Back to Journals » International Journal of General Medicine » Volume 15
Cardiovascular Risk Among Saudi Adults with Prediabetes: A Sub-Cohort Analysis from the Heart Health Promotion (HHP) Study
Authors Fayed A, Alzeidan R, Esmaeil S, Elmorshedy H, Ismail D, Elkouny R, Wahabi HA ![]()
Received 10 May 2022
Accepted for publication 1 August 2022
Published 29 August 2022 Volume 2022:15 Pages 6861—6870
DOI https://doi.org/10.2147/IJGM.S374190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Amel Fayed,1 Rasmieh Alzeidan,2 Samia Esmaeil,3 Hala Elmorshedy,1 Doaa Ismail,4 Roaa Elkouny,5 Hayfaa A Wahabi3,6
1College of Medicine, Clinical Department, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2College of Medicine, Cardiac Sciences Department, King Saud University, Riyadh, Saudi Arabia; 3Research Chair of Evidence-Based Healthcare and Knowledge Translation, King Saud University, Riyadh, Saudi Arabia; 4Department of Physical Medicine, Rheumatology & Rehabilitation, Tanta University, Faculty of Medicine, Tanta, Egypt; 5College of Medicine, Alfaisal University, Riyadh, Saudi Arabia; 6Department of Family and Community Medicine, King Saud University Medical City and College of Medicine, Riyadh, Saudi Arabia
Correspondence: Samia Esmaeil, Research Chair of Evidence-Based Healthcare and Knowledge translation, King Saud University, P.O. Box: 145111, Riyadh, 11362, Saudi Arabia, Tel +966 500-243-112, Email [email protected]
Background: This study aimed to estimate the prevalence of prediabetes among Saudi adults and to evaluate their risk of developing cardiovascular diseases.
Methods: This is a cohort of 2470 Saudi adults attending employee clinics in the university hospital. WHO-STEPs approach was used to collect sociodemographic (age, gender, and education), clinical (body mass index and blood pressure) and laboratory data (HbA1c, lipid profile and vitamin D concentration). Prediabetes was defined according to HbA1c level of 5.7– 6.4%. Cardiovascular risk (CVR) scores were evaluated using the Framingham Risk Score. SPSS was used for data analysis to investigate the relation between different CVR and prediabetes.
Results: Prediabetes affected 25.1% of the study population. Males had higher rates of prediabetes than females (27.5% versus 23.5%). The prevalence of prediabetes increased from 11.6% among young individuals (18– 29 years) to 56.0% among participants 60 years and older. Prediabetes patients exhibited considerably higher levels of all cardiovascular risk factors and nearly half of them (49.3%) had at least two risk factors. The prevalence of intermediate CVR among prediabetics was 13.2% compared to just 2.9% among the normal group, and high CVR was defined in 3.7% among prediabetics compared to only 1.7% in the normal group. Having prediabetes increased the odds to develop higher CVR of 2.64 times compared to those without prediabetes (OR = 2.64, 95% CI = 1.51– 4.64) and the level of vitamin D did not affect the odds of CVR.
Conclusion: Prediabetes is quite prevalent among Saudi adults, and they are at a higher risk of cardiovascular diseases. Patients with prediabetes have higher cardiac risk scores when compared to normal participants across the whole spectrum of (25(OH)D) concentrations. Additionally, no significant correlation was observed between HbA1c and (25(OH)D) levels in prediabetics or normoglycemic subjects.
Keywords: prediabetes, cardiovascular risk, Framingham cardiovascular risk score, Saudi Arabia
Introduction
Although the state of hyperglycemia in prediabetes is too low to be considered frank diabetes mellitus (DM), it is also too high to be considered normoglycemic; prediabetes is therefore defined as an intermediate state of hyperglycemia between normoglycemia and diabetes mellitus.1
Recent studies have shown that prediabetes is not as benign as it was previously thought to be; it can increase the risk of developing DM in the future along with all its complications such as diabetic retinopathy, neuropathy, nephropathy, macrovascular diseases, and cardiovascular diseases (CVD).2,3 Furthermore, other studies confirmed that autonomic and somatic peripheral nerve damage that occurs in DM can occur in the early phases of disturbed glucose tolerance.4,5
Symptoms of insulin resistance syndrome, such as upper-body obesity, hypertension, and dyslipidemia, have been found in most patients with prediabetes. These characteristics result in advanced atherosclerotic vascular changes, which are frequently preceded by endothelium-dependent vasodilation, vascular smooth muscle dysfunction, and increased arterial resistance, predisposing those patients to CVD.6,7
Recently, it has been found by studies that patients with DM and prediabetes have lower vitamin D concentrations (25(OH)D) and that supplementation of vitamin D can modify the progression of prediabetes to DM as well as prevent cardiovascular events among prediabetics.8,9 Vitamin D stimulates insulin receptors and enhances insulin response to glucose; supplementing vitamin D along with the appropriate therapy might be beneficial for long-term glucose control in DM.10
While there is a growing body of literature in Saudi Arabia on cardiovascular health and metabolic diseases, data from large cohort studies (of prediabetic patients) are considered critical for planning and prioritizing health services. Additionally, to the best of our knowledge, there is scarce research about the interaction between (25(OH)D) and CVD among healthy Saudi adults. The objectives of this cohort study are to estimate the prevalence of prediabetes in a large sample of adults in Saudi Arabia and to evaluate the risk of developing CVD in prediabetic and healthy individuals.
Materials and Methods
The study followed the standards of the Helsinki Declaration after receiving approval from King Saud University’s Institutional Review Board (IRB) (reference number 13–3721). All participants signed informed consent forms.
The original cohort included 4500 participants recruited from employee clinics in King Saud University Hospital that serve the employees and their families.11 There was no gender restriction; however, there was an age restriction – only participants above 18 were invited to join the study. For this study, we excluded participants diagnosed with DM and those who were not Saudi; hence, there were a total of 2470 participants in the current study.
The sociodemographic data (age, gender, and educational level), data about tobacco use, history of hypertension and DM, and anthropometric and biochemical measurements were collected using the World Health Organization (WHO) stepwise approach to chronic disease risk factor Surveillance-Instrument v2.1.12
All participants were required to fast for at least 12 hours before giving blood samples. Glycosylated hemoglobin (HbA1c), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), and triglycerides were measured.
Blood samples were taken for (25(OH)D) quantification, and the processed sera were kept at −80°C until they were analyzed. The serum 25(OH)D concentration was determined using a commercial enzyme-linked immunosorbent test (ELISA) (K2110, Immunodiagnostic [Dutch Company], Holland).
The assessment of the 10-year risk of coronary heart disease (CHD) was done using the Framingham risk score (FRS) which is one of the most widely used cardiovascular risk calculators in clinical practice. It considers age, gender, smoking status, lipid profile, and blood pressure to estimate the 10-year risk of coronary heart diseases and identifies high-risk patients effectively. An FRS of 10% or less indicated a low CVD risk, 10% to 19% was considered moderate risk, and 20% or more was considered high risk.13
Definitions
- Prediabetes: According to the American Diabetes Association, an HbA1c value of 5.7–6.4% was considered as prediabetes.14
- CVR scores were determined using the Framingham Coronary Heart Risk Score, and the cohort was classified into three categories based on their values: low risk (less than 10%), intermediate risk (10–20%), and high risk (more than 20%).15
- Current smokers were defined as those who smoked at least one cigarette daily for the preceding six months, one cigar or water pipe weekly for the preceding six months, or one waterpipe tobacco smoke/shisha session per month for the preceding three months, while “non-smokers” were defined as those who have never smoked.16
- Physical inactivity: a participant was considered physically inactive if not satisfying any of the following WHO criteria: 60 minutes of intense activity or 150 minutes of moderate activity each week.17
- Obesity: The research population was separated into five categories based on body mass index (BMI): underweight, normal weight, overweight, obese (class I), and morbidly obese (Class II and III): <18.5; 18.5–24.9; 25–29.9; 30–34.9; ≥35 Kg/m2, respectively.18
- Dyslipidemia: Participants were considered to have dyslipidemia if their lipid profile met the National Cholesterol Education Program (NCEP) criteria for dyslipidemia (elevated cholesterol, elevated triglycerides, high HDL-C level and low LDL-C).19
Statistical Analysis
Data was analyzed using the SPSS (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp). Continuous variables were reported as means with standard deviations, while categorical variables were presented as frequencies with equivalent percentages. Pearson’s Chi-square tests for comparing different proportions and t-test for comparing numerical variables were used.
Regression models were developed to test the independent effect of prediabetes and the risk of developing CVD after adjustment of different confounders. For logistic regression statistical analysis, patients with moderate and high risk for CHD as measured by FRS were considered as one category compared to those with low risk. For linear correlations with HbA1c and 25(OH)D we considered the original FRS score without categorization.
Adjusted Odds Ratio (OR) and its 95% Confidence Intervals (CI) were reported and a P-value of less than 0.05 was considered statistically significant.
Ethical Statement
The approval letter (number 13–3721) of King Saud University – Institutional Review Board (IRB) was sought prior to the study commencement. The informed written consent was obtained from each participant before questionnaire completion and blood sample withdrawal. The study was conducted as per the principles expressed by Declaration of Helsinki.
Results
Patients with prediabetes constituted 25.1% of the studied sample. When comparing males to females, the males had a higher likelihood of having prediabetes than the females (27.5% versus 23.5%). When looking at the prevalence according to age groups, the nadir was in the age group of 18–29 at 11.6%, whilst the zenith was in the 60 plus age group at 56.0%. Similarly, when comparing the prevalence in accordance with BMI, the lowest prevalence was in the underweight category at 9.8%, and the highest was in the morbidly obese category at 40.5% (Table 1).
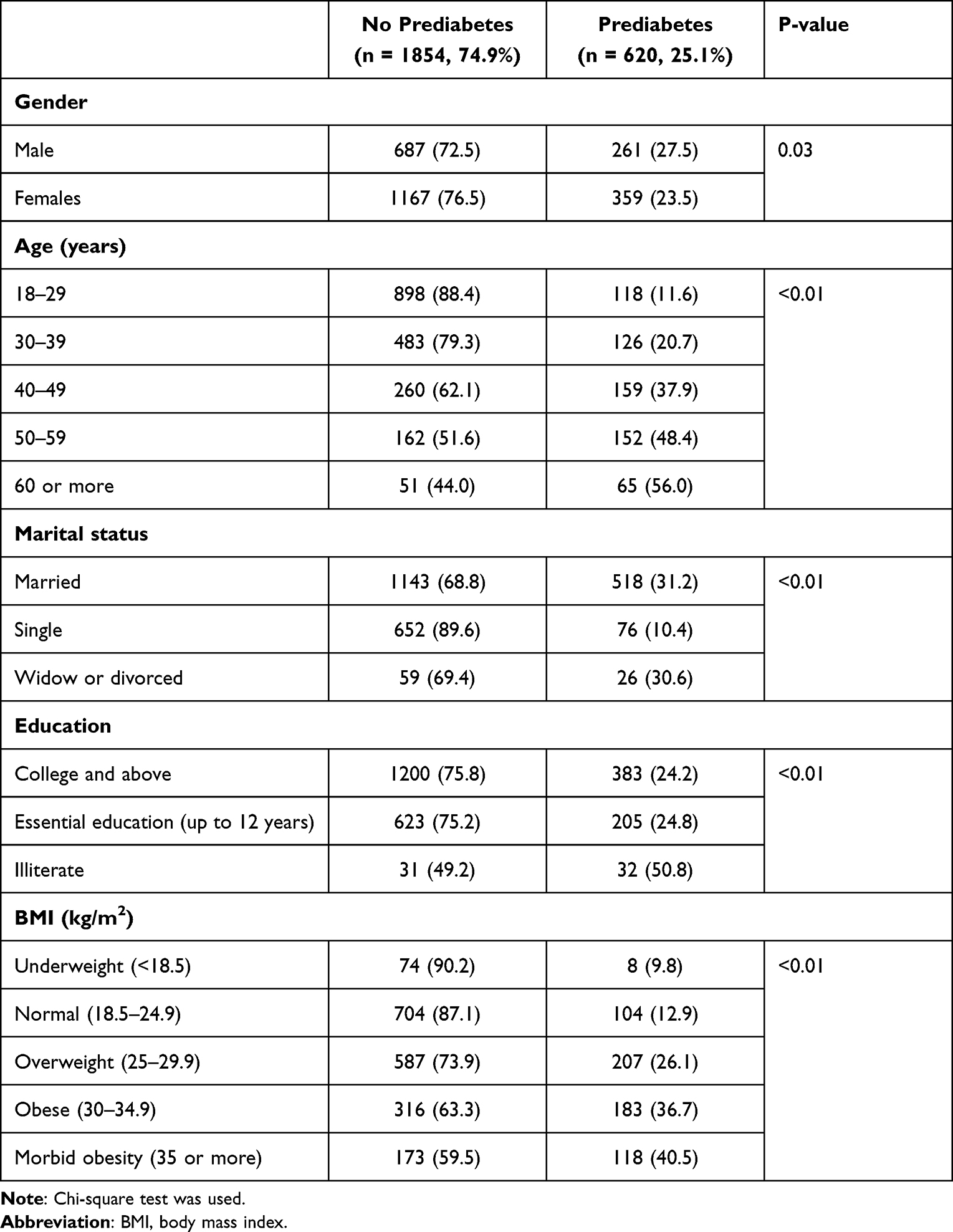 |
Table 1 Sociodemographic Profile of the Studied Sample |
Patients with prediabetes had significantly higher levels of all CVD risk indicators when compared to healthy participants, including obesity, physical inactivity, high blood pressure, elevated cholesterol levels, elevated triglyceride levels, low HDL levels, high LDL levels, and hyperglycemia. No significant difference in smoking habits or (25(OH)D) levels were observed between the groups (Table 2). En masse, only 6.1% of the prediabetic patients had no CVD risk factors; 49.3% had at least 2 CVD risk factors.
 |
Table 2 Comparison of Cardiovascular Risk Factors Between Participants with and without Prediabetes |
Intermediate CVR had a prevalence of 13.2% among prediabetics, while in the normal group, it was only 2.9%. The prevalence of high CVR was 3.7% in prediabetics compared to 1.7% in the normal group (p-value <0.01) (Table 2).
The independent effect of prediabetes on having CVR (intermediate and high) was investigated using a multivariate logistic regression model which was adjusted for sociodemographic factors (education and marital status). Having prediabetes increased the odds of developing a higher CVR by 2.64 times compared to those without prediabetes (OR = 2.64, 95% CI = 1.51–4.64, p < 0.01) (Table 3).
 |
Table 3 Multivariate Regression Model for Independent Effect of Prediabetes and Vitamin D on the Cardiac Risk |
Investigating the correlation between (25(OH)D) level and FRS among prediabetes and normal participants showed that patients with prediabetes have a higher CVR scores when compared to normal participants across the whole spectrum of (25(OH)D) concentrations (Figure 1). Additionally, no significant correlation was observed between HbA1c and (25(OH)D) levels in prediabetic or normoglycemic subjects (r = 0.02, p = 0.92) (Figure 2). The level of (25(OH)D) did not affect the odds of CVD risk among the studied sample (Table 3).
 |
Figure 1 Correlation between HbA1c and vitamin D among prediabetics and normoglycemic participants. |
 |
Figure 2 Predicted linear correlation between Vitamin D level and Framingham Cardiac Risk Score among prediabetes and normal participants. |
Discussion
This study revealed a relatively high prevalence of prediabetes among a large cohort of Saudi adults; prediabetes was more frequently reported among older male participants and those with a higher BMI. Prediabetes aggravated the risk of CVD, while (25(OH)D) did not significantly affect CVD risk among this cohort.
In 2014, an alarming finding from a Saudi Arabian national study of households reported that almost half of the adult population have a degree of impaired glucose metabolism with an overt diabetes prevalence of 25.4% and prediabetes of 25.5%.20 These figures were recently confirmed by studies that investigated the epidemiology of diabetes among a different Saudi population.21–23 A recent study, which was conducted among elite football players found that the prevalence of prediabetes was 7.9% in the players compared to 18.78% in matched nonathlete controls.24 The findings of this study add to the growing evidence of the alarming situation of glucose intolerance among the Saudi community.
When compared to the global prevalence data, the current study’s prediabetes prevalence of 25.1% is deemed quite high. According to the International Diabetes Federation (IDF), the prevalence of prediabetes in the Middle East and North Africa is 8.2% (which is estimated to reach 9.4% in 2045); the IDF observed the highest prevalence of prediabetes in North America at 15.4% (which is expected to be 16.7% in 2045).25 The high prevalence of prediabetes in our study was predicted since we defined prediabetes using HbA1c - a more precise measure; studies using HbA1c criteria often found a greater prevalence of prediabetes.26,27 This high prevalence of prediabetes is expected considering the high prevalence of obesity, physical inactivity, and urbanization among Saudi Arabia’s population, which have exacerbated the incidence of prediabetes and DM across various geographies and demographic groups.28,29
Similar to our findings, the prevalence of prediabetes is reported more among males from different communities and ethnic groups.30,31 Advancing age and obesity are among the well-established risk factors for both DM and prediabetes.30 The average fasting blood glucose levels rise with age due to the carbohydrate challenge exerted against the metabolic homeostasis in the elderly populations.32 Additionally, obesity is highly correlated with insulin resistance, as indexed by elevated homeostatic model assessment (HOMA-IR) levels, and it even intensifies the risk of development of overt Type 2 diabetes (T2DM) among patients with prediabetes.33
When compared to healthy patients in the current study, those with prediabetes had significantly greater levels of all CVD risk factors, including hypertension, dyslipidemia, and the 10-year cardiovascular risk as determined by the FRS. These findings are in line with the substantial amount of evidence that shows that DM increases the risk of CVD well before clinical illness develops.3,34,35
CVD, stroke, and peripheral vascular disease are all macrovascular illnesses linked to T2DM and the traditional risk factors (dyslipidemia, obesity, and hypertension) are very prevalent in people with prediabetes as shown by many researchers.34,36 The pathophysiological changes that lie behind this scene include loss of beta-cell volume, endothelial dysfunction, arterial stiffness, increased lipolysis and dysregulated cytokines.2
Several studies indicated that vitamin D, obesity, DM, and CVD are related, but the nature of these connections remains unclear.37 Vitamin D promotes anti-inflammatory synthesis and lowers pro-inflammatory cytokine production that can decrease the mitochondrial damage which causes insulin resistance. Additionally, vitamin D supports epigenomes – DM and insulin resistance are commonly associated with DNA hypermethylation, which inactivates several genes. Vitamin D increases DNA demethylase expression, counteracting this process. On the other hand, Vitamin D is connected to numerous CVDs, including infectious myocarditis, which is caused by aberrant immunological reactions as a result of vitamin D receptor inadequacy.38,39
In the current study, we found that people with prediabetes have greater CVR scores than normal participants regardless of their (25(OH)D) levels, we also did not identify a significant link between HbA1c and (25(OH)D) levels in prediabetics or healthy participants.
The results of this study support the premise that vitamin D is unlikely to make a significant difference in reducing DM and hypertension risks.40 Many systematic reviews and meta-analysis denied the effectiveness of vitamin D in reducing the systolic blood pressure or improving the arterial stiffness. However, many of these systematic reviews showed high level of heterogeneity among the included studies; therefore, caution is needed when evaluating the evidence supporting the effectiveness of vitamin D on CVR.37 Additionally, those epidemiological observations that supported the link between vitamin D deficiency, hypertension, and DM point to an association rather than a causality relationship.41,42
Considering the high prevalence of prediabetes and the greater risk of CVD that comes with it, it is imperative that we implement an effective diabetes-related CVD management program in Saudi Arabia or the burden of CVD associated with diabetes will skyrocket.
We are aware of some limitations in the current study as the nature of collecting the data about glucose impairment, cardiovascular parameters, and vitamin D at the same time affected the ability to investigate the temporal relationship among all these parameters. However, the large sample size and the completeness of all data will support the evidence revealed in this study.
Conclusion
Prediabetes is quite prevalent among Saudi adults, and they are at a higher risk of cardiovascular diseases. Patients with prediabetes have higher cardiac risk scores when compared to normal participants across the whole spectrum of (25(OH)D) concentrations. Additionally, no significant correlation was observed between HbA1c and (25(OH)D) levels in prediabetics or normoglycemic subjects.
Abbreviations
HHP, Heart Health Promotion; CVR, Cardiovascular risk; DM, Diabetes mellitus; CVD, Cardiovascular disease; CHD, Coronary heart disease; FRS, Framingham risk score; HbA1c, Glycosylated haemoglobin; HDL-C, High-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, Total cholesterol.
Data Sharing Statement
Most of the data needed is included in the published article. However, more data is available from the King Saud University Ethics Committee for researchers who meet the criteria for access to confidential data. The ethics committee contact details for data requests are: [email protected]. This contact point is completely independent of all researchers.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was funded by Princess Nourah bint Abdulrahman University researchers supporting project (number PNURSP2022R21) Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang Y, Cai X, Mai W, Li M, Hu Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. BMJ. 2016;355:i5953. doi:10.1136/bmj.i5953
2. Dimova R, Tankova T, Chakarova N, Groseva G, Dakovska L. Cardiovascular autonomic tone relation to metabolic parameters and hsCRP in normoglycemia and prediabetes. Diabetes Res Clin Pract. 2015;109(2):262–270. doi:10.1016/j.diabres.2015.05.024
3. Dimova R, Tankova T, Guergueltcheva V, et al. Risk factors for autonomic and somatic nerve dysfunction in different stages of glucose tolerance. J Diabetes Complications. 2017;31(3):537–543. doi:10.1016/j.jdiacomp.2016.11.002
4. Stino AM, Smith AG. Peripheral neuropathy in prediabetes and the metabolic syndrome. J Diabetes Investig. 2017;8(5):646–655. doi:10.1111/jdi.12650
5. Bansal V, Kalita J, Misra UK. Diabetic neuropathy. Postgrad Med J. 2006;82(964):95–100. doi:10.1136/pgmj.2005.036137
6. Brannick B, Dagogo-Jack S. Prediabetes and cardiovascular disease: pathophysiology and interventions for prevention and risk reduction. Endocrinol Metab Clin North Am. 2018;47(1):33–50. doi:10.1016/j.ecl.2017.10.001
7. Wasserman DH, Wang TJ, Brown NJ. The vasculature in prediabetes. Circ Res. 2018;122(8):1135–1150. doi:10.1161/circresaha.118.311912
8. Martins D, Wolf M, Pan D, et al. Prevalence of cardiovascular risk factors and the serum levels of 25-hydroxyvitamin D in the United States: data from the Third National Health and Nutrition Examination Survey. Arch Intern Med. 2007;167(11):1159–1165. doi:10.1001/archinte.167.11.1159
9. Friedman TC. Vitamin D supplementation to prevent the progression of prediabetes to diabetes: getting closer to a recommendation. Transl Res. 2011;158(5):273–275. doi:10.1016/j.trsl.2011.06.007
10. Dimova R, Tankova T, Chakarova N. Vitamin D in the spectrum of prediabetes and cardiovascular autonomic dysfunction. J Nutr. 2017;147(9):1607–1615. doi:10.3945/jn.117.250209
11. Alzeidan R, Rabiee F, Mandil A, Hersi A, Fayed A. Non-communicable disease risk factors among employees and their families of a Saudi university: an epidemiological study. PLoS One. 2016;11(11):e0165036. doi:10.1371/journal.pone.0165036
12. World Health Organization. STEPS instrument. WHO; 2022. Available from: https://www.who.int/ncds/surveillance/steps/STEPS_Instrument_v2.1.pdf.
13. Bosomworth NJ. Practical use of the Framingham risk score in primary prevention: Canadian perspective. Can Fam Physician. 2011;57(4):417–423.
14. Association AD. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;37(Supplement_1):S81–S90. doi:10.2337/dc14-S081.
15. D’Agostino RB
16. Wipfli H. The Tobacco Atlas, Fourth Edition. Am J Epidemiol. 2012;176(12):1193. doi:10.1093/aje/kws389
17. World Health Organization. Part 4: conducting the survey, data entry, data analysis, and reporting and disseminating results. Available from: https://www.who.int/ncds/surveillance/steps/Part4.pdf.
18. Obesity. WHO. Available from: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle—who-recommendations.
19. National Cholesterol Education Program (US).Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143–3421. doi:10.1161/circ.106.25.3143
20. Al-Rubeaan K, Al-Manaa HA, Khoja TA, et al. Epidemiology of abnormal glucose metabolism in a country facing its epidemic: Saudi-DM study. J Diabetes. 2015;7(5):622–632. doi:10.1111/1753-0407.12224
21. Al-Rubeaan K, Al-Manaa HA, Khoja TA, et al. A community-based survey for different abnormal glucose metabolism among pregnant women in a random household study (Saudi-DM). BMJ Open. 2014;4(8):8. doi:10.1136/bmjopen-2014-005906
22. El-Kebbi IM, Bidikian NH, Hneiny L, Nasrallah MP. Epidemiology of type 2 diabetes in the Middle East and North Africa: challenges and call for action. World J Diabetes. 2021;12(9):1401–1425. doi:10.4239/wjd.v12.i9.1401
23. Alkhaldy AA, Rizq NK, Del Jaylan SA, Alkendi EA, Alghamdi WM, Alfaraidi SM. Dietary intake and physical activity in relation to insulin resistance in young overweight Saudi females: an exploratory pilot study. Prev Nutr Food Sci. 2019;24(4):373–380. doi:10.3746/pnf.2019.24.4.373
24. Meo SA, Abukhalaf AA, Alomar AA, Alessa OM, Sumaya OY, Meo AS. Prevalence of prediabetes and type 2 diabetes mellitus in football players: a novel multi football clubs cross sectional study. Int J Environ Res Public Health. 2021;18(4):4. doi:10.3390/ijerph18041763
25. IDF diabetes atlas eighth edition; 2022. Available from: https://diabetesatlas.org/upload/resources/previous/files/8/IDF_DA_8e-EN-final.pdf.
26. Hostalek U. Global epidemiology of prediabetes – present and future perspectives. Clin Diabetes Endocrinol. 2019;5(1):5. doi:10.1186/s40842-019-0080-0
27. Blum J, Aeschbacher S, Schoen T, et al. Prevalence of prediabetes according to hemoglobin A1c versus fasting plasma glucose criteria in healthy adults. Acta Diabetol. 2015;52(3):631–632. doi:10.1007/s00592-014-0659-y
28. Al-Zahrani JM, Aldiab A, Aldossari KK, et al. Prevalence of prediabetes, diabetes and its predictors among females in Al Kharj, Saudi Arabia: a cross-sectional study. Ann Glob Health. 2019;85(1):109. doi:10.5334/aogh.2467
29. Al-Raddadi R, Bahijri SM, Jambi HA, Ferns G, Tuomilehto J. The prevalence of obesity and overweight, associated demographic and lifestyle factors, and health status in the adult population of Jeddah, Saudi Arabia. Ther Adv Chronic Dis. 2019;10:2040622319878997. doi:10.1177/2040622319878997
30. Cowie CC, Casagrande SS, Geiss LS, et al. Prevalence and Incidence of type 2 diabetes and prediabetes. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, editors. Diabetes in America. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018.
31. Perry IJ, Wannamethee SG, Walker MK, Thomson AG, Whincup PH, Shaper AG. Prospective study of risk factors for development of non-insulin dependent diabetes in middle aged British men. BMJ. 1995;310(6979):560–564. doi:10.1136/bmj.310.6979.560
32. Pataky MW, Young WF, Nair KS. Hormonal and metabolic changes of aging and the influence of lifestyle modifications. Mayo Clinic Proc. 2021;96(3):788–814. doi:10.1016/j.mayocp.2020.07.033
33. Martinez KE, Tucker LA, Bailey BW, LeCheminant JD. Expanded normal weight obesity and insulin resistance in US adults of the National Health and Nutrition Examination Survey. J Diabetes Res. 2017;2017:9502643. doi:10.1155/2017/9502643
34. Hu FB, Stampfer MJ, Haffner SM, Solomon CG, Willett WC, Manson JE. Elevated risk of cardiovascular disease prior to clinical diagnosis of type 2 diabetes. Diabetes Care. 2002;25(7):1129–1134. doi:10.2337/diacare.25.7.1129
35. Dimova R, Chakarova N, Grozeva G, Tankova T. Evaluation of the relationship between cardiac autonomic function and glucose variability and HOMA-IR in prediabetes. Diabetes Vasc Dis Res. 2020;17(5):1479164120958619. doi:10.1177/1479164120958619
36. Cai X, Zhang Y, Li M, et al. Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis. BMJ. 2020;370:m2297. doi:10.1136/bmj.m2297
37. Veloudi P, Jones G, Sharman JE. Effectiveness of vitamin D supplementation for cardiovascular health outcomes. Pulse. 2017;4. doi:10.1159/000452742
38. Galușca D, Popoviciu MS, Babeș EE, et al. Vitamin D implications and effect of supplementation in endocrine disorders: autoimmune thyroid disorders (Hashimoto’s disease and Grave’s disease), diabetes mellitus and obesity. Medicina. 2022;58:2. doi:10.3390/medicina58020194
39. Babeș EE, Lucuța DA, Petcheși CD, et al. Clinical features and outcome of infective endocarditis in a university hospital in Romania. Medicina. 2021;57:2. doi:10.3390/medicina57020158
40. Al-Sumaih I, Johnston B, Donnelly M, O’Neill C. The relationship between obesity, diabetes, hypertension and vitamin D deficiency among Saudi Arabians aged 15 and over: results from the Saudi health interview survey. BMC Endocr Disord. 2020;20(1):81. doi:10.1186/s12902-020-00562-z
41. Gupta AK, Brashear MM, Johnson WD. Prediabetes and prehypertension in healthy adults are associated with low vitamin D levels. Diabetes Care. 2011;34(3):658–660. doi:10.2337/dc10-1829
42. Pinelli NR, Jaber LA, Brown MB, Herman WH. Serum 25-hydroxy vitamin D and insulin resistance, metabolic syndrome, and glucose intolerance among Arab Americans. Diabetes Care. 2010;33(6):1373–1375. doi:10.2337/dc09-2199
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.