Back to Journals » Patient Preference and Adherence » Volume 20
Caregivers’ Preference for Antipsychotic Medication for Youth Less Than 18 Years-Old: A Discrete Choice Experiment Pilot
Authors Fu YH, Bozzi LM, Butler B, dosReis S ![]()
Received 27 February 2026
Accepted for publication 14 May 2026
Published 30 May 2026 Volume 2026:20 605661
DOI https://doi.org/10.2147/PPA.S605661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yu-Hua Fu,1 Laura M Bozzi,1 Beverly Butler,2 Susan dosReis1,3
1Department of Practice, Sciences, and Health Outcomes Research, University of Maryland Baltimore, School of Pharmacy, Baltimore, MD, USA; 2Swats, LLC, Manchester, MD, USA; 3PAVE Center, University of Maryland Baltimore, School of Pharmacy, Baltimore, MD, USA
Correspondence: Susan dosReis, Department of Practice, Sciences, and Health Outcomes Research, University of Maryland School of Pharmacy, 220 North Arch Street, 12th Floor, Baltimore, MD, 21201, USA, Email [email protected]
Background: Antipsychotics are often prescribed for youth with complex mental health conditions but carry risks of metabolic adverse effects. Caregivers play a key role in weighing the potential benefit of treating the underlying mental health condition with the potential risk of side effects.
Objective: To evaluate caregivers’ preferences for the benefits and risks of antipsychotic medication for their child and to assess how these preferences relate to treatment acceptability.
Methods: We recruited 26 caregivers of youth < 18 years-old across the greater Baltimore region to pilot test a discrete choice experiment (DCE). The DCE included nine choice tasks, each with three profiles and six attributes per profile, with three for the risks (weight gain, diabetes, cholesterol) and three for the benefits (self-harm episodes, aggressive behavior, hospitalizations) of antipsychotics. For each choice task, participants first selected the most acceptable profile; second, indicated if they would use their chosen profile. Conditional logit models estimated part-worth utilities. We calculated the relative attribute importance and assessed trade-offs between attributes. Summing the part-worth utilities for attributes within each DCE profile, we identified profiles with the largest utility and assessed the acceptance of the profile chosen.
Results: Participants were, on average, 44 years-old; 76% were biological mothers. Nearly half of the youth (46%) had prior psychiatric hospitalization, 70% had aggression towards property, and 90% had aggression towards others. Reduction in hospitalizations (34%), days with aggressive behavior (22%), and self-harm episodes (15%) achieved greater relative importance than diabetes risk (14%), weight gain (11%), and high cholesterol (4%). Participants accepted 2.21 hospitalizations per year to reduce diabetes risk from four-fold to two-fold. Sixty-five percent of the profiles selected were those participants would use.
Conclusion: Prioritizing outcomes over the antipsychotic metabolic adverse effects underscores the importance of eliciting caregiver preferences for the benefits and risks of medication.
Plain Language Summary: This preference survey study asked caregivers of a child who may have been treated with an antipsychotic medication to consider the benefits and risks of the medication. Six attributes of the medication that caregivers considered included the benefits of reductions in hospitalizations, aggressive behavior, and self-harm along with the risks of weight gain, diabetes, and high cholesterol. The most important attributes when choosing an antipsychotic medication for their child were hospitalizations and the number of days without aggressive behavior, suggesting caregivers are willing to accept the adverse effects of antipsychotic medications to achieve these outcomes.
Keywords: antipsychotic, child mental health, discrete choice experiment, caregiver preference, benefit–risk
Introduction
Mental and developmental disorders affected an estimated 27.7% of children aged 3 to 17 in the United States in 2021 and the past decade has witnessed a steady increase in their incidence and prevalence.1–3 These conditions are linked to poor short- and long- term health and social outcomes, including poor overall physical health, more chronic diseases, lower educational attainment, reduced economic stability, and challenges transitioning into adulthood.4 Psychotropic medications are frequently considered first-line treatments for managing many of these disorders.5
Aggressive behavior among youth with mental and developmental disorders often requires pharmacologic intervention.6,7 Antipsychotic medications are commonly used to manage aggression in youth, but they are associated with metabolic adverse events. Youth can gain 7% or more of their body weight in the first six weeks of treatment.8 Other studies have reported a twofold increase in obesity, a threefold increase in type 2 diabetes, and nearly threefold higher odds of developing cardiovascular conditions among youth prescribed antipsychotics compared with those not treated with psychotropic medications.9–11
Decisions to initiate an antipsychotic medication for a youth require caregivers to weigh the potential benefits against the potential adverse effects. Understanding trade-offs among the benefits and risks is crucial for supporting patient-centered informed decision-making and enhancing treatment satisfaction, which can ultimately lead to better adherence and the promotion of safe and effective antipsychotic use in pediatric mental health care.12,13 Studies in adult samples have shown that caregiver preferences and tolerability for antipsychotic side effects affect willingness to initiate treatment.14 Among caregivers of adult patients, hospitalization and symptom improvement are important factors in initiating antipsychotic treatment.15 To date, there have been no investigations into caregiver preferences for initiating an antipsychotic medication for their child.
To address this gap, we developed a discrete choice experiment (DCE) to examine how caregivers navigate these complex decisions. While the origin of DCEs emerged from health economics,16 this method is applicable for healthcare decision making.17 Importantly, stakeholder engagement in DCEs is also growing as a method to enhance implementation of effective healthcare interventions.18 We implemented a stakeholder-engaged approach to identify the key attributes of antipsychotics that caregivers consider when making decisions to use this medication for their child with mental and developmental disabilities. We sought to answer the question, “Do caregivers prioritize the medication benefits over the risks associated with antipsychotic use?” The goals of this pilot study were to assess the relative importance of the attributes of antipsychotic benefits and risks among caregivers who were considering treatment for a youth and to identify trade-offs among these attributes. The findings are intended to enable broader application of our DCE to inform patient-centered decision-making for antipsychotic medication treatment in youth.
Methods
Attribute Selection
The attributes and corresponding levels were identified through a structured and iterative process that integrated data from qualitative interviews, a targeted literature review, and stakeholder-engaged feedback via focus groups. We conducted a secondary analysis of transcribed 1:1 in-depth interviews with caregivers of a child who had a mental health condition and a developmental disability, which were part of a grant funded by the Patient Centered Outcomes Research Institute.19 The qualitative interviews were analyzed for caregiver-identified outcomes that they hoped to achieve by using an antipsychotic medication for their child. Three domains emerged from the qualitative interviews: efficacy of managing aggressive behavior towards self, others, and property; the impact of residential placement on medication complexity; distance to a provider for medication management. We reviewed the literature to identify the key side effects of weight gain, risk of type 2 diabetes, and risk of high cholesterol. The authors (BB and SDR) synthesized the data from the qualitative interviews with the information from the literature review to identify nine attributes: weight gain, diabetes risk, high cholesterol risk, aggression towards self, aggression towards others, verbal aggression, impact of residential placement on medication use, number of hospitalizations per year, and distance to a provider. To refine the attributes and levels, two authors (BB and SDR) conducted a focus group with eight caregivers of a child who had been prescribed an antipsychotic. Based on their feedback, we omitted two attributes (i.e., impact of residential placement on medication use, and distance to provider) and we retained levels that were deemed important. Aggression towards self was framed as self-harm. Aggression towards others and verbal aggression were combined as these were seen as general aggressive behavior towards others.
The final framework included six attributes, each with three levels (i.e., distinct categories representing varying magnitudes or severity of an outcome; see Figure 1A). Three attributes of the caregiver-defined benefits of the medication included the extent to which the antipsychotic reduced the number of self-harm episodes, the number of days the youth exhibited aggressive behavior, and the number of mental health-related hospitalizations. Three attributes of the risk of antipsychotic medication included weight gain, the risk of diabetes, and the risk of elevated cholesterol.8–10,20 Each attribute had three mutually exclusive levels, with lower levels reflecting a reduction in the magnitude or severity.
 |
Figure 1 Discrete choice experiment framework and example choice task. (A) presents the full list of attribute domains and corresponding attribute levels. (B) provides an example of a discrete choice experiment choice set, followed by a question asking whether the caregiver participant would use the option they selected. |
Discrete Choice Experiment (DCE) Design
The DCE was developed as an orthogonal array using SAS® macros to establish the experimental design for the choice tasks.21 We selected a full factorial, orthogonal array with 96% D-efficiency for the DCE design. There were nine choice tasks, each displayed three profiles with six attributes per profile. One level from each attribute was displayed in each profile, which resulted in all attribute levels being displayed the same number of times across all choice tasks.
In each choice task, participants were asked to review each of the three profiles and select the one that was most acceptable to them. A follow-up question after each choice task required participants to indicate whether they would use the selected option. This enabled distinguishing selections that were acceptable.
Study Sample
Participants were recruited with the assistance of one of the authors (BB) who worked with families in community clinics and organized support groups in the greater Baltimore Metropolitan Area. Eligible participants were caregivers of youth aged ≤18 years-old who had been offered or had taken an antipsychotic medication within the past 12 months. A brief telephone screen was conducted to determine eligibility for the study.
Our target sample was caregivers of youth for whom antipsychotic medication is prescribed for the management of aggression, severe mood disorders, or the irritability associated with autism. This is the population to whom our sample of youth less than 18 years old generalizes.
Survey Administration
We piloted the DCE in an online survey using the Qualtrics web-based platform. All participants provided informed consent prior to completing the online survey. After completing the survey, participants received a $20 gift card. The targeted sample size for this pilot was 30, of which 26 were enrolled, yielding a response rate of 87%.
Survey Instrument
The final survey included 60 multiple-choice questions across three sections: (1) demographic information about the caregiver (ie., age, sex, race/ethnicity, relation to the child, marital status, education, household size and income, employment status and residential community) and the child (ie, sex, race/ethnicity, school grade), (2) current care management for the child, (3) clinical characteristics (i.e., speech impairment, aggressive behaviors, mental health diagnoses, psychotropic medication, and mental health or behavior care), and (4) the DCE. An example of the DCE choice task is shown in Figure 1B. We followed the established checklist for reporting DCE in health (Supplementary Material 1).22 A copy of the survey is available in Supplementary Material 2.
Statistical Analysis
Completed surveys were downloaded as an Excel file and converted to a SAS® dataset. Descriptive statistics were used to summarize demographic characteristics of the participants and their children. A conditional logit regression estimated the part-worth utilities and 95% confidence intervals (CI) from the DCE responses. Part-worth utilities with positive values above zero reflect desirable attributes and negative values below zero reflect undesirable attributes. We used established methods to quantify the relative attribute importance using the min-max difference and to estimate the benefit-risk trade-offs.23–25 Responses to the follow-up question were analyzed to identify the selected profiles that participants indicated they would use. We summed the part-worth utilities across all attributes in the profile and ranked the profiles from the highest to the lowest.26 We evaluated the attribute levels and total utility in the profiles selected as acceptable All data were analyzed using SAS® 9.4 (Carey, NC) and STATA 14.
Results
Characteristics of Participants and Their Child
The demographic characteristics of the 26 participants and their child are presented in Table 1. Participants had a mean age of 44 years, were predominantly biological mothers (77.0%), and 38.4% of the sample comprised single-parent households. The majority was employed (73.1%), had a college degree (77.0%), and resided in a suburban community (84.6%).
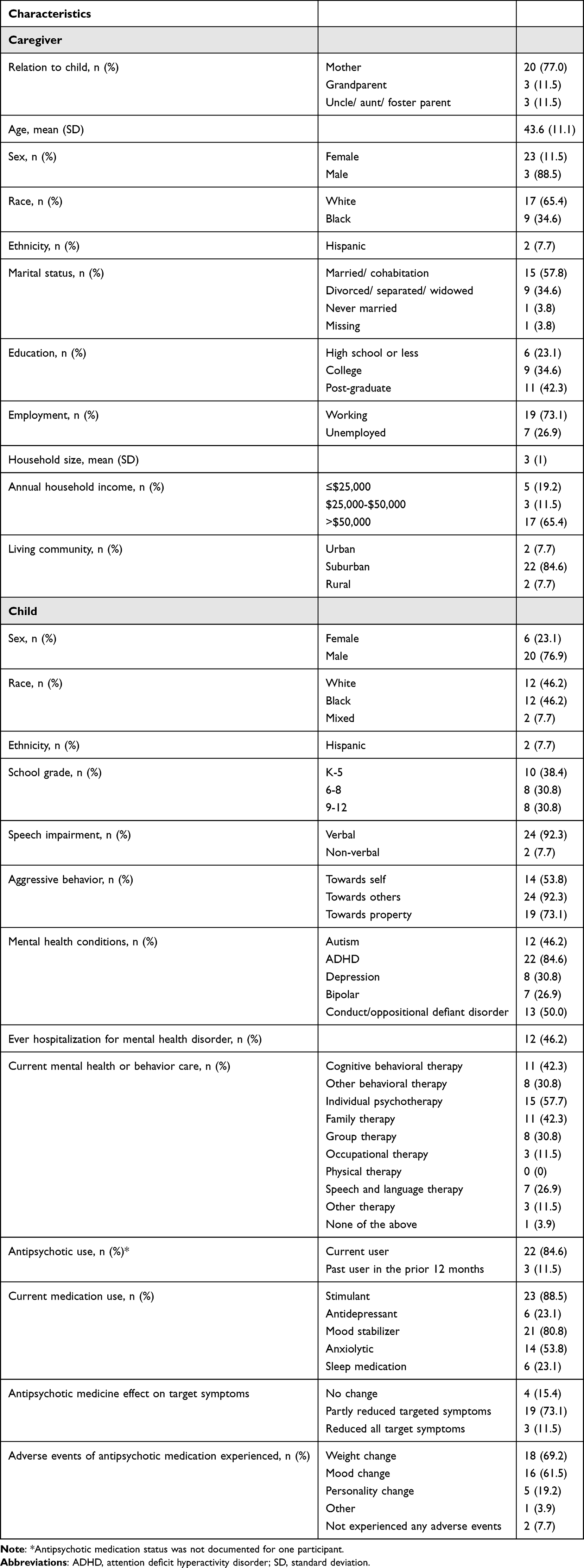 |
Table 1 Characteristics of Study Sample of Caregivers and Their Child |
Nearly 80% of the children were male and 69.2% were in grades K through 8. The most common diagnosis was attention-deficit/hyperactivity disorder (ADHD; 84.6%) and 46.2% had an autism spectrum disorder. Most of the children exhibited aggressive behavior.
The most reported mental health or behavioral therapy was individual psychotherapy (57.7%), followed by family therapy (42.3%) and cognitive behavioral therapy (42.3%). Most youth (84.6%) were currently taking an antipsychotic, and 11.5% had used the medication in the past year (Table 1). All caregivers indicated that their child was taking other psychotropic medications. Specifically, most youth also were taking stimulants (88.5%) and mood stabilizers (80.8%). There were 69.2% of participants who reported weight gain in their child following antipsychotic use, and 61.5% noted mood changes. Many (73.1%) indicated that targeted symptoms were only partially reduced, while 15.4% observed no improvement at all.
Preferences for Attributes of Antipsychotic Medication
The part-worth utilities, also referred to as preference weights, for each level across attributes are displayed in Figure 2. The utility values decreased as weight gain, diabetes risk, self-harm episodes, and hospitalizations increased. Negative preferences for weight gain of 20 pounds or more plateaued with little change in the part-worth utility. Cholesterol risk had little impact on preferences with part-worth utilities around zero.
 |
Figure 2 Part-worth utilities and 95% confidence intervals for attribute levels by attribute. |
The relative attribute importance is shown in Figure 3. Participants prioritized the potential benefits of antipsychotics (i.e., hospitalizations (34%), days without aggressive behaviors (22%), and self-harm episodes (15%)) over the potential risks (i.e., diabetes risk (14%), weight gain (11%), and high cholesterol (4%)). Estimating trade-offs between attributes, participants would accept 2.21 hospitalizations per year in exchange for a decrease from four-fold to double the risk of diabetes.
 |
Figure 3 Relative attribute importance of antipsychotic medication in caregiver decision-making for their child (n=26). |
Acceptance of Selected Antipsychotic Profiles
We summed the part-worth utilities for all attributes in the profile to obtain the total profile utility. Table 2 summarizes the nine top-ranked choice task profiles from the DCE based on the total utility. The acceptance percentage reflects the proportion of participants who selected the profile that indicated they would use the profile. The most acceptable profile (65.4%) included the lowest risk of weight gain, diabetes, self-harm, and hospitalizations and the most days without aggressive behavior. Profiles that participants indicated they would follow included the maximum days without aggressive behavior, but variable weight gain (10–20 pounds) and diabetes risk. A considerable proportion (42.3%) would use a profile with 30-pound weight gain, three-fold risk of diabetes, and 15% risk of elevated cholesterol in exchange for four days per week without aggressive behavior.
 |
Table 2 Total Utility and Attributes for the Nine Most Acceptable Profiles |
Discussion
This pilot study assessed caregivers’ preferences for using an antipsychotic medication for their child, providing valuable insight into caregivers’ consideration of the benefits and risks when making treatment decisions. We aimed to determine if caregivers prioritize the benefits of antipsychotic medication over the risks when considering antipsychotic treatment for their youth with mental and behavioral disorders. Our study found that the patient-informed benefits of antipsychotic medications had a higher relative importance than the risks of these medications. Specifically, the most important attributes when choosing an antipsychotic medication for their child were hospitalizations and the number of days without aggressive behavior. Preference for one hospitalization and four days per week without aggressive behavior were consistent across all analyses, with strong part-worth utility, high relative importance, and contribution to the most acceptable profiles. This suggests that caregivers are willing to accept the adverse metabolic effects of antipsychotic medications to achieve these outcomes.
The findings can be considered in the context of the intersection of many factors that affect adherence to antipsychotic medications. We found that reducing hospitalizations was an important factor influencing caregivers’ preference for antipsychotic medication for their child. Zhang et al similarly reported the importance of reducing hospitalizations in an adult sample.15 The effectiveness of antipsychotics in reducing hospitalizations could ultimately promote adherence. A noted barrier to treatment adherence is antipsychotic side effects,27 and we found that weight gain was tolerable to a certain extent. These findings highlight the importance of ongoing shared decision-making to ensure personalized care that can promote treatment adherence.28
It is important to acknowledge youth’s preferences and experiences with antipsychotic medication. Several qualitative studies of youth experiences with antipsychotic use found the benefits of symptom relief were countered by adverse effects on their mental and physical well-being.29,30 These findings are in contrast with our study, where caregivers prioritized the benefits over the potential risks.
The DCE was developed using a patient-engaged process to elicit outcomes that were meaningful to caregivers who considered antipsychotic medication for their child. We piloted the DCE to evaluate the sensitivity of preferences to changes in the attribute levels. Caregivers would not accept more than two hospitalizations per year or less than four days without aggressive behavior. Aggressive behaviors in youth may lead to residential or other institutional placement.31 Antipsychotic medication can minimize aggression and thereby allow youth to remain at home with their families. Thus, the importance of days without aggressive behavior relates to safety concerns and can keep families intact and youth in the community. Weight gain of more than 20 pounds was not acceptable, which suggests this was a ceiling regardless of gains in other outcomes. Despite the potential for elevated cholesterol following antipsychotic use, caregivers’ preferences were not impacted by changes in this risk. It is possibly due to the limited research showing a consistent finding on cholesterol risk.10,20
Research Implications
This pilot revealed that 65% of the sample would accept the profile with the highest overall utility. The fact that not all participants would accept this profile suggests that caregivers may be highly risk-averse or that the benefits were not sufficient to outweigh the risks. Aggressive behavior affects all family members and society across all settings,32–35 so it is possible that one hospitalization and four days without aggressive behavior was not enough to alleviate the disruption to others. Prior research has shown that antipsychotics have a moderate effect on reducing aggression.6 While we generated profiles using existing literature and caregiver input, the low favorability of the hypothetical profiles points to dissatisfaction with current treatment options, which could hinder long-term medication adherence.36
The predominance of males and history of aggressive behavior in the child sample align with existing literature showing that behavioral disorders are more common in boys.37 The high prevalence of aggressive behaviors and polypharmacy in this study sample highlights the complexity of managing these conditions.38,39 Given the challenges in managing complex mental health conditions, understanding caregiver preferences is critical to supporting shared decision-making and promoting long-term treatment adherence.12,40 The study findings underscore the importance of integrating caregiver preferences into treatment planning. Future research should refine DCE attribute levels to better capture benefit-risk trade-offs and align more closely with what caregivers’ value most.
Strengths and Limitations
Our study has several notable strengths. We implemented continuous stakeholder engagement through the development and piloting of the DCE. This is among the first studies to implement a DCE to quantify caregiver preferences for antipsychotic medications for their child. The two-part choice task question enabled a better understanding of the acceptance of the profiles presented. This offers a more holistic view of preferences and attempts to minimize bias in the inferences from the findings.41
This pilot study is not without limitations. Despite the focus group input on the adequacy of the level ranges, it is possible that they did not vary enough to influence choices. This was a small pilot study conducted in a single geographic location, and so the findings may not generalize to other regions. We aimed to enroll participants with lived experience in managing youth with serious mental health and developmental disabilities, as this is the target population who receives antipsychotic medication. However, we did not enroll adolescents, which is an important perspective to capture in future studies. Research in cancer and dementia show that disease severity can influence preferences;42,43 however, we were unable to measure disease severity and thus cannot evaluate whether this affected preferences. Lastly, we did not measure preferences at initiation of the antipsychotic medication; thus, participants past experiences may have affected their preferences for the choice task selections.
Conclusions
This study offers important insights into how adult caregivers evaluate the benefits and risks of an antipsychotic when deciding to initiate this medication for their child. Our findings generalize to youth with a mental health-related disorder or disability and for whom an antipsychotic medication may be indicated. Prioritization of minimizing hospitalizations and maximizing days without aggressive behavior indicated a strong emphasis on immediate and observable beneficial outcomes. The relatively low acceptance rate for profiles with the most favorable options suggests that available treatment options are not achieving the outcomes most important to caregivers. A deeper understanding of caregiver preferences can help align treatment plans with family values. Future research can build upon this work by including larger and more diverse populations and by exploring strategies to better tailor treatment options to caregiver needs and expectations.
Abbreviations
CI, confidence interval; DCE, discrete-choice experiment.
Data Sharing Statement
The survey instrument is available in Supplementary Materials, but participant-level responses cannot be released due to privacy protections.
Ethics Approval
The University of Maryland Institutional Review Board reviewed and approved this study (HP-00080094). Participants provided informed consent prior to completing the survey. This study complies with the Declaration of Helsinki.
Acknowledgments
We are grateful for the patient communities and stakeholders whose expertise and engagement were essential to making this work possible. This work was presented as an oral podium at the 2024 Annual Meeting for ISPOR - Professional Society for Health Economics and Outcomes Research (https://www.valueinhealthjournal.com/article/S1098-3015(24)00181-5/fulltext#).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
Dr Laura Bozzi reports personal fees as a current employee of Johnson & Johnson, outside the submitted work. The authors have no other competing interests to declare that are directly or indirectly related to the work submitted for publication.
References
1. Leeb RT. Trends in mental, behavioral, and developmental disorders among children and adolescents in the US, 2016–2021. Prev Chronic Dis. 2024;21. doi:10.5888/pcd21.240142
2. Cree RA, Bitsko RH, Robinson LR, et al. Health care, family, and community factors associated with mental, behavioral, and developmental disorders and poverty among children aged 2–8 years — United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(50):1377–11. doi:10.15585/mmwr.mm6750a1
3. Tkacz J, Brady BL. Increasing rate of diagnosed childhood mental illness in the United States: incidence, prevalence and costs. Public Health Pract. 2021;2:100204. doi:10.1016/j.puhip.2021.100204
4. Whitney DG, Peterson MD. US national and state-level prevalence of mental health disorders and disparities of mental health care use in children. JAMA Pediat. 2019;173:389–391. doi:10.1001/jamapediatrics.2018.5399
5. Altuwairqi Y. Trends and prevalence of psychotropic medication use in children and adolescents in the period between 2013 and 2023: a systematic review. Cureus. 2024;16:e55452. doi:10.7759/cureus.55452
6. Pappadopulos E, Woolston S, Chait A, Perkins M, Connor DF, Jensen PS. Pharmacotherapy of aggression in children and adolescents: efficacy and effect size. J Can Acad Child Adolesc Psych. 2006;15:27–39.
7. Zahrt DM, Melzer-Lange MD. Aggressive behavior in children and adolescents. Pediatrics Rev. 2011;32:325–332. doi:10.1542/pir.32-8-325
8. De Hert M, Dobbelaere M, Sheridan EM, Cohen D, Correll CU. Metabolic and endocrine adverse effects of second-generation antipsychotics in children and adolescents: a systematic review of randomized, placebo controlled trials and guidelines for clinical practice. Eur Psych. 2011;26:144–158. doi:10.1016/j.eurpsy.2010.09.011
9. Fedorowicz VJ, Fombonne E. Metabolic side effects of atypical antipsychotics in children: a literature review. J Psychopharmacol. 2005;19:533–550. doi:10.1177/0269881105056543
10. McIntyre RS, Jerrell JM. Metabolic and cardiovascular adverse events associated with antipsychotic treatment in children and adolescents. Arch Pediatrics Adolescent Med. 2008;162:929–935. doi:10.1001/archpedi.162.10.929
11. Man KKC, Shao S-C, Chang Y-C, et al. Cardiovascular and metabolic risk of antipsychotics in children and young adults: a multinational self-controlled case series study. Epidemiol Psychiatr Sci. 2021;30:e65. doi:10.1017/S2045796021000494
12. Eigenhuis E, van Buuren VEM, Boeschoten RE, Muntingh ADT, Batelaan NM, van Oppen P. The effects of patient preference on clinical outcome, satisfaction and adherence within the treatment of anxiety and depression: a meta-analysis. Clin Psychol Psychother. 2024;31:e2985. doi:10.1002/cpp.2985
13. Wilder CM, Elbogen EB, Moser LL, Swanson JW, Swartz MS. Medication preferences and adherence among individuals with severe mental illness who completed psychiatric advance directives. Psychiatr Serv. 2010;61:380–385. doi:10.1176/appi.ps.61.4.380
14. Maravic M, Birch K, Nguyen AT, Subasinghe A, Stafford E, Zacker C. Quantifying the tolerability of antipsychotic treatment-related side effects in schizophrenia: a survey study of patients and caregiver proxies. PPA. 2025;19:2821–2834. doi:10.2147/PPA.S466742
15. Zhang W, He S, Wilson L, et al. Factors influencing patient and caregiver preferences for antipsychotic treatment of schizophrenia in China: a discrete choice experiment. Patient Prefer Adherence. 2023;17:1421–1430. doi:10.2147/PPA.S403252
16. Lancsar E, Savage E. Deriving welfare measures from discrete choice experiments: inconsistency between current methods and random utility and welfare theory. Health Econ. 2004;13:901–907. doi:10.1002/hec.870
17. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making: a user’s guide. Pharmacoeconomics. 2008;26:661–677. doi:10.2165/00019053-200826080-00004
18. Salloum RG, Shenkman EA, Louviere JJ, Chambers DA. Application of discrete choice experiments to enhance stakeholder engagement as a strategy for advancing implementation: a systematic review. Implement Sci. 2017;12:140. doi:10.1186/s13012-017-0675-8
19. dosReis S, Castillo WC, Ross M, Fitz-Randolph M, Vaughn-Lee A, Butler B. Attribute development using continuous stakeholder engagement to prioritize treatment decisions: a framework for patient-centered research. Value Health. 2016;19:758–766. doi:10.1016/j.jval.2016.02.013
20. Rogdaki M, McCutcheon RA, D’Ambrosio E, et al. Comparative physiological effects of antipsychotic drugs in children and young people: a network meta-analysis. Lancet Child Adolescent Health. 2024;8:510–521. doi:10.1016/S2352-4642(24)00098-1
21. Kuhfeld WF. Marketing Research Methods in SAS. 2003.
22. Ride J, Goranitis I, Meng Y, LaBond C, Lancsar E. A reporting checklist for discrete choice experiments in health: the DIRECT checklist. Pharmacoeconomics. 2024;42:1161–1175. doi:10.1007/s40273-024-01431-6
23. de Bekker-Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21:145–172. doi:10.1002/hec.1697
24. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16:3–13. doi:10.1016/j.jval.2012.08.2223
25. Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health--a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14:403–413. doi:10.1016/j.jval.2010.11.013
26. Hauber AB, González JM, Groothuis-Oudshoorn CGM, et al. Statistical methods for the analysis of discrete choice experiments: a report of the ISPOR conjoint analysis good research practices task force. Value Health. 2016;19:300–315. doi:10.1016/j.jval.2016.04.004
27. Klein CC, Modi AC, Welge JA, et al. Adherence rates and barriers to second-generation antipsychotic medication use in youth with bipolar spectrum disorders who have overweight/obesity. J Child Adolescent Psychopharmacol. 2024;34:353–358. doi:10.1089/cap.2024.0011
28. Grünwald LM, Thompson J. Re-starting the conversation: improving shared decision making in antipsychotic prescribing. Psychosis. 2021;13:373–377. doi:10.1080/17522439.2021.1903979
29. Murphy AL, Gardner DM, Kisely S, Cooke C, Kutcher SP, Hughes J. A qualitative study of antipsychotic medication experiences of youth. J Can Acad Child Adolesc Psych. 2015;24:61–69.
30. Grey H, Lindsey L. Lived experiences of shared decision-making in young adults prescribed antipsychotics: a qualitative interview study. Int J Clin Pharm. 2026. doi:10.1007/s11096-026-02090-7
31. Rose RA, Lanier P. A longitudinal study of child maltreatment and mental health predictors of admission to psychiatric residential treatment facilities. Int J Environ Res Public Health. 2017;14:1141. doi:10.3390/ijerph14101141
32. Gopalan G, Dean-Assael K, Klingenstein K, Chacko A, McKay MM. Caregiver depression and youth disruptive behavior difficulties. Soc Work Ment Health. 2011;9:56–70. doi:10.1080/15332985.2010.494528
33. Bastiaens LJ, Bastiaens IK. Youth aggression: economic impact, causes, prevention, and treatment. Psychiatric Times. 2006;23:36.
34. Moffitt TE. Adolescence-Limited and Life-Course-Persistent Antisocial Behavior: A Developmental Taxonomy. Biosocial Theories of Crime. 2017;69–96.
35. Wesseldijk LW, Dieleman GC, van Steensel FJA, et al. Risk factors for parental psychopathology: a study in families with children or adolescents with psychopathology. Eur Child Adolesc Psychiatry. 2018;27:1575–1584. doi:10.1007/s00787-018-1156-6
36. Kalaman CR, Ibrahim N, Shaker V, et al. Parental factors associated with child or adolescent medication adherence: a systematic review. Healthcare (Basel). 2023;11:501. doi:10.3390/healthcare11040501
37. Sun H-L, He F, Rao -W-W, et al. Gender differences in behavioral and emotional problems among school children and adolescents in China: National survey findings from a comparative network perspective. Journal of Affective Disorders. 2025;369:227–233. doi:10.1016/j.jad.2024.09.067
38. O’Brien MJ, Pauls AM, Cates AM, Larson PD, Zorn AN. Psychotropic medication use and polypharmacy among children and adolescents initiating intensive behavioral therapy for severe challenging behavior. J Pediatr. 2024;271:114056. doi:10.1016/j.jpeds.2024.114056
39. Aymerich C, Bullock E, Rowe SMB, Catalan A, de PGS. Aggressive behavior in children and adolescents with bipolar spectrum disorder: a systematic review of the prevalence, associated factors, and treatment. JAACAP Open. 2025;3:42–55. doi:10.1016/j.jaacop.2024.02.009
40. Dayabandara M, Hanwella R, Ratnatunga S, Seneviratne S, Suraweera C, de Silva VA. Antipsychotic-associated weight gain: management strategies and impact on treatment adherence. Neuropsychiatr Dis Treat. 2017;13:2231–2241. doi:10.2147/NDT.S113099
41. de Corte K, Cairns J, Grieve R. Stated versus revealed preferences: an approach to reduce bias. Health Econ. 2021;30:1095–1123. doi:10.1002/hec.4246
42. Bechthold AC, Azuero A, Puga F, et al. What is most important to family caregivers when helping patients make treatment-related decisions: findings from a national survey. Cancers (Basel). 2023;15:4792. doi:10.3390/cancers15194792
43. Regier DA, Taylor JO, Ho A, Borson S, Turner AM. Care preferences for persons with cognitive impairment: a discrete choice experiment. Alzheimer’s & Dementia. 2026;22:e71107. doi:10.1002/alz.71107
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.