Back to Journals » Patient Preference and Adherence » Volume 17
Capturing What Matters with Patients’ Bypass Behavior? Evidence from a Cross-Sectional Study in China
Authors Xie W, Liu J ![]() , Huang Y, Xi X
, Huang Y, Xi X
Received 23 November 2022
Accepted for publication 18 February 2023
Published 8 March 2023 Volume 2023:17 Pages 591—604
DOI https://doi.org/10.2147/PPA.S395928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Wenwen Xie, Jiayuan Liu,* Yuankai Huang,* Xiaoyu Xi
The Research Center of National Drug Policy & Ecosystem, China Pharmaceutical University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyu Xi, Email [email protected]
Background: In China, bypassing is becoming increasingly prevalent. Such behavior, as going directly to upper-level health-care facilities without a primary care provider (PCP) referral when facing non-critical diseases, contrasts to “expanding the role of PCPs as the first-contact of care”, may cause unneglectable damage to the healthcare system and people’s physical health.
Objective: To examine the relationship between patient experience in primary health-care clinics (PHCs) and their bypass behavior.
Methods: A cross-sectional study was designed for data collection. From July 2021 to August 2021, we conducted a questionnaire survey nationally. Fifty-three investigators were dispatched to 212 pre-chosen PHCs, around which 1060 interviewees were selected to gather information, using a convenience sampling. The primary independent variable was scores measured by Chinese Primary Care Assessment Tool (PCAT-C) to quantify patients’ experience at PHCs. The dependent variable was a binary variable measured by a self-developed instrument to identify whether participants actually practiced bypassing. Covariates were well-screened determinants of patients’ bypass behavior including socio-demographic factors, policy factors, and health-care suppliers. Binary logistic regression analysis was employed to evaluate the association of patients’ experience with their bypass behavior.
Findings: A total of 928 qualified questionnaires were obtained. The first contact dimension (OR 0.961 [95% CI 0.934 to 0.988], P = 0.005) and continuity dimension (OR 1.034 [95% CI 1.000 to 1.068], P = 0.047) of patients’ experience were significantly associated with patients’ bypass behavior (P < 0.05). In addition, age (OR 1.072, [95% CI 1.015– 1.132], P = 0.013) and gender (OR 2.044, [95% CI 1.139– 3.670], P = 0.017) also made a statistically significant difference.
Conclusion: Enhancement in patient experience at PHCs may help reduce their bypass behavior. Specifically, efforts are needed to improve primary care accessibility and utilization. The positive correlation between bypassing rates and continuity scores may require more attention on strengthening PCPs’ technical quality besides the quality of interpersonal interactions.
Keywords: China, bypass behavior, patient experience, primary care, continuity
Plain Language Summary
What is known on this topic
- The prevalent bypass behavior in China contradicts its “promoting primary care providers (PCPs) as the first-contact of care” goal, which reduces healthcare system efficiency and aggravates patients’ disease burden.
- Studies had proved that poor patient-perceived quality of care may lead to bypass behavior, and patient experience is an outstanding indicator for the quality of primary care.
- No country-specific study had been conducted to explore Chinese patients’ experience in primary health-care clinics (PHCs) and its impact on their bypass behavior.
What this study adds
- This study specifically ascertained two domains of patients’ experience—first contact dimension and continuity dimension, where PCPs could put efforts on to retain patients.
- Initiatives to improve primary care accessibility and utilization are needed.
- The positive correlation between bypass rates and continuity scores may require more attention to strengthen PCPs’ technical quality besides the quality of interpersonal interactions.
Introduction
In face of population aging and increases in prevalence of chronic diseases, China is reshaping its healthcare system with a primary care‐oriented approach.1 It aims to enhance patients’ overall health-seeking efficiency and facilitate their rational utilization of medical resources by matching patients’ health-care needs and health-care services including specialty referrals.2
However, bypass, defined specifically as going directly to a higher-level health-care facility without referring from a primary care provider (PCP) when facing non-critical diseases, is becoming increasingly prevalent.3,4 Such behavior contrasts to “expanding the role of PCPs as the first-contact of care”. On the one hand, it wastes resources and skills of providers serving primary health-care clinics (PHCs), and squeezes resources for patients in need of high-level care.5 On the other hand, it causes physicians’ burnout with largely minor illnesses, which seriously undermines their role in addressing advanced medical conditions and engaging in research.6
Apart from these, direct access to a higher-level facility brought patients with higher medical costs,7 lower quality of care, as well as the potential of treatment delay.8 Given the above unneglectable damage to the healthcare system and people’s physical health, it is of great importance and necessity to refrain such irrational health-seeking behavior among Chinese residents.
Globally, many countries attempted to mitigate patients’ bypass behavior by exploring factors and devising effective interventions accordingly. Based on the literature, multiple factors were found to be critical in explaining bypass phenomenon. Firstly, important demographic and socioeconomic factors such as age,9–11 gender,12–15 marital status,16,17 educational attainment,12,16,17 income,9 and health conditions.12,18,19 In general, female and the rich had a higher probability to bypass, while effect of the rest was still controversial across different studies. Secondly, provider characteristics including size and availability of the practice,20,21 geographical accessibility,19–22 service quality and mix,12,20,23–25 cost26 and ownership.20,27 Large local providers with extensive technological capabilities and better service quality decreased bypassing, while long distance worked the opposite. Patients with lower income would bypass expensive local facilities, and private providers were more preferred among US rural residents. In addition, improved insurance coverage28,29 and lack of drug30–32 would both encourage patients’ bypass behavior, which could be classified as medical policies.16,19–22
To divert patients to primary care, China had undertaken various initiatives such as constructing more PHCs nationwide to improve healthcare accessibility, introducing the “Family Doctor Plan” to promote integrated care, and setting gradient reimbursement rates to reduce copayments for patients who visited PCPs prior to accessing the services of a specialist. But they almost did not work.33
Recently, with the care model shifting from “disease-centered” to “patient-centered”, patient-perceived quality of care received a higher-level attention.33 Patient experience, an outstanding indicator of patient-perceived quality of care reported from patients’ perspective, is being increasingly used to assess the quality of primary and higher-level care performance.34 According to the 1994 American Institute of Medicine’s definition, primary care had four core attributes including accessibility, continuity, coordination and comprehensiveness. Researches had proved that better performance in one or several of these dimensions related to a decrease of bypassing: Parents waiting longer were more likely to access emergency department35 directly, and longer travel time also increased the probability of bypassing, reflecting the essential role of accessibility. As for continuity, providers in good attitudes36 and with a deeper communication with patients37 were less bypassed. Having a regular PCP could enhance patient–physician relationship thus led to a 9% reduction in bypass rates.3 Additionally, patients’ lack of knowledge in available service items was also a significant reason for PHCs’ skipping.37
However, very few studies but one from Japan adopted Japanese Primary care assessment tool (JPCAT), which included four core (first-contact care, ongoing care, coordinated care and comprehensive care) and three derivative dimensions (family-centered care, community-oriented care and culturally competent care), fully embodied all four attributes of primary care and found that primary care providers’ efforts to improve patient experience should help to ensure the appropriate use of health-care services under loosely regulated gatekeeping systems.38 Given patient experience is context dependent, country-specific analysis is necessary to gain deeper insights into Chinese residents’ experience in primary care facilities and its impact on bypassing.
To fill this gap, we conducted a nationwide cross-sectional survey, using a widely established Chinese Primary care assessment tool (PCAT-C), to assess a hypothesis: In China, patients’ better experience in primary care facilities could reduce their probability of bypassing. The significance of this research is that it aimed to identify key patient experience dimensions where improvements could be made to enhance patient-perceived quality of care, so as to mitigate the unreasonable bypass behavior in China and throughout the whole world.
Methods
Research Design
Based on informed consent and voluntary participation, a cross-sectional study was conducted for the collection of data.
Study Area
Chinese healthcare system follows a 3-tier hierarchical structure. This study focuses on the lowest level, ie, primary health-care institutions, including community health service centers/stations and rural clinics.
Study Variables
Bypass was the dependent variable. Patient experience was the independent variable. Control variables included patients’ socio-demographic, medical policy, and health-care supplier factors. Questionnaire consisted of 3 parts.
Part 1: Socio-demographic factors, policy factors, and health-care suppliers, which were suggested contributing to bypass behavior in previous studies.39 Socio-demographic factors concerned age, gender, region, education level, marital status, employment status, annual personal/family income and the number of children in different ages. Policy factors mainly included basic medical insurance participation, commercial medical insurance participation, basic drug supply and frequency of contact with PCP.40,41 Health-care suppliers examined the impact of other hospitals except PHCs on bypassing, including quantity of the nearest second- or third-class medical institutions, whether distance and the time to the nearest second- or third-class institutions is less than distance or time to the primary care facilities, in common and convenient transportation.19,33,42,43
Part 2: dependent variable – Bypass. This study adapted the tool from a Japanese study to identify participants’ bypass behavior, which was determined by their response to the following questions:
Did you ever visit a hospital directly without referral from your usual PCP when you have a common health problem (colds, cough, fever, diabetes, hypertension, coronary heart disease and all chronic diseases) in the past year?
Participants were asked to answer on a binary scale (“yes” or “no”). If participants answered “yes” to the first question, they were then asked the following detailed questions on bypass behavior.
- “Did you or your family know that your PCP could provide services you need for your illness when making the above choice?”26 A. Yes, but we did not choose B. No, we did not know C. Not sure.
- “Did you ever visit a hospital directly without referral from your usual PCP on weekdays during the normal office hours of the clinics in the past year?” A. Yes. B. No.
- “Did you ever visit a hospital emergency department directly without referral from your usual PCP in the past year?” A. Yes. B. No.
- “Did you ever need hospitalization without referral from your usual PCP in the past year?” A. Yes. B. No.
Only when the participant answered affirmatively to question (1) and (2), and negatively to question (3) and (4), was s/he determined to have had a bypass visit.
Part 3: independent variable – Patient experience. Chinese Primary Care Assessment Tool (PCAT-C, 36 items) was used to measure six core primary care attributes: first contact, continuity, coordination, comprehensiveness, Family-centeredness, and community orientation.44 A 4-point Likert-type scale was applied to measure certainty as to whether a service was received, ranging from “1” (“Definitely Not”) to “4” (“Definitely”). A neutral response of “Not sure/don’t remember” was provided for the lack of knowledge about a characteristic. Likert scales were finally converted to scores ranging from 0 to 100 by dividing the Likert scale by 4 and multiplying by 100. Each dimension score is the mean of all item scores within that dimension. The total score is the mean scores of six dimensions, with higher scores indicating better performance.
Sampling and Sampling Instruments
A convenience sampling strategy was adopted. All 31 provinces (autonomous regions and municipalities directly under the Central Government) in mainland China were included in the sampling. First, 106 cities with good accessibility and not influenced by COVID-19 were selected. These cities were not evenly distributed in each province, with a maximum of 13 in Jiangsu province and a minimum of 1 in both Hainan and Qinghai provinces. Then, in each selected city, by calling the managers, two primary care facilities in regular operation and with high reception volume were preliminarily identified. Last, around each institution, at least five interviewees were invited to participate and complete the questionnaire by convenience. This ensured that at least 1060 samples can be acquired in total. Hong Kong, Macau, and Taiwan were excluded because the public health system of these three provincial administrative regions is distinctively different from the system applied in mainland China.
The inclusion criteria were as follows: (1) over 18 years old; (2) have health-seeking experience in the last year; (3) willing and able to complete the questionnaire; and the most critically, (4) owning a usual PCP. Two questions were developed to identify a patient’s usual PCP: 1) Is there a doctor that you usually visit if you are sick or need advice about your health? 2) Is there a doctor who knows you best as a person? An interviewee was considered to have a usual PCP at the clinic if s/he positively answered both questions and both two doctors were the same primary physician.
Questionnaire was translated and pre-tested among residents selected around 3 primary health-care facilities in Nanjing, Jiangsu Province, China. Both scales had acceptable reliability and validity (Cronbach’s α 0.937, KMO 0.925 for Bypass and Cronbach’s α 0.783, KMO 0.865 for PCAT-C).
Data Collection and Management
The survey was conducted from July to August, 2021. According to the geographically neighboring principle, the number of PHCs was evenly distributed to 53 investigators, thus each one was responsible for four PHCs in two cities. Potential participants were firstly introduced with the background, content and purpose of the investigation. Those who were willing to participate in the investigation were brought to an undisturbed place, signed the consent form and filled questionnaire using an online survey system on mobile phones or tablet computers. During the whole survey process, investigators should not provide any views about the questionnaire, but only the requirements or instructions for the questionnaire filling.
We selected undergraduates who had medical backgrounds as investigators. Before formal investigation, they are trained with the background, purpose of the research, etiquette, skills to access potential participants, emergencies dealing methods and the use of research software. If participants’ quantity in one city did not meet the requirements, investigator can negotiate with the researcher, who will contact other PHCs and dispatch investigators to collect data for supplement.
Two researchers took the responsibility of reviewing the uploaded data. Once errors or damage were found, investigators were immediately informed to correct by return visits if necessary.
Data Analysis Methods
A binary logit model was employed to explore the correlation between each independent variable and patients’ bypass behavior. Stata 15.0 was used for data analysis, with 0.05 as the level of significance. Variance inflation factor (VIF) was used to evaluate the multicollinearity. An independent variable would be removed until all the VIF values dropped under 10.
Using respectively the PCAT-C total score and scores of six dimensions as main independent variables, two kinds of models were established. To assess the robustness of the results, patient experience, and socio-demographic variables were included first, then medical policy and health-care supplier factors in the sequence. Finally, we developed four models. The results of all models were consistent, indicating the relative robustness of the final model.
Results
Descriptive Analysis
Of the 1060 questionnaires distributed, 928 eventually passed the screening process. Among the 132 excluded questionnaires, 82 were incomplete, 42 were not common sense, and eight were damaged in the data file. Descriptive statistics were performed and the main results were as follows: Among the participants, 58.80% were women, 66.70% were married, and 67.60% were from cities. Age ranged from 18 to 87, with an average of 40. Respondents had a degree of university or above account for 35.70%, and most were employed (50.70%). In addition, almost all (97.1%) participated the national basic medical insurance, but only 32.6% had commercial medical insurance. Bypass rate was 11.10%. The total mean score of patient experience was 73.89 (SD = 9.78). As for each dimension, the comprehensive got the highest score of 79.30 (SD = 15.77), followed by family-centered 78.19 (SD = 16.45), continuity 76.75 (SD = 10.30), and coordination 71.35 (SD = 16.94). The last two dimensions were first contact and community orientation, with only 71.26 (SD = 10.13) and 60.87 (SD = 16.97) respectively. For full details see Table 1.
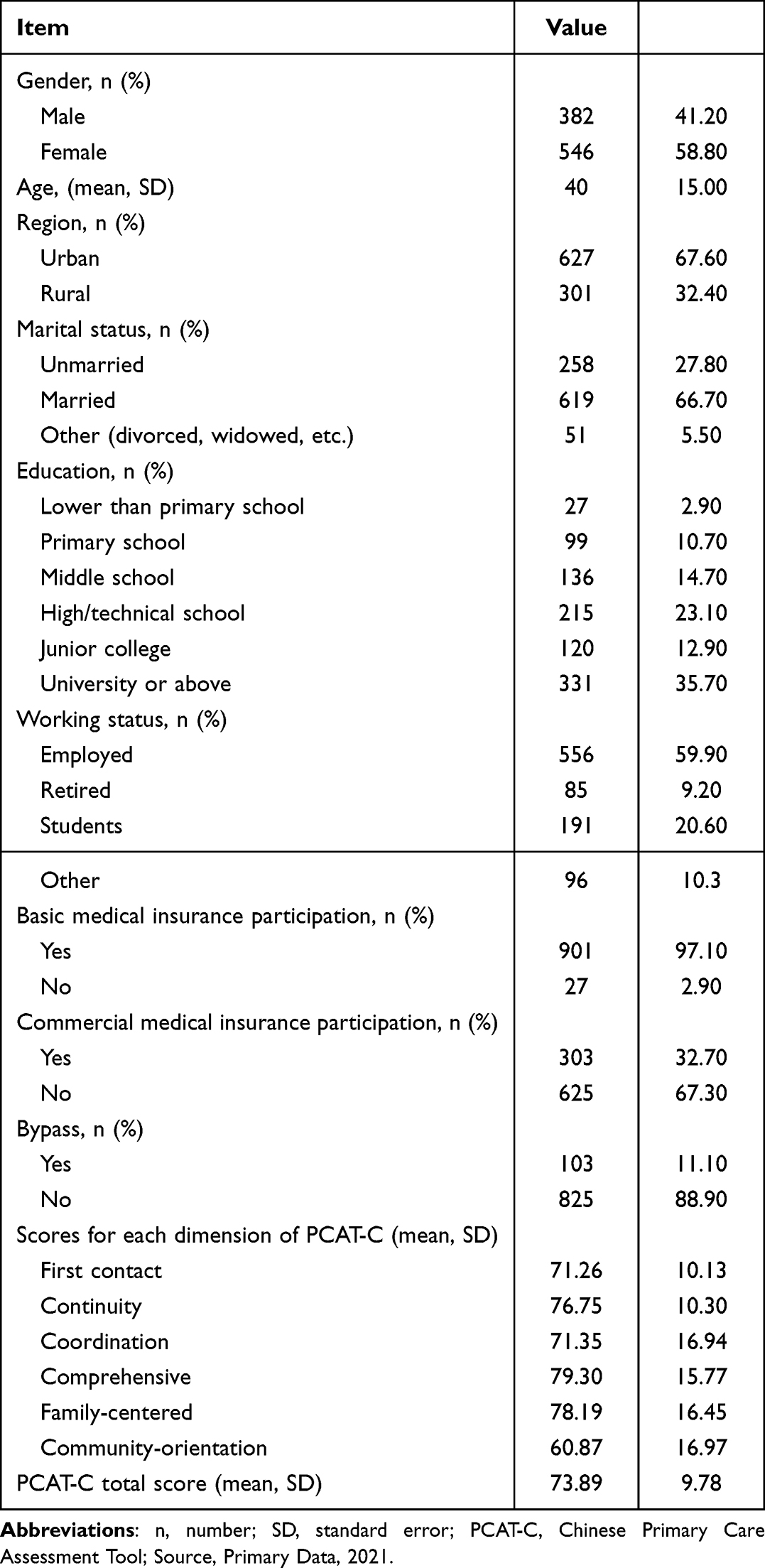 |
Table 1 Sociodemographic Profile and Descriptive Statistics of the Participants (N = 928) |
Regression Analysis
Results of the regression were presented as follows. For the two models using total PCAT-C scores, R2 were 0.0511 and 0.0674 (Table 2). For the two models using scores of six dimensions, R2 were 0.0746 and 0.0933 (Table 3). Apparently, models with more control variables showed a better explanation of the dependent variable. No independent variables were removed for suspected multicollinearity, and the regression results were relative stable among different models. The following interpretation will on the basis of model 2 and model 4.
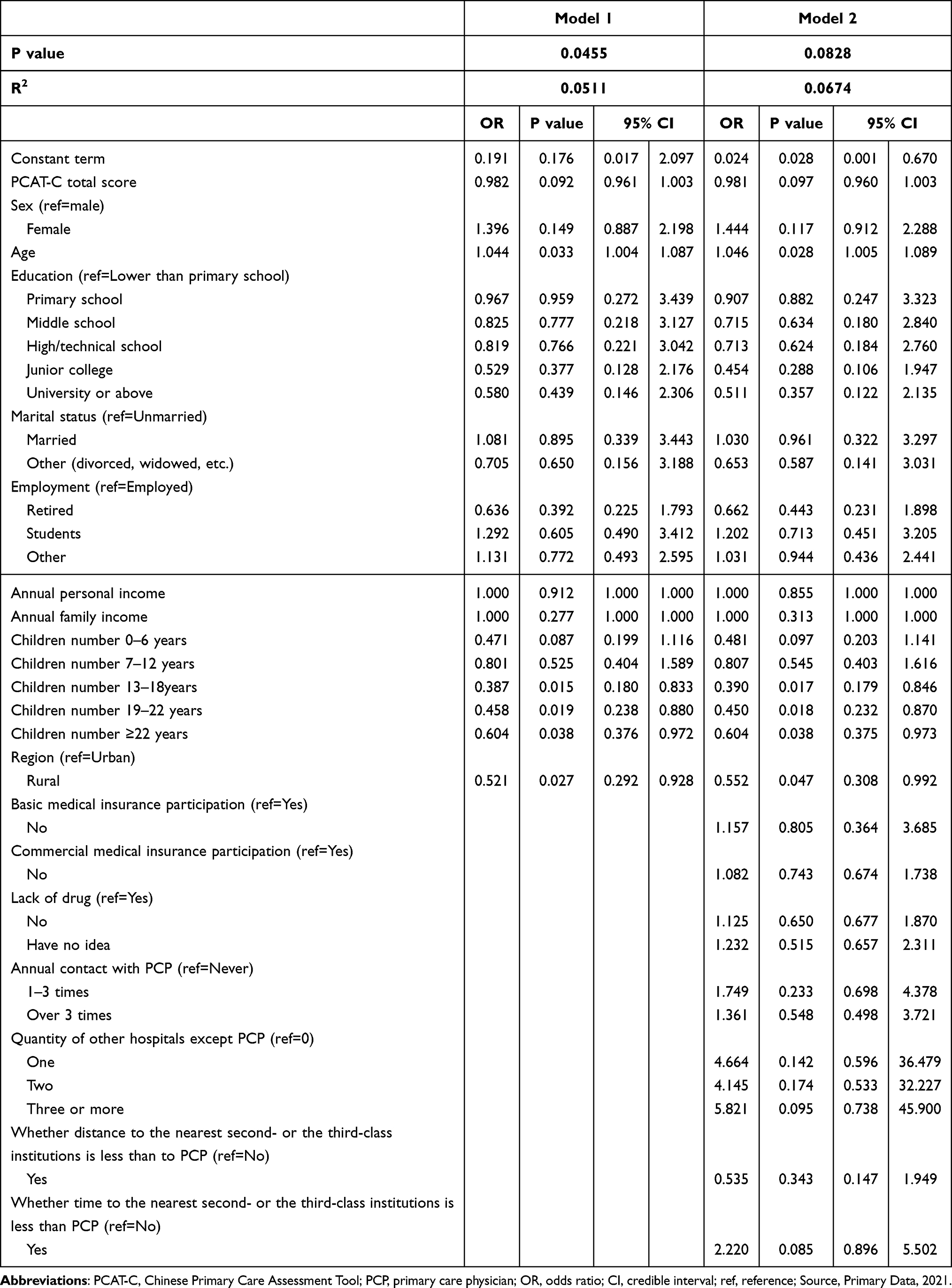 |
Table 2 Regression Analysis of Factors Associated with Patients’ Bypass Behavior (Total PCAT-C Score, N = 928) |
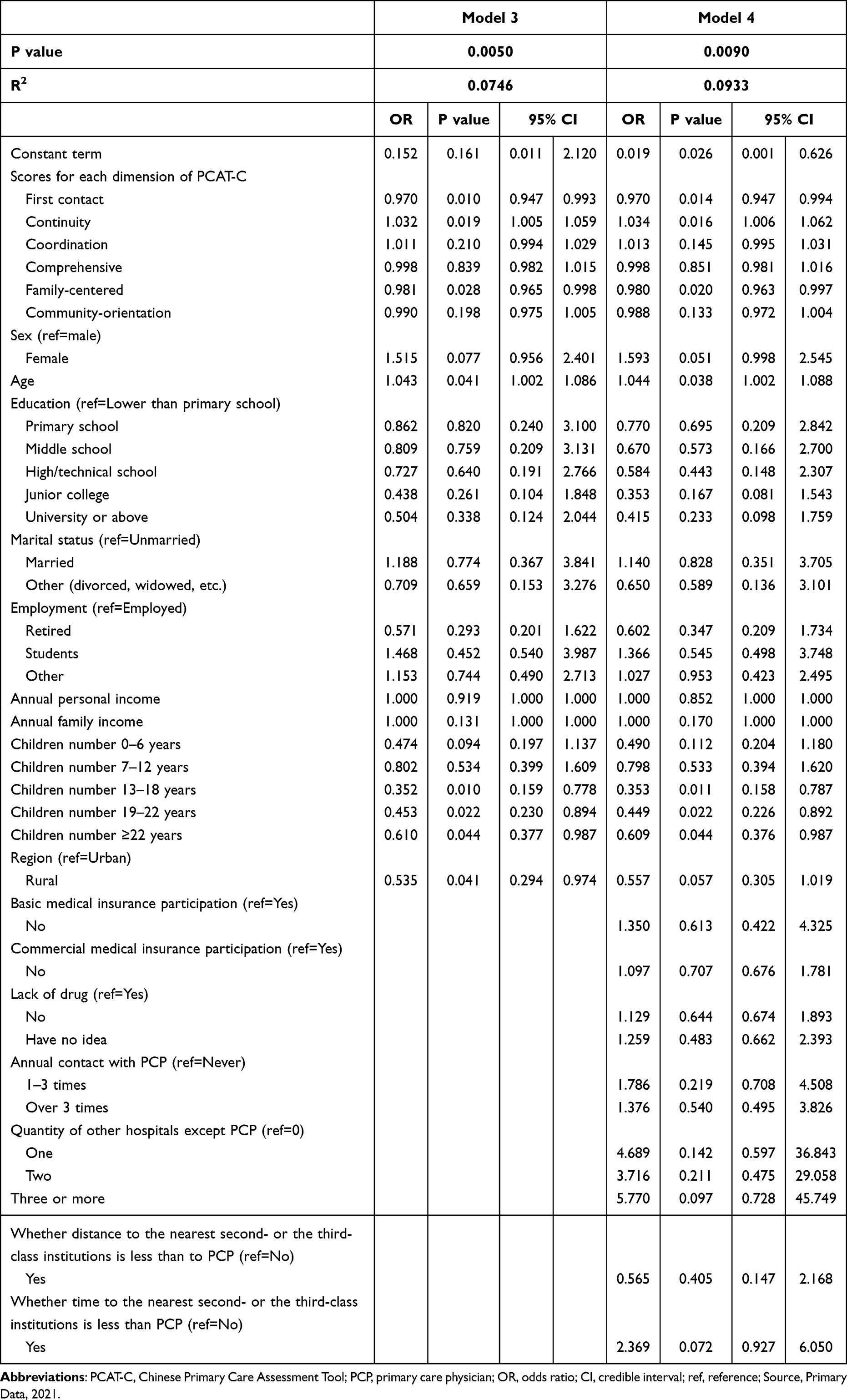 |
Table 3 Regression Analysis of Factors Associated with Patients’ Bypass Behavior (Scores of Six Dimensions, N = 928) |
Patient Experience
Under the significance level of 0.10, PCAT-C total score was negatively correlated with the probability of bypassing (OR 0.981 [95% CI 0.960 to 1.003, P = 0097]), as found in model 2, Table 2.
As shown in model 4, Table 3, patients with high scores in first contact (OR 0.970 [95% CI 0.947 to 0.994], P = 0.014), and family-centered (OR 0.980 [95% CI 0.963 to 0.997], P = 0.020) had lower probability to bypass their PCPs. But those with higher scores in the dimension of continuity (OR 1.034 [95% CI 1.006 to 1.062], P = 0.016) were more likely to practice bypass.
Other Factors
There were also some other factors significantly associated with patients’ bypass behavior:
According to model 2, older patients had a higher probability to bypass (1.046, [95% CI 1.005–1.089], P = 0.028). Compared to urban, rural patients were less likely to bypass (0.552, [95% CI 0.308–0.992], P = 0.047). Besides, for patients with children between 13–18, 19–22 and over 22 years old, increase in the quantity of children will significantly lower the odds ratio to practice bypass (0.390, [95% CI 0.179–0.846], P = 0.017), (0.450, [95% CI 0.232–0.870], P = 0.018), and (0.604, [95% CI 0.375–0.973], P = 0.038) respectively.
For model 4, similarly, older patients were more likely to bypass (1.044, [95% CI 1.002–1.088], P = 0.038). The quantity increase of children aged 13–18 (0.353, [95% CI 0.158–0.787], P = 0.011), 19–22 (0.449, [95% CI 0.226–0.892], P = 0.022), and over 22 years old (0.609, [95% CI 0.376–0.987], P = 0.044) were associated with a lower probability of bypassing.
Discussion
The results supported our hypothesis: In China, patients’ better experience in primary care facilities could reduce their probability of bypassing. In the following, we will first discuss the influence mechanism of the outcome and give practical suggestions. Then, the methodological contribution to the studying area. And last, the existing limitations and avenues for future research.
Influence Mechanism and Practical Suggestions
Our results showed that the higher the patient’s rating of continuity, the greater the likelihood of bypassing. It contrasts to the conclusions of most previous studies that “good continuity significantly increases patient satisfaction”,45–48 and proves that other factors might affect patients’ bypass behavior.
The schematic diagram of influence mechanism is shown in Figure 1. According to “structure-process-outcome” framework, the process quality of medical services comprises two parts: interpersonal quality and technical quality. In this study, patient experience measured by PCAT-C only reflected the former. In the marketing literature, similarly, an essential way to ‘own’ a consumer is to build a high-trust relationship with him/her, which also consists of two aspects: affective trust and cognitive trust.49
 |
Figure 1 Schematic diagram of influence mechanism. |
Affective trust is the confidence in a provider on the basis of feelings generated by the level of care and concern they demonstrate. It is characterized by feelings of security and perceived strength of the relationship.50 A high rating of the continuity means PCPs’ patience and full understanding of their patients’ condition, treatment plans or even treatment burden. All of these increased patients’ sense of security and promoted a firm interpersonal relationship with their PCPs, thus enhanced their affective trust. On the other hand, cognitive trust is a willingness to rely on a service provider based on specific instances of reliable conduct,50 which reflects their competence and reliability. In China, However, the low proportion of qualified PCPs51 and inadequate equipment and supplies at PHCs52,53 made it difficult to guarantee the technical quality of primary care. This directly undermined their ability in diseases diagnosis and treatment, which led to a decrease in patients’ cognitive trust in their PCPs. Therefore, patients’ good experience in continuity only represents the high-level in the quality of interpersonal interactions out of patients’ affective trust in their PCPs. Nevertheless, existed technical quality deficiency and brought low cognitive trust will ultimately lead them direct to large hospitals. In addition, their ambiguous attitude towards “Would you like to see another doctor in a different place if possible?” also confirmed that their loyalty to their PCPs is not high.
In summary, improvement in continuity dimension alone has been far from enough to discourage patients’ bypassing of PHCs in China. We need to enhance both the quality of interpersonal care and technology simultaneously. For the former, we can refer the continuity dimension to promote regular contact between patients and the same physician, encourage physicians to fully communicate with their patients, to follow up for a better understand about their patients’ overall health status. For the latter, first, local public sectors should continue to provide financial and strategic support to eliminate physical and human capital constraints faced by PHCs. Second and most critically, PCPs should continuously equip themselves with advanced medical knowledge through various channels to improve their capacity. Besides, we should also encourage more construction of qualified and accredited third-party testing facilities with advanced equipment to address the low level of PHCs testing and waste of resources caused by repeat testing.54 In addition, based on their own characteristics, PHCs can provide featured programs such as Chinese medicine services, self-funded physical examination programs and high-quality dental services, which can help to enhance their service capacity, improve their market competitiveness and win patients’ loyalty at the same time.55
Residents with higher scores in first contact dimension had a lower probability of bypassing primary care facilities. This can be explained by Skinner’s positive reinforcement theory:56 Reinforcement means increasing the response rate of a behavior. Any stimulus or events that could increase the response probability could be a reinforcer.
In this study, “convenient and timely access to PHCs when new medical needs arise” acted as the reinforcer. It helps people realize the advantages of primary care in treating non-critical conditions in terms of low cost, high geographic accessibility, and short waiting time, which improved patients’ perceived benefits of primary care,3,57–59 and increased the frequency of the responsive behavior (ie, reduced bypass probability in their subsequent choice of care).
First contact is the core dimension that the other patient experience dimensions depend on. Continuity, coordination, and comprehensive service provision can take place successfully only when primary care is accessible and available. Improved primary care therefore requires an expanded role of PCPs as the first contact of care: First, continuing to encourage residents to seek care at PHCs.45,60 Previous studies had demonstrated its positive effects on increasing the utilization of primary care among residents. Second, encouraging residents to sign up with family physicians and making them become their usual source of care (USC). The importance of having a USC in accessing health-care services has been well documented.3 Furthermore, people who contracted family doctors of PHCs were more likely to own a USC.61–63 In addition, strengthening chronic diseases management at the primary level.64 Finally, increasing publicity to improve patient awareness of primary care function. Bypass behavior may reveal that patients were unaware of the services scope provided in the township institutions.65 Therefore, public sectors should make more efforts on propaganda by means of billboards and mass media, which is of great significance for patients to understand the role of different tired medical institutions and to choose an appropriate facility whenever they need.
In terms of control variables, age was positively associated with PHCs’ bypassing, which is consistent with existing evidence.9–11 It can be interpreted that elders are more health-conscious, they are more experienced in health-seeking and capable of self-diagnosing for common diseases. Thus, when a doctor visit was required, they were more likely in severe condition, which increased their likelihood to bypass primary care.17,23 In addition, the tendency to bypass was significantly higher in urban areas, where the upper-level facilities are easily accessible22 and people are more capable in paying medical expenses.10 Effect of the quantity of children aged 13 years or older on bypassing was also significant. The more children in the family, the more stressful to raise them, so inexpensive and convenient PHCs are more likely to become their first choice.
Methodological Contribution
This study represents the first attempt in China to systematically assess the correlation between patient experience in PHCs and their bypass behavior.
In China, patients’ unwillingness to get treated at PHCs was widely adopted as the surrogate indicator of bypass. This assumption may be inappropriate: studies had proved that although they were willing to seek care at PHCs, bypassing still happened due to their long-standing wrong notion and bad habits of directly going to big hospitals, or their tendencies to avoid risks.66,67 Therefore, we chose patients’ actual healthcare visiting for identification, which can better represent the real bypass situation in China. In the absence of an agreed measurement tool, we adapted the questionnaire used in a Japanese study, and further excluded those who bypass due to unclear of PHC’s service scope, making our bypass rates more accurate.
In assessing patients’ perception of healthcare quality, patient satisfaction played a key role in previous literature.46,68,69 Despite these, it is subjective and often non-specific. In contrast, patient experience reflected patient’s actual experience, not only avoided value judgments and effects of existing expectations, but also had been recognized as one of the three pillars of healthcare quality, and increasingly used to assess the quality of primary and higher-level care performance.70 That is why we chose it as our key independent variable. Meanwhile, PCAT-C, applying for the measurement of patient experience, had been strictly adapted and used in patient surveys across several Chinese cities, verifying its good reliability and validity.44,63,71–73
In summary, differing from the deficiency and inaccuracy among variables in previous literature, this study screened variables strictly, combined with mature instruments, and collected data from 928 residents across 31 provinces in China. All of these made our results comprehensively represent the current patients’ bypass situation as well as their perceived quality of primary care, and further provided sound support for the subsequent analysis and conclusion.
Limitations and Avenues for Future Research
This study has several limitations. First, there is not an agreed tool worldwide for our “bypass” definition, ie, “patients going directly to a higher-level facility without referral from their PCPs”. Therefore, the reliability of our self-designed questionnaire needs further validation. Besides, for lack of a clear scope of non-critical diseases in China, this study did not trace the specific illnesses type patients suffered when identifying bypass, which should be taken into consideration in future studies.
Second, PCAT-C focused on interpersonal quality of healthcare, but it cannot well reflect the technical quality of PCPs. Further studies should be conducted to verify whether low technical quality could explain the paradoxical effect of primary care continuity.
Third, our sampling was conducted from July to August 2021, and only convenience sampling was adopted. These may bring us sampling errors. Fortunately, descriptive statistics results indicated that the above concerns had no serious effects. In the future, if possible, sampling at different periods of the year and stratified sampling strategy could be considered to enhance the representation of the sample.
Last, as many variables were obtained by assessing respondents’ previous experiences, it may lead us the false results due to recall bias. To minimize these, future studies could ask them to answer based on the latest visiting experience.
Conclusion
Our findings highlighted the effect of enhanced patient experience at PHCs on their reduced bypass behavior. The prevalent irrational health-seeking behavior could be attributed to the underperformance of first contact and continuity of services provided by PHCs, which may help policymakers develop strategies to mitigate bypass.
To improve primary care utilization and accessibility, continue efforts should be put to strengthen the role of PHCs as the first-contact for patients’ common diseases, to encourage residents to contract with family physicians, and to educate and propaganda in avoiding bypass caused by unawareness of PHC’s service scope. Moreover, the positive correlation between bypass and continuity scores suggested that more attention should be paid to strengthening the technical quality of primary care physicians as well as the establishment of a long-term relationship with a usual primary care physician.74
Ethical Approval
Questionnaire used in this study was examined and approved by the Ethics Committee of China Pharmaceutical University. We declare that our study complies with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. Chen H, Chi I, RJJoa L, et al. Hospital utilization among Chinese older adults: patterns and predictors. J Aging Health. 2019;31(8):1454–1478. doi:10.1177/0898264318780546
2. Chen ZJTL. Launch of the health-care reform plan in China. Lancet. 2009;373(9672):1322–1324. doi:10.1016/S0140-6736(09)60753-4
3. Feng D, Zhang D, Li B, et al. Does having a usual primary care provider reduce patient self-referrals in rural China’s rural multi-tiered medical system? A retrospective study in Qianjiang District, China. BMC Health Serv Res. 2017;17(1):778. doi:10.1186/s12913-017-2673-6
4. Liu Y, Zhong L, Yuan S, et al. Why patients prefer high-level healthcare facilities: a qualitative study using focus groups in rural and urban China. BMJ Global Health. 2018;3(5):e000854. doi:10.1136/bmjgh-2018-000854
5. Tsai JC-H, Chen W-Y, Liang Y-W. Nonemergent emergency department visits under the National Health Insurance in Taiwan. Health Policy. 2011;100(2–3):189–195. doi:10.1016/j.healthpol.2010.10.007
6. Chen K-Y, Yang C-M, Lien C-H, et al. Burnout, job satisfaction, and medical malpractice among physicians. Int J Med Sci. 2013;10(11):1471–1478. doi:10.7150/ijms.6743
7. Gotsadze G, Bennett S, Ranson K, et al. Health care-seeking behaviour and out-of-pocket payments in Tbilisi, Georgia. Health Policy Plan. 2005;20(4):232–242. doi:10.1093/heapol/czi029
8. Pollack CE, Rastegar A, Keating NL, et al. Is self‐referral associated with higher quality care? Health Serv Res. 2015;50(5):1472–1490. doi:10.1111/1475-6773.12289
9. Yao J, Agadjanian VJ. Bypassing health facilities in rural Mozambique: spatial, institutional, and individual determinants. BMC Health Serv Res. 2018;18(1):1–11. doi:10.1186/s12913-018-3834-y
10. Sanders SR, Erickson LD, Call VR, et al. Rural health care bypass behavior: how community and spatial characteristics affect primary health care selection. J Rural Health. 2015;31(2):146–156. doi:10.1111/jrh.12093
11. Shah R. Bypassing birthing centres for child birth: a community-based study in rural Chitwan Nepal. BMC Health Serv Res. 2016;16(1):1–8. doi:10.1186/s12913-016-1848-x
12. Akin JS, Hutchinson P. Planning. Health-care facility choice and the phenomenon of bypassing. Health Policy Plan. 1999;14(2):135–151. doi:10.1093/heapol/14.2.135
13. Rao KD, Sheffel A. Quality of clinical care and bypassing of primary health centers in India. Soc Sci Med. 2018;207:80–88. doi:10.1016/j.socscimed.2018.04.040
14. Panezai S, Saqib SE, Ahmad M. Gender differences in client satisfaction and its relationship with utilization of primary health care services in Pakistan. J Geograp Soc Sci. 2019;1(1):30–43.
15. Panezai S, Ahmad MM, Saqib SE, et al. A gender-based assessment of utilization of primary health care services and associated factors in Pakistan. Ponte J. 2020;76(1/1). doi:10.21506/j.ponte.2020.1.7
16. Damrongplasit K, Wangdi T. Healthcare utilization, bypass, and multiple visits: the case of Bhutan. Int J Health Econ Manag. 2017;17(1):51–81. doi:10.1007/s10754-016-9194-4
17. Liu JJ, Bellamy G, Barnet B, et al. Bypass of local primary care in rural counties: effect of patient and community characteristics. Ann Fam Med. 2008;6(2):124–130. doi:10.1370/afm.794
18. Fletcher A, Samson R, McLeod K. Are patients bypassing paediatric cardiology outreach clinics? Cardiol Young. 2017;27(5):1014–1017. doi:10.1017/S1047951116002973
19. Tai WTC, Porell FW, Adams EK. Hospital choice of rural Medicare beneficiaries: patient, hospital attributes, and the patient–physician relationship. Health Serv Res. 2004;39(6p1):1903–1922. doi:10.1111/j.1475-6773.2004.00324.x
20. Escarce JJ, Kapur K. Do patients bypass rural hospitals?: determinants of inpatient hospital choice in rural California. J Health Care Poor Underserved. 2009;20(3):625–644. doi:10.1353/hpu.0.0178
21. Leonard KL, Mliga GR, Haile Mariam D. Bypassing health centres in Tanzania: revealed preferences for quality. J Afr Econ. 2002;11(4):441–471. doi:10.1093/jae/11.4.441
22. Varkevisser M, van der Geest SA. Why do patients bypass the nearest hospital? An empirical analysis for orthopaedic care and neurosurgery in the Netherlands. Eur J Health Econ. 2007;8(3):287–295. doi:10.1007/s10198-006-0035-0
23. Liu J, Bellamy GR, McCormick M. Patient bypass behavior and critical access hospitals: implications for patient retention. J Rural Health. 2007;23(1):17–24. doi:10.1111/j.1748-0361.2006.00063.x
24. Paul BK, Rumsey DJ. Primary care providers bypassing in rural Kansas. Trans Kans Acad Sci. 2002;105(1):79–90. doi:10.2307/3627974
25. Sanders SR, Erickson LD, Call VR, et al. Middle-aged and older adult health care selection: health care bypass behavior in rural communities in Montana. J Appl Gerontol. 2017;36(4):441–461. doi:10.1177/0733464815602108
26. Gauthier B, Wane W. Bypassing health providers: the quest for better price and quality of health care in Chad. Soc Sci Med. 2011;73(4):540–549. doi:10.1016/j.socscimed.2011.06.008
27. Roh CY, Moon MJ. Nearby, but not wanted? The bypassing of rural hospitals and policy implications for rural health care systems. Policy Stud J. 2005;33(3):377–394. doi:10.1111/j.1541-0072.2005.00121.x
28. Rasoulynejad AS. Study of self-referral factors in the three-level healthcare delivery system, Kashan, Iran, 2000. Rural Remote Health. 2004;4(4):1–11. doi:10.22605/RRH237
29. Xu JM, Wang YF. Analysis of urban residents’ willingness and influencing factors to seek first contact in community health organizations in Huai’an City. J Mod Prev Med. 2020;47(22):4110–4113+4136.
30. Abere TM, Atnafu DD, Mulu Y. Self-referral and associated factors among patients attending adult outpatient departments in Debre tabor general hospital, North West Ethiopia. BMC Health Serv Res. 2021;21(1). doi:10.1186/s12913-021-06642-7
31. Wang SY, Zhang R, Liu L, et al. Study on the willingness and influencing factors of the community first consultation of residents in Panjin City. J Commun Med. 2021;19(10):4. doi:10.19790/j.cnki.JCM.2021.10.04
32. Xu JM. Investigation on willingness of first-visit at grassroots medical institution among residents in a community of Huai’an City under the background of hierarchical medical care. J Med Soc. 2021;34(9):5. doi:10.13723/j.yxysh.2021.09.014
33. Li C, Chen Z, Khan MM. Bypassing primary care facilities: health-seeking behavior of middle age and older adults in China. BMC Health Serv Res. 2021;21(1):1–12. doi:10.1186/s12913-021-06908-0
34. Browne K, Roseman D, Shaller D, et al. Analysis & commentary measuring patient experience as a strategy for improving primary care. Health Aff. 2010;29(5):921–925. doi:10.1377/hlthaff.2010.0238
35. Brousseau DC, Bergholte J, Gorelick MH. The effect of prior interactions with a primary care provider on nonurgent pediatric emergency department use. Arch Pediatr Adolesc Med. 2004;158(1):78–82. doi:10.1001/archpedi.158.1.78
36. Pillay I, Mahomed OH. Prevalence and determinants of self referrals to a District-Regional Hospital in KwaZulu Natal, South Africa: a cross sectional study. Pan Afr Med J. 2019;33. doi:10.11604/pamj.2019.33.4.16963
37. Kulu-Glasgow I, Delnoij D, de Bakker D. Self-referral in a gatekeeping system: patients’ reasons for skipping the general-practitioner. Health Policy. 1998;45(3):221–238. doi:10.1016/s0168-8510(98)00045-1
38. Aoki T, Yamamoto Y, Ikenoue T, et al. Effect of patient experience on bypassing a primary care gatekeeper: a multicenter prospective cohort study in Japan. J Gen Intern Med. 2018:722–728. doi:10.1007/s11606-017-4245-1
39. Chen MT, Mei WH. Development status of the gate-keeper system and it’s influencing factors of residents’ gate-keeper in China. J Med Soc. 2016;29(4):3. doi:10.13723/j.yxysh.2016.04.008
40. Song R, Shen Y, Yu MJ, et al. Analysis of first visit status of “1+1+1” contracted residents and related factors in Ruijinerlu Community of Shanghai. J Shanghai Med. 2021;42(6):5. doi:10.3969/j.issn.1006-1533.2021.06.005
41. Forrest CB, Weiner JP, Fowles J, et al. Self-referral in point-of-service health plans. JAMA. 2001;285(17):2223–2231. doi:10.1001/jama.285.17.2223
42. Bezu S, Binyaruka P, Mstad O, et al. Pay-for-performance reduces bypassing of health facilities: evidence from Tanzania. Soc Sci Med. 2021:268. doi:10.1016/j.socscimed.2020.113551
43. Fu XL, Chen D, Shi SH, et al. The selection of the first medical institution and its influencing factors, Henan. J Modern Prev Med. 2021;48(9):5.
44. Yang H, Shi L, Lebrun LA, et al. Development of the Chinese primary care assessment tool: data quality and measurement properties. Int J Qual Health Care. 2013;25(1):92–105. doi:10.1093/intqhc/mzs072
45. Rocha KB, Rodríguez-Sanz M, Pasarín MI, et al. Assessment of primary care in health surveys: a population perspective. Eur J Public Health. 2012;22(1):14–19. doi:10.1093/eurpub/ckr014
46. Sans-Corrales M, Pujol-Ribera E, Gene-Badia J, et al. Family medicine attributes related to satisfaction, health and costs. Fam Pract. 2006;23(3):308–316. doi:10.1093/fampra/cmi112
47. Fan VS, Burman M, McDonell MB, et al. Continuity of care and other determinants of patient satisfaction with primary care. J Gen Intern Med. 2005;20(3):226–233. doi:10.1111/j.1525-1497.2005.40135.x
48. Cabana MD, Jee SH. Does continuity of care improve patient outcomes. J Fam Pract. 2004;53(12):974–980. doi:10.1093/fampra/cmh613
49. Johnson D, Grayson K. Cognitive and affective trust in service relationships. J Bus Res. 2005;58(4):500–507. doi:10.1016/S0148-2963(03)00140-1
50. Edell JA, Burke MC. The power of feelings in understanding advertising effects. J Consum Res. 1987;14(3):421–433. doi:10.1086/209124
51. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395(10239):1802–1812. doi:10.1016/S0140-6736(20)30122-7
52. Zhao SC, Tong XY, Zhang AQ, et al. Study on the influence of patients’ trust mode and level on the willingness of primary first visit. J Chin Health Policy. 2021;14(8):5. doi:10.3969/j.issn.1674-2982.2021.08.003
53. Yu XQ, Zhou SW, Huang X, et al. Satisfactory degree of the community residents in Zhongshan on community health services and its influencing factors. J Chin Primary Health Care. 2014;28(001):41–43. doi:10.3969/j.issn.1001-568X.2014.01.0014
54. Wang J. Quality Evaluation of Community Health Service Based on Patients’ Experience in One District in Changchun. MD: Jilin University; 2018.
55. Ali A, Panezai SJS, Publishing A. Assessing the quality of primary health care services at basic health units in Quetta City, Balochistan, Pakistan. Public Health Res. 2021;11:111–112.
56. Zhang L. The Application of Skinner’s Reinforcement Theory in Senior High School History Teaching. MD: Chongqing Normal University; 2016.
57. Damiano PC, Momany ET, Tyler MC, et al. Cost of outpatient medical care for children and youth with special health care needs: investigating the impact of the medical home. Pediatrics. 2006;118(4):e1187–e1194. doi:10.1542/peds.2005-3018
58. Starfield B, Shi L. The medical home, access to care, and insurance: a review of evidence. Pediatrics. 2004;113(5 Suppl):1493–1498. doi:10.1542/peds.113.5.1469
59. Smith PJ, Santoli JM, Chu SY, et al. The association between having a medical home and vaccination coverage among children eligible for the vaccines for children program. Pediatrics. 2005;116(1):130–139. doi:10.1542/peds.2004-1058
60. Wei X, Li H, Yang N, et al. Comparing quality of public primary care between Hong Kong and Shanghai using validated patient assessment tools. PLoS One. 2015;10(3):e0121269. doi:10.1371/journal.pone.0121269
61. Tsai J, Shi L, Yu WL, et al. Usual source of care and the quality of medical care experiences: a cross-sectional survey of patients from a Taiwanese community. Med Care. 2010;48(7):628–634. doi:10.1111/j.1475-6773.2004.00324.x
62. Xu KT. Usual source of care in preventive service use: a regular doctor versus a regular site. Health Serv Res. 2002;37(6):1509–1529. doi:10.1111/1475-6773.10524
63. Kuang L, Liang Y, Mei J, et al. Family practice and the quality of primary care: a study of Chinese patients in Guangdong Province. Fam Pract. 2015;32(5):557–563. doi:10.1093/fampra/cmv064
64. Liang -L-L, Huang N, Shen Y-J, et al. Do patients bypass primary care for common health problems under a free-access system? Experience of Taiwan. BMC Health Serv Res. 2020;20(1):1–10. doi:10.1186/s12913-020-05908-w
65. Panezaia S, Ahmadb MM, Saqibc SJ. Exploring the reasons for underutilization of primary health care services in Pakistan: a qualitative analysis. PONTE Int J Sci Res. 2020;76(12/1). doi:10.21506/j.ponte.2020.12.19
66. Zhao L, Wang XW, Kong XJ, et al. Analysis of the influence factors on the first visit willingness of primary hospital of patients in tertiary hospital based on theory of planned behavior. J Chin Hospital Manag. 2021;41(4):5.
67. Gao Y. A Study on the Influencing Factors of Residents’ Choice of Medical Institutions and the Gap Between Willingness and Behavior in Hierarchic Care. MD: East China Normal University; 2020.
68. Guo Y, Kuroki T, Yamashiro S, et al. Illness behaviour and patient satisfaction as correlates of self-referral in Japan. Fam Pract. 2002;19(4):326–332. doi:10.1093/fampra/19.4.326
69. Paddison CA, Abel GA, Roland MO, et al. Drivers of overall satisfaction with primary care: evidence from the English General Practice Patient Survey. Health Expect. 2015;18(5):1081–1092. doi:10.1111/hex.12081
70. Ren Y, Zhang T, Thomas S, et al. An investigation of patients′ experience on using community health services in Beijing. J Chin Gen Pract. 2007;10(21):4. doi:10.3969/j.issn.1007-9572.2007.21.003
71. Wang W, Haggerty J. Development of primary care assessment tool–adult version in Tibet: implication for low-and middle-income countries. Prim Health Care Res Dev. 2019;20. doi:10.1017/S1463423619000239
72. Li H, Wei X, Wong MC-S, et al. A cross-sectional comparison of perceived quality of primary care by hypertensive patients in Shanghai and Shenzhen, China. Medicine. 2015;94(34). doi:10.1097/MD.0000000000001388
73. Shi J, Jin H, Shi L, et al. The quality of primary care in community health centers: comparison among urban, suburban and rural users in Shanghai, China. BMC Fam Pract. 2020;21(1):1–10. doi:10.21203/rs.3.rs-28943/v2
74. Duckett J, Hunt K, Munro N, et al. Does distrust in providers affect health-care utilization in China? Health Policy Plan. 2016;31(8):1001–1009. doi:10.1093/heapol/czw024
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.