Back to Journals » Journal of Pain Research » Volume 19
CARE – A Retrospective, Dual-Cohort, 24-Week Real-World Study from the German Pain e-Registry on the Effectiveness and Safety of CBD-Dominant Oral Cannabis Extracts versus THC/Dronabinol in Older Patients with Chronic Pain
Authors Überall MA ![]() , Müller-Schwefe PCG
, Müller-Schwefe PCG ![]() , Küster MA, Müller-Schwefe GH
, Küster MA, Müller-Schwefe GH
Received 4 July 2025
Accepted for publication 17 February 2026
Published 7 March 2026 Volume 2026:19 551457
DOI https://doi.org/10.2147/JPR.S551457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Michael A Überall,1 Philipp Christian Gerhard Müller-Schwefe,2 Michael A Küster,3 Gerhard HH Müller-Schwefe2
1IFNAP – Private Institute of Neurological Sciences; O. Meany-MDPM GmbH, Nürnberg, 90411, Germany; 2Interdisciplinary Center for Pain & Palliative Care Medicine, Göppingen, 76033, Germany; 3Interdisciplinary Center for Pain & Palliative Care Medicine, Bonn, 53177, Germany
Correspondence: Michael A Überall, Private Institute of Neurological Sciences – IFNAP, Center of Excellence in Health Care Research, Nordostpark 51, Nürnberg, 90411, Germany, Tel +49 911 21773760, Fax +49 911 21773761, Email [email protected]
Background: Pharmacological treatment of chronic pain in older adults presents a therapeutic challenge. The severity of symptoms contrasts with the risk–benefit ratio of available drugs, especially in the presence of comorbidities and polypharmacy. This underlines the need to evaluate alternative therapies such as cannabis-based medicines (CBM).
Objective: To assess the safety, tolerability and effectiveness of cannabidiol (CBD)-dominant full-spectrum extracts (CBD > tetrahydrocannabinol [THC]) versus pure THC/dronabinol (THC/DRO) in patients aged ≥ 65 years with chronic or refractory pain.
Methods: Retrospective, longitudinal, exploratory analysis of anonymized data from the German Pain e-Registry. Two propensity-score-matched cohorts of 484 patients each were evaluated over ≥ 24 weeks. The primary composite endpoint required no discontinuation due to an adverse drug reaction (ADR) AND a clinically relevant improvement (≥ 20 mm VAS or ≥ 50% from baseline) in average 24-h pain intensity (PIX), pain-related disability (mPDI), or nighttime sleep (mPDI subitem #6). Secondary analyses covered pain intensities, daily-life functioning, quality of life, well-being and affective distress. Safety analyses included ADR frequency, spectrum, and concomitant analgesic use.
Results: Both treatments were associated with symptom relief. Greater improvements were observed with CBD > THC across all domains (all p < 0.001). ADRs were less frequent with CBD > THC (104 vs 342 events), with fewer patients affected (15.5% vs 35.7%) and lower discontinuation rates (5.6% vs 19.2%; all p < 0.001). The composite endpoint was achieved by 85.7% (CBD > THC) vs 21.9% (THC/DRO; p < 0.001; OR 21.5; RR 3.9; effect size 0.640; NNT 2).
Conclusion: In this real-world cohort of older adults with chronic pain, CBD-dominant extracts were associated with more favorable multidimensional outcomes and better tolerability than THC/DRO. Findings are exploratory and warrant confirmation in randomized controlled trials.
Trial Registration: HMA-EMA Catalogues of Real-World Data Sources and Studies. http://www. https://encepp.europa.eu/index_en, EU PAS number EUPAS1000000490.
Keywords: chronic pain, elderly, cannabis, CBD, THC, dronabinol, real-world evidence study, German pain e-registry
A Letter to the Editor has been published for this article.
A Response to Letter by Drs Qiang has been published for this article.
Introduction/Background
Persistent pain is a common and complex therapeutic challenge in older adults.1,2 While the prevalence of chronic pain increases with age,3 effectiveness and benefit-risk ratio of conventional pharmacological treatments decrease, particularly in the context of multimorbidity and polypharmacy.4,5 Non-steroidal anti-inflammatory drugs (NSAIDs) are recommended as the first-line treatment for mild to moderate nociceptive pain (frequently affecting the elderly); however, they are frequently inappropriate because of several age-related risks and comorbidities (gastrointestinal bleeding and ulceration, hypertension, heart failure, myocardial infarction, stroke, and kidney dysfunction).6 Although estimated to be better tolerated than NSAIDs, the pain-relieving effect of acetaminophen is often limited, leading to patients exceeding the recommended dosage, which in turn increases the risk of serious liver toxicity, especially in those with liver disease or malnutrition (both more common in the elderly).7 In addition, more recent data suggest increased risks of gastrointestinal, cardiovascular, and renal complications with acetaminophen in people aged ≥65 years, questioning its overall safety profile.8 Due to these disadvantages, opioid analgesics are frequently prescribed as alternatives to the elderly, but their use is a double-edged sword because their pain-relieving effects are linked to significant tolerability issues in geriatric patients (eg, opioid-induced constipation [OIC], respiratory depression, physical dependence, tolerance development, cognitive impairments, somnolence, dizziness, falls, and addiction).9,10 Antidepressants or anticonvulsants (recommended either for mixed or neuropathic pain) are also not ideal for the elderly because of a broad range of safety and tolerability concerns (eg, sedation, dizziness, delirium, cognitive impairment, anticholinergic burden, weight gain, and edema) and the risk of relevant drug-to-drug interactions.11,12
Owing to the discrepancy between insufficient (and often delayed) analgesic effects and frequent (sometimes severe and often rapid onset) adverse effects, there is a considerable need for alternative options to manage pain in the growing population of older adults worldwide.13 Against this background, cannabis-based medicines (CBMs) have gained increasing attention as adjunctive or alternative therapies for chronic pain management and are increasingly being explored as options for chronic pain in elderly patients.14,15 While research is still emerging, several potential advantages have been identified with the clinical use of cannabinoids in daily practice (eg, multimodal symptom benefit, sleep improvement, reduction of anxiety, agitation, and stress, and reduction of analgesic use), which make them a topic of interest for this population.16,17
Among the more than 100 phytocannabinoids identified to date, delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) are the two most well-known and evaluated components used for pain management.18,19 THC, the primary psychoactive compound, exerts analgesic and antispasmodic effects via CB1 receptors in the central nervous system (CNS), and its use is associated with significant risks of CNS side effects, especially in older individuals. CBD is more accurately described as a non-intoxicating cannabinoid with minimal psychotropic properties. It acts as an allosteric modulator of CB1 (including THC activity) and via multiple other receptors (eg, serotonin, vanilloid, adenosine), and is believed to modulate pain perception with a more favorable safety profile while counteracting THC-related psychoactive side effects.
Despite the increasing clinical use of both CBM types (either as monotherapy or in variable combinations), no direct comparative studies have been published on their relative efficacy and safety in older patients with therapy-resistant chronic pain so far.20 Preclinical data on the effects of CBD and THC, as well as the (few) available clinical studies, suggest that CBD/THC combinations may exert antispasmodic and analgesic effects beyond those of either compound alone.21–23 However, clinical evidence remains limited and mixed, with some studies reporting neutral or inconclusive results, underscoring the need for further investigation. Based on this background, we hypothesized that treatment with CBD-dominant CBMs would be associated with more favorable analgesic efficacy and tolerability compared to THC/dronabinol in elderly patients aged ≥65 years.
Study Objective
This study aimed to evaluate real-world clinical practice data to assess the 24-week safety, tolerability, and effectiveness of cannabidiol (CBD)-rich cannabis-based medicines (CBD > THC) compared with pure tetrahydrocannabinol/dronabinol (THC/DRO) in patients aged ≥65 years with chronic or therapy-refractory pain.
Methods
Study Design and Data Source
CARE (EU PAS registration number: 1000000490) is a non-interventional, retrospective, dual-cohort study based on anonymized real-world data from the German Pain e-Registry (GPeR). The registry, developed by the private Institute of Neurological Sciences (IFNAP) on behalf of the German Pain Association and hosted by the O.Meany-MDPM GmbH on behalf of the German Pain League, facilitates standardized documentation of pain treatments using validated patient-reported measures (PRMs).24 Data were primarily provided by patients, verified for plausibility by healthcare providers, and anonymized before analysis.
CBM-Treatments Under Evaluation
For this study, only extemporaneous oral CBM preparations were considered. Two groups were analyzed: (A) CBD-dominant extracts (CBD > THC; defined as oral cannabis-based medicines in which the documented CBD content exceeded the THC content) and (B) pure THC/dronabinol (THC/DRO). Other CBM forms (eg, THC-dominant combinations, inhaled or topical products) were excluded. Prescriptions could occur “off-label” or “no-label” in line with German regulations.
Population and Data Selection
Patients were eligible if they were aged ≥65 years, received either CBD > THC or THC/DRO, and had ≥24 weeks of documented follow-up. Exclusion criteria were palliative care and active psychiatric disease (both defined based on physician documentation and registry coding). No formal sample size calculation was performed; instead, all available eligible datasets were included.
Evaluated Parameters
The results were analyzed using standardized, scientifically validated self-report questionnaires (“patient-reported measures”, PRMs) to reflect patients’ assessments of their treatment. All parameters selected and evaluated in this study are part of the German Pain Questionnaire and German Pain Diary25 and are routinely used in Germany to document pain management and treatment response, as recommended by national pain associations and patient organizations.24
For methodological reasons, only part of the data available in the GPeR was used for the analysis: lowest (LPI), average (API), and highest (HPI) 24-hour pain intensities, each measured on a 100 mm visual analogue scale (VAS, 0–100 mm with 0 = non pain and 100 = worst pain imaginable);26 the 24-hour pain intensity index (PIX), calculated as the arithmetic mean of LPI, API, and HPI; the modified Pain Disability Index (mPDI) as a parameter for documenting pain-related impairment of activities of daily living (VAS, 0–100 mm; 0 = no disability, 100 = worst disability imaginable),27 including subscale #6 to assess pain-related sleep problems (VAS, 0–100 mm; 0 = non sleep problems, 100 = worst sleep problems imaginable); quality-of-life impairment by pain (QLIP), based on a 40 point numerical rating scale (NRS40) with 0 = worst impairment possible and 40 = no impairment;25 general wellbeing via the Marburg Questionnaire on Habitual Health Findings (MQHHF), based on a 35 point NRS (NRS35) with 0 = worst restriction possible and 35 = no restriction;28 physical and mental health via the Veterans-Rand short form 12 component scores (VR12-PCS/MCS), standardized to a mean of 50 and standard deviation of 10 in the German population;29 affective distress focusing on depression, anxiety and stress via the Depression, Anxiety-Stress Scale (DASS-21);30 CBM dosing; and the spectrum and frequency of adverse drug reactions (ADRs), including ADR-related treatment discontinuations. In addition, key demographic parameters and baseline findings (age, gender, phenotype, duration of illness, pain severity graded according to the Chronic Pain Grading Scale [CPGS],31 and concomitant analgesic medication) were included and used for propensity score–based matching to reduce confounding (see below).
Cohort Matching
To minimize confounding, propensity score matching (PSM) was applied (logistic regression including age, sex, pain phenotype, duration, severity, and co-analgesic use; nearest-neighbor, caliper 0.15, without replacement). PSM was performed in a 1:1 ratio and patients without a suitable match were excluded. After matching, covariate distribution was checked to ensure comparability.32
Handling of Missing Data
Missing values were imputed using last observation carried forward (LOCF) for non-primary endpoints and baseline observation carried forward (BOCF) otherwise. Sensitivity checks were done to exclude systematic bias due to missing data. Missing values were explored descriptively and checked for specific patterns and possible correlations with the other parameters.
Statistical Analysis
Continuous variables were summarized as mean (±SD) and categorical variables as frequencies (%). Between-group comparisons used Student’s T-test (continuous) or chi-squared test (categorical). Effect sizes were expressed as odds ratios (OR), risk ratios (RR), Cohen’s d, number needed to treat (NNT/NNH), and Phi coefficient, with 95% confidence intervals. The significance level was set at p < 0.05. Given the exploratory nature of this study, all analyses were descriptive and hypothesis-generating; Bonferroni correction for multiplicity was only performed for the primary endpoint analysis; all other tests were performed without corresponding adjustments.
All descriptive and efficacy analyses were performed using PASW Statistics (version 18.0). ADRs were coded using MedDRA (version 27.0 2024AA). If multiple diagnoses/symptoms were reported, the corresponding ADRs were split before coding, and ADR frequencies were evaluated at both patient- and event-based levels. Pharmacological measures were classified according to their main therapeutic use on the basic principle of only one descriptor of the Anatomical Therapeutic Code (ATC), comorbid conditions based on German version of 10th revision of the International Classification of Diseases (ICD-10).
Tables and graphs were rendered using Microsoft Excel® for Microsoft 365 MSO (Version 2504 Build 16.0.18730.20122).
Study Endpoints
The primary endpoint was a composite and defined as the proportion of patients who did not discontinue treatment due to an adverse drug reaction (ADR) and who achieved a clinically relevant improvement (≥20 mm on the visual analogue scale [VAS] or ≥50% reduction from baseline) in at least one of the following parameters: the composite pain index (PIX), the modified Pain Disability Index (mPDI), or pain-related sleep disturbance (mPDI subscale #6). Secondary endpoints included changes in pain intensities (LPI, API, HPI, PIX), disability in daily life, quality of life, well-being, affective distress, and the use of concomitant analgesics. Safety endpoints comprised the frequency and spectrum of ADRs, ADR-related discontinuations, dosing, and treatment duration.
Ethics
This non-interventional study was conducted in accordance with the Declaration of Helsinki and relevant national and regulatory requirements. As this retrospective study referred to depersonalized data from routine care (ie, regarding both patients and physicians or treatment facilities), no approval from an ethics committee was required. The study concept and evaluation of anonymized GPeR data were reviewed and approved by the steering committees of the German Pain Association and the German Pain League, with the latter paying particular attention to ensuring that patient rights are upheld within the framework of this study. All participants (physicians and patients) provided written informed consent prior to participation in the GPeR, authorizing the use of their anonymized data for healthcare research purposes. The study concept has been registered in the European Medicines Agency (EMA) registry for non-interventional/epidemiological studies (EUPAS identifier: EUPAS1000000490) to make this evaluation public.
Reporting
Reporting of this study followed the STROBE recommendation (Strengthening the Reporting of Observational Studies in Epidemiology) to ensure clarity, transparency, and reproducibility and to support readers in evaluating the validity of our study.33
Availability of Data, Resources and Reporting Procedures
The data supporting this analysis are derived from the German Pain e-Registry. The dataset is not publicly available but may be accessible for research purposes upon reasonable request and with permission of the German Pain League.
Results
Data Selection
Based on the in/exclusion criteria and the GPeR population on the reference date (June 30, 2024; n = 401856), 46,081 data sets (11.5%) were identified in which patients reported the first use of a CBM (Figure 1). About 12,401 (3.1%) were 65 years of age or older and provided evaluable information for at least six months thereafter using the GPeR documentation standards (enabling an assessment of safety/tolerability and efficacy of their CBM treatments according to this study concept). Of these, 2848 patients (22.9%) reported the use of CBD-dominant oral CBM, and 547 (4.4%) reported using pure THC/DRO preparations. As a result of the propensity score matching process, the data of 484 patients (17.0 and 88.5% of the available elderly CBM population) were ultimately selected for this analysis and formed study cohorts A (CBD > THC) and B (THC/DRO).
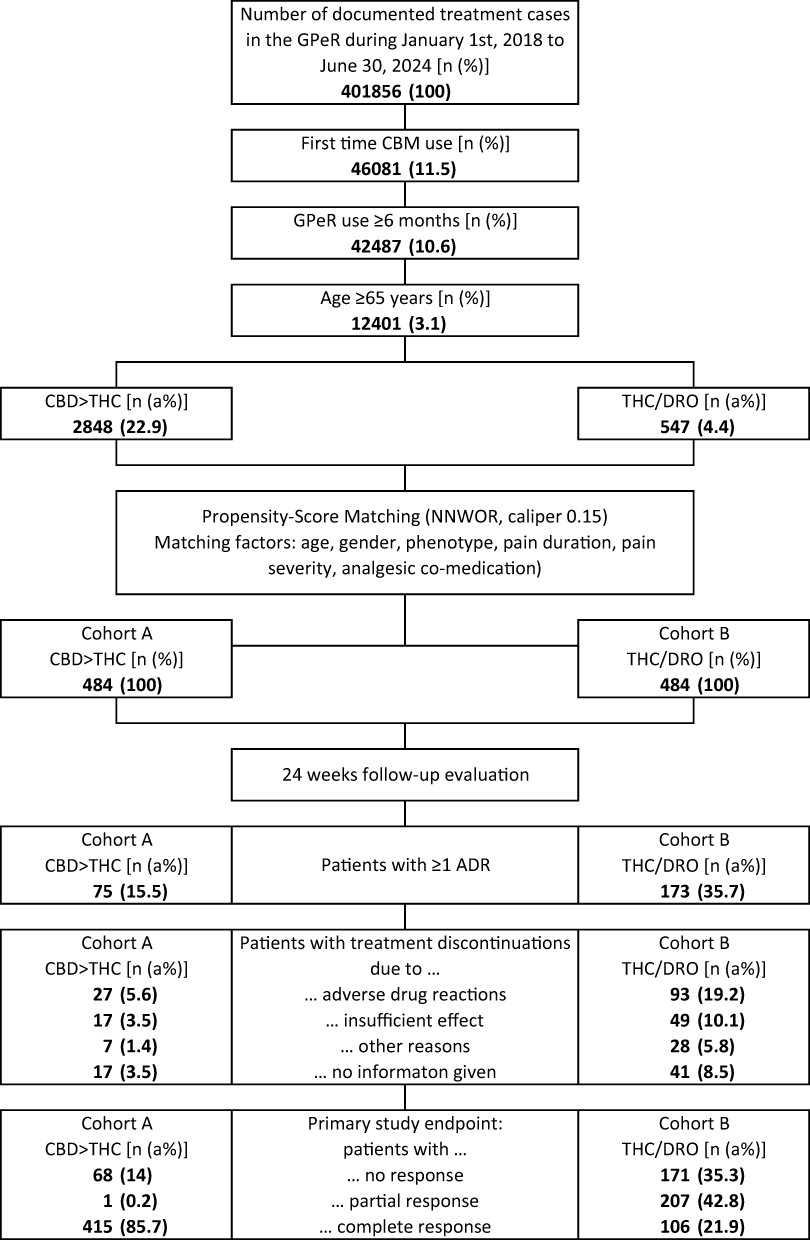 |
Figure 1 Diagram of patient data selection and flow. Abbreviations: GPeR, German Pain e-Registry; n, number, %, percent; CBM, cannabis-based medicine; CBD, cannabidiol; THC, tetrahydrocannabinol; DRO, dronabinol; a%, adjusted percent; NNWOR, nearest neighbor without replacement; ADR, adverse drug reaction. |
Patient Demographics and Non-Pain Baseline Characteristics
An overview of demographic characteristics, comorbidities, and non-pain-related concomitant therapies is presented in Table 1. The average (sd) age in cohort’s A/B was 76.0/76.1 (7.9 each) years (p = 0.986), with 71.3% (n = 345) of patients older than 70 years at the start of treatment, and 29.5% (n = 143) over 80 years. Around six out of the patients (63.6%) were female. Patients reported on average ± sd 3.8 ± 1.5 non-pain-related comorbidities and 78.7/76.7 of patients in cohort A/B documented the simultaneous existence of three or more concurrent diseases, most frequently in the circulatory/cardiovascular system (63.6/63.8%), the endocrine/metabolic system (46.5/46.1%), the musculoskeletal system (39.0/39.9%), and the respiratory system (35.7/36.8%).
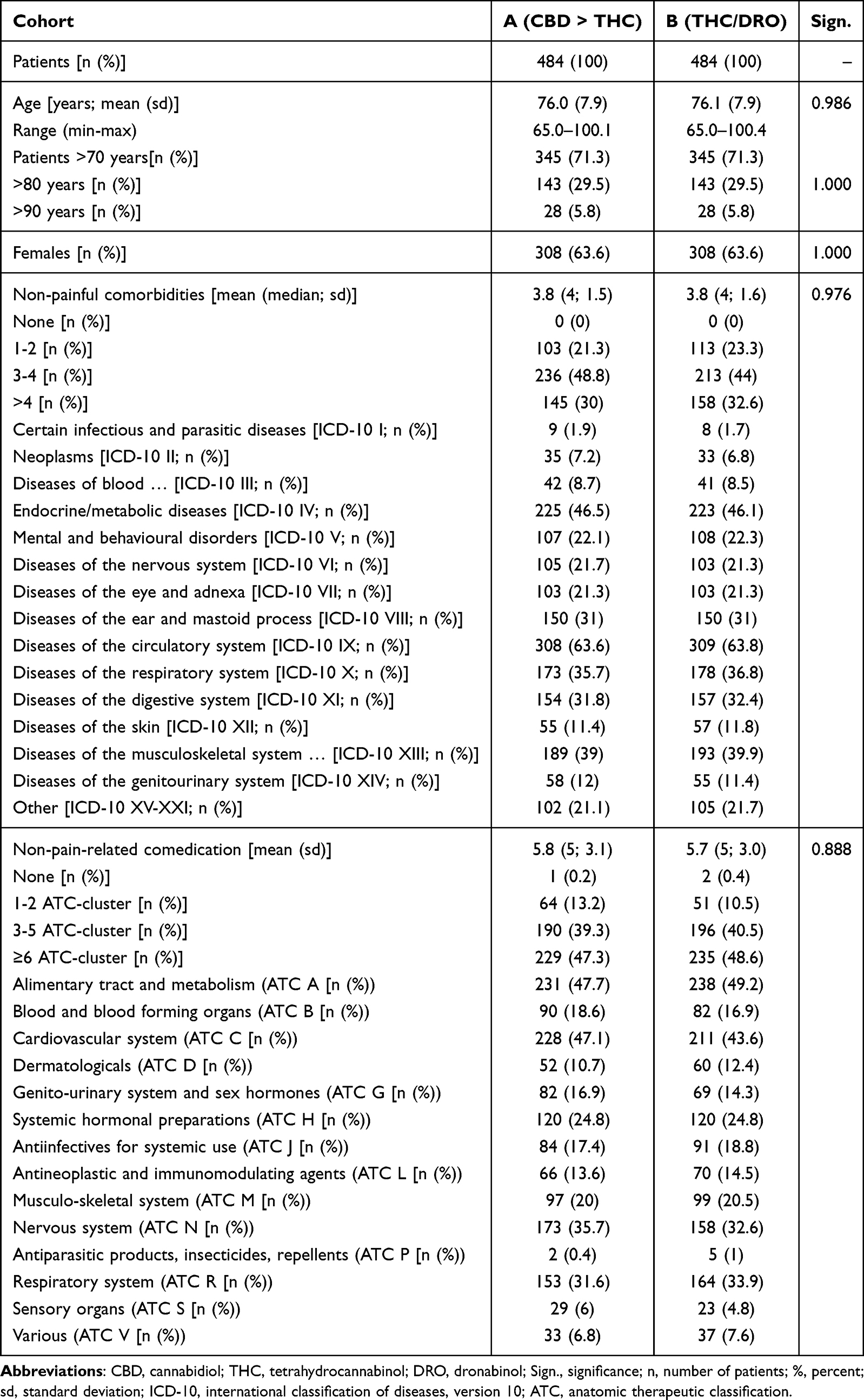 |
Table 1 Demographic and Non-Pain Baseline Characteristics |
Nearly all patients in cohort’s A/B (99.8/99.6%) reported the use of non-pain-related medications, most frequently within ATC categories A (alimentary tract and metabolism: 47.7/49.2%), C (cardiovascular system: 47.1/43.6%), N (nervous system: 35.7/32.6%), and R (respiratory system: 31.6/33.9%). With 47.3/48.6% nearly half of patients in both cohorts documented the simultaneous intake of drugs belonging to six or more different ATC-clusters. On an average (sd), patients reported the use of 5.8 (3.1)/5.7 (3.0) non-pain drugs per day.
Baseline Pain, Disease and Treatment Characteristics
Table 2 provides an overview of the relevant baseline findings for patients in both cohorts prior to treatment onset. Average (median) pain duration was 16.9 (12.0/11.5) years and patients reported on average (sd) 2.9 (1.5) body regions affected by pain, most frequently the lower back (34.1/33.5%), the back (24.4/25.8%), the abdomen (24.2/25.0%) and the hip (20.9/20.7%). Pain severity, assessed using the Chronic Pain Grading Scale (CPGS), was high: 30.0/30.4% of patients in cohort A/B documented a CPGS grade 3 and 54.1/53.7% grade 4. Pain phenotype was most frequently mixed (53.7/56.4%), followed by nociceptive (24.2/23.6%), and neuropathic (22.1/20.0%) pain syndromes. The cumulative number of analgesics and co-analgesics taken prior to CBM was 7.8 on average (median 8, sd 2.5) in both cohorts. Antidepressants were the most frequently reported prior treatment (93.6/94.0%), followed by mild opioid analgesics (MOA, 79.3/78.9%), nonsteroidal anti-inflammatory drugs (NSAIDs; 78.9% each), strong opioid analgesics (SOA; 73.6/72.9%), nonopioid analgesics (NOA; 72.9/72.5%), and anticonvulsants (69.2/68.8%). At the timepoint of treatment initiation with the index medications, patients took on average 4.9 (median 5, sd 1.8) different co-/analgesics, most frequently antidepressants (88.8/89.3%), anticonvulsants (71.5/71.7%) and strong opioid analgesics (56.2/56.4%).
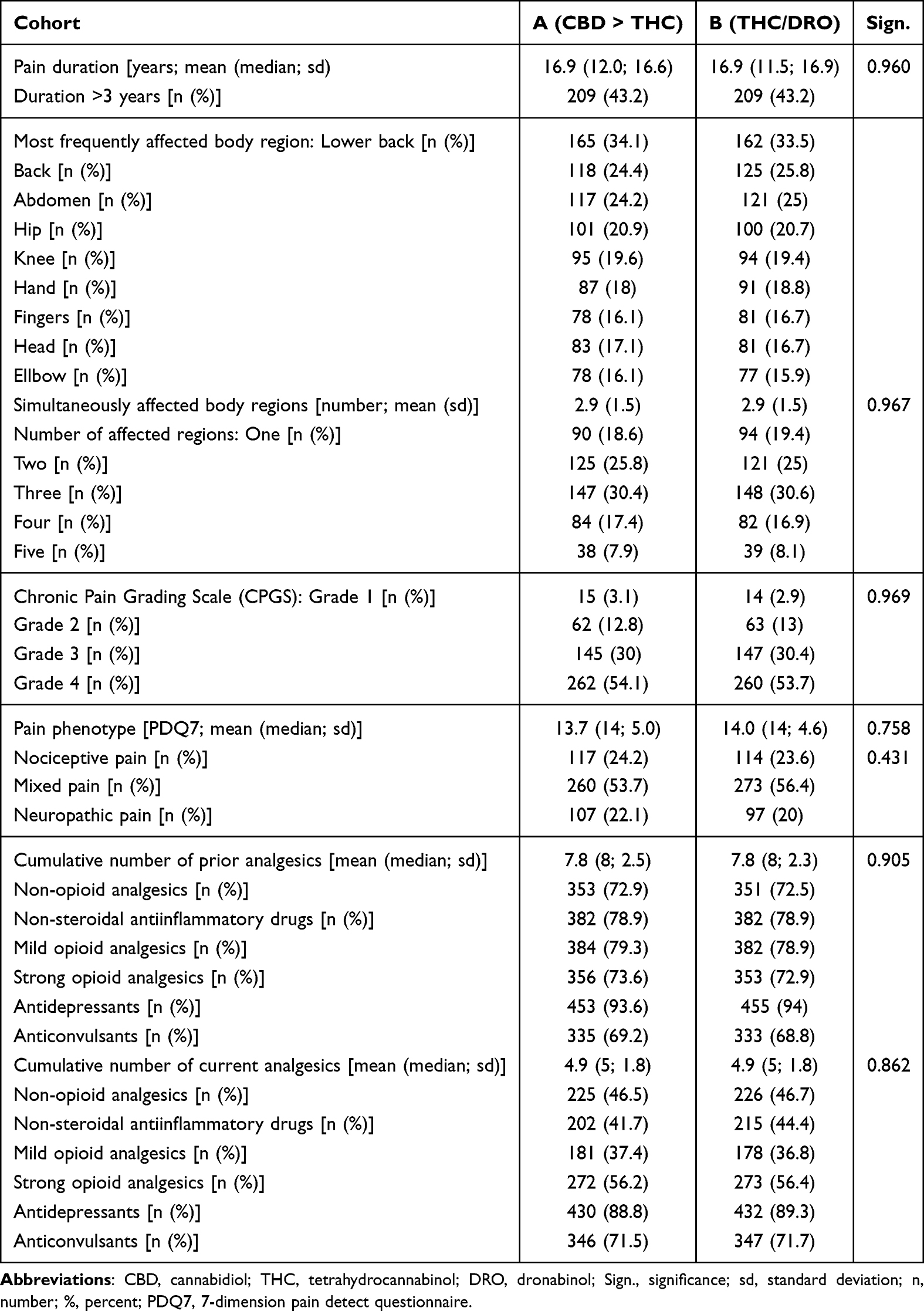 |
Table 2 Pain Phenomenology and Baseline Treatment Characteristics |
Although pain parameters were not part of the cohort matching, the PSM procedure resulted in comparable baseline values in terms of cohort means, standard deviations, and frequencies of clinically relevant abnormalities in the evaluated parameters (Table 3). Reported lowest (LPI; 26.2 mm VAS each), average (API; 54.8/54.7 mm VAS), and highest (HPI; 85.0/84.8 mm VAS) 24-hour pain intensities were significant as well and the proportion of patients with corresponding intensity values beyond established limits (LPI > 30 mm VAS: 32.9/35.3%, API > 50 mm VAS: 53.9/53.7%; HPI > 70 mm VAS: 91.9/92.6%). The 24-hour pain intensity index (PIX) relevant for the calculation of the primary endpoint was 55.3 ± 7.7/55.2 ± 7.0 mm VAS for patients in cohort A/B at baseline, and seven to eight out of ten patients in both treatment cohorts (75.8/76.4%) documented daily PIX values above 50 mm VAS.
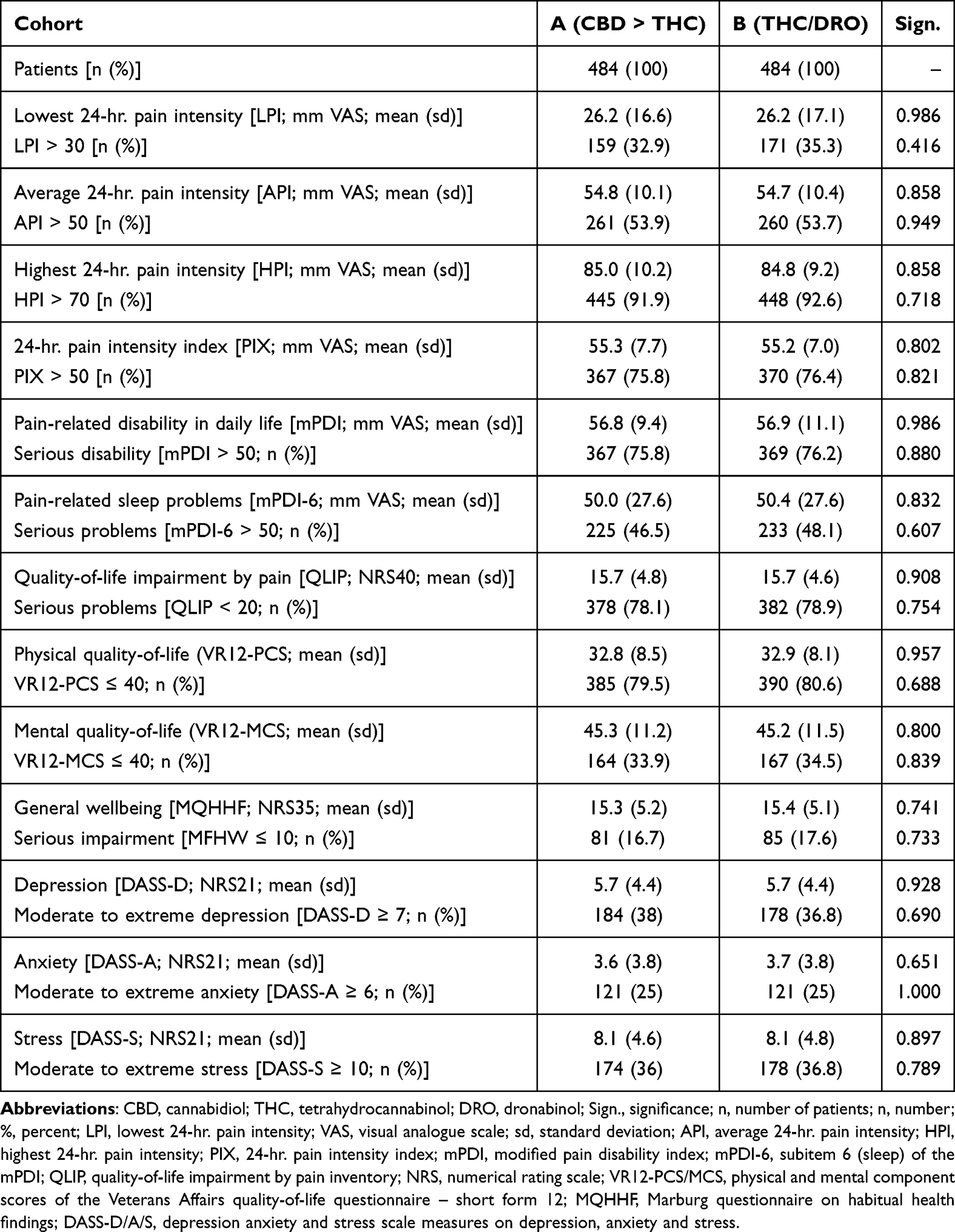 |
Table 3 Baseline Pain Characteristics |
Pain-related disabilities were significant in daily life. On average (±sd), patients in cohort’s A/B reported mPDI values of 56.8 ± 9.4/56.9 ± 11.1 mm VAS, and in 75.8/76.2% the mPDI scores above 50 mm VAS (considered indicative of severe impairments in daily life). Pain-related sleep problems were documented to be 50.0/50.4 mm VAS on average (sd 27.6 each), and with 46.5/48.1% nearly half of patients in both cohorts reported mPDI-6 scores of more than 50 mm VAS (indicating severe pain-related sleep problems).
Quality-of-life impairment by pain was significant and reported to be on average (sd) 15.7 (4.8/4.6) in both cohorts. Nearly eight of ten patients (78.1/78.9%) presented with QLIP sum scores <20, indicating serious problems. Physical quality-of-life (as assessed with the VR12-PCS) was calculated to be with 32.8/32.9, significantly impaired (79.5/80.6% of patients scored 40 or even less), as well as the mental QoL (VR12-MCS) with 45.3/45.2 (and 33.9/34.5% of patients scored ≤40).
Overall well-being was calculated to be 15.3 ± 5.2/15.4 ± 5.1 on the MQHHF, and 16.7/17.6% of patients reported serious impairments, paralleled by DASS-21 scores indicating moderate to extreme forms of either depression in 38.0/36.8%, anxiety in 25.0% each, and stress in 36.0/36.8% of patients.
CBM Treatment
Details of the CBM retention rate of patients in cohorts A and B are summarized in Table 4 and Figure 2. Until the end of the 24-week evaluation period, 62 patients in cohort A (14.0%) vs 211 in cohort B (43.6%) discontinued CBM treatment (p < 0.001; ES: 0.326, OR 4.7, RR 3.1), most frequently because of ADRs (5.6 vs 19.2%; p < 0.001; ES: 0.207), inadequate efficacy (3.5 vs 10.1%; p < 0.001; ES: 0.131), and other reasons (1.4 vs 5.8%; p < 0.001; ES: 0.116); 35/41 patients (7.2/8.5%) discontinued treatment without providing details on the reason (p = 0.001; ES 0.104).
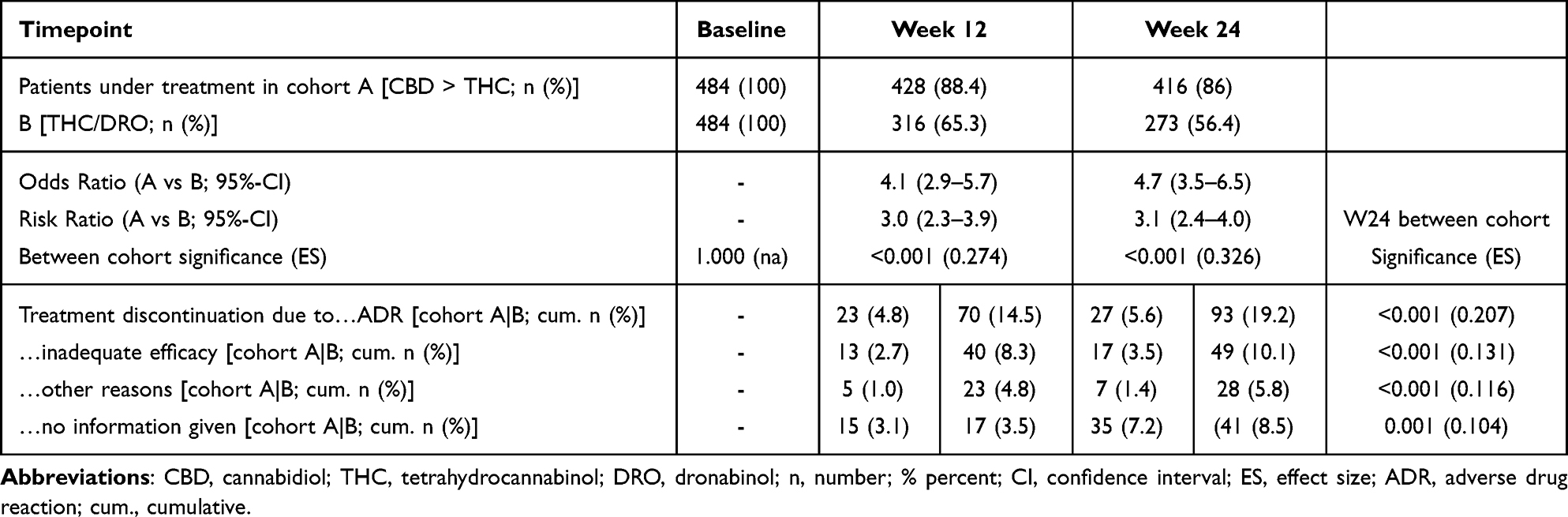 |
Table 4 Treatment Maintenance and Discontinuation Rates |
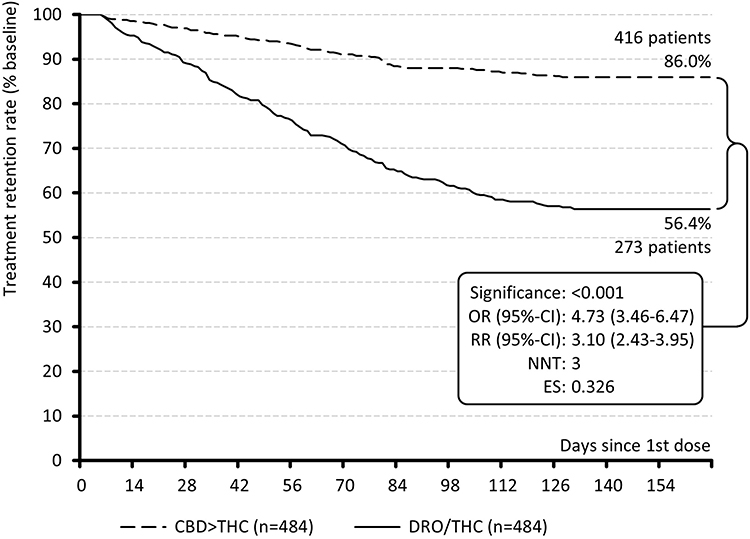 |
Figure 2 Treatment retention rate. Abbreviations: OR, odds ratio; CI, confidence interval; RR, risk ratio; NNT, number needed to treat; ES, effect size; CBD, cannabidiol; THC, tetrahydrocannabinol; DRO, dronabinol. |
Average daily THC-dose in cohort A/B was 17.2/16.2 mg at the end of week 12 (p < 0.001), and 16.2/18.6 mg at the end of week 24 (p < 0.001; ES: 0.965). Corresponding daily CBD dosages at the end of weeks 12/24 were 33.6/33.5 mg, resulting in an average calculated CBD:THC ratio of 2.1:1 in cohort A. At the end of week 24, 72.9% of patients with CBMs in cohort A reported the use of a fixed full-spectrum CBM, whereas 27.1% reported the use of a free combination of THC and CBM-containing products.
Safety and Tolerability
Overall, both CBM therapies proved to be safe. No patient evaluated in this study died from a CBM-related ADR, and regardless of their severity and potential impact on the continuation of therapy, the ADRs we evaluated were temporary and resolved spontaneously, after dose adjustment, or upon discontinuation of therapy.
Until the end of the 24-week evaluation period, 75 vs 173 patients in cohorts A vs B (15.5 vs 35.7%; p < 0.001; OR, 3.0; RR, 2.3; NNH, 5) documented a total of 104 vs 342 ADRs (see Table 5). As previously described, 27 vs 93 patients (5.6 vs 19.2%) discontinued treatment for this reason (p < 0.001; OR, 4.0; RR, 3.4; NNH, 7). Overall, most common ADRs (>2% of all patients) were dizziness (5.5%), headache (3.8%), muscle weakness (3.3%), somnolence (3.1%), euphoria (2.8%), increased appetite (2.5%) and anxiety (2.2%). Between cohort differences (A/B) were found for dizziness (1.9/9.1%), somnolence (1.2/5.0%), euphoria (1.0/4.5%), anxiety (0.2/4.1%), feeling drunk (0/2.3%; all p < 0.001), followed by concentration difficulties (0.6/2.7%; p = 0.012), increased appetite (1.2/3.7%; p = 0.013), tremors and falls (0.4/2.1%; p = 0.02), and fatigue (0.8/2.7%; p = 0.028). The organ systems most frequently affected were the nervous system with 141 ADRs (40/101) and the psychiatric system with 91 ADRs (15/76).
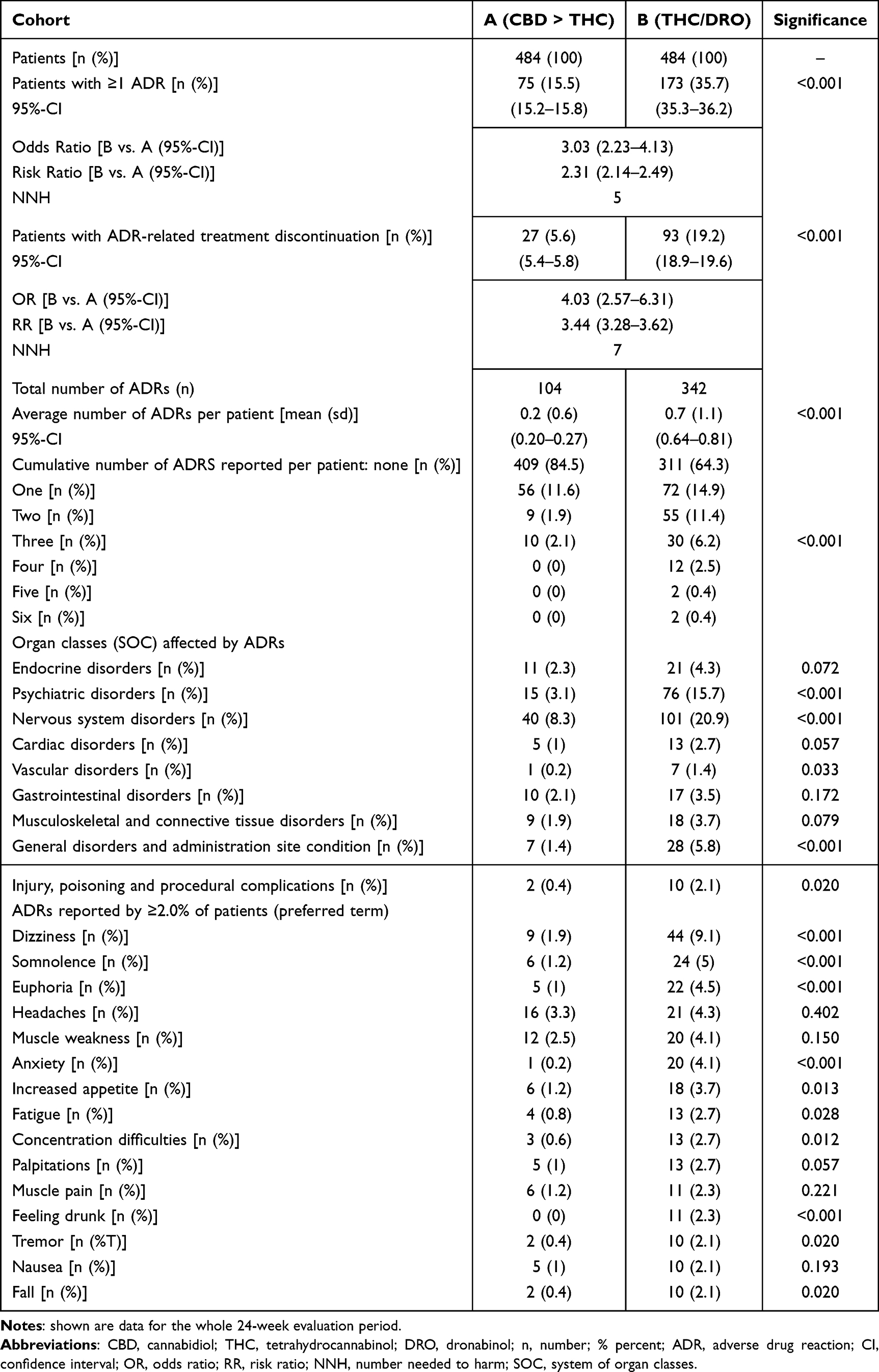 |
Table 5 Safety and Tolerability Data |
Figure 3 shows the time course of the reported ADRs (Figure 3A) and subsequent ADR-related treatment discontinuation (Figure 3B). Average (±sd) ADR manifestation in cohort A/B occurred on day 55.1 ± 31.5/68.0 ± 36.1 (median: 55/68; range: 6–126/6-131) and ADR-related treatment termination on day 62.6 ± 30.2/59.4 ± 34.4 (median: 65/58; range: 6–128/6-131).
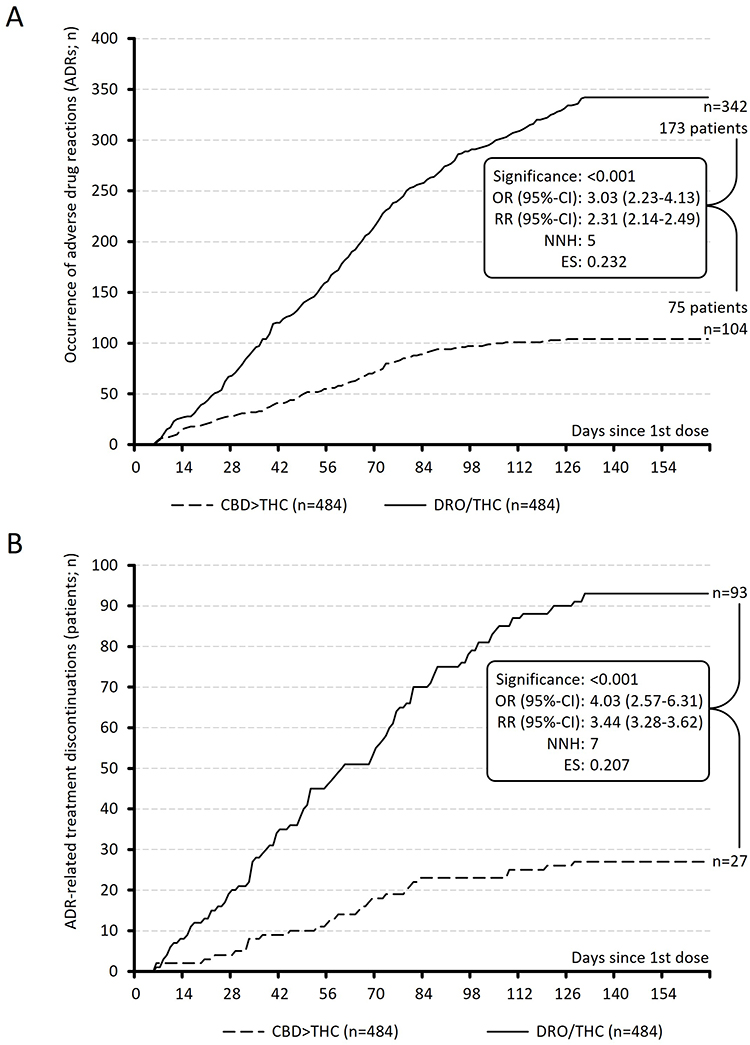 |
Figure 3 Adverse drug reactions and related treatment discontinuation rates. Abbreviations: OR, odds ratio; CI, confidence interval; RR, risk ratio; NNH, number needed to harm; ES, effect size; CBD, cannabidiol; THC, tetrahydrocannabinol; DRO, dronabinol. Notes: Upper (A): time course of the occurrence of adverse drug reactions (ADR); lower (B): time course of the ADR-related treatment discontinuations. |
Effects on Pain Intensities and Pain Phenotype
As shown in Table 6, patients in both cohorts reported significant reductions in all pain intensities compared to baseline at weeks 12 and 24. Between-cohort comparisons indicated greater improvements with CBD > THC than with THC/DRO (p < 0.001 for all). At week 24, absolute changes in LPI/API/HPI were –20.1/–33.1/–51.4 mm in cohort A and –6.4/–18.3/–26.8 mm in cohort B, corresponding to relative improvements of –76.6%/–60.5%/–60.5% vs –24.5%/–33.4%/–31.6% (all p < 0.001).
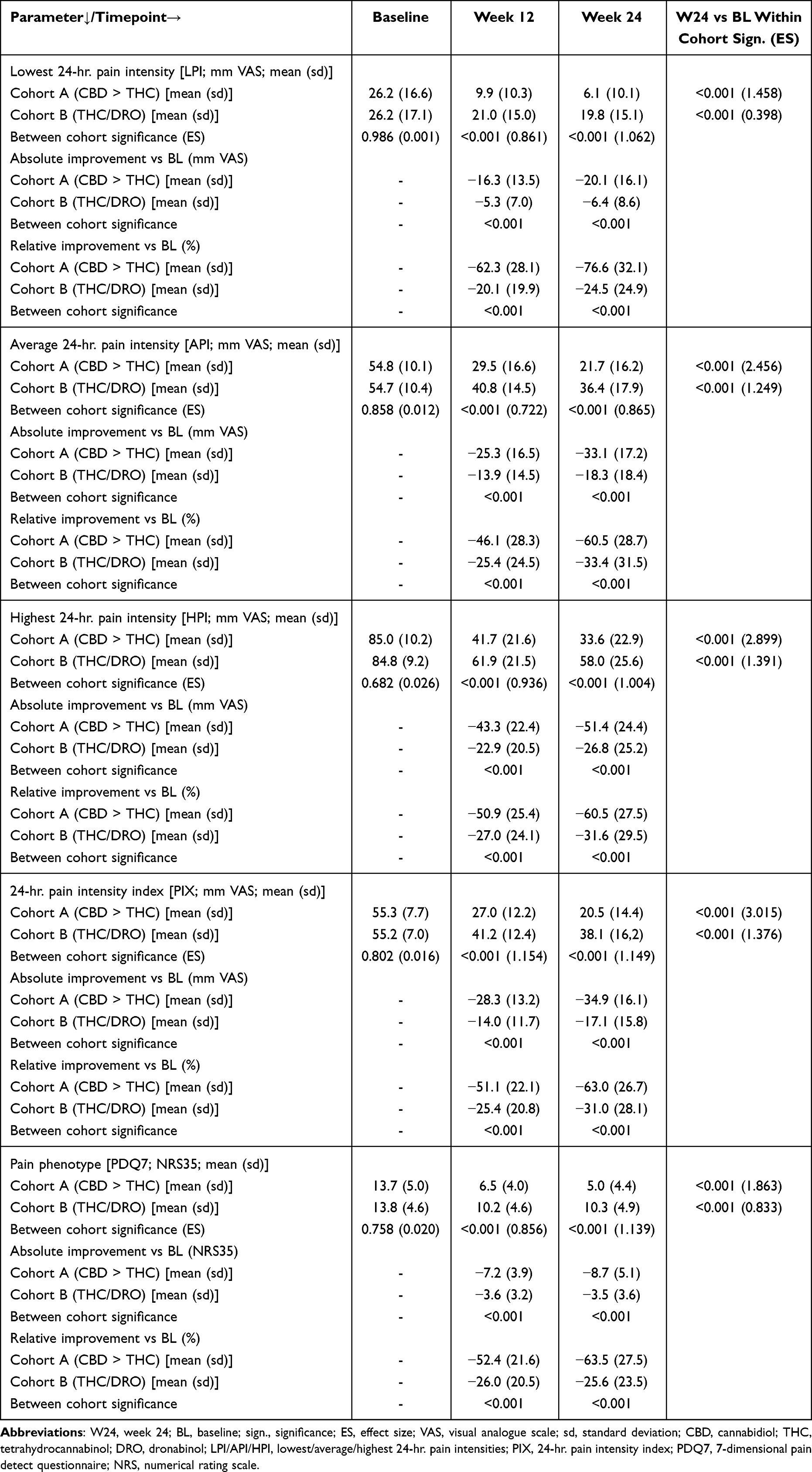 |
Table 6 Treatment Effects on Pain Intensity and Pain Phenotype |
For the 24-hour pain intensity index (PIX), baseline values were 55.3 ± 7.7 mm in cohort A and 55.2 ± 7.0 mm in cohort B (p = 0.802). At week 12, values decreased to 27.0 ± 12.2 vs 41.2 ± 12.4 mm, and at week 24 to 20.5 ± 14.4 vs 38.1 ± 16.2 mm (both p < 0.001). Absolute improvements from baseline were at week 24–34.9 vs –17.1 mm, and corresponding relative improvements –63.0% vs –31.0% (p < 0.001; ES: 3.015 vs 1.376; Figures 4 and 5). At week 24, 86.0% of patients in cohort A vs 53.9% in cohort B achieved an absolute PIX reduction ≥20 mm, and 85.1% vs 40.1% achieved a relative reduction ≥50% (both p < 0.001; Figures 4, 5B and C).
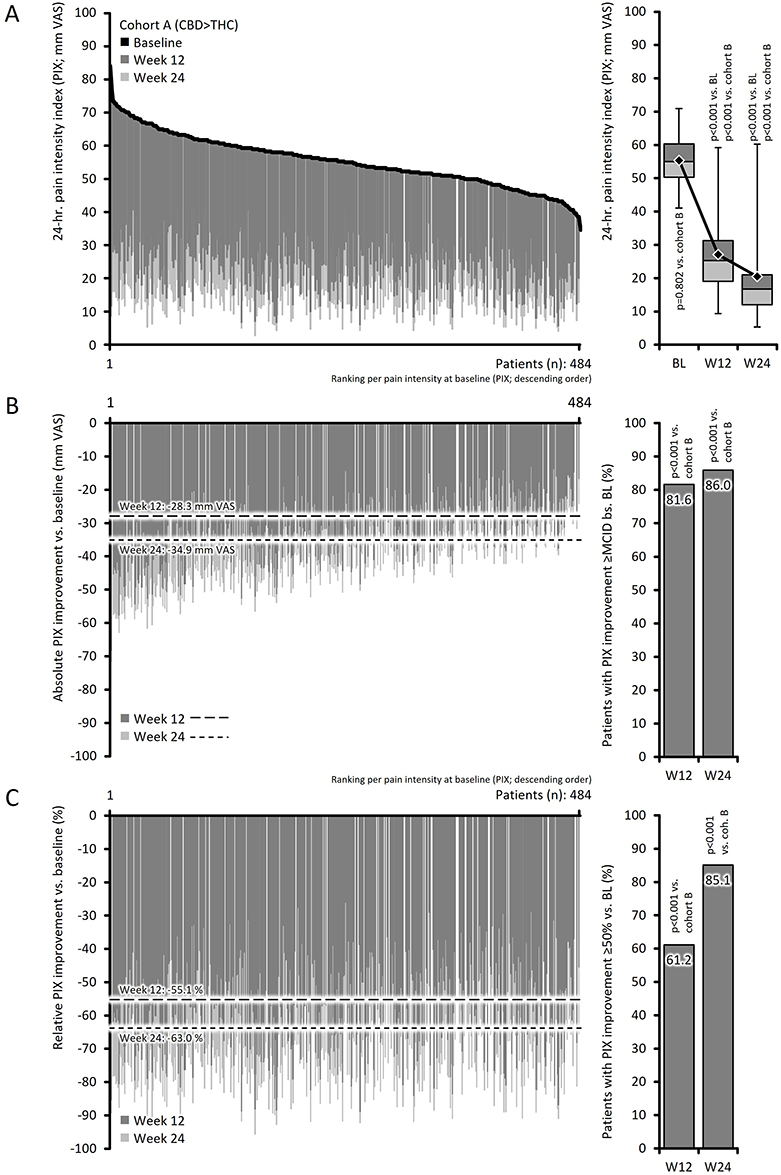 |
Figure 4 Analgesic effects of CBD > THC on 24-hr. pain intensity index (PIX). Abbreviations: PIX, pain intensity index; VAS, visual analogue scale; CBD, cannabidiol; THC, tetrahydrocannabinol; BL, baseline. Notes: Upper panel (A) – left side: change of the 24-hr. pain intensity index (PIX; mm VAS) from baseline (black line; patients ranked from left to right by descending pain intensity at baseline) to week 12 (dark grey columns) and to week 24 (light grey columns); right side: box-and-whisker plot (box: 25,50, 75% percentiles; whiskers: 2.5 and 97.5% percentiles) for PIX at baseline, week 12 and week 24 (including corresponding means shown as diamonds). Middle panel (B) – left: absolute PIX improvements until week 12 (dark grey) and week 24 (light grey) vs baseline including average changes (dashed lines); right: proportion of patients with PIX improvements ≥20 mm VAS at week 12/24. Lower panel (C) – left: relative PIX improvements; right: proportion of patients with PIX improvements ≥50% at week 12/24. |
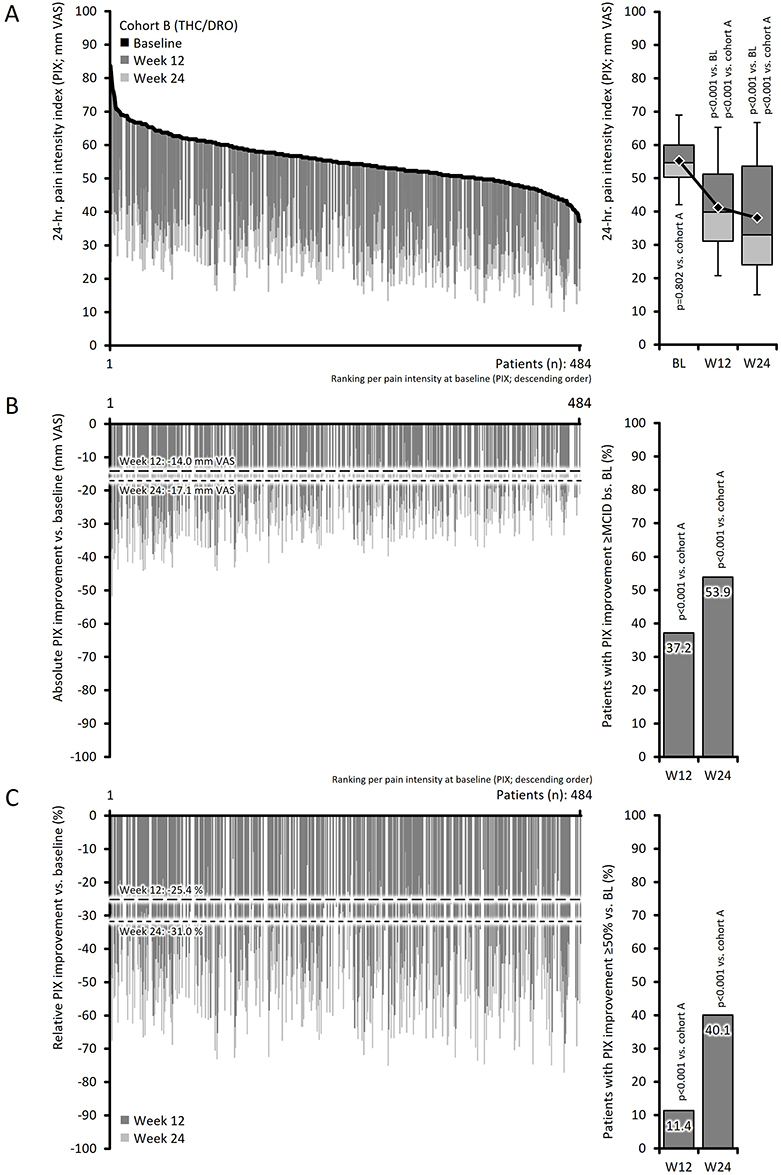 |
Figure 5 Analgesic effects of THC/DRO on 24-hr. pain intensity index (PIX). Abbreviations: PIX, pain intensity index; VAS, visual analogue scale; THC, tetrahydrocannabinol; DRO, dronabinol; BL, baseline. Notes: Upper panel (A) – left side: change of the 24-hr. pain intensity index (PIX; mm VAS) from baseline (black line; patients ranked from left to right by descending pain intensity at baseline) to week 12 (dark grey columns) and to week 24 (light grey columns); right side: box-and-whisker plot (box: 25,50, 75% percentiles; whiskers: 2.5 and 97.5% percentiles) for PIX at baseline, week 12 and week 24 (including corresponding means shown as diamonds). Middle panel (B) – left: absolute PIX improvements until week 12 (dark grey) and week 24 (light grey) vs baseline including average changes (dashed lines); right: proportion of patients with PIX improvements ≥20 mm VAS at week 12/24. Lower panel (C) – left: relative PIX improvements; right: proportion of patients with PIX improvements ≥50% at week 12/24. |
Mean (sd) PDQ7 scores, reflecting pain phenotype, decreased from 13.7 (5.0)/13.8 (4.6) at baseline to 6.5 (4.0)/10.2 (4.6) at week 12 and to 5.0 (4.4)/10.3 (4.9) at week 24 (p < 0.001 vs baseline for both; ES: 1.863 vs 0.833). Absolute and relative changes differed significantly between cohorts at each time point (p < 0.001). These shifts were accompanied by marked changes in phenotype distribution: the proportion of patients with PDQ7 values suggestive of neuropathic pain declined from 22.1%/20.0% to 3.5%/8.7%, and those with mixed phenotypes from 53.7%/56.4% to 7.6%/31.2% at week 24 (all p < 0.001).
Effects on Disability, Sleep, Quality of Life, Well-Being, and Affective Distress
Parallel to the reductions in pain intensity, patients in both cohorts reported significant improvements in pain-related disability, sleep, and quality of life (Table 7). At baseline, mean (±sd) mPDI scores were comparable between cohorts (56.8 ± 9.4 vs 56.9 ± 11.1 mm VAS; p = 0.986). By week 24, scores had decreased to 21.3 vs 39.1 mm VAS (p < 0.001 vs baseline for both; ES: 2.785 vs 1.310). Between-cohort analyses showed significantly greater absolute and relative improvements with CBD > THC (p < 0.001; ES: 1.147).
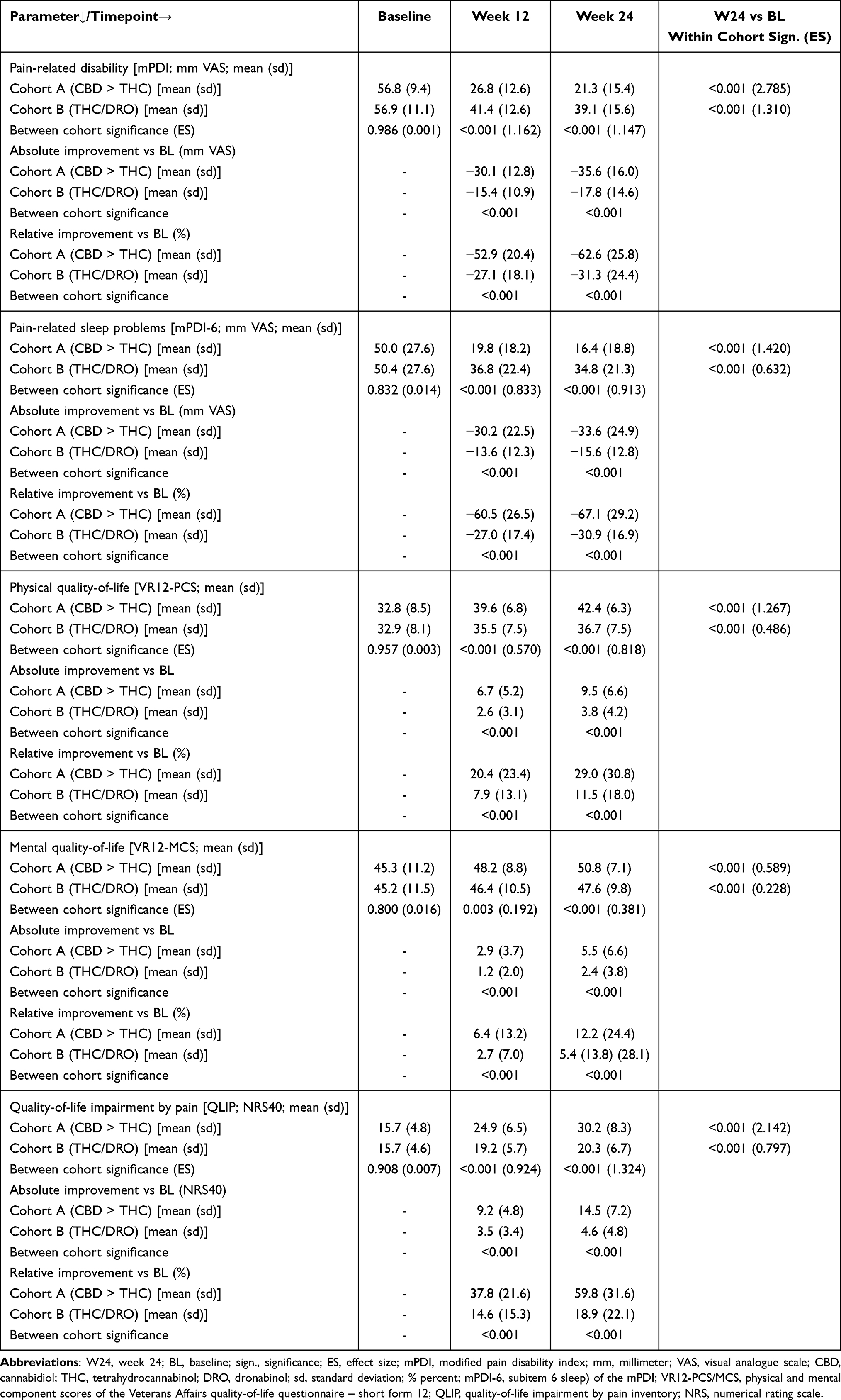 |
Table 7 Treatment Effects on Pain-Related Disability, Sleep and Quality-of-Life |
Pain-related sleep problems improved from 50.0 (±27.6) vs 50.4 (±27.6) mm VAS at baseline (p = 0.832) to 16.4 (±18.8) vs 34.8 (±21.3) mm VAS at week 24 (p < 0.001 vs baseline for both; ES: 1.420 vs 0.632). Between-group differences were significant (p < 0.001; ES: 0.913).
VR-12 physical and mental component scores were significantly below population norms at baseline (32.8 vs 32.9 for PCS, 45.3 vs 45.2 for MCS; p = 0.957 and p = 0.800). By week 24, both cohorts improved, with larger changes in the CBD > THC group (p < 0.001; ES: 0.818 for PCS and 0.381 for MCS). QLIP scores also increased significantly in both groups, with mean improvements corresponding to ES: 2.142 vs 0.797 (p < 0.001).
Effects on general well-being and affective distress are shown in Table 8. At baseline, the proportion of patients with significant impairments in well-being was 16.7% vs 17.6% (p = 0.733). Under CBM therapy, these rates decreased to 2.1% vs 6.8% at week 12 and 1.7% vs 5.4% at week 24 (p < 0.001 for both; ES: 0.101). At baseline, at least moderate depression, anxiety, and stress were present in 38.0% vs 36.8% (p = 0.690), 25.0% in both groups (p = 1.000), and 36.0% vs 36.8% (p = 0.009). By week 24, these rates decreased to 8.5% vs 20.0% for depression, 6.6% vs 16.1% for anxiety, and 7.2% vs 18.4% for stress (p < 0.001 for all within-group changes). Between-cohort differences favored the CBD > THC group (p < 0.001 for all).
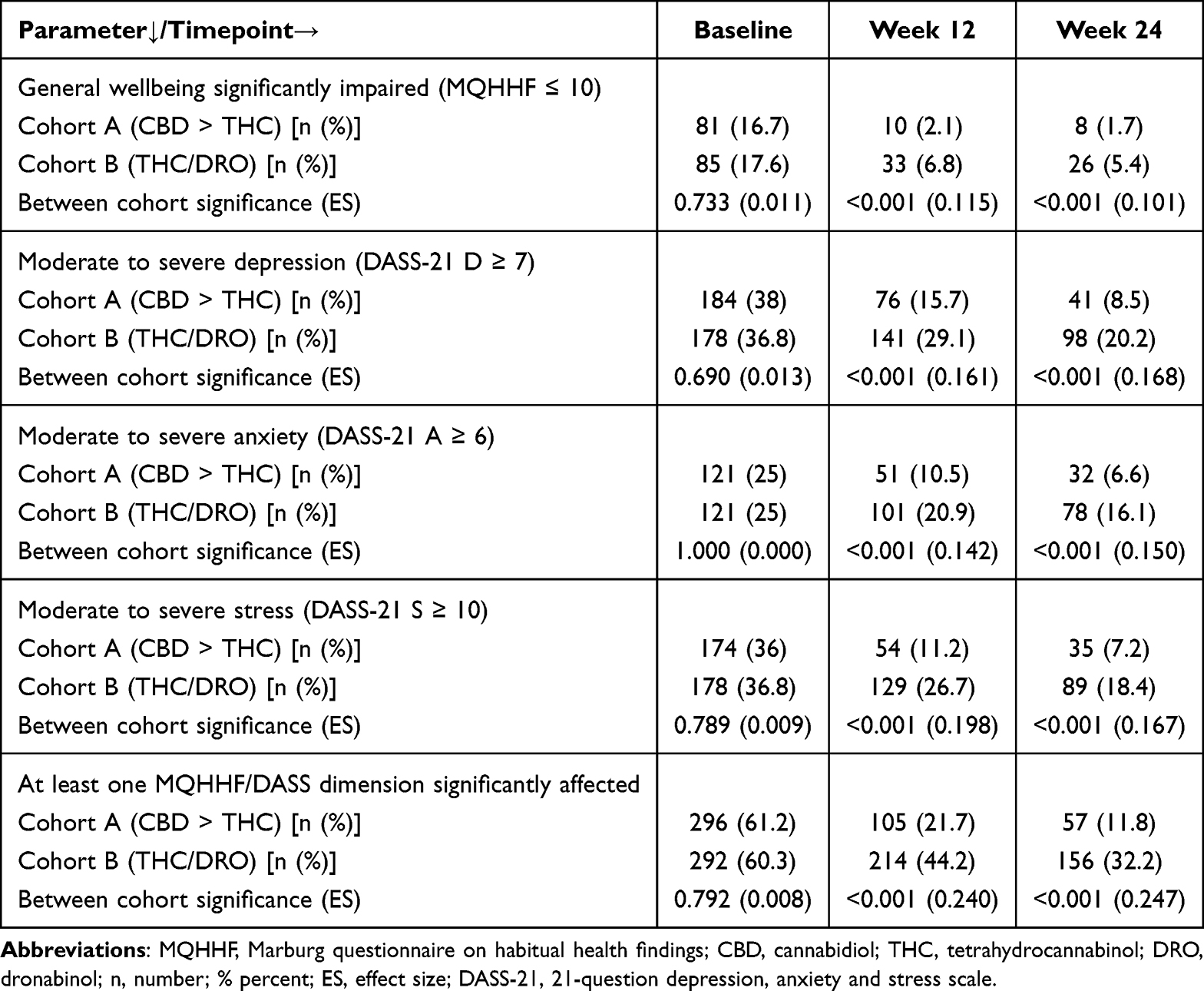 |
Table 8 Treatment Effects on Overall Wellbeing and Affective Distress |
Global Treatment Effects
Figure 6 summarizes relative improvements in pain and pain-related dimensions at weeks 12 and 24 compared with baseline. Both individual and average improvement rates differed significantly between the two treatment cohorts at both evaluation points (week 12 in Figure 6A; week 24 in Figure 6B; p < 0.001 for all parameters). Symptom relief increased further between week 12 and week 24, while between-cohort effect sizes remained comparable, averaging (±sd) 1.1 ± 0.3 at week 12 and 1.2 ± 0.4 at week 24 (Figure 6C).
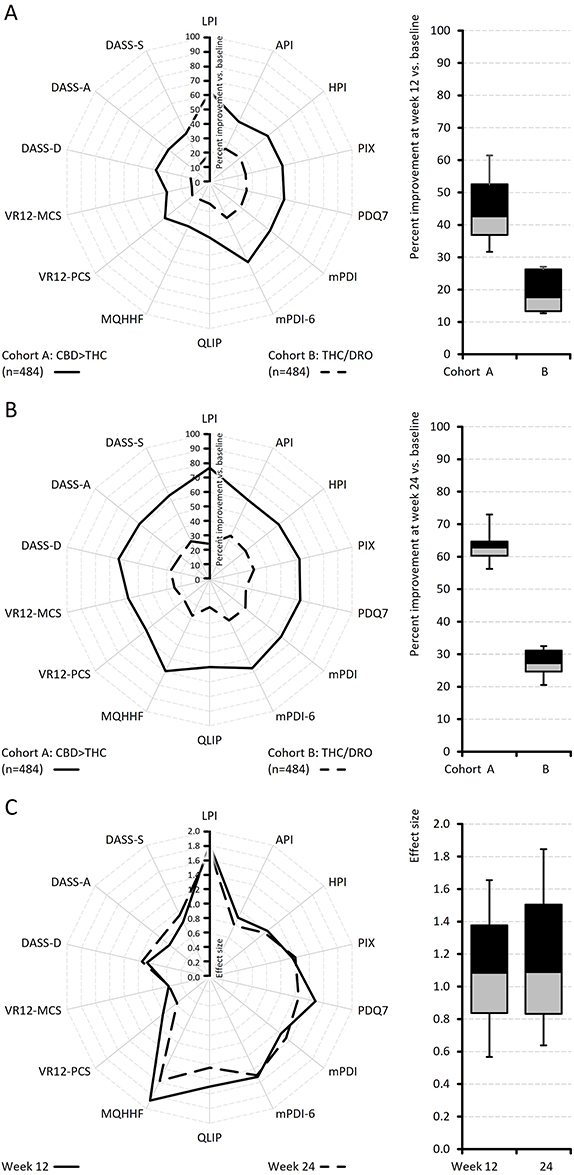 |
Figure 6 Global treatment effects. Abbreviations: LPI, lowest 24-hr. pain intensity; API, average 24-hr. pain intensity; HPI, highest 24-hr. pain intensity; PIX, 24-hr. pain intensity index; PDQ7, 7-dimensional pain detect questionnaire; mPDI, modified pain disability index; mPDI-6, subitem 6 (sleep) of the mPDI; QLIP, quality-of-life impairment by pain inventory; MQHHF, Marburg questionnaire on habitual health findings; VR12-PCS/MCS, physical and mental component scores of the Veterans Affairs quality-of-life questionnaire – short form 12; DASS-D/A/S, depression anxiety and stress scale measures on depression, anxiety and stress; CBD, cannabidiol; THC, tetrahydrocannabinol; DRO, dronabinol. Notes: Upper panel (A), left: spider graph with the percent improvements vs baseline at week 12 for both treatment cohorts; right: box-and-whisker plot (box: 25,50, 75% percentiles; whiskers: 10 and 90% percentiles) for the average improvements vs baseline. Middle panel (B), left: percent improvements vs baseline at week 24 for both treatment cohorts; right: corresponding box-plots. Lower panel (C), left: between cohort effect sizes for week 24 vs baseline improvements; right: corresponding box-plots. |
The largest between-cohort effect sizes were observed for lowest 24-hour pain intensity (LPI; 1.7 at week 12 and 1.8 at week 24), general well-being (MQHHF; 1.6/1.9), sleep disturbance (mPDI-6; 1.5/1.5), disability in daily life (mPDI; 1.3/1.3), pain phenotype (PDQ7; 1.3/1.5), and the composite 24-hr. pain index (PIX; 1.2/1.2).
Effects on Analgesic Comedication
In parallel with the reductions in pain, the use of CBM was associated with significant decreases in concomitant analgesics and co-analgesics (Figure 7 and Table 9). By week 12, 70.5% of patients in the CBD > THC cohort and 38.2% in the THC/DRO cohort had completely discontinued at least one of their baseline analgesics (Figure 7A). By week 24, these proportions increased to 86.1% vs 55.1% (p < 0.001 for within-cohort changes vs baseline and for between-cohort comparisons at both time points; Figure 7B).
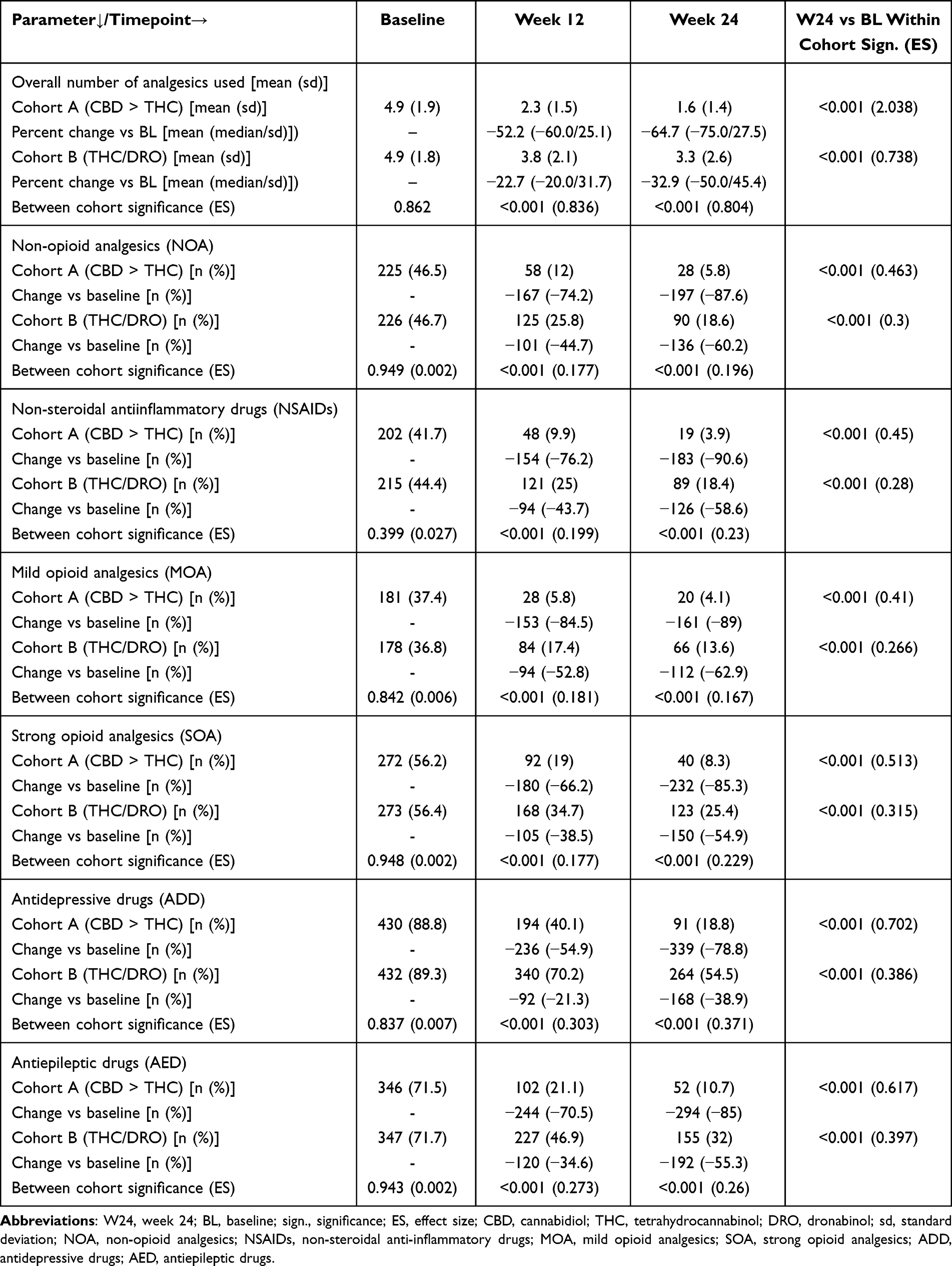 |
Table 9 Use of Analgesic Co-Medication |
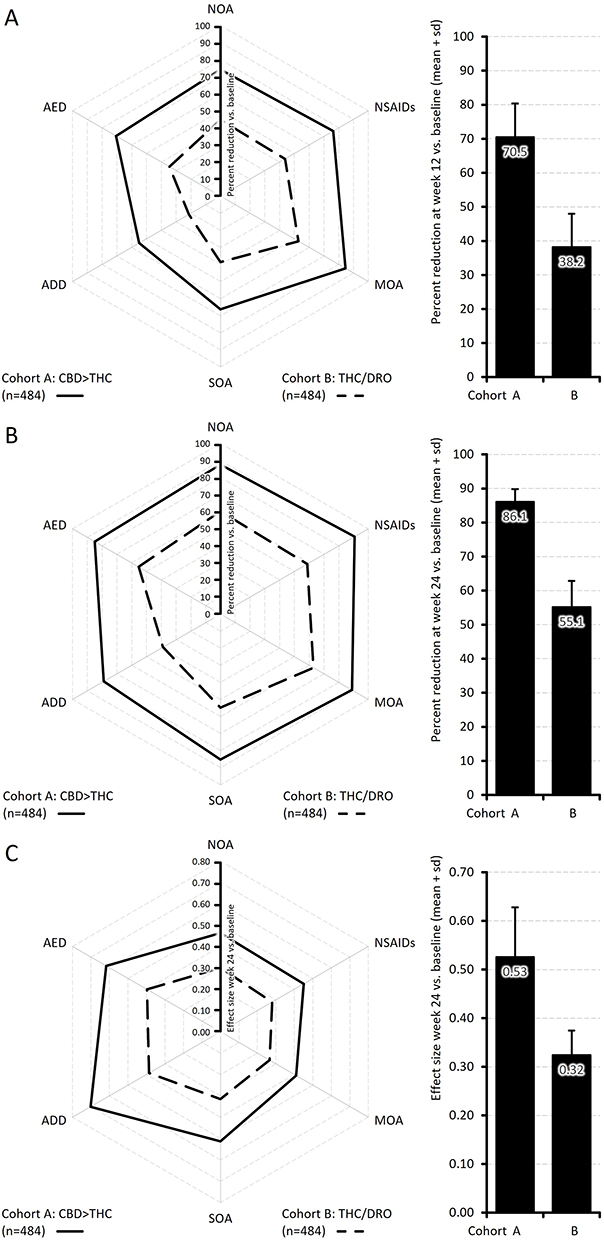 |
Figure 7 Analgesic co-medication. Abbreviations: NOA, non-opioid analgesics; NSAIDs, non-steroidal anti-inflammatory drugs; MOA, mild opioid analgesics; SOA, strong opioid analgesics; ADD, antidepressant drugs; AED, antiepileptic drugs; CBD, cannabidiol; THC, tetrahydrocannabinol; DRO, dronabinol; sd, standard deviation. Notes: Upper panel (A), left: spider graph with the percent reductions of analgesic use vs baseline at week 12 for both treatment cohorts; right: average reduction rates vs baseline. Middle panel (B), left: percent reductions vs baseline at week 24 for both treatment cohorts; right: average reduction rates vs baseline. Lower panel (C), left: between cohort effect sizes for week 24 vs baseline reductions; right: average effect sizes. |
At the end of the 24-week evaluation period, discontinuation rates in cohorts A vs B were 87.6% vs 60.2% for non-opioid analgesics, 90.6% vs 58.6% for non-steroidal anti-inflammatory drugs, 89.0% vs 62.9% for mild opioids, 85.3% vs 54.9% for strong opioids, 78.8% vs 38.9% for antidepressants, and 85.0% vs 55.3% for antiepileptics (p < 0.001 for all between-cohort comparisons).
The average (±sd) number of analgesics taken decreased from 4.9 ± 1.9 at baseline to 2.3 ± 1.5 by week 12 and to 1.6 ± 1.4 by week 24 in the CBD > THC cohort, and from 4.9 ± 1.8 to 3.8 ± 2.1 and 3.3 ± 2.6, respectively, in the THC/DRO cohort. This corresponded to relative reductions of –52.2% and –64.7% in cohort A, and –22.7% and –32.9% in cohort B (p < 0.001 vs baseline for both; ES: 2.038 vs 0.738).
Primary Study Endpoint
Based on the four primary endpoint components – (a) no ADR-related discontinuation of treatment and simultaneous documentation of a clinically relevant reduction in (b) the 24-hour pain index (PIX), (c) pain-related impairment in daily life (mPDI), and (d) pain-related sleep disturbances (mPDI-6) – the proportion (95% CI) of full responders at the end of the 24-week evaluation period was 85.7% (85.4–86.1) in cohort A vs 21.9% (21.5–22.3) in cohort B (p < 0.001; ES: 0.640; OR: 21.5; RR: 3.9; NNT: 2; Table 10).
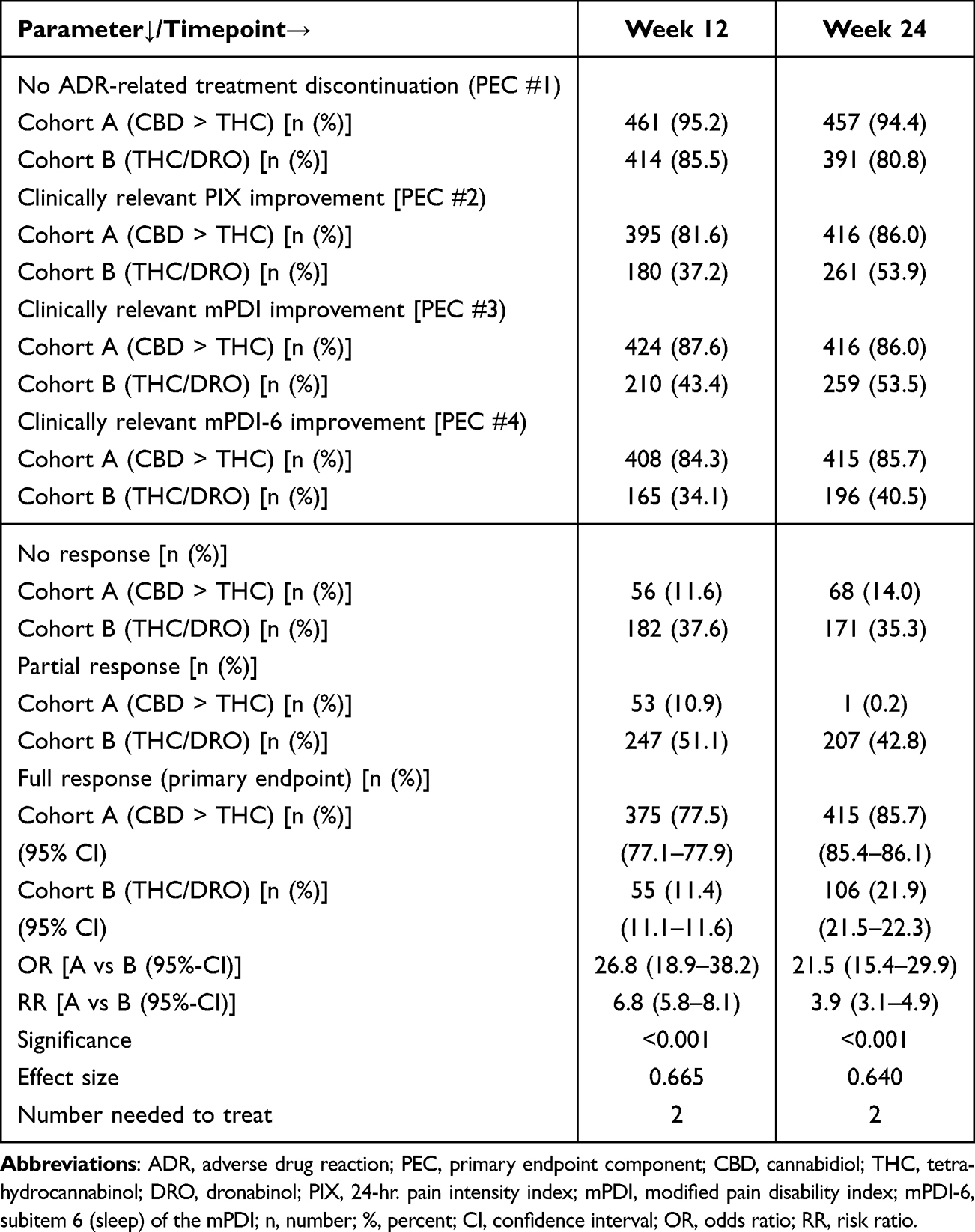 |
Table 10 Primary Endpoint |
Non-response according to these criteria was documented at week 24 in 14.0% of patients in cohort A and 35.3% in cohort B (p < 0.001; OR: 0.30 [0.22–0.41]; RR: 0.40 [0.37–0.43]; ES: 0.247).
Discussion
To our knowledge, CARE represents the first large real-world evaluation of oral cannabis-based medicines (CBM) specifically in older patients with chronic pain. Over a 24-week observation period, both CBD > THC and THC/DRO therapies were associated with clinically relevant improvements in pain intensity, pain-related disability, sleep disturbance, quality of life, and psychological well-being. However, the extent of improvement and the rates of ADR-related discontinuations differed between the two treatment groups, with CBD > THC being associated with more favorable outcomes. These findings expand the limited evidence based on the use of CBM in elderly patients and complement previous clinical and observational studies on cannabinoids in pain medicine.34–37
The present findings are in line with previous clinical trials and systematic reviews indicating that cannabinoids may reduce chronic pain and improve related outcomes in selected patient populations.38,39 However, most of the published trials have focused on mixed-age cohorts or younger adults, whereas evidence for elderly patients remains sparse. In this context, CARE adds information by specifically addressing patients aged ≥65 years, a group often underrepresented in randomized controlled trials.1,2,40
While some reviews have reported modest or inconsistent treatment effects,38 others have suggested potential benefits particularly for neuropathic pain and sleep disturbance.34,36 The observation in CARE that CBD-dominant CBMs were associated with lower discontinuation rates and fewer ADRs than THC/DRO may reflect the modulating effects of CBD on THC-induced side effects, as described in preclinical and clinical work.34 Nevertheless, direct comparisons are difficult, given differences in study design, CBM formulations, treatment durations, and patient populations.
Several mechanisms may contribute to the observed differences between CBD > THC and THC/DRO treatment. Preclinical and clinical data suggest that CBD interacts with multiple receptor systems and may modulate the psychoactive effects of THC.41,42 CBD has also been reported to exert anti-inflammatory, anxiolytic, and sleep-modulating properties,23,42,43 which could explain the broader spectrum of improvements observed in the present study. Furthermore, CBD may attenuate THC-induced adverse reactions, potentially contributing to the lower discontinuation rates seen in the CBD > THC group.43
It should be noted, however, that these interpretations remain hypothetical. The precise mechanisms underlying the clinical effects of CBD-rich CBMs in elderly patients with chronic pain have not been fully elucidated and warrant further investigation in controlled studies.
An additional observation in CARE was the substantial reduction in concomitant analgesic and co-analgesic use during CBM therapy. Patients treated with CBD > THC were more likely to discontinue non-opioid analgesics, NSAIDs, opioids, antidepressants, and anticonvulsants compared to those treated with THC/DRO. These findings are consistent with previous reports suggesting that cannabinoids may reduce the need for other analgesics, including opioids.44
While clinically relevant, these observations may be influenced by multiple factors (eg, patient or physician preference, tolerability issues, or changes in pain perception over time) and should be interpreted cautiously pending confirmation in prospective trials.
Limitations
The CARE project complied with the STROBE guidelines and followed the recommendations of the European Medicines Agency (EMA) regarding non-interventional pharmacological studies. The study was prospectively registered in the European ENCePP registry and conducted in compliance with the EU-GDPR, according to the recommendations of good clinical practice (GCP) and the Declaration of the World Medical Association in Helsinki.
Nevertheless, we are aware that the results of our study should be interpreted with several limitations in mind. First, its retrospective, observational design does not allow for causal inference. Although propensity score matching (PSM) was applied to harmonize baseline characteristics between the cohorts, this approach cannot fully replace the methodological rigor of randomization and blinding and therefore residual confounding from unmeasured variables cannot be excluded.
Second, all outcomes were based on patient-reported measures (PRMs) from the German Pain e-Registry. While these instruments are standardized and validated for pain research in Germany,24,25 they remain subject to recall and reporting bias.
Third, no formal sample size calculation was performed prior to the analysis. Post-hoc power estimates indicate that the available sample was sufficient to detect the observed between-group differences, but these calculations cannot substitute a predefined biometric planning.
Fourth, the study population was derived exclusively from Germany, which may limit generalizability to other healthcare systems and cultural contexts.
Finally, cannabinoid formulations were restricted to oral CBD > THC extracts and THC/DRO preparations; the results therefore cannot be extrapolated to other CBM formulations (eg, THC-dominant extracts, inhaled products, or topical applications).
Conclusions
In this real-world, retrospective study of elderly patients with chronic pain, both CBD > THC and THC/DRO therapies were associated with clinically relevant improvements in pain, disability, sleep, quality of life, psychological well-being, and use of analgesics. Differences between the two CBM regimens were observed, with CBD > THC showing lower discontinuation rates and numerically greater improvements across multiple outcomes.
These findings provide exploratory evidence supporting the potential of CBD-dominant CBMs in this patient population, but they are not conclusive. Prospective, randomized, and controlled trials are needed to confirm the effectiveness and safety of CBD-rich preparations and to clarify their role within multimodal pain management.
Acknowledgments
The concept for this evaluation of depersonalized routine data provided by the German Pain e-Registry was developed by M.A.U. at the Institute of Neurological Sciences (IFNAP) on behalf of the German Pain Association (Deutsche Gesellschaft für Schmerzmedizin, DGS) and the German Pain League (DSL). Its realization has been performed by O.Meany–Medical Data & Project Management GmbH, Nordostpark 51, 90411 Nürnberg, Germany, and funded by an unrestricted scientific grant from Stadapharm GmbH, Stadastraße 2-18, 61118 Bad Vilbel. Neither Stadapharm nor its employees influenced data acquisition, the conduct of this analysis, or the interpretation and publication of the results. M.A. U., G.H.H.M.-S., P.C.G.M.-S., and M.A.K. are physicians and are independent of any significant or relevant financial or other relationship to the sponsor, except for minor reimbursements for occasional lectures or consulting fees. M.A.U is an honorary member of the management boards of the German Pain Association and the German Pain League, Director of the private Institute of Neurological Sciences, and CEO of the O. Meany - MDPM GmbH, both Nordostpark 51, 90411 Nürnberg, Germany. The German Pain e-Registry (GPeR) was developed by the private Institute of Neurological Sciences (IFNAP), Nordostpark 51, 90411 Nürnberg, and is hosted by the O. Meany Medical Data & Project Management GmbH, Nordostpark 51, 90411 Nürnberg, under the control of the IFNAP. Since January 2015, GPeR has collected standardized real-world data from daily routine medical care via the online application iDocLive®. O.Meany–MDPM GmbH holds the legal right to use anonymized data from GPeR for healthcare research purposes, including the study entitled CARE. This right is based on comprehensive contractual agreements, including informed written consent obtained from both the participating physicians and patients. These agreements authorize the use of depersonalized data (with all identifiable information removed) for research purposes and allow the aggregated results of such studies to be shared with research partners (eg, health insurance providers, scientific institutions, professional associations, and pharmaceutical companies) in tabular or graphical forms (free of charge or, if applicable, also against payment). The CARE study was a retrospective analysis based exclusively on fully anonymized routine care data (with no identifiable information regarding patients, physicians, or treatment facilities). Therefore, ethics committee approval was not required for this study. The study concept and use of depersonalized data were reviewed and endorsed by the steering committees of the German Pain Association and German Pain League, with special attention given to patient rights and data protection. All participating physicians and patients provided written informed consent prior to their participation in the GPeR, explicitly authorizing the use of their anonymized data for healthcare research, including this study.
Data from this analysis were presented at the Annual Congress of the German Pain Association, March 13-15, 2025, Frankfurt, Germany and 131. Annual Conference of the German Society of Internal Medicine, Mai 3-6, 2025, Wiesbaden, Germany.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
M.A.U. received financial support and/or expenses in form of research money, consultancy fees and/or renumerations for lecture activities from: Abbvie, Almirall, Averitas, Avextra, Dermapharm, Forum für Medizinische Fortbildungen – FOMF, Glaxo Smith Kline, Grünenthal, Hexal, Johnson & Johnson, MCM Klosterfrau, Nestle, Stadapharm, Strathmann, Teva, Tilray, Trommsdorf, and Viatris. P.C.G.M.-S. received financial support and/or expenses in the form of consultancy fees from Forum für Medizinische Fortbildungen (FOMF), Grünenthal, Lundbeck, SinCephalea, Stadapharm, Teva, Vayamed, and Vertanical. M.A.K. received financial support and expenses in the form of consultancy fees from Hexal, Lilly, Lundbeck and Novartis. The authors report no other conflicts of interest in this work.
References
1. Domenichiello AF, Ramsden CE. The silent epidemic of chronic pain in older adults. Prog Neuropsychopharmacol Biol Psychiatry. 2019;93:284–27.
2. Dagnino APA, Campos MM. Chronic pain in the elderly: mechanisms and perspectives. Front Hum Neurosci. 2022;16:736688. doi:10.3389/fnhum.2022.736688
3. LaRowe LR, Miaskowski C, Miller A, et al. Prevalence and sociodemographic correlates of chronic pain among a nationally representative sample of older adults in the United States. J Pain. 2024;25(10):104614. doi:10.1016/j.jpain.2024.104614
4. Chan HKI, Chan CPI. Managing chronic pain in older people. Clin Med. 2022;22(4):292–294. doi:10.7861/clinmed.2022-0274
5. Pickering G, Kotlińska-Lemieszek A, Krcevski Skvarc N, et al. Pharmacological pain treatment in older persons. Drugs Aging. 2024;41(12):959–976. doi:10.1007/s40266-024-01151-8
6. Ribeiro H, Rodrigues I, Napoleão L, et al. Non-steroidal anti-inflammatory drugs (NSAIDs), pain and aging: adjusting prescription to patient features. Biomed Pharmacother. 2022;150:112958. doi:10.1016/j.biopha.2022.112958
7. Liu R, Xu W, Zhu H, et al. Aging aggravates Acetaminophen-induced acute liver injury and inflammation through inordinate C/EBPα-BMP9 crosstalk. Cell Biosci. 2023;13(1):61. doi:10.1186/s13578-023-01014-6
8. Kaur J, Nakafero G, Abhishek A, Mallen C, Doherty M, Zhang W. Incidence of side effects associated with acetaminophen in people aged 65 years or more: a prospective cohort study using data from the clinical practice research datalink. Arthritis Care Res. 2025;77(5):666–675. doi:10.1002/acr.25471
9. Gazelka HM, Leal JC, Lapid MI, Rummans TA. Opioids in older adults: indications, prescribing, complications, and alternative therapies for primary care. Mayo Clin Proc. 2020;95(4):793–800. doi:10.1016/j.mayocp.2020.02.002
10. Yoshikawa A, Ramirez G, Smith ML, et al. Opioid use and the risk of falls, fall injuries and fractures among older adults: a systematic review and meta-analysis. J Gerontol a Biol Sci Med Sci. 2020;75(10):1989–1995. doi:10.1093/gerona/glaa038
11. Schwan J, Sclafani J, Tawfik VL. Chronic Pain Management in the Elderly. Anesthesiol Clin. 2019;37(3):547–560.
12. Narayan SW, Naganathan V, Vizza L, et al. Efficacy and safety of antidepressants for pain in older adults: a systematic review and meta-analysis. Br J Clin Pharmacol. 2024;90(12):3097–3118.
13. Ong T, Thiam CN. Special consideration for pain management in the older person. Clin Med. 2022;22(4):295–297.
14. Minerbi A, Häuser W, Fitzcharles MA. Medical cannabis for older patients. Drugs Aging. 2019;36(1):39–51.
15. Levy C, Galenbeck E, Magid K. Cannabis for symptom management in older adults. Med Clin North Am. 2020;104(3):471–489.
16. Gastmeier K, Gastmeier A, Rottmann F, Herdegen T, Böhm R. Cannabinoide reduzieren den Opioidverbrauch bei älteren Schmerzpatienten: eine retrospektive Dreijahresauswertung einer ambulanten kassenärztlichen Praxis [Cannabinoids reduce opioid use in older patients with pain: retrospective three-year analysis of data from a general practice]. Schmerz. 2023;37(1):29–37. [German]. doi:10.1007/s00482-022-00642-0
17. Bell AD, MacCallum C, Margolese S, et al. Clinical practice guidelines for cannabis and cannabinoid-based medicines in the management of chronic pain and co-occurring conditions. Cannabis Cannabinoid Res. 2024;9(2):669–687. doi:10.1089/can.2021.0156
18. Friedman D, French JA, Maccarrone M. Safety, efficacy, and mechanisms of action of cannabinoids in neurological disorders. Lancet Neurol. 2019;18(5):504–512. doi:10.1016/S1474-4422(19)30032-8
19. Rock EM, Parker LA. Constituents of Cannabis sativa. Adv Exp Med Biol. 2021;1264:1–13.
20. Porter B, Marie BS, Milavetz G, Herr K. Cannabidiol (CBD) use by older adults for acute and chronic pain. J Gerontol Nurs. 2021;47(7):6–15. doi:10.3928/00989134-20210610-02
21. Mathew RJ, Wilson WH, Chiu NY, Turkington TG, Degrado TR, Coleman RE. Regional cerebral blood flow and depersonalization after tetrahydrocannabinol administration. Acta Psychiatr Scand. 1999;100(1):67–75. doi:10.1111/j.1600-0447.1999.tb10916.x
22. Beal JE, Olson R, Laubenstein L, et al. Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. J Pain Symptom Manage. 1995;10(2):89–97. doi:10.1016/0885-3924(94)00117-4
23. Bergamaschi MM, Queiroz RH, Chagas MH, et al. Cannabidiol reduces the anxiety induced by simulated public speaking in treatment-naïve social phobia patients. Neuropsychopharmacology. 2011;36(6):1219–1226. doi:10.1038/npp.2011.6
24. Deutsche Gesellschaft für Schmerzmedizin e.V. (German Pain Society). iDocLive® Documentation Platform [WWW Document]. URL Available from: https://www.dgschmerzmedizin.de/.
25. Casser HR, Hüppe M, Kohlmann T, et al. German pain questionnaire and standardised documentation with the KEDOQ-Schmerz. Der Schmerz. 2012;26(2):168–175. doi:10.1007/s00482-011-1142-0
26. Heller GZ, Manuguerra M, Chow R. How to analyze the visual analogue scale: myths, truths, and clinical relevance. Scand J Pain. 2016;13:67–75. doi:10.1016/j.sjpain.2016.06.012
27. S TRCCJTK, Chibnall JT, Krause S. The pain disability index: psychometric properties. Pain. 1990;40:171–182. doi:10.1016/0304-3959(90)90068-O
28. Basler HD. Marburger Fragebogen zum habituellen Wohlbefinden. Untersuchung an Patienten mit chronischem Schmerz [The Marburg questionnaire on habitual health findings--a study on patients with chronic pain. Schmerz. 1999;13(6):385–391. [German]. doi:10.1007/s004820050216
29. Selim AJ, Rothendler JA, Qian SX, Bailey HM, Kazis LE. The history and applications of the veterans RAND 12-item health survey (VR-12). J Ambul Care Manage. 2022;45(3):161–170. doi:10.1097/JAC.0000000000000420
30. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety & Stress Scales.
31. Von Korff M, Ormel J, Keefe FJ, Dworkin SF. Grading the severity of chronic pain. Pain. 1992;50(2):133–149. doi:10.1016/0304-3959(92)90154-4
32. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
33. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
34. Ueberall MA, Essner U, Vila Silván C, Mueller-Schwefe GHH. Comparison of the effectiveness and tolerability of nabiximols (THC:CBD) oromucosal spray versus oral dronabinol (THC) as add-on treatment for severe neuropathic pain in real-world clinical practice: retrospective analysis of the German Pain e-Registry. J Pain Res. 2022;15:267–286. doi:10.2147/JPR.S340968
35. Dykukha I, Malessa R, Essner U, Überall MA. Nabiximols in chronic neuropathic pain: a meta-analysis of randomized placebo-controlled trials. Pain Med. 2021;22(4):861–874. doi:10.1093/pm/pnab050
36. Ueberall MA, Vila Silván C, Essner U, Effectiveness M-SGHH. Safety, and tolerability of nabiximols oromucosal spray vs typical oral long-acting opioid analgesics in patients with severe neuropathic back pain: analysis of 6-month real-world data from the german pain e-registry. Pain Med. 2022;23(4):745–760. doi:10.1093/pm/pnab263
37. Ueberall MA, Horlemann J, Schuermann N, Kalaba M, Ware MA. Effectiveness and tolerability of dronabinol use in patients with chronic pain: a retrospective analysis of 12-week open-label real-world data provided by the german pain e-registry. Pain Med. 2022;23(8):1409–1422. doi:10.1093/pm/pnac010
38. Sic A, George C, Gonzalez DF, Tseriotis VS, Knezevic NN. Cannabinoids in chronic pain: clinical outcomes, adverse effects and legal challenges. Neurol Int. 2025;17(9):141. doi:10.3390/neurolint17090141
39. Karst M, Meissner W, Sator S, Keßler J, Schoder V, Häuser W. Full-spectrum extract from Cannabis sativa DKJ127 for chronic low back pain: a Phase 3 randomized placebo-controlled trial. Nat Med. 2025;31(12):4189–4196. PMID: 41023483. doi:10.1038/s41591-025-03977-0
40. Noroozian M, Raeesi S, Hashemi R, Khedmat L, Pain VZ. The neglect issue in old people’s life. Open Access Maced J Med Sci. 2018;6(9):1773–1778. doi:10.3889/oamjms.2018.335
41. Henson JD, Vitetta L, Hall S. Tetrahydrocannabinol and cannabidiol medicines for chronic pain and mental health conditions. Inflammopharmacology. 2022;30(4):1167–1178. doi:10.1007/s10787-022-01020-z
42. Wright M, Di Ciano P, Brands B. Use of cannabidiol for the treatment of anxiety: a short synthesis of preclinical and clinical evidence. Cannabis Cannabinoid Res. 2020;5:191–196. doi:10.1089/can.2019.0052
43. Laprairie RB, Bagher AM, Kelly ME, Denovan-Wright EM. Cannabidiol is a negative allosteric modulator of the cannabinoid CB1 receptor. Br J Pharmacol. 2015;172(20):4790–4805. doi:10.1111/bph.13250
44. Nielsen S, Picco L, Murnion B, et al. Opioid-sparing effect of cannabinoids for analgesia: an updated systematic review and meta-analysis of preclinical and clinical studies. Neuropsychopharmacology. 2022;47(7):1315–1330. doi:10.1038/s41386-022-01322-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.