Back to Journals » Journal of Pain Research » Volume 18
Can Ziconotide Be Used to Replace Opioids? Exploratory Clinical Experience in 5 Patients Treated in the Pain Unit
Authors Canovas Martínez L ![]() , Gago Diéguez N, Carrera Sieiro JL, López Díez R, García González C, Ortolá Más E, Almenara S
, Gago Diéguez N, Carrera Sieiro JL, López Díez R, García González C, Ortolá Más E, Almenara S
Received 19 March 2025
Accepted for publication 3 August 2025
Published 17 September 2025 Volume 2025:18 Pages 4859—4870
DOI https://doi.org/10.2147/JPR.S528946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Timothy Atkinson
Luz Canovas Martínez,1 Noelia Gago Diéguez,2 Jackeline Lucia Carrera Sieiro,2 Rocío López Díez,2 Cristina García González,2 Elena Ortolá Más,2 Susana Almenara3
1Pain Unit, University Hospital of Ourense, Ourense, Spain; 2Anesthesiology, University Hospital of Ourense, Ourense, Spain; 3Clinical Pharmacology, Princess University Hospital, Madrid, Spain
Correspondence: Luz Canovas Martínez, Head of the Pain Unit, University Hospital of Ourense, Calle Ramón Puga 52, Ourense, 32005, Spain, Email [email protected]
Background: Ziconotide and morphine are intrathecal (IT) drugs approved by the FDA and EMA for the treatment of chronic pain. The aim of this study was to determine whether opioid rescue can be achieved by gradually increasing doses of ziconotide, and to establish a practical protocol for its implementation.
Methods: Five patients unresponsive to IT morphine due to lack of efficacy or adverse events such as endocrine dysfunction, constipation and tolerance were selected. All had refractory, neuropathic or mixed pain. Ziconotide was gradually introduced while maintaining or reducing morphine doses in proportion to the ziconotide titration. Dose adjustments were made every 2 weeks, with a weekly ziconotide increase of 0.5 μg.
Results: Of the five patients, three were female and two were male, with ages ranging from 53 to 75 years. Two had cancer (one with colon cancer and one with osteosarcoma), two had persistent spinal pain syndrome type 2, and one had spastic paraparesis. After 6 weeks of ziconotide treatment, all individuals showed a substantial reduction in daily morphine dosage (from 10 to 5.5 mg/day), which was associated with improved control of adverse events. Similarly, notable reductions were observed in pain intensity (from 8.0 to 2.5, measured by VAS) and neuropathic symptoms (from 6.0 to 2.0, measured by DN4). The most frequently improved neuropathic symptoms included tingling (4 patients), hypoesthesia to touch (3 patients), and pain evoked by brushing (3 patients). The duration of the rescue protocol ranged from 5 to 11 weeks.
Conclusion: Intrathecal opioid rescue with ziconotide emerges as a viable therapeutic option for patients with refractory pain and a neuropathic component, or for those who develop adverse events associated with IT morphine. Low doses and slow titration of ziconotide may help minimize adverse events while maintaining analgesic benefit.
Plain Language Summary: Ziconotide and morphine are two medications used to treat chronic pain by delivering the drugs directly into the spinal fluid. While both are approved by health authorities like the FDA and EMA, some patients have problems with morphine, such as side effects or not working well enough. This study looked at whether ziconotide could help these patients by reducing the need for morphine and controlling their pain more effectively.
Five patients who did not respond well to morphine or had side effects were included in the study. The researchers gradually increased the dose of ziconotide while either keeping the morphine dose the same or reducing it. The patients’ pain and side effects were carefully monitored.
The results showed that all the patients were able to significantly reduce their morphine doses, which helped to reduce unwanted side effects. At the same time, their pain levels decreased, and their neuropathic symptoms (pain caused by nerve damage) improved. The rescue period lasted from 5 to 11 weeks.
In conclusion, ziconotide may be a good alternative for people who have problems with morphine or have pain that does not respond to traditional treatments. Using low doses of ziconotide and increasing them slowly helps to minimize side effects while maintaining analgesic benefit.
Keywords: morphine, rescue, slow titrations, undesirable effects, ziconotide
A Letter to the Editor has been published for this article.
Introduction
Ziconotide is a non-opioid analgesic drug, with the ability to bind reversibly and selectively to sensitive N-type calcium channels located in the superficial lamina of the dorsal horn of the spinal cord. Its analgesic action is mediated by preventing the flow of calcium ions towards the presynaptic nociceptor terminals of the A∂- and C-fibers.1,2
Both, ziconotide and morphine are intrathecal (IT) drugs approved by the FDA and EMA for the treatment of chronic pain. Their use as monotherapy has a 1A recommendation level and a strong consensus level.3 Although mixtures are not officially approved, these drugs can be combined when monotherapy fails treating pain syndromes.3 However, evidence for specific drug combinations and doses is still unclear.
Our hypothesis is that the gradual introduction of ziconotide to first-line IT analgesia in Europe could provide adequate pain relief and reduce the burden of IT morphine in patients with refractory chronic pain without a history of psychosis.
Several studies have reported the successful use of combined IT morphine and ziconotide therapy.4,5 Besides, studies in experimental animals show that the combination of ziconotide and IT morphine produces synergistic analgesic effects.1,6 Morphine and ziconotide have demonstrated a supra-additive and probably synergistic effect on A∂-mediated nociception, likely due mediated through their action at presynaptic and postsynaptic sites, respectively, suggesting the involvement of different mechanisms of action.6
Patients most likely to benefit from opioid rescue with ziconotide include young adults under 50 years of age, particularly those at risk for or exhibiting neuroendocrine dysfunction secondary to morphine, and patients requiring progressive increases in morphine, with the associated risk of tolerance and hyperalgesia, report of intolerable adverse events and/or granuloma formation.5,7
The most potentially serious adverse event associated with long-term use of IT opioids is respiratory depression, but there are other undesirable effects such as endocrinopathy and constipation, and even decreased libido and hypogonadotropic hypogonadism.7,8 Therefore, it is advisable to closely monitor neuroendocrine function both before and during IT opioid therapy.
There is also an increased risk of non-infectious inflammatory masses, or granulomas, at the tip of the catheter in patients receiving high-dose IT opioids. The formation of granulomas has the potential to result in spinal cord compression, which may subsequently give rise to a range of neurological complications, ranging in severity from loss of analgesia to a complete paralysis of the lower extremities or paraplegia.7
Patients with advanced age, morbid obesity, sleep apnea, and/or cardiopulmonary disease must be carefully considered, as there is an increased risk of respiratory depression and exacerbation of their cardiopulmonary problem in those patients using increasing doses of IT morphine.5 Finally, when the analgesia provided by IT morphine is inadequate and/or the patient still has refractory neuropathic symptoms and bone metastases, an opioid rescue with ziconotide must be taken into account.9
While the adverse effects of IT morphine are well documented, ziconotide also carries potential risks, most notably psychiatric side effects such as confusion, hallucinations, and mood changes, particularly at high doses or with rapid titration. Therefore, patient selection and cautious up-titration are essential for minimizing risks and optimizing outcomes.
Despite increasing clinical interest, there is still a lack of standardized protocols for ziconotide titration and opioid rescue, and evidence supporting the effectiveness of gradual ziconotide replacement for IT morphine in real-world settings remains limited.
The aim of this study was to assess whether opioid rescue with ziconotide -defined here as the replacement of IT morphine with ziconotide- can be successfully implemented, and to establish a practical protocol for its use in routine clinical settings. However, given the small sample size of our study, the findings should be viewed as preliminary and hypothesis-generating, supporting the need for further research.
Methods
Subject Population and Study Protocol. Inclusion Criteria
Patients with chronic oncological or non-oncological pain treated with IT morphine who showed a lack of analgesic response or treatment-related adverse events. The study was conducted in University Hospital of Ourense with previous approval by the Ethics Committee from the same hospital, and in accordance with the Declaration of Helsinki and the Good Clinical Practice Guidelines. All patients signed the written informed consent form for implantation and data collection and publication. After patient selection, and given the narrow therapeutic range of IT ziconotide,10 we performed a refill every two weeks, mainly due to the absence of a single guideline on the dose of IT morphine in combination with ziconotide. We based the initial dose of ziconotide on evidence suggesting an initial dose of 0.5 μg/day and an increase of 0.5 μg/day, once a week.11 When ziconotide was used in combination with morphine, ziconotide was considered the primary drug. The decrease in morphine dose was equivalent to the increase in ziconotide dose. In patients experiencing pain despite treatment due to lack of efficacy, presence of neuropathic or mixed component or bone metastases, morphine doses were maintained and ziconotide doses were increased. The dose was changed every 2 weeks, considering the increase of 0.5 μg per week of ziconotide (Figure 1). For patients who presented morphine-related effects, a dose reduction of morphine equivalent to ziconotide increase was considered (Figure 2). Oral morphine supplements were prescribed to avoid withdrawal syndrome.
 |
Figure 1 Dose titration every 2 weeks based on 0.5 µg/week increments. |
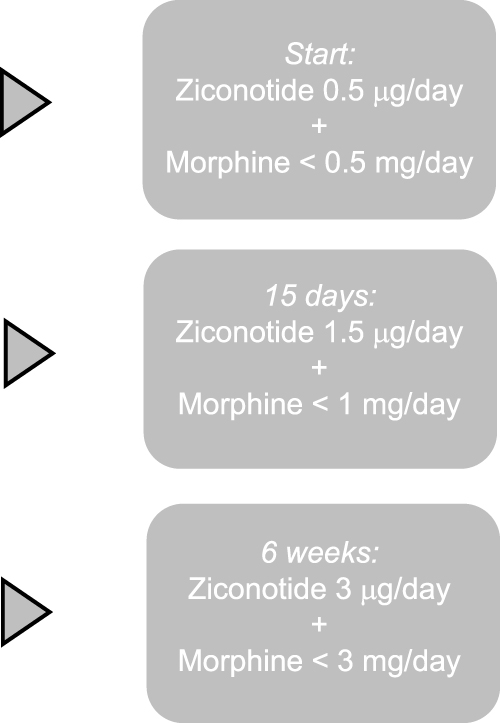 |
Figure 2 Progressive reduction of intrathecal morphine and titration of ziconotide over a 6-week period. |
Clinical Evaluation
Patients were assessed at the baseline visit, at the beginning of the third and sixth weeks, continuing at this cadence until symptom control was achieved, and then coinciding with the recharge. The following variables were assessed:
- Pain intensity: Measured by Visual Analogue Scale (VAS), scoring from 0–10 (0: absence pain, 10: worst pain).
- Neuropathic pain questionnaire-10 items (DN4): Consisting of 10 items and the total score is calculated as the sum of the 10 items. The presence of neuropathic pain is considered when DN4> 4/10.
- Eastern Cooperative Oncologic Group (ECOG): Quality of life scale for patients scoring from 0 to 5 (0=normal activity, 5: death).
- Patient Global Impression of Improvement (PGI-I) scale: Scoring from 1 to 7 (1: much better, 7: much worse).
- Adverse events: Adverse events potentially related to IT morphine (eg, sedation, drowsiness, constipation, respiratory depression) and ziconotide (eg, confusion, decreased level of consciousness, hallucinations, dizziness, myalgia) were recorded at each follow-up visit. Regarding the ziconotide-related adverse events, if symptoms were mild, the dose was reduced by 0.5 µg/day, and if symptoms persisted despite dose reduction, ziconotide was discontinued. CK levels were monitored routinely. The increase in CK associated with the drug, which usually occurs during the first two months of treatment, was managed according to the presence or absence of symptoms. If an asymptomatic increase in CK was observed, the dose of ziconotide was maintained. If myalgia symptoms occurred in the context of elevated CK, the dose was reduced. Oral morphine supplements were prescribed to prevent withdrawal symptoms in patients undergoing morphine dose reductions.
Statistical Methods
The scores on the VAS and DN4 scale were compared before (baseline) and 6 weeks after the application of the rescue protocol with ziconotide. Morphine doses were compared before (baseline) and 6 weeks after the application of the rescue protocol with ziconotide. Data for quantitative variables are shown as median (IQR), data for qualitative variables are described as number and frequency in percentage. The Wilcoxon signed rank test was applied to compare paired quantitative data.
No formal sample size calculation was performed, as this was a preliminary investigation aimed at evaluating the potential of intrathecal ziconotide as an alternative to morphine in patients with chronic pain who experienced either insufficient analgesia or opioid-related adverse effects. The primary objective was to observe potential clinical effects and feasibility, with findings intended to inform future research involving larger patient populations.
Results
Demographic Characteristics
A total of 5 patients unresponsive to IT morphine and with refractory, neuropathic or mixed pain were selected. The rescue protocol was used in these 5 patients: 3 were treated with IT polyanalgesia of morphine and bupivacaine; 1 with IT morphine and baclofen; and 1 with IT morphine monotherapy. Among these patients, two had oncologic conditions: stage IV colon adenocarcinoma, experiencing neuropathic and bone pain due to pelvic and sacrum invasion, succumbed 18 months post-implantation of the IT device; a long-term survivor of femur osteosarcoma.
Patient data, including demographic characteristics, clinical diagnoses, pump flow, baseline IT load, and reasons for initiating rescue, are represented in Table 1 for each patient. All patients presented chronic and severe pain at baseline and all but one had neuropathic symptoms. All described morphine-related adverse events: constipation, tolerance and, in one case, endocrine dysfunction. One of them, diagnosed with spastic paraparesis, had spasticity despite treatment with baclofen.
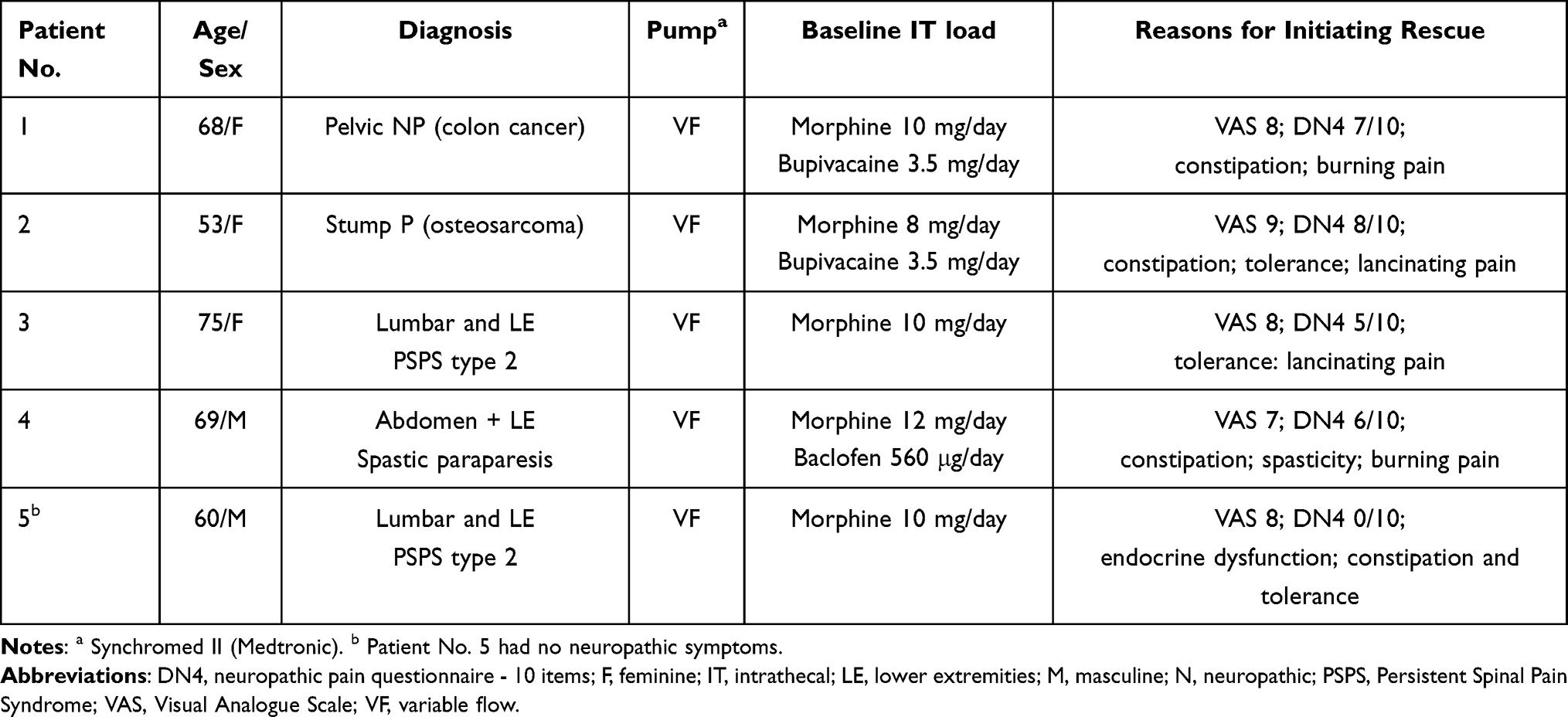 |
Table 1 Demographic Characteristics, Clinical Diagnoses, Baseline Intrathecal Load, and Reasons for Initiating Rescue |
Clinical Evaluation results
Table 2 presents the time since IT device implantation, the initiation and duration of the ziconotide rescue protocol, the final IT medication dosage, and patient-reported evaluation scale results for each individual. After 6 weeks of ziconotide treatment, all individuals showed a substantial reduction in daily morphine dosage from 10 to 5.5 mg/day, which allowed adequate control of adverse events. No adverse events were observed as a result of ziconotide administration or morphine dose reduction. Similarly, a notable reduction was observed in pain intensity from 8.0 to 2.5 (measured by VAS), and in neuropathic symptoms from 6.0 to 2.0 (measured by DN4) (Table 3; Figures 3–5).
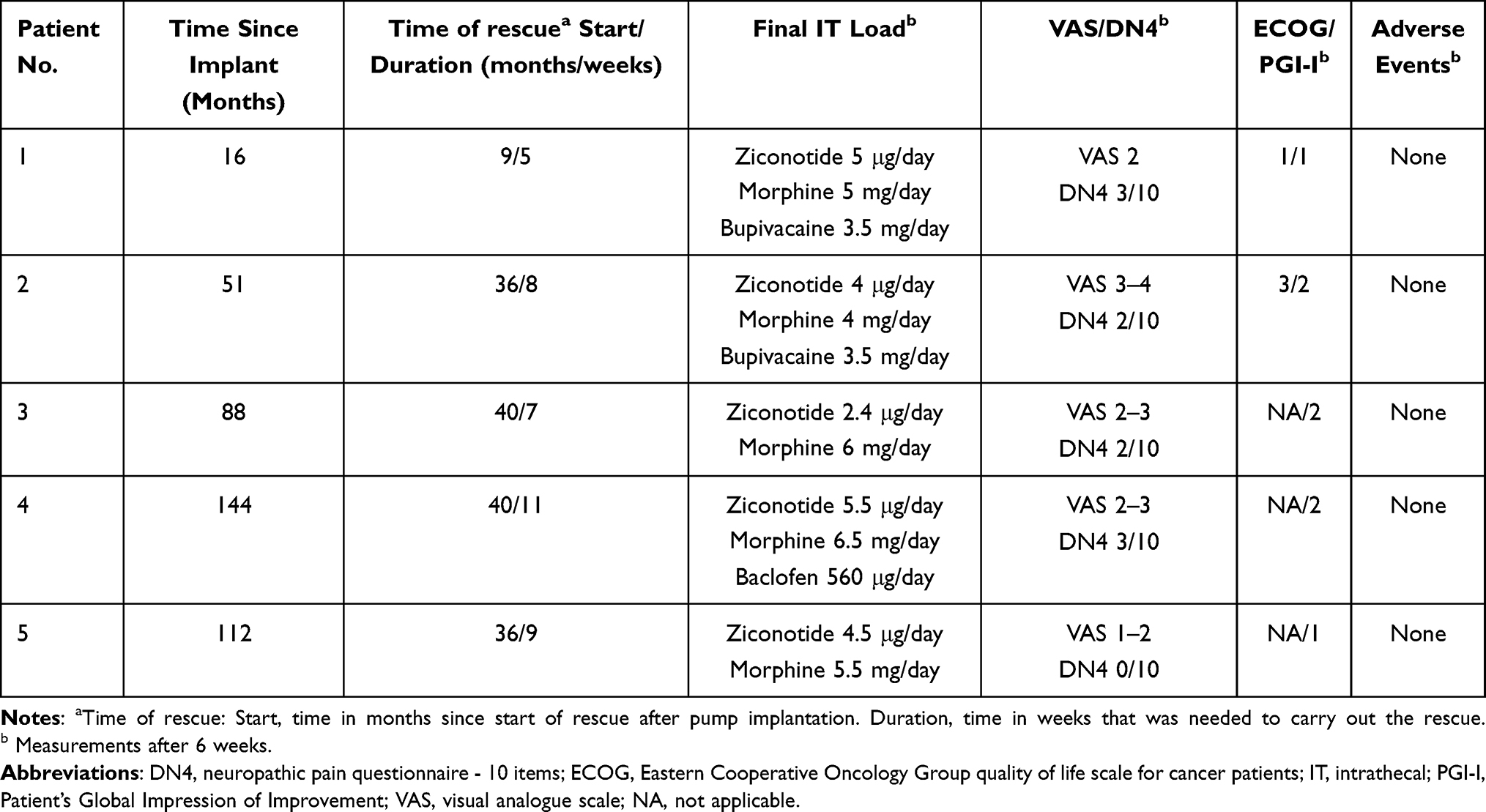 |
Table 2 Time Since Implantation, Initiation and Duration of Rescue Protocol, and Patient-Reported Evaluation Scales |
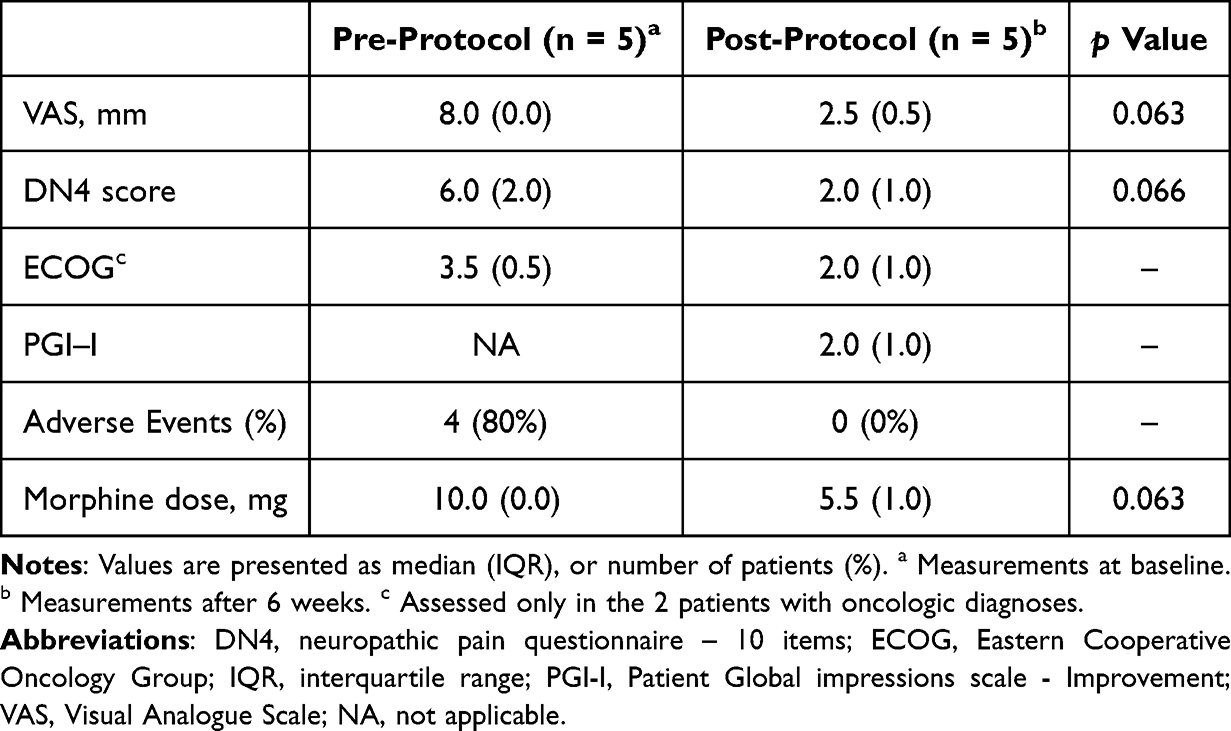 |
Table 3 Clinical Changes After 6 weeks of Ziconotide Rescue Protocol |
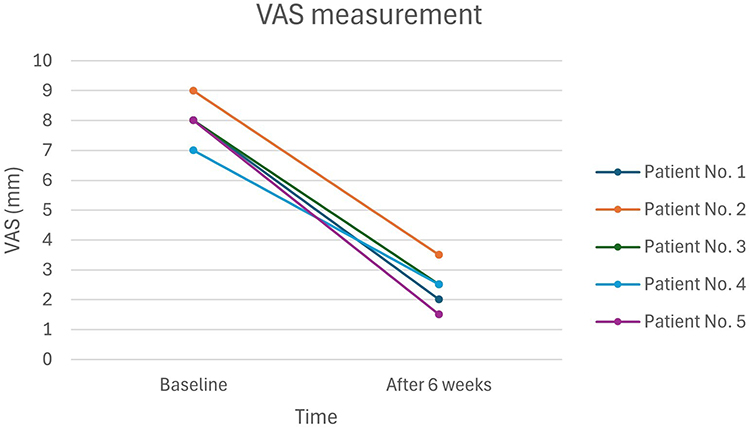 |
Figure 3 Changes in pain intensity (VAS) after 6 weeks of ziconotide rescue protocol. |
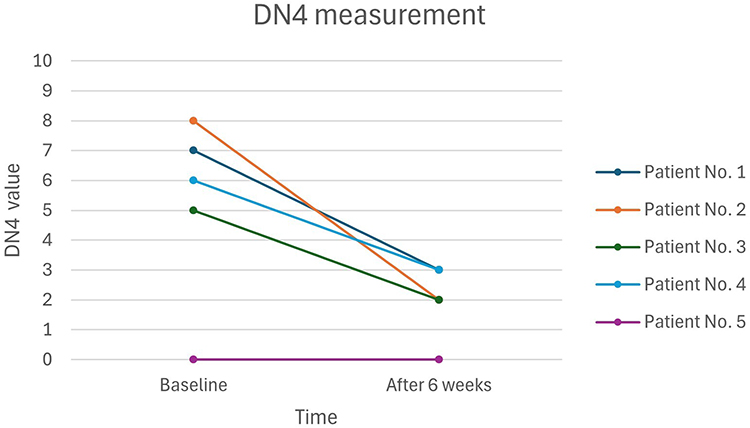 |
Figure 4 Changes in neuropathic symptoms (DN4) after 6 weeks of ziconotide rescue protocol. |
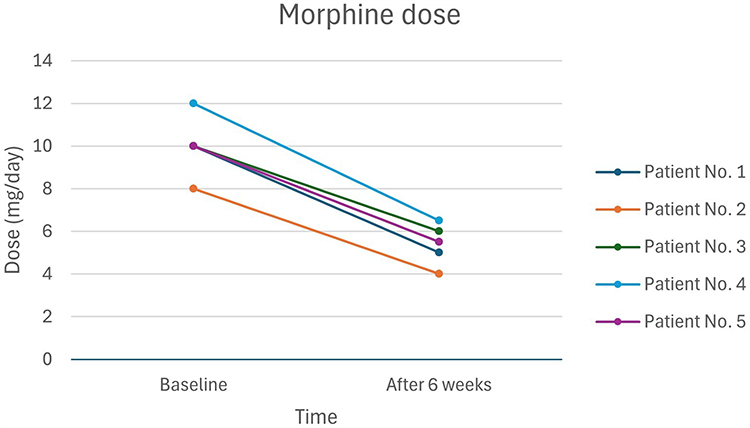 |
Figure 5 Changes in daily intrathecal morphine dose after 6 weeks of ziconotide rescue protocol. |
The ECOG performance status was assessed only in the two oncologic patients. After 6 weeks, ECOG improved from 3 to 1 in Patient No. 1, and from 4 to 3 in Patient No. 2.
Table 4 shows the changes in the 10-item DN4 questionnaire for each patient, except for Patient 5, who did not present any neuropathic symptoms. The most frequently improved neuropathic symptoms were tingling (in 4 patients), hypoesthesia to touch (in 3 patients), and pain evoked by brushing (in 3 patients). The duration of the rescue protocol ranged from 5 to 11 weeks, after which drug doses remained stable and could even be reduced in one patient.
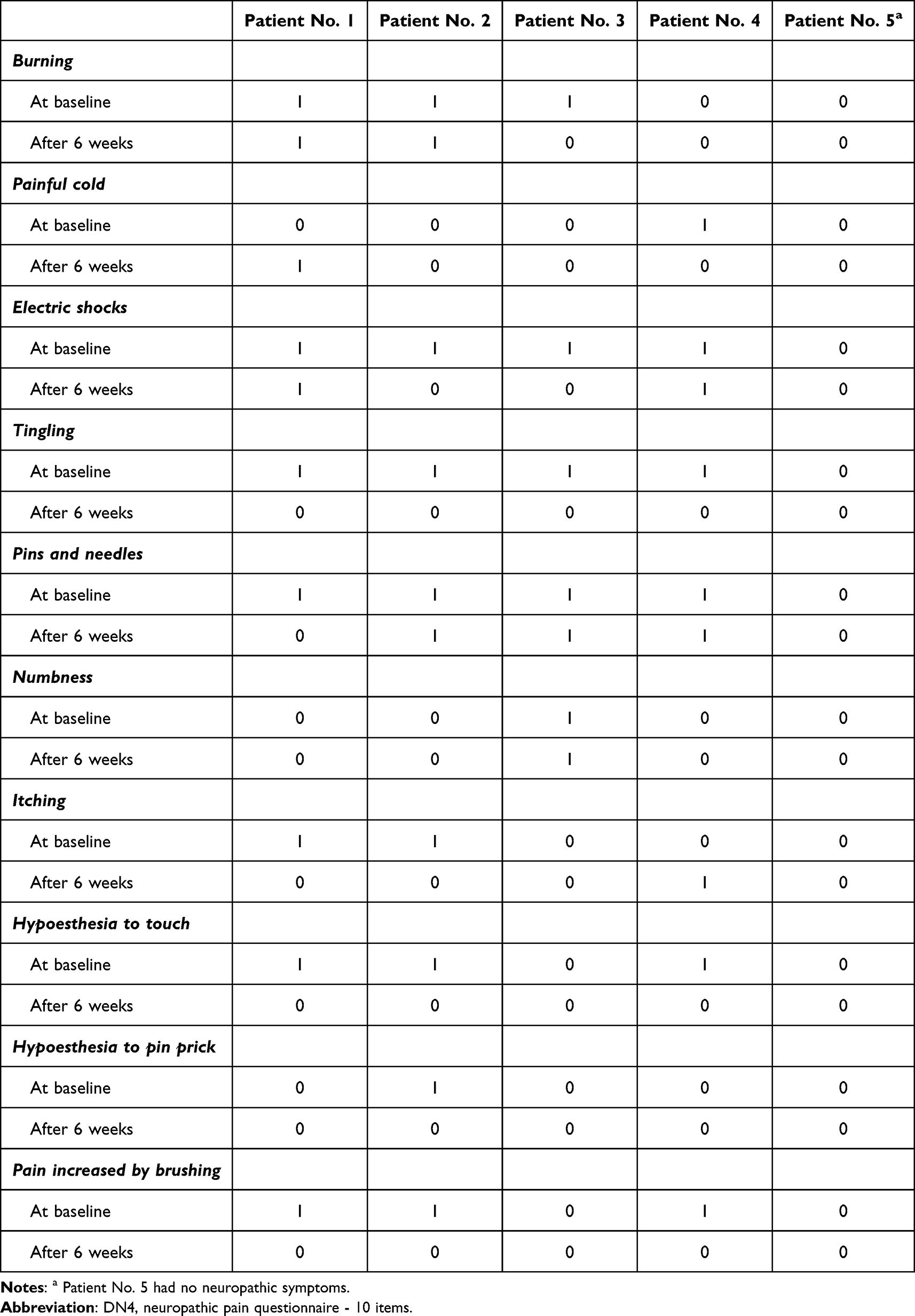 |
Table 4 Changes in the 10-Item Neuropathic Symptom (DN4) Questionnaire After 6 weeks of Ziconotide Rescue Protocol |
Table 5 illustrates the protocol implementation of ziconotide rescue regimen in a patient initially receiving 10 mg/day of IT morphine who developed endocrine dysfunction, tolerance, and constipation, highlighting the potential value of the proposed strategy.
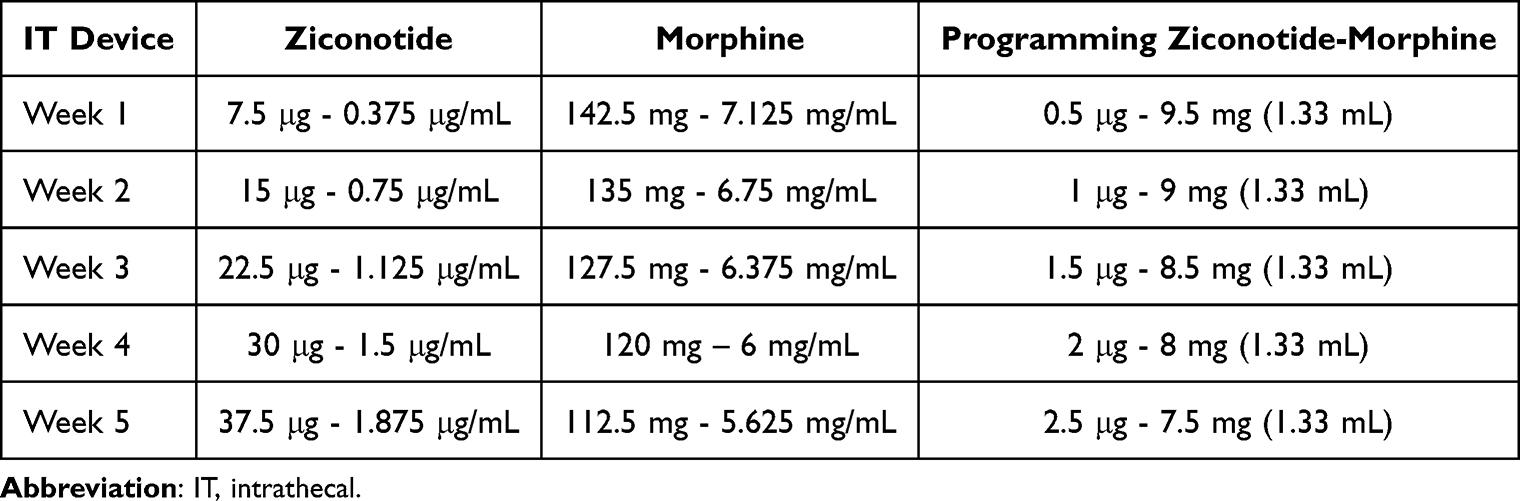 |
Table 5 Five-week Rescue Protocol – Ziconotide Titration and Morphine Reduction |
Discussion
The primary objective of our study was to evaluate whether ziconotide could serve as an effective IT rescue strategy in patients previously treated with morphine, with a focus on pain relief, reduction in neuropathic symptoms, and opioid sparing. In our cohort of patients with severe chronic pain and limited response to morphine based IT regimens, the coadministration of ziconotide led to meaningful improvements across these parameters.
The combination of ziconotide and morphine not only resulted in a substantial reduction in pain intensity and neuropathic symptoms, but also allowed a reduction in daily IT morphine dosage. This reduction in IT morphine was associated with the mitigation of morphine-related adverse events, such as constipation, tolerance, and endocrine dysfunction, which was translated into an overall improvement in patient well-being, as perceived through global improvement measures. These findings directly support the initial study objectives by demonstrating the potential of ziconotide to enhance analgesia and minimize opioid-related toxicity in patients already receiving IT morphine. Despite the lack of statistical significance, the observed effect sizes suggest a strong clinical signal, warranting further evaluation in larger studies.
The rationale behind the synergistic use of ziconotide and morphine lies in their shared target of presynaptic neurons, specifically N-type calcium channels. While morphine acts on both presynaptic and postsynaptic neurons, the addition of ziconotide enhances the blockade of synaptic transmission in cells harboring N-type calcium channels. Therefore, the addition of ziconotide to an IT opioid would result in a more complete blockade of synaptic transmission in cells carrying N-type calcium channels [9] and such a combination may therefore be beneficial in patients with severe chronic pain who do not respond adequately to morphine.
It is well known that neuropathic pain does not respond adequately to opioids. Experimental animal studies have demonstrated downregulation of spinal opioid receptors after nerve injury, providing a plausible explanation for the diminished efficacy of spinal morphine in patients with neuropathic pain. Furthermore, the elevated demand for opioids among patients with neuropathic pain amplifies the probability of experiencing adverse events.12
Ziconotide offers additional clinical advantages over other IT drugs due to its non-opioid mechanism of action, lack of tolerance development, and reversible side-effect profile. Therefore, if patients experience adverse events, they usually disappear within a few days to two weeks by reducing or stopping the dose.13 A gradual titration enables patients to attain higher doses of ziconotide without experiencing adverse events. This advantage positions ziconotide as a valuable therapeutic option for patients with chronic pain with a neuropathic component. In addition, ziconotide has been shown to be effective in patients with refractory neuropathic pain in several studies,14,15 an effect that has been observed in our patients. In our study, no adverse events were reported with ziconotide, and analgesic benefits were preserved even with reduced morphine dosing, further supporting its role as a rescue agent.
Additionally, unlike IT morphine, ziconotide has not shown tolerance as evidenced by long-term studies such as the 12-month PRIZM study.16 During PRIZM study, patients on ziconotide exhibited stable doses or even reductions after 12 months, contrasting the need for escalating doses seen with morphine. In contrast, the adverse events associated with IT morphine, including hyperalgesia, tolerance development, and the potential for granuloma formation, make it a less favorable option. These results were consistent with our patients, as there was no development of tolerance in our cohort, and morphine dosage could be reduced without compromising analgesia.
The introduction of ziconotide in morphine-treated patients is particularly pertinent for younger or reproductive-active patients, as the endocrine adverse events associated with morphine -such as loss of libido, decreased testosterone levels in men, and the risk of osteoporosis, along with hypogonadotropic hypogonadism and amenorrhea or irregular menstrual cycles- are less appealing for individuals in this demographic state. On the contrary, patients receiving ziconotide do not experience these adverse effects, making it the preferred drug for this subgroup or a potential means of reducing morphine doses in these patients.14 However, our current findings do not directly support such recommendations, as all patients in this study were middle-aged or elderly, and given the theoretical benefit of ziconotide in this population, further exploration is necessary in future studies.
Based on the results of our study, low doses and slow titration appear to reduce the occurrence of adverse events. However, the delayed onset of the analgesic effect of ziconotide, coupled with slow tissue penetration and a lag between pharmacokinetics and pharmacodynamics, needs a cautious and patient-centric approach for individualized dosage adjustment.17
Although the differences observed after 6 weeks of the ziconotide rescue protocol in VAS, DN4, and morphine dose did not reach conventional statistical significance (p = 0.06), the effect sizes were substantial. It is likely that with a larger sample size, these differences could achieve statistical significance. These findings indicate a promising clinical trend that warrants further investigation.
Beyond its important impact on pain relief and reduction of adverse events, the addition of ziconotide as an opioid rescue notably improved patients’ overall quality of life, as reflected by their global impression of improvement. Consequently, morphine rescue with ziconotide emerges as a viable therapeutic strategy for patients with refractory neuropathic pain, and individuals susceptible to the diverse adverse events associated with IT morphine.
The main potential limitation of this study is the small sample size, as only 5 patients were included. This limited number restricts the generalizability of the findings and limits the statistical power. While the study used a within-subjects pre-post design -comparing clinical variables before and after the ziconotide rescue protocol- there was no external control group (eg, placebo or alternative treatment), which restricts the ability to attribute changes solely to the intervention. All clinical assessments were self-reported by the patients, which minimizes the risk of observer bias. However, the open-label nature of the study may have introduced reporting or expectation bias, particularly given the subjective nature of the primary endpoints, such as pain intensity and perceived improvement. In addition, factors such as the relatively high cost of ziconotide and the need for careful patient selection may limit its broader use and should be taken into account in clinical decision-making. These limitations should be considered when interpreting the results. Nonetheless, this was a preliminary, feasibility-focused investigation conducted in a real-world clinical setting, and the observed improvements in morphine reduction, pain intensity, and neuropathic symptoms are promising. These results suggest the potential benefits of opioid rescue with ziconotide and warrant further investigation in larger, controlled trials.
Future research should aim to validate these preliminary findings through larger, randomized controlled trials. Comparative studies evaluating different titration strategies for ziconotide, as well as head-to-head trials against other non-opioid analgesics, such as baclofen or clonidine, may help refine treatment protocols. Additionally, long-term studies assessing functional outcomes, patient adherence, and cost-effectiveness would be valuable for informing clinical decision-making.
Conclusions
In summary, intrathecal opioid rescue with ziconotide emerges as a viable therapeutic option for patients with refractory pain with a neuropathic component, and for those who experience adverse events associated with intrathecal morphine. The use of low doses and slow titration of ziconotide may help minimize adverse events while preserving analgesic benefit. Despite the small sample size and preliminary nature of this study, these findings suggest a promising strategy for enhancing pain management in selected patient populations and warrant further investigation in larger studies.
Data Sharing Statement
Data involved in this study are available on reasonable request from the corresponding author.
Acknowledgments
The author thanks Esther Pellicer, paid with the unrestricted grant provided by Esteve Pharmaceuticals SA, for writing assistance of the manuscript and helping with the submission process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Esteve Pharmaceuticals SA, who provided an unrestricted grant. Esteve Pharmaceuticals was not involved in the conception, collection, analysis, and interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brogan SE, Sindt JE, Odell DW, Gulati A, Dupoiron D. Controversies in intrathecal drug delivery for cancer pain. Reg Anesth Pain Med. 2023;48(6):319–325. doi:10.1136/rapm-2022-103770
2. Pope JE, Deer TR, Amirdelfan K, McRoberts WP, Azeem N. The pharmacology of spinal opioids and ziconotide for the treatment of non-cancer pain. Curr Neuropharmacol. 2017;15(2):206–216. doi:10.2174/1570159x14666160210142339
3. Deer TR, Pope JE, Hayek SM, et al. The Polyanalgesic Consensus Conference (PACC): recommendations on Intrathecal Drug Infusion Systems Best Practices and Guidelines. Neuromodulation. 2017;20(2):96–132. doi:10.1111/ner.12538
4. Alicino I, Giglio M, Manca F, Bruno F, Puntillo F. Intrathecal combination of ziconotide and morphine for refractory cancer pain: a rapidly acting and effective choice. Pain. 2012;153(1):245–249. doi:10.1016/j.pain.2011.10.002
5. Deer TR, Pope JE, Hanes MC, McDowell GC. Intrathecal Therapy for Chronic Pain: a Review of Morphine and Ziconotide as Firstline Options. Pain Med. 2019;20(4):784–798. doi:10.1093/pm/pny132
6. Pirec V, Laurito CE, Lu Y, Yeomans DC. The combined effects of N-type calcium channel blockers and morphine on A delta versus C fiber mediated nociception. Anesth Analg. 2001;92(1):239–243. doi:10.1097/00000539-200101000-00046
7. Adler JA, Lotz NM. Intrathecal pain management: a team-based approach. J Pain Res. 2017;10:2565–2575. doi:10.2147/JPR.S142147
8. Diasso PDK, Abou-Kassem D, Nielsen SD, Main KM, Sjøgren P, Kurita GP. Long-term opioid treatment and endocrine measures in chronic non-cancer pain patients. Eur J Pain. 2023;940–951. doi:10.1002/ejp.2136
9. Puntillo F, Giglio M, Preziosa A, et al. Triple Intrathecal Combination Therapy for End-Stage Cancer-Related Refractory Pain: a Prospective Observational Study with Two-Month Follow-Up. Pain Ther. 2020;9(2):783–792. doi:10.1007/s40122-020-00169-1
10. Lambe T, Duarte R, Eldabe R, et al. Ziconotide for the Management of Cancer Pain: a Budget Impact Analysis. Neuromodulation. 2023;26(6):1226–1232. doi:10.1016/j.neurom.2022.08.458
11. Matis G, De Negri P, Dupoiron D, Likar R, Zuidema X, Rasche D. Intrathecal pain management with ziconotide: time for consensus? Brain Behav. 2021;1(Suppl 1):e02055. doi:10.1002/brb3.2055
12. Kim JY, Lee YH, Kim JY, Lee HH, Kim YH. Intrathecal drug delivery to treat intractable neuropathic pain following Sjögren’s syndrome-induced transverse myelitis: a case report. Medicine. 2021;100(22):e26141. doi:10.1097/MD.0000000000026141
13. Staats PS, Luthardt F, Shipley J, Jackson C, Fischer K. Long-term intrathecal ziconotide therapy: a case study and discussion. Neuromodulation. 2001;4(3):121–126. doi:10.1046/j.1525-1403.2001.00121.x
14. Brookes ME, Eldabe S, Batterham A. Ziconotide Monotherapy: a Systematic Review of Randomised Controlled Trials. Curr Neuropharmacol. 2017;15(2):217–231. doi:10.2174/1570159x14666160210142056
15. Viswanath O, Urits I, Burns J, et al. Central Neuropathic Mechanisms in Pain Signaling Pathways: current Evidence and Recommendations. Adv Ther. 2020;37(5):1946–1959. doi:10.1007/s12325-020-01334-w
16. Deer T, Rauck RL, Kim P, et al. Effectiveness and Safety of Intrathecal Ziconotide: interim Analysis of the Patient Registry of Intrathecal Ziconotide Management (PRIZM). Pain Pract. 2018;18(2):230–238. doi:10.1111/papr.12599
17. McDowell II GC, Pope JE. Intrathecal Ziconotide: dosing and Administration Strategies in Patients With Refractory Chronic Pain. Neuromodulation. 2016;19(5):522–532. doi:10.1111/ner.12392
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.