Back to Journals » Cancer Management and Research » Volume 10
Castleman’s disease in the HIV-endemic setting
Authors Mahroug E, Sher-Locketz C, Desmirean M, Abayomi EA, Tomuleasa C, Grewal R
Received 29 May 2018
Accepted for publication 31 July 2018
Published 12 October 2018 Volume 2018:10 Pages 4553—4563
DOI https://doi.org/10.2147/CMAR.S175648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Antonella D'Anneo
This paper has been retracted.
Esam-Rajab Mahroug, 1 Candice Sher-Locketz, 1 Minodora-Silvia Desmirean, 2,3 Emmanuel-Akinola Abayomi, 1,4 Ciprian Tomuleasa, 3,5,6 Ravnit Grewal 1,7
1Division of Haematology, Department of Pathology, University of Stellenbosch, Tygerberg Academic Hospital, Cape Town, South Africa; 2Department of Pathology, Military Hospital of Cluj Napoca, Cluj Napoca, Romania; 3Department of Hematology, Iuliu Hatieganu University of Medicine and Pharmacy, Cluj Napoca, Romania; 4Department of Hematology, Nigeria Institute for Medical Research, Lagos, Nigeria; 5Research Center for Functional Genomics and Translational Medicine, Iuliu Hatieganu University of Medicine and Pharmacy, Cluj Napoca, Romania; 6Department of Hematology, Ion Chiricuta Clinical Research Center, Cluj Napoca, Romania; 7Department of Pathology, South African Bioinformatics Institute, University of The Western Cape, Bellville, South Africa
Introduction: Castleman’s disease (CD), first described by Benjamin Castleman in 1954, is a giant or angiofollicular lymph node hyperplasia, described as a rare monotypic polyclonal B-cell lymphoproliferative disorder with an incompletely understood pathogenesis and variable clinical behavior. This study aimed to determine the incidence of CD diagnosis over an 11-year period. Additionally, the study aimed to describe the demographic, laboratory, and pathological features of CD.
Methods: This is a retrospective study where the demographic and laboratory data were retrieved from the Tygerberg Academic Hospital (TAH) patient electronic records and Tygerberg Lymphoma Study Group (TLSG) and statistical analysis performed on the patients diagnosed with CD.
Results: Fifty-four patients were diagnosed with CD during this period. The median age at presentation was 39 years (range: 9– 58). HIV serology was available in 53 patients, of which 51 were HIV-positive and two were HIV-negative. The history of initiation of antiretroviral therapy at diagnosis was available in 43 patients (38 on treatment, four were not on treatment, and one defaulted treatment). The median CD4 count was 232.50 cells/μL (range: 2– 883). The HIV viral load was performed in 43 patients at diagnosis, which was < 49 HIV-1 RNA copies/μL in more than half of the patients (58%). Diagnosis was made on lymph node biopsies in 53 patients, with one case diagnosed on a spleen biopsy. Kaposi sarcoma was found on the same tissue biopsy in 13 cases. A bone marrow biopsy was performed in 31 patients. The predominant features noted were a disorganized hypercellular marrow with plasmocytosis.
Conclusion: CD is a rare polyclonal B-cell lymphoproliferative disorder. However, we demonstrated a significant increase in the incidence of HIV-associated multicentric CD over the last decade in our area in South Africa.
Keywords: Castleman’s disease, HIV-endemic setting, HHV-8 status, CD4 count, clinicopathological correlation
Introduction
Castleman’s disease (CD), also known as giant or angiofollicular lymph node hyperplasia, is a rare monotypic polyclonal B-cell lymphoproliferative disorder with an incompletely understood pathogenesis and variable clinical behavior. The disease likely encompasses several clinical and pathological entities with overlapping features. It was first described in 1954 by Benjamin Castleman, a pathologist who reported a patient presented with fever and weakness with mediastinal lymphadenopathy.1 The histological features were so distinctive that they were later characterized as the typical hyaline vascular variant of CD.1 In 1972, several cases with novel histologic characteristics were diagnosed and called plasma cell variant.2 CD has been classified clinically according to the extent of lymphadenopathy into unicentric Castleman’s disease (UCD) and multicentric Castleman’s disease (MCD). UCD cases mostly show hyaline vascular variant histology, while the plasma cell variant is less commonly encountered. The majority of the MCD cases have plasma cell variant histology especially in the setting of HIV infection.3,4 The rarity of the disease and its clinical–pathological heterogeneity have precluded comprehensive studies to be conducted, and the current knowledge is based mainly on retrospective case series studies and histological reviews. MCD is a rare disease with an increasing prevalence on HIV-infected individuals. South Africa has the largest HIV epidemic in the world, with an estimated 7 million people living with HIV in 2015, hence the rationale for studying the incidence of this disease in this setting.5–7 To the best of our knowledge, there are very limited data from South Africa and the African continent regarding the epidemiology of CD. We conducted a thorough literature search for similar studies in South Africa and the African content. The only study that we found is a descriptive retrospective study conducted at Chris Hani Baragwanath Academic Hospital (CHBAH), Johannesburg, South Africa, over a 25-year period (1990–2014).8 On the African landscape, however, only isolated case reports have been published. Thus, we anticipate that this study will shed some light on the epidemiology of CD in the HIV-endemic setting and may direct the way in how we approach the diagnosis and staging using bone marrow biopsy of this condition. CD comprises different subtypes, with different prognoses. Both unicentric and multicentric have specific systemic manifestations and could be associated with Kaposi sarcoma (KS), Hodgkin’s or non-Hodgkin’s lymphomas, as well as POEMS syndrome. The cause and pathogenesis of CD can be split into three main subtypes namely UCD, idiopathic MCD, and human herpesvirus-8-associated MCD (HHV8+ MCD). In our case series, we focus on HHV8+ MCD.
The main aim of the study is to bring a new highlight in the landscape of viral infections and CD. It assesses the incidence of CD diagnosed at Tygerberg Academic Hospital (TAH) over an 11-year period. Additionally, the study aims to describe the demographic, laboratory, and pathological features of CD cases diagnosed at TAH during the same period. The objectives of the research were to correlate various histological variants of CD in relation to the HIV status and document the human herpesvirus-8 (HHV8) (latency-associated nuclear antigen [LANA]) immunohistochemistry (IHC) result on the tissue biopsy. Secondary objectives were to determine the frequency of codiagnosis of KS in relation to the CD4 count of the patient, as well as to document the marrow involvement and bone marrow histological and IHC features of CD in order to highlight how bone marrow assessment in such cases should be made.
Methods
Study population
This study is a retrospective observational study, which is part of a larger study under the Tygerberg Lymphoma Study Group (TLSG) at Tygerberg Hospital that was started in 2007 and its ethical approval number is HREC No: N07/03/068. Thus, it is a retrospective descriptive study of CD cases diagnosed in the Division of Anatomical Pathology and Division of Haematopathology, Department of Pathology, National Health Laboratory Service (NHLS), TAH during the period January 2007 to December 2017. Data for the study were extracted from Tygerberg Hospital patient electronic records of investigations through Disa laboratory (Disalab version 04.16.04.373) and TrakCare IT systems using the key word “Castleman disease.” The database of the TLSG was also used for CD data collection. The data obtained were carefully reviewed to avoid duplication and to apply the inclusion and exclusion criteria. All data were collected on Microsoft Excel® spread sheet and submitted for analysis to the statistician.
Inclusion and exclusion criteria
All patients newly diagnosed with CD by tissue biopsy and confirmed by IHC stains in the Division of Anatomical Pathology, NHLS - Tygerberg Hospital as well as the Division of Hematology were included. The exclusion criteria refer to all patients diagnosed with relapsed CD, as well to all patients who had a lymph node histological feature suggestive of CD, but not confirmed by IHC.
Data analysis
Categorical data were described using charts and expressed in proportions and percentages. The continuous data were described using mean and SD if normally distributed; however, median and range were used to describe continuous data if the distribution is skewed. The chi-squared test was used to compare categorical variables between the groups while independent t-test used for normally distributed continuous variable and Mann–Whitney test for continuous variables with skewed distribution, as previously described.9–12
Results
Demographics
Data were obtained from 54 patients who were diagnosed with CD on tissue biopsy from January 2007 to December 2017 in the Department of Anatomical Pathology, National Health Laboratory Service-TAH. Out of the 54 cases diagnosed with CD, there were two (3.7%) HIV-negative cases, 51 (94.4%) HIV-positive cases, and in a single case the HIV status was unknown. There was an increasing trend in the number of HIV-associated MCD with a peak of 13 cases diagnosed in 2015, the number of cases declined slightly in 2016 to nine cases, however in general cases have steadily increased since 2007. The mean age at diagnosis was 38.15 years, the age range was 9–58 years, and median age was 39 years. Only one patient was diagnosed with CD in the first decade of life. There were six (11.1%) cases that were diagnosed in the third decade of life (20–29 years), 20 (37%) cases in the fourth decade of life (30–39 years), 21 (38.9%) cases in the fifth decade of life (40–49 years), and six (11.1%) cases in the sixth decade of life (50–59 years). There were 27 (50%) male patients and 27 (50%) female patients. Our findings showed an equal male to female ratio (Figures S1–S5).
CD4 count and HIV viral load (VL)
In our cohort, 51 (94.4%) patients were HIV-positive, only two (3.7%) patients were HIV-negative, and in one patient the HIV status was unknown (1.9%). Out of the 51 HIV-positive patients, 38 (74.5%) patients were on antiretroviral therapy (ART) at the time of diagnosis, four (7.9%) patients were not on treatment, one (1.9%) patient defaulted treatment, and in eight (15.7%) patients the treatment history was unknown. The treatment history of the patients was obtained from the histological reports.
Forty-eight (94.1%) of the HIV-positive patients had their CD4 counts performed at the time of diagnosis and in three (5.9%) of the HIV-positive patients the CD4 count was unknown. The median CD4 count was 232.50 cell/μL (range: 2–883 cells/μL). In 42% of the patients, the CD4 count was <200 cells/μL, while in 29% of the patients the CD4 counts were between 200 and 350 cells/μL. The CD4 counts ranged between 351 and 500 cells/μL in 14% of the patients and >500 cells/μL in 15% of the patients at the onset of diagnosis (Figure 1).
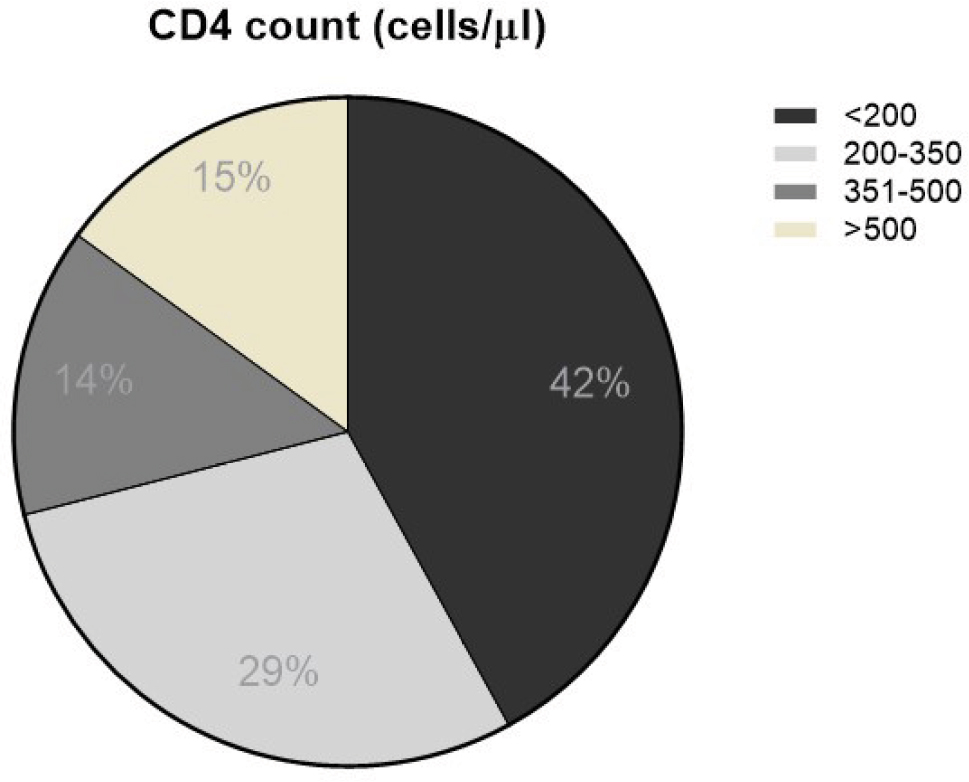 | Figure 1 CD4 counts of the patients included in the study. |
HIV VLs showed significant variability between patients; however, many patients had very low or undetectable VLs. Forty-three of the HIV-positive patients had their VLs measured around the time of diagnosis of CD. More than half of the patients (58%) had VL <49 RNA copies/μL. Only one patient (2%) had a VL between 50 and 99 RNA copies/μL. The VL was between 100 and 1,000 RNA copies/μL in five patients (12%) and 12 (28%) patients had a VL >1,000 RNA copies/μL. Out of the 12 patients with a VL >1,000 RNA copies/μL, four patients were on ART, one not on ART, one defaulted ART, and in six patients the ART history was unknown (Figure 2).
 | Figure 2 Viral load of the patients included in the study. Abbreviations: HHV, human herpesvirus; IHC, immunohistochemistry. |
Histology of CD
The diagnosis of CD was made on a lymph node biopsy in total n=53 (98.1%) patients, with only one patient (1.8%) being diagnosed on splenic tissue. The diagnosis of CD on tissue biopsies was made by two independent anatomical pathologists. Histological variants were reported in 37 (37/54) (68.5%) patients diagnosed with CD. The hyaline vascular variant was reported in the two HIV-negative patients. In HIV-associated MCD, plasma cell variant was the most common variant reported in 20/35 (57%) patients followed by mixed variant (23%). The hyaline vascular variant was reported in 17% of the cases and only one (3%) case was reported as plasmablastic variant (Figure 3). A characteristic histological finding is that the plasmablasts are all IgM lambda but polyclonal.
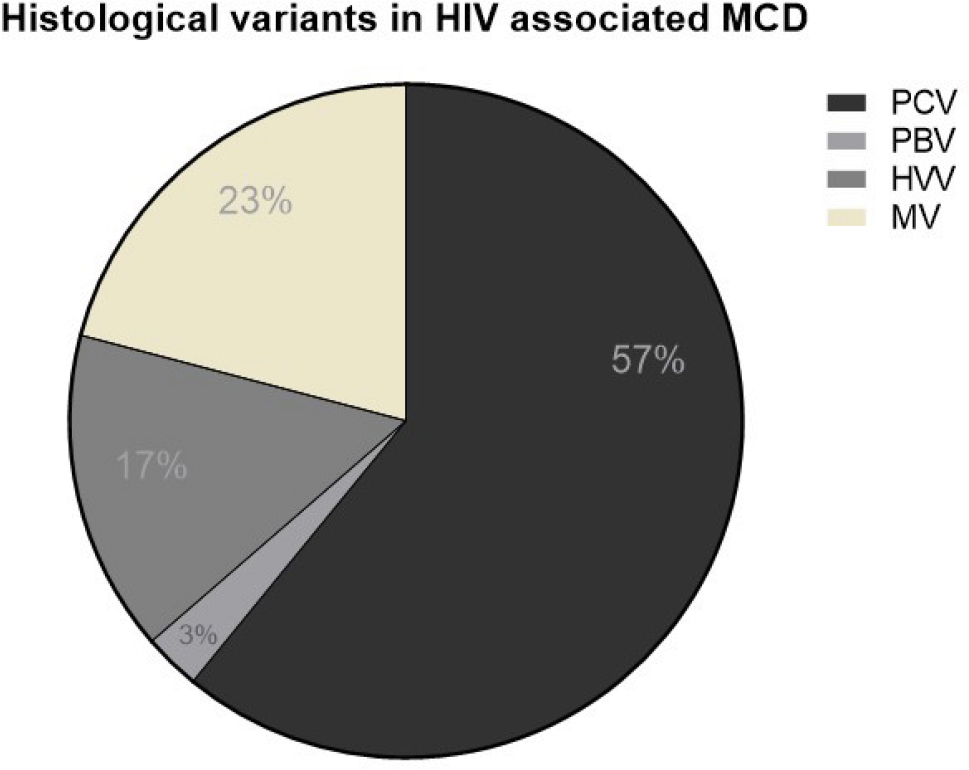 | Figure 3 Histological subtypes of the patients included in the study. Abbreviations: MCD, multicentric Castleman’s disease; PCV, plasma cell variant; PBV, Patent blue V; HVV, hyaline vasculare variant; MV, multicentric varian. |
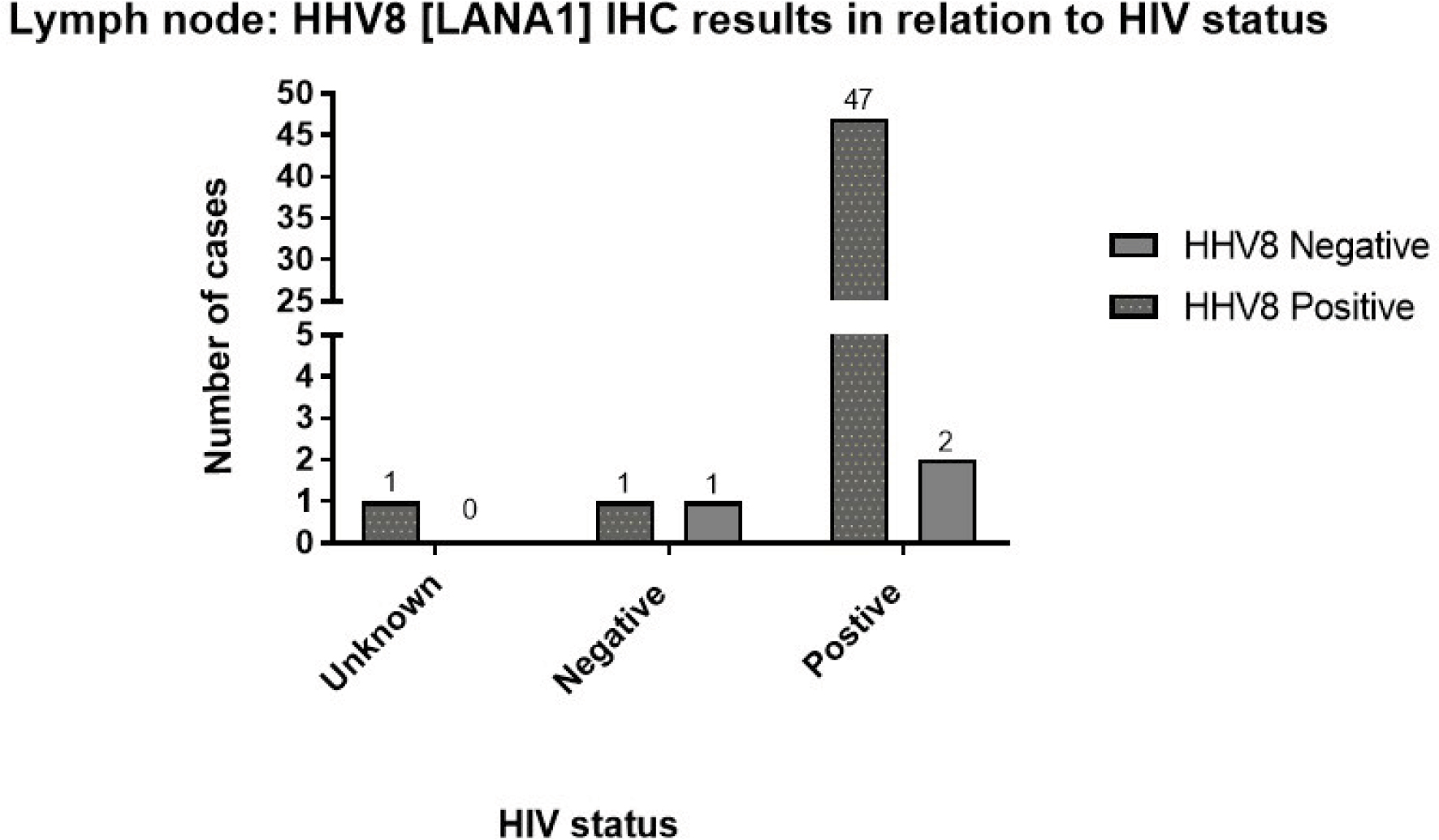
The coexistence of KS was seen in 13 (24.1%) cases, and all the cases were HIV-positive. When compared with the group of patients with only CD on tissue biopsy (41/54), the cohort of patients with coexisting KS (13/54) was associated with a younger median age at presentation (33.31 vs 39.68 years, P=0.036), lower median platelet count (57 vs 199.5×109/L, P=0.006), and CD4 count <200 cells/μL (66.7% vs 33.3%, P=0.042) (Tables 1 and 2). HHV8 (LANA-1) IHC stain was requested in 52 of the cases and it was positive in 49 (94.2%) of the cases, while it was negative in three (5.8%) of the cases. In the 49 cases with HHV8 infection, 47 cases were HIV-positive, one patient was HIV-negative, and in a single case the HIV status was unknown. In the three cases where HHV8 was negative, one was HIV-negative and two were HIV-positive cases (Figure 4).
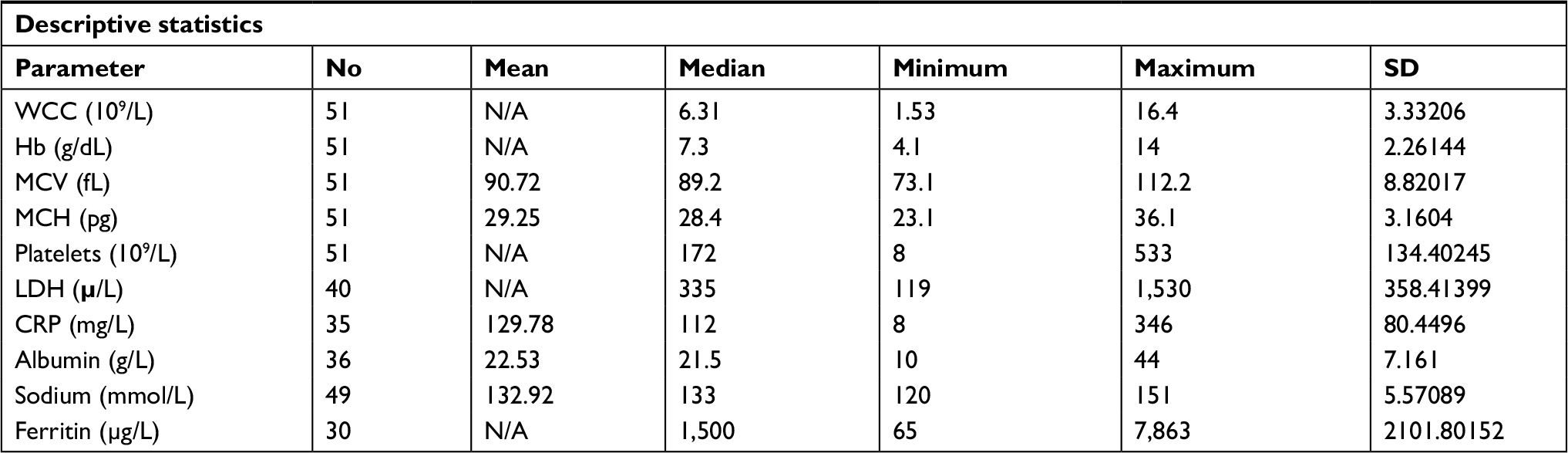 | Table 1 Laboratory data at the time of diagnosis of CD (or the earliest available after diagnosis) Abbreviations: CD, Castleman disease; CRP, C reactive protein; LDH, lactate dehydrogenase; MCH, mean corpuscular hemoglobin; MCV, mean corpuscular volume; WCC, white cell count; N/A, not available. |
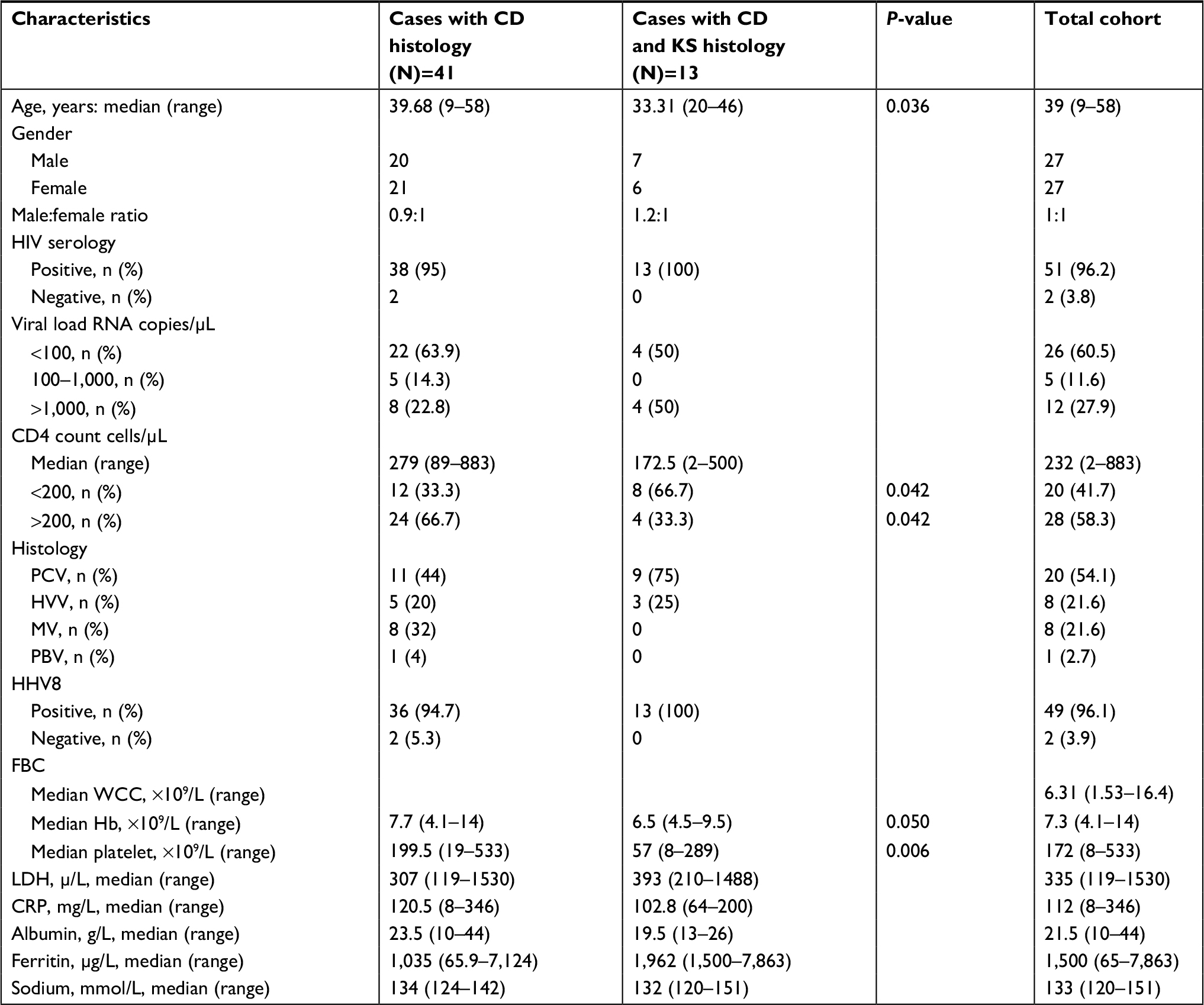 | Table 2 Comparison of patients with coexistence KS on same tissue with CD patients Abbreviations: CD, Castleman disease; KS, Kaposi sarcoma; HHV, human herpesvirus; CRP, C reactive protein; FBC, full blood count; LDH, lactate dehydrogenase; MV, mean value; HVV, hyaline vascular variant; PBV, plasma cell variant; WCC, white cell count. |
 | Figure 4 HHV8 status of the patients included in the study. Abbreviation: HHV, human herpesvirus. |
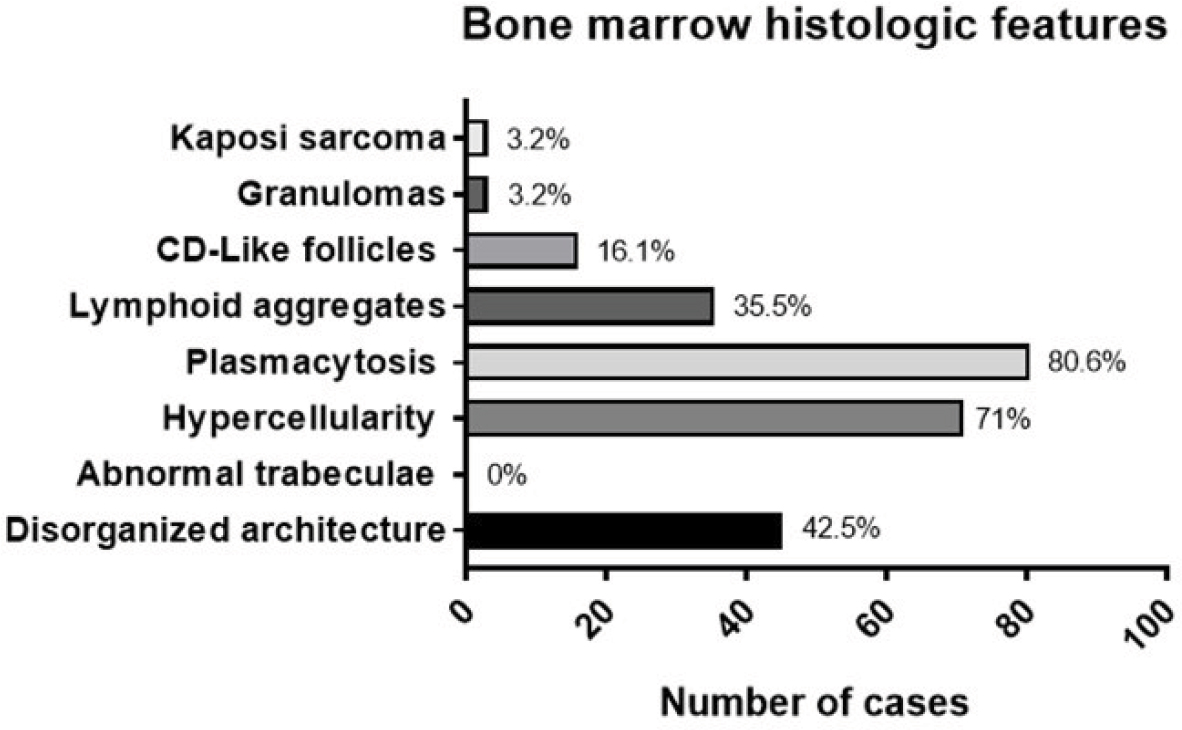
Bone marrow biopsy of CD
Thirty-one (31/54) patients diagnosed with CD had bone marrow biopsy procedures performed at the time of diagnosis. Plasmocytosis was found in 25/31 (80.6%) patients who underwent bone marrow biopsies, hypercellularity was found in 22/31 (71%), and the bone marrow architecture was disorganized in 14/31 (45.2%) of the cases. Lymphoid aggregates were detected in 11/31 (35.5%) of the cases. CD-like follicles were detected in 5/31 (16.1%) of the cases and granulomas were detected in only one case. Histologic features suggestive of bone marrow infiltration by KS were reported in one case. HHV8 (LANA-1) IHC stain was requested in only 10 cases and was found to be positive in 2/10 (20%) cases, while it was negative in the rest of the cases.
Discussion
Our article describes 54 patients newly diagnosed with CD over an 11-year period from January 2007 to December 2017. Almost all the diagnoses were made on lymph node biopsies with one exception of a case diagnosed on a splenectomy specimen. An increasing trend of incidence of diagnosis of CD in an HIV-endemic setting was reported by Abayomi et al, who had published preliminary findings of the TLSG where they reported only four cases of CD over 8 years (2002–2009).5 In comparison, the presently described data show a significant increase in the incidence of diagnoses of CD in an HIV-endemic setting, with 50 cases diagnosed over the subsequent 7 years (2010–2017). A retrospective study conducted at Chris Hani Baragwanath Academic Hospital (CHBAH) in Johannesburg, South Africa, over a 25-year period (1990–2014) identified 38 patients diagnosed with CD. It was reported that 57.9% of MCD cases were diagnosed in the last 5 years of the study.13 This study together with our findings shows an increase in the incidence of diagnosis of MCD in the HIV-endemic setting of South Africa in the last decade. Even if we did not include clinical features in our study to confidently classify our cases into UCD and MCD, HIV infection has been associated with MCD (71.4%) vs UCD (1.7%), according to a large single institution retrospective study.14 In our study, 94.4% of the patients were HIV seropositive. We think there are multiple possible causes behind this significant and steady increase in the incidence of diagnosing HHV8-associated MCD in HIV-positive patients at our center. First, there has been an increase in the prevalence of HIV in South Africa from 10.6% in 2008 to 18.2% in 2014. Second, South Africa launched its ATR program in 2004 with an increasing ART HIV population coverage each year.15–17 This might have resulted in improved survival and decreased death rates in HIV people from other causes like opportunistic infections. Third, emigration of people from other provinces and the continent of Africa to the Western Cape might contribute to the trend of increasing incidence of this rare disease.
The overall median age at diagnosis in our cohort was 39 years with a mean of 38.1 years (range: 9–58 years) and a male to female ratio of 1:1. These findings are similar to those found in the study conducted at CHBAH, where the median age was 36 years and mean was 37 years at the time of diagnosis with a male to female ratio of 1.2:1. The median age at presentation of HIV-associated MCD in South Africa appears to be compatible with the high prevalence of HIV infection among the 30- to 40-year age group, and it is slightly lower in contrast to retrospective studies from France, UK, or Australia (median: 41.4, 42, and 43 years), respectively.15,18,19 A male predominance was observed in the largest single institution case series to date and in one systematic review, whereas in our series the incidence was equal in men and women.20,21
In our case series, most patients diagnosed with CD were HIV-positive, ie, 51/54 (94.4%), two patients (3.7%) were HIV-negative and in one patient the HIV status was unknown. This finding correlates with the literature and is what we expected due to the high HIV infection prevalence in South Africa. There were 38 (74.5%) patients on ART at the time of diagnosis. However, the duration of treatment was unfortunately unknown. The median CD4 count at presentation was 232.5 cells/μL (range: 2–883 cells/μL) with most of the patients (71%) with a CD4 count <350 cells/μL. The VL was undetectable (<20 or <40 HIV-1 RNA copies/μL according to the assay used) in 58% of patients who had their VL measured around the time of diagnosis. The median CD4 count was comparable with other studies (the range median CD4 count: 174–275 cells/μL). The percentage of patients with an undetectable VL at diagnosis (58%) was higher than other studies conducted in France, UK, or Australia. In these countries, studies reported undetectable HIV-1 RNA in 26%, 44%, and 45.5% of the patients on ARTs, respectively.18,19 However, the limits of detection of HIV-1 RNA and the way of reporting the results were different among the studies. Our study showed that most of the patients with CD had a CD4 count <350 cells/μL. Still, the range of the CD4 count was significantly wide (2–883 cells/μL). Furthermore, we can conclude from our results that the suppression of the HIV VL below detectable limits does not prevent the development of MCD. On the contrary, it may contribute to an increased incidence of HIV-associated MCD.
The pathology reports for the diagnosis of CD were made on lymph node tissues in 53 patients, whereas in one patient the diagnosis was made on a splenic biopsy. The histological variant was not reported in 31.5% of the cases. In HIV-associated MCD, PCV was the most frequently reported variant (57%), whereas MV was reported in 23% of the cases, HVV in 17%, and plasmablastic variant in 3% of the patients. PCV and MV constitute 80% of the variants reported in HIV-associated MCD. The coexistence of KS was reported in 24.1% of the cases. When compared with the group of cases with only CD histology, we report that the coexistence of KS is associated with a younger age at presentation, lower platelet counts, and a CD4 count of <200 cells/μL. These findings were expected as KS is an AIDS-defining illness. In our study, HHV8 (LANA-1) IHC stain was requested and reported in all cases except two cases diagnosed with CD in 2010. This staining was positive in scattered plasmablasts in mantle zones in 49/52 (94.2%) of the tissues examined (HHV8-associated CD) and was negative in 3/52 (5.8%) cases. In one case, HHV8 IHC stain was positive in scattered cells and there was a focal collection of HHV8-positive plasmablastic cells almost forming a sheet, with no light chain restriction. The EBER-ISH was positive in scattered cells with the histologic features of CD observed on H&E. These findings were interpreted as plasmablastic variant of MCD. Thirty-one patients who were diagnosed with CD had bone marrow biopsy procedures performed (30 HIV-positive and one HIV-negative). The bone marrow biopsy indications were to investigate causes of cytopenia(s) and to exclude marrow infiltration by infections or malignancies. We reviewed all the 31 bone marrow biopsy reports and found that an increase in plasma cells in the bone marrow biopsies as well as bone marrow hypercellularity was the most prominent feature. Plasmocytosis was found in 80.6% of the bone marrow biopsies. The plasma cell percentages in the bone marrow were variable with range from 6% to 70% of nucleated cells and commonly had an interstitial or perivascular distribution and rarely a diffuse distribution. The plasma cells were polytypic in all cases.
CD-like follicles were detected in 5/31 (16.1%) of the cases. Two cases showed typical CD-like follicles with germinal center and mantle zones consisting of small lymphocytes arranged in concentric layers. The other three cases showed large lymphoid aggregates with vague concentric layers of lymphocytes and increased vascularity suggestive of CD infiltration of the bone marrow.
HHV8 (LANA-1) IHC stain was requested in 10 cases where five bone marrow biopsies had CD-like follicles, while the other five cases were without CD-like follicles. We found that HHV8 was detected in 2/10 (20%) cases with CD-like follicles. In our series, the rate of requesting HHV8 IHC and detection of HHV8-positive mononuclear cells were lower than what has been reported in other studies, which showed higher rate of detecting HHV8-positive mononuclear cells in the bone marrow (50%–80%) of the cases (38, 40). This indicates the need to request HHV8 on all patients with suspected CD even if the typical features are not noted. In this series, we detected CD-like follicles in 5/31 (16.1%) of the bone marrow biopsies, which is comparable with the study published by Bacon et al that found CD-like follicles in 3/13 (23.1%) of the cases.22–24
Conclusion
CD is a rare condition. However, in the setting with an increasing prevalence of HIV infection, as is the case of South Africa, we report a parallel and significant increase in the incidence of HIV-associated MCD in the last decade. This change is likely due to the continuous change in ART therapy protocols in South Africa since 2004 when ART was made available in the public hospitals. This means that we are now going to see more CD cases and therefore need to create more awareness about this disease in our setting. Finally, our findings also highlight the need for HIV-related cancer registries in South Africa and Africa as a whole.
Acknowledgments
We thank National Health Laboratory Service (NHLS) and Tygerberg Lymphoma Study Group (TLSG) for using their database. We thank W Kleynhans from IT Department for his help in data capturing and Innocent Karangwa from Biostatistics department for his help in the statistical analysis. We acknowledge Stellenbosch University (SU) and Human Research Ethics Department. We acknowledge Cancer Association of South Africa (CANSA). This is a substudy of the larger TLSG, which was approved by the Human Research Ethical Committee (HREC) of the SU. Approval no: S17/10/194. The research was carried out in accordance with all legal and ethical laws, respecting the legislation of both the Republic of South Africa and the European Union. The data are deidentified and does not require patient consent. No potential conflict of interest is reported. CT was supported from Romanian Government research grants awarded to (FDI 2018-0071), as well as by a National Research Grant awarded for Frontiers Research Projects (PCCF 2018-2022).
Disclosure
The authors report no conflicts of interest in this work.
References
Castleman B, Towne VW. Case records of the Massachusetts General Hospital: Case No. 40231. N Engl J Med. 1954;250(23):1001–1005. | ||
Keller AR, Hochholzer L, Castleman B. Hyaline-vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locations. Cancer. 1972;29(3):670–683. | ||
Dispenzieri A, Armitage JO, Loe MJ, et al. The clinical spectrum of Castleman’s disease. Am J Hematol. 2012;87(11):997–1002. | ||
Ye B, Gao SG, Li W, et al. A retrospective study of unicentric and multicentric Castleman’s disease: a report of 52 patients. Med Oncol. 2010;27(4):1171–1178. | ||
Abayomi EA, Somers A, Grewal R, et al. Impact of the HIV epidemic and Anti-Retroviral Treatment policy on lymphoma incidence and subtypes seen in the Western Cape of South Africa, 2002-2009: preliminary findings of the Tygerberg Lymphoma Study Group. Transfus Apher Sci. 2011;44(2):161–166. | ||
Grewal R, Irimie A, Naidoo N, et al. Hodgkin’s lymphoma and its association with EBV and HIV infection. Crit Rev Clin Lab Sci. 2018;55(2):102–114. | ||
Grewal R, Cucuianu A, Swanepoel C, et al. The role of microRNAs in the pathogenesis of HIV-related lymphomas. Crit Rev Clin Lab Sci. 2015;52(5):232–241. | ||
Fetica B, Pop B, Lisencu C. A report of six cases. Clujul Med. 2014;87(3):192–197. | ||
Tomuleasa C, Selicean S, Gafencu G, et al. Fibroblast dynamics as an in vitro screening platform for anti-fibrotic drugs in primary myelofibrosis. J Cell Physiol. 2018;233(1):422–433. | ||
Berce C, Muresan MS, Soritau O, et al. Cutaneous wound healing using polymeric surgical dressings based on chitosan, sodium hyaluronate and resveratrol. A preclinical experimental study. Colloids Surf B Biointerfaces. 2018;163:155–166. | ||
Frinc I, Dima D, Chitic M, et al. Transthoracic ultrasonography for the follow-up of a chronic lymphocytic leukemia patient with chemotherapy-induced immunosuppression prior to allogeneic stem cell transplantation. A case report. Med Ultrason. 2017;19(3):330–332. | ||
Messinger CJ, Gurzau ES, Breitschwerdt EB, et al. Seroprevalence of Bartonella species, Coxiella burnetii and Toxoplasma gondii among patients with hematological malignancies: a pilot study in Romania. Zoonoses Public Health. 2017;64(6):485–490. | ||
Naresh KN, Rice AJ, Bower M. Lymph nodes involved by multicentric Castleman disease among HIV-positive individuals are often involved by Kaposi sarcoma. Am J Surg Pathol. 2008;32(7):1006–1012. | ||
Oksenhendler E, Boutboul D, Fajgenbaum D, et al. The full spectrum of Castleman disease: 273 patients studied over 20 years. Br J Haematol. 2018;180(2):206–216. | ||
Goudge J, Ngoma B. Exploring antiretroviral treatment adherence in an urban setting in South Africa. J Public Health Policy. 2011;32(Suppl 1):S52–S64. | ||
Peltzer K, Friend-du Preez N, Ramlagan S, Anderson J. Antiretroviral treatment adherence among HIV patients in KwaZulu-Natal, South Africa. BMC Public Health. 2010;10:111. | ||
Gari S, Doig-Acuña C, Smail T, Malungo JR, Martin-Hilber A, Merten S. Access to HIV/AIDS care: a systematic review of socio-cultural determinants in low and high income countries. BMC Health Serv Res. 2013;13:198. | ||
Bower M, Newsom-Davis T, Naresh K, et al. Clinical features and outcome in HIV-associated multicentric Castleman’s disease. J Clin Oncol. 2011;29(18):2481–2486. | ||
Loi S, Goldstein D, Clezy K, Milliken ST, Hoy J, Chipman M. Castleman’s disease and HIV infection in Australia. HIV Med. 2004;5(3):157–162. | ||
Powles T, Stebbing J, Bazeos A, et al. The role of immune suppression and HHV-8 in the increasing incidence of HIV-associated multicentric Castleman’s disease. Ann Oncol. 2009;20(4):775–779. | ||
Mylona EE, Baraboutis IG, Lekakis LJ, Georgiou O, Papastamopoulos V, Skoutelis A. Multicentric Castleman’s disease in HIV infection: a systematic review of the literature. AIDS Rev. 2008;10(1):25–35. | ||
Bacon CM, Miller RF, Noursadeghi M, McNamara C, Du MQ, Dogan A. Pathology of bone marrow in human herpes virus-8 (HHV8)-associated multicentric Castleman disease. Br J Haematol. 2004;127(5):585–591. | ||
Venkataraman G, Uldrick TS, Aleman K, et al. Bone marrow findings in HIV-positive patients with Kaposi sarcoma herpesvirus-associated multicentric Castleman disease. Am J Clin Pathol. 2013;139(5):651–661. | ||
Powles T, Stebbing J, Bazeos A, et al. The role of immune suppression and HHV-8 in the increasing incidence of HIV-associated multicentric Castleman’s disease. Ann Oncol. 2009;20(4):775–779. |
Supplementary materials
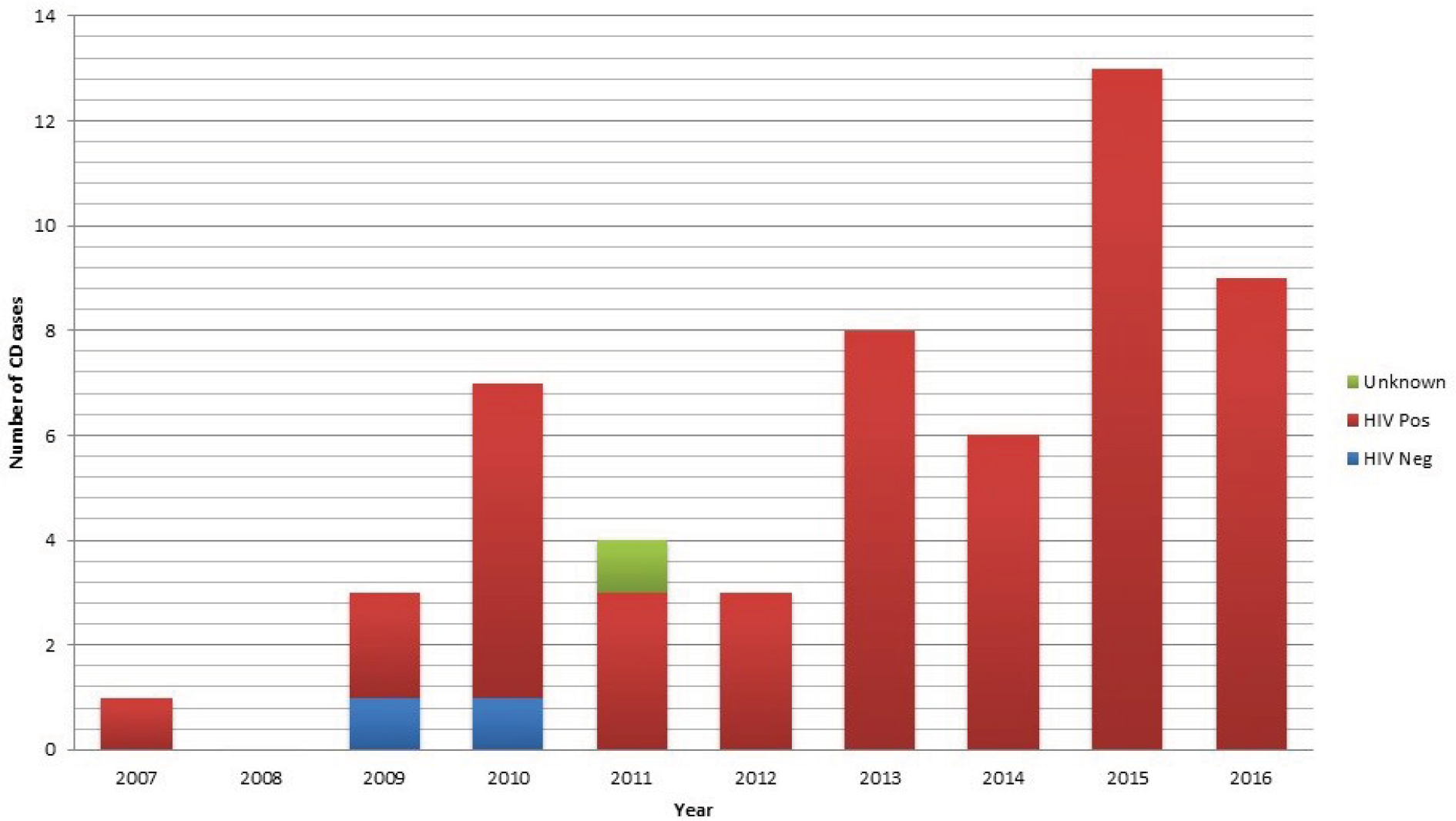 | Figure S1 Bar graph depicts number of patients and their HIV status diagnosed at TAH from 2007-2017 Abbreviations: CD, Castleman’s disease; TAH, Tygerberg Academic Hospital. |
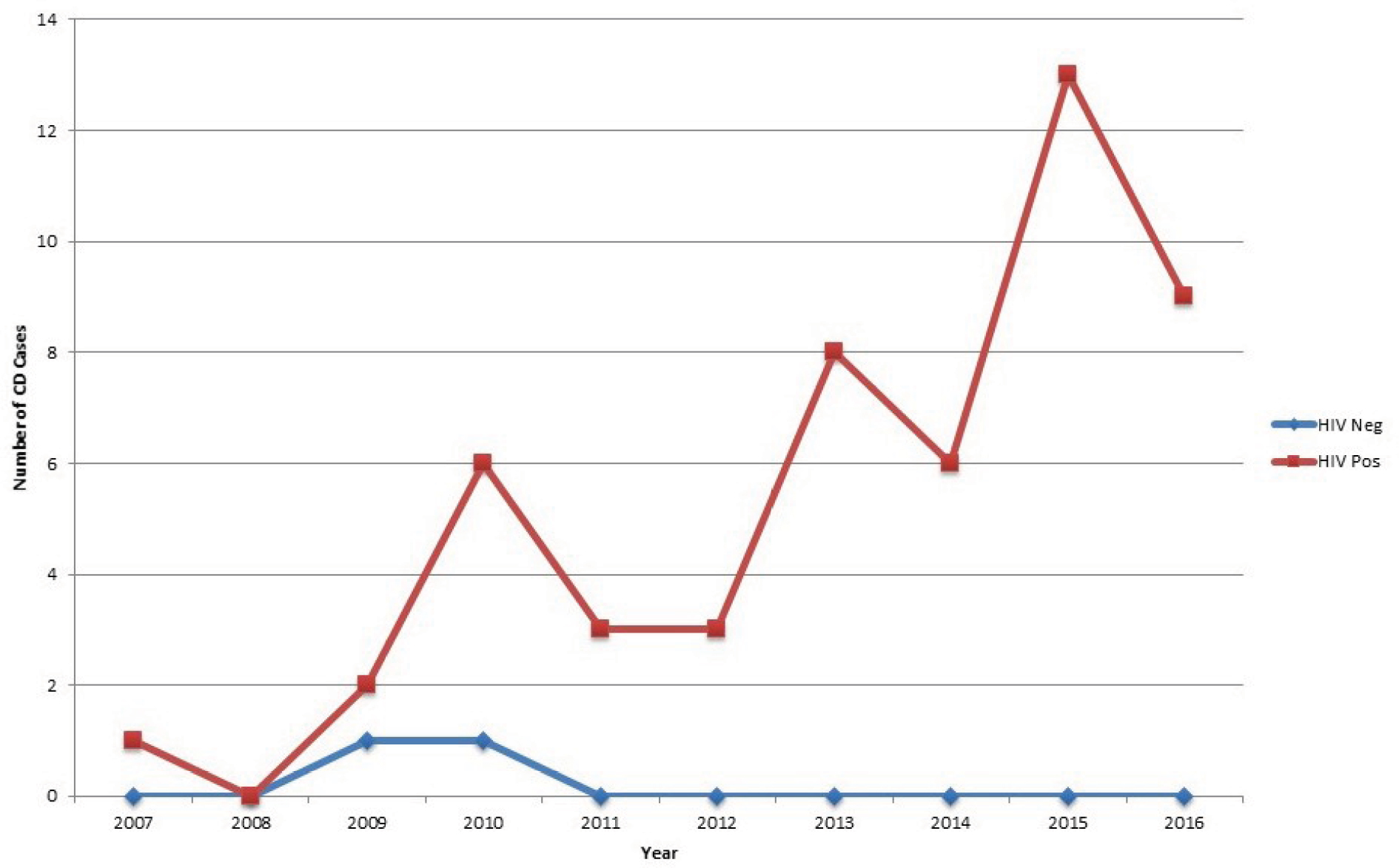 | Figure S2 Chart shows trend of incidence of diagnosis of Castleman disease at TAH over a period of ten years. Abbreviations: CD, Castleman’s disease; TAH, Tygerberg Academic Hospital. |
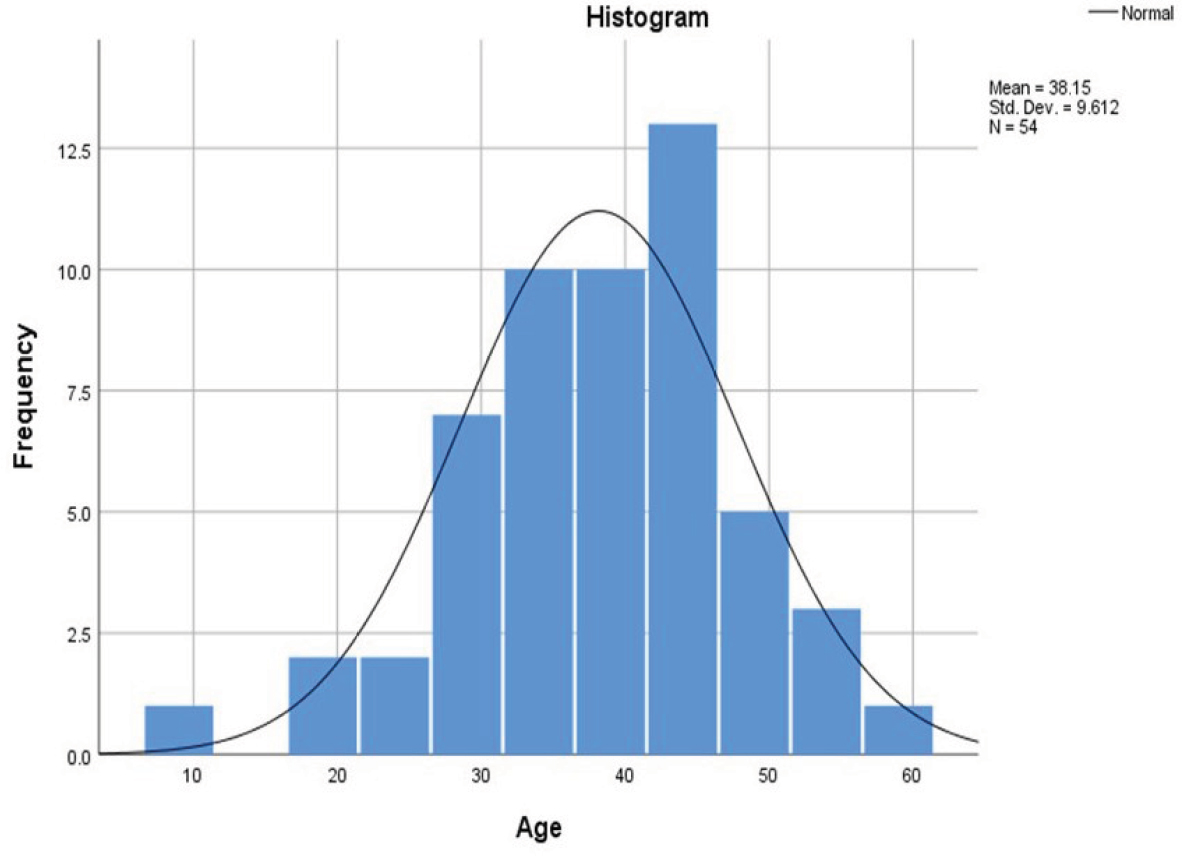 | Figure S3 Histogram showing age (years) distributions of patients with Castleman disease. |
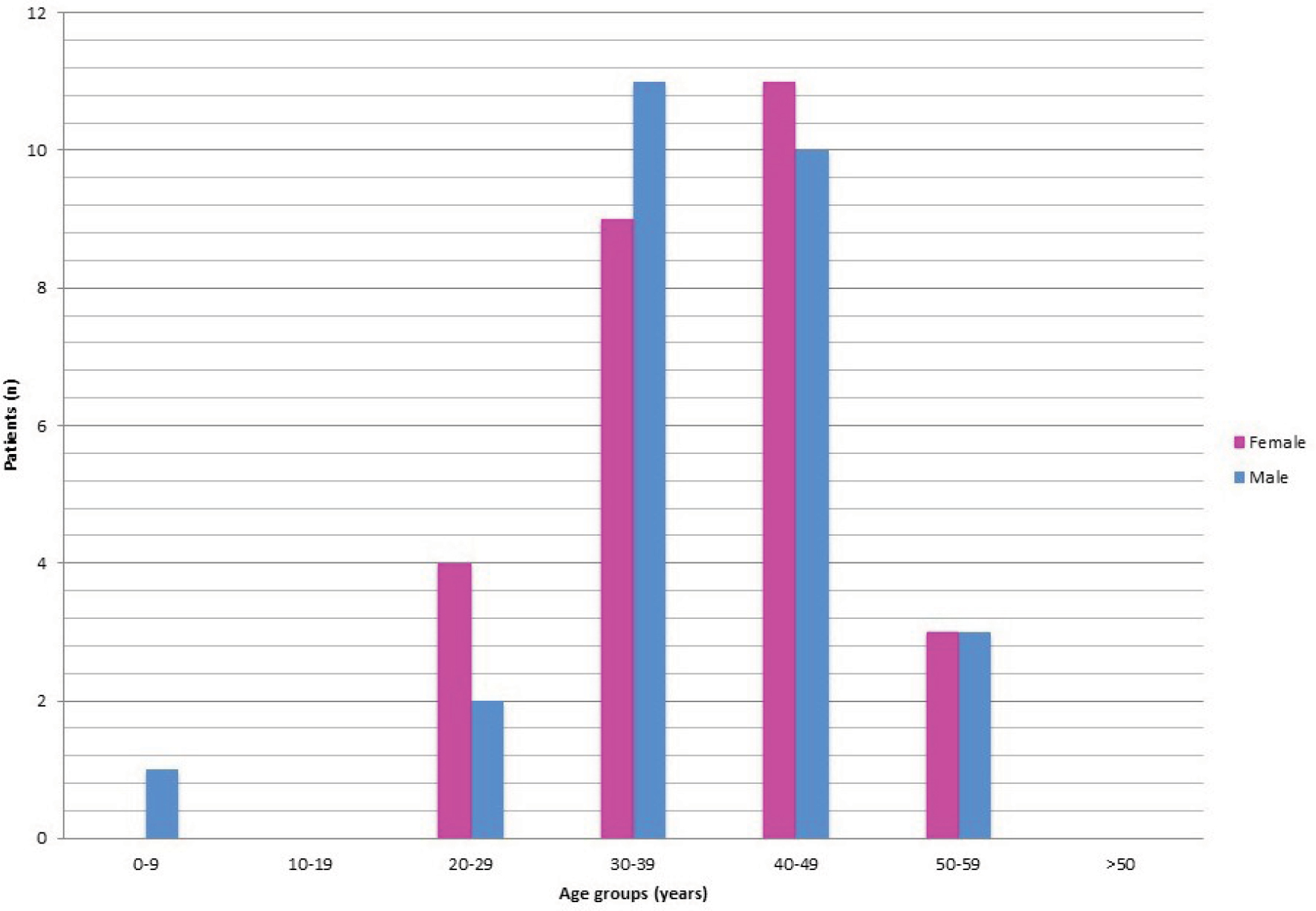 | Figure S4 Bar graph depicts number CD patients were diagnosed at TAH by the age group and gender. Abbreviations: CD, Castleman’s disease; TAH, Tygerberg Academic Hospital. |
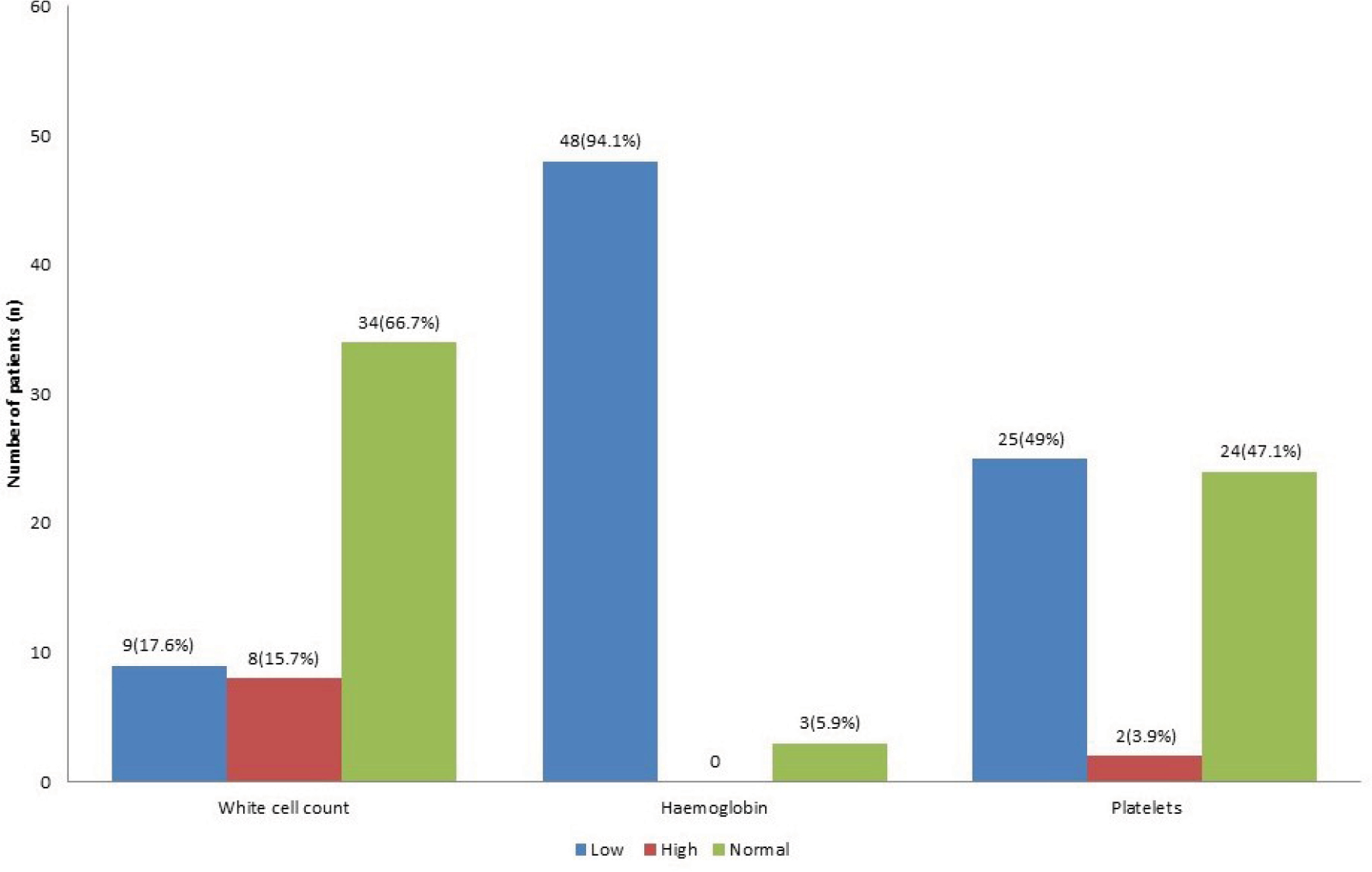 | Figure S5 Chart showing frequency of FBC abnormalities for patients at diagnosis. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.