Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Can We Adapt Neoadjuvant Rectal (NAR) Score with Systemic Immune-Inflammation Index (SII) and Prognostic Nutritional Index (PNI) as Prognostic Factors in Locally Advanced Breast Cancer?
Authors Yüksel C ![]() , Dogan M, Çulcu S, Doğan L
, Dogan M, Çulcu S, Doğan L
Received 10 November 2025
Accepted for publication 14 February 2026
Published 20 February 2026 Volume 2026:18 578298
DOI https://doi.org/10.2147/BCTT.S578298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Cemil Yüksel,1 Mutlu Doğan,2 Serdar Çulcu,3 Lütfi Doğan4
1Department of Surgical Oncology, Mersin City Training and Research Hospital, Mersin, Türkiye; 2Department of Medical Oncology, Dr. Abdurrahman Yurtaslan Oncology Training and Research Hospital, Ankara, Türkiye; 3Department of Surgical Oncology, Ankara University School of Medicine, Ankara, Türkiye; 4Department of Surgical Oncology, Ankara Etlik City Training and Research Hospital, Ankara, Türkiye
Correspondence: Cemil Yüksel, Department of Surgical Oncology, Mersin City Training and Research Hospital, Mersin, Türkiye, Tel +90 535 443 1647, Email [email protected]
Background: Breast cancer is the most common malignancy among women, and despite therapeutic advances, many still present with locally advanced disease. Identifying simple prognostic tools to predict outcomes after neoadjuvant therapy remains a challenge. The neoadjuvant rectal (NAR) score, systemic immune-inflammation index (SII), and prognostic nutritional index (PNI) have shown prognostic value in various malignancies. In this study, we evaluated their prognostic significance in patients with locally advanced breast cancer (LABC).
Methods: We retrospectively analyzed 187 female LABC patients treated with anthracycline- and taxane-based neoadjuvant chemotherapy between 2011 and 2020. HER2-positive patients also receive anti-HER2 therapy. The NAR score was calculated using the Valentini formula, and the SII and PNI were determined before (bNAT) and after (aNAT) the neoadjuvant treatment. Receiver operating characteristic (ROC) analysis defined the cut-off values for NAR (28.35), SII (bNAT: 656; aNAT: 687), and PNI (bNAT: 42.5; aNAT: 40.5). Associations with clinicopathological variables, disease-free survival (DFS), and overall survival (OS) were analyzed using the chi-square, Mann–Whitney U, and Kaplan–Meier tests.
Results: Of all patients, 62% had low NAR scores (≤ 28.35) and 38% had high scores (> 28.35). High NAR scores correlated with advanced stage, lymphovascular invasion, lower pathological complete response (pCR), and higher mortality (p < 0.01). Post-treatment, the SII increased (p = 0.012), while the PNI decreased (p = 0.001). Low PNI (aNAT < 40.5) was associated with higher mortality (p = 0.027) and axillary nodal positivity (p = 0.033). The median follow-up period was 46 months.
Conclusion: High NAR and low post-treatment PNI were associated with a poor prognosis in patients with LABC. These accessible parameters may complement the existing prognostic models; however, prospective validation in larger cohorts is warranted and the retrospective design and single-center nature of the study should be considered when interpreting results.
Keywords: neoadjuvant rectal score, systemic immune inflammation index, breast cancer, prognostic nutritional index, prognostic factors
Introduction
Breast cancer is the most common malignancy and second most common cause of cancer-related deaths in females all around the world.1 According to cancer statistics by Siegel et al, 297790 new cases of breast cancer and 43170 deaths related to breast cancer are expected in 2023.1 Despite the higher incidence of breast cancer, the mortality rate has decreased owing to early diagnosis and treatment advances in recent years. However, many patients are at an advanced stage of the disease, particularly in developing countries. Neoadjuvant treatment is the gold standard treatment for locally advanced stage breast cancer. The pathological response to neoadjuvant treatment is a prognostic factor for breast cancer.2 A positive correlation between pathological complete response (pCR) and long-term outcomes is best documented for triple-negative breast cancer (TNBC), then by HER2 positive (HER2 score of +3 by immunohistochemistry (IHC) or +2 by IHC & positive by in situ hybridization, ISH) breast cancer and hormone receptor-positive [estrogen receptor (ER) and/or progesterone receptor (PR)] breast cancer, respectively.3,4 Its significance as a surrogate marker in “all” breast cancer subtypes remains controversial.4,5 Therefore, biomarkers other than intrinsic subtypes are needed to determine the best candidates for neoadjuvant treatment in locally advanced-stage breast cancer.
Neoadjuvant treatment, such as neoadjuvant chemoradiotherapy or total neoadjuvant treatment, is also the standard treatment for locally advanced rectal cancer. However, pathological response rates differ according to clinical and pathological features, almost in locally advanced-stage rectal cancer. All these points led to the discovery of biomarkers for selecting the best candidates for better outcomes in terms of response rates and survival.
The struggle to explore potential surrogate markers in clinical trials has raised several questions. Overall survival (OS) is a perfect primary endpoint in clinical trials despite some difficulties, such as longer follow-up durations. In locally advanced-stage cancer, pCR with neoadjuvant treatment is a commonly used primary endpoint and a surrogate marker in neoadjuvant treatment trials. However, the utility of these parameters may be somewhat difficult in retrospective studies, especially those with a small number of patients and short follow-up durations. Therefore, in addition to the clinical and pathological features of retrospective studies, we focused on the prognostic scoring systems and inflammatory parameters.
Neoadjuvant rectal (NAR) score is a prognostic scoring system that has been shown to be a “potential” surrogate marker in rectal cancer.6,7 It has also been reported to have prognostic and predictive value in patients with gastric cancer for whom perioperative chemotherapy is indicated.8
The relationship between cancer and inflammation is a well-known process with complex interactions for intracellular signaling pathways, immune reactions in both tumor and tumor microenviroment. Inflammatory response plays a key role in these interactions. Therefore, inflammatory indices, such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune inflammation index (SII), and prognostic nutritional index (PNI), have been claimed to be prognostic factors in some solid tumors, especially in metastatic disease in recent decades.9–11 The prognostic and predictive value of these parameters was also evaluated in patients with locally advanced stage cancer, as in locally advanced stage breast cancer.12 Eraslan et al reported that SII might be a possible predictive marker for pCR with neoadjuvant chemoradiotherapy in locally advanced-stage rectal cancer.12
Encouraging data for NAR score in locally advanced stage rectal cancer and probably in other cancers, besides inflammatory indices in many solid tumors led us to search their potential prognostic and predictive values in locally advanced stage breast cancer as an unmet need in this area. In the present study, we aimed to evaluate the prognostic role of the NAR score in addition to the SII and PNI in patients with locally advanced-stage breast cancer receiving neoadjuvant treatment.
Despite the widespread use of neoadjuvant therapy in locally advanced breast cancer, there is currently no simple composite scoring system that integrates clinical downstaging and pathological response to predict long-term outcomes. The neoadjuvant rectal (NAR) score, originally developed for rectal cancer is based on the degree of tumor and nodal downstaging following neoadjuvant treatment and has been validated as a surrogate prognostic marker in rectal and gastric cancer. Given that tumor burden reduction and nodal response after neoadjuvant therapy are also critical determinants of prognosis in breast cancer, we hypothesized that the NAR score could be biologically and clinically adaptable to locally advanced breast cancer. In addition, systemic inflammatory and nutritional indices such as SII and PNI may reflect host-tumor interactions and treatment related immune modulation, potentially complementing the NAR score in prognostic stratification.
Materials and Methods
Patients with locally advanced-stage breast cancer who were followed-up at our center were included in the study. All patients received neoadjuvant treatment. The patient received neoadjuvant chemotherapy with doxorubicin and taxane. HER2 positive ones received anti-HER2 treatment in a neoadjuvant setting and continued as an adjuvant. Anti-HER2 treatment was administered as trastuzumab with or without pertuzumab, according to the local approval and reimbursement procedures in those years. Hormone receptor-positive patients received additional adjuvant endocrine treatment. In addition to the NAR score, SII, and PNI, the clinical and pathological characteristics of the patients were also evaluated. The pathological and clinical features of patients were recorded using a local registration database.
Neoadjuvant rectal (NAR) scores and inflammatory indices were estimated based on related parameters in our database. Inflammatory indices such as SII and PNI were estimated at baseline (ie, bNAT and aNAT, respectively. The nomogram by Valentini et al was used to calculate the NAR score calculation.13 The formula for the NAR score is as follows: [5 ypN − 3 (cT − ypT) + 12]2 / 9.61. In this formula, ypT and ypN indicate the T and N stages after neoadjuvant treatment, respectively, while cT indicates the clinical T stage at baseline. All data were recorded in number formats for the cT (0,1,2,3,4), ypT (0,1,2,3), and ypN (0,1,2,3) stages. The NAR score cutoff value was estimated as 28.35 with 62.5% sensitivity and 65.4% specificity. Patients were grouped into the NAR score low (NAR-L, ≤ 28.35) and high (NAR-H,>28.35) subgroups.
Cutoff values for NAR, SII, and PNI were defined by ROC (receiver operating curve (ROC) analysis. Systemic inflammatory indices were calculated as follows: SII [neutrophils (109/L) × platelets (109/L) / lymphocytes (109/L]) and PNI [albumin (g/L) + (5× lymphocytes (109/L]). Cut-off values for the SII and PNI were determined before and after neoadjuvant treatment. The cut-off values were defined as 656 (bNAT) and 687 (aNAT) for SII and 42.5 (bNAT) and 40.5 (aNAT) for PNI.
Correlations among pathological features, sentinel lymph node (SLN) and axillary lymph node (ALN) positivity rates, and NAR scores were evaluated using the chi-square test. ALN positivity ratio (ALNR) was estimated as the number of involved lymph nodes/excised lymph nodes for all sentinel and non-sentinel lymph nodes. We also evaluated the prognostic significance of the SII and PNI.
Statistical Analyses
Statistical analyses were performed using IBM SPSS Statistics for Windows software v.11.5 (IBM, NY, USA). For descriptive analysis, quantitative variables were presented as mean ± standard deviation and median (range: minimum- maximum), whereas qualitative variables were presented as the number of patients (ie, percentage). Since normal distribution assumptions were not realized, whether there was a difference between the categories of the qualitative variables, including two categories in terms of quantitative variables, was analyzed using the Mann–Whitney U-test. Chi-square test and Fisher’s exact test were used to evaluate the relationship between the two qualitative variables.
No invasive tumor in the breast and/or lymph nodes after neoadjuvant treatment was defined as pathological complete response (pCR). The interval between the initiation of neoadjuvant treatment and recurrence was defined as disease free survival (DFS) whereas the interval between the initiation of neoadjuvant treatment and death due to any cause was defined as overall survival (OS). Median follow-up and survival analyses were performed using the Kaplan-Meier method, with comparison of groups using the Log rank test. Receiver operating characteristic (ROC) curve analysis was performed to quantify the area under the ROC curve (AUC) for cut-off values. The statistical significance level for the p-value was set at 0.05.
Results
Patients’ and Tumor Characteristics
Between December 2011 and November 2020, 187 patients with locally advanced-stage breast cancer were retrospectively evaluated. Patients with inadequate data and/or those lost to follow-up were also excluded. All the patients were female and underwent surgery after neoadjuvant treatment. Neoadjuvant treatment included anthracyclines and taxanes as chemotherapy in addition to anti-HER2 treatment in HER2 positive ones. HER2 positivity rate was 14.97% (n: 28). Of twenty-eight HER2 positive patients, 24 (85.72%) received neoadjuvant anti-HER2 therapy. After 4 AC (doxorubicine/cyclophosphamide, every 3 weeks), they received 3 months of anti-HER2 treatment with taxanes [4 docetaxel/trastuzumab/pertuzumab, every 3 weeks), 12w PTP (paclitaxel/trastuzumab/pertuzumab, every week), 12w PT (paclitaxel/trastuzumab, every week). All patients received perioperative anti-HER2 treatment for 52 weeks as continuation of adjuvant trastuzumab therapy. Unfortunately, adjuvant TDM1 could not be administered to all patients with residual disease because it was not reimbursed in our country. Of the remaining four patients, one received only adjuvant trastuzumab, and three received neither adjuvant nor neoadjuvant anti-HER2 treatment. All the patients with ER-positive disease received adjuvant endocrine therapy.
The median age of the patients was 54 years (range: 31–79). The patient characteristics are summarized in Table 1. Most patients were ER-positive (n = 158, 84.49%), luminal B-like HER2 negative (n = 105, 56.15%), grade 3 (n = 121, 64.71%), and stage 3 (n = 81, 43.31%) disease. The lymphovascular space invasion (LVI) and perineural invasion (PnI) rates were as 42.78% (n = 80) and 34.76% (n = 65), respectively. Half (n = 102, 54.54%) had upper-outer quadrant localization. Sentinel lymph node (SLN) biopsy was performed in 88 patients (47.06%), with a positivity rate of 45.45%. The median number of excised SLN and positive SLN was 3 (range: 1–10) and 0 (range: 0–5), respectively. Axillary dissection (AD) was applied in 144 (77%) patients, of these, it was applied as a part of modified radical mastectomy (MRM) in 128 (68.45%) patients and with breast conserving surgery (BCS) in 16 (8.55%) patients. The median values were 15 (range: 5–21) for excised lymph nodes and 3 (range: 0–21) for positive lymph nodes. There was a positive correlation between the ALNR and mortality. Patients with an ALNR (>0.19) had a higher mortality rate (p = 0.001). Those with more positive ALN (> 3.5) had a shorter OS (p = 0.016). Additionally, patients with higher metastatic non-sentinel lymph nodes (>3.5) and non-sentinel ALNR (> 0.23) had higher mortality rates without a significant effect on OS (p = 0.649 and p = 0.722, respectively). Sentinel ALNR was not a prognostic factor for OS (p = 0.962). The number of excised SLNB was not a prognostic factor (p = 0.756). Interestingly, the median DFS and OS were both 22 months, with a median follow-up of 22 (3–109) months.14 In the second analysis, with a median follow-up of 46 (3–135) months, the median OS was 46 and 43 months, respectively. An earlier interim analysis was performed; however, all survival analyses presented in this study are based on the updated cohort with a median follow-up of 46 months. There were no statistically significant differences in prognostic factors in our second analysis.
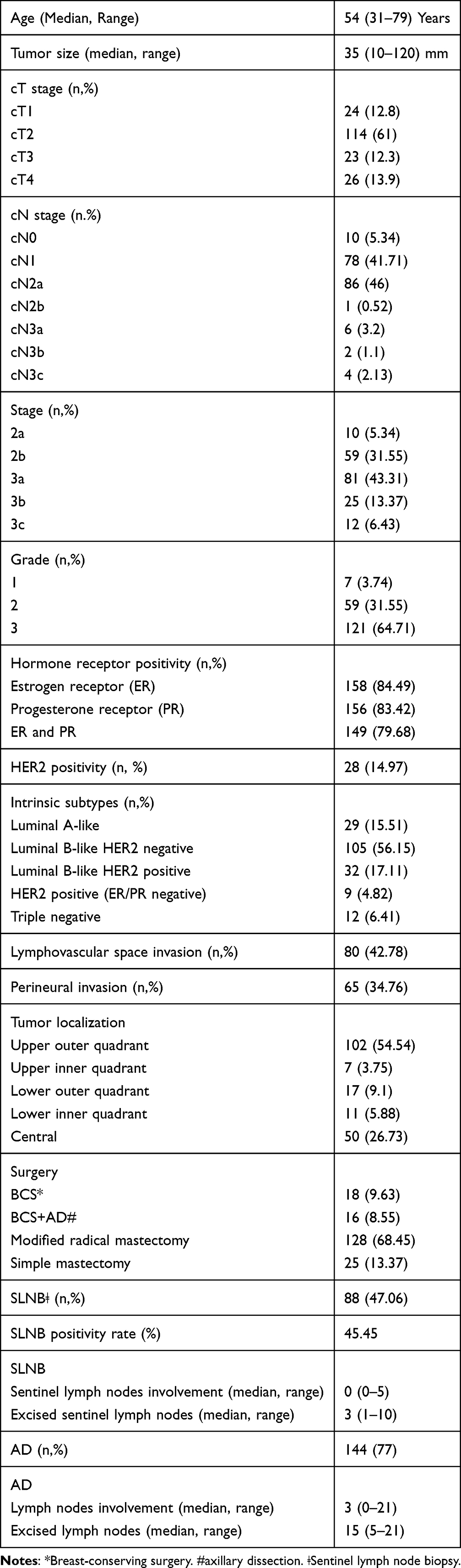 |
Table 1 Patient Characteristics |
NAR Score, Systemic Inflammatory Indices (SII) and Prognostic Nutritional Index (PNI)
One hundred and sixteen (62%) patients had NAR-L scores (<28.35) whereas 71 (38%) had NAR-H scores (>28.35). The median age was 54 years for both NAR-L (range: 31–79) and NAR-H (range: 27–79) subgroups. (Table 2) In our first analysis, with a median follow-up of 22 months (range: 3–109) months, the mortality rate was higher in the NAR-H subgroup, without a difference in OS (p = 0.009, p = 0.07). The median OS was 45 and 50 months in the NAR-H and NAR-L subgroups, respectively (P = 0.07) (Figure 1).14 The NAR-H subgroup had a significantly shorter DFS, despite a shorter median DFS in both subgroups (p = 0.01). The median DFS times were 42.5 months in NAR-H subgroup whereas it was 43 months in the NAR-H and NAR-L subgroups, respectively. Patients in the NAR-H subgroup had higher rates of advanced-stage disease at diagnosis, LVI, and PnI (p: 0.001, p: 0.001 and p = 0.001, respectively). Patients in the NAR-H subgroup had more luminal-like (ER+/PR+) disease (P = 0.011, P = 0.004, and P = 0.001, respectively). Axillary nodal involvement was positively correlated with the NAR score. Axillary nodal involvement and SLN positivity rates were higher in the NAR-H subgroup (p = 0.001 and p = 0.001, respectively). However, the SLNB rate was lower in the NAR-H group (P = 0.001). They also had a higher number of MRM during the surgical procedure (p = 0.001). Lower pCR and higher distant metastasis rates were observed in this subgroup (p = 0.001 and p = 0.001, respectively).
 |
Table 2 Relationship Between NAR Score & Pathological Features |
 |
Figure 1 Kaplan–Meier overall survival curves according to NAR-H and NAR-L subgroups. The blue line (0.00) represents the NAR-L group, while the red line (2.00) represents the NAR-H group. Survival distributions were compared using the Log rank test (log-rank p = 0.07). |
Systemic inflammatory indices were significantly higher after neoadjuvant treatment, whereas PNI was significantly lower after neoadjuvant treatment (p = 0.012, p = 0.001). The patients were categorized SII (bNAT, aNAT) and PNI (bNAT, aNAT) according to the cut-off levels, as mentioned previously. The SII (aNAT) was significantly higher than the SII (bNAT) (p = 0.012). However, there was no correlation between the SII (bNAT) and SII (aNAT) and mortality (p = 0.959, p = 0.716). In contrast, the PNI (aNAT) was significantly lower than the PNI (bNAT) (p = 0.001). Patients with a lower PNI (aNAT) had a higher mortality rate (P = 0.027). However, there was no significant difference in survival in terms of median PNI (bNAT) and PNI (aNAT) (p = 0.133, p = 0.107). The median OS was 49 months in the PNI (aNAT)-low and 43.5 months in PNI (aNAT)-high subgroups, respectively. None of these parameters showed prognostic significance for pCR, ALN positivity, DFS or OS. The SII (bNAT) was positively correlated with the PnI, whereas the PNI (bNAT) was positively correlated with the cT stage (p = 0.027, p = 0.006). Patients with a high PNI (aNAT) tended to have fewer excised ALNs (p = 0.05). The ALN positivity rate was higher in PNI (aNAT)-low patients (p = 0.033).
Discussion
The NAR score is a prognostic factor for rectal cancer. In this study, we evaluated the prognostic and predictive role of the NAR score for neoadjuvant chemotherapy in addition to the SII and PNI in locally advanced stage breast cancer. To the best of our knowledge, this is the first study to evaluate the role of NAR score in breast cancer. It should be emphasized that the associations observed in this study reflect correlations rather than causal relationships, given the retrospective design and the absence of multivariate modeling.
In locally advanced stage breast cancer, pCR is a considerable surrogate marker in clinical trials, especially in HER2 positive and triple negative breast cancer.15,16 However, prognostic and predictive markers are required to select the best candidates for neoadjuvant treatment to achieve better pCR rates. In our study, the NAR score was shown to have a prognostic significance similar to that of rectal cancer. NAR-H score (>28.35) was defined as a poor prognostic factor (p = 0.009). Lower pCR and higher LVI and PNI with higher postoperative ALN positivity rates were observed in those with NAR-H scores (all p <0.001). The NAR score formula includes cT, pT, and pN as the pathological features.13 As expected, higher T and N stages were associated with higher NAR scores. Therefore, a higher NAR score almost in breast cancer is a poor prognostic factor for BC. However, all our patients had locally advanced-stage breast cancer. Therefore, there must be other poor prognostic factors rather than the NAR-H score. Despite its prognostic associations, the clinical applicability of the NAR score in breast cancer may be limited. Unlike rectal cancer, breast cancer exhibits substantial biological heterogeneity, diverse intrinsic subtypes, and long-term recurrence patterns that may not be fully captured by downstaging-based composite scores. Therefore, the NAR score should not be considered a standalone clinical decision-making tool in breast cancer, but rather a potential adjunct marker that requires further validation. In contrast to rectal cancer, where neoadjuvant-induced tumor regression closely correlates with long-term outcomes, survival in breast cancer—particularly hormone receptor–positive disease—is influenced by prolonged biological behavior and adjuvant systemic therapies, which may dilute the prognostic impact of early pathological response–based scores.
The tumor microenvironment also plays a critical role in cancer biology via interactions between pro- and anti-tumor immune cells.17 Inflammatory and immune markers, such as NLR, PLR and tumor infiltrating lymphocytes (TILs) were shown to have prognostic and predictive significance for response to neoadjuvant treatment in triple negative breast cancer.17,18 In a metaanalysis of 7657 cancer patients in 22 studies, a high SII was confirmed to be a poor prognostic factor.19 We considered that PNI might have an additive prognostic and predictive value with SII in our study, as PNI was also shown to be a prognostic factor in cancer.11 However, to the best of our knowledge, the relationship between SII, PNI, and NAR score and changes in these parameters with neoadjuvant treatment has not been evaluated in breast cancer. All of these parameters are easily accessible in daily practice. Therefore, evaluation of these simple parameters and their changes with systemic treatment might have additional significance in parallel with the changes in the tumor and tumor microenvironment. Therefore, we evaluated the SII and PNI before (bNAT) and after (aNAT) neoadjuvant treatment. We determined that PNI [ie, albumin (g/dL] + 5 × lymphocyte (109/L]) was higher in those with a higher basal SII (p = 0.027). Lymphocytes are immune cells that are possible indicators of systemic inflammation. We also showed that a decrease in the PNI with neoadjuvant treatment was a poor prognostic factor (p = 0.027). So, higher basal lymphocytes and a decrease in lymphocytes with neoadjuvant treatment might have contributed to a decrease in immune response and poor prognosis, as if in our study. Patients with lower PNI after neoadjuvant treatment had higher rates of postoperative ALN positivity and mortality, supporting the hypothesis mentioned above (p = 0.033, p = 0.027). Although neutrophils are also immune cells, they may have less significance in immunmodulation and immune response. In our study, there was a significant increase in the SII after neoadjuvant treatment (p = 0.012). According to the SII formula [neutrophil (109/L) × platelet (109/L)) / lymphocyte (109/L)], an increase in neutrophil and/or a decrease in lymphocyte counts leads to a higher SII. Therefore, a decrease in lymphocytes by neoadjuvant treatment might have affected the lower PNI and higher SII in our study.
Our study has some limitations. First, it had a retrospective design. Second, it had a relatively small sample size and heterogeneity to identify the survival outcomes. Third, there may have been more changes during neoadjuvant treatment cycles. These changes may be correlated with other parameters. However, we evaluated the inflammatory parameters (albumin, neutrophils, lymphocytes, and platelets) before and after neoadjuvant treatment. The relatively limited sample size restricts the ability to perform robust multivariate and subgroup analyses and therefore the findings should be interpreted as exploratory. Cut-off values were derived using ROC analyses within the same cohort which may introduce overfitting and limits generalizability. External validation in independent cohorts is therefore required. As multivariate Cox regression analyses were not performed, the prognostic associations observed in this study should not be interpreted as independent effects. Although longer follow-up is required to fully capture long-term survival outcomes in breast cancer, the current follow-up duration allows assessment of early prognostic signals after neoadjuvant therapy. Treatment heterogeneity, particularly among HER2-positive patients due to historical reimbursement limitations, represents an additional limitation that may have influenced outcome interpretation.
In conclusion, our study revealed that NAR score and (aNAT) can be adapted to breast cancer as prognostic factors. NAR-H score (>28.35) and PNI (aNAT)-low (<40.5) were associated with poor prognosis. The SII (bNAT)-high subgroup had higher PnI values. The changes in PNI and SII with neoadjuvant treatment may contribute to further interventions in the management of patients with locally advanced-stage breast cancer. These parameters are readily available in daily clinical practice. However, further randomized clinical trials are required to confirm this hypothesis. We consider that not only basal SII (bNAT) and PNI (bNAT) levels, but also changes with systemic treatment (ie, aNAT values) seem to have clinical significance in addition to the NAR score. Therefore, the evaluation of SII and PNI with NAR scores in our study revealed a combined easy strategy for the prediction of neoadjuvant treatment efficacy in locally advanced-stage breast cancer. These findings should be interpreted within the context of an exploratory, retrospective analyses and should not be considered directly clinically actionable without further prospective validation.
Ethics Approval and Consent to Participate
This retrospective study was approved by the Ethics Committee of Dr. Abdurrahman Yurtaslan Oncology Training and Research Hospital (Approval No: 2020-11/895). The requirement for informed consent was waived due to the retrospective nature of the study. All procedures were conducted in accordance with the principles of the Declaration of Helsinki. All patient data were anonymized prior to analysis and handled in strict accordance with institutional policies and the principles of data confidentially and privacy.
Funding
No specific funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Clancy E. ACS report shows prostate cancer on the rise, cervical cancer on the decline. Renal Urol News. 2023.
2. Bear HD, Anderson S, Smith RE, et al. Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer: national surgical adjuvant breast and bowel project protocol B-27. J clin oncol. 2006;24(13):2019–9. doi:10.1200/JCO.2005.04.1665
3. Von Minckwitz G, Untch M, Blohmer J-U, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin oncol. 2012;30(15):1796–1804. doi:10.1200/JCO.2011.38.8595
4. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. doi:10.1016/S0140-6736(13)62422-8
5. Montemurro F, Di Cosimo S. Pathological complete response in breast cancer patients receiving neoadjuvant chemotherapy. Breast. 2014;23(5):690–691. doi:10.1016/j.breast.2014.06.007
6. Rosello S, Frasson M, García-Granero E, et al. Integrating downstaging in the risk assessment of patients with locally advanced rectal cancer treated with neoadjuvant chemoradiotherapy: validation of Valentini’s nomograms and the neoadjuvant rectal score. Clin Colorectal Canc. 2018;17(2):104–112.e2. doi:10.1016/j.clcc.2017.10.014
7. Sun Y, Zhang Y, Wu X, et al. Prognostic significance of neoadjuvant rectal score in locally advanced rectal cancer after neoadjuvant chemoradiotherapy and construction of a prediction model. J Surg Oncol. 2018;117(4):737–744. doi:10.1002/jso.24907
8. Ucar G, Acikgoz Y, Ergun Y, et al. Prognostic and predictive value of NAR score in gastric cancer. J Gastrointest Canc. 2021;52(3):1054–1060. doi:10.1007/s12029-020-00537-2
9. Dogan M, Eren T, Ozdemir N, et al. The relationship between platelet–lymphocyte ratio, neutrophil–lymphocyte ratio, and survival in metastatic gastric cancer on firstline modified docetaxel and cisplatinum plus 5 Fluorourasil Regimen: a single institute experience. Saudi J Gastroenterol. 2015;21(5):320. doi:10.4103/1319-3767.166207
10. Li C, Tian W, Zhao F, et al. Systemic immune-inflammation index, SII, for prognosis of elderly patients with newly diagnosed tumors. Oncotarget. 2018;9(82):35293. doi:10.18632/oncotarget.24293
11. Dogan M, Algin E, Guven ZT, et al. Neutrophil–lymphocyte ratio, platelet–lymphocyte ratio, neutrophil–platelet score and prognostic nutritional index: do they have prognostic significance in metastatic pancreas cancer? Curr Med Res Opin. 2018;34(5):857–863. doi:10.1080/03007995.2017.1408579
12. Eraslan E, Adas YG, Yildiz F, et al. Systemic immune-inflammation index (SII) predicts pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer. J Coll Physicians Surg Pak. 2021;30(4):399–404.
13. Valentini V, van Stiphout RGPM, Lammering G, et al. Nomograms for predicting local recurrence, distant metastases, and overall survival for patients with locally advanced rectal cancer on the basis of European randomized clinical trials. J Clin Oncol. 2011;29(23):3163–3172. doi:10.1200/JCO.2010.33.1595
14. Yüksel C, Doğan M, Çulcu S, et al. Abstract P4-06-05: can we adapt neoadjuvant rectal (NAR) score besides sytemic immun inflammation index (SII) and prognostic nutritional index (PNI) as prognostic factors to locally advanced breast cancer? Cancer Res. 2022;82(4_Supplement):
15. Schettini F, Pascual T, Conte B, et al. HER2-enriched subtype and pathological complete response in HER2-positive breast cancer: a systematic review and meta-analysis. Cancer Treat Rev. 2020;84:101965. doi:10.1016/j.ctrv.2020.101965
16. Krystel-Whittemore M, Xu J, Brogi E, et al. Pathologic complete response rate according to HER2 detection methods in HER2-positive breast cancer treated with neoadjuvant systemic therapy. Breast Cancer Res Treat. 2019;177(1):61–66. doi:10.1007/s10549-019-05295-9
17. Geršak K, Geršak BM, Gazić B, et al. The possible role of anti-and protumor-infiltrating lymphocytes in pathologic complete response in early breast cancer patients treated with neoadjuvant systemic therapy. Cancers. 2023;15(19):4794. doi:10.3390/cancers15194794
18. Kusama H, Kittaka N, Soma A, et al. Predictive factors for response to neoadjuvant chemotherapy: inflammatory and immune markers in triple-negative breast cancer. Breast Cancer. 2023;30:1–9.
19. Yang R, Chang Q, Meng X, et al. Prognostic value of systemic immune-inflammation index in cancer: a meta-analysis. J Cancer. 2018;9(18):3295. doi:10.7150/jca.25691
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Prognostic Nutritional Index-Based Nomogram to Predict Breast Cancer Metastasis: A Retrospective Cohort Validation
Chen Z, Gao H, Cheng M, Song C
Breast Cancer: Targets and Therapy 2025, 17:497-510
Published Date: 10 June 2025
Risk Factors and Prognosis Analysis of Infiltrating Micropapillary Carcinoma of Breast: A Retrospective Study
He P, Sha Y, Lu Y, Li T, Li X, Liu Y, Pang H, Han J, Yuan Q
Breast Cancer: Targets and Therapy 2026, 18:612948
Published Date: 19 June 2026