Back to Journals » Drug, Healthcare and Patient Safety » Volume 18
Capecitabine Dosage as an Independent Prognostic Factor for the Development of Hand-Foot Syndrome: A Competing Risk Analysis
Authors Chantharakhit C ![]() , Patumanond J
, Patumanond J ![]() , Phinyo P
, Phinyo P ![]() , Chai-Adisaksopha C
, Chai-Adisaksopha C
Received 13 September 2025
Accepted for publication 28 January 2026
Published 4 February 2026 Volume 2026:18 567407
DOI https://doi.org/10.2147/DHPS.S567407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Siew Siang Chua
Chaichana Chantharakhit,1,2 Jayanton Patumanond,3 Phichayut Phinyo,2,4 Chatree Chai-Adisaksopha5
1Division of Medical Oncology, Department of Internal Medicine, Buddhasothorn Hospital, Chachoengsao, Thailand; 2Department of Biomedical Informatics and Clinical Epidemiology (BioCE), Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 3Clinical Epidemiology and Clinical Statistics Unit, Faculty of Medicine, Naresuan University, Phitsanulok, Thailand; 4Center for Clinical Epidemiology and Clinical Statistics, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 5Division of Hematology, Department of Internal Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Correspondence: Chaichana Chantharakhit, Division of Medical Oncology, Department of Internal Medicine, Buddhasothorn Hospital, Chachoengsao, Thailand, Email [email protected]
Purpose: Capecitabine, an oral prodrug of 5-fluorouracil, commonly causes hand-foot syndrome (HFS). Although clinical predictors of HFS have been reported, causal evidence supporting dosage as an independent prognostic factor remains limited. Because competing events may preclude HFS, this study evaluated the prognostic role of capecitabine dosage in grade 2– 3 HFS using a competing risk analysis.
Patients and Methods: A retrospective observational cohort study was conducted. Capecitabine dosage was the exposure of interest. Potential confounders including sex, combination chemotherapy, and estimated glomerular filtration rate (eGFR) were identified using a directed acyclic graph. The primary endpoint was time from treatment initiation to grade 2– 3 HFS. A multivariable competing risk analysis was performed using the Lambert model, with loss to follow-up, severe diarrhea, sepsis, and death defined as competing events. Capecitabine dosage was categorized (2000– 4000 mg/day) to facilitate clinical interpretability.
Results: Among 596 patients, 132 (22.2%) developed grade 2– 3 HFS, with a median onset time of 63 days (interquartile range, 42– 84). Higher capecitabine dosage was independently associated with an increased risk of HFS, with the greatest effect observed at 4000 mg/day compared with 2000 mg/day (aHR 4.41; 95% CI, 1.31– 14.81; p = 0.016), demonstrating a clear dose-dependent increase in risk. In addition, higher dosage was associated with a shorter model-predicted median time to HFS onset.
Conclusion: This study confirms capecitabine dosage as an independent prognostic factor for grade 2– 3 HFS, with significantly increased risk at 4000 mg/day and a shorter median time to HFS onset as dosage increases. These findings underscore the importance of careful dosing and support the implementation of evidence-based strategies for dose adjustment in high-risk patients.
Keywords: capecitabine dosage, hand-foot syndrome, prognostic factor, competing risk analysis
Introduction
Capecitabine, an oral prodrug widely used in cancer chemotherapy, is converted to 5-fluorouracil (5-FU) in the liver and tumor tissues.1–3 Most 5-FU is rapidly inactivated, while only a small fraction (1–5%) forms active metabolites that inhibit thymidylate synthase and disrupt DNA/RNA synthesis.4 Hand–foot syndrome (HFS) is a common toxicity associated with capecitabine, characterized by erythema, pain, swelling, and blistering of the palms and soles, which can lead to functional impairment, reduced quality of life, and frequently necessitates dose reduction, treatment interruption, or discontinuation. It results from 5-FU induced skin damage, with high eccrine gland density in the palms and soles promoting local drug accumulation and HFS development.5,6
Grade ≥2 HFS occurs in 21–27% of patients receiving capecitabine.7,8 Reported risk factors include older age, female sex, high body surface area, low albumin, ethnicity, prolonged treatment, renin–angiotensin system inhibitor use, elevated folate, and higher dosage.7–10 HFS imposes a significant burden by impairing quality of life and often necessitates treatment interruption, dose adjustment, or discontinuation.11 Early identification of high-risk patients may allow timely intervention, maintain quality of life, and support continued therapy.
Although prior studies have identified higher capecitabine dosage as a risk factor for HFS, the evidence on dose levels remains inconsistent. Most previous research has been exploratory rather than explanatory, leaving the causal effect unclear.7,8,10 This study aimed to evaluate the effect of increasing capecitabine dosage on the risk of developing grade 2–3 HFS, expressed as hazard ratios, and to assess its impact on time to onset using model-predicted median times. Because patients may experience competing clinical events before developing HFS, a competing risk analysis was applied to obtain unbiased estimates of HFS risk and time to event outcomes.
Materials and Methods
Study Design
This prognostic factor study employed a retrospective observational cohort design conducted at a single referral hospital in Thailand. Data were extracted from electronic medical records between January 2018 and December 2024. The study protocol was approved by the Institutional Review Board and Ethics Committee (BSH-IRB 002/2568) and registered with the Thai Clinical Trials Registry (TCTR20250419006).
Study Population
The study population comprised consecutive adult cancer patients aged 18 years or older who received capecitabine-based chemotherapy at a single referral hospital in Thailand during the study period. Inclusion criteria were adult cancer patients who received capecitabine-based chemotherapy. Exclusion criteria included patients with missing data on the prescribed capecitabine dosage. Dosage, frequency and numbers of cycle of chemotherapy were decided by treating physician. All patients were followed at three‑week intervals during each treatment cycle to monitor and assess the development of HFS until completion of capecitabine therapy.
Study Size Estimation
The sample size estimation was based on previous study, which reported a 26.8% incidence of grade 2–3 HFS among patients receiving capecitabine-based chemotherapy.8 In that study, 34.72% of patients receiving capecitabine at doses greater than 3000 mg/day developed grade 2–3 HFS, compared to 21.05% among those receiving less than 3000 mg/day, with a ratio of low- to high-dose patients of 1.8:1. Using a two-sample comparison of proportions, the calculating sample size required 140 patients in the high-dose group and 252 in the low-dose group, totaling 392 patients.
Data Collection
Data were extracted from electronic medical records by trained investigators using a standardized data collection form. Baseline data included sex, age, body mass index (BMI), body surface area (BSA), and Eastern Cooperative Oncology Group (ECOG) performance status before treatment. Laboratory measures included estimated glomerular filtration rate (eGFR) and serum albumin. Clinical variables included cancer type, prophylactic use of topical diclofenac for HFS prevention, combination chemotherapy, capecitabine dosage, dosing frequency, and number of chemotherapy cycles. Capecitabine is available in 500 mg tablets, and the prescribed daily doses were classified as 2000, 2500, 3000, 3500, and 4000 mg/day, corresponding to the actual dosage regimens for each patient. Outcomes recorded were the grade of HFS and other complications, including diarrhea, sepsis, and death. To ensure data accuracy, a random subset of records was independently cross-checked by a second investigator. Potential prognostic and confounding factors were identified using a directed acyclic graph (DAG) (Figure 1), with sex, combination chemotherapy, and eGFR considered key confounders. In the DAG, capecitabine dosage (green) is the exposure of interest, and grade 2–3 HFS (blue) is the outcome. Arrows indicate hypothesized causal pathways. Pink nodes represent potential confounders that may influence both exposure and outcome. The DAG was constructed based on previously reported risk factors shown to be associated with the development of HFS.
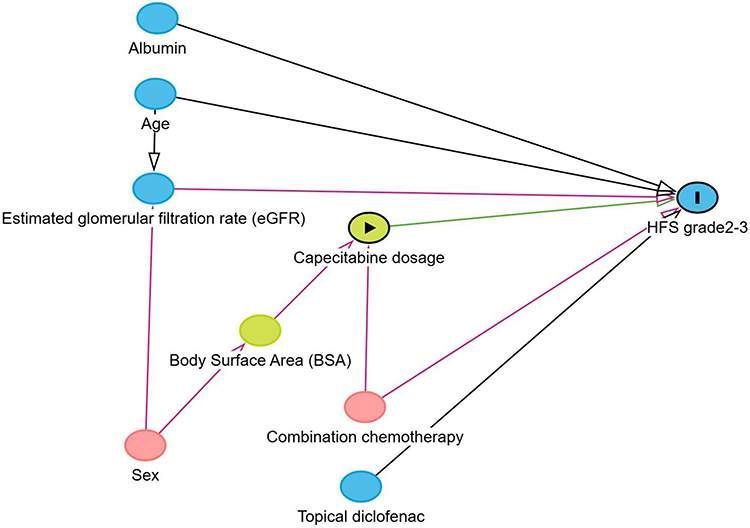 |
Figure 1 Directed acyclic graph (DAG) illustrating the hypothesized causal relationships among clinical and treatment-related variables associated with the development of grade 2–3 hand–foot syndrome in patients receiving capecitabine. Capecitabine dosage (green) represents the exposure of interest, and grade 2–3 hand–foot syndrome (blue) represents the outcome. Pink nodes indicate potential confounders that may influence both exposure and outcome, and arrows denote hypothesized causal pathways. |
Outcome
The study endpoints were evaluated using the cumulative incidence of grade 2–3 HFS and the model-predicted median time to onset. The primary endpoint was the first occurrence of grade 2 or 3 HFS confirmed by physical examination. The severity of HFS was assessed by attending oncologists using the National Cancer Institute’s Common Terminology Criteria for Adverse Events (NCI CTCAE), version 5.0. As this was an observational study in a routine clinical setting, assessors were not blinded to capecitabine dosage. Grading was defined as follows: Grade 1 (mild), minimal skin changes or dermatitis (eg, erythema, edema, or hyperkeratosis) without pain; Grade 2 (moderate), skin changes (eg, peeling, blisters, bleeding, fissures, edema, or hyperkeratosis) with pain limiting instrumental activities of daily living (ADL); and Grade 3 (severe), severe skin changes with pain limiting self-care ADL.12 The median time to event was estimated using competing risk analysis.
Statistical Analysis
All statistical analyses were performed using Stata version 19 (StataCorp LLC, College Station, TX, USA). Categorical variables were summarized as frequencies and percentages. For continuous variables, data distribution was assessed using histograms, and variables were reported as mean with standard deviation or median with interquartile range (IQR), as appropriate. Non-parametric survival comparisons for time-to-event outcomes between categorical variables at the specified time point of interest were performed using the Log rank test. Categorical variables were analyzed with the Chi-square test or Fisher’s exact test, as appropriate. Continuous variables were analyzed using either the independent t-test or the Mann–Whitney U-test, depending on data distribution. A p-value of less than 0.05 was considered statistically significant.
Missing Data Management
This study was conducted as an explanatory analysis focusing on the causal effect of capecitabine dosage. The exposure variable, capecitabine dosage, was not imputed; patients with missing dosage data were therefore excluded from the analysis. Baseline confounder variables predefined using a DAG were eligible for imputation. For confounder variables with less than 50% missing data, missing values were handled using multiple imputation.
Competing Risk Analysis
A competing risk model was used to assess the association between capecitabine dosage and the occurrence of grade 2–3 HFS, in which the dosage of interest was the initially prescribed daily dosage prior to the development of grade 2–3 HFS. Other severe toxicities, including grade 3 diarrhea, sepsis, death, and loss to follow-up, were considered as competing events. These events were classified as competing because they could result in premature discontinuation of capecitabine treatment before the development of grade 2–3 HFS, which was the primary event of interest. These competing outcomes were incorporated into the statistical model to appropriately account for competing events that preclude the occurrence of the primary outcome, thereby yielding unbiased estimates of HFS risk and time-to-event outcomes. stcrprep was used to prepare data for competing risks analysis with time-dependent weights to estimate subdistribution hazard ratios.13 Multivariable competing risk analysis was performed using the Lambert model, which applied parametric distributions to the cause-specific cumulative incidence function (CIF). This approach allows the use of standard Stata survival analysis commands to analyze competing risks. Standard survival distributions, including Exponential, Weibull, Gompertz, and Gamma, were evaluated to determine the best-fitting model based on Akaike’s Information Criterion (AIC). Additionally, cumulative incidence functions were plotted to demonstrate the risk of grade 2–3 HFS at different capecitabine dosage levels, accounting for competing events.
Results
Between January 2018 and December 2024, 597 cancer patients received capecitabine treatment with one patient excluded due to missing essential dosage data, resulting in a final cohort of 596 patients (Figure 2). The median follow-up duration was 126 days. The median number of capecitabine treatment cycles was higher among patients with grade 2–3 HFS (147 cycles vs 126 cycles). The median time to onset of grade 2–3 HFS was 63 days (interquartile range [IQR], 42–84), which is equivalent to about three treatment cycles of capecitabine. Baseline characteristics at the median time to onset of grade 2–3 HFS were largely comparable between patients who developed HFS and those who did not, with no statistically significant differences in age, sex, BMI, BSA, ECOG performance status, renal function, or serum albumin (Table 1). Treatment characteristics were summarized in Table 2, which details the distribution of capecitabine dosage levels stratified by the development of grade 2–3 HFS. The distribution of combination chemotherapy agents was similar between groups (p = 0.166), with oxaliplatin being the most commonly used agent. In contrast, capecitabine dosage significantly differed between groups, with the highest dosage group (4000 mg/day) showing a notably greater proportion of HFS cases (6.82% vs 1.51%).
 |
Table 1 Baseline Characteristics and Non-Parametric Survival Comparison of Grade 2–3 HFS at the Median Onset Time |
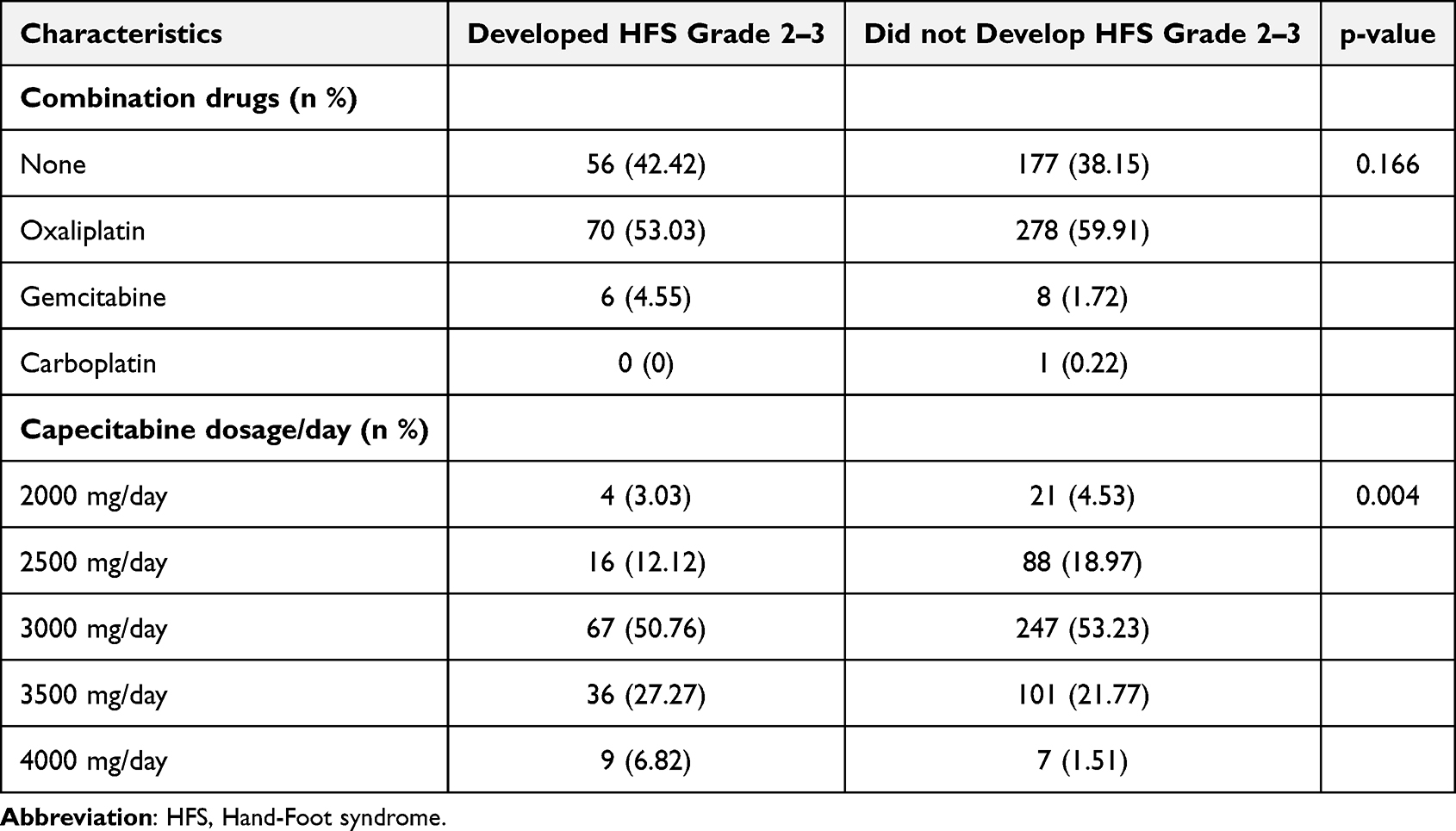 |
Table 2 Capecitabine Dosage and Combination Drug in Patients with and without HFS Grades 2–3 |
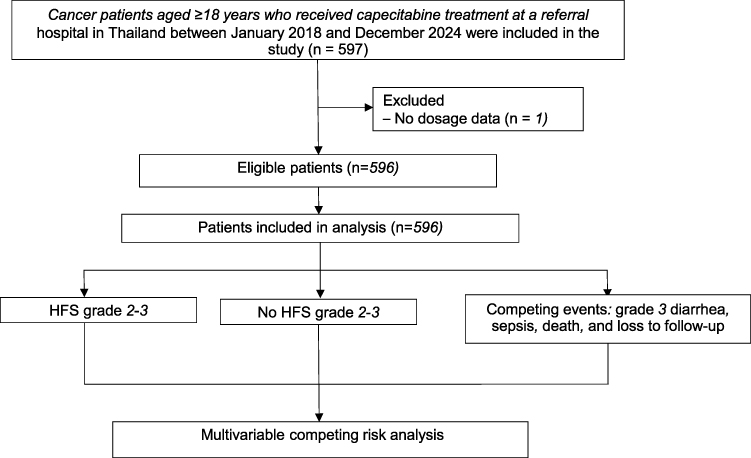 |
Figure 2 Study flow. |
Among 596 patients included in the analysis, 132 (22.2%) developed grade 2–3 HFS, which was considered the primary event of interest. A total of 385 patients (64.6%) completed capecitabine treatment without developing grade 2–3 HFS and were classified as having no event. Competing events included other grade 3 toxicities, such as diarrhea or sepsis, in 45 patients (7.6%), death from any cause in 5 patients (0.8%), and loss to follow-up in 29 patients (4.9%).
Multivariable competing risk analysis demonstrated a dose-dependent association between capecitabine dosage and the development of grade 2–3 HFS (Table 3). Increasing capecitabine dosage was associated with a progressive rise in the risk of grade 2–3 HFS. Compared with 2000 mg/day, the adjusted hazard ratios were 0.92 (95% CI, 0.30 to 2.80) for 2500 mg/day, 1.34 (0.47 to 3.85) for 3000 mg/day, 1.73 (0.58 to 5.20) for 3500 mg/day, and 4.41 (1.31 to 14.81; p = 0.016) for 4000 mg/day, with a statistically significant increase in risk observed at the highest dosage. The cumulative incidence of grade 2–3 HFS stratified by capecitabine dosage is presented in Figure 3.
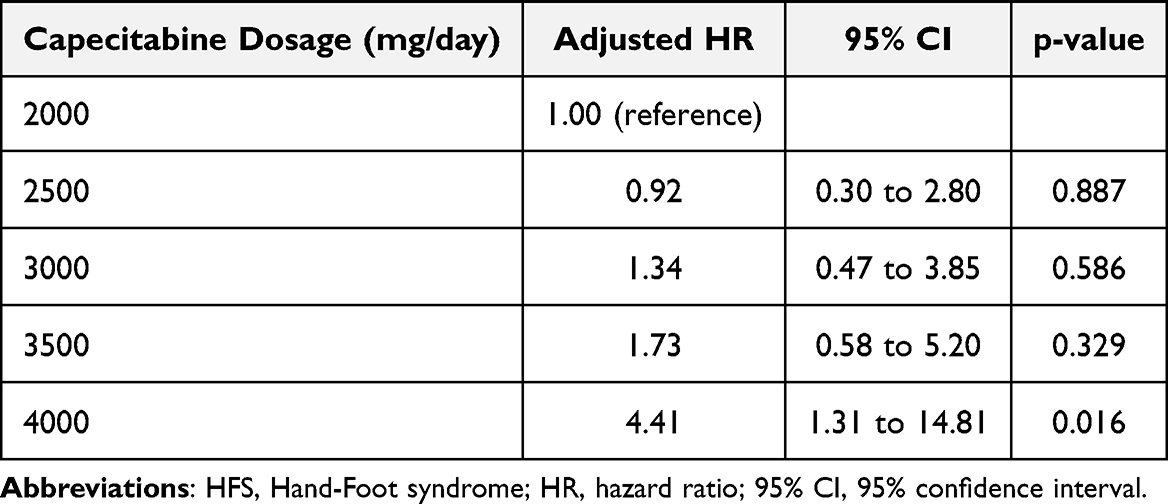 |
Table 3 Adjusted Hazard Ratios by Capecitabine Dosage for Grade 2–3 HFS |
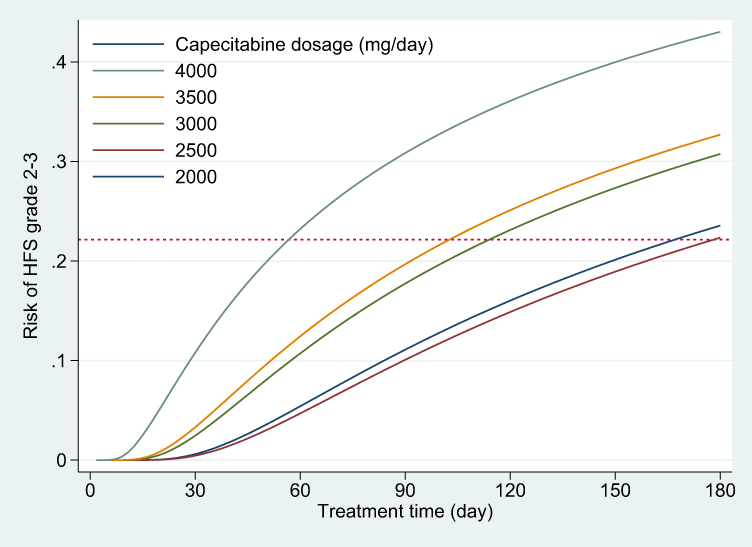 |
Figure 3 Cumulative Incidence of grade 2–3 HFS by capecitabine dosage: adjusted competing risk analysis. |
Using a generalized gamma regression model within the competing risk framework, higher capecitabine dosage was associated with a shorter predicted median time to the development of grade 2–3 HFS. The predicted median time decreased in a dose-dependent manner: 839.8 days (95% CI, 145.3 to 1534.2) at 2000 mg/day, 895.4 days (95% CI, 306.3 to 1484.6) at 2500 mg/day, 573.2 days (95% CI, 240.7 to 905.7) at 3000 mg/day, 516.0 days (95% CI, 162.3 to 869.7) at 3500 mg/day, and 285.2 days (95% CI, 22.3 to 548.1) at 4000 mg/day. A slightly longer predicted median time was observed at 2500 mg/day compared with 2000 mg/day. This difference was small and not statistically significant. These findings suggest that increasing dosage not only raises the risk but also accelerates the onset of grade 2–3 HFS. The predicted median time across dosage levels is illustrated in Figure 4.
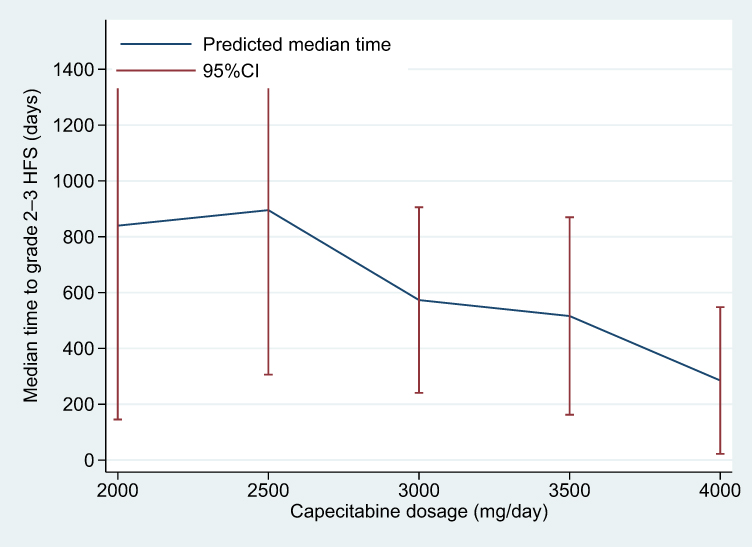 |
Figure 4 Predicted median time to grade 2–3 HFS by capecitabine dosage based on adjusted competing risk generalized gamma regression model. |
Overall, the results consistently demonstrate a clear dose–response relationship, with higher capecitabine doses associated with a substantially increased risk and a shorter predicted time to the development of grade 2–3 HFS.
Discussion
In this study of 596 cancer patients treated with capecitabine, approximately one in five developed grade 2–3 HFS, a clinically relevant toxicity that often leads to dose reduction or treatment interruption. Our findings highlighted a clear, dose-dependent relationship between capecitabine dosage and the risk of developing grade 2–3 HFS, even after adjusting for relevant clinical confounders and accounting for competing events through a multivariable competing risk analysis.
Patients who developed grade 2–3 HFS were slightly older, consistent with previous reports identifying age as a risk factor for capecitabine-related toxicity.7,8,14,15 Notably, the incidence of HFS increased with higher daily capecitabine dosages. Specifically, the adjusted hazard ratio at 4000 mg/day was more than four times that of the reference group (2000 mg/day), confirming a strong, dose-dependent relationship (adjusted HR 4.41, 95% CI 1.31 to 14.81, p = 0.016). These findings were consistent with previous reports, further supporting that capecitabine-related toxicity, including HFS, is more prevalent at higher dose intensities.7–9 In addition to increased risk, higher capecitabine dosage was associated with earlier onset of HFS. Within the competing-risk framework, generalized gamma regression demonstrated a dose-dependent reduction in the predicted median time to onset of grade 2–3 HFS, decreasing from 839.8 days at 2000 mg/day to 285.2 days at 4000 mg/day. These median times represent model based predictions derived from the parametric competing risk model rather than empirically observed median onset times. These findings indicate that higher capecitabine doses are associated with both an increased risk and earlier clinical manifestation of HFS. Notably, Figure 4 shows a slightly shorter predicted median time at 2000 mg/day compared with 2500 mg/day. This minor inversion is consistent with the survival-time regression, in which 2000 mg/day served as the reference (adjusted HR = 1.00) and 2500 mg/day had an adjusted HR of 0.92 (<1), suggesting a marginally longer time to event at 2500 mg/day. However, this difference is not statistically significant. Compared with predicted median times, adjusted hazard ratios yielded more stable estimates with narrower confidence intervals.
Although the median number of treatment cycles was higher in the HFS group, the use of combination chemotherapy regimens did not significantly differ between groups. This suggests that capecitabine itself, rather than the cumulative cytotoxicity effect from combination therapy, may play a more direct role in the development of HFS. The use of a competing risk model strengthens the analysis by addressing the impact of treatment discontinuation due to other toxicities, sepsis, or death, which can obscure the true incidence of HFS when traditional survival models were used. Therefore, our findings provided a more accurate estimate of HFS risk in real-world clinical settings.
Current understanding of the pathogenesis of capecitabine-induced HFS emphasizes the role of genetic susceptibility variants involved in the drug’s metabolic biotransformation. Key enzymes implicated in this process include carboxylesterase 2 (CES2), cytidine deaminase (CDA), thymidine phosphorylase (TP), thymidylate synthase (TS), and dihydropyrimidine dehydrogenase (DPD). Among these, specific polymorphisms namely CDA 943insC and CES2 Exon36046G/A have been reported to be potentially associated with an increased risk of severe adverse effects, including grade 3 HFS and grade 3–4 diarrhea.16–18 In addition, a recent study identified cadherin-4 (CDH4) rs13689 as a potential genetic biomarker for predicting an increased risk of capecitabine-induced HFS. The C allele of this variant may interfere with microRNA-mediated regulation of CDH4 expression, resulting in dysregulated cadherin signaling in skin cells and increased susceptibility to HFS.19 These findings underscore the emerging role of pharmacogenomics in anticipating and managing chemotherapy-related toxicities. However, molecular testing for these genetic abnormalities is not yet feasible for routine clinical practice and cannot be widely used as a criterion for evaluating patients who are to receive capecitabine treatment.
Several studies indicated that capecitabine may trigger an inflammatory response in the skin, potentially medicated by the overexpression of cyclooxygenase-2 (COX-2), which contributes to the development of HFS. TP, the enzyme responsible for the final activation step of capecitabine, is present at elevated levels in tumor tissues, as well as in the certain normal tissues, including the skin.4 Increased TP expression in the skin result in enhanced local activation of capecitabine, leading to localized toxicity and the development of HFS.20–22 Understanding these mechanisms is essential for the development of effective prevention and therapeutic strategies for capecitabine-induced HFS.10,23 Real-world data on these mechanisms are limited, and further investigation is needed.
A key strength of this study is the clear objective to assess the effect of capecitabine dosage using a DAG to adjust for confounding factors, a methodological step that was often not used or inadequately addressed in previous research.7,8,10 Another strength is the use of competing risk analysis, which incorporates the time-dependent nature of capecitabine exposure and accounts for competing events that may preclude the occurrence of HFS, thereby providing a more accurate estimation of the causal relationship between dosage and grade 2–3 HFS. While most previous studies have focused on exploratory evaluations of associations between risk factors and HFS, this study provides confirmatory evidence of specific causal relationships.
However, this study has several limitations. First, the classification of HFS severity relied on clinical documentation, which may be subject to misclassification bias. Variability in the recognition, grading, and reporting of HFS among clinicians could have affected the accuracy of outcome assessment, particularly in borderline cases between grade 1 and grade 2. Second, genetic data were not available in this cohort, limiting the ability to account for pharmacogenetic variants that may influence capecitabine metabolism and toxicity. Previous studies have suggested that polymorphisms in CES2, CDA, and CDH4 may be associated with an increased risk of HFS. Therefore, future prospective studies incorporating genotypic data are warranted to improve the precision of prognostic models. Lastly, although dose intensity was considered, cumulative capecitabine exposure in each treatment cycle was not evaluated. These pharmacologic factors may also contribute to the development of HFS and should be further investigated in future research. In addition, the retrospective observational design may be subject to residual confounding from unmeasured factors, which could not be fully accounted for despite multivariable adjustment.
Conclusion
The results suggest that clinicians should exercise caution when initiating or escalating capecitabine doses to 4000 mg/day, especially in older patients or those with additional risk factors for toxicity. Notably, higher capecitabine dosage was associated not only with an increased risk of grade 2 to 3 HFS, but also with a shorter median time to HFS onset as the dosage level increased. These findings highlight the importance of individualized treatment planning and early preventive monitoring strategies, particularly during the initial treatment cycles in patients receiving higher doses. Future research should focus on developing predictive models that incorporate clinical, pharmacologic, and genomic variables to optimize the safe and effective use of capecitabine. Moreover, the findings from this study may inform practical guidance for dose adjustment and support the implementation of prophylactic strategies in high-risk patients.
Declaration of AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the author(s) used ChatGPT5 in order to check and correct grammatical errors during the manuscript writing process. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Data Sharing Statement
The data that supports the findings of this study is available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki (2013 revision) and approved by the Institutional Review Board and Ethics Committee of Buddhasothorn Hospital (BSH-IRB 002/2568). As this was a retrospective chart review using de-identified data, informed consent was waived. The study was registered with the Thai Clinical Trials Registry (TCTR20250419006), and all data were maintained under strict confidentiality.
Acknowledgments
This study was partially supported by the Division of Medical Oncology, Department of Internal Medicine, Buddhasothorn Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received from public, commercial, or not-for-profit agencies for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Koukourakis GV, Kouloulias V, Koukourakis MJ, Zacharias GA, Zabatis H, Kouvaris J. Efficacy of the oral fluorouracil pro-drug capecitabine in cancer treatment: a review. Molecules. 2008;13(8):1897–11. doi:10.3390/molecules13081897
2. Knikman JE, de Vries N, Rosing H, Cats A, Guchelaar HJ, Beijnen JH. Development of a UPLC-MS/MS assay for the quantitative determination of Capecitabine, 5’-deoxy-5-fluorocytidine (5’-dFCR), 5’-deoxy-5-fluorouridine (5’-dFUR), 5’-fluorouracil (5-FU), and α-fluoro-β-alanine (FBAL). Pharmazie. 2023;78(8):107–112. doi:10.1691/ph.2023.3001
3. Miura K, Kinouchi M, Ishida K, et al. 5-FU metabolism in cancer and orally-administrable 5-FU drugs. Cancers. 2010;2(3):1717–1730. doi:10.3390/cancers2031717
4. de With M, van Doorn L, Maasland DC, et al. Capecitabine-induced hand-foot syndrome: a pharmacogenetic study beyond DPYD. Biomed Pharmacother. 2023;159:114232. doi:10.1016/j.biopha.2023.114232
5. Baack BR, Burgdorf WH. Chemotherapy-induced acral erythema. J Am Acad Dermatol. 1991;24(3):457–461. doi:10.1016/0190-9622(91)70073-b
6. Saif MW. Capecitabine and hand-foot syndrome. Expert Opin Drug Saf. 2011;10(2):159–169. doi:10.1517/14740338.2011.546342
7. King TL, Voon PJ, Yuen KH, Mohamed Noor DA. Hand-foot syndrome in cancer patients on capecitabine: examining prevalence, impacts, and associated risk factors at a cancer centre in Malaysia. Support Care Cancer. 2024;32(6):345. doi:10.1007/s00520-024-08490-7
8. Chantharakhit C, Sujaritvanichpong N. Predictive factors for the development of capecitabine-induced hand-foot syndrome: a retrospective observational cohort study. Ann Med Surg. 2024;86(1):73–77. doi:10.1097/ms9.0000000000001487
9. Kanbayashi Y, Taguchi T, Ishikawa T, Otsuji E, Takayama K. risk factors of capecitabine-induced hand-foot syndrome: a single-institution, retrospective study. Oncology. 2023;101(7):407–414. doi:10.1159/000529851
10. Yap YS, Kwok LL, Syn N, et al. Predictors of hand-foot syndrome and pyridoxine for prevention of capecitabine-induced hand-foot syndrome: a randomized clinical trial. JAMA Oncol. 2017;3(11):1538–1545. doi:10.1001/jamaoncol.2017.1269
11. Gressett SM, Stanford BL, Hardwicke F. Management of hand-foot syndrome induced by capecitabine. J Oncol Pharm Pract. 2006;12(3):131–141. doi:10.1177/1078155206069242
12. Abdul Kareem S, Joseph SG, Wilson A, Kareem SA, Kunjumon Vilapurathu J. Incidence and severity of hand-foot syndrome in cancer patients receiving infusional 5-fluorouracil or oral capecitabine-containing chemotherapy regimens. Journal of Oncology Pharmacy Practice. 2025;31(2):203–209. doi:10.1177/10781552241228175
13. Lambert PC. The estimation and modelling of cause-specific cumulative incidence functions using time-dependent weights. Stata J. 2017;17(1):181–207. doi:10.1177/1536867X1701700110
14. van Beek MWH, Roukens M, Jacobs WCH, Timmer-Bonte JNH, Kramers C. Real-world adverse effects of capecitabine toxicity in an elderly population. Drugs Real World Outcomes. 2018;5(3):161–167. doi:10.1007/s40801-018-0138-9
15. Meulendijks D, van Hasselt JGC, Huitema ADR, et al. Renal function, body surface area, and age are associated with risk of early-onset fluoropyrimidine-associated toxicity in patients treated with capecitabine-based anticancer regimens in daily clinical care. Eur J Cancer. 2016;54:120–130. doi:10.1016/j.ejca.2015.10.013
16. Caronia D, Martin M, Sastre J, et al. A polymorphism in the cytidine deaminase promoter predicts severe capecitabine-induced hand-foot syndrome. Clin Cancer Res. 2011;17(7):2006–2013. doi:10.1158/1078-0432.Ccr-10-1741
17. Ribelles N, López-Siles J, Sánchez A, et al. A carboxylesterase 2 gene polymorphism as predictor of capecitabine on response and time to progression. Curr Drug Metab. 2008;9(4):336–343. doi:10.2174/138920008784220646
18. Loganayagam A, Arenas Hernandez M, Corrigan A, et al. Pharmacogenetic variants in the DPYD, TYMS, CDA and MTHFR genes are clinically significant predictors of fluoropyrimidine toxicity. Br J Cancer. 2013;108(12):2505–2515. doi:10.1038/bjc.2013.262
19. Ruiz-Pinto S, Pita G, Martín M, et al. Regulatory CDH4 genetic variants associate with risk to develop capecitabine-induced hand-foot syndrome. Clin Pharmacol Ther. 2021;109(2):462–470. doi:10.1002/cpt.2013
20. Yang B, Xie X, Lv D, et al. Capecitabine induces hand-foot syndrome through elevated thymidine phosphorylase-mediated locoregional toxicity and GSDME-driven pyroptosis that can be relieved by tipiracil. Br J Cancer. 2023;128(2):219–231. doi:10.1038/s41416-022-02039-3
21. Saif MW, Juneja V, Black G, Thronton J, Johnson MR, Diasio RB. Palmar-plantar erythrodysesthesia in patients receiving capecitabine and intratumor thymidine phosphorylase and dihydropyrimidine dehydrogenase: is there a pharmacologic explanation? Support Cancer Ther. 2007;4(4):211–218. doi:10.3816/SCT.2007.n.017
22. Milano G, Etienne-Grimaldi MC, Mari M, et al. Candidate mechanisms for capecitabine-related hand-foot syndrome. Br J Clin Pharmacol. 2008;66(1):88–95. doi:10.1111/j.1365-2125.2008.03159.x
23. Santhosh A, Sharma A, Bakhshi S, et al. Topical diclofenac for prevention of capecitabine-associated hand-foot syndrome: a double-blind randomized controlled trial. J Clin Oncol. 2024;42(15):1821–1829. doi:10.1200/jco.23.01730
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.