Back to Journals » Clinical Interventions in Aging » Volume 18
Can We Slow Down Biological Age Progression? Study Protocol for the proBNPage Reduction (PBAR) Randomized, Double-Blind, Placebo-Controlled Trial (Effects of 4 “Anti-Aging” Food Supplements in Healthy Older Adults)
Authors Muscari A ![]() , Forti P, Brizi M, Magalotti D, Capelli E, Potì S, Piro F, Pandolfi P, Perlangeli V, Ramazzotti E, Barbara G
, Forti P, Brizi M, Magalotti D, Capelli E, Potì S, Piro F, Pandolfi P, Perlangeli V, Ramazzotti E, Barbara G
Received 22 May 2023
Accepted for publication 7 August 2023
Published 27 October 2023 Volume 2023:18 Pages 1813—1825
DOI https://doi.org/10.2147/CIA.S422371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Antonio Muscari,1 Paola Forti,1,2 Mara Brizi,2 Donatella Magalotti,2 Eleonora Capelli,2 Simona Potì,2 Filomena Piro,3 Paolo Pandolfi,4 Vincenza Perlangeli,4 Eric Ramazzotti,5 Giovanni Barbara1,2 On behalf of PBAR Study Group
1Department of Medical and Surgical Sciences, University of Bologna, Bologna, Italy; 2Medical-Surgical Department of Digestive, Hepatic and Endocrine-Metabolic Diseases, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy; 3Pharmaceutical Department, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy; 4Epidemiological and Health Promotion Unit, Department of Public Health, AUSL Bologna, Bologna, Italy; 5LUM Metropolitan Laboratory, AUSL Bologna, Bologna, Italy
Correspondence: Antonio Muscari, Department of Medical and Surgical Sciences, S. Orsola-Malpighi Hospital, Via Albertoni, 15, Bologna, 40138, Italy, Tel +39-347-1126386, Fax +39-051-6362210, Email [email protected]
Purpose: The availability of a simple and reliable marker of biological age might allow an acceleration of the research in the field of longevity extension. Previous studies suggest that this marker might be the N-terminal of B-type natriuretic peptide precursor (NT-proBNP), from which proBNPage, a biological age surrogate, can be calculated. Objectives of the study: 1) To fine-tune the method of proBNPage progression assessment and 2) To establish whether 4 “anti-aging” treatments, which provided promising results in previous studies, can modify proBNPage progression.
Patients and Methods: This is a double-blind randomized placebo-controlled clinical trial on 120 adults aged 65– 80 years, free of cardiovascular diseases. Participants will be randomized into 3 groups: A) Coenzyme Q10 100 mg bid + Selenium 100 mcg; B) Resveratrol 350 mg bid + TA-65 (Astragalus Membranaceus extract) 100U; C) Placebo-1 bid + Placebo-2. They will be followed for 2 years and checked 8 times, to assess both proBNPage progression and treatment safety. Secondary variables (handgrip strength, aerobic capacity at the step test and quality of life) will also be assessed. Primary outcome will be the demonstration of significant changes of proBNPage, compared to baseline, in the 3 groups at 6, 12, 18 and 24 months. Secondary outcome will be the demonstration of similar changes of secondary variables. Statistical analyses will be mainly performed by repeated measures ANOVA (both according to intention to treat and per protocol) and paired t tests. The study was approved by the Ethics Committee Area Vasta Emilia Centro, Emilia-Romagna Region, ID: 64/2022/Sper/AOUBo. Trial registration: ClinicalTrials.gov, NCT05500742.
Conclusion: The use of proBNPage as a surrogate of biological age may prove an easy method to select anti-aging treatments worthy of further, more complex assessments.
Keywords: anti-aging treatments, biological age, food supplements, longevity, NT-proBNP, study protocol, randomized clinical trial
Introduction
Despite the wide literature concerning anti-aging treatments, so far, no definite evidence of efficacy has been obtained in humans. The main problem is that human life is relatively long so that, to assess the effect of any treatment on longevity, similarly long studies are needed. In addition, to demonstrate significant reductions in mortality, large samples are needed too. Thus, even though several promising treatments have been found in animal models, convincing evidence of efficacy in humans has not come yet.
In an attempt to overcome these difficulties, in recent years several indicators of biological age have been proposed.1 Biological age may be defined as a measure, more reliable than chronological age, of how close to death an individual is. If such an indicator were available, assessing the efficacy of possible treatments would be relatively easy: few years of follow-up in relatively small groups might be sufficient to ascertain the arrest or even the inversion of the rise of the indicator, rather than many years on large samples to demonstrate a lower mortality in the treated group than in the placebo group.
The main indicators of biological age so far proposed are as follows: telomere length in leukocytes,2 DNA methylation (or “epigenetic clock”),3–5 several interpretations of metabolome6 and proteome7 in serum, clinical-anamnestic composite indices of frailty8,9 and composite indices of laboratory variables.10,11 However, despite this plenty of potential indicators, none of them is routinely used in laboratories, either because of the difficulty of affecting their values or due to the complexity of measurements, or because of a non-demonstrated superiority compared to chronological age, or for all these causes together.
In 2021, we proposed a new simple method to obtain a surrogate of biological age (“proBNPage”), starting from the single laboratory variable NT-proBNP (the N-terminal fragment of B-type natriuretic peptide precursor).12,13 NT-proBNP is easily measurable in most laboratories. It is commonly used as a marker of heart failure, as it is released from the ventricular and atrial myocardium undergoing mechanical or ischemic stress. In addition, it is a good indicator of the risk of death even in subjects without cardiovascular diseases14,15 and, in particular, we have shown that NT-proBNP is associated with cardiovascular16 and all-cause12 mortality more strongly than chronological age in older adults. Several studies (both cross-sectional and longitudinal) have shown that this marker progressively increases with age12,17–19 and that its values are higher in women.12,17,20 In addition, NT-proBNP is correlated with chronological age more strongly than all the main laboratory variables that had previously been proposed as biomarkers of biological age (as shown by us12 and also by others21). Thus, starting from the equations of the regression lines of chronological age with the natural logarithm of NT-proBNP in a large sample of older adults (with the only exclusions of subjects with atrial fibrillation and heart failure) we obtained two simple formulas, one for each sex, which allow the calculation of a “proBNPage”, in years, from the serum concentration of NT-proBNP.12
Among the main categories of possible anti-aging treatments, three have provided promising results in experimental studies and, for some aspects, even in humans: antioxidants,22–24 telomerase activators25,26 and inhibitors of the Target of Rapamycin (TOR) enzyme system.27–30 To test, for the first time, the possible practical use of proBNPage, we have designed a longitudinal study aimed at assessing the progression of proBNPage in small groups of older adults, together with the effects induced on it by 4 food supplements, which are representative of the three above categories.
Methods
Study Objectives
- Primary objective: To describe the spontaneous longitudinal course of proBNPage in the placebo group, in order to find the parameters (minimum time to obtain a significant increment, increment size and variability) useful to design future studies on anti-aging treatments.
- Secondary objective: To ascertain whether any of the food supplements proposed can favor a non-significant increase (or even a reduction) of proBNPage, compared to the placebo group, over the period of study.
Study Design and Main Reference Data
This is a double-blind clinical trial with stratified randomization into 3 parallel groups (one placebo group and two food supplement-treated groups) (Figure 1).
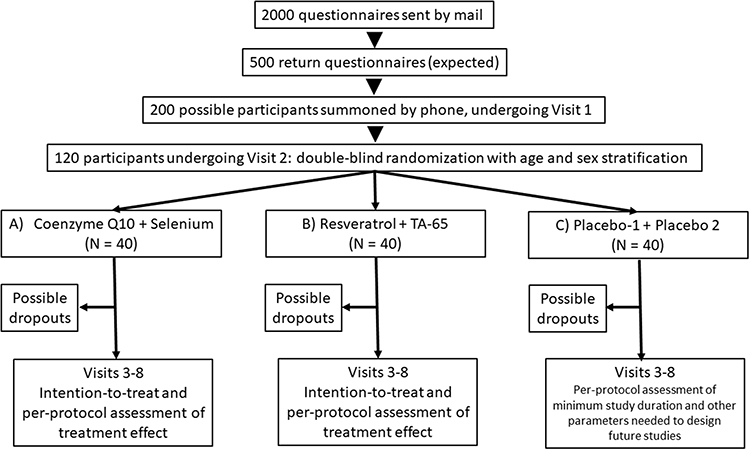 |
Figure 1 Schematic representation of study design. |
Protocol version: Version 2 – February 4, 2022.
Ethics Committee Approval
Comitato Etico di Area Vasta Emilia Centro della Regione Emilia-Romagna (CE-AVEC), ID: 64/2022/Sper/AOUBo, March 16, 2022 (see Supplement for the List of Documents Submitted to the Ethics Committee). The study will be conducted in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Trial registration: ClinicaTrials.gov (US NIH), ID: NCT05500742, August 19, 2022.
Recruitment: Start November 2, 2022–End November 15, 2022.
End of study (expected last visit): November 30, 2024.
The SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials)31 checklist was followed in the preparation of this paper.
Sample Size and Study Duration Determination
To establish the minimum sample size, so that results may be obtained with a probability of first type error <0.05 and a power of 0.80, a few preliminary parameters are needed: standard deviation of the studied variable (proBNPage) in the population, standard deviation of the predicted effect in a longitudinal study, and correlation coefficient “r” between baseline values and post-treatment values. So far, no longitudinal study on proBNPage has been performed. Thus, this information is not available, and has been approximated using the data collected by us in a previous cross-sectional study12 (Table 1).
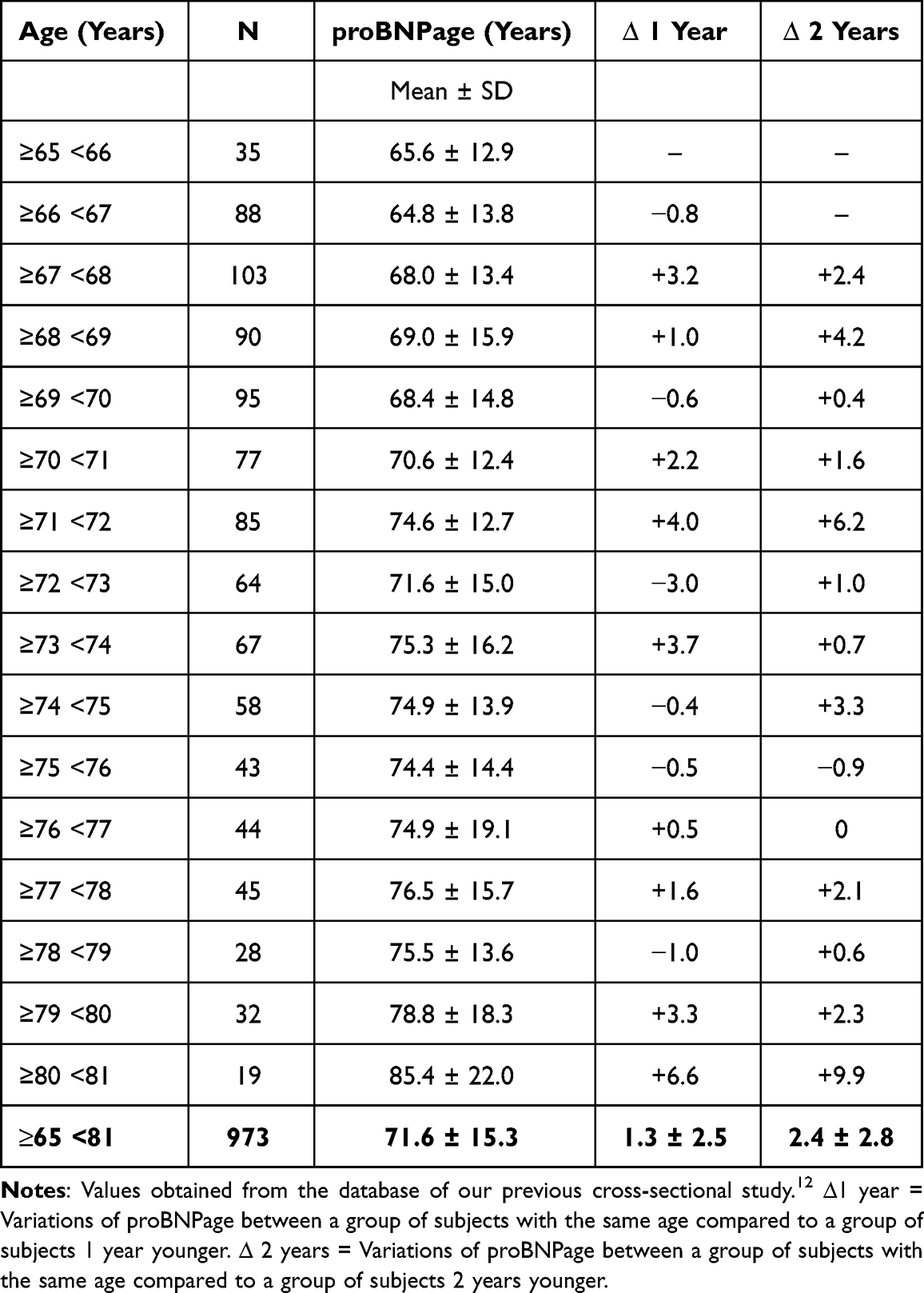 |
Table 1 Mean Course of proBNPage in Relation to Chronological Age |
Considering the variations of proBNPage between a group of subjects with the same age and a group of subjects 1 year older, in some cases, reductions were obtained (instead of the expected increases). Thus, if treatments were administered for 1 year only, casual reductions of proBNPage might occur, leading to erroneous conclusions of favorable effects of the treatments. Considering instead the variations of proBNPage between each age group and the group 2 years older, only in 1 case over 14 a decrease in proBNPage occurred. From this observation, we decided to prolong the study for 2 years. However, it is possible that during the proposed longitudinal study we could even conclude that shorter intervals are sufficient.
The mean effect, ie the mean increase in proBNPage every two years of chronological age, was 2.4 ± 2.8 years. In addition, the 14 proBNPage mean values were related to the 14 proBNPage mean values obtained after 2 years of age, and the correlation coefficient of these two series was 0.791. In this way, the starting parameters necessary for sample size calculation were obtained.
Sample size calculation was set on the basis of analysis of variance for repeated measures, using WebPower software.32 For 3 study groups (1 placebo + 2 groups with food supplements) and 2 time assessments (each time vs baseline), the sample size of each group depends on the main interest of the study: changes due to time (“within” groups), differences between treatments and placebo (“between” groups), or both assessments together (“between-within interaction”).
Within: N = 8; Between: N = 50; Between-Within interaction: N = 9.
The main interests of our study concern the “within” and “between-within” assessments, which would allow a minimum sample of 9 × 3 = 27 subjects. To account for probable dropouts and possible greater variability than expected and to allow possible subgroup analysis, we decided to multiply this estimate by 4, thus reaching a sample size of 40 × 3 = 120 subjects.
Sample Selection
One hundred and twenty older subjects of both sexes will be selected. They should be substantially healthy people, because the study is aimed at ascertaining the possibility to use proBNPage to monitor aging progression independently of the presence of pathologies, especially cardiovascular diseases, which might alter the rate of NT-proBNP release. The sample will be the result of 3 consecutive selection procedures.
First Selection
Names and addresses of potential participants will be obtained from lists provided by the local Department of Public Health, including subjects aged 65–80 years, living in Bologna near the S. Orsola-Malpighi University Hospital, taking no more than 4 drugs a day and without recent (<3 years) hospital admissions. By random choice, 2000 subjects (1000 men and 1000 women, 62/63 for each of the 16 age classes for each sex) with the above characteristics will receive a letter with the invitation to participate, including a synthetic description of trial design, together with a 6-page questionnaire for preliminary health status assessment. The questionnaire will contain questions concerning demographic information, risk factors, previous and present cardiovascular and non-cardiovascular diseases, muscle/joint pain, falls and medications taken. The Physical Activity Scale for the Elderly (PASE)33 and the Euro QoL 5-Dimension quality of life assessment34 will also be included in the questionnaire. For acceptation, the volunteers will return the compiled questionnaire by mail in a pre-stamped envelope or by e-mail.
Second Selection
Five hundred people (25%) are expected to respond and, according to the information provided with the questionnaires, 200 of them will be selected by the steering committee (see inclusion and exclusion criteria, Table 2) and summoned by phone for the first visit. Before the visit, they will also receive a copy of the informative documentation to be subsequently signed.
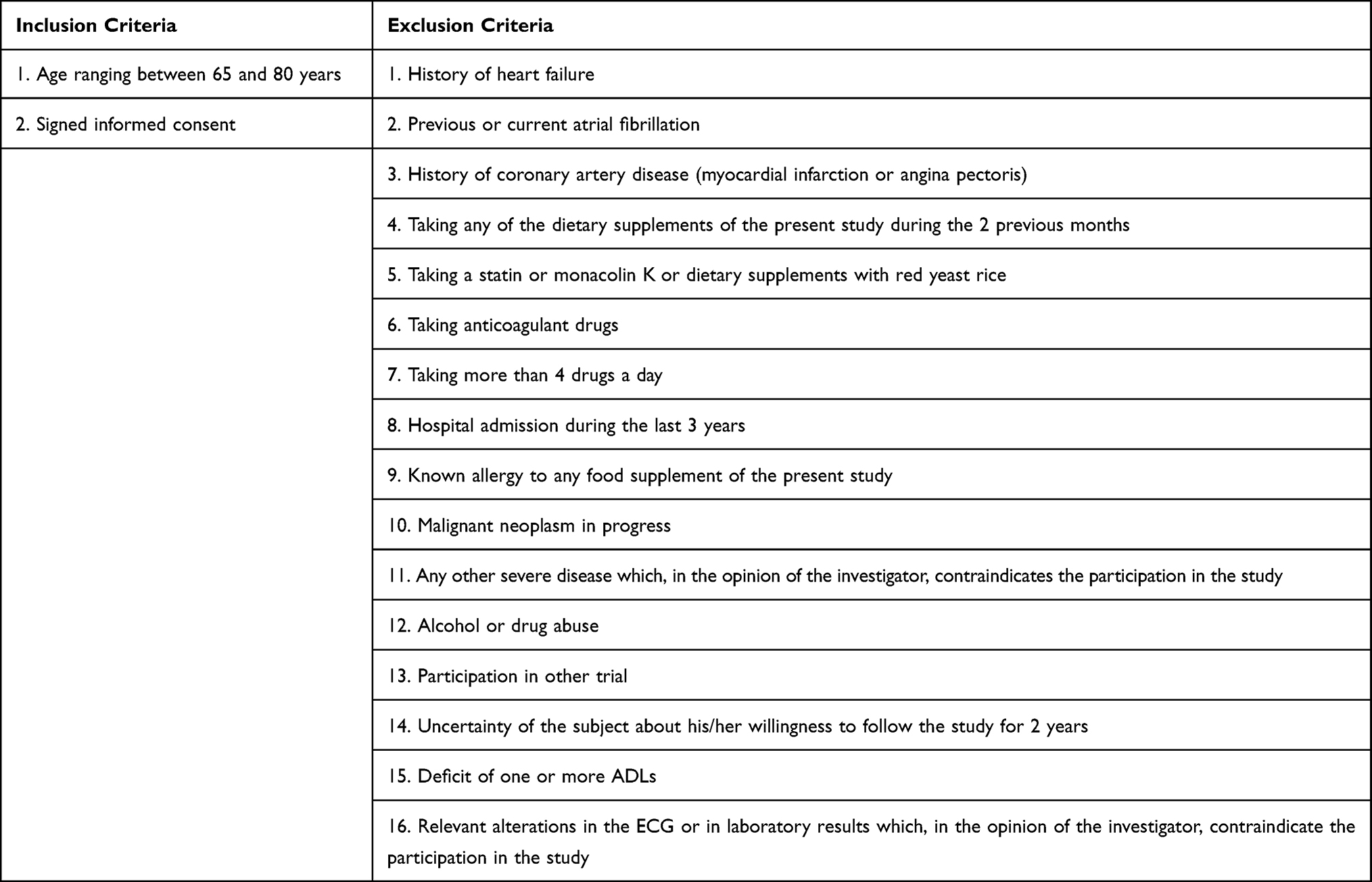 |
Table 2 Inclusion and Exclusion Criteria |
Third Selection
During Visit 1 (Screening assessment), after further explanation of the study by the investigators and after signing the informed consent (an additional signature will also be requested for withdrawal and storage of serum samples for possible future determinations), the subjects willing to participate will undergo fasting venous blood sampling for routine laboratory determinations, anamnestic investigation (basal activities of daily living (ADL),35 instrumental activities of daily living (IADL)36 and comparison of the information provided with the questionnaire with all available documentation), medical examination (with weight, height, 2 measurements of blood pressure by automatic sphygmomanometer and finger oxygen saturation), and ECG. Taking into account all these items of information, according to the inclusion and exclusion criteria (Table 2), 60 men and 60 women will be selected by the steering committee to be randomized. Taking a statin is an exclusion criterion because statins could lower coenzyme Q10 levels37 and mildly activate telomerase.38 The 120 selected patients will be summoned by phone for the second visit.
Study Procedures
During Visit 2 (Baseline assessment) the selected subjects will undergo venous blood sampling for NT-proBNP measurement. This will be performed on whole blood by fluorescence immune assay (Quidel Cardiovascular Inc., San Diego, USA). The following functional tests will also be performed: 1) Step test (time in seconds needed to ascend and descend 2 steps 20 times),39 2) Handgrip strength (strength measured in Kg, the highest of 2 measurements), 3) Euro QoL-5D questionnaire (quality of life).34
For stratified randomization, participants will be subdivided into 4 strata according to the following characteristics:
- 30 women with age < the median age of women (“young” women)
- 30 women with age ≥ the median age of women (“old” women)
- 30 men with age < the median age of men (“young” men)
- 30 men with age ≥ the median age of men (“old” men)
Using randomization lists, computer-generated by our hospital Research and Innovation Unit and kept concealed for the investigators, the subjects belonging to each stratum will be equally distributed among the 3 treatment groups (10 subjects of each stratum in each group), so that relevant random imbalances of age and sex among groups should be avoided. In particular, bags progressively numbered from 001 to 120 (001–030 “young” women stratum, 031–060 “old” women stratum, 061–090 “young” men stratum, 091–120 “old” men stratum), prepared by our hospital pharmacy according to the above randomization lists and containing boxes of treatment for 6 months, will be sequentially handed by the investigator (A.M.) to participants according to the stratum they belong to. Besides investigators, also trial participants will be blinded about treatment allocation. Unblinding will occur at the end of the study, after closure of the database. Emergency unblinding by the pharmacy is also admitted for single participants who will interrupt the trial because of serious adverse events.
The subsequent assessments will be Visit 3: 14 days, Visit 4: 3 months, Visit 5: 6 months, Visit 6: 12 months, Visit 7: 18 months, Visit 8: 24 months, with the following scheduled activities (Figure 2):
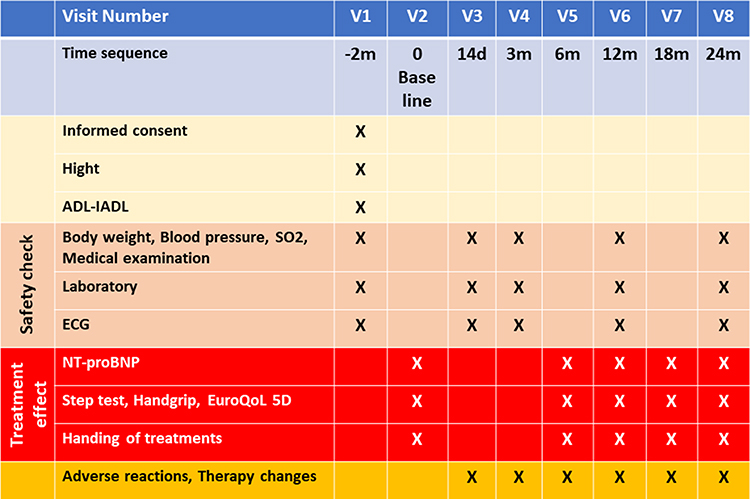 |
Figure 2 Schedule of study activities. |
Possible protocol amendments will be submitted to the Ethics Committee, reported in the ClinicalTrials.gov registry and possibly communicated to participants.
Interventions
- Group A: Coenzyme Q10 (CoQ10) 100 mg (Q10 Gold, Pharma Nord ApS, Vejle, Denmark), 1 capsule bid + Selenium 100 mcg (SelenoPrecise, Pharma Nord) 1 tablet in the evening. This combination was chosen because it was previously found to reduce cardiovascular mortality in older adults.40
- Group B: Resveratrol 350 mg (NOW Foods, Bloomingdale, IL, USA) 1 capsule bid + TA-65,100 U (T.A. Sciences, New York, NY, USA) 1 capsule in the evening. This combination was chosen because resveratrol, a powerful antioxidant, also seems to be able to activate telomerase,41,42 thus enhancing the action of TA-65.43
- Group C: Placebo-1 (externally identical to the coenzyme Q10 capsule) 1 capsule bid + Placebo-2 (externally identical to Selenium tablet) 1 tablet in the evening, both provided by Pharma Nord.
To ensure blindness, capsules and tablets will be inserted by our pharmacy into boxes that are indistinguishable from the outside. In particular, every 6 months each participant will receive a bag containing one box with “Treatment 1” (to be taken twice a day) and one box with “Treatment 2” (to be taken once a day).
Primary Variable to Assess Treatment Effect
The primary variable to assess the effect of treatments is proBNPage. According to our previous study,12 proBNPage will be calculated separately for the 2 sexes, starting from NT-proBNP, with the following formulas:
- proBNPagemen = [ln(NT-proBNP)+1.2958]/0.0827
- proBNPagewomen = [ln(NT-proBNP)-1.5258]/0.0478
After these calculations, proBNPage will be treated as a single variable, independent of sex.
Secondary Variables to Assess Treatment Effect
To assess the possible effect of treatments on aging progression, the following secondary variables will also be utilized:
Primary and Secondary Outcomes
Primary outcome will be the demonstration of significant or non-significant changes of proBNPage, compared to baseline, in the 3 treatment groups at 6, 12, 18 and 24 months.
Secondary outcome will be the demonstration of significant or non-significant changes of secondary variables, compared to baseline, in the 3 treatment groups at 6, 12, 18 and 24 months.
Safety Variables
Management of Adverse Events
The possible appearance of suspected adverse events will be actively investigated during all visits, and participants will be allowed to report them at any time by phone or email. Suspected adverse events will be assessed, managed and reported in the database by the steering committee, and their frequency will be documented at the end of the study. Serious adverse events will be a cause of participant exclusion and will be promptly reported to the sponsor.
Statistical Analysis
ProBNPage is normally distributed,12 and its statistical assessment can be performed with parametric tests. The minimum time needed to obtain a significant increment of proBNPage from baseline will be established in the subjects of the placebo group whose proBNPage value at each tested time will be available. For this purpose, Student’s t test for paired data will be used.
The assessment of the possible effects of the treatments on the progression of proBNPage will be performed both according to intention to treat (in all randomized patients) and per protocol (only in the patients with proBNPage available at the tested time). In the intention-to-treat analysis, missing values will be imputed with the multiple imputation method. The possible presence of proBNPage changes within and between groups will be initially tested by repeated measures analysis of variance, with reference to the “between-within” interaction. Then, the assessments on “within” time changes will be performed, in each group, by t-tests for paired data. The differences among baseline values will be tested by analysis of variance (ANOVA). Finally, if the number of participants in subgroups will be ≥ the minimum expected (see Sample size determination), the assessments will be repeated separately in subgroups with the following characteristics: 1) Men/Women; 2) Younger/Older (with respect to the median ages in the 2 sexes); 3) Difference between baseline proBNPage and chronological age over/under the median difference.
Possible changes and differences for secondary variables (step test, handgrip strength and Euro QoL 5D visual analog scale) will be sought in the same way described for proBNPage (after normalization in case of non-gaussian distribution).
Finally, baseline values of safety variables will be compared among groups to detect possible random imbalances. In addition, possible important changes of safety variables will be promptly reported to participants.
Two-tailed tests will be performed throughout to demonstrate superiority of food supplement compared to placebo in arresting outcome variables’ progression, and P values <0.05 will be considered significant.
Statistical tests will be performed with SPSS software v. 27 (IBM, Armonk, New York) and R-based software (StatPlus, AnalystSoft Inc, Walnut, California).
Data Management
All data will be collected in strictly pseudonym form (each subject will only be identified by a progressive 3-digit code) and will be recorded in a Research Electronic Data Capture (REDCap) database,45 under the administration of the Innovation and Research Unit of our hospital. In the database, there will be an automatic range check for data input. Personal information about participants will be kept strictly confidential by the investigators. Investigators, sponsor and all those authorized by the investigators (upon reasonable request) will have access to the final dataset. No data monitoring committee has been created for this spontaneous, non-profit, monocentric study. However, auditing procedures to verify the correct application of the protocol may be performed by delegates of the Ethics Committee or of Regulatory Authorities. No interim analyses are planned.
Discussion
With this study, we will try to define a method that may allow to select, in the simplest possible way, anti-aging treatments deserving to be confirmed by large mortality trials. Our hope is that this preliminary assessment of treatments may be based on small samples of subjects, to be followed for relatively short periods of time. At the end of the present longitudinal study, we will understand whether the observation period can be contained within 2 years, and we will obtain the statistical parameters needed to establish the sample size of future similar evaluations, parameters that will be more precise compared to the preliminary estimates obtained by us from a previous cross-sectional study.
For the choice of treatments, in the present study we have sought the best compromise among available scientific evidence, safety and ease of obtaining the substances on the market.
- CoQ10 is a powerful antioxidant that exerts fundamental functions for cell respiration and energy production. Aging and statins decrease its levels.37,46 Its supplementation reduced cardiovascular and total mortality in heart failure patients.47 In addition, at the dose of 100 mg bid, together with selenium 200 mcg, it reduced cardiovascular mortality in older adults.40 CoQ10 is practically free of harmful effects.48 Possible interactions with warfarin were reported49 but were not confirmed.50
- Selenoproteins contribute to the antioxidant systems of our organism. Selenium blood levels and selenium intake with diet are inversely associated with mortality.51,52 As previously highlighted, together with CoQ10 it reduced mortality in older adults.40 In subjects less than 65 years old, high doses (300 mcg/day) have been reported to be associated with an increase in mortality.53 In Italy, a maximum dose of 100 mcg/day is allowed.
- Resveratrol has powerful antioxidant and anti-inflammatory effects54 and, in addition, it seems to be able to activate telomerase41,42 and inhibit the TOR system.55,56 Beneficial effects have been documented on insulin resistance, inflammation and blood pressure, as well as a possible anti-cancer action.57,58 Resveratrol prolonged life in Drosophila, nematodes, killifish and obese or ill mice,59–61 but it is not known whether it can influence longevity in humans. At high doses (≥1000 mg/day) adverse effects (especially gastrointestinal) have been reported.61,62 However, doses should be high enough, because resveratrol has a low bio-availability.63,64
- TA-65 is a derivative of Astragalus Membranaceus root. In humans, TA-65 has been shown to favor the elongation of telomeres in chromosomes,43 which could favor longevity,26 and showed favorable effects on age-related macular degeneration65 and on blood parameters in patients with metabolic syndrome.66 In healthy volunteers, the 100U dose had better effects than the 500U dose, in reducing the number of senescent T lymphocytes.67 TA-65 obtained the GRAS certification (Generally Recognized As Safe).
Strengths – If small samples and short observation periods were sufficient to demonstrate significant effects on proBNPage, this would be an advantage compared to traditional studies on human longevity. Another advantage would be the use of paired tests (to demonstrate significant, or non-significant, proBNPage changes in each treatment group) with respect to unpaired tests (to compare mortality between different groups): in fact, paired tests are known to be more sensitive and powerful than unpaired tests. Finally, compared to other more complex methods to estimate biological age,2–7 proBNPage is based on NT-proBNP measurement, an easily performed method that is already available in most laboratories.
Limitations – NT-proBNP is released by the heart, so, strictly speaking, proBNPage can be more properly considered an estimate of the biological age of the heart. Although the latter is influenced by the general aging of the organism and probably can in turn influence it, some organs or body structures can undergo accelerated aging processes, which may interfere with longevity independently of the heart. Similarly, the treatments to test might have significant effects on aging, without having the ability to modify NT-proBNP release. In addition, in the presence of heart pathologies, NT-proBNP release increases, which can lead to excessively pessimistic estimates of the biological age of the whole individual. This suggests performing a selection of the subjects to include in the sample, with the intention to follow the progression of biological age in the absence of factors that may distort its estimate. However, the utilization of selected samples might limit the generalizability of the results to the whole population. Finally, if a treatment has the ability to limit NT-proBNP release from the heart, this does not automatically ensure that mortality will be reduced. At the end, this demonstration, as well as the generalization of results, will only come from large-dimensional and long-duration studies. However, the relevant time and economic commitment that these studies require might be justified by the previous demonstration, in humans, of a favorable effect on proBNPage.
Conclusions
The use of proBNPage as an indicator of biological age may provide several advantages in the selection of anti-aging treatments but could also prove ineffective for a series of reasons. With the present study, we will try to clarify some of these uncertainties, assessing 4 of the most promising, presently available, anti-aging treatments.
Acknowledgments
This study is made possible thanks to the generous support of the manufacturers of the food supplements, who will donate their products: Pharma Nord (coenzyme Q10, selenium, placebo 1 and 2), NOW Foods (resveratrol) and TA Sciences (TA-65). We also thank Quidel for donating part of the reagents for NT-proBNP measurements. Finally, we are indebted to Professor Marco Zoli, who contributed with advice and financial support before his retirement, with Sabrina Fontana, for her logistic support, and with the staff of the Research and Innovation Unit of the IRCCS Azienda Ospedaliero-Universitaria di Bologna, for continuous organizational help.
The authors present this paper on behalf of the PBAR study group: Steering Committee (the Investigators): Antonio Muscari, Paola Forti, Mara Brizi, Donatella Magalotti, Giovanni Barbara. Public Health Department: Vincenza Perlangeli, Paolo Pandolfi. Nursing staff: Eleonora Capelli, Sabrina Fontana, Manuel Cadario, Barbara Ciuffi, Alessandra Maselli, Giuseppe Smiriglio, Pasqualina Vitali, Simona Potì. Pharmacy: Filomena Piro, Giulia Piazza, Michele Meneghello, Alessandra Stancari. Schools of Geriatrics and Internal Medicine: Vittorio Dugato, Pietro Dalmonte, Lucia Bosi, Lucia Biondi, Giulia Perlini, Giovanni B. Berti, Irene Ghillani, Sara Sabatini, Elena Denicolò, Maria D’Errico, Claudia Asperti, Alessandra Mollicone, Giulia Dei, Marco Domenicali. Statistics and database support: Helena Policardi, Dino Gibertoni. Laboratory: Eric Ramazzotti, Rita Mancini.
Funding
This spontaneous non-profit study is supported by Now Foods, Pharma Nord, TA Sciences and Quidel, who will donate their products. It is funded by grants from the Italian Ministry of University and Research (MUR). Sponsor of the study is IRCCS Azienda Ospedaliero-Universitaria di Bologna, via Albertoni 15, 40138 Bologna, Italy. Neither funder nor sponsor nor pharma companies had or will have any role in study design, collection, analysis and interpretation of data, writing the report and the decision to submit the report for publication. The sponsor is the administrator for the REDCap database.
Disclosure
Professor Giovanni Barbara reports personal fees from Aboca, AB Biotics, Agave, Alfasigma, Allergan, Arena, AstraZeneca, Bayer, Biocodex, Bromatech, Cadigroup, Diadema, GE Healthcare, Falk Pharma, IMA, Mayoly, Malesci, Nestlè, Parmalat, Sanofi, Schwabe Pharma, Sofar, Yakult, and Zespri, outside the submitted work. In addition, Professor Giovanni Barbara has a patent Metodo e kit per la diagnosi della sensibilita’ al glutine non associata alla celiachia with paid royalties. The authors report no other conflicts of interest in this work.
References
1. Lohman T, Bains G, Berk L, Lohman E. Predictors of biological age: the implications for wellness and aging research. Gerontol Geriatr Med. 2021;7:23337214211046419. doi:10.1177/23337214211046419
2. Sanders JL, Newman AB. Telomere length in epidemiology: a biomarker of aging, age-related disease, both, or neither? Epidemiol Rev. 2013;35:112–131.
3. Hannum G, Guinney J, Zhao L, et al. Genome-wide methylation profiles reveal quantitative views of human aging rates. Mol Cell. 2013;49:359–367. doi:10.1016/j.molcel.2012.10.016
4. Horvath S. DNA methylation age of human tissues and cell types. Genome Biol. 2013;14(10):R115. doi:10.1186/gb-2013-14-10-r115
5. Perna L, Zhang Y, Mons U, Holleczek B, Saum K-U, Brenner H. Epigenetic age acceleration predicts cancer, cardiovascular, and all-cause mortality in a German case cohort. Clin Epigenetics. 2016;8(1):64. doi:10.1186/s13148-016-0228-z
6. Johnson LC, Parker K, Aguirre BF, et al. The plasma metabolome as a predictor of biological aging in humans. Geroscience. 2019;41:895–906. doi:10.1007/s11357-019-00123-w
7. Menni C, Kiddle SJ, Mangino M, et al. Circulating proteomic signatures of chronological age. J Gerontol a Biol Sci Med Sci. 2015;70:809–816. doi:10.1093/gerona/glu121
8. Rockwood K, Blodgett JM, Theou O, et al. A frailty index based on deficit accumulation quantifies mortality risk in humans and in mice. Sci Rep. 2017;7:43068. doi:10.1038/srep43068
9. Kim S, Jazwinski SM. Quantitative measures of healthy aging and biological age. Healthy Aging Res. 2015;4:26. doi:10.12715/har.2015.4.26
10. Liu Z, Kuo PL, Horvath S, Crimmins E, Ferrucci L, Levine M. A new aging measure captures morbidity and mortality risk across diverse subpopulations from NHANES IV: a cohort study. PLoS Med. 2018;15:e1002718. doi:10.1371/journal.pmed.1002718
11. Waziry R, Gras L, Sedaghat S, et al. Quantification of biological age as a determinant of age-related diseases in the Rotterdam Study: a structural equation modeling approach. Eur J Epidemiol. 2019;34:793–799. doi:10.1007/s10654-019-00497-3
12. Muscari A, Bianchi G, Forti P, Magalotti D, Pandolfi P, Zoli M; Pianoro Study Group. N-terminal pro B-type natriuretic peptide (NT-proBNP): a possible surrogate of biological age in the elderly people. Geroscience. 2021;43:845–857. doi:10.1007/s11357-020-00249-2
13. Muscari A, Bianchi G, Forti P, Magalotti D, Pandolfi P, Zolia M; Pianoro Study Group. The association of proBNPage with manifestations of age-related cardiovascular, physical and psychological impairment in community dwelling older adults. Geroscience. 2021;43:2087–2100. doi:10.1007/s11357-021-00381-7
14. Wang TJ, Larson MG, Levy D, et al. Plasma natriuretic peptide levels and the risk of cardiovascular events and death. N Engl J Med. 2004;350:655–663. doi:10.1056/NEJMoa031994
15. McKie PM, Rodeheffer RJ, Cataliotti A, et al. Amino-terminal pro-B-type natriuretic peptide and B-type natriuretic peptide: biomarkers for mortality in a large community-based cohort free of heart failure. Hypertension. 2006;47:874–880.
16. Muscari A, Bianchi G, Forti P, et al. A comparison of risk factors as predictors of cardiovascular and non-cardiovascular mortality in the elderly people--relevance of N-terminal pro-B-type natriuretic peptide and low systolic blood pressure. Int J Clin Pract. 2013;67:1182–1191. doi:10.1111/ijcp.12195
17. Redfield MM, Rodeheffer RJ, Jacobsen SJ, Mahoney DW, Bailey KR, Burnett JC. Plasma brain natriuretic peptide concentration: impact of age and gender. J Am Coll Cardiol. 2002;40:976–982. doi:10.1016/S0735-1097(02)02059-4
18. Wang TJ, Larson MG, Levy D, et al. Impact of age and sex on plasma natriuretic peptide levels in healthy adults. Am J Cardiol. 2002;90:254–258.
19. Luchner A, Behrens G, Stritzke J, et al. Long-term pattern of brain natriuretic peptide and N-terminal pro brain natriuretic peptide and its determinants in the general population: contribution of age, gender, and cardiac and extra-cardiac factors. Eur J Heart Fail. 2013;15:859–867. doi:10.1093/eurjhf/hft048
20. Loke I, Squire IB, Davies JE, Ng LL. Reference ranges for natriuretic peptides for diagnostic use are dependent on age, gender and heart rate. Eur J Heart Fail. 2003;5:599–606. doi:10.1016/S1388-9842(03)00108-9
21. Crimmins EM, Thyagarajan B, Kim JK, Weir D, Faul J. Quest for a summary measure of biological age: the health and retirement study. Geroscience. 2021;43:395–408. doi:10.1007/s11357-021-00325-1
22. Aune D, Keum N, Giovannucci E, et al. Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies. Am J Clin Nutr. 2018;108:1069–1091. doi:10.1093/ajcn/nqy097
23. Sadowska-Bartosz I, Bartosz G. Effect of antioxidants supplementation on aging and longevity. Biomed Res Int. 2014;2014:404680. doi:10.1155/2014/404680
24. Bjelakovic G, Nikolova D, Gluud C. Antioxidant supplements and mortality. Curr Opin Clin Nutr Metab Care. 2014;17:40–41. doi:10.1097/MCO.0000000000000009
25. Aubert G. Telomere dynamics and aging. Prog Mol Biol Transl Sci. 2014;125:89–111.
26. Boccardi V, Paolisso G. Telomerase activation: a potential key modulator for human healthspan and longevity. Ageing Res Rev. 2014;15:1–5. doi:10.1016/j.arr.2013.12.006
27. Weindruch R, Walford RL, Fligiel S, Guthrie D. The retardation of aging in mice by dietary restriction: longevity, cancer, immunity and lifetime energy intake. J Nutr. 1986;116:641–654. doi:10.1093/jn/116.4.641
28. Weichhart T. mTOR as regulator of lifespan, aging, and cellular senescence: a mini-review. Gerontology. 2018;64:127–134. doi:10.1159/000484629
29. Singh M, Jensen MD, Lerman A, et al. Effect of low-dose rapamycin on senescence markers and physical functioning in older adults with coronary artery disease: results of a pilot study. J Frailty Aging. 2016;5(4):204–207. doi:10.14283/jfa.2016.112
30. Walters HE, Cox L. mTORC inhibitors as broad-spectrum therapeutics for age-related diseases. Int J Mol Sci. 2018;19:2325. doi:10.3390/ijms19082325
31. Chan AW, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. doi:10.1136/bmj.e7586
32. Zhang Z, Yuan KH. Practical Statistics Power Analysis Using Webpower and R. Granger, IN: ISDSA Press; 2018.
33. Washburn RA, Smith KW, Jette AM, Janney CA. The physical activity scale for the elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46:153–162. doi:10.1016/0895-4356(93)90053-4
34. EuroQol Group. EuroQol - a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208. doi:10.1016/0168-8510(90)90421-9
35. Katz S, Akpom CA. A measure of primary sociobiological functions. Int J Health Serv. 1976;6(3):493–508. doi:10.2190/UURL-2RYU-WRYD-EY3K
36. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179–186. doi:10.1093/geront/9.3_Part_1.179
37. Chan DC, Pang J, Watts GF. Pathogenesis and management of the diabetogenic effect of statins: a role for adiponectin and coenzyme Q10? Curr Atheroscler Rep. 2015;17:472. doi:10.1007/s11883-014-0472-7
38. Boccardi V, Barbieri M, Rizzo MR, et al. A new pleiotropic effect of statins in elderly: modulation of telomerase activity. FASEB J. 2013;27:3879–3885. doi:10.1096/fj.13-232066
39. Petrella RJ, Koval JJ, Cunningham DA, Paterson DH. A self-paced step test to predict aerobic fitness in older adults in the primary care clinic. J Am Geriatr Soc. 2001;49:632–638. doi:10.1046/j.1532-5415.2001.49124.x
40. Alehagen U, Johansson P, Björnstedt M, Rosén A, Dahlström U. Cardiovascular mortality and N-terminal-proBNP reduced after combined selenium and coenzyme Q10 supplementation: a 5-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. Int J Cardiol. 2013;167:1860–1866. doi:10.1016/j.ijcard.2012.04.156
41. Xia L, Wang XX, Hu XS, et al. Resveratrol reduces endothelial progenitor cells senescence through augmentation of telomerase activity by Akt-dependent mechanisms. Br J Pharmacol. 2008;155:387–394. doi:10.1038/bjp.2008.272
42. Wang XB, Zhu L, Huang J, et al. Resveratrol-induced augmentation of telomerase activity delays senescence of endothelial progenitor cells. Chin Med J. 2011;124:4310–4315.
43. Salvador L, Singaravelu G, Harley CB, Flom P, Suram A, Raffaele JM. A natural product telomerase activator lengthens telomeres in humans: a randomized, double blind, and placebo controlled study. Rejuvenation Res. 2016;19(6):478–484. doi:10.1089/rej.2015.1793
44. Savoia E, Fantini MP, Pandolfi PP, Dallolio L, Collina N. Assessing the construct validity of the Italian version of the EQ-5D: preliminary results from a cross-sectional study in North Italy. Health Qual Life Outcomes. 2006;4:47. doi:10.1186/1477-7525-4-47
45. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381. doi:10.1016/j.jbi.2008.08.010
46. Kalén A, Appelkvist EL, Dallner G. Age-related changes in the lipid compositions of rat and human tissues. Lipids. 1989;24:579–584. doi:10.1007/BF02535072
47. Mortensen SA, Rosenfeldt F, Kumar A, et al. Q-SYMBIO Study Investigators. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: results from Q-SYMBIO: a randomized double-blind trial. JACC Heart Fail. 2014;2:641–649. doi:10.1016/j.jchf.2014.06.008
48. Fu X, Ji R, Dam J. Acute, subacute toxicity and genotoxic effect of Bio-Quinone Q10 in mice and rats. Regul Toxicol Pharmacol. 2009;53:1–5. doi:10.1016/j.yrtph.2008.09.003
49. Landbo C, Almdal TP. Interaktion mellem warfarin og coenzym Q10 [Interaction between warfarin and coenzyme Q10]. Ugeskr Laeger. 1998;160:3226–3227. Danish.
50. Engelsen J, Nielsen JD, Hansen KF. Effekten af Coenzym Q10 og Ginkgo biloba på warfarindosis hos patienter i laengerevarende warfarinbehandling. Et randomiseret, dobbeltblindt, placebokontrolleret overkrydsningsforsøg [Effect of Coenzyme Q10 and Ginkgo biloba on warfarin dosage in patients on long-term warfarin treatment. A randomized, double-blind, placebo-controlled cross-over trial]. Ugeskr Laeger. 2003;165:1868–1871. Danish.
51. Giovannini S, Onder G, Lattanzio F, et al. Selenium concentrations and mortality among community-dwelling older adults: results from IlSIRENTE study. J Nutr Health Aging. 2018;22:608–612. doi:10.1007/s12603-018-1021-9
52. Sun JW, Shu XO, Li HL, et al. Dietary selenium intake and mortality in two population-based cohort studies of 133 957 Chinese men and women. Public Health Nutr. 2016;19:2991–2998. doi:10.1017/S1368980016001130
53. Rayman MP, Winther KH, Pastor-Barriuso R, et al. Effect of long-term selenium supplementation on mortality: results from a multiple-dose, randomised controlled trial. Free Radic Biol Med. 2018;127:46–54. doi:10.1016/j.freeradbiomed.2018.02.015
54. Ghanim H, Sia CL, Abuaysheh S, et al. An antiinflammatory and reactive oxygen species suppressive effects of an extract of Polygonum cuspidatum containing resveratrol. J Clin Endocrinol Metab. 2010;95(9):E1–E8. doi:10.1210/jc.2010-0482
55. Timmers S, Konings E, Bilet L, et al. Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell Metab. 2011;14:612–622. doi:10.1016/j.cmet.2011.10.002
56. Lam YY, Peterson CM, Ravussin E. Resveratrol vs. calorie restriction: data from rodents to humans. Exp Gerontol. 2013;48:1018–1024. doi:10.1016/j.exger.2013.04.005
57. Li YR, Li S, Lin CC. Effect of resveratrol and pterostilbene on aging and longevity. Biofactors. 2018;44:69–82. doi:10.1002/biof.1400
58. Brown VA, Patel KR, Viskaduraki M, et al. Repeat dose study of the cancer chemopreventive agent resveratrol in healthy volunteers: safety, pharmacokinetics, and effect on the insulin-like growth factor axis. Cancer Res. 2010;70:9003–9011. doi:10.1158/0008-5472.CAN-10-2364
59. Hector KL, Lagisz M, Nakagawa S. The effect of resveratrol on longevity across species: a meta-analysis. Biol Lett. 2012;8(5):790–793. doi:10.1098/rsbl.2012.0316
60. Wang C, Wheeler CT, Alberico T, et al. The effect of resveratrol on lifespan depends on both gender and dietary nutrient composition in Drosophila melanogaster. Age. 2013;35:69–81. doi:10.1007/s11357-011-9332-3
61. Baur JA, Pearson KJ, Price NL, et al. Resveratrol improves health and survival of mice on a high-calorie diet. Nature. 2006;444:337–342. doi:10.1038/nature05354
62. Shaito A, Posadino AM, Younes N, et al. Potential adverse effects of resveratrol: a literature review. Int J Mol Sci. 2020;21:2084. doi:10.3390/ijms21062084
63. Walle T. Bioavailability of resveratrol. Ann N Y Acad Sci. 2011;1215:9–15. doi:10.1111/j.1749-6632.2010.05842.x
64. Patel KR, Scott E, Brown VA, Gescher AJ, Steward WP, Brown K. Clinical trials of resveratrol. Ann N Y Acad Sci. 2011;1215:161–169. doi:10.1111/j.1749-6632.2010.05853.x
65. Dow CT, Harley CB. Evaluation of an oral telomerase activator for early age-related macular degeneration - a pilot study. Clin Ophthalmol. 2016;10:243–249. doi:10.2147/OPTH.S100042
66. Fernandez ML, Thomas MS, Lemos BS, et al. TA-65, A telomerase activator improves cardiovascular markers in patients with metabolic syndrome. Curr Pharm Des. 2018;24:1905–1911. doi:10.2174/1381612824666180316114832
67. Singaravelu G, Harley CB, Raffaele JM, Sudhakaran P, Suram A. Double blind, placebo controlled, randomized trial demonstrates telomerase activator TA-65 decreases immunosenescent CD8+CD28- T cells in humans. OBM Geriatrics. 2021;5:1. doi:10.21926/obm.geriatr.2102168
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.