")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Care Burden and Life Satisfaction of Caregivers Who are Providing Home Health Care to Patients
Authors Sezek I, Cubukcu M , Muderrısoglu S
Received 19 June 2023
Accepted for publication 28 September 2023
Published 16 October 2023 Volume 2023:16 Pages 2139—2150
DOI https://doi.org/10.2147/RMHP.S426598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Isa Sezek,1 Mahcube Cubukcu,2 Secıl Muderrısoglu3
1Yesil Kent Family Health Center, Samsun, Turkey; 2Department of Family Medicine, Samsun University Faculty of Medicine, Samsun, Turkey; 3Department of Biochemistry, Ondokuz Mayis University, Health Sciences Institute, Samsun, Turkey
Correspondence: Mahcube Cubukcu, Department of Family Medicine, Samsun University Faculty of Medicine, Canik Kampüsü, Merkez sokak, No: 40-2/1 55080 Canik, Samsun, Turkey, Tel +90 505 233 22 32 ; +903623111500-7125, Fax +903623130200, Email [email protected]; [email protected]
Background: This study aims to evaluate the care burden and life satisfaction in caregivers who are providing home health care to patients and determine the relationship between life satisfaction and care burden.
Methods: This cross-sectional descriptive study was performed on 133 caregivers who provided home health care to patients and 133 control groups between February and December 2020. Care burden was evaluated using the Zarit Burden Inventory (ZBI), and life satisfaction was evaluated using the Satisfaction with Life Scale (SWLS).
Results: The mean age of hundred thirty-three caregivers was 52.5± 10.5 years, and that of the control group was 51.2± 9.9 years. The mean ZBI score of the caregivers was 47.0± 16.4. According to the ZBI score, 46.6% of the caregivers had a moderate care burden and 21.8% had a heavy caregiver burden. The caregiver burden was higher in those with a low education level, those without social insurance, those who felt insufficient in care, and those who did not receive help from other family members. The SWLS score of caregivers was significantly lower than that of control group (p< 0.001). The SWLS score was lower in those with a low education level and those without an employee as a caregiver. There was a negative correlation between SWLS and ZBI score (p< 0.001).
Conclusion: Caregivers of patients receiving home health-care services are exposed to a significant care burden. The care burden was higher in those with a low education level, those without social insurance, those who felt insufficient in care, and those who did not receive help from other family members. The care burden affects the satisfaction of life.
Keywords: caregiver, care burden, home health care, life satisfaction, patients
Introduction
According to Turkish Statistical Institute data, older adults aged over 65 years constitute 7.8% of Turkey’s total population.1 In particular, a long-term and demanding maintenance process can result in a burden of maintenance. The deterioration of the balance between the care needs of the caregivers and their own needs and the negative physical, social, and psychological situations they encounter in relation to the care are defined as the burden of the caregiver. Especially in the care of dementia, stroke, and functionally dependent individuals, caregivers face more negativities.2
Home care service was defined in Turkey in 2005 in the Regulation on Home Health-Care Services. Home care services have had many different purposes such as providing health services to poor people, reducing hospital density, and preventing infectious diseases.3 In addition, it was stated that the burden of caregivers could be reduced with the home care of stroke patients and the training of their caregivers. Home health care does not just target the patient. Furthermore, it includes caregivers and other individuals in the home.4 Caregivers should be educated about the needs and illness of the caregiver. This training should include how to transfer the patient to a place and how the patient can be removed. Especially in elderly individuals, falls and fall-related complications are frequently observed and cause significant consequences.5
Life satisfaction reflects the perceived difference between one’s needs and desires and realities as a link to areas of functionality and activity/participation. Life satisfaction in general is a structure of subjective well-being related to how people evaluate the quality of certain aspects of their lives, such as work, marriage, health, entertainment, religion, and so on.6
The rational aspect of life satisfaction is a consequence of an individual’s process of coping and adaptation. Three theories have been proposed to explain life satisfaction: The “set point” theory focuses on mental processes that maintain a stable attitude toward life. The “comparison” theory, on the other hand, involves a comparison of life perceptions about how life should be in the evaluation of life satisfaction rather than a continuous process of judgment. The “affect” theory, on the other hand, accepts happiness as a continuous mental process and is concerned with how individuals feel.7
Life satisfaction decreased in the companions of individuals receiving inpatient treatment in internal and surgical clinics, and similarly, a strong relationship was observed between life satisfaction, burnout, and burden of care. It is proposed to reduce the burden of care and burnout of caregivers, to support caregivers to increase life satisfaction, to employ personnel who will share the burden of caregivers in patient care, to prevent labor and economic loss of caregivers, and to provide basic patient care to caregivers.8
Knowing the characteristics of caregivers is important to identify the group at risk for difficulty, establish support groups according to these characteristics, and to develop this home health care. It was aimed to evaluate the care burden and life satisfaction of caregivers who are providing to home care patients and determine the relationship between life satisfaction and the care burden. We hypothesized that caregiver burden was negatively associated with life satisfaction.
Methods
The descriptive study was conducted between February 01 and December 2020 in Samsun province. Of the 133 patients and caregivers were visited by the Samsun Training and Research Hospital home health-care team. There were 2946 patients receiving Samsun Training and Research Hospital home health-care services. The minimum necessary sample size was calculated for at least 113 people with 80% power, a 95% confidence (d=0.05) interval, and a 10% (p=0.1, q=0.9) acceptable margin of error. Inclusion in this study was only eligible for participants who: (1) were age ≥ 18 years; (2) were the primary caregivers of the home care patients and provided care half than 6 months; (3) were members of the patient’s immediate families; (4) were not having problem understanding, reading, and writing in Turkish; (5) were having a comprehensive understanding to fill in the questionnaires completely. Those who did not want to participate in the study (n=3) and could not fully answer the research questions (n=4) were also excluded from the study. The caregivers and patients were selected to the study groups by randomization test methods. The caregivers who received home care patients and people similar to their caregivers in terms of age and gender were selected as the control group.
The current study was conducted under the Declaration of Helsinki. To carry out the research, permission was obtained from the Ethics Committee of Health Sciences University Faculty of Medicine, Samsun Training and Research Hospital, numbered 2020/1/1 with the decision number 954. Our study complies with the Declaration of Helsinki. Data were collected by the investigator through face-to-face interviews with caregivers and control group. Due to the roles imposed by social life in Turkey, most of the non-professional or professional caregivers are women. Therefore, equalizing the numbers of men and women in this study will cause the distribution to be non-normal. Sociodemographic characteristics form and life satisfaction were evaluated with the “Satisfaction with Life Scale” (SWLS) in both caregivers and control groups. Zarit Burden Inventory (ZBI) was used to measure caregiver burden. ZBI was developed by Zarit et al to assess the level of burden on caregivers.9 The Turkish validity and reliability of the scale were determined by Inci et al in 2008. The Cronbach's alpha coefficient for the interview ranged from 0.87 to 0.99. It was used to evaluate the caregiving difficulties experienced by caregivers of individuals in need of care. The scale, which the caregiver or the researcher can fill out, consists of 22 statements that determine caregiving’s effect on the individual’s life (physical, mental, and social well-being). The scale includes Likert-type assessment ranging from 0 to 4 as “never”, “rarely”, “sometimes”, “often”, and “always.” On this scale, a minimum of 0 and a maximum of 88 points can be obtained. The items in the scale are generally related to the social and emotional domains, and the higher the scale score indicates that the extent of the distress is also great. Corresponding definitions in scoring are as follows: 0–20 points: “no care burden”, 21–40 points: “mild care burden”, 41–60 points: “moderate care burden”, and 61–88 points: “heavy care burden.”10 This scale, developed by Diener, Emmons, Larsen, and Griffin (1985), consists of five items expressed in the same direction. Responses are on a Likert-type scale ranging from 1 to 7 (“strongly disagree” to “strongly agree”).11 Turkish validity and reliability studies have been conducted by Dagli and Baysal.12 This scale was applied to both caregivers and the control group.
Statistical Analysis
Statistical analysis was made using the IBM SPSS Statistics Version 15.0 (Chicago, USA) package program. The conformity of the variables to the normal distribution was examined using visual (histogram and probability graphs) and analytical methods (Kolmogorov Smirnov, Shapiro–Wilk test). Descriptive statistics are expressed as mean and standard deviation in normally distributed numerical data, median, and lower-upper values in non-normally distributed data, and numbers and percentages in nominal data. Normally distributed numerical variables are “independent t-tests” between two groups, variables that were not normally distributed were analyzed using the “Mann Whitney U-test” between the two groups and the “Kruskal Wallis test” between three or more groups. “Chi-square analysis” was used to compare the nominal data. In correlation analyses, the “Spearman correlation test” was preferred for normal distributed variables. A p-value < 0.05 was considered significant.
Results
The study was conducted with 133 female participants in the caregiver group and 133 female participants in the control group. The mean age of caregivers was 52.5±10.5 years, and the control group was 51.2±9.9 years. 87.2% (n=116) of the caregivers lived with their family and 6% (n=8) lived with their spouse. Of the control group, 69.9% (n=93) lived with their family and 30.1% (n=40) lived with their spouse. Caregivers tended to live with their families (p<0.001). The proportion of participants with social insurance among caregivers was significantly lower than in the control group (p<0.001). 46.6% (n=62) of the caregivers were primary school graduates. 29.3% (n=39) of the control group were primary and university graduates. There was a significant difference between the groups in terms of education level (p<0.001). 36.8% (n=49) of the control group were literate and primary school graduates. 69.9% (n=93) of the caregivers were literate and primary school graduates. The educational level of the caregivers was significantly lower than that of the control group (p<0.001). 76.7% (n=102) of the caregivers were married. 80.5% (n=107) of the control group were married. 61.7% (n=82) of the caregivers were housewives. 39.1% (n=52) of the control group were housewives. A significant difference was observed between the groups according to the work status (p<0.001). The number of active employee participants in the caregiver group was significantly lower than that in the control group (p<0.001). Of the 85% of caregivers living in the city, of the 98.5 caregivers” control group resided in city. There was a significant difference between the groups in living place. The proportion of participants residing in the city center among caregivers was significantly lower than in the control group (p<0.001) While there was no difference between the groups in terms of smoking (p=1ç000), alcohol use was significantly higher in the control group (p=0.001). While 78.2% (n=104) of the caregivers had social insurance, 97.7% (n=130) of the control group had social insurance. There was a significant difference between the groups in terms of social insurance (p<0.001) (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Caregivers and Control Group |
Of the 39.8% of caregivers were the daughter-in-law of the patient. Of the 52.6% of participants were caring due to family responsibility. Of the 39.1% (n=52) caregivers stated that they had difficulty in meeting their basic needs during their hospital stay. All caregivers stated that they were responsible for maintenance at all hours of the day. The duration of patient care was 1–4 years in 50.4% (n=67) of the caregivers. While 68.9% (n=82) of the caregivers felt sufficient in the care, 86.5% (n=115) of the caregivers stated that they were satisfied with the care. 37.6% (n=47) of caregivers felt the need for counseling on care. The most difficult situation in care (48.1%) was compliance with the diet. 74.4% (n=99) of the caregivers cared for the patient alone. 70.7% (n=94) of caregivers felt the need for assistance in care (Table 2).
 |
Table 2 Care-Related Characteristics of Caregivers |
The mean ZBI score of the caregivers was. 47.0±16.4 (min=6, max=79). According to the ZBI score, 46.6% of the caregivers had a moderate care burden and 21.8% had a heavy caregiver burden. The mean ZBI score of caregivers with low education levels was 50.6±14.2, and the average ZBI score of those with high education levels was 38.7±18.3. Caregivers with low levels of education had a significantly higher ZBI score (p<0.001) (Table 3).
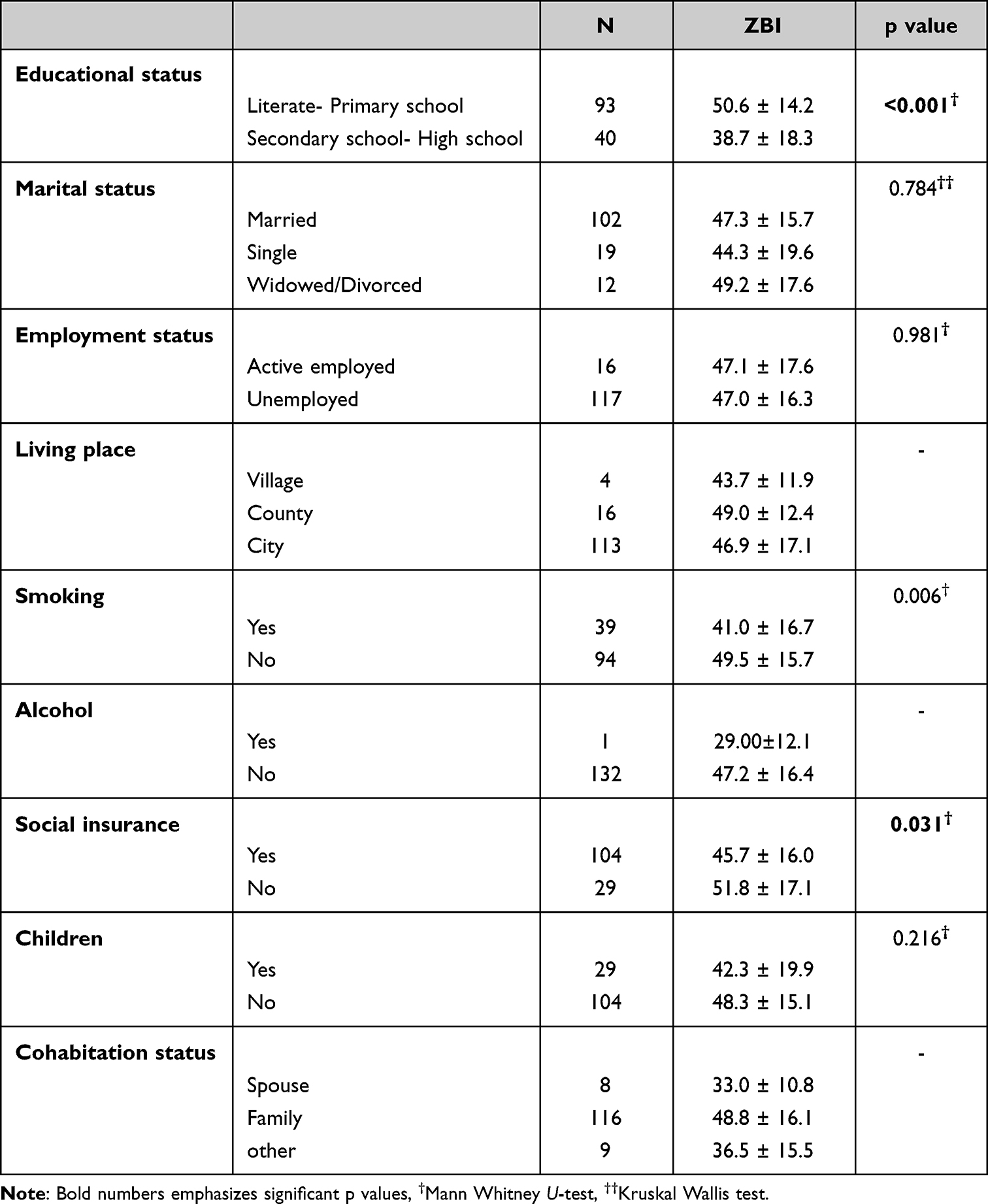 |
Table 3 The Relationship Between ZCBS and Socio-Demographic Factors in Caregivers |
The ZBI score of the caregivers who smoked was 41.0 ± 16.7, and the score of non-users was 49.5 ± 15.7. The ZBI score of those with social insurance was 45.7 ± 16.0, and the score of those without social insurance was 51.8 ± 17.1. Those with social insurance had significantly lower scores than those without a ZBI score (p=0.031) (Table 3).
The ZBI score was 47.2 ± 16.3 for those with family responsibilities, 43.9 ± 17.3 for those with emotional ties, 58.4 ± 14.6 for those with no one to care, 46.0 ± 12.8 for those with religious beliefs. The ZBI score is significantly higher in those whose reason for care is that there is no one to look after them than in caregivers for other reasons (p=0.024). The ZBI score of those who felt sufficient in care was 43.7 ± 17.4, and the score of those who felt inadequate was 52.8 ± 11.9. Those who feel adequate in care have a significantly lower ZCBS score than those who feel inadequate (p=0.010). Those who received help from other family members had a CBS score of 39.9 ± 16.9, and those who did not receive help had a ZBI score of 50.4 ± 15.1. The ZBCS score of those who getting help from other family members was significantly lower than those who did not gettinghelp others (p=0.001) (Table 4).
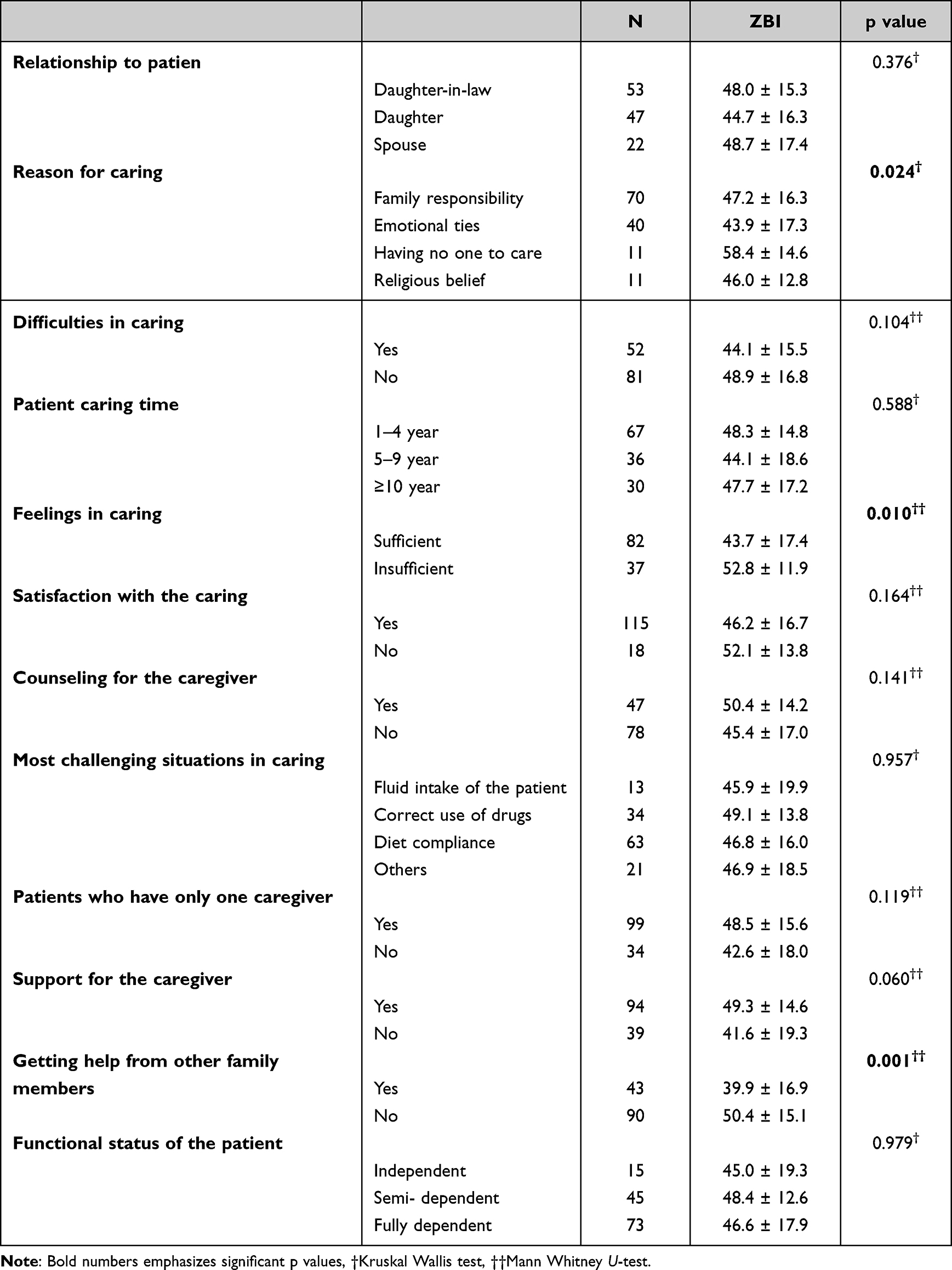 |
Table 4 Analysis of ZBI Scores According to Caring-Related Characteristics |
Life Satisfaction and Related Characteristics
SWLS score was 17.0 ± 5.4 for caregivers with low educational levels, 21.6 ± 5.5 for those with high education levels. Those with a low level of education had a significantly lower SWLS score than those with a high level of education (p<0.001). The SWLS score of active employede caregivers was 21.6 ± 6.6, and the SWLS score of nonemployed caregivers was 18.0 ± 5.6. The SWLS score of active employed caregivers was significantly higher than nonemployed caregivers (p=0.020). The SWLS score of smoking caregivers was 20.7 ± 5.7, and the SWLS score of non-smoking caregivers was 17.4 ± 5.6. The SWLS score of the smoking caregivers was significantly higher than that of non-smoking caregivers (p=0.003). Among caregivers, the SWLS score did not differ significantly according to marital status (p=0.873), social insurance (p=0.081) and child presence (p=0.277). Since the number of participants in the subgroups of the living place and cohabiting status was very small, they were not included in the analysis (Table 5).
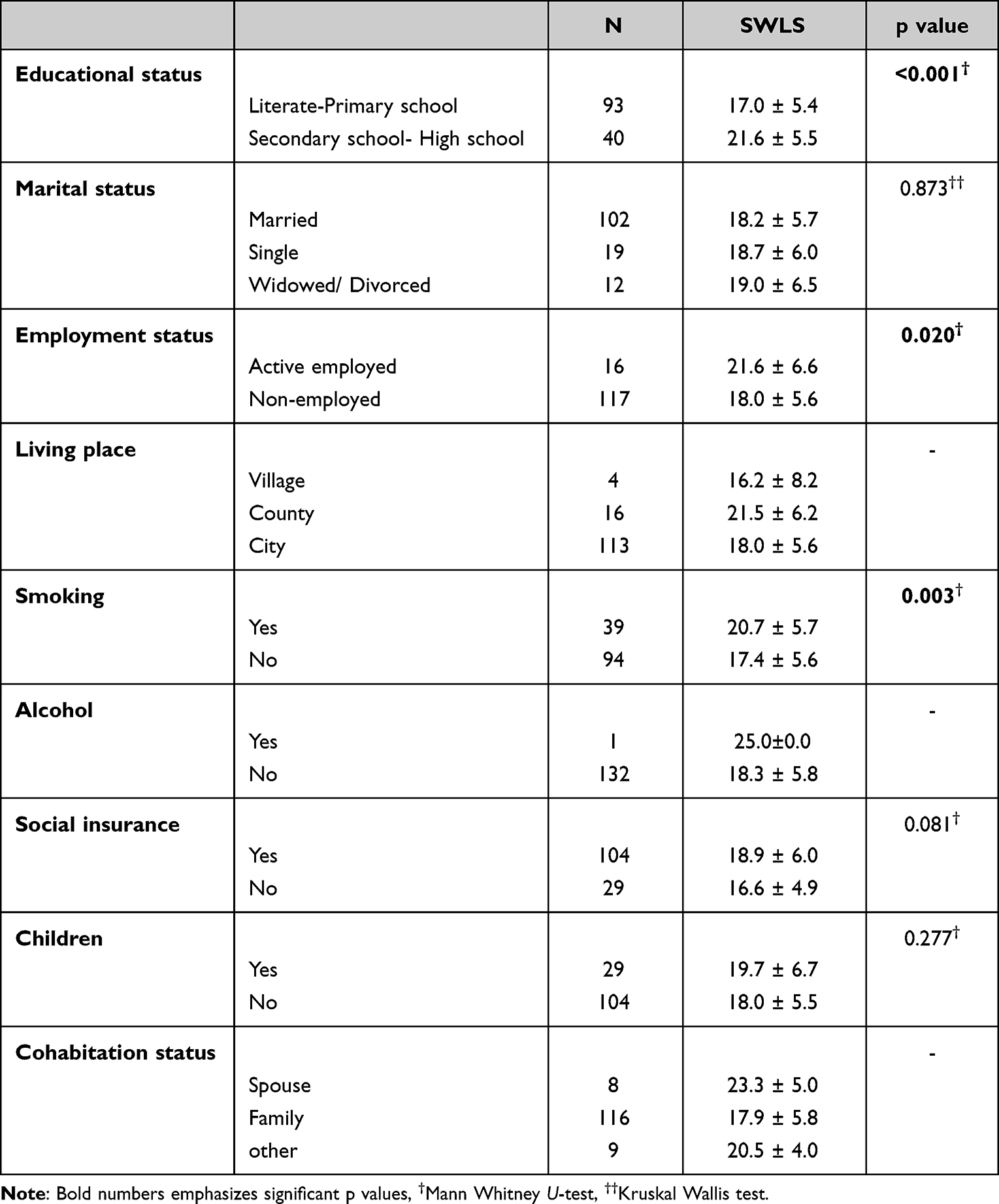 |
Table 5 The Relationship Between SWLS Scores and Socio-Demographic Factors in Caregivers |
Among the features related to care with the SWLS scorerelationship to the patient (p=0.187), reason for caring (p=0.566), difficulties in caring (p=0.141), duration of patient caring (p=0.402), feeling adequate in caring (p=0.111), satisfaction with caring (p=0.607) counseling for the caregiver (p=0.683), most difficultsituations in caring (p=0.398), being the only one caregiver(p=0.261), counselingin caring (p=0.178), getting help from other family members (p=0.148) and the patient’s functional status (p=0.545) were not found to be related (Table 6). The SWLS score of the caregivers was significantly lower than that of the control group (p<0.001) (Table 7).
 |
Table 6 Analysis of SWLS Scores Based on Characteristics Associated with Caring |
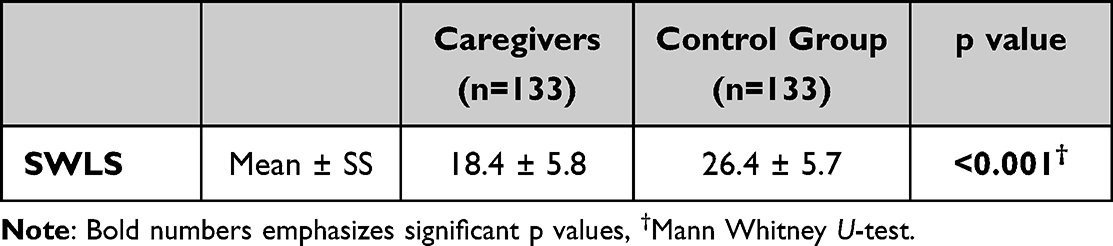 |
Table 7 Distribution of SWLS Scores in Caregivers and Control Groups |
The mean SWLS score was 18.4 ± 5.8 in caregivers and 26.4 ± 5.7 in the control group (Figure 1).
 |
Figure 1 Distribution of SWLS scores in caregivers and control groups. |
There was no significant correlation between the age of the caregivers and their SWLS (p=0.583) and ZBI (p=0.186) scores. A significant negative correlation was observed between the SWLS scores and the ZBI scores of the caregivers (rho=−0.635, p<0.001) (Figure 2).
 |
Figure 2 Correlation between ZBI and SWLS score in caregivers. |
Discussion
In our study, it was seen that the burden of care was high in those who cared for patients who received home health services. In addition, as the burden of care increased in caregivers, life satisfaction assessed by the SWLS decreased.
In the study conducted by Danaci and Koc,13 caregiver burden and life satisfaction were evaluated in patients admitted to the emergency department, and the high level of education of caregivers and actively re associated with high life satisfaction, similar to our findings. On the other hand, our study found that life satisfaction was not affected by care-related characteristics. Since the disease severity of patients receiving home health care is high, they are often functionally dependent and the duration of care covers every hour of the day, the relationship between care-related characteristics and life satisfaction may not be clearly understood. However, the correlation between the burden of care and life satisfaction provided more comprehensive information on this subject.
In a 2018 study by Sandstedt et al14 caregivers of amyotrophic lateral sclerosis patients were evaluated. Quality of life and life satisfaction were observed to be below the reference values in 49 caregivers. In the study, it was seen that the age, gender, depression, or anxiety of the caregiver were effective in the life satisfaction of the caregivers. Due to the low quality of life and life satisfaction of caregivers, it has been reported that caregivers should be taken into consideration in the planning of health services and supports to be provided.
In our study, it was observed that life satisfaction was higher in those with high education levels and in those who were actively employed. Results similar to our findings have previously been reported in different caregivers.
In the study of Erkan et al,15 it was reported that the burden of care in individuals receiving home health services was often at the intermediate-advanced level.
Liu et al16 reported that sleepiness was a common physical problem for caregivers, and some of them had moderate-to-severe depression and anxiety. A lower functional status of the patient was associated with higher caregiver burden. Furthermore, they reported poorer physical status compared with before caregiving began, lower life satisfaction, and higher degrees of depression and anxiety were associated with higher caregiver burden.
In line with the study conducted by Karakas and Pehlivan,17 it was reported that the ZBI score was 42.8 ± 16.2 similar to our study.
In the study conducted by Tayaz and Koc,18 the ZBI score of the caregivers of the patients staying in the care and rehabilitation centers was 29.4 ± 9.8.
In our study, it was observed that the care burden score of the caregivers of the patients who were given home health services was 47.0 ± 16.4. Meanwhile, in our study, it was not examined that the burden of care decreased in individuals receiving home health-care services. However, advanced monitoring of caregiver burden in a significant number of caregivers indicates that home health care serves the right population.
In the study of Oedekoven et al,19 it was reported that the burden of care was lower in caregivers with a high level of education. In those with a low level of education, the low level of knowledge required for care may be associated with an increased burden of care. Not knowing how to deal with the negativity caused by care can again lead to an increase in the burden of care. In addition, in our study, it was observed that the burden of caregivers was higher in those who did not have social insurance. The lack of social insurance can be an indicator of a low economic level. Therefore, difficulties in meeting maintenance, which incurs a significant cost, may have increased the burden of care.
Limitation
Our study was limited to our patients and caregivers who were registered in the home health-care service unit by applying to our hospital. In addition, there are only female caregivers in our study.
Conclusion
Care burden and satisfaction with life were at a moderate level. Education level and social insurance status were significantly correlated with care burden. In line with the results of the analysis, the burden of care was greater in those with low levels of education, those without social insurance, those who felt inadequate in care, and those who did not receive help from other family members. There is a negative relationship between care burden and life satisfaction. Individuals who have risk factors for the burden of care, such as feeling inadequate in care and lack of social insurance, should be identified and these individuals should be supported before the negative effects of the burden of care arise. By reducing or preventing the burden of care, the life satisfaction of caregivers can be increased, and the care provided to patients can be improved by supporting caregivers.
Acknowledgment
Thanks to all participants. Informed consent was obtained from all individual participants included in the study.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Isik K, Erci B. Life satisfaction and care burden of caregivers who provide care at home to elderly patients and the influencing factors. Turkiye Klinikleri J Nurs Sci. 2018;10(1):11–17. doi:10.5336/nurses.2017-55380
2. Adib-Hajbaghery M, Ahmadi B. Caregiver burden and its associated factors in caregivers of children and adolescents with chronic conditions. Int J Community Based Nurs Midwifery. 2019;7(4):258–269. doi: 10.30476/IJCBNM.2019.73893.0.
3. Tekin C. Developments in the field of home patient care services. FU Med J Health Sci. 2018;32(2):115–117.
4. Ugur HG, Erci B. The effect of home care for stroke patients and education of caregivers on the caregiver burden and quality of life. Acta Clin Croat. 2019;58(2):321–332. doi:10.20471/acc.2019.58.02.16
5. Sharif SI, Al-Harbi AB, Al-Shihabim AM, Al-Daour DS, Sharif RS. Falls in the elderly: assessment of prevalence and risk factors. Pharm Pract (Granada). 2018;16(3):1206. doi:10.18549/pharmpract.2018.03.1206
6. Dong HJ, Larsson B, Dragioti E, Bernfort L, Levin LA, Gerdle B. Factors associated with life satisfaction in older adults with chronic pain (PainS65+). J Pain Res. 2020;13:475–489. doi:10.2147/JPR.S234565
7. Celik SS, Celik Y, Hikmet N, Khan MM. Factors affecting life satisfaction of older adults in Turkey. Int J Aging Hum Dev. 2018;87(4):392–414. doi:10.1177/0091415017740677
8. Kalayci I, Ozkul M. An evaluation in terms of companion actors’ life satisfaction, maintenance, burden and burnout levels and related factors (SDU Research and Application Hospital). Turk Stud. 2018;13 10 :417–446. doi:10.7827/TurkishStudies.13515
9. Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980;20(6):649–655. doi:10.1093/geront/20.6.649
10. Inci FH, Erdem M. Validity and reliability of the Burden Interview and its adaptation to Turkish. J Nursology. 2008;11(4):85–95.
11. Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49(1):71–75. doi:10.1207/s15327752jpa4901_13
12. Dagli A, Baysal N. Adaptation of the satisfaction with life scale into Turkish: the study of validity and reliability. Electron J Soc Sci. 2016;15(59):1250–1263. doi:10.17755/esosder.75955
13. Danaci E, Koc Z. Caregiving Burden and life satisfaction among caregivers of cancer patients admitted to the emergency department. Clin Nurs Res. 2018;27(7):800–825. doi:10.1177/1054773817708083
14. Sandstedt P, Littorin S, Cröde Widsell G, et al. Caregiver experience, health-related quality of life and life satisfaction among informal caregivers to patients with amyotrophic lateral sclerosis: a cross-sectional study. J Clin Nurs. 2018;27(23–24):4321–4330. doi:10.1111/jocn.14593
15. Erkan H, Altuntus M. Evaluation of care burden for the patients receiving home health care. Ankara Med J. 2019;3:591–601. doi:10.17098/amj.624528
16. Liu S, Li C, Shi Z, et al. Caregiver burden and prevalence of depression, anxiety and sleep disturbances in Alzheimer’s disease caregivers in China. J Clin Nurs. 2017;26(9–10):1291–1300. doi:10.1111/jocn.13601
17. Karakas N, Pehlivan E. Care burden and quality of life of home caregivers. Med Science. 2020;9(3):714–720. doi:10.5455/medscience.2020.02.016
18. Tayaz E, Koc A. Evaluation of the relationship between perceived burden of care and quality of life in caregivers of disabled individuals. Bakirkoy Med J. 2018;14:44–52. doi:10.5350/btdmjb.20160726012929
19. Oedekoven M, Amin-Kotb K, Gellert P, Balke K, Kuhlmey A, Schnitzer S. Associations between informal caregivers’ burden and educational level. GeroPsych J Gerontopsychology Geriatr Psychiatry. 2019;32(1):19–29. doi:10.1024/1662-9647/a000199
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.