Back to Journals » Infection and Drug Resistance » Volume 15
Carbapenem-Resistant Gram-Negative Bacilli Causing Ventilator Associated Pneumonia: Study of MASTDISCS Combi Carba Plus for Detection of Carbapenemase Producing Enterobacterales
Authors Hegazy EE ![]() , Bahey MG, Abo Hagar AM
, Bahey MG, Abo Hagar AM ![]() , Elkholy AA, Mohamed EA
, Elkholy AA, Mohamed EA
Received 21 August 2022
Accepted for publication 18 October 2022
Published 31 October 2022 Volume 2022:15 Pages 6331—6342
DOI https://doi.org/10.2147/IDR.S385294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Eman E Hegazy,1 Marwa Gamal Bahey,1 Alaa Mohammed Abo Hagar,2 Amira Abdelgalil Elkholy,3 Esraa A Mohamed1
1Department of Medical Microbiology and Immunology, Faculty of Medicine, Tanta University, Tanta, Egypt; 2Department of Anesthesiology, Surgical Intensive Care and Pain Medicine, Faculty of Medicine, Tanta University, Tanta, Egypt; 3Department of Chest Diseases, Faculty of Medicine, Tanta University, Tanta, Egypt
Correspondence: Eman E Hegazy, Tel +20 10 99008274, Email [email protected]
Background: Ventilator-associated pneumonia (VAP) caused by carbapenem-resistant gram-negative bacteria has been proven to be an escalating public health challenge in Egypt owing to its high mortality rate and raised health care costs.
Purpose: Detection of carbapenem-resistant gram-negative bacilli among VAP patients, genotypic identification of carbapenemase genes in the isolated strains with evaluation of their impact on patient outcome and detection of carbapenemase-producing enterobacterales by MASTDISCS combi Carba plus disc system.
Methods: Broncho-alveolar lavage fluid (BALF) and endotracheal aspirate were collected aseptically from clinically suspected VAP patients. Pathogen identification and antibiotic sensitivity testing were done. Carbapenemase-encoding genes (blaKPC, blaNDM, and blaOXA-48) were tested by PCR in all carbapenem-resistant gram-negative isolates. Performance of MASTDISCS combi Carba plus in isolated Enterobacterales was assessed in relation to the PCR results.
Results: Eighty-three carbapenem-resistant gram-negative isolates were detected. The most frequent pathogens were Klebsiella pneumoniae, Acinetobacter baumannii and Pseudomonas aeruginosa representing 34.9%, 20.5% and 18.1%, respectively. blaKPC was the predominant gene. Patients with persistent mechanical ventilation less than 15 days and Pseudomonas aeruginosa infection were significantly associated with a higher death rate. MAST-Carba plus had the highest sensitivity, specificity, positive and negative predictive values for detecting OXA-48 carbapenemases representing 81.8%, 92.5%, 75% and 94.9%, respectively.
Conclusion: Worse outcome in VAP patients was associated with carbapenem-resistant gram-negative bacilli. MASTDISCS combi Carba plus is an efficient simple method for identification of different carbapenemases among enterobacterales.
Keywords: Mast DISCS, carbapenemase, enterobacterales, ventilator-associated pneumonia, VAP
Introduction
Ventilator-associated pneumonia (VAP) is one of the most important hospital acquired infections in intensive care unit (ICU) patients, which is usually associated with prolonged hospital stay, empirical antibiotic use and high morbidity and mortality rates.1,2
The microorganisms that cause VAP differ between countries and even between ICUs; however, among gram-negative bacteria, P. aeruginosa, Acinetobacter spp., and Enterobacterales are commonly found. Methicillin-resistant staphylococcus aureus and Streptococcus spp. are accused of being responsible for VAP among gram-positive pathogens.3
Carbapenem is the most important antibiotic class that is considered the drug of choice in cases of VAP. However, the frequent and indiscriminate use of carbapenems results in development of carbapenem-resistant gram-negative bacteria (CR-GNB).4
Different mechanisms are involved in emergence of carbapenem resistance; the most reliable one is production of carbapenemases, which were either chromosomally or plasmid mediated or both, resulting in rapid spread of carbapenem resistance among different bacterial species.5,6
Three Ambler classes of carbapenemase genes have been recognized since 1993; class A carbapenemase (Klebsiella pneumoniae carbapenemase, KPC) enzymes that are able to degrade carbapenems, penicillin and cephalosporins; class B metallo-beta-lactamases (MBLs) that include Verona integron-encoded metallo-beta-lactamase (VIM), New Delhi metallo-beta-lactamases (NDM) and imipenemase (IMP) type enzymes that can perform variable hydrolysis effects against beta-lactams with exclusion of monobactam (aztreonam) and class D carbapenem-hydrolysing oxacillinase-like OXA-48 enzymes that show decreased effectiveness against 3rd and 4th generation cephalosporins and carbapenems with high activity against penicillin. Carbapenemase genes like NDM, KPC and OXA-48 are more likely involved in carbapenem resistance in Enterobacteriaceae-resistant isolates.7–9
It is essential to detect the presence of carbapenemase genes rapidly and accurately to control spread of infection and to select different treatment lines.6 Genotypic identification of carbapenemase genes by polymerase chain reaction (PCR) remains the gold standard method for both specific and accurate detection of different antibiotic-resistant genes.10
Variable methods such as Carba NP and modified carbapenem inactivation method (mCIM) are available for detection of carbapenemase ability of the organism phenotypically irrespective to carbapenemase genes. The MASTDISCS combi Carba plus disc system (MAST-Carba plus; Mast Group Ltd., UK) is another promising method, which depends on 5 discs: faropenem (disc A) and MBLs inhibitor (disc B), KPC inhibitor (disc C), AmpC inhibitor (disc D) and temocillin together with MBLs inhibitor (disc E) for detection of carbapenemase producing Enterobacteriaceae.11,12 Therefore, this study was designed to detect carbapenem-resistant gram-negative bacilli isolated from VAP patients, genotypic identification of carbapenemase genes (blaKPC, blaNDM, and blaOXA-48) in the isolated strains, evaluation of their impact on patient outcome together with assessment of MASTDISCS combi Carba plus disc system as a method for rapid phenotypic detection of carbapenemase-producing Enterobacterales.
Materials and Methods
Study Design
This prospective randomized cross-sectional study was carried out over 12 months duration from June 2021 to June 2022 in the Medical Microbiology and Immunology Department and Intensive Care Units (ICUs) of Tanta University Hospitals, where the hospitals serve approximately 190,000 patients per year and have a total of 2035 beds, including 116 beds in the ICUs. The study was approved by the Institutional Review Board of the Faculty of Medicine, Tanta University, Egypt (approval code 35342/3/22). The study was conducted in accordance with the Declaration of Helsinki guidelines.
Sample Size
According to previously recorded Egyptian research data, VAP ranges from 15 to 45% and varies greatly across the country. In a recent study at Tanta University Hospitals, the incidence of VAP in all ICU patients studied was 38.4%.13
The sample size (n) was determined using the formula:  14, where n = sample size = Z value is 1.96, for a confidence level (α) of 95%, P = expected proportion (in proportion of one. If VAP infection was 38.4%, according to a previously published study,13 so P = 0.38.4, and d = precision = 0.06. So, the calculated minimal sample size will be “357”.
14, where n = sample size = Z value is 1.96, for a confidence level (α) of 95%, P = expected proportion (in proportion of one. If VAP infection was 38.4%, according to a previously published study,13 so P = 0.38.4, and d = precision = 0.06. So, the calculated minimal sample size will be “357”.
Study Subjects
All intubated patients admitted to ICUs and clinically presented with signs and symptoms of nosocomial lower respiratory tract infection and a two-day history of invasive mechanical ventilation were enrolled in this study. Patient medical history was recorded, including name, age, gender, admission date, associated comorbidity, duration of ventilation, length of hospitalization and clinical outcome. Patients whose clinical samples tested positive for carbapenem-resistant gram-negative bacilli were incorporated in the demographic and outcome measure analyses. Patients with clinically and radiologically confirmed pneumonia at admission were excluded.
Sample Collection
Broncho-alveolar lavage fluid (BALF) and endotracheal aspirates were collected in sterile containers following strict aseptic precautions. In order to ensure participant privacy and data confidentiality, each sample was assigned a code number, and transferred as soon as possible to the Microbiology and Immunology Department laboratory.
Identification of bacterial Isolates
Samples were cultivated on blood agar, nutrient agar, chocolate agar, and MacConkey agar plates (Oxoid, UK). The plates were incubated aerobically at 37°C for 24–48 hours. Phenotypic detection of the isolated pathogens was based primarily on standard microbiological procedures such as colony morphology, gram staining reaction, and biochemical reactions.15 According to the gram staining reaction, isolates were characterized and only gram-negative bacteria were further processed. Verification of gram-negative bacterial isolates was done using Vitek-2 automated system (Biomérieux, Marcy-LÉtoile, France) following the manufacturer’s instructions. All isolates of Enterobacterales, Acinetobacter species, and Pseudomonas that were phenotypically identified and confirmed by vitek-2 were stored at −80C in brain heart infusion broth (Oxoid, UK) containing 20% glycerol until use.
Antimicrobial Susceptibility Testing
All identified enterobacterales and non-fermenter isolates (Acinetobacter species and Pseudomonas spp) were assessed for antibiotic susceptibility by modified Kirby Bauer disc diffusion method on Muller–Hinton agar plates (Oxoid, UK) and the Vitek-2 automated system with the AST-gram-negative card (Biomérieux, Marcy-LÉtoile, France). The antibiotics used were ceftriaxone (30 μg), amikacin (30 μg), ciprofloxacin (5 μg), ampicillin (10 μg), cefoxitin (30 μg), amoxicillin-clavulanate (10 μg), gentamicin (10 μg), aztreonam (30 μg), tigecycline (15μg), cefepime (30 μg), piperacillin-tazobactam (10 μg), ceftazidime (30 μg), levofloxacin (5 μg), co-trimoxazole (30 μg), imipenem (10 μg) and meropenem (10 μg). The strains were characterized as susceptible, intermediate or resistant according to the Clinical and Laboratory Standard Institute (CLSI) guidelines.16
Molecular Detection of Carbapenemase Genes
Using PCR-based methods, the presence carbapenemase genes (blaKPC, blaNDM, and blaOXA-48) were investigated in all phenotypically detected carbapenem-resistant isolates using a panel of primer: blaKPC-F 5’-CGTCTAGTTCTGCTGTCTTG −3’; blaKPC-R 5’-CTTGTCATCCTTGTTAGGCG-3’, blaNDM-F 5’-GGTTTGGCGATCTGGTTTTC-3’ blaNDM-R 5’-CGGAATGGCTCATCACGATC-3’, and blaOXA-48-F 5’-GCGTGGTTAAGGATGAACAC-3’ blaOXA-48-R 5’-CATCAAGTTCAACCCAACCG −3’.17
Extraction and Purification of Total Bacterial Genomic DNA
Total bacterial genomic DNA was purified in concordance with the manufacturer’s protocol of the E.Z.N.A.® Bacterial DNA Kit (D3350-01, Omega BIO-TEK, USA).
PCR Amplification and Analysis of Data
Dream Taq Green PCR Master Mix (2X) (K1081, Thermo Fisher, USA) was applied for specific gene amplification as per manufacturer protocol using Creacon (Holland, Inc) Polymerase Chain Reaction (PCR) system cycler. The PCR conditions were constructed according to Michodigni et al.17 The amplified PCR products were separated through agarose gel electrophoresis and then stained with ethidium bromide. Gel documentation system (Geldoc-it, UVP, England) was used for visualization and analysis of data utilizing Totallab analysis software (ww.totallab.com, Ver.1.0.1).
Performance of MASTDISCS Combi Carba Plus as Rapid Phenotypic Detection of Carbapenemase Production
All enterobacterale isolates exhibiting resistance to carbapenems were screened for carbapenemase production phenotypically using the MASTDISCS combi Carba plus (MASTDISCS combi-D73C, Bootle, UK). Briefly, as shown in the manufacturer’s guidelines, fresh, pure colonies of the bacterium were dissolved in physiological saline to make a suspension of 0.5 McFarland turbidity standard, which was homogeneously spread by sterile swabs on Mueller–Hinton agar plates (Oxoid, UK). Then, the five antibiotic discs were arranged on the cultivated agar, leaving adequate distance between them for forming definite zones of inhibition. The plates were incubated for 18 to 24 hours at 37°C, and the diameters of inspected zones of inhibition were calculated and documented, while any small apparent colonies within the zone were neglected. The disc with no zone of inhibition was listed as 6 mm. The presence of MBLs was suggested by ≥5 mm discrepancy in disc zone diameters, noticed only between disc B and disc A while, the difference between disc C or disc D and disc A was <5 mm. Additionally, KPC production was identified if there was only ≥5 mm variance between disc C and disc A (but not between disc B or disc D and disc A); the presence of a 5 mm zone difference between both discs C and D in comparison to disc A was an indication of AmpC production with porin loss. If there were no synergistic effects between discs A–D, a detection of 10 mm in the diameter of the inhibition zone around disc E was evidence of OXA-48 carbapenemase production.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics for Windows, Version 25.0. (IBM Corp, 2017). Numbers and percentages were used to present qualitative data. Median and interquartile ranges were used to assess non-normally distributed continuous data. The diagnostic performance of KPC, MBL and OXA-48 was expressed as sensitivity, specificity, positive and negative predictive values. Cox regression analysis was done to measure hazard ratio and its 95% confidence interval. Statistical significance was considered at P-value ≤0.05.
Results
Out of 357 patients on mechanical ventilation, only 250 developed VAP. Fungal infection, gram-positive, and gram-negative bacterial infection were detected in 35, 68 and 147 patients, respectively. In gram-negative bacterial infection, 64 isolates were sensitive to carbapenems while 83 isolates showed resistance to carbapenems.
The clinical and demographic data of patients with carbapenem-resistant gram-negative bacteria are illustrated in Table 1, including age, sex, associated comorbidities, duration of hospitalization, days of ventilation and the outcome. Most cases were male (61.4%), aged from 32 to 63 years. The average duration of hospital stay ranged between 10–20 days; in addition, most patients needed mechanical ventilation for 7–13 days. Trauma, diabetes mellitus and chronic diseases as liver diseases, renal diseases, cancer, ischemic insult and chest diseases were present in these patients. Moreover, death occurred in 30.1% of cases during the period of our study.
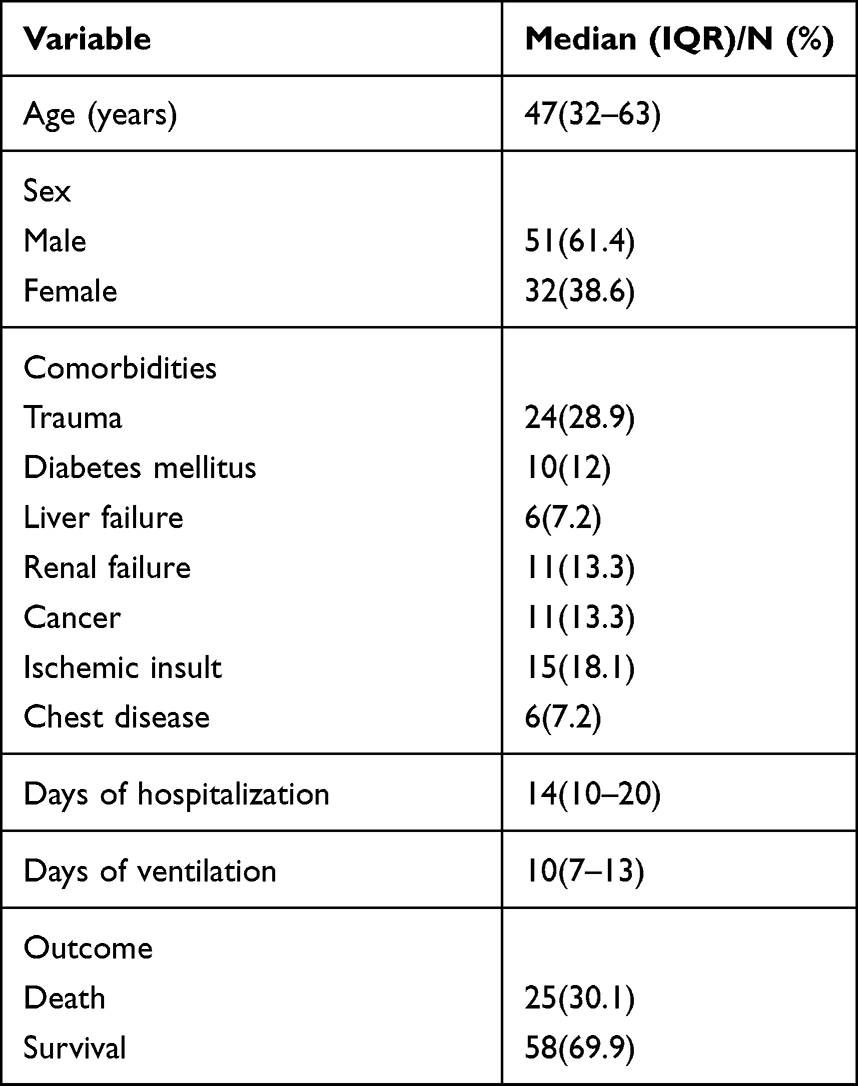 |
Table 1 Demographic and Clinical Data of Studied Patients |
K. pneumonia was the most frequent gram-negative organism detected, followed by A. baumannii, P. aeruginosa and E. coli, representing 34.9%, 20.5%, 18.1% and 12%, respectively. Other organisms were detected in different percentages, as shown in Table 2. As regarding carbapenemase gene detection by PCR, blaKPC, blaNDM, and blaOXA-48 were mostly detected in K. pneumoniae species in variable percentages (37.9%, 20.7% and 20.7%, respectively) and only 2 cases of K. pneumoniae were negative for all three genes. The incidence of these previously mentioned genes in other detected organisms is illustrated in Table 2. Both blaKPC and blaNDM were detected together in 2 cases of K. pneumoniae and 4 cases of P. aeruginosa infection; in addition, both blaKPC and blaOXA-48 existed together in 2 cases of K. pneumoniae while 2 cases of A. baumannii infection showed both blaNDM and blaOXA-48 genes. This data is well demonstrated in Table 2 and Figure 1.
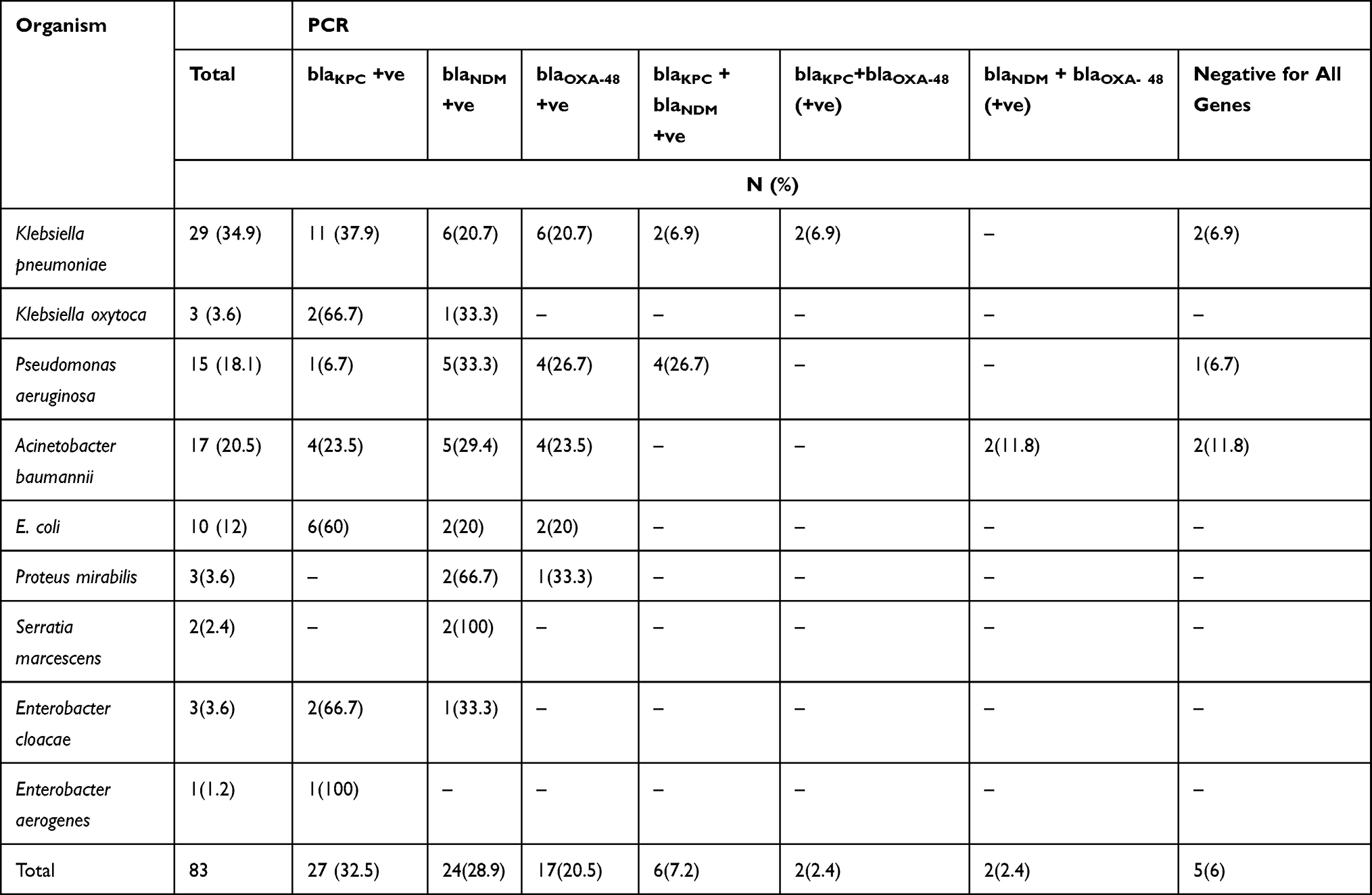 |
Table 2 Genotypic Detection of Carbapenemase Genes in Carbapenem-Resistant Gram-Negative Bacilli |
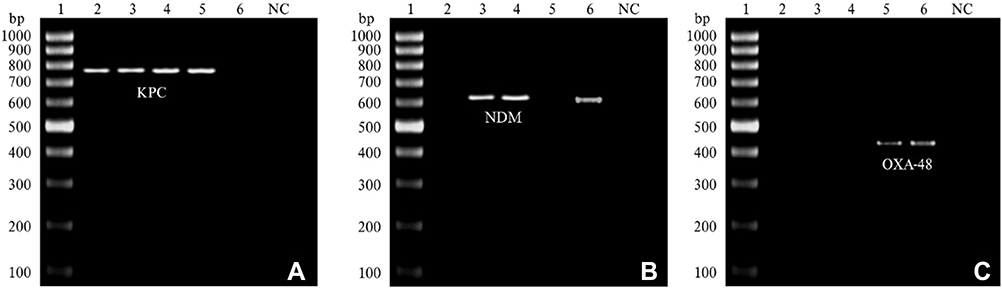 |
Figure 1 Agarose gel electrophoresis of blaKPC, blaNDM, and blaOXA-48 carbapenemase genes amplicons. DNA ladder 100 bp in lane 1. (A) Lanes (2, 3, 4 and 5) positive for blaKPC gene (798bp). (B) Lanes (3, 4, and 6) positive for blaNDM gene (621bp). (C) lanes (5, 6): positive for blaOXA-48 gene (438 bp). Abbreviations: DNA, deoxyribonucleic acid; bp, base pair. |
Figure 2 and Table 3 show the results of MASTDISCS combi Carba plus disc system in detection of carbapenemase ability in enterobacterales; 2 cases of K. pneumoniae infection and only one case of E. coli and Serratia marcescens were negative by MASTDISCS combi Carba plus disc system. All cases of K. oxytoca, Proteus, Enterobacter cloacae and Enterobacter aerogenes infection were positive by MASTDISCS combi Carba plus disc system. A. baumannii and P. aeruginosa were not tested by MASTDISCS combi Carba plus disc system.
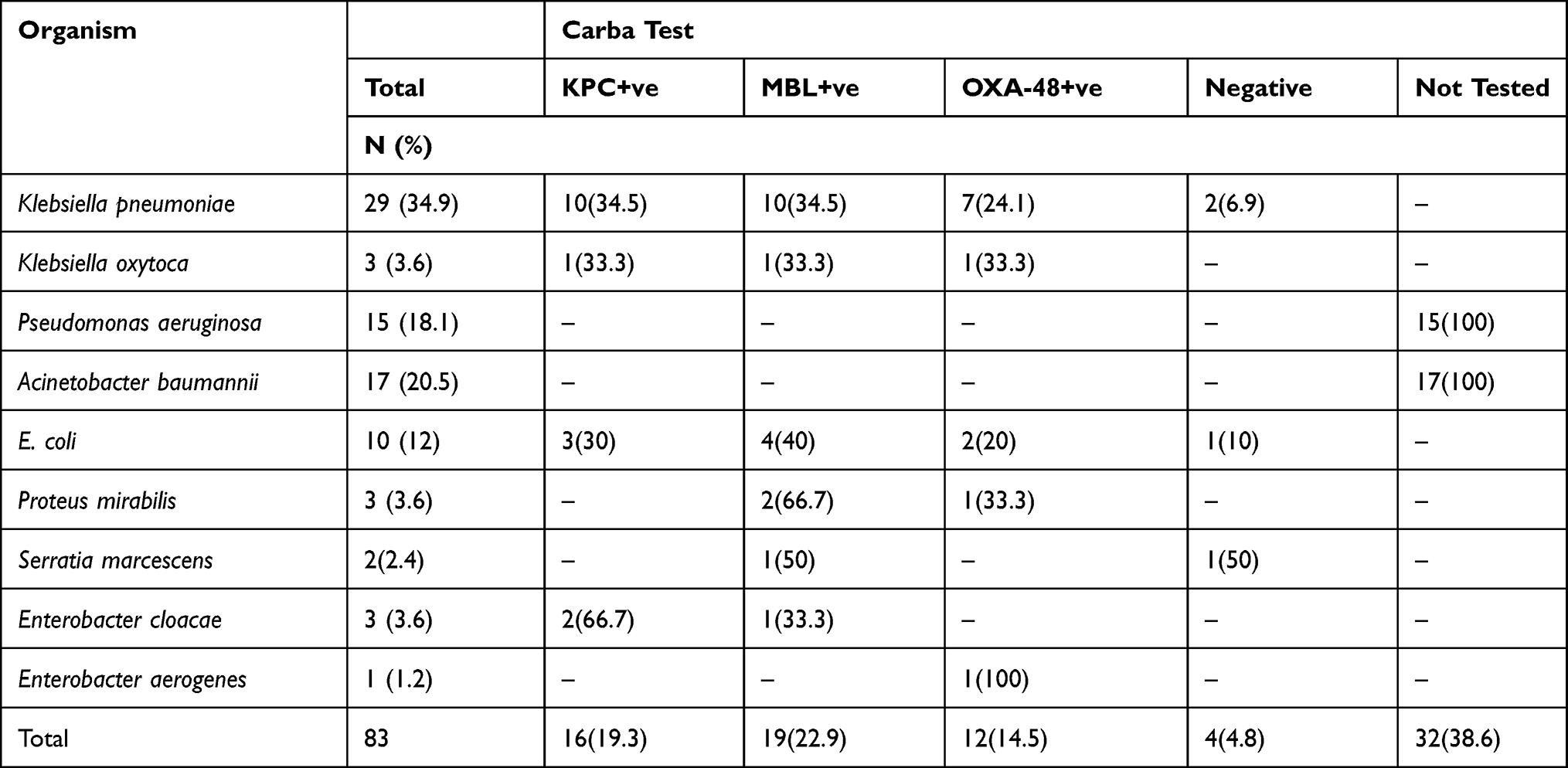 |
Table 3 MASTDISCS Combi Carba Plus Disc System Results in Carbapenem-Resistant Gram-Negative Bacilli |
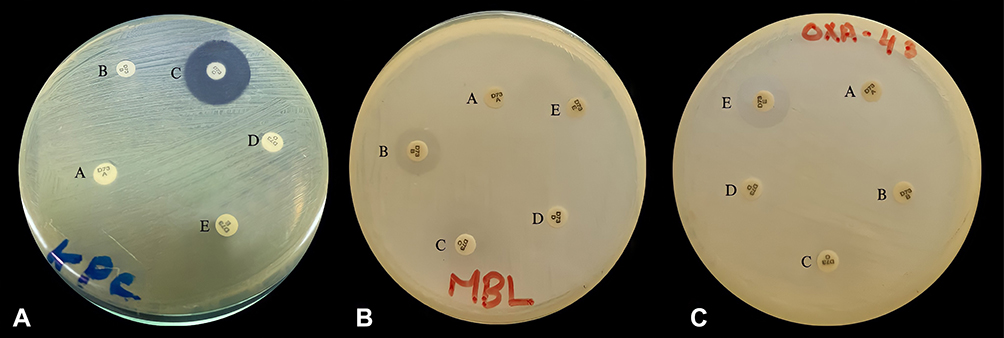 |
Figure 2 Positive results of MAST-Carba plus assay .(A) KPC positive, the diameter difference between disc C and disc A was ≥5 mm and <5 mm difference between disc B or disc D and disc A. (B) MBL positive, the diameter difference between disc B and disc A was ≥5 mm and <5 mm difference between disc C or disc D and disc A. (C) OXA-48 positive, the zone of inhibition around disc E was ≤10 mm with no synergy between discs A–D. |
As regarding sensitivity, specificity, positive and negative predictive values of MASTDISCS combi Carba plus disc system in relation to PCR, the test showed the highest sensitivity and specificity levels concerning OXA-48 carbapenemase (81.8% and 92.5%, respectively). The sensitivity and specificity regarding the other genes are shown in Table 4.
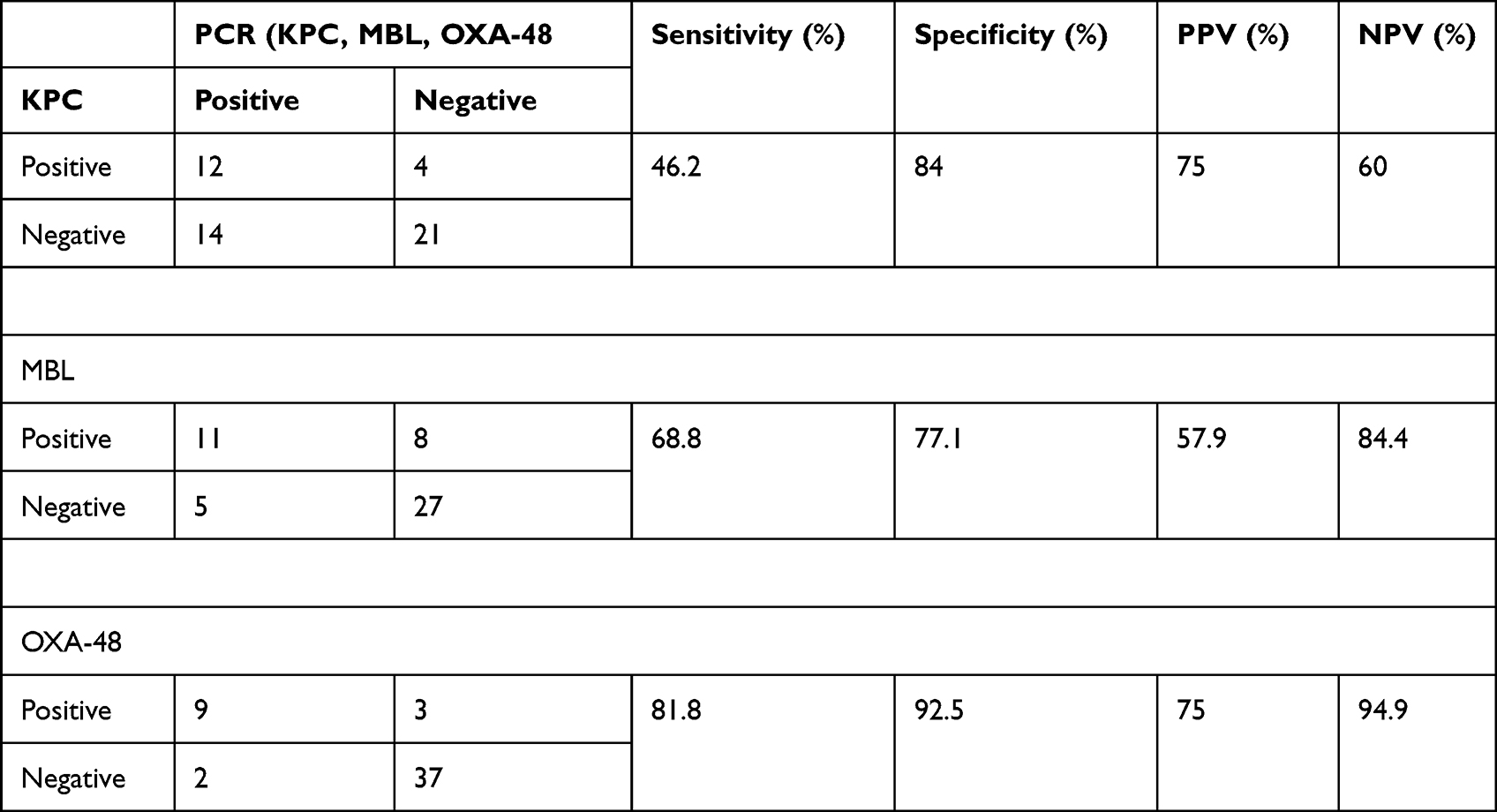 |
Table 4 Sensitivity, Specificity, Positive and Negative Predictive Values of MASTDISCS Combi Carba Plus Disc System in Comparison to PCR |
Regarding the potential predictors of death in the present study, it was detected that mechanical ventilation persistent for less than 15 days and P. aeruginosa species infection were associated with higher death rates, and the results were statistically significant with p-values of 0.008 and 0.006, respectively, as shown in Table 5.
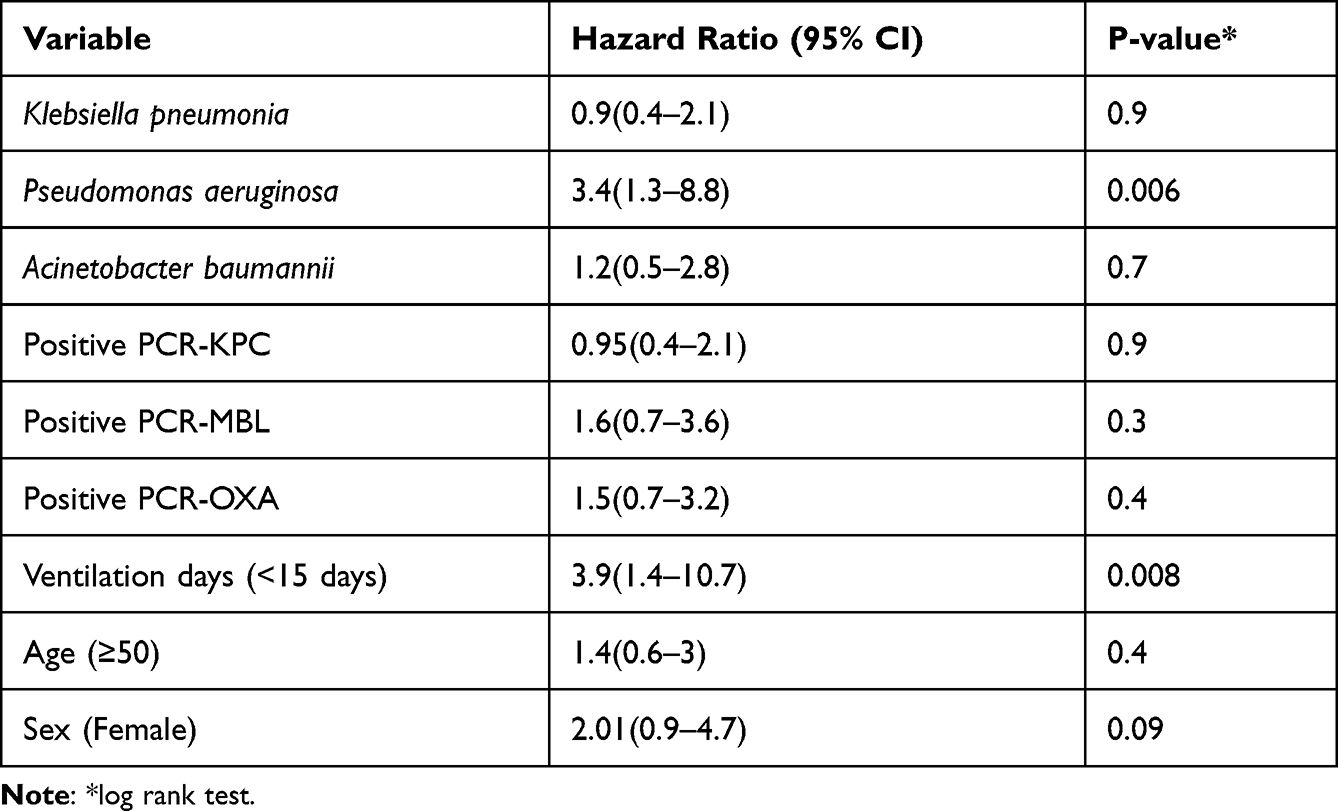 |
Table 5 Univariate Cox Proportional Hazards Regression of the Association Between Demographic and Clinical Variables with Respect to Overall Survival |
Discussion
Carbapenem resistance in gram-negative bacteria is considered one of the most devastating problems, especially in VAP patients in critical care units.18 Nordmann and Poirel documented that Enterobacteriaceae, P. aeruginosa and A. baumannii are the most common microorganisms involved in carbapenem resistance.19 Therefore, early detection of CR-GNB and the carbapenemase gene responsible for its resistance is essential for better selection of the appropriate antimicrobial therapy, improving the outcome and achieving the best infection control measures.12
This study was designed to identify the prevalence of CR-GNB infections, assess their impact on patient outcome, detect the presence of carbapenemase genes in the isolated strains by PCR and to assess the use of MASTDISCS combi Carba plus in the armamentarium of phenotypic identification of carbapenemase-producing enterobacterales isolated from VAP patients in ICUs.
Eighty-three CR-GNB infections were isolated from 250 microbiologically confirmed VAP patients (33%). The present study detected a greater prevalence of CR-GNB infections in males, representing 61.4% of patients. These results match those of studies carried out by Farag et al, Djordjevic et al, and Rana et al.18,20,21 Furthermore, the age of presentation in our study ranged from 32 to 63 years, with an average duration of hospital stay of 14 days. This is quite similar to Khairy et al, who reported that prolonged hospital stay of more than 10 days was associated with higher incidence of carbapenem resistance.22 This can be explained by the fact that patients with prolonged hospital stay were more liable to higher rates of nosocomial infection and invasive procedures that necessitate improper use of combined antibiotics as empirical treatment.23
Various comorbidities were identified as risk factors for VAP development. In our study, trauma was the most important predisposing factor, representing 28.9%, followed by different chronic diseases. These findings agree with those of previous studies in which VAP developed in patients with severe injuries due to coagulopathy on top of early trauma.24–26 Meanwhile, Chang et al, Jimenez-Trujillo et al and Liu et al listed different chronic diseases as commonly associated factors in VAP patients, which occur in old patients with depressed immunity that subsequently renders them more susceptible to severe bacterial infection.27–29 As regarding the outcome in VAP patients, death occurred in 30.1% throughout the study duration. This finding was similar to those of Kalil et al and Chouhdari et al, in which the mortality rates ranged between 20–50% and 41%, respectively.30,31 However, in the study by Melsen et al, only 9% of VAP patients died.32 On the contrary, death rate may be close to zero in less severe underlying conditions. This variation may be due to the difference in severity of the underlying systemic condition, duration of hospital stay, mechanical ventilation, concomitant bacterial infection, and emergence of antibiotic resistance.33
Concerning the type of bacteria detected in the current study, K. pneumoniae was the predominant isolate, followed by A. baumannii, P. aeruginosa and E. coli, representing 34.9%, 20.5%, 18.1% and 12%, respectively. This result was in agreement with Mohammed et al and Gajdacs et al.34,35 In contrast, greater prevalence of P. aeruginosa was detected in other studies.36,37 Meanwhile, Chen et al, Kumari et al, and Sadigov et al reported that A. baumannii was the most prevalent CR-GNB pathogen, accounting for 78.7%, 37.4%, and 37.1%, respectively.38–40 This variation could be the result of geographical differences between the countries, patient population and clinical setting.20
Determination of whether the gram-negative isolate is a carbapenemase producer is essential for epidemiological studies and also for selection of the appropriate treatment for infections.41 With respect to carbapenemase gene identification by PCR, the blaKPC gene achieved the highest level (32.5%), followed by the blaNDM gene (28.9%), and finally the blaOXA-48 gene (20.5%). K. pneumoniae was the most common organism harboring the 3 genes. Similarly, an elevated level of blaKPC expression among carbapenem-resistant K. pneumoniae isolates was identified in the Hussein et al and Lopes et al studies.42,43 Nevertheless, Raheel et al showed that the most commonly presented gene was the blaOXA-48 (96.2%) and least frequent gene was the blaKPC (7.5%).44
In addition, one other study reported that OXA-48 and NDM1 were frequently detected in Enterobacteriaceae, while KPC was not detected.45 Furthermore, other studies stated that blaNDM was the predominant gene.46,47 The major differences were likely due to different geographic region, antibiotics policy in different health care settings and methods of gene identification.48
In our study, more than one resistance gene was detected in different isolates. KPC and MBL, KPC and OXA-48 or MBL and OXA-48 coexisted in K. pneumoniae, P. aeruginosa, and A. baumannii isolates. Several studies revealed that K. pneumoniae and A. baumannii harbored more than one gene, making them more likely to be multi- or pan-drug resistant.49–53 This finding can be challenged due to risk of resistance transmission and restricted antibiotics valuable for treatment, as old antibiotics such as colistin are losing efficacy.54,55 Interestingly, five organisms were negative to all studied carbapenemase genes in the present study. However, Haji et al reported only two isolates that do not show any genes.52
The efficacy of MAST-Carba plus in detection of carbapenemase activity was evaluated in relation to PCR results. The highest sensitivity, specificity, positive and negative predictive values was reported for OXA-48 detection (81.8% 92.5%, 75% and 94.9, respectively). This agrees with Hu et al, who detected the highest values for the same gene.11 The high positive predictive value can be explained by the resistance of K. pneumoniae to temocillin, which presents in disc E of MAST-Carba plus and is associated with false-positive results.56,57 KPC detection in our study showed the lowest sensitivity, specificity, positive and negative predictive values by MAST-Carba plus (46.2%, 84%, 75% and 60%, respectively). As regarding MBL gene, its sensitivity, specificity, positive and negative predictive values were intermediate between the two genes. This agrees with Hu et al, who reported the lowest sensitivity of MAST-Carba plus to KPC gene in comparison to OXA-48 and MBL genes.11 In contrast to our result, MAST-Carba plus can detect 5/5 OXA-48, 15/15 MBL and 2/2 KPC with 100% sensitivity.12 The discrepancy of the values is due to geographical and racial differences and the inability of MAST-Carba plus to detect strains producing two genes together. Since VAP caused by CR-GNB is associated with high mortality rate, identifying risk factors and outcomes is critical for guiding therapeutic options. The current study evaluated the predictors of mortality of these patients and detected that mechanical ventilation persistent for less than 15 days and P. aeruginosa species infection were significantly associated with higher death rates. Consistent with our findings, Micek et al found that P. aeruginosa infection is responsible for one-third to half of all VAP-associated deaths.58 Meanwhile, Sadigov et al reported that the only independent risk factor for increased hospital mortality in VAP patients was A. baumannii infection.40 However, in previous studies, length of hospital stays more than 9 days preceding the incidence of nosocomial pneumonia was a significant predictor of mortality.38,59 Prolonged hospitalization was linked to higher risk of infection with antibiotic resistant pathogens, which resulted in higher mortality. However, Tuon et al reported that the VAP patients older than 50 years were exposed to higher mortality rate.60 Also, Feng et al found that age more than 70 years was one of the predictors of mortality in nosocomial pneumonia caused by GNB.61 Lack of Ampc gene detection was the main limitation in the current study, hence further studies of longer duration and with a higher number of enterobacterale isolates are required to monitor the role of MASTDISCS combi plus in identification of this gene. Furthermore, other MBL genes like VIM and IMP were not tested in our study.
Conclusion
This study emphasized high incidence of carbapenem-resistant gram-negative bacilli causing pneumonia in mechanically ventilated patients,which focused attention on using MASTDISCS combi Carba plus for rapid detection of carbapenemase producers to improve the outcome in these critically ill patients.
Ethical Approval
The study was approved by the Institutional review board of the Faculty of Medicine, Tanta University, Egypt (approval code 35342/3/22) and was designed according to Declaration of Helsinki guidelines. Written informed consent from the first-degree relatives was obtained.
Consent to Publish
Written informed consent was obtained from the first-degree relatives of each participant to publish their data in this journal.
Acknowledgments
The authors express their great appreciation to all members of the ICUs, Chest and Medical Microbiology and Immunology departments, Tanta University, Egypt for their help throughout the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rosenthal VD, Al-Abdely HM, El-Kholy AA, et al. International nosocomial infection control consortium report, data summary of 50 countries for 2010–2015: device-associated module. Am J Infect Control. 2016;44(12):1495–1504. doi:10.1016/j.ajic.2016.08.007
2. Kalanuria AA, Mirski M, Ziai W. Ventilator-associated pneumonia in the ICU. In: Annual Update in Intensive Care and Emergency Medicine; Vol. 2014, 2014: 65–77.
3. Koenig SM, Truwit JD. Ventilator-associated pneumonia: diagnosis, treatment, and prevention. Clin Microbiol Rev. 2006;19(4):637–657. doi:10.1128/CMR.00051-05
4. Abdeta A, Bitew A, Fentaw S, et al. Phenotypic characterization of carbapenem non-susceptible gram-negative bacilli isolated from clinical specimens. PLoS One. 2021;16(12):e0256556. doi:10.1371/journal.pone.0256556
5. Yan WJ, Jing N, Wang SM, et al. Molecular characterization of carbapenem-resistant Enterobacteriaceae and emergence of tigecycline non-susceptible strains in the Henan province in China: a multicentrer study. J Med Microbiol. 2021;70(3). doi:10.1099/jmm.0.001325.
6. Shaker OA, Gomaa HE, ElMasry SA, Halim RM, Abdelrahman AH, Kamal JS. Evaluation of combined use of temocillin disk and mastdisks inhibitor combination set against polymerase chain reaction for detection of carbapenem-resistant Enterobacteriaceae. Open Access Maced J Med Sci. 2018;6(2):242. doi:10.3889/oamjms.2018.090
7. Paskeh MD, Moghaddam MJ, Salehi Z. Prevalence of plasmid-encoded carbapenemases in multi-drug resistant Escherichia coli from patients with urinary tract infection in northern Iran. Iran J Basic Med Sci. 2020;23(5):586. doi:10.22038/ijbms.2020.34563.8199
8. Sheikh AF, Shahin M, Shokoohizadeh L, Ghanbari F, Solgi H, Shahcheraghi F. Emerge of NDM-1-producing multidrug-resistant Pseudomonas aeruginosa and co-harboring of carbapenemase genes in South of Iran. Iran J Public Health. 2020;49(5):959.
9. Han R, Shi Q, Wu S, et al. Dissemination of carbapenemases (KPC, NDM, OXA-48, IMP, and VIM) among carbapenem-resistant Enterobacteriaceae isolated from adult and children patients in China. Front Cell Infect Microbiol. 2020;10:314. doi:10.3389/fcimb.2020.00314
10. Algammal AM, El-Sayed ME, Youssef FM, et al. Prevalence, the antibiogram and the frequency of virulence genes of the most predominant bacterial pathogens incriminated in calf pneumonia. AMB Express. 2020;10(1):1–8. doi:10.1186/s13568-020-01037-z
11. Hu W, Li M, Lu W, Guo S, Li J. Evaluation of MASTDISCS combi Carba plus for the identification of metallo‐β‐lactamases, KPC and OXA‐48 carbapenemase genes in Enterobacteriaceae clinical isolates. Lett Appl Microbiol. 2020;70(1):42–47. doi:10.1111/lam.13240
12. Ohsaki Y, Kubo R, Hobson J, et al. MASTDISCS combi Carba plus, a simple method for discriminating carbapenemase‐producing Enterobacteriaceae, including OXA‐48‐type producers. Microbiol Immunol. 2018;62(1):60–65. doi:10.1111/1348-0421.12553
13. Elkolaly RM, Bahr HM, El-Shafey BI, Basuoni AS, Elber EH. Incidence of ventilator-associated pneumonia: Egyptian study. Egypt J Bronchol. 2019;13(2):258–266. doi:10.4103/ejb.ejb_43_18
14. Daniel W. Biostatistics: A Foundation for Analysis in the Health Sciences.
15. Forbes BA, Sahm DF, Weissfeld AS. Study Guide for Bailey and Scott’s Diagnostic Microbiology-E-Book. Elsevier Health Sciences; 2016.
16. Clinical and Laboratory Standards Institute [CLSI]. Performance Standards for Antimicrobial Susceptibility Testing; Supplement M100.
17. Michodigni NF, Nyacheo A, Akhwale JK, Magoma G, Kimang’a AN. Molecular Identification of Co-existence of Carbapenemase and extended-spectrum β-lactamase genes in Klebsiella pneumoniae clinical isolates, and their phylogenetic patterns in Kenya. Adv Microbiol. 2021;11(8):399–415. doi:10.4236/aim.2021.118030
18. Farag AM, Tawfick MM, Abozeed MY, Shaban EA, Abo-Shadi MA. Microbiological profile of ventilator-associated pneumonia among intensive care unit patients in tertiary Egyptian hospitals. J Infect Dev Countries. 2020;14(02):153–161. doi:10.3855/jidc.12012
19. Nordmann P, Poirel L. Epidemiology and diagnostics of carbapenem resistance in gram-negative bacteria. Clin Infect Dis. 2019;69(Supplement_7):S521–8. doi:10.1093/cid/ciz824
20. Djordjevic ZM, Folic MM, Jankovic SM. Distribution and antibiotic susceptibility of pathogens isolated from adults with hospital-acquired and ventilator-associated pneumonia in intensive care unit. J Infect Public Health. 2017;10(6):740–744. doi:10.1016/j.jiph.2016.11.016
21. Rana G, Sharma S, Hans C. Ventilator-associated pneumonia in the ICU: microbiological Profile. J Bacteriol Mycol. 2017;4:165–168.
22. Khairy RM, Mahmoud MS, Shady RR, Esmail MA. Multidrug‐resistant Klebsiella pneumoniae in hospital‐acquired infections: concomitant analysis of antimicrobial resistant strains. Int J Clin Pract. 2020;74(4). doi:10.1111/ijcp.13463
23. Gao B, Li X, Yang F, et al. Molecular epidemiology and risk factors of ventilator-associated pneumonia infection caused by carbapenem-resistant Enterobacteriaceae. Front Pharmacol. 2019;10:262. doi:10.3389/fphar.2019.00262
24. Michetti CP, Prentice HA, Rodriguez J, Newcomb A. Supine position and nonmodifiable risk factors for ventilator-associated pneumonia in trauma patients. Am J Surg. 2017;213(2):405–412.
25. Arumugam SK, Mudali I, Strandvik G, El-Menyar A, Al-Hassani A, Al-Thani H. Risk factors for ventilator-associated pneumonia in trauma patients: a descriptive analysis. World J Emerg Med. 2018;9(3):203. doi:10.5847/wjem.j.1920-8642.2018.03.007
26. Younan D, Lin E, Griffin R, et al. Early trauma-induced coagulopathy is associated with increased ventilator-associated pneumonia in spinal cord injury patients. Shock. 2016;45(5):502–505.
27. Chang L, Dong Y, Zhou P. Investigation on risk factors of ventilator-associated pneumonia in acute cerebral hemorrhage patients in intensive care unit. Can Respir J. 2017;2017:1–4. doi:10.1155/2017/7272080
28. Jiménez-Trujillo I, Jiménez-García R, de Miguel-Díez J, et al. Incidence, characteristic and outcomes of ventilator-associated pneumonia among type 2 diabetes patients: an observational population-based study in Spain. Eur J Intern Med. 2017;40:72–78. doi:10.1016/j.ejim.2017.01.019
29. Liu Y, Di Y, Fu S. Risk factors for ventilator-associated pneumonia among patients undergoing major oncological surgery for head and neck cancer. Front Med. 2017;11(2):239–246. doi:10.1007/s11684-017-0509-8
30. Kalil AC, Metersky ML, Klompas M, et al. Executive summary: management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):575–582. doi:10.1093/cid/ciw504
31. Chouhdari A, Shokouhi S, Bashar FR, et al. Is a low incidence rate of ventilation associated pneumonia associated with lower mortality? A descriptive longitudinal study in Iran. Tanaffos. 2018;17(2):110.
32. Melsen WG, Rovers MM, Koeman M, Bonten MJ. Estimating the attributable mortality of ventilator-associated pneumonia from randomized prevention studies. Crit Care Med. 2011;39(12):2736–2742. doi:10.1097/CCM.0b013e3182281f33
33. Melsen WG, Rovers MM, Groenwold RH, et al. Attributable mortality of ventilator-associated pneumonia: a meta-analysis of individual patient data from randomised prevention studies. Lancet Infect Dis. 2013;13(8):665–671. doi:10.1016/S1473-3099(13)70081-1
34. Mohamed A, Daef E, Nafie A, Shaban L, Ibrahim M. Characteristics of Carbapenem-resistant gram-negative bacilli in patients with ventilator-associated pneumonia. Antibiotics. 2021;10(11):1325. doi:10.3390/antibiotics10111325
35. Gajdács M, Ábrók M, Lázár A, et al. Detection of VIM, NDM and OXA-48 producing carbapenem resistant Enterobacterales among clinical isolates in Southern Hungary. Acta Microbiol Immunol Hung. 2020;67(4):209–215. doi:10.1556/030.2020.01181
36. Gupta R, Malik A, Rizvi M, Ahmed M, Singh A. Epidemiology of multidrug-resistant Gram-negative pathogens isolated from ventilator-associated pneumonia in ICU patients. J Glob Antimicrob Resist. 2017;9:47–50. doi:10.1016/j.jgar.2016.12.016
37. Rezai MS, Ahangarkani F, Rafiei A, Hajalibeig A, Bagheri-Nesami M. Extended-spectrum beta-lactamases producing Pseudomonas aeruginosa isolated from patients with ventilator associated nosocomial infection. Arch Clin Infect Dis. 2018;13(4). doi:10.5812/archcid.13974
38. Chen CY, Yang KY, Peng CK, et al. Clinical outcome of nosocomial pneumonia caused by Carbapenem-resistant gram-negative bacteria in critically ill patients: a multicenter retrospective observational study. Sci Rep. 2022;12(1):1. doi:10.1038/s41598-021-99269-x
39. Kumari M, Verma S, Venkatesh V, et al. Emergence of blaNDM-1 and blaVIM producing Gram-negative bacilli in ventilator-associated pneumonia at AMR Surveillance Regional Reference Laboratory in India. PLoS One. 2021;16(9):e0256308. doi:10.1371/journal.pone.0256308
40. Sadigov A, Mamedova I, Mammmadov K. Ventilator-associated pneumonia and in-hospital mortality: which risk factors may predict in-hospital mortality in such patients? J Lung Health Dis. 2019;3(4):8–12. doi:10.29245/2689-999X/2019/4.1157
41. Tsai YM, Wang S, Chiu HC, Kao CY, Wen LL. Combination of modified carbapenem inactivation method (mCIM) and EDTA-CIM (eCIM) for phenotypic detection of carbapenemase-producing Enterobacteriaceae. BMC Microbiol. 2020;20(1):1–7. doi:10.1186/s12866-020-02010-3
42. Hussein NH, Hussein AL-Kakei SN, Taha BM. The predominance of Klebsiella pneumoniae carbapenemase (KPC-type) gene among high-level carbapenem-resistant Klebsiella pneumoniae isolates in Baghdad, Iraq. Mol Biol Rep. 2022;26:1–6.
43. Lopes E, Saavedra MJ, Costa E, de Lencastre H, Poirel L, Aires-de-Sousa M. Epidemiology of carbapenemase-producing Klebsiella pneumoniae in northern Portugal: predominance of KPC-2 and OXA-48. J Glob Antimicrob Resist. 2020;22:349–353. doi:10.1016/j.jgar.2020.04.007
44. Raheel A, Azab H, Hessam W, Abbadi S, Ezzat A. Detection of carbapenemase enzymes and genes among carbapenem-resistant Enterobacteriaceae isolates in Suez Canal University Hospitals in Ismailia, Egypt. Microbes Infect Dis. 2020;1(1):24–33. doi:10.21608/mid.2020.25702.1007
45. Memish ZA, Assiri A, Almasri M, et al. Molecular characterization of carbapenemase production among gram-negative bacteria in Saudi Arabia. Microb Drug Resist. 2015;21(3):307–314. doi:10.1089/mdr.2014.0121
46. Vamsi SK, Moorthy RS, Hemiliamma MN, Shravani S. Phenotypic and genotypic detection of carbapenemase production among gram negative bacteria isolated from hospital acquired infections. Saudi Med J. 2022;43(3):236–243. doi:10.15537/smj.2022.43.3.20210809
47. Naim H, Rizvi M, Gupta R, et al. Drug resistance and molecular epidemiology of carbapenem resistant gram-negative bacilli isolates. J Glob Infect Dis. 2018;10(3):133. doi:10.4103/jgid.jgid_74_17
48. Al-Ouqaili MT. Identification of an OprD and blaIMP gene-mediated carbapenem resistance in Acinetobacter baumannii and Pseudomonas aeruginosa among patients with wound infections in Iraq. Asian J Pharmaceut. 2018;12:03.
49. Ain NU, Iftikhar A, Bukhari SS, et al. High frequency and molecular epidemiology of metallo-β-lactamase-producing gram-negative bacilli in a tertiary care hospital in Lahore, Pakistan. Antimicrob Resist Infect Control. 2018;7(1):1–9. doi:10.1186/s13756-018-0417-y
50. Sadeghi MR, Ghotaslou R, Akhi MT, Asgharzadeh M, Hasani A. Molecular characterization of extended-spectrum β-lactamase, plasmid-mediated AmpC cephalosporinase and carbapenemase genes among Enterobacteriaceae isolates in five medical centres of East and West Azerbaijan, Iran. J Med Microbiol. 2016;65(11):1322–1331. doi:10.1099/jmm.0.000356
51. Masseron A, Poirel L, Ali BJ, Syed MA, Nordmann P. Molecular characterization of multidrug-resistance in Gram-negative bacteria from the Peshawar teaching hospital, Pakistan. New Microbes New Infect. 2019;32:100605. doi:10.1016/j.nmni.2019.100605
52. Haji SH, Aka ST, Ali FA. Prevalence and characterisation of carbapenemase encoding genes in multidrug-resistant Gram-negative bacilli. PLoS One. 2021;16(11):e0259005. doi:10.1371/journal.pone.0259005
53. Okoche D, Asiimwe BB, Katabazi FA, Kato L, Najjuka CF. Prevalence and characterization of carbapenem-resistant Enterobacteriaceae isolated from Mulago National Referral Hospital, Uganda. PLoS One. 2015;10(8):e0135745. doi:10.1371/journal.pone.0135745
54. Solgi H, Badmasti F, Aminzadeh Z, et al. Molecular characterization of intestinal carriage of carbapenem-resistant Enterobacteriaceae among inpatients at two Iranian university hospitals: first report of co-production of bla NDM-7 and bla OXA-48. Eur J Clin Microbiol Infect Dis. 2017;36(11):2127–2135. doi:10.1007/s10096-017-3035-3
55. Di Tella D, Tamburro M, Guerrizio G, Fanelli I, Sammarco ML, Ripabelli G. Molecular epidemiological insights into colistin-resistant and carbapenemases-producing clinical Klebsiella pneumoniae isolates. Infect Drug Resist. 2019;12:3783. doi:10.2147/IDR.S226416
56. Zioga A, Miriagou V, Tzelepi E, et al. The ongoing challenge of acquired carbapenemases: a hospital outbreak of Klebsiella pneumoniae simultaneously producing VIM-1 and KPC-2. Int J Antimicrob Agents. 2010;36(2):190–191. doi:10.1016/j.ijantimicag.2010.04.002
57. Mathers AJ, Crook D, Vaughan A, et al. Klebsiella quasipneumoniae provides a window into carbapenemase gene transfer, plasmid rearrangements, and patient interactions with the hospital environment. Antimicrob Agents Chemother. 2019;63(6):13–18. doi:10.1128/AAC.02513-18
58. Micek ST, Wunderink RG, Kollef MH, et al. An international multicenter retrospective study of Pseudomonas aeruginosa nosocomial pneumonia: impact of multidrug resistance. Crit Care. 2015;19(1):1–8. doi:10.1186/s13054-015-0926-5
59. Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J. 2017;50(3):23.
60. Tuon FF, Graf ME, Merlini A, et al. Risk factors for mortality in patients with ventilator-associated pneumonia caused by carbapenem-resistant Enterobacteriaceae. Brazil J Infect Dis. 2017;21(1):1–6. doi:10.1016/j.bjid.2016.09.008
61. Feng DY, Zhou YQ, Zou XL, et al. Factors influencing mortality in hospital-acquired pneumonia caused by Gram-negative bacteria in China. J Infect Public Health. 2019;12(5):630–633. doi:10.1016/j.jiph.2019.02.014
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.