")
Back to Journals » The Application of Clinical Genetics » Volume 15
Case Report of a Juvenile Patient with Autism Spectrum Disorder with a Novel Combination of Copy Number Variants in ADGRL3 (LPHN3) and Two Pseudogenes
Authors Maurer MH , Kohler A , Hudemann M, Jüngling J, Biskup S, Menzel M
Received 5 February 2022
Accepted for publication 25 August 2022
Published 2 September 2022 Volume 2022:15 Pages 125—131
DOI https://doi.org/10.2147/TACG.S361239
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Francis Ali-Osman
Martin H Maurer,1 Anja Kohler,1 Melanie Hudemann,1 Jerome Jüngling,2 Saskia Biskup,2,3 Martin Menzel1
1Mariaberg Hospital for Child and Adolescent Psychiatry, Gammertingen, Germany; 2Zentrum für Humangenetik, Tübingen, Germany; 3Center for Genomics and Transcriptomics, CeGaT GmbH, Tübingen, Germany
Correspondence: Martin H Maurer, Mariaberg Hospital for Child and Adolescent Psychiatry, Burghaldenstraße 12, Gammertingen, 72501, Germany, Tel +49 7124 9237200, Fax +49 7124 923555, Email [email protected]
Abstract: We report the finding of two copy number variants (CNVs) in a 12-year-old boy presenting both with autism spectrum disorder (ASD) and attention deficit/hyperactivity disorder (ADHD). Clinical features included aggressive behavior, mood instability, suicidal statements, repetitive and restrictive behavior, sensitivity to noise, learning problems and dyslexia, though no intellectual disability was present. Using array-based comparative genomic hybridization (array-CGH), we identified two CNVs, both triplex duplications of 324 kb on 3p26.3, and 284 kb on 4q13.1, respectively. One of the CNVs is located on chromosome 4q13.1 in the region of the gene encoding for adhesion G protein-coupled receptor L3 (ADGRL3, former name: latrophilin-3, LPHN3), the other on chromosome 3p26.3 in the region of the two pseudogenes AC090043.1 and RPL23AP39. The patient described in the present study showed increased symptoms under methylphenidate treatment but responded positively to 3 mg per day of the atypical neuroleptic drug aripiprazole. To our knowledge, this is the first report of a CNV in the ADGRL3 gene and its first association with ASD in humans.
Keywords: latrophilin-3, LPHN3, adhesion G protein-coupled receptor L3, ADGRL3, autism spectrum disorder, ASD
Introduction
In recent years, a large number of candidate genes associated with autism spectrum disorder (ASD) has been identified,1–6 most of them involved in neurodevelopmental pathways such as axon guidance, synapse assembly, neural progenitor cell migration and differentiation.7 A near relationship to other neurodevelopmental disorders, most prominently, attention deficit/hyperactivity disorder (ADHD) has been described both in animal models and clinical samples.1,8 One of these, the Adhesion G protein-coupled receptor L3 (ADGRL3, old name: latrophilin-3, LPHN3) has been linked to attention deficit hyperactivity disorder (ADHD) and substance use disorders (SUDs), where its function in hyperactivity and locomotor activity has been reported.1,9,10 ADGRL3 is of special interest in neurodevelopmental disorder research, since it belongs to a group of postsynaptic adhesion G protein coupled receptors (GPCRs) of the latrophilin family, mediating target recognition in synapse assembly.11 In a clinical context, ADGRL3 is also of interest for pharmacogenetics, since it predicts the responsiveness to medication such as methylphenidate (MPH).9,12 So far, no clinically associated coding variants of ADGRL3 have been found in humans,13 but the non-coding single nucleotide polymorphism (SNP) rs2271338 seems to impair ADGRL3 expression.10
In this case report, we report the finding of two copy number variants (CNVs) in a 12-year-old child presenting both with ASD and ADHD. One of the CNVs is located in the region of ADGRL3, the other in the region of pseudogenes AC090043.1 and RPL23AP39. To our knowledge, this is the first report of a CNV in the ADGRL3 gene, and its association with ASD in humans.
Patient
Clinical Description and Developmental History
Informed consent for publication of the clinical material has been obtained by the patient and his caregivers, respectively. This case report did not require the additional approval of the institutional ethics review board of Mariaberg e. V., since this case report is in accordance with the requirements for diagnostic purposes required by federal law in Germany (“Gendiagnostik-Gesetz”, GenDG) and does not comply with the requirements for prognostic clinical studies. Therefore, no additional approval of the institutional ethics review board had been issued. The authors declare that all procedures have been performed in accordance with the principles stated in the Declaration of Helsinki besides informed consent and anonymization. The male patient was first seen in our out-patient clinic at age 12 years 3 months, and presented with aggressive behavior, mood instability, suicidal statements, repetitive and restrictive behavior, sensitivity to noise, learning problems and dyslexia. Body height 149.0 cm (40th percentile), weight 37.2 kg (25th percentile), head circumference 54.0 cm (41st percentile). No dysmorphic signs. Development: Born at week 41+3 of gestation with body weight 4075 g, length 54 cm, head circumference 34.5 cm, APGAR 7/8/10 by Cesarean section, two days earlier minor car accident. Early motor development with problems in coordination and walking, speech development with articulation disorder and difficulties in word finding, persisting until present. Fecal soiling until first years of primary school. No fantasy play, nor role play. Somatic clinical features included fronto-temporal spikes and spike-wave patterns on EEG without signs of epilepsy, hearing loss on the left ear, and hypothyreosis.
Three siblings of 10 years, 8 years, and 6 years did not show any clinical signs. Unfortunately, parents and sibling did not consent to genetic testing, though clinically relevant and recommended by the genetic counselor.
A treatment with MPH with a maximum of 70 mg per day increased symptoms and showed adverse effects, such as loss of appetite, weight loss, irritability, agitation, and increased emotional instability with periods of whining, thus we recommended the withdrawal of MPH and starting a neuroleptic medication with 3 mg of aripiprazole per day orally. Under this medication, the patient showed less frequent aggression, milder episodes, and the ability for increased self-regulation. Reducing group size in school and therapy improved the interaction of the patient with his peers, parents, and teachers.
Neuropsychological Testing
Neuropsychological testing using the Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV)14 resulted in the following standard values: Verbal Comprehension Index (VCI) 110, Perceptual Reasoning Index (PRI) 121, Working Memory Index (WMI) 102, and Processing Speed Index (PSI) 86, and Full Scale IQ (FSIQ) 110. Autism-related testing included the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2),15 module 3, revealed autism based on a social affect score of 9 and a restricted and repetitive behaviors score of 4. The Autism Related Interview, Revised (ADI-R),16 interviewing the parents, resulted in the following scores: reciprocal social interactions 15 (cut-off: 10), language and communication 18 (cut-off: 8), restricted, repetitive and stereotyped behaviors and interests 3 (cut-off: 3), abnormal development until the age of 36 months 3 (cut-off: 1). The Marburg Rating Scale for the Asperger Syndrome (MBAS)17 was positive with a score of 109 (cut-off: 103).
The Child Behavioral Checklist (CBCL/6-18R)18 revealed high T-values in the scales Anxious/Depressed (T = 87), Social Problems (T = 96), Thought, Sleep, and Repetitive Problems (T = 75), Attention Problems (T = 79), and Aggressive Behavior (T = 76). The Youth Self Report (YSR/11-18R)18 reported high T-values in the scales Anxious/Depressed (T = 72), Withdrawn/Depressed (T = 79), Somatic Complaints (T = 84), Social Problems (T = 81), Thought, Sleep, and Repetitive Problems (T = 70), Attention Problems (T = 84), and Aggressive Behavior (T = 74). The Teacher’s Report Form (TRF/6-18R)18 reported high values in the scales Somatic Complaints and Aggressive Behavior (no T-values available).
The Diagnostic System for Mental Disorders in Childhood and Adolescence, Second Edition (DISYPS-II)19 reported clinically significant symptom scales in ADHD, depression, and anxiety. Scales for conduct disorder and severe developmental disorders were in the sub-threshold region. The Five-to-Fifteen (FTF) questionnaire20 for the assessment of ADHD and comorbid conditions revealed problems in motor skills (both gross and fine motor skills), executive functions (attention, hyperactive/impulsive, planning and organizing), perception (body perception, visual perception), language, learning (reading/writing, coping in learning), social skills, and emotional/behavioral problems.
Materials and Methods
CNV Analysis
Genetic testing was performed at age 13 years 7 months. In this study, we used the Agilent Human Genome CGH Sureprint G3 180k Oligo Microarray (Agilent, Waldbronn, Germany) for CNV analysis. This array contains about 180,000 gene probes of the human genome with a resolution of about 100 kb. The microarray experiment was conducted by CeGaT (Tübingen, Germany) according to the manufacturer’s protocol. Genes involved in the CNVs detected from this study were annotated according to the human reference genome hg19 (GRCh37).
Chromosome Analysis
Chromosome analysis was carried out by GTG (G-bands by trypsin using Giemsa)-banding of 5 metaphases using standard protocols. In total, 15 metaphases had been counted with a minimum of 400 bands per haploid karyotype.
Results
Chromosome Analysis
Chromosome analysis revealed a male karyotype of 46, XY. No structural chromosome abnormalities had been found.
Array CGH Analysis
Array CGH analysis found a total of two CNVs, classified as variants of unknown significance (VUS) (Figure 1). The first CNV was found as interstitial duplication of 3 copies at chromosome 3p26.3, starting from nucleotide position 1,515,856 and ending at nucleotide position 1,840,338, with a minimal total size of 324 kb. Using the UCSC Genome Browser21 (https://genome-euro.ucsc.edu/cgi-bin/hgGateway), two pseudogenes have been annotated in this region, representing non-protein coding genes or gene fragments. The first is named AC090043.1 (Ensembl ENSG00000184423.5), with genomic coordinates chr3:1,637,461–1,637,929. The second is named ribosomal protein L23a pseudogene 39 (RPL23AP39) (Ensembl ENSG00000214074), with genomic coordinates chr3:1,771,754–1,772,158.
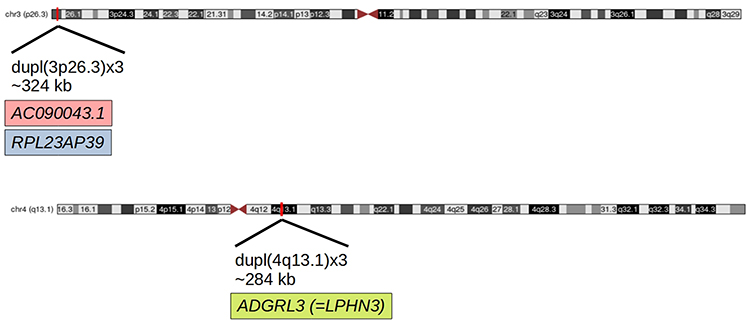 |
Figure 1 Representations of the findings of two CNVs on chromosomes 3p26.3 and 4q13.1 in the 12-year-old male patient. |
The second CNV was found as interstitial duplication of 3 copies at chromosome 4q13.1, starting from nucleotide position 62,241,702 and ending at nucleotide position 62,525,578, with a total size of 284 kb. Using the UCSC Genome Browser21 (https://genome-euro.ucsc.edu/cgi-bin/hgGateway) and the DECIPHER22 (https://www.deciphergenomics.org), this CNV contains the ADGRL3 gene (Adhesion G Protein-Coupled Receptor L3, old name: LPHN3, latrophilin 3).
Bioinformatics and Database Search
In the EVIDENCE database,23 we found 15 pathogenic, 20,110 VUS, and 426 likely benign entries for ADGLR3 (https://3billion.io/gene/ADGRL3/). Of these, phenotype entries for 14 patients have been reported in the following classes with the respective frequencies: Abnormalities of the nervous system 57.1%, abnormalities of head or neck 42.9%, abnormalities of the musculoskeletal system 28.6%, abnormalities of the cardiovascular system 14.3%, abnormalities of the eye 14.3%, constitutional symptoms 7.1%, and growth abnormalities 7.1%.
Using the ClinVar database24 (https://www.ncbi.nlm.nih.gov/clinvar/?term=ADGRL3%5Bgene%5D), we found 15 pathogenic, 1 likely pathogenic, 10 VUS, and 4 likely benign entries for ADGLR3. For the other CNV on 3p26.3, the only entry in the ClinVar database is the one of our group (https://www.ncbi.nlm.nih.gov/clinvar/variation/624500/?oq=1515856-1840338andm=GRCh37%2Fhg19±3p26.3(chr3:1515856-1840338)x3#id_first).
No entries for both CNVs have been found in the gnomAD database for the control population nor in the Geno2MP database for a disease population.25
Discussion
CNVs on 3p26.3 and 4q13.1
In this case report, we describe a male patient, presenting in our outpatient clinic at the age of 12 years and 3 months with signs both of ASD and ADHD. Genetic testing revealed two CNVs, one duplication of 324 kb on chromosome 3p26.3, with pseudogenes AC090043.1 and RPL23AP39, whereas the other duplication of 284 kb on chromosome 4q13.1 contains ADGRL3. The coding region of ADGRL3 encompasses the position chr4:62,363,012–62,599,271, a total of 236 kb in 6 exons. In our findings, the duplication is located on chr4:62,241,702–62,525,578, thus starting in front of the coding region. With regard to the other CNV on 3p26.3, there is no information available on the regulation, or function, of the pseudogenes.
With regard to CNVs in ADGLR3, the DECIPHER database22 reports a total of 22 entries, of which 13 contain a deletion (59%) and 9 contain a duplication (41%). One patient showed hyperactivity, whereas ASD was not reported. With regard to CNVs in RPL23AP39, a total of 194 entries have been described, of which one patient showed hyperactivity, and six patients showed autism-related symptoms. With regard to CNVs in the pseudogene AC090043.1, no entries have been found in the DECIPHER database.
Double-Diagnosis of ASD and ADHD in the Patient
Until recently, the combined diagnosis of ADHD and ASD was not regarded as appropriate in children,26 a broader discussion led to more and more combined diagnoses of ADHD and ASD, since both were regarded as neurodevelopmental disorders, both in DSM-5,27 as well as in ICD-11.28 In the patient described in our study, diagnostic criteria were met for both ADHD and ASD, thus we followed the recommendation of a combined diagnosis. In a first approach, we recommended MPH treatment, aiming at the reduction of ADHD symptoms, mainly hyperactivity and impulsivity. In animal models, several studies have shown that MPH reduced hyperactivity and impulsivity in zebrafish loss-of-function mutants for the LPHN3 ortholog lphn3.1,29,30 but with regard to our patient, MPH treatment increased ADHD symptoms. Thus, besides standard treatment options including cognitive behavioral therapy, we recommended neuroleptic treatment with the atypical antipsychotic drug aripiprazole in a pragmatic approach, since treatment with MPH resulted in more frequent and severe aggressive behavior. Of note, although there is an empirical recommendation for the use of aripiprazole for irritability in children with ASD,31 this treatment must be regarded as “off-label” use, since there is no general approval by the respective regulatory authority in Germany for the use of aripiprazole in ASD in minors. In our clinical follow-up, we evaluated the pharmacological treatment as supportive for the patient, allowing him to participate in school and family activities.
ADGRL3 in ADHD and ASD
ADGRL3 (old name: LPHN3) belongs to the family of latrophilins, a family of adhesion GPCRs located at the postsynaptic membrane, and involved in synaptic assembly and transmission.11 ADGRL3 has been associated by linkage analysis in ADHD patients.9,32,33 It has been shown that ADGRL3 expression was decreased in ADHD patients by up to 40%,10 but the molecular mechanisms remain unclear. It has been speculated that dopamine transmission is one of the major actors.34,35 No information about the function of ADGRL3 in ASD is available.
Support for the Double-Hit Hypothesis of ASD?
A number of variants in single genes have been identified in ASD, but there remain questions about the complex inheritance patterns of ASD.36 Several studies did not only identify a single CNV in ASD patients, but several, leading to a “two-hit”, or “multiple hit” model of ASD.36–38 Of note, not only CNVs contribute to the “two-hit” model, but also other influences of greater significance, such as drug use in pregnancy,39 or “adolescence”40 in general. In the latter study, the authors identified social processes, humoral changes, and neuronal re-organization in transition from childhood into adulthood not only as risk factors, but as actual noxious agent as the second hit to a vulnerable adolescent brain impaired by neurodevelopmental structural damage as the first hit.40 In this context, we prefer to use the term “two-hit model” only with regard to genetic alterations, in similarity to the two-hit model of carcinogenesis.41 A major limitation of our study is that we cannot provide genetic data on parents and siblings of the patient, since they did not consent to genetic testing. Thus, we can only speculate on factors such as the penetrance of the observed CNVs, as well as the influence of the combination of both. ASD is regarded as multifactorial disorder with contributions both from genetic and environmental influences.42 However, the unknown genetic information on parents and siblings limit the evaluation of genetic and environmental interactions (GxE) and therefore the power of this study.
Conclusion
In the present study, we describe the finding of two CNVs in a patient presenting with ASD and ADHD symptoms. Whereas one of the CNVs in the ADGRL3 region on chromosome 4q13.1 has been linked to ADHD and SUD, no evidence has been reported that ADGRL3 may also be involved in ASD. With regard to the second CNV on chromosome 3p26.3, involving the two pseudogenes AC090043.1 and RPL23AP39, no information about their regulation, or function, is available. Whereas a single CNV, the one on 3p26.3, or on 4q13.1 by itself, may not be sufficient to evoke ASD symptoms, the combination of the two add to the full spectrum of ASD. On the other hand, and this is the main limitation of our findings, we cannot rule out that there is a different explanation of ASD in the patient described in the present study, such as an undetected additional genetic variant, or a non-genetic cause of ASD in this patient.
Abbreviations
ADGRL3, Adhesion G protein-coupled receptor L3; ADHD, attention deficit hyperactivity disorder; ADI-R, Autism Related Interview, Revised; ADOS-2, Autism Diagnostic Observation Schedule, Second Edition; Array-CGH, Array-based Comparative Genomic Hybridization; ASD, autism spectrum disorder; bp, base pairs; CNV, copy number variant; EEG; electroencephalography, FSIQ, Full Scale IQ; GPCR, G protein coupled receptor; GTG, G-bands by trypsin using Giemsa; kb, kilobases; LPHN3, latrophilin-3; MBAS, Marburg Rating Scale for the Asperger Syndrome; MPH, methylphenidate; PRI, Perceptual Reasoning Index; PSI, Processing Speed Index; SNP, single nucleotide polymorphism; VCI, Verbal Comprehension Index; VUS, variants of unknown significance; WISC-IV, Wechsler Intelligence Scale for Children, Fourth Edition; WMI, Working Memory Index.
Disclosure
Prof. Dr. Martin Maurer reports grants, personal fees, non-financial support from Ärztliche Akademie für Psychotherapie von Kindern und Jugendlichen e. V., outside the submitted work; In addition, Prof. Dr. Martin Maurer has a patent WO03035684A1 licensed to Axaron Bioscience, a patent WO03076950A2 licensed to Axaron Bioscience, a patent WO2005063966A2 licensed to Axaron Bioscience, a patent WO2006008582A1 licensed to Sygnis Bioscience, a patent WO2006048298A1 licensed to University of Heidelberg; and held shares of the biotech companies Sygnis Bioscience, and Qiagen, within the last 36 months prior to publication. The authors report no other conflicts of interest in this work.
References
1. Dalla Vecchia E, Mortimer N, Palladino VS, et al. Cross-species models of attention-deficit/hyperactivity disorder and autism spectrum disorder: lessons from CNTNAP2, ADGRL3, and PARK2. Psychiatr Genet. 2019;29(1):1–17. doi:10.1097/ypg.0000000000000211
2. Rosenfeld JA, Ballif BC, Torchia BS, et al. Copy number variations associated with autism spectrum disorders contribute to a spectrum of neurodevelopmental disorders. Genet Med. 2010;12(11):694–702. doi:10.1097/GIM.0b013e3181f0c5f3
3. Rylaarsdam L, Guemez-Gamboa A. Genetic causes and modifiers of autism spectrum disorder. Front Cell Neurosci. 2019;13:385. doi:10.3389/fncel.2019.00385
4. Walker S, Scherer SW. Identification of candidate intergenic risk loci in autism spectrum disorder. BMC Genomics. 2013;14:499. doi:10.1186/1471-2164-14-499
5. Nisar S, Bhat AA, Masoodi T, et al. Genetics of glutamate and its receptors in autism spectrum disorder. Mol Psychiatry. 2022;27(5):2380–2392. doi:10.1038/s41380-022-01506-w
6. Almandil NB, AlSulaiman A, Aldakeel SA, et al. Integration of transcriptome and exome genotyping identifies significant variants with autism spectrum disorder. Pharmaceuticals. 2022;15(2). doi:10.3390/ph15020158
7. Maurer MH. Genomic and proteomic advances in autism research. Electrophoresis. 2012;33(24):3653–3658. doi:10.1002/elps.201200382
8. Kappel DB, Schuch JB, Rovaris DL, et al. ADGRL3 rs6551665 as a common vulnerability factor underlying attention-deficit/hyperactivity disorder and autism spectrum disorder. Neuromolecular Med. 2019;21(1):60–67. doi:10.1007/s12017-019-08525-x
9. Arcos-Burgos M, Jain M, Acosta MT, et al. A common variant of the latrophilin 3 gene, LPHN3, confers susceptibility to ADHD and predicts effectiveness of stimulant medication. Mol Psychiatry. 2010;15(11):1053–1066. doi:10.1038/mp.2010.6
10. Martinez AF, Abe Y, Hong S, et al. An ultraconserved brain-specific enhancer within ADGRL3 (LPHN3) underpins attention-deficit/hyperactivity disorder susceptibility. Biol Psychiatry. 2016;80(12):943–954. doi:10.1016/j.biopsych.2016.06.026
11. Südhof TC. Synaptic neurexin complexes: a molecular code for the logic of neural circuits. Cell. 2017;171(4):745–769. doi:10.1016/j.cell.2017.10.024
12. Lange M, Froc C, Grunwald H, Norton WHJ, Bally-Cuif L. Pharmacological analysis of zebrafish lphn3.1 morphant larvae suggests that saturated dopaminergic signaling could underlie the ADHD-like locomotor hyperactivity. Prog Neuropsychopharmacol Biol Psychiatry. 2018;84(PtA):181–189. doi:10.1016/j.pnpbp.2018.02.010
13. Orsini CA, Setlow B, DeJesus M, et al. Behavioral and transcriptomic profiling of mice null for Lphn3, a gene implicated in ADHD and addiction. Mol Genet Genomic Med. 2016;4(3):322–343. doi:10.1002/mgg3.207
14. Petermann F, Petermann U. Wechsler Intelligence Scale for Children.
15. Poustka L, Rühl D, Feineis-Matthews S, Poustka F, Hartung M, Bölte S. [Autism Diagnostic Observation Schedule - 2, German version].Diagnostische Beobachtungsskala für Autistische Störungen - 2.
16. Bölte S, Poustka F, Rühl D, Schmötzer G. [Autism Diagnostic Interview - Revised, German version]. Diagnostisches Interview für Autismus - Revidiert. Hogrefe; 2006.
17. Kamp-Becker I, Remschmidt H. [MBAS – Marburg Rating Scale for Asperger's Syndrome]. MBAS – Marburger Beurteilungsskala zum Asperger-Syndrom. In: Remschmidt H, Kamp-Becker I, editors. Asperger-Syndrom. Springer; 2006:241–254.
18. Döpfner M, Plück J, Kinnen C. [German School Age Form of the Child Behavior Checklist of Thomas M. Achenbach. Parent's version for the questionnaire about the behavior of children and adolescents (CBCL/6-18R), teacher's version for the questionnaire about the behavior of children and adolescents (TRF/6-18R), adolescent version of the questionnaire (YSR/11-18R)]. Deutsche Schulalter-formen der Child Behavior Checklist von Thomas M. Achenbach. Elternfragebogen über das Verhalten von Kindern und Jugendlichen (CBCL/6-18R), Lehrerfragebogen über das Verhalten von Kindern und Jugendlichen (TRF/6-18R), Fragebogen für Jugendliche (YSR/11-18R). Hogrefe; 2014.
19. Döpfner M, Görtz-Dorten A, Lehmkuhl G. [Diagnostic System for mental diseases according to ICD-10 and DSM-IV for children and adolescents]. Diagnostik-System für psychische Störungen nach ICD-10 und DSM-IV für Kinder und Jugendliche - II (DISYPS-II). Hogrefe; 2008.
20. Kadesjö B, Janols LO, Korkman M, et al. The FTF (Five to Fifteen): the development of a parent questionnaire for the assessment of ADHD and comorbid conditions. Eur Child Adolesc Psychiatry. 2004;13(Suppl 3):3–13. doi:10.1007/s00787-004-3002-2
21. Kent WJ, Sugnet CW, Furey TS, et al. The human genome browser at UCSC. Genome Res. 2002;12(6):996–1006. doi:10.1101/gr.229102
22. Firth HV, Richards SM, Bevan AP, et al. DECIPHER: database of chromosomal imbalance and phenotype in humans using ensembl resources. Am J Hum Genet. 2009;84(4):524–533. doi:10.1016/j.ajhg.2009.03.010
23. Seo GH, Kim T, Park J-Y, et al. Pilot study of EVIDENCE: high diagnostic yield and clinical utility of whole exome sequencing using an automated interpretation system for patients with suspected genetic disorders. bioRxiv. 2019:628438. doi:10.1101/62843
24. Landrum MJ, Lee JM, Riley GR, et al. ClinVar: public archive of relationships among sequence variation and human phenotype. Nucleic Acids Res. 2014;42:D980–5. doi:10.1093/nar/gkt1113
25. Wang J, Al-Ouran R, Hu Y, et al. MARRVEL: integration of human and model organism genetic resources to facilitate functional annotation of the human genome. Am J Hum Genet. 2017;100(6):843–853. doi:10.1016/j.ajhg.2017.04.010
26. Rommelse N, Visser J, Hartman C. Differentiating between ADHD and ASD in childhood: some directions for practitioners. Eur Child Adolesc Psychiatry. 2018;27(6):679–681. doi:10.1007/s00787-018-1165-5
27. American Psychiatric Association, American Psychiatric Association. DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
28. World Health Organization. International classification of diseases for mortality and morbidity statistics (11th Revision); 2021. Available from: https://icd.who.int/browse11/l-m/en.
29. Lange M, Norton W, Coolen M, et al. The ADHD-linked gene Lphn3.1 controls locomotor activity and impulsivity in zebrafish. Mol Psychiatry. 2012;17(9):855. doi:10.1038/mp.2012.119
30. Lange M, Norton W, Coolen M, et al. The ADHD-susceptibility gene lphn3.1 modulates dopaminergic neuron formation and locomotor activity during zebrafish development. Mol Psychiatry. 2012;17(9):946–954. doi:10.1038/mp.2012.29
31. Hirsch LE, Pringsheim T. Aripiprazole for autism spectrum disorders (ASD). Cochrane Database Syst Rev. 2016;(6):CD009043. doi:10.1002/14651858.CD009043.pub3
32. Bruxel EM, Salatino-Oliveira A, Akutagava-Martins GC, et al. LPHN3 and attention-deficit/hyperactivity disorder: a susceptibility and pharmacogenetic study. Genes Brain Behav. 2015;14(5):419–427. doi:10.1111/gbb.12224
33. Ribasés M, Ramos-Quiroga JA, Sánchez-Mora C, et al. Contribution of LPHN3 to the genetic susceptibility to ADHD in adulthood: a replication study. Genes Brain Behav. 2011;10(2):149–157. doi:10.1111/j.1601-183X.2010.00649.x
34. Gomez-Sanchez CI, Carballo JJ, Riveiro-Alvarez R, et al. Pharmacogenetics of methylphenidate in childhood attention-deficit/hyperactivity disorder: long-term effects. Sci Rep. 2017;7(1):10391. doi:10.1038/s41598-017-10912-y
35. Mathiasen S, Palmisano T, Perry NA, et al. G12/13 is activated by acute tethered agonist exposure in the adhesion GPCR ADGRL3. Nat Chem Biol. 2020;16(12):1343–1350. doi:10.1038/s41589-020-0617-7
36. Leblond CS, Heinrich J, Delorme R, et al. Genetic and functional analyses of SHANK2 mutations suggest a multiple hit model of autism spectrum disorders. PLoS Genet. 2012;8(2):e1002521. doi:10.1371/journal.pgen.1002521
37. Gau SS, Liao HM, Hong CC, Chien WH, Chen CH. Identification of two inherited copy number variants in a male with autism supports two-hit and compound heterozygosity models of autism. Am J Med Genet B Neuropsychiatr Genet. 2012;159(6):710–717. doi:10.1002/ajmg.b.32074
38. Guo H, Duyzend MH, Coe BP, et al. Genome sequencing identifies multiple deleterious variants in autism patients with more severe phenotypes. Genet Med. 2019;21(7):1611–1620. doi:10.1038/s41436-018-0380-2
39. Ackerman S, Schoenbrun S, Hudac C, Bernier R. Interactive effects of prenatal antidepressant exposure and likely gene disrupting mutations on the severity of autism spectrum disorder. J Autism Dev Disord. 2017;47(11):3489–3496. doi:10.1007/s10803-017-3246-6
40. Picci G, Scherf KS. A two-hit model of autism: adolescence as the second hit. Clin Psychol Sci. 2015;3(3):349–371. doi:10.1177/2167702614540646
41. Knudson AG
42. Almandil NB, Alkuroud DN, AbdulAzeez S, AlSulaiman A, Elaissari A, Borgio JF. Environmental and genetic factors in autism spectrum disorders: special emphasis on data from Arabian studies. Int J Environ Res Public Health. 2019;16(4). doi:10.3390/ijerph16040658
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.