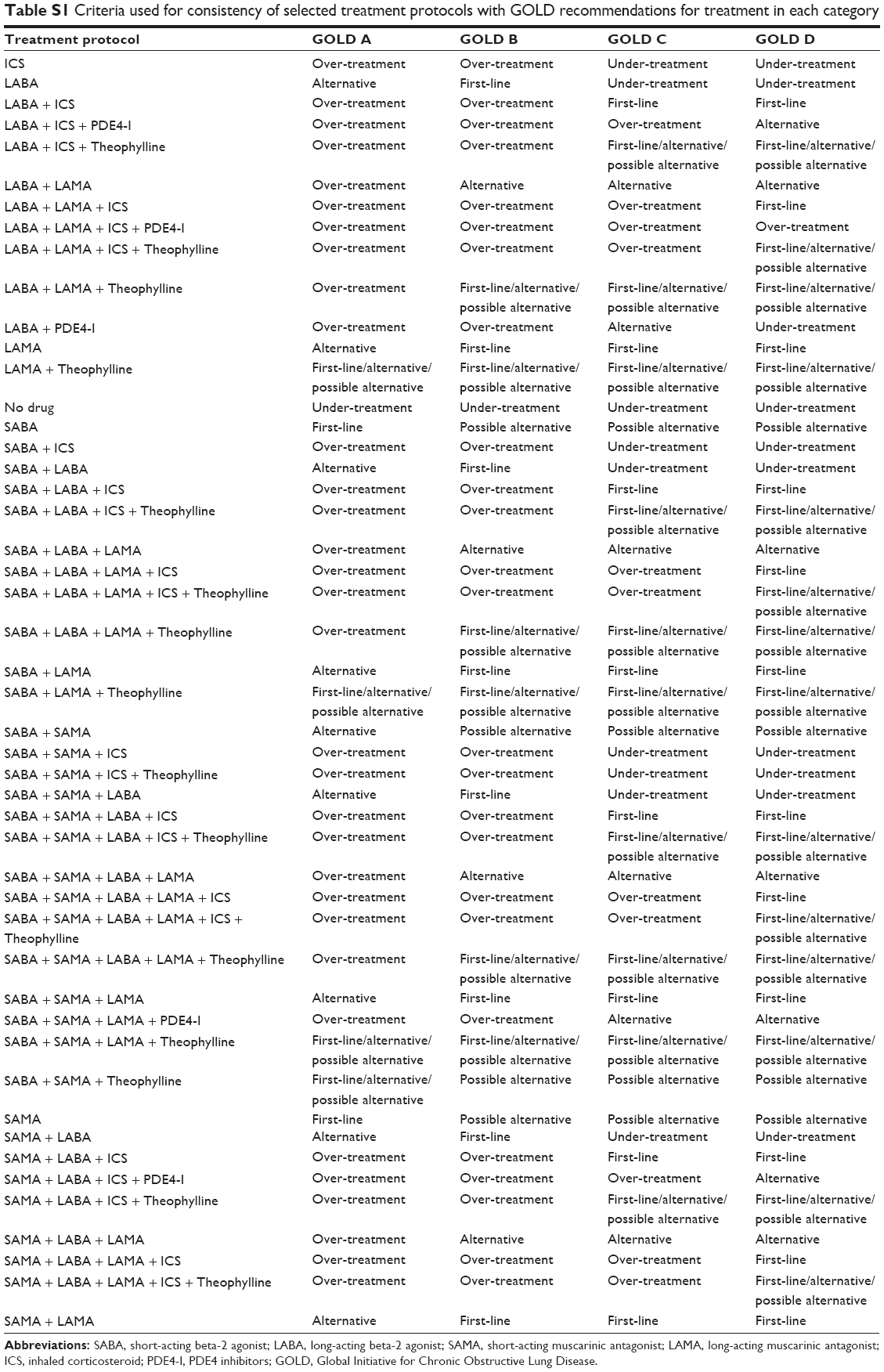 | Table S1 Criteria used for consistency of selected treatment protocols with GOLD recommendations for treatment in each category |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.