Back to Journals » Infection and Drug Resistance » Volume 19
Case Report: Rare Community-Acquired Pneumonia with Concurrent Methicillin-Resistant Staphylococcus aureus and Cryptococcus neoformans Infection in an Immunocompetent Young Male
Authors Ye J ![]() , Sun L, Lv D, Zhao S, Mao Q, Xu Y, Chen Y
, Sun L, Lv D, Zhao S, Mao Q, Xu Y, Chen Y ![]()
Received 15 November 2025
Accepted for publication 22 January 2026
Published 27 January 2026 Volume 2026:19 581754
DOI https://doi.org/10.2147/IDR.S581754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Jiayuan Ye,1,* Lu Sun,2,* Dong Lv,3 Shanshan Zhao,4 Qiuqin Mao,5 Yuxiang Xu,6 Yan Chen2
1Department of Infectious Diseases, Shangyu People’s Hospital of Shaoxing, Shaoxing University, Shaoxing, Zhejiang, People’s Republic of China; 2Department of Infectious Diseases, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 3Department of Respiratory, Shangyu People’s Hospital of Shaoxing, Shaoxing University, Shaoxing, Zhejiang, People’s Republic of China; 4Department of Clinical Laboratory, Shangyu People’s Hospital of Shaoxing, Shaoxing University, Shaoxing, Zhejiang, People’s Republic of China; 5Department of Nursing, Shangyu People’s Hospital of Shaoxing, Shaoxing University, Shaoxing, Zhejiang, People’s Republic of China; 6Medical Department, Shangyu People’s Hospital of Shaoxing, Shaoxing University, Shaoxing, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Chen, Department of Infectious Diseases, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, 310016, People’s Republic of China, Email [email protected] Yuxiang Xu, Medical Department, Shangyu People’s Hospital of Shaoxing, Shaoxing University, No. 517, Minsheng Avenue, Baiguan Street, Shangyu District, Shaoxing, Zhejiang, People’s Republic of China, Tel + 86 0575 82185313, Email [email protected]
Abstract: Cryptococcal pneumonia predominantly occurs in immunocompromised patients, but its incidence among immunocompetent individuals has been increasing in recent years. However, cases of co-infection with Cryptococcus neoformans and community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) in immunocompetent hosts remain exceedingly rare. This study reports on a previously healthy 30-year-old male who presented with 20-days cough and 1-day fever. Through nanopore targeted sequencing (NTS) of bronchoalveolar lavage fluid (BLAF) and traditional microbial culture, he was ultimately diagnosed with a co-infection of C. neoformans and CA-MRSA. The patient showed significant improvement after treatment with oral linezolid (0.6 g twice daily) for 2 weeks and oral fluconazole (400 mg once daily) for 6 months. This case highlights that even immunocompetent individuals can simultaneously contract multiple community-acquired pathogens, while also underscoring the clinical utility of NTS in the early diagnosis of co-infections and detection of resistance genes.
Keywords: community-acquired methicillin-resistant Staphylococcus aureus, Cryptococcus neoformans, pulmonary infection, nanopore sequencing, case report
Introduction
Pulmonary infection is a leading global cause of morbidity and mortality.1 Among respiratory pathogens, Cryptococcus neoformans and community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) are clinically significant. C. neoformans predominantly infects immunocompromised hosts, causing pneumonia with characteristic imaging findings,2,3 while CA-MRSA can lead to severe pneumonia with high mortality.4,5
Although community-acquired pneumonia is typically monomicrobial,6 polymicrobial infections—common in immunocompromised patients and linked to poorer outcomes6,7—are increasingly recognized in immunocompetent hosts. Risk factors such as viral co-infection, advanced age, or diabetes may exacerbate this risk.8–10 The synergistic mechanisms in immunocompetent hosts remain unclear but may involve immune modulation,11 and co-infections often result in more complex clinical courses regardless of immune status.12
Notably, in China, immunocompetent individuals account for up to 69.7% of pulmonary cryptococcosis cases—approximately double the global rate,13–15 highlighting the need to consider this pathogen even without overt immunodeficiency. The disease shows male predominance and nonspecific manifestations.16,17
Given the rarity and diagnostic challenge of CA-MRSA and C. neoformans co-infection in immunocompetent hosts, this report presents a relevant case to discuss its clinical characteristics.
Case Presentation
A 30-year-old immunocompetent male presented with a 20-day history of persistent cough and 1-day of low-grade fever. His symptoms began with a minimally productive cough on November 24, 2024 (Day 1). Initial outpatient laboratory tests were obtained. Empirical treatment with azithromycin and symptomatic therapy was unsuccessful. On Day 18 (December 12), the onset of fever prompted a chest CT scan, the results of which are detailed in the Radiological Findings section (Figure 1), leading to hospitalization on Day 20 (December 14). Intravenous(IV) levofloxacin (0.5 g once daily) was initiated. Two days after admission (Day 22, December 16), bronchoscopy was performed. The obtained bronchoalveolar lavage fluid (BALF) sample was sent simultaneously for NTS, bacterial culture, and fungal culture. Analysis of the BALF was positive for cryptococcal antigen, and NTS (December 18) detected C. neoformans (26,235 copies/mL) and Staphylococcus aureus (19,630 copies/mL; mecA+), later confirmed by bacterial culture as MRSA (December 20, Figure 2A) and fungal culture isolating C. neoformans (December 21, Figure 2B), resulting in successful transition to oral linezolid (0.6 g twice daily) plus fluconazole (400 mg once daily) with 2-week antibacterial and 6-month antifungal therapy demonstrating radiographic resolution (Figure 3) at follow-up.
 |
Figure 1 Chest CT demonstrates multiple bilateral pulmonary infiltrates, with evidence of cavitation as indicated by the red arrow. |
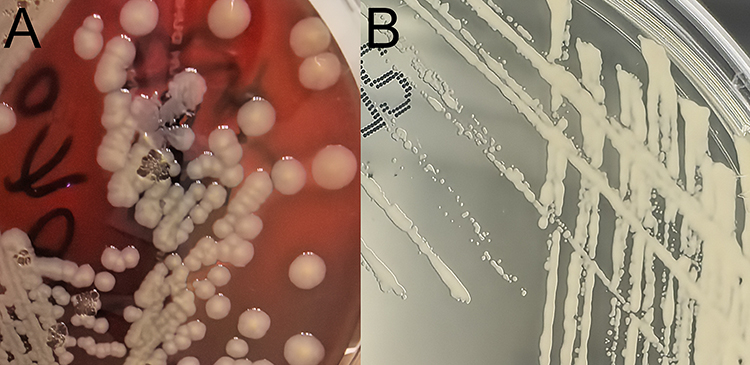 |
Figure 2 (A) Twenty-four-hour culture on blood agar revealed medium-sized, round, convex colonies with smooth surfaces and a clear zone of hemolysis. (B) Following 48 hours of incubation, cream-colored, yeast-like colonies appeared that were round, convex, with smooth and moist surfaces. |
 |
Figure 3 Follow-up chest CT shows resolution of the lesion, as indicated by the red arrow. |
Physical Examination Revealed
T 36.5°C, HR 116 bpm, RR 20 breaths/min, BP 140/92 mmHg; specialist examination showed clear consciousness, normal mental status, no jaundice in skin or sclera, clear lung sounds with moist rales bilaterally, regular heart rhythm without pathological murmurs, soft and non-tender abdomen with no rebound tenderness, normal limb mobility, and no significant edema in lower extremities.
Medical history indicated good baseline health with no chronic conditions, including no history of HIV, Hepatitis B or C, hypertension, diabetes mellitus, hepatic steatosis, chronic kidney disease, malignancy, or rheumatic/autoimmune diseases, and no use of medications such as systemic corticosteroids. The patient reported occasional exposure to pigeon droppings within the past year.
Laboratory Findings
(November 24, 2024): Initial blood tests indicated a mild leukocytosis (WBC 10.1 × 109/L) with a normal differential. The level of high-sensitivity C-reactive protein (hs-CRP) was marginally elevated at 0.8 mg/L. Other routine parameters, including platelet count, were within normal ranges.
(December 13, 2024): WBC 10.0 × 10^9/L (neutrophils 50.4%), hemoglobin 157 g/L, platelets 209 ×10^9/L, hs-CRP 0.5 mg/L, SAA < 2.00 mg/L, ESR 4 mm/h, PCT 0.030 ng/mL; immunocompetent status with negative immunofixation electrophoresis and blood cultures; negative serum cryptococcal antigen, (1→3)-β-D-glucan, and galactomannan tests; normal hepatic/renal function and electrolytes; unremarkable Electrocardiogram (ECG); and negative T-cell Spot Test (T-SPOT) (see Table 1 for complete details).
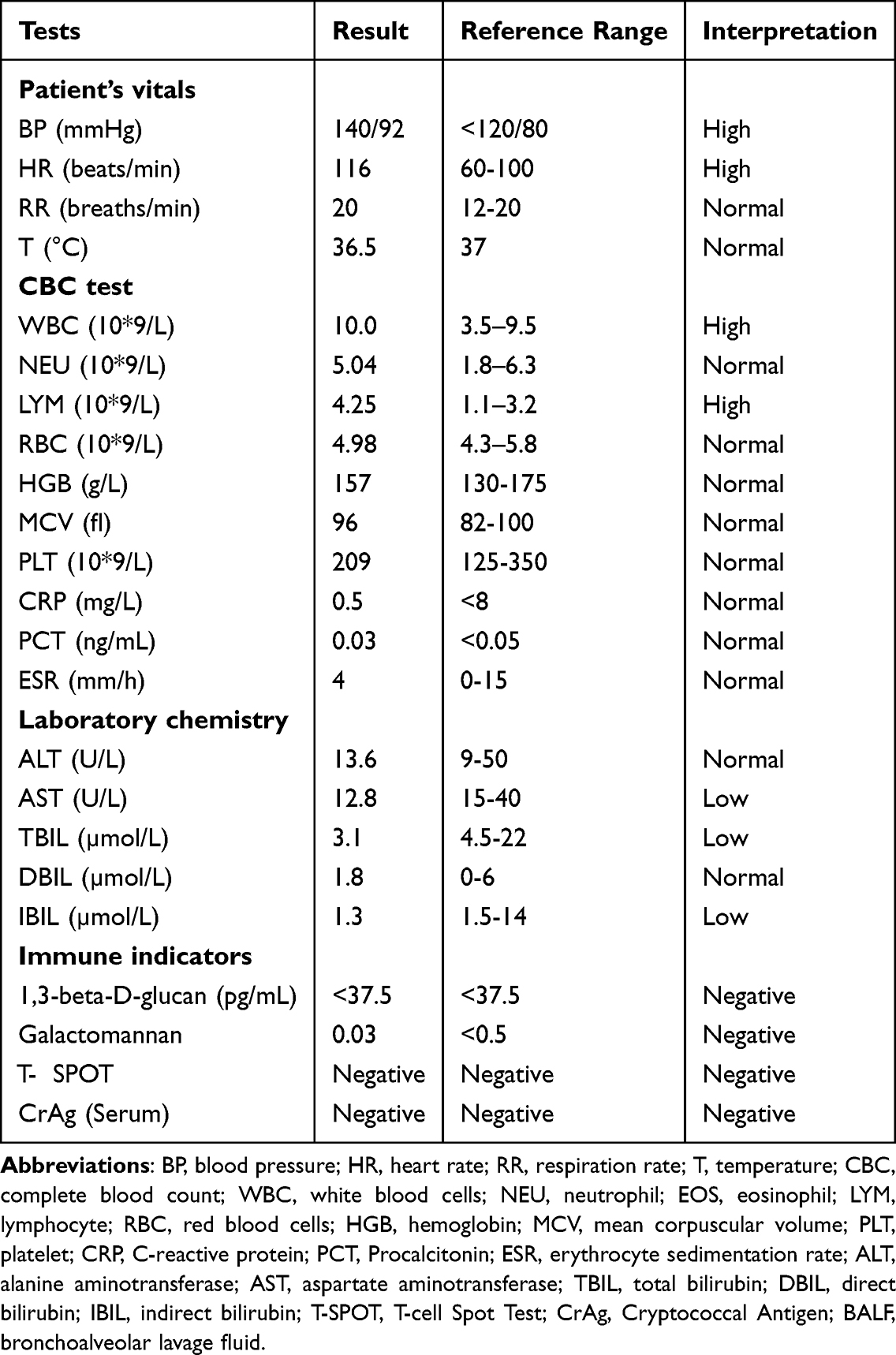 |
Table 1 The Physical Examination Data and Laboratory Test Results |
Radiological Findings
(December 12, 2024): A chest CT revealed multiple pulmonary infiltrates with cavitation in both lungs (Figure 1).
(June 1, 2025): A follow-up chest CT demonstrated significant resolution of the lesions (Figure 3).
NTS Testing
BALF samples (>5 mL) were collected and promptly transported on dry ice to Hangzhou Dean Medical Laboratory for NTS.
Bacterial Culture
BALF was centrifuged at 3000 rpm for 15 minutes. After removing the supernatant, the sediment was inoculated onto blood agar and chocolate agar plates followed by overnight incubation at 35°C with 5% CO2. On blood agar, round, convex, smooth colonies with transparent β-hemolytic halos were observed after 24 hours (Figure 2A). Gram staining revealed Gram-positive cocci predominantly arranged in irregular grape-like clusters, with occasional single cells, pairs, tetrads, and short chains. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS, Bruker) identified the isolate as Staphylococcus aureus (score: 2.4) (Figure 4A). Antimicrobial susceptibility testing for Staphylococcus aureus was performed using the VITEK 2 system with the AST-GP67 card (bioMérieux, France), with results interpreted according to the Clinical and Laboratory Standards Institute (CLSI M100) breakpoints. The detailed profile is presented in Table 2.
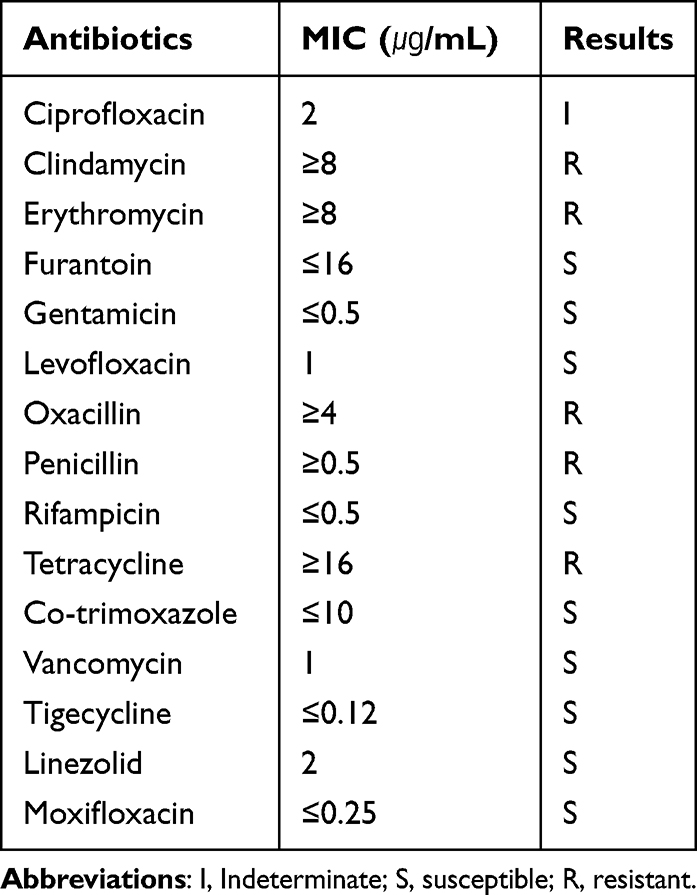 |
Table 2 Drug Susceptibility Testing of MRSA Strains |
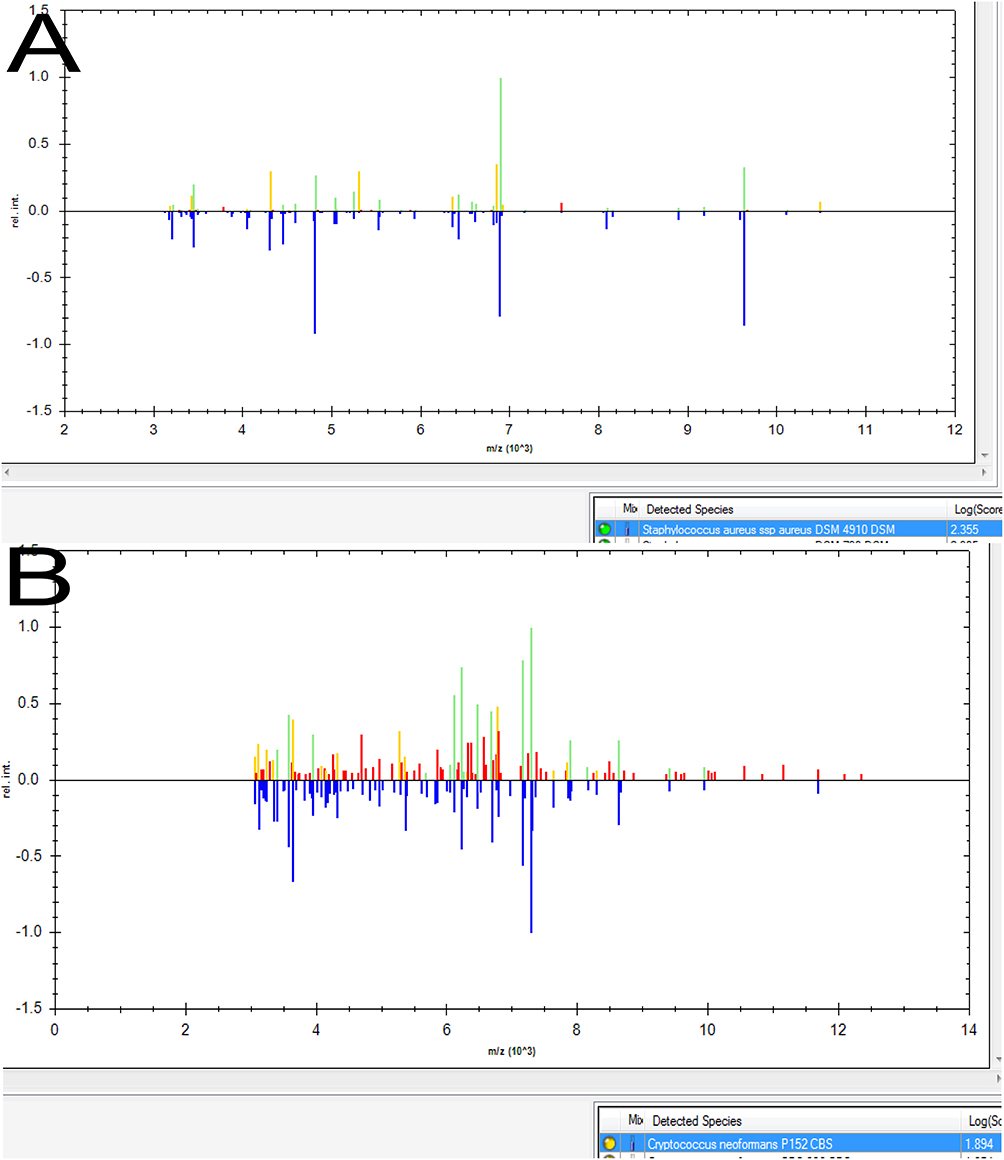 |
Figure 4 MALDI-TOF MS identification of the isolates. (A) Staphylococcus aureus (score: 2.4). (B) Cryptococcus neoformans (score: 1.9). |
Fungal Culture
BALF sediment was similarly processed and cultured on Sabouraud dextrose agar for 48 hours, yielding creamy, smooth, yeast-like colonies. India ink staining demonstrated round, encapsulated yeast cells with prominent refractile halos under dark-field microscopy, some showing budding but no hyphae (Figure 2B). Gram staining revealed large, Gram-positive (blue-purple) spherical cells with occasional “beaded” connections between them. MALDI-TOF MS (Bruker) confirmed C. neoformans (score: 1.9) (Figure 4B). Antifungal susceptibility testing for C. neoformans was conducted using the VITEK 2 system with the AST-YS03 yeast card (bioMérieux). Interpretive criteria were referenced as follows: CLSI breakpoints for fluconazole and EUCAST epidemiological cut-off values (ECOFFs) for other agents. The results are provided in Table 3.
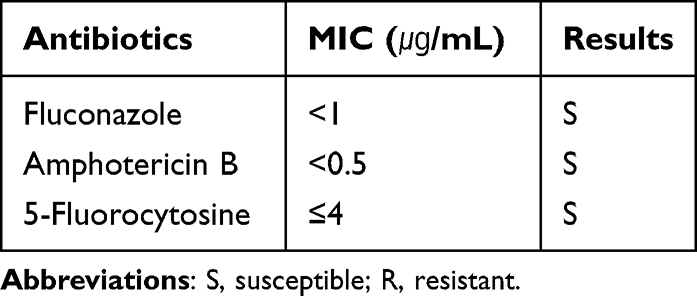 |
Table 3 Drug Susceptibility Testing of Cryptococcus Strains |
Molecular Characterization
Multilocus sequence typing (MLST) was performed for molecular characterization of the isolates. For Staphylococcus aureus, revealing the isolate belonged to sequence type (ST) 4513 (clonal complex 59, CC59). For C. neoformans, identifying the isolate as molecular type C. neoformans (serotype A, VNI), with sequence type ST5.
Treatment
The patient initially received intravenous levofloxacin (0.5 g once daily) for 3 days following admission, which improved fever but failed to alleviate cough. Upon definitive diagnosis of CA-MRSA and C. neoformans co-infection through BALF NTS and cultures, antimicrobial therapy was adjusted to oral linezolid (0.6 g twice daily) targeting CA-MRSA for 2 weeks. This agent was chosen based on its confirmed susceptibility profile (Table 2), optimal pharmacokinetics for pulmonary infection, and high oral bioavailability, which supported a complete course of outpatient therapy. Treatment was combined with oral fluconazole (400 mg once daily) for 6 months as anti-cryptococcal treatment. Follow-up imaging demonstrated significant radiographic improvement after completion of antifungal therapy.
Discussion
The present case of co-infection with Cryptococcus neoformans and CA-MRSA in an immunocompetent host highlights several important clinical and diagnostic considerations. This case involves a 30-year-old immunocompetent male with no significant medical history but documented pigeon exposure. Pigeon droppings provide a nitrogen-rich environment that promotes the growth and long-term persistence of C. neoformans. Human infection typically occurs via inhalation of aerosolized particles from disturbed contaminated sites, which aligns with the patient’s exposure history.18 The diagnostic challenge was evidenced by initially negative serum cryptococcal antigen testing, with definitive diagnosis ultimately requiring NTS, culture, and BALF cryptococcal antigen detection. This serological false-negative phenomenon may occur when cryptococcal infection remains localized to the lungs without hematogenous dissemination, resulting in serum circulating capsular antigen (CrAg) levels below detection thresholds.19
CA-MRSA refers to MRSA strains circulating in community settings. In recent years, CA-MRSA infections have emerged as a growing public health concern.20 Distinct from traditional healthcare-associated MRSA, CA-MRSA predominantly affects younger patients under 30 years old, most without typical healthcare exposures or other risk factors.21 Notably, MRSA accounts for up to 9% of community-acquired pneumonia (CAP) cases, with MRSA pneumonia demonstrating substantial mortality and serving as an independent prognostic factor.22,23 As a common human commensal, Staphylococcus aureus colonizes the skin, cutaneous glands, and mucous membranes (eg, nares and gut) of healthy individuals without causing symptoms.24 Epidemiological studies indicate approximately 20% of individuals are persistent nasal carriers, 30% intermittent carriers, while the remaining 50% generally remain non-carriers.25 Infection occurs when nasopharyngeal colonizers are aspirated into the lower respiratory tract - the most frequent pathogenic mechanism for Staphylococcus aureus pneumonia.26 In this case, BALF NTS detected Staphylococcus aureus carrying the mecA resistance gene, and combined with cavitary lesions on chest CT, we confirmed concurrent CA-MRSA infection. Fortunately, timely antibiotic adjustment to linezolid following pathogen identification led to successful treatment.
The mechanisms underlying co-infection with Cryptococcus and MRSA in immunocompetent hosts remain incompletely understood, as demonstrated in this case. Current evidence suggests Cryptococcus may modulate host immune responses through multiple pathways to facilitate infection in immunocompetent individuals.27 Potential mechanisms include: (1) suppression of neutrophil recruitment and pro-inflammatory cytokine production in lung tissue;28 (2) interference with dendritic cell-mediated Th1/Th17 immune responses and downregulation of pulmonary chemokine expression.29 These immunomodulatory effects may lead to compromised protective immune responses. Notably, neutrophil dysfunction or inadequate recruitment can create a favorable microenvironment for MRSA to evade host clearance mechanisms and proliferate in lung tissue, ultimately causing pneumonia or even sepsis.30 Furthermore, impaired Th1/Th17 responses significantly weaken host defenses against MRSA, facilitating bacterial transition from colonization to invasive infection by breaching mucosal barriers.31 Integrating these mechanisms, we hypothesize this patient likely experienced the following pathological sequence: persistent cryptococcal infection altered local immune microenvironments (particularly through neutrophil and Th1/Th17 response suppression), thereby creating favorable conditions for secondary MRSA infection that promoted progression from colonization to invasive disease. This explains the universal risk of poor outcomes: while immunocompromised patients suffer from invasion due to barrier loss, immunocompetent hosts (as in this case) face diagnostic delays due to localized immune dysregulation. Consequently, suspicion for co-infection must be upheld across all patients.
Current studies have confirmed that mixed infectious pneumonia is often associated with more complex clinical courses and worse prognoses.32 Therefore, rapid and accurate pathogen identification is crucial for clinical decision-making. However, conventional etiological detection methods (including microbial culture, Polymerase Chain Reaction (PCR) techniques, and antigen/antibody immunoassays) exhibit significant limitations: prolonged detection time, low positivity rates, and limited pathogen spectrum coverage, making them inadequate for meeting the diagnostic needs of critical infections.33 As an emerging third-generation sequencing technology, NTS demonstrates the following notable advantages: ultra-long read lengths (tens to hundreds of kilobases) with rapid sequencing capability;34 real-time data reading and analysis functions enabling simultaneous detection of antimicrobial resistance (AMR) phenotypes; these characteristics render it particularly valuable in infectious disease surveillance and genomic research.35 In this case, NTS successfully identified both Cryptococcus and MRSA within 24 hours, while traditional culture methods required over 72 hours to yield final results - a striking contrast highlighting NTS’s superior timeliness. Based on these findings, we recommend that for immunocompetent patients with complex chest imaging manifestations, clinicians should maintain high suspicion for community-acquired co-infections. In such scenarios, early application of NTS for rapid pathogen identification and resistance analysis represents an optimal diagnostic strategy.
Conclusion
This study reports a rare case of concomitant pulmonary cryptococcosis and CA-MRSA infection in an immunocompetent host, where NTS enabled rapid pathogen detection within 24 hours followed by culture confirmation, with successful treatment using linezolid-fluconazole combination therapy. This case highlights that clinicians should consider polymicrobial infections even in immunocompetent individuals presenting with radiologically complex community-acquired pneumonia. NTS technology, with its rapid and precise detection capabilities, serves as a valuable complement to conventional microbiological testing, offering a novel approach for early diagnosis of challenging infections, though the synergistic pathogenic mechanisms warrant further investigation.
Abbreviations
CA-MRSA, community-acquired methicillin-resistant Staphylococcus aureus; NTS, nanopore targeted sequencing; BALF, bronchoalveolar lavage fluid; IV, intravenous; BP, blood pressure; HR, heart rate; RR, respiration rate; T, temperature; CBC, complete blood count; WBC, white blood cells; NEU, neutrophil; EOS, eosinophil; LYM, lymphocyte; RBC, red blood cells; HGB, hemoglobin; MCV, mean corpuscular volume; PLT, platelet; CRP, C-reactive protein; PCT, Procalcitonin; ESR, erythrocyte sedimentation rate; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TBIL, total bilirubin; DBIL, direct bilirubin; IBIL, indirect bilirubin; T-SPOT, T-cell Spot Test; CrAg, Cryptococcal Antigen; BALF, bronchoalveolar lavage fluid; ECG, Electrocardiogram; MALDI-TOF MS, Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry; ST, sequence type; MLST, multi-locus sequence typing; CAP, community-acquired pneumonia; PCR, Polymerase Chain Reaction; AMR, antimicrobial resistance.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Approval and Consent to Participate
All procedures performed in the study involving human participants were in accordance with the ethical standards of the Ethics Committee of the Shangyu People’s Hospital of Shaoxing, no institutional approval is needed to publish the details of this case.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Written consent is available by request.
Acknowledgments
We thank the patient and their family for their selfless assistance. This manuscript does not involve any uncropped Gels and Blots images, such as those from Western Blot experiments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Program of Zhejiang Provincial Center for Disease Control and Prevention (Grant No.2026JKY288) and the Science and Technology Program of Shaoxing Municipal (Grant No.2025A14025).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Magill SS, Edwards JR, Bamberg W, et al. Multistate point-prevalence survey of health care-associated infections. New Engl J Med. 2014;370(13):1198–10. doi:10.1056/NEJMoa1306801
2. Onyishi CU, May RC. Human immune polymorphisms associated with the risk of cryptococcal disease. Immunology. 2022;165(2):143–157. doi:10.1111/imm.13425
3. Maziarz EK, Perfect JR. Cryptococcosis. Infect Dis Clin North Am. 2016;30(1):179–206. doi:10.1016/j.idc.2015.10.006
4. Self WH, Wunderink RG, Williams DJ, et al. Staphylococcus aureus community-acquired pneumonia: prevalence, clinical characteristics, and outcomes. Clin Infect Dis. 2016;63(3):300–309. doi:10.1093/cid/ciw300
5. Tadros M, Williams V, Coleman BL, et al. Epidemiology and outcome of pneumonia caused by methicillin-resistant Staphylococcus aureus (MRSA) in Canadian hospitals. PLoS One. 2013;8(9):e75171. doi:10.1371/journal.pone.0075171
6. Bjarnason A, Westin J, Lindh M, et al. Incidence, etiology, and outcomes of community-acquired pneumonia: a population-based study. Open Forum Infect Dis. 2018;5(2):ofy010. doi:10.1093/ofid/ofy010
7. Wang J, Han Y, Feng J. Metagenomic next-generation sequencing for mixed pulmonary infection diagnosis. BMC Pulm Med. 2019;19(1):252. doi:10.1186/s12890-019-1022-4
8. Shi Y, Shi X, Liang J, et al. Aggravated MRSA pneumonia secondary to influenza A virus infection is derived from decreased expression of IL-1β. J Med Virol. 2020;92(12):3047–3056. doi:10.1002/jmv.26329
9. Wu HY, Chang PH, Huang YS, et al. Recommendations and guidelines for the diagnosis and management of coronavirus Disease-19 (COVID-19) associated bacterial and fungal infections in Taiwan. J Microbiol Immunol Infect. 2023;56(2):207–235. doi:10.1016/j.jmii.2022.12.003
10. Wang M, Li W, Wang H, Song P. Development and validation of machine learning-based models for predicting healthcare-associated bacterial/fungal infections among COVID-19 inpatients: a retrospective cohort study. Antimicrob Resist Infect Control. 2024;13(1):42. doi:10.1186/s13756-024-01392-7
11. Kanneganti TD, Hardt WD. Pathogen’s dynamic standoff with the host. Curr Opin Microbiol. 2021;
12. Shah MM, Hsiao EI, Kirsch CM, Gohil A, Narasimhan S, Stevens DA. Invasive pulmonary aspergillosis and influenza co-infection in immunocompetent hosts: case reports and review of the literature. Diagn Microbiol Infect Dis. 2018;91(2):147–152. doi:10.1016/j.diagmicrobio.2018.01.014
13. Yao K, Qiu X, Hu H, et al. Pulmonary cryptococcosis coexisting with central type lung cancer in an immuocompetent patient: a case report and literature review. BMC Pulm Med. 2020;20(1):161. doi:10.1186/s12890-020-01200-z
14. Hou X, Kou L, Han X, Zhu R, Song L, Liu T. Pulmonary cryptococcosis characteristics in immunocompetent patients-A 20-year clinical retrospective analysis in China. Mycoses. 2019;62(10):937–944. doi:10.1111/myc.12966
15. Wang Y, Gu Y, Shen K, et al. Clinical features of cryptococcosis in patients with different immune statuses: a multicenter study in Jiangsu Province-China. BMC Infect Dis. 2021;21(1):1043. doi:10.1186/s12879-021-06752-x
16. Ou XT, Wu JQ, Zhu LP, et al. Genotypes coding for mannose-binding lectin deficiency correlated with cryptococcal meningitis in HIV-uninfected Chinese patients. J Infect Dis. 2011;203(11):1686–1691. doi:10.1093/infdis/jir152
17. Shirley RM, Baddley JW. Cryptococcal lung disease. Curr Opin Pulm Med. 2009;15(3):254–260. doi:10.1097/MCP.0b013e328329268d
18. Zhao Y, Ye L, Zhao F, et al. Cryptococcus neoformans, a global threat to human health. Infect Dis Poverty. 2023;12(1):20. doi:10.1186/s40249-023-01073-4
19. Yuqiao X, Wenying X, Fang N. False-Negative serum cryptococcal antigen lateral flow immunoassay result for a patient with disseminated cryptococcal disease. Infect Drug Resist. 2020;2877–2881. doi:10.2147/idr.s265784
20. Yarovoy JY, Monte AA, Knepper BC, Young HL. Epidemiology of community-onset Staphylococcus aureus bacteremia. West J Emerg Med. 2019;20(3):438–442. doi:10.5811/westjem.2019.2.41939
21. Naimi TS, LeDell KH, Como-Sabetti K, et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA. 2003;290(22):2976–2984. doi:10.1001/jama.290.22.2976
22. He H, Wunderink RG. Staphylococcus aureus Pneumonia in the Community. Semin Respir Crit Care Med. 2020;41(4):470–479. doi:10.1055/s-0040-1709992
23. Aliberti S, Reyes LF, Faverio P, et al. Global initiative for meticillin-resistant Staphylococcus aureus pneumonia (GLIMP): an international, observational cohort study. Lancet Infect Dis. 2016;16(12):1364–1376. doi:10.1016/s1473-3099(16)30267-5
24. Lakhundi S, Zhang K. Methicillin-ResistantStaphylococcus aureus: molecular characterization, evolution, and epidemiology. Clin Microbiol Rev. 2018;31(4). doi:10.1128/cmr.00020-18
25. David MZ, Mennella C, Mansour M, Boyle-Vavra S, Daum RS. Predominance of methicillin-resistant Staphylococcus aureus among pathogens causing skin and soft tissue infections in a large urban jail: risk factors and recurrence rates. J Clin Microbiol. 2008;46(10):3222–3227. doi:10.1128/jcm.01423-08
26. Paling FP, Wolkewitz M, Bode LGM, et al. Staphylococcus aureus colonization at ICU admission as a risk factor for developing S. aureus ICU pneumonia. Clin Microbiol Infect. 2017;23(1):
27. Wang J, Zeng Y, Luo W, Xie X, Li S. The role of cryptococcus in the immune system of pulmonary cryptococcosis patients. PLoS One. 2015;10(12):e0144427. doi:10.1371/journal.pone.0144427
28. Cheng PY, Sham A, Kronstad JW. Cryptococcus gattii isolates from the British Columbia cryptococcosis outbreak induce less protective inflammation in a murine model of infection than Cryptococcus neoformans. Infect Immun. 2009;77(10):4284–4294. doi:10.1128/iai.00628-09
29. Angkasekwinai P, Sringkarin N, Supasorn O, et al. Cryptococcus gattii infection dampens Th1 and Th17 responses by attenuating dendritic cell function and pulmonary chemokine expression in the immunocompetent hosts. Infect Immun. 2014;82(9):3880–3890. doi:10.1128/iai.01773-14
30. Zhang J, Shao Y, Wu J, et al. Dysregulation of neutrophil in sepsis: recent insights and advances. Cell Commun Signal. 2025;23(1):87. doi:10.1186/s12964-025-02098-y
31. Lin L, Ibrahim AS, Xu X, et al. Th1-Th17 cells mediate protective adaptive immunity against Staphylococcus aureus and Candida albicans infection in mice. PLoS Pathog. 2009;5(12):e1000703. doi:10.1371/journal.ppat.1000703
32. Shen X, Feng B, Shi W, Cheng W, Zhang T. Concomitant viral and bacterial pneumonia among patients in ICU with mechanical respiratory support. J Infect Dev Ctries. 2022;16(9):1482–1489. doi:10.3855/jidc.12999
33. Zheng Y, Qiu X, Wang T, Zhang J. The diagnostic value of metagenomic next-generation sequencing in lower respiratory tract infection. Front Cell Infect Microbiol. 2021;11:694756. doi:10.3389/fcimb.2021.694756
34. Schmidt J, Blessing F, Fimpler L, Wenzel F. Nanopore sequencing in a clinical routine laboratory: challenges and opportunities. Clin Lab. 2020;66(6). doi:10.7754/Clin.Lab.2019.191114
35. Liu PY, Wu HC, Li YL, et al. Comprehensive pathogen identification and antimicrobial resistance prediction from positive blood cultures using nanopore sequencing technology. Genome Med. 2024;16(1):141. doi:10.1186/s13073-024-01416-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.