")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Care-Seeking for Fever for Children Under the Age of Five Before and After the Free Healthcare Initiative in Burkina Faso: Evidence from Three Population-Based Surveys
Authors Negatou M, Ouedraogo M, Donnen P, Paul E , Samadoulougou S , Kirakoya-Samadoulougou F
Received 6 January 2021
Accepted for publication 14 April 2021
Published 19 May 2021 Volume 2021:14 Pages 2065—2077
DOI https://doi.org/10.2147/RMHP.S297983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Mariamawit Negatou,1 Mady Ouedraogo,2 Philippe Donnen,3 Elisabeth Paul,3 Sekou Samadoulougou,4,5,* Fati Kirakoya-Samadoulougou1,*
1Centre de Recherche en Epidémiologie, Biostatistiques et Recherche Clinique, École de Santé Publique, Université Libre de Bruxelles, Bruxelles, Belgique; 2Institut National de la Statistique et de la Démographie (INSD), Ouagadougou, Burkina Faso; 3Centre de Recherche en Politiques et Systèmes de Santé – Santé Internationale, École de Santé Publique, Université Libre de Bruxelles, Bruxelles, Belgique; 4Centre for Research on Planning and Development (CRAD), Laval University, Quebec City, Quebec, G1V 0A6, Canada; 5Evaluation Platform on Obesity Prevention, Quebec Heart and Lung Institute, Quebec City, Quebec, G1V 4G5, Canada
*These authors contributed equally to this work
Correspondence: Mariamawit Negatou
Centre de Recherche en Épidémiologie, Biostatistique et Recherche Clinique, École de Santé Publique, Université Libre de Bruxelles, Bruxelles, Belgique
Tel +251911747363
Email [email protected]
Background: In 2016, a free healthcare policy (FHP) was implemented in Burkina Faso for children under the age of five. In our study, we aimed to determine the prevalence of care-seeking for a fever in children under the age of five before and after the implementation of the FHP and to analyze the determinants of not seeking care under the FHP.
Methods: The data of three nationally representative surveys were used to evaluate the trends of the prevalence of care-seeking. We performed a modified Poisson regression using a generalized estimating equation to determine the factors associated with not seeking care.
Results: The prevalence for care seeking increased from 57.5% (95% CI, 54.2– 60.8) in 2014 to 72.3% (95% CI, 68.1– 76.2) in 2017. Children from the poor quintile were less likely to seek care when compared to children from the poorest quintile (prevalence ratio (PR) = 0.7 (95% CI, 0.5– 0.9)). Caregivers who did not have messages regarding malaria in the past six months were more likely not to seek care (PR = 0.8 (95% CI, 0.7– 0.9)). Caregivers of children aged 36– 59 months were more likely not to seek care compared to those aged < 12 months (PR = 1.6 (95% CI, 1.2– 2.1)). Children from the Boucle du Mouhoun region (PR = 1.9 (95% CI, 1.2– 3.2)) and the Centre-Est region (PR = 1.9 (95% CI, 1.2– 3.0)) were more likely not to seek care compared to children from the Sud Ouest region.
Conclusion: Our study showed an increase in the prevalence of care-seeking after the implementation of the FHP. Even if this is encouraging, these findings highlight the critical importance of non-financial barriers to care-seeking. Maintaining FHP and tackling the barriers should be considered by policy makers to increase care-seeking.
Keywords: fever, free healthcare policy, care-seeking, children under-five, Burkina Faso
Background
Fever is among the early signs that are easily identifiable by children’s caregivers.1 Pneumonia and malaria are two of the most frequent diseases that cause fever in children and are the leading causes of death in children under five in sub-Saharan Africa (SSA). These diseases are public health issues that affect millions of people and cause significant mortality and morbidity every year, especially in SSA.2,3 In 2016, 312,417 deaths in children under five were due to respiratory infections in this region,4 while 285,000 deaths were due to malaria.5
A vast array of control measures have been put into place to prevent these diseases in most SSA countries. Since malaria is vector-borne, one of the most effective measures is vector control, eg, insecticide-treated mosquito nets. Other common ways of preventing malaria are the intermittent preventive treatment of malaria in pregnant women and infants and seasonal malaria chemoprevention in children under the age of five.6 To prevent febrile illness caused by pneumonia, vaccines against causative agents, adequate nutrition, good hygiene, and decreasing indoor air pollution have been recommended by the World Health Organization.7 These interventions and preventive measures have played an important role in decreasing child mortality due to febrile illnesses.7,8
In Burkina Faso, despite the many preventive measures that have been implemented, malaria remains the most common cause of febrile illness. Severe malaria was responsible for 3180 deaths in children under the age of five in 2018,9 making it the leading cause of hospitalization and death for this age group.9 As fever is an early symptom identifiable by caregivers, timely care-seeking for a fever has been identified as a key component in reducing severe complications, sequelae, and death.10
Even though safe and effective treatments are available, multiple factors can potentially cause caregivers not to seek appropriate care. One factor is limited financial resources—patients can use up to one-third of their total income for both direct and indirect costs,11 which can reduce the number of people seeking care. Like many other countries in Africa, Burkina Faso does not have a functional health insurance system, with a low healthcare coverage of approximately 39%.12 Thus, people are required to make out-of-pocket payments whenever they seek care. This causes a financial barrier for those who have a low income and especially for the vulnerable groups comprised of women and children. In 2006, Burkina Faso launched a national healthcare policy for pregnant women and newborns, requiring pregnant women to pay only 20% of their medical costs;13 however, since women and children are the most affected and to further reduce child mortality, in 2016, the government decided to completely abolish direct healthcare payments for both pregnant women and children under the age of five.12 This policy aimed to increase care-seeking by reducing direct payments.
Even though free treatment is available, other care-seeking behaviors can potentially impede caregivers from seeking timely and appropriate healthcare. Studies conducted in Malawi, for instance, showed that household and individual factors such as the mother’s level of education, the child’s age, the position of the child in the family, the religion, and the wealth index of the household, as well as environmental factors such as region, distance from the nearest health facility, and residential area (urban/rural) play an important role in care-seeking.14,15 A study conducted in Mozambique showed that the mother’s age, religion, and sex of the head of the household were potential determinants of care-seeking for a fever.16
In our study, we had two objectives, with the intent to develop new strategies to increase the utilization of health services and hence to improve health impacts. First, we aimed to evaluate whether there has been an increase in care-seeking for children under the age of five with a fever after the launch of the free healthcare policy in 2016 in Burkina Faso. Second, we aimed to identify the remaining barriers preventing caregivers from seeking care despite the implementation of this new policy.
Methods
Study Design and Data Sources
This was a secondary analysis of data from three population-based surveys collected in 2010, 2014, and 2017 in Burkina Faso—the 2010 Demographic and Health Survey (DHS) and the 2014 and the 2017 Malaria Indicator Survey (MIS) data collected by the National Institute of Statistics and Demography (NISD). The objective of the DHS was to provide socioeconomic, demographic, and health indicators,17 while that of the MIS was to provide a reliable database to assess the impact of the different strategies that were put in place to combat malaria.18,19 Our study included children under the age of five that had a fever two weeks prior to the surveys.
Data Collection Tools
Two types of questionnaires were used during the survey: Household questionnaire and the Women questionnaire. With the household questionnaire basic-sociodemographic characteristics and characteristic of the household were collected. Using the women questionnaire, information about sociodemographic information about the women, about reproduction, knowledge about malaria and information about fever and treatment for their children were collected. For women who had children further questions were asked to collect information about the children.19
Setting
The surveys were conducted in Burkina Faso, which is a landlocked country located in West Africa. It has an area of 272,967 km2, and in 2017, the population was estimated to be 19,632,147.19 Women aged 15–49 years and children aged 0–5 years represent 24% and 17% of the total population, respectively.19 Burkina Faso is made up of 13 administrative regions and 352 municipalities.18,19
Variables
Dependent Variable
The outcome variable was the proportion of children under the age of five who caregivers sought care for a fever.
Independent Variables
Based on a literature review, we identified the following independent variables that were relevant to household, mother/caregivers, and child characteristics that could influence care-seeking:19–24
–Child characteristics: gender of the child (male or female); the age of the child in months (<12 months, 12–35 months, or 36–59 months); the place where care was first sought (public, private, or traditional/other).
–Mother’s characteristics: age of the mother (15–24 years, 25–34 years, or ≥35 years); education level of the mother (none, primary and secondary, or higher); the number of living children (1–2, 3–4, or ≥5); religion (Christian, Muslim, traditional/other, or no religion); information about malaria: Answer to the question “Have you heard or seen any message about malaria during the last six months?” (yes or no).
–Household characteristics: region of residence (13 regions of Burkina Faso); place of residence (urban or rural); head of the household (male or female); age of the household head (15–24 years, 25–34 years, 35–49 years, ≥50 years); wealth index (poorest, poor, middle, rich, or richest). Note that the wealth index was calculated by collecting data from the household about the type of water access and sanitation available in the house, the availability of electricity, and the number of people per room …;18,19 a score was given for each household.
For the 2017 survey, the variable distance to the health facility (<5 km or ≥5 km) was calculated at the health district level and approximated by the average distance to the health center. We considered the distance to be the same for all clusters belonging to the same district.
Statistical Analysis
For our analysis, the data from the surveys were merged. The “Svy” survey command was used to account for the complex survey design using the sampling weight provided by the DHS. Data were weighted to be representative at the national and regional levels.
Descriptive analyses were used to summarize the socioeconomic and demographic characteristics of the mothers and the demographics characteristics of the children. They were presented as a percentage for the categorical data. The Pearson’s chi-square test was used to compare the characteristics of the 2010, 2014, and 2017 data.
Prevalence ratios (PRs) were obtained using a modified Poisson regression model that used the generalized estimating equation. A univariate analysis was first performed to analyze the potential factors associated with not seeking care after the implementation of the new policy. Both PR and its respective 95% confidence interval are presented for the 2017 MIS data. Variables that were significant at the 0.1 level in the univariate analyses were included in the multivariable analyses. The variables that were reported in the literature (ie, age of the child, sex of the child, age of the mother, educational level, distance from the health facility, and place of residence)20,21 to be associated were also included. The Wald test was used to obtain the p-value for the variables with more than two categories.
Statistical analyses were performed using the Stata 15 software and a significance level of 0.05 was chosen for all analyses.
Results
A total of 2950 children under the age of five who had a fever in the last two weeks were surveyed in 2010; using the same criteria, 2617 children were surveyed in 2014 and, similarly, 1220 children in 2017.
Characteristics of the Study Population
The characteristics of the febrile children and their mothers are presented in Table 1. From the selected participants, approximately half of the children were male (51.9% in 2010, 51.4% in 2014, and 51.0% in 2017). Fever was less common in children aged <12 months when compared to other age groups in all surveys (20.5% in 2010, 17.1% in 2014, and 21.9% in 2017). We observed that the distribution of patients according to the age of the mother, the gender of the household head, and the number of living children was similar for 2010, 2014, and 2017. In 2014, approximately four out of five (79.5%) mothers of children who had a history of fever did not have any education; this number decreased to 75.0% in 2017. The percentage of women who had either heard or seen a message regarding malaria in the past six months was 44.9% in 2014 but increased to 62.7% in 2017. The proportion of children that had a fever differed by region.
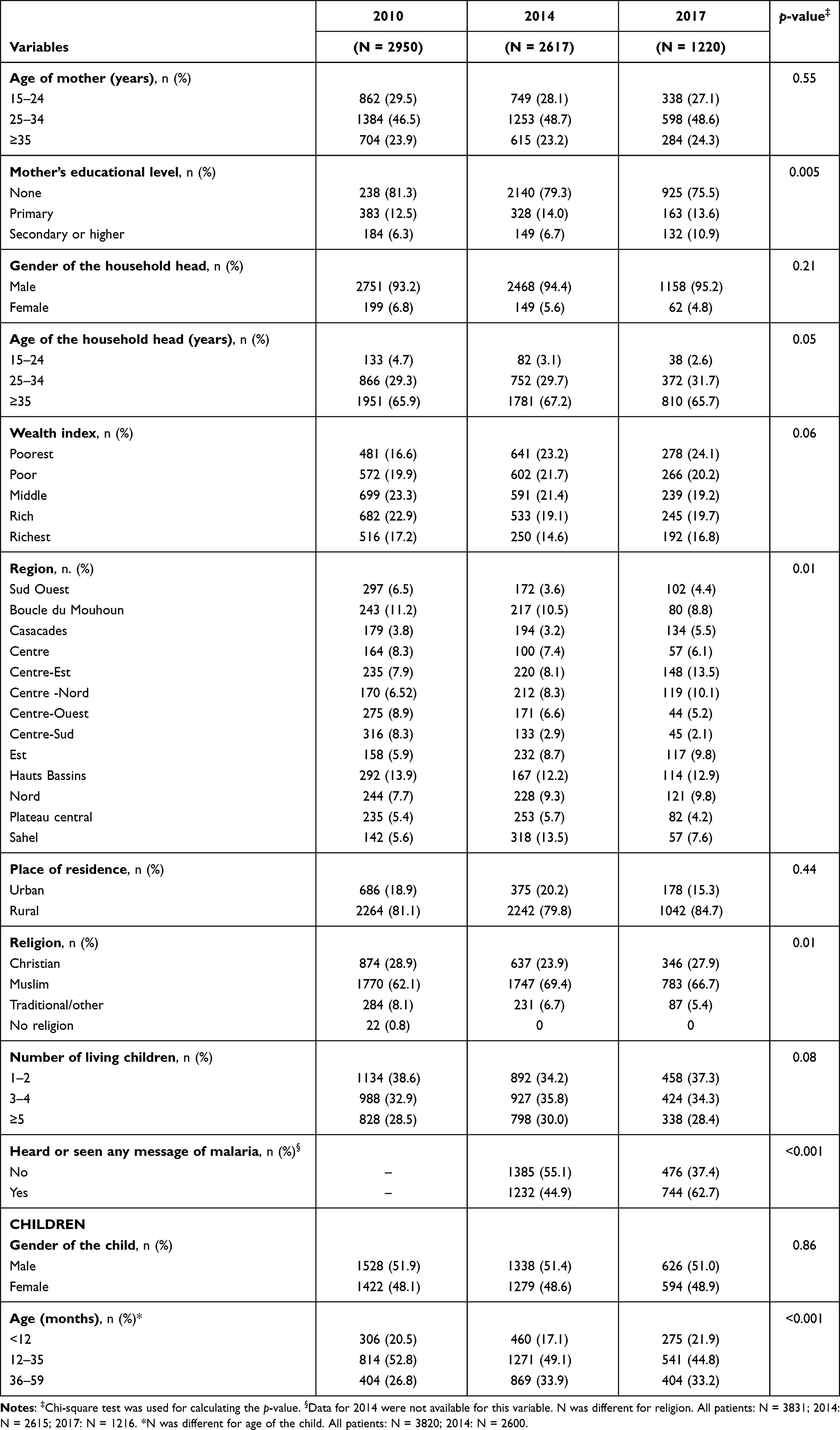 |
Table 1 Characteristics of the Children Who Had a Fever in the Last Two Weeks in 2010, 2014, and 2017 |
Evolution of Care-Seeking for a Fever Before and After the Launch of FHP
In 2010, 53.4% (95% confidence interval (CI), 50.4–56.4) of the children with a history of fever sought care. This proportion increased to 57.5% (95% CI, 54.2–60.8) in 2014 and 72.3% (95% CI, 68.1–76.2) in 2017.
The number of children that sought care from traditional healers decreased from 14.6% (95% CI, 12.3–17.20) to 2.3% (95% CI, 1.3–3.8) between 2010 and 2017. The number of children that sought care decreased also from 5.0% (95% CI, 3.6–6.9) to 2.2% (95% CI, 1.1–4.2) in private health facilities. The proportion of those who first sought care for a fever from public facilities increased from 79.7% (95% CI, 76.7–82.5) to 95.6% (95% CI, 93.4–97.3) over the studied period (Figure 1).
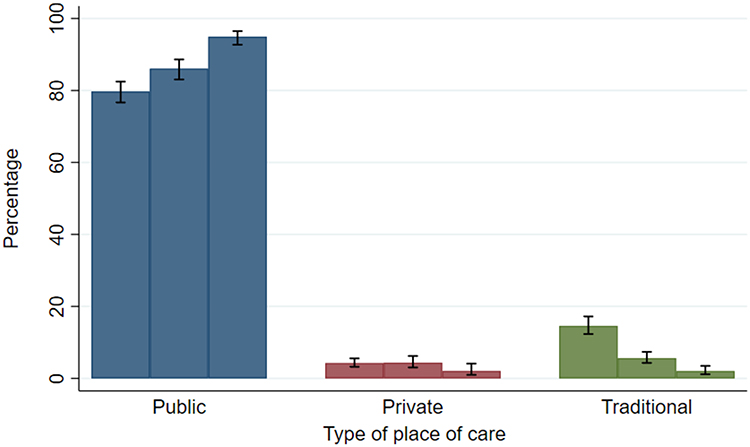 |
Figure 1 Place where care was sought first for febrile children by survey. |
After the launch of the FHP, the proportion of children that sought care for a fever increased in most of the regions. In 2010, Cascades, Sud–Ouest, Centre–Ouest, Boucle du Mouhoun, and the Sahel regions had a proportion of care-seeking below 50% (Figure 2); by 2014, only three regions (Hauts-Bassins, Sud–Ouest, and Sahel) were below 50%. In 2017, more than 50% of children with a fever had sought care in all regions of the country, and five regions (Nord, Plateau-central, Center, Cascades, and Sud Ouest) recorded a care-seeking rate of 80% (Figures 3 and 4).
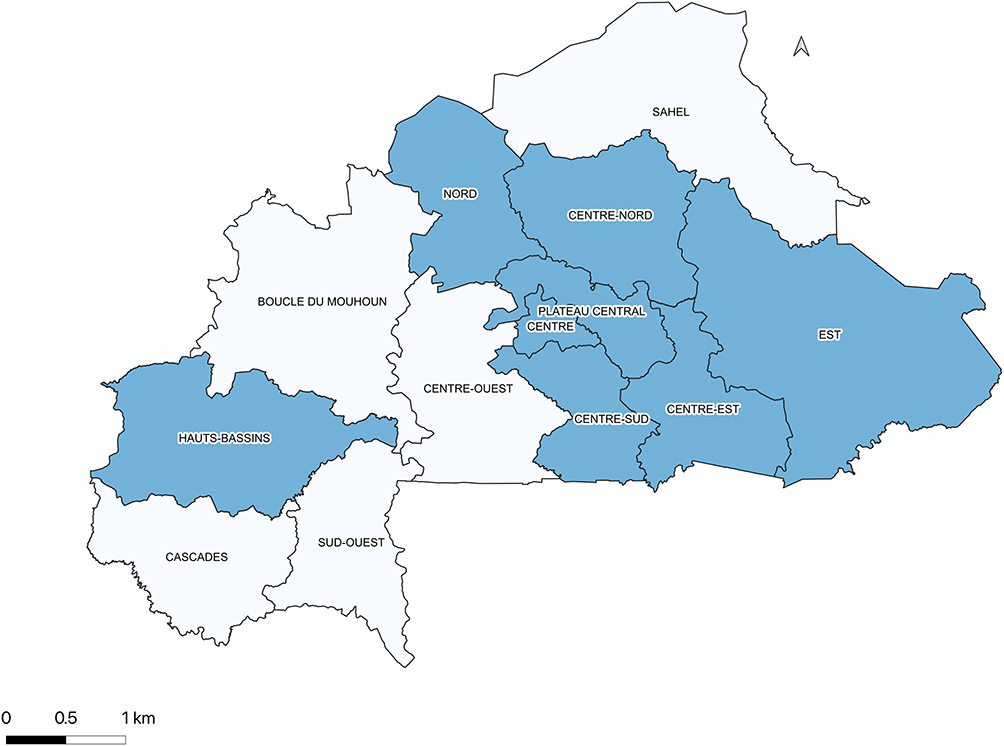 |
Figure 2 The proportion of children under the age of five for whom care was sought for a fever by region in Burkina Faso in 2010. |
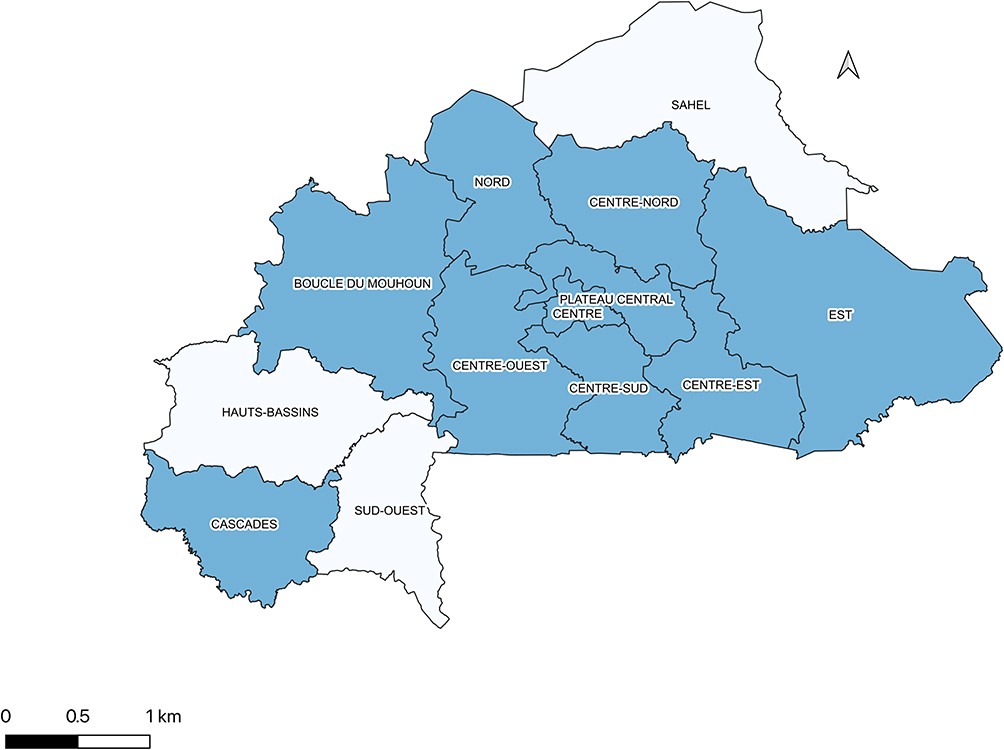 |
Figure 3 The proportion of children under the age of five for whom care was sought for a fever by region in Burkina Faso in 2014. |
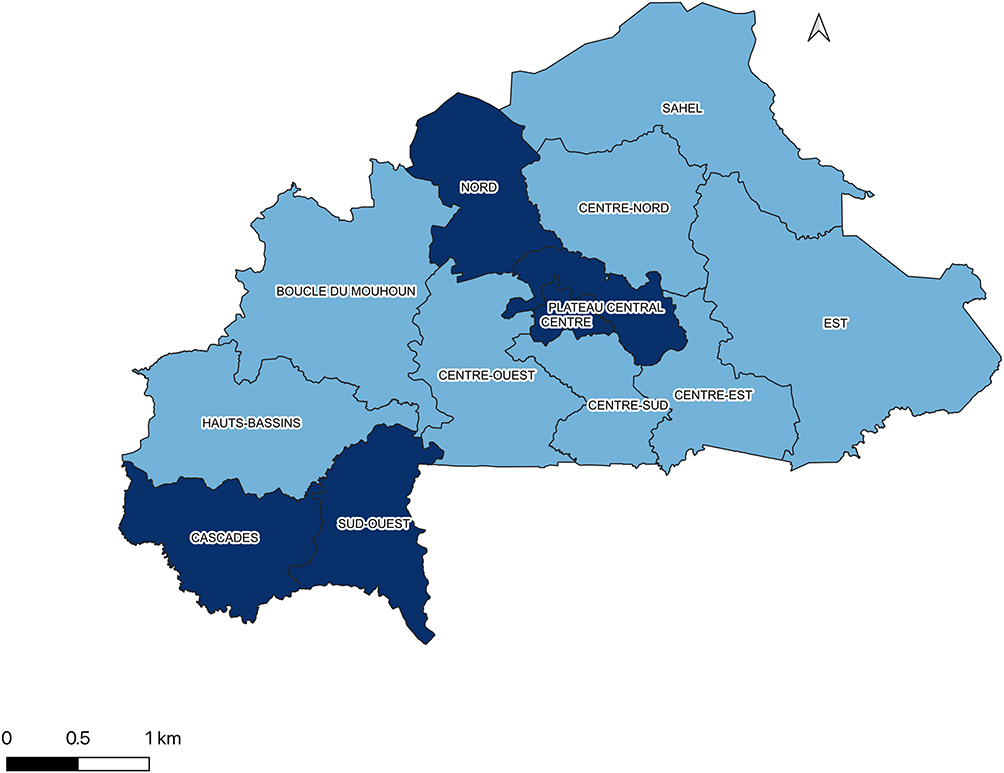 |
Figure 4 The proportion of children under the age of five for whom care was sought for a fever by region in Burkina Faso in 2017. |
In contrast, three regions (Boucle du Mouhoun, Centre–Ouest, and Centre–Est) experienced a decrease in care-seeking between 2014 and 2017. This decrease was more pronounced in the Centre–Est region (from 72% in 2014 to 63% in 2017). The highest increase in care-seeking was seen in the Sud–Ouest region, where the proportion of children that sought care increased from 46% in 2014 to 81% in 2017.
Predictors of Not Seeking Care for a Fever
In the multivariable analysis, the wealth level, region, child’s age, and lack of exposure to messages regarding malaria in the past six months were significantly associated with not seeking care for a fever (Table 2). Indeed, not seeking care for a fever was significantly more likely in a household in the poorest quintile. Children from the poor quintile were less likely to not seek care compared to children from the poorest quintile (PR = 0.7 (95% CI, 0.5–0.9)) and compared to children from the richest quintile. Children with mothers not exposed to a message about malaria in the past six months were more likely not to seek care for a fever (PR = 0.8 (95% CI, 0.7–0.9)). We also observed that when the age of the child increased, healthcare was less likely to be sought. Children whose ages were between 36 and 59 months were more likely not to seek care compared to those aged less than 12 months (PR=1.6 (95% CI, 1.2–2.1)).
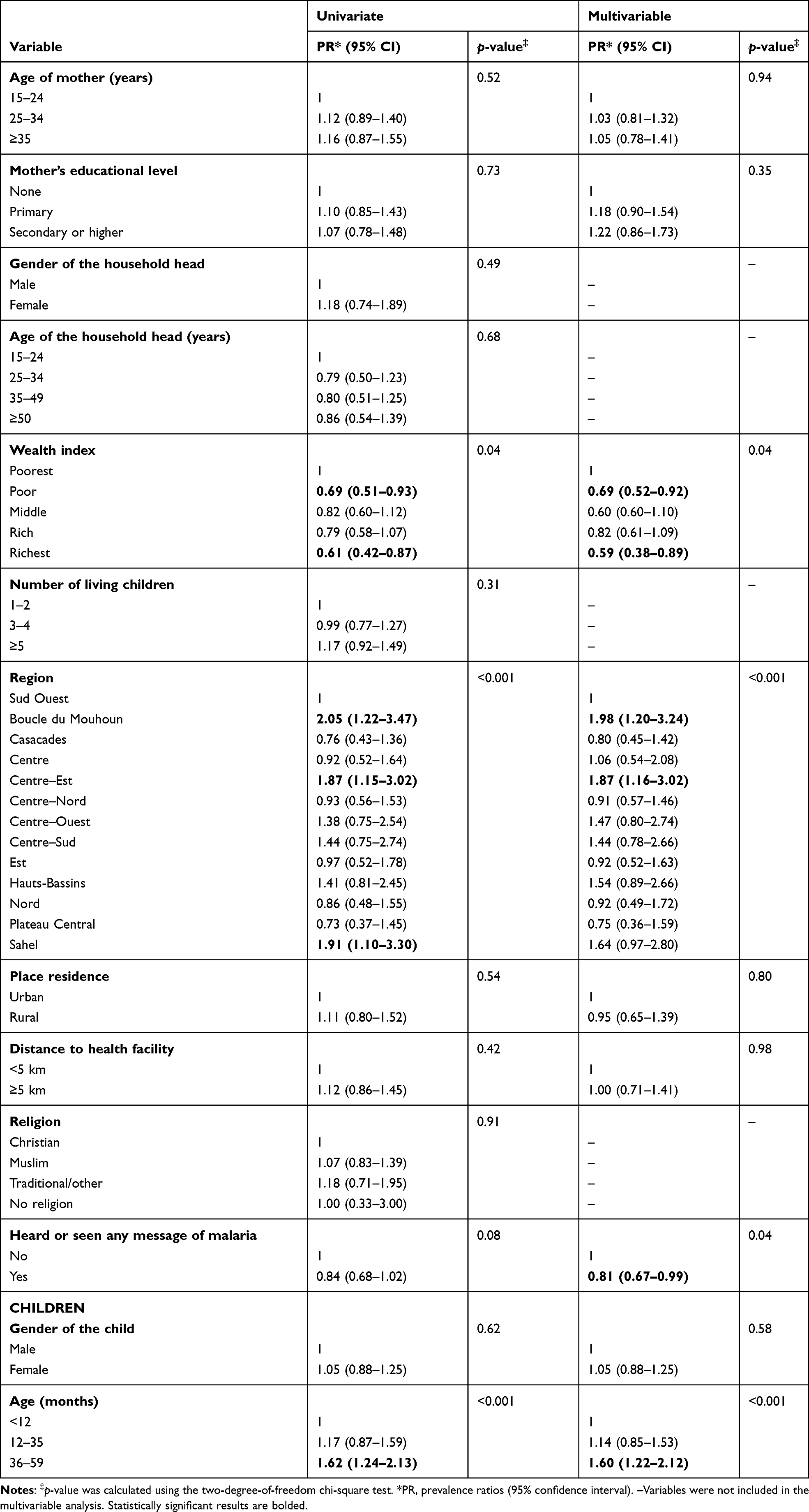 |
Table 2 Univariate and Multivariable Analyses of the Determinants of Not Seeking Care for a Fever in 2017 |
Concerning regions, children from the Boucle du Mouhoun region (PR = 1.9 (95% CI, 1.2–3.2)) and the Centre–Est region (PR = 1.9 (95% CI, 1.2–3.0)) were more likely not to seek care compared to children from the Sud–Ouest region.
In the Centre–Est, Centre–Sud, Nord and Plateau-centrale regions, the non-use of healthcare was significantly lower than in the Centre region. The rural areas had a high PR for non-use of healthcare when compared to urban areas.
Discussion
Our study showed a 35% increase in care-seeking after the implementation of the FHP between 2010 and 2017. Similar findings were documented in a study conducted in Sierra Leone in 2013, where the prevalence of children seeking care for diarrhea and pneumonia increased after the implementation of the Free Health Care Initiative.20 This increase was observed mostly within public health facilities. The free healthcare policy has been implemented in all public health facilities, this could explain the increase in the use of public facilities and the decrease in the use of private facilities.22
This study suggests that free healthcare is not the only measure necessary to increase the prevalence of children seeking care for a fever. Besides financial barriers, there is a whole series of non-financial barriers that play a role in care-seeking—wealth index, regions, having heard or seen messages about malaria, and the age of the child were all associated with not seeking care for a fever in children under the age of five.
The wealth index of the household was significantly associated with not seeking care for a fever. Not seeking care was more prevalent among children who belonged to the lowest socioeconomic status. Similar results were found in other studies in Myanmar and Mozambique.16,23 Even though free healthcare is available, other factors can play a role in a household with a low socioeconomic status, such as the distance to the nearest healthcare facility, the quality of the roads, access to transportation, and waiting times. We cannot exclude competing needs in low socioeconomic households, it is difficult for caregivers to take their children to seek care when they have to tend to other household chores, for those who have to work in the farm taking the children to the hospital may result in loss of income if they miss a day of work.
However, these results differ from those of a study conducted in rural Burkina Faso after user fees were reduced for pregnant women. The study showed that women from the poor quintile were the ones who utilized the maternal care service the most when compared to women from the rich quintile.27 A possible explanation is that when initiatives were put in place, free products were given to both those who sought care and those who came from the low socioeconomic status, who may have needed these products.27 These initiatives can also be implemented to encourage mothers to seek care for their children who have a fever. However, not having to pay for medical care may not be enough to offset all the burdens experienced by caregivers.
Our results indicate important differences in not seeking care for a fever by region. The Boucle du Mouhoun and Centre–Est regions were two of the regions where care-seeking decreased between 2010 and 2017. Children from these two regions were less likely to seek care for a fever when compared to the Sud–Ouest region. This may be explained by the fact that, according to the World Bank, in these two regions, poverty is high, and half of the population lives below the poverty line.24 In addition, according to the national survey on the provision of health services and the quality of healthcare, the Boucle du Mouhoun region has a diagnostic capacity for malaria lower than the national average.25 Furthermore, a significant number of people were not satisfied with the quality of services provided by their healthcare facilities.26 The main reason given for this dissatisfaction is that the waiting time is too long.27 For the Sahel region, the prevalence of not seeking care was elevated, even if it was not significant for the multivariable analysis. The reason for the elevated prevalence could be explained by the distance to health facilities. Compared to other regions, it takes them the longest to reach healthcare facilities—on average, it can take up to one hour.27
As these regions have a higher poverty rate, they have less health infrastructure, the commute time to a health facility is high on average, the number of diagnostic equipment is lacking, and the quality of services may be too low. These factors may contribute to the high prevalence of not seeking care in these regions. Free healthcare is important, and investments should be made to provide effective and rapid treatment.
The age of the child was a significant predictor for not seeking care. As the child’s age increased, care-seeking behavior for a child with a fever became less likely. The child’s age being over 36 months was the second highest factor that contributed to not seeking care. This result is similar to a study conducted in Ethiopia where younger children were more likely to be taken to a healthcare facility for a fever compared to older children.28 More attention is paid to the health of infants, and thus caregivers may be aware that younger children may be at higher risk of getting seriously ill—this could explain why they are likely to seek care for them; however, caregivers should also be encouraged to seek care for older children. Another explanation could be that older children have experienced multiple episodes of fever before, and given that it is not their first time, caregivers may be more experienced in dealing with their older children’s illnesses.
Not having heard or seen any messages regarding malaria was significantly associated with not seeking care. The mothers not exposed to messages about malaria in the last six months were less likely to seek care for a fever. A study conducted in Malawi showed that mothers who knew about malaria were more likely to seek care than those who did not know.21 The mothers that had not heard or seen information about malaria may not have enough information about fever and the dangers of not seeking treatment. This shows the importance of providing consistent and continuous information regarding diseases to caregivers as it has a positive impact; therefore, we encourage policy makers to continue to raise awareness for potential illnesses in children.
This study has a few limitations. The first is that the data were not collected during the same season, which could potentially be a problem as fever due to malaria increases during seasonal peaks. Desirability bias can also be a limitation; when answering the questions, caregivers may have wanted to provide an answer seen as socially favorable or culturally acceptable—this limitation may have been reduced, since the interviewers were trained.
Despite these limitations, the strength of this study is that the surveys used nationally representative samples that covered all regions of the country and had high response rates and by identifying barriers policy makers can improve the FHP so that all children can benefit from this policy. Recognizing non-financial barriers that can impede care seeking is important for policy makers, they can expect the challenges the policy faces to be sustainable in the long term. Our findings are not only useful for Burkina Faso but also to other African countries that are implementing these kind pf policies, they can expect the challenges beforehand and make improvements before launching their free healthcare policies.
Conclusion
Our study showed an increase in the prevalence of care-seeking for a fever after the implementation of the FHP in Burkina Faso. Despite this encouraging increase, treatment was still not sought for approximately 25% of children under the age of five. Non-financial barriers such household socioeconomic status, age of the child and not having continuous awareness about febrile illnesses have been identified as barriers preventing caregivers from seeking care for children under the age of five after the implementation of the FHP. Regional disparities in care seeking for children under the age of five have also been observed. These factors should be tackled first as part of a new strategy to increase the prevalence of care-seeking for children under the age of five. Such a behavioral change should be supported more forcefully, especially in the identified regions with poor health care utilization.
Abbreviations
EA, enumeration area; CDC, Center for Disease Control and Prevention; CI, confidence interval; DHS, Demographic and Health Survey; FHP, free healthcare policy; Km2, square kilometer; MIS, Malaria Indicator Survey; NISD, National Institute of Statistics and Demography; OR, odds ratio; PR, prevalence ratio; SMC, seasonal malaria chemoprevention.
Ethical Consideration
This study is a secondary analysis of Burkina Faso data. The surveys have been performed by ICF international and the Institut national de la statistique et de la démographie of Burkina Faso. We have received permission to download and use these data from DHS program (https://dhsprogram.com). Ethical clearance for the surveys was obtained by the Institutional Review Board of ICF International and the Institut national de la statistique et de la Démographie of Burkina Faso. More details about ethical standards are available at: https://dhsprogram.com/methodology/Protecting-the-Privacy-of-DHS-Survey-Respondents.cfm
Acknowledgments
The authors would like to thank the DHS program for providing the datasets used in this study. The authors also thank Dr Bognini Joel for assisting with data management.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any funding for this work.
Disclosure
The authors declare they have no competing interests.
References
1. Sajadi MM, Bonabi R, Sajadi M-RM, Mackowiak PA. Akhawaynī and the first fever curve. Clin Infect Dis. 2012;55:976–980. doi:10.1093/cid/cis596
2. Sanyang Y. Prevalence of under-five years of age mortality by infectious diseases in West African region. Int J Afr Nurs Sci. 2019;11:100175.
3. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385:430–440. doi:10.1016/S0140-6736(14)61698-6
4. Troeger C, Blacker BF, Khalil IA, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18:1211–1228. doi:10.1016/S1473-3099(18)30362-1
5. World Health Organization. Malaria in children under five; 2018. Available from: http://www.who.int/malaria/areas/high_risk_groups/children/en/.
6. Prevention C-C for DC. CDC - malaria - malaria worldwide - how can malaria cases and deaths be reduced?; 2019 Available from: https://www.cdc.gov/malaria/malaria_worldwide/reduction/index.html.
7. WHO/UNICEF. Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025. World Health Organization; 2013.
8. Prevention C-C for DC; 2020. CDC - malaria - malaria worldwide - impact of malaria. Available from: https://www.cdc.gov/malaria/malaria_worldwide/impact.html.
9. Ministère de la santé/Burkina Faso. Annuaire statistique 2018, Direction générale des études et des statistiques sectorielles. 2019.
10. World Health Organization. World malaria report; 2019. Available from: https://www.who.int/publications-detail/world-malaria-report-2019.
11. Roll Back Malaria Department W. Malaria control today. 2005.
12. Ridde V, Yaméogo P. How Burkina Faso used evidence in deciding to launch its policy of free healthcare for children under five and women in 2016. Palgrave Commun. 2018;4:1–9. doi:10.1057/s41599-018-0173-x
13. Ganaba R, Ilboudo PGC, Cresswell JA, et al. The obstetric care subsidy policy in Burkina Faso: what are the effects after five years of implementation? Findings of a complex evaluation. BMC Pregnancy Childbirth. 2016;16:84. doi:10.1186/s12884-016-0875-2
14. Chitunhu S, Musenge E. Direct and indirect determinants of childhood malaria morbidity in Malawi: a survey cross-sectional analysis based on malaria indicator survey data for 2012. Malar J. 2015;14:265. doi:10.1186/s12936-015-0777-1
15. Nkoka O, Chuang T-W, Chen Y-H. Multilevel analysis of factors associated with treatment-seeking behaviors among caregivers with febrile children in Malawi. Am J Trop Med Hyg. 2019;100:1454–1465. doi:10.4269/ajtmh.18-0900
16. Cassy A, Saifodine A, Candrinho B, et al. Care-seeking behaviour and treatment practices for malaria in children under 5 years in Mozambique: a secondary analysis of 2011 DHS and 2015 IMASIDA datasets. Malar J. 2019;18:115. doi:10.1186/s12936-019-2751-9
17. Institut National de la Statistique et de la Démographie (INSD) et ICF International. (2012) Enquête Démographique et de Santé et à Indicateurs Multiples du Burkina Faso 2010. 2012.
18. Institut National de la Statistique et de la Démographie (INSD) et ICF International. (2015) Enquête Démographique et de Santé et à Indicateurs Multiples du Burkina Faso 2014. 2012.
19. Institut National de la Statistique et de la Démographie (INSD) et ICF International. (2018) Enquête Démographique et de Santé et à Indicateurs Multiples du Burkina Faso 2017–2018. 2012.
20. Diaz T, George AS, Rao SR, et al. Healthcare seeking for diarrhoea, malaria and pneumonia among children in four poor rural districts in Sierra Leone in the context of free health care: results of a cross-sectional survey. BMC Public Health. 2013;13:157. doi:10.1186/1471-2458-13-157
21. Oyekale AS. Assessment of Malawian mothers’ malaria knowledge, healthcare preferences and timeliness of seeking fever treatments for children under five. Int J Environ Res Public Health. 2015;12:521. doi:10.3390/ijerph120100521
22. Bicaba F, Browne L, Kadio K, Bila A, Bicaba A, Druetz T. National user fee abolition and health insurance scheme in Burkina Faso: how can they be integrated on the road to universal health coverage without increasing health inequities? J Glob Health. 2020;10(1). doi:10.7189/jogh.10.010319
23. Min KT, Maung TM, Oo MM, et al. Utilization of insecticide-treated bed nets and care-seeking for fever and its associated socio-demographic and geographical factors among under-five children in different regions: evidence from the Myanmar Demographic and Health Survey, 2015–2016. Malar J. 2020;19:7. doi:10.1186/s12936-019-3088-0
24. World Bank Group. Burkina Faso: poverty, vulnerability, and income source. 2016.
25. Ministère de la Santé. Enquête nationale sur les prestations des services de santé et la qualité des données sanitaires. 2014.
26. Institut National de la Statistique et de la Démographie (INSD). Analyse des résultats de l’Enquête annuelle sur les conditions de vie des ménages et du suivi de la pauvreté. 2007.
27. Institut National de la Statistique et de la Démographie (INSD) et ICF International. (2007) Enquête annuelle sur les conditions de vie des ménages, 2007. 2012.
28. Simieneh MM, Mengistu MY, Gelagay AA, Gebeyehu MT. Mothers’ health care seeking behavior and associated factors for common childhood illnesses, Northwest Ethiopia: community based cross-sectional study. BMC Health Serv Res. 2019;19:59. doi:10.1186/s12913-019-3897-4
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.