Back to Journals » Open Access Emergency Medicine » Volume 13
Can Professional Motorcyclists Be an Asset in the Immediate Post-Crash Care System in Benin? Baseline of Knowledge and Practices in the City of Cotonou (Benin)
Authors Glèlè-Ahanhanzo Y ![]() , Kpade A
, Kpade A ![]() , Kpozèhouen A
, Kpozèhouen A ![]() , Levêque A, Ouendo EM
, Levêque A, Ouendo EM
Received 18 June 2020
Accepted for publication 27 October 2020
Published 6 January 2021 Volume 2021:13 Pages 1—11
DOI https://doi.org/10.2147/OAEM.S267828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Yolaine Glèlè-Ahanhanzo,1 Angélique Kpade,2 Alphonse Kpozèhouen,1 Alain Levêque,3 Edgard-Marius Ouendo4
1Multidisciplinary Research Unit for Road Crashes Prevention (ReMPARt), Epidemiology and Biostatistic Department, Regional Institute of Public Health, Ouidah, Benin; 2Cotonou Army Training Hospital, Cotonou, Benin; 3Center for Research in Epidemiology, Biostatistics and Clinical Research, Public Health School (Université Libre de Bruxelles), Brussels, Belgium; 4Health Policies and Systems Department, Regional Institute of Public Health, Ouidah, Benin
Correspondence: Yolaine Glèlè-Ahanhanzo
Multidisciplinary Research Unit for Road Crashes Prevention (ReMPARt), Epidemiology and Biostatistic Department, Regional Institute of Public Health, Slaves Road, BP: 384, Ouidah, Benin
Tel +229 95966858
Email [email protected]
Purpose: The situation of road crashes-related deaths remains problematic in low-income countries. The present study aims at analyzing the first-aid knowledge and practices of professional motorcyclists (PMs) in the city of Cotonou in Benin.
Materials and Methods: This is a cross-sectional analytical study conducted from 25 March to 19 April 2019 in Cotonou and concerned PMs registered in a fleet who gave their consent to participate in the study. The World Health Organization’s two-stage adaptive cluster sampling technique was applied to select the eligible PMs while respecting the proportionality rate per fleet. A logistic regression analysis was done and the odds ratios were estimated with 95% confidence interval.
Results: The 430 PMs surveyed were all middle-aged men with an average age of 38.38 (± 8.70). Among them, 62.56% knew at least one of the emergency phone numbers for the ambulance, police or fire services and 49.53% of the PMs knew at least one of the 3 techniques evaluated. In addition, 33.23% of PMs who had witnessed at least an RC stated that they had alerted the emergency services, and 32.27% said they had helped the victims. The main reason given for the lack of initiative in RCs was lack of knowledge of the course of action to take (19.64%). The level of knowledge was associated with the level of education (AOR: 3.11; CI 95%: 1.79– 5.43) and with the length of experience (AOR: 2.56; CI 95%: 1.58– 4.18).
Conclusion: This study reveals that the level of knowledge and practice of PMs in the field of first aid in Cotonou is low and demonstrates the relevance and the need to include this target group in the first-aid chain for road crashes in Benin.
Keywords: road crashes, first aid, motorcycles, professional corporations
Introduction
According to most recent estimates by the World Health Organization (WHO), there are still more than one million road deaths per year. The situation in low-income countries is more critical because road crashes (RC) mortality has not improved since 2013, with death statistics that have not declined and a risk of pre-hospital mortality that is twice as high as in high-income countries.1,2
According to the literature, nearly 40% of pre-hospital deaths can be prevented with basic first-aid care. As such, the responsiveness and efficiency of the immediate post-crash management system help to reduce pre-hospital mortality in RCs.3–6 In developing countries, there is evidence that immediate post-crash management systems are inefficient and ineffective.7–9 In these contexts, it is therefore necessary to propose appropriate strategies to improve these systems. In the case of RCs, there is an opportunity to intervene at the scene of the crash. Witnesses or those who arrive first at the scene of an RC can play a vital role in the provision of emergency care, and contribute significantly with basic first aid.10−12 First-aid measures are a set of basic methods and techniques that are properly implemented to relieve urgency and reduce mortality in the pre-hospital setting.13 Interventions by laypersons in the case of RCs are not uncommon; however, their nature, relevance and effectiveness remain to be demonstrated, although the goodwill of the parties concerned cannot be denied.12,14,15 They vary greatly in nature, ranging from families to taxi drivers, and intervene, to varying degrees, in the majority of cases.14,16 To hope for the effectiveness of these interventions, it is necessary at least that the interveners have a satisfactory level of knowledge and practical skills in the domain. According to the literature review, the level of knowledge and practice of first aid is usually low among laypersons.17,18 However, several studies have also shown on the one hand, that the level of knowledge is associated with the level of practice and on the other hand that training can improve both the level of knowledge and practice of first aid.17–20
In Benin, professional motorcyclists (PMs) are the most common type of mobile layperson, especially in large cities. In the case of RCs, they are most often the first on the scene. With the required skills, they could represent a real opportunity for alerting and administering first aid before the arrival of the emergency services. To support the strategic decisions aimed at improving the chain of intervention in immediate post-crash situations in Benin, this study aims at analyzing the knowledge and practices of professional drivers in first aid in the city of Cotonou in Benin.
Materials and Methods
Framework of the Study
The study was conducted in Benin, a country in West Africa. It is a coastal country that covers about 115,000 km2 and has a population of 11 million spread over 12 departments. Its economic capital, Cotonou, is located in the department of Littoral. It covers an area of 79 km2 and has a resident population estimated at around 1 million. Internal road transport is provided largely (75%) by PMs.
In Benin, the profession of motorcycle driver emerged first in urban areas with the unemployment crisis and to meet an effective demand for transport. It is an informal sector activity that has not yet managed to be regulated. One of the reasons for the proliferation of PM is the relative ease of access into this business. Indeed, practicing this profession in Benin does not require any particular training. There is no training structure to become a PM, no level of education is required and there is no obligation to have a driving license. All that is required is the ability to ride a motorcycle that can be acquired by the PM himself or by working for a motorcycle owner through lease contracts. There are three kinds of PMs: those who are in the business permanently, those who do so to supplement their wages and those who go there while expecting to get a better job. In fact, the real number of PM in the country is not well known. The Integrated Modular Survey on Household Living Conditions (EMICoV) counted about 11,796 MTCs in Benin in 2007 and recent estimates put the figure at over 250,000 in 2017. In addition, a study carried out in 2012 estimated that there were 10,610 new entries registered per year in the city of Cotonou in this activity, bringing the number of PM in Cotonou from 80,000 to 160,000 between 2010 and 2013.21,22
In cities, the PMs are organized as fleets; in Cotonou, these fleets contain about 80% of the PMs.23 The fleets are small areas on the roadside, in the shade, often delimited by an enclosure (places where customers concentrate) that allow drivers to park their motorcycles safely during rest periods. These fleets are counted by city councils in their enumeration efforts and are the best structured way to find the PMs.
Concerning the accident data of the country, which are greatly underestimated,1 the national road safety center reports an annual average of 5356 road crashes between 2008 and 2015 noted by the police forces with 49.25% involving at least one motorized two-wheel vehicle.24–26 The latter constitute the majority of the rolling stock in Benin whose statistics report 479 977 motorized two-wheel vehicles registered between 2016 and 2018 out of a total of 566 277 registered vehicles, ie 84.8%. However, it should be noted that the motorized two-wheel vehicles were not required to be registered until 2014 and that their real number may still be underestimated.27,28 According to national statistics on road crashes, in 2015, out of a total of 2893 road crashes involving at least a motorcyclist, 236 concerned PM, ie nearly 10%.26
Study Design, Study Population and Sampling Procedure
It was a cross-sectional analytical study that took place from 25 March to 19 April 2019 in Cotonou. Included in the sample were PMs who were registered in a fleet and who gave their consent to participate in the study. The minimum sample size was calculated according to the Schwartz formula with a default prevalence of 50%, an accuracy of 5% and a threshold of 5%; the minimum number of subjects was estimated at 384 PMs. With a 10% increase for non-responses, we retained 430 PMs. The WHO’s two-stage adaptive cluster sampling technique was applied to select the PMs to be included in the study while respecting the rate of proportionality per fleet. The sample frame was based on the list of PM fleets in the thirteen districts of the city, provided by the Cotonou city council.
Data Collection
The data was collected by questionnaire (supplementary material). The questionnaire was administered by interviewers previously trained on the filling. The data collection tool was previously tested on PMs selected on fleets not included in the study. The respondents were contacted and interviewed on the fleets.
Variables
Three main groups of variables were explored for PMs. The first group concerned socio-demographic characteristics (age, educational level, marital status), professional characteristics (status in the profession, professional experience, possession of a driving license), and PM history of RC (RC witness experience, RC victim experience). The second group involved variables related to the level of knowledge on raising the alert in the event of an RC and first-aid knowledge. To assess knowledge on raising the alert in the event of an RC, the variables used were knowledge of the legal duty to rescue, and knowledge of at least one emergency number for an RC (police or fire service). For first-aid act knowledge, the variables were knowledge of the lateral safety position (Yes/No), knowledge of wounds and hemorrhages management (Yes/No), and knowledge of fractures management (Yes/No). The various sources of information from PMs on alert and first aid were examined. We assessed an overall level of knowledge on first aids which has been considered adequate if the PM knows at least one of the emergency phone numbers and if he knows at least a first-aid gesture among the 03 evaluated. The third group comprised the practice variables. These concerned only PMs who reported having witnessed at least one RC. Two variables were considered in this group: the act of raising the alert (Yes/No); and the practice of at least one first-aid action (Yes if reported/No). The reasons for non-practice were also explored. We also assessed an overall level of first-aid practice which was considered adequate if the PM declared having given the alert or performed a first-aid gesture. This variable mainly reflects the willingness to provide assistance, since the practices were self-reported and could not be directly observed. The overall level of first-aid knowledge and the overall level of first-aid practice were considered as the dependent variables and the associated factors were sought.
Statistical Analysis
The data were processed using the software Epi Info and Stata 15. The usual descriptive statistics were presented with comparison made with Pearson test of chi.2 The factors linked to the level of overall knowledge of first aids and the level of overall practice in first aids were selected at a threshold of 20% using the univariate analysis and were added to a multivariate logistic regression model using a descending stepwise procedure. The associations were assessed using crude odds ratios and adjusted odds ratios (AOR) with a confidence interval of 95% (CI 95%). The adequacy of the final model was tested using the Hosmer and Lemeshow test. The threshold of 5% was retained for the meaning of statistical tests.
Ethical Statement
The study protocol received internal institutional ethical approval from the Regional Institute of Public Health under the reference number 038-EPIDEMIO/IRSP/2019. Data were collected anonymously after obtaining informed and written consent from the PMs. Confidentiality was respected for data processing.
Results
Descriptive Characteristics of PMs
The PMs in the sample were all middle aged with an average age of 38.38 (±8.70). The typical profile was that of a 30- to 44-year-old (77.71%), married or living in a couple (92.29%). About a third were uneducated. A large majority owned a mobile phone (98.33%). They were mainly permanent drivers (77.57%). The average length of professional experience was 8.4 (±7.48) years with 42.52% of them having less than 5 years’ professional experience. At least 22.14% of them had at least one driving license, and more than 4 out of 10 had already had experience of at least one RC (Table 1).
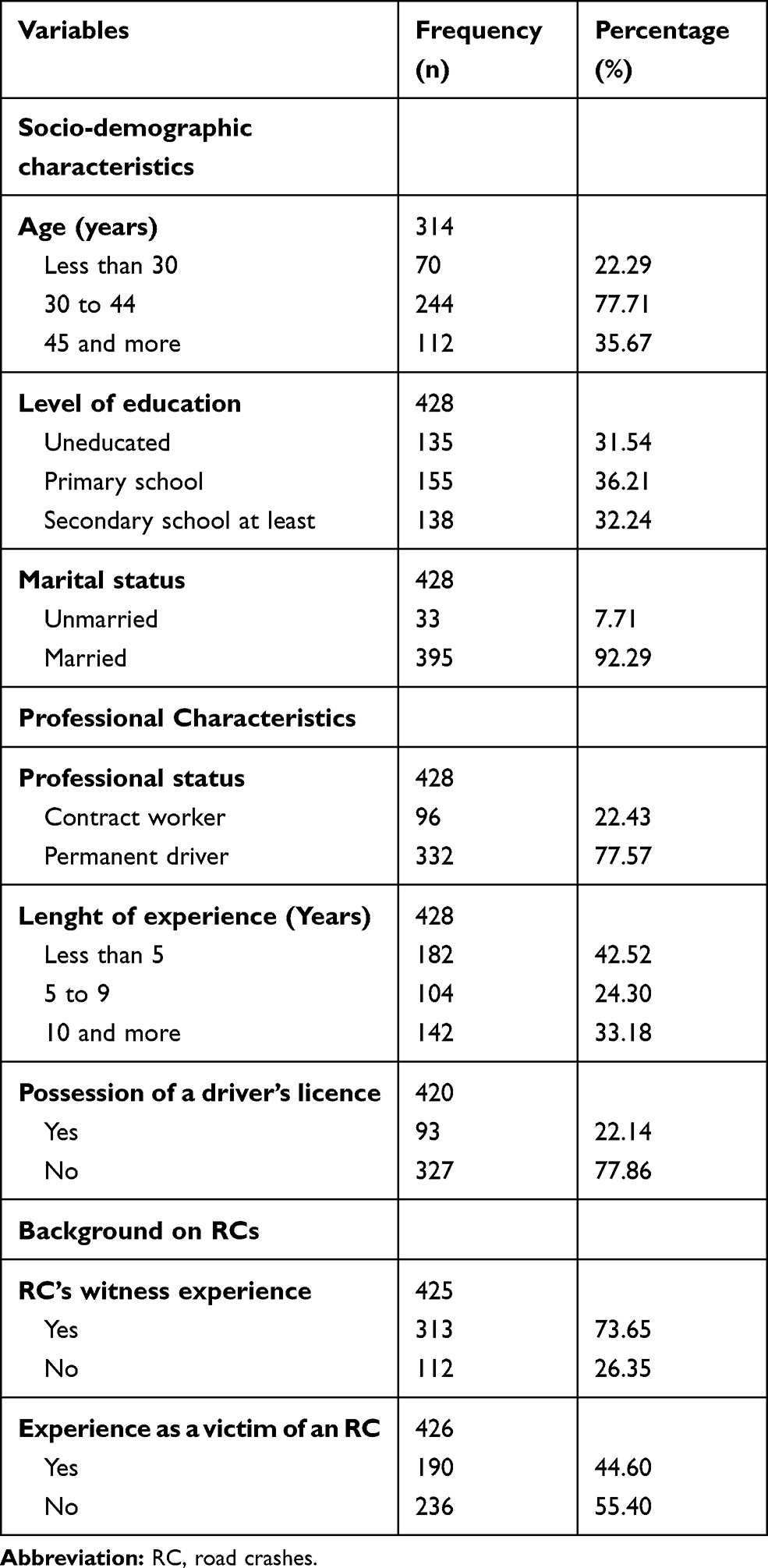 |
Table 1 Characteristics of Professional Motorcyclists, Cotonou, 2019 |
Level of Knowledge About Raising the Alert and Carrying Out First Aid in an RC
With regard to raising the alert, 93.19% of the PMs knew about the existence of legislation requiring the duty to rescue in an RC, 39.91% knew the number of the fire service and 23.94% knew the number of the police. In the sample, 62.56% of the PMs knew at least one of the emergency numbers: the police or fire service. For first responders, 49.53% of the PMs knew at least one of the 3 techniques evaluated. Specifically, 21.60% of the PMs were aware of the lateral safety position whereas the principles of management of injuries/hemorrhages was known by 13.15% of the PMs, and the management of fractures was known by 32.86% of them. There was also a small proportion of uneducated PMs who knew at least one emergency number compared to PMs with a minimum primary education level (p = 0.000). The proportion of PMs with knowledge of at least one first-aid technique was also lower in subjects under the age of 30 (p = 0.015), in those with less than 5 years of experience (p = 0.000), and in those who did not hold a driver’s license (p = 0.026). This proportion was also higher among PMs who had already experienced an RC (Table 2). About 1 out of 10 PMs reported receiving information on first responder alert and response (46 PMs) and the main source of information was training in a variety of settings. The majority of them, 93.22%, reported being interested in first-aid training.
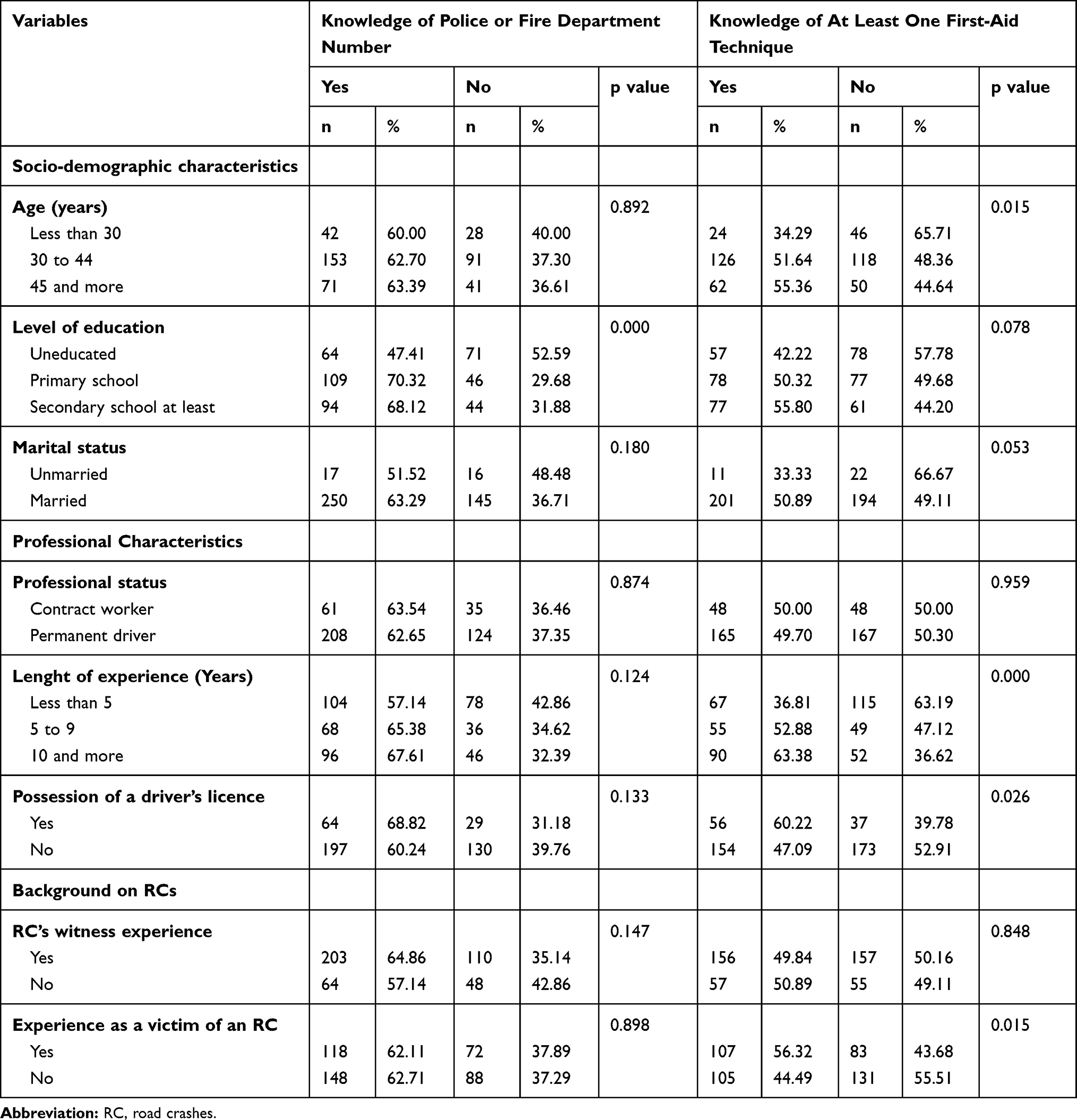 |
Table 2 Knowledge for Raising the Alert and First-Aid Techniques in PMs in the Event of an AR (n=430), Cotonou, Bénin, 2019 |
As far as the overall level of knowledge is concerned, it was adequate for 148 PMs out of the 430, ie a proportion of 34.42. After adjustment for the other variables in multivariate analysis, it appears that it is associated with the level of education with a higher probability of having an adequate overall level of knowledge among PMs with primary education (AOR: 2.77; CI 95%: 1.61–4.76) and those with minimum secondary education level (AOR: 3.11; CI 95%: 1.79–5.43) compared to uneducated PM. In the same trend, we note an association with professional seniority with a higher probability of having an adequate level of overall knowledge among PM between 5 and 10 years of seniority (AOR: 2.21; CI 95%: 1.3–3.76) and among PM with at least 10 years of seniority (AOR: 2/56; CI 95%: 1.58–4.18) compared to PM exercising for less than 5years (Table 4)
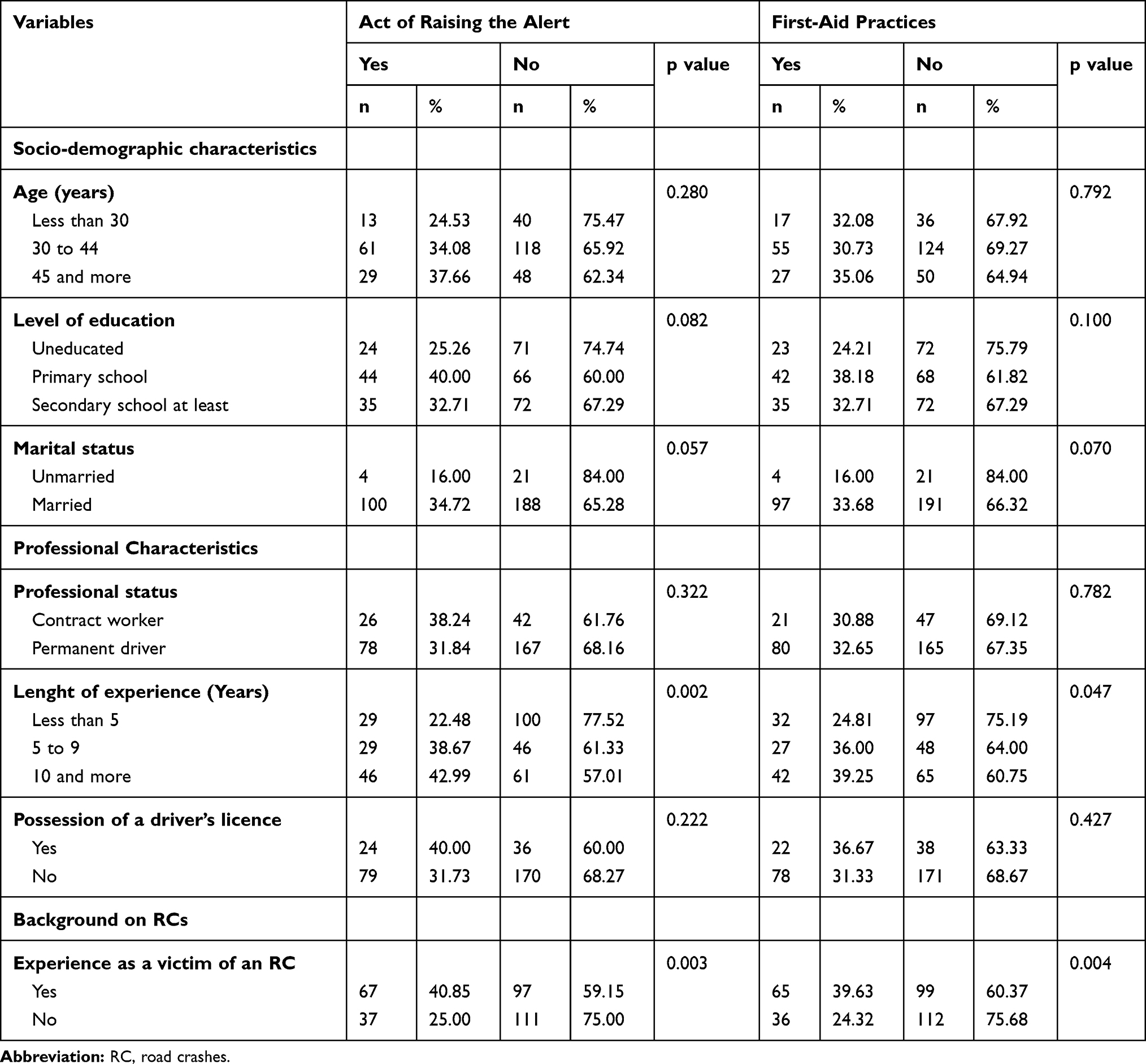 |
Table 3 Act of Raising the Alert and First-Aid Practices Among PMs Witnessing AR (n=313), Cotonou, Bénin, 2019 |
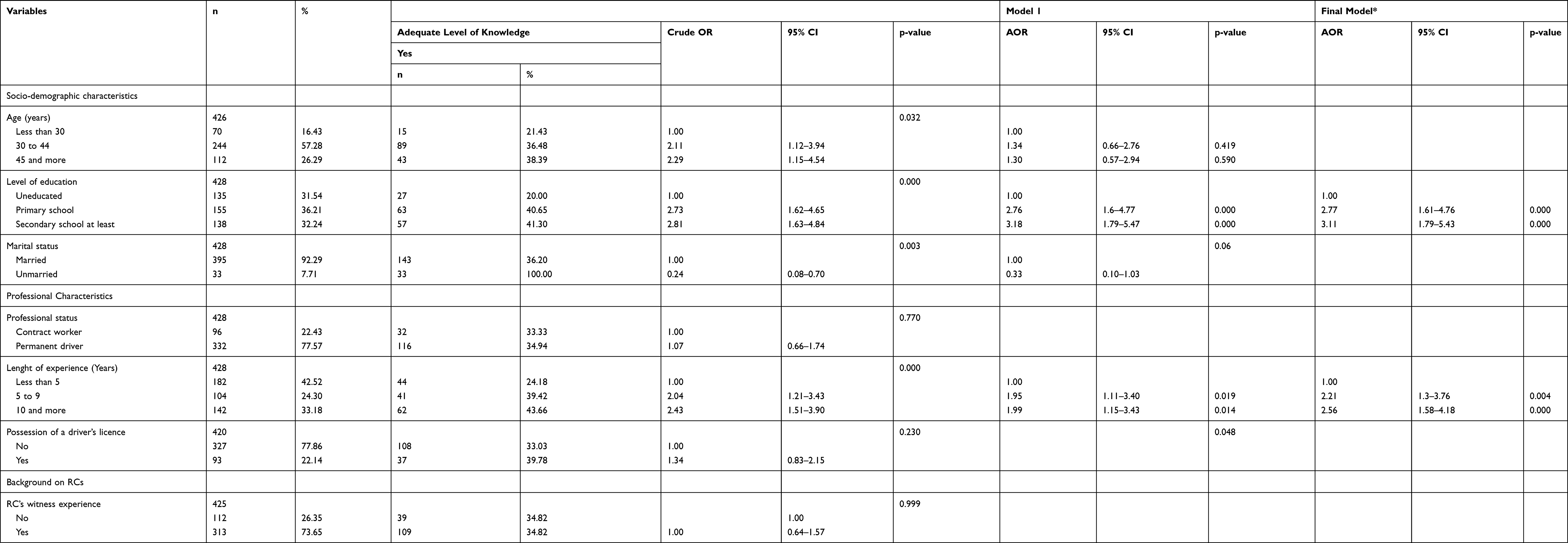 |
Table 4 Level of Knowledge in First Aids and Associated Factors Among PMs, Benin, 2019: Univariate and Multivariate Analysis (n=430) |
Alert and First-Aid Practices in Road Accidents
Of the 430 PMs, 313 (73.65%) had already witnessed at least one RC. In this group, 33.23% said they had alerted the emergency services and 32.27% said they had helped the victims by a first-aid action. The proportion of PMs reporting alert or rescue practices was lower among PMs with less than 5 years of experience (Table 3). The main reasons given for the lack of initiative of practices at RCs were lack of knowledge to act (19.64%), fear of aggravating the situation (15.18%), and the fact that first-aid response was not part of the PM’s remit (13.39%). The main reason for not raising the alert was that the alert had already been given (12/22, 54.55%).
Concerning the overall level of practice, it was adequate for 149 PMs among the 313 who declared to have witnessed at least once a road crash, ie a proportion of 47.60. In multivariate analysis, the findings reveal a statistically significant association with educational level, professional seniority and previous experience as a CR victim (Table 5). Thus, after adjustment on the other variables in multivariate analysis, it appears that it was associated with education level with a higher probability of having an adequate level of overall practice among PM with primary education level (AOR: 2.61; CI 95%: 1.42–4.77) and those with minimum secondary education level (AOR: 1.90; CI 95%: 1.05–3.46) compared to uneducated PM. In the same trend, there is an association with professional seniority with a higher probability of having an adequate level of overall practice among PM with between 5 and 10 years of seniority (AOR: 2.16; CI 95%: 1.17–3.98) and among PM with at least 10 years of seniority (AOR: 1.83; CI 95%: 1.05–3.20) compared to PM exercising for less than 5 years. Moreover, the previous experience of victim of RC is also associated with the level of practice (AOR: 2.37; CI 95%: 1.46–3.85)
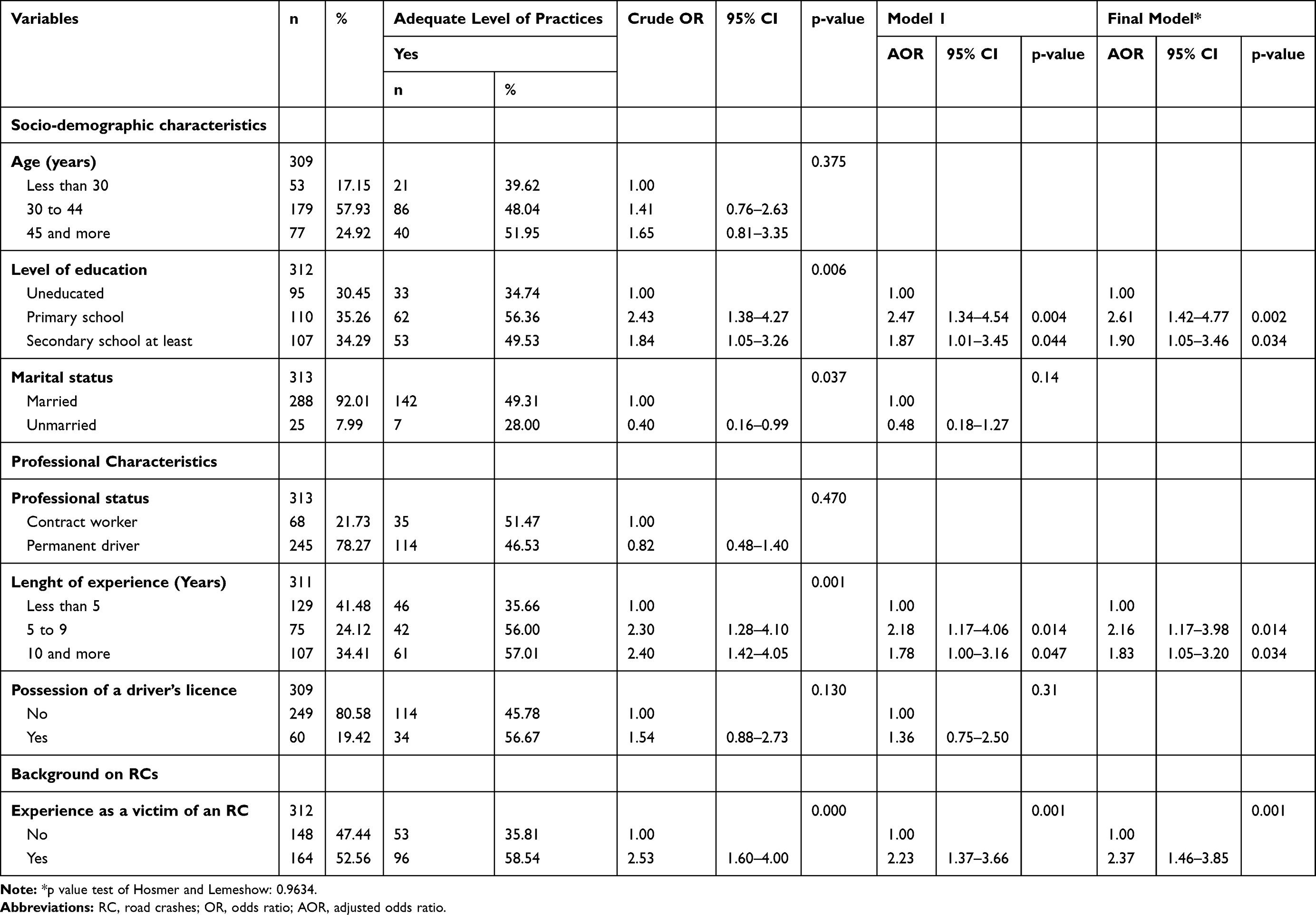 |
Table 5 Level of Practices in First Aids and Associated Factors Among PMs, Benin, 2019: Univariate and Multivariate Analysis (n=313) |
Discussion
The purpose of this study was to describe the level of knowledge and practices regarding first-aid interventions among PMs in the city of Cotonou, as part of research to find innovative ways to strengthen the immediate post-crash chain in urban areas.1,29 The results showed a satisfactory knowledge of the legal framework, and a low level of knowledge of the means of raising the alert and of first-aid techniques. In addition, the level of overall knowledge was associated with the level of education, length of experience. The level of practice was also low and the main reasons given for non-practice were related to the level of knowledge of the course of action to take in an RC.
The socio-demographic characteristics of the PMs in the sample were similar to those found in a previous study on PMs conducted in Cotonou in 2016 and confirmed that the profession of PM concerns young, exclusively male subjects with, for the most part, long-standing professional experience of 5 years.30 This profile should be an asset for ensuring the sustainability of interventions if PMs are integrated into the immediate post-crash management system, given the age of the subjects and their stability in employment. Stability is confirmed by the fact that, in this sample, more than 9 out of 10 PMs reported being permanent in the profession. In addition, about 7 out of 10 had already witnessed an RC; these figures were very close to those reported by authors in the Dominican Republic (68%) and confirm the key position of PMs in certain contexts as witnesses of RCs and as potential contributors in the management of RCs.31
As far as the level of knowledge is concerned, information on the existence of a legal duty to rescue was known by most of the PMs in the study; however, the emergency telephone numbers (police and fire service) were less well known, especially that of the police. The emergency line should be a freephone line, and if possible unique, with all the infrastructure necessary to ensure fluidity, because it was also shown that setting up a single emergency phone number could help reduce mortality related to RC.9 A real communication strategy should be deployed around it to ensure that it is as widely known as possible, as was the case in a study in India where 98.4% of the interviewed drivers knew the emergency services number.32 In our context, the police are still perceived as a source of repression, although the system implemented in the country as part of their intervention in RCs is coupled with that of the fire service, and this service is free. In addition, the populations are not sufficiently aware of these services (police and fire) and in particular their different financial and administrative implications, which can limit their use. The results of the study can therefore be explained by insufficient communication surrounding the activities of these different services in the event of RCs. The knowledge of first aid was also low in our study, which can be explained by the fact that it involves technical gestures that, although simple to learn, require some information or training. Very few PMs said that they had received any information on the subject. This observation is very close to those made in the literature on this topic. For example, in the Dominican Republic, only 15.8% of PMs had received first-aid training.31 As regards practices, the level was low and the reasons given related to self-awareness of lack of skills in the matter. Nevertheless, the findings show an adequate level of practices (self-reported) among almost 50% of PMs who declared to have witnessed at least once a road crash. This indicates a certain willingness within the group to assist in case of RC. It was also noted that work experience, education, driver license and RC victim experience were factors in favor of a higher level of knowledge or practice. This is because these are all skill-building factors. The relationship between the level of education and the level of first-aid knowledge was confirmed by the works of the literature especially in Tanzania.10 Indeed, education improves access to information, while professional experience strengthens acquisition, and driver training provides specific information on road safety issues that also offers basic information on first aid. The role of training in the implementation of first-aid procedures in RCs has been demonstrated by the literature, not only as a factor for improving knowledge, but also as a trigger for practices in real-life situations.19,20,33,34 It is therefore relevant to envisage interventions aimed at strengthening the capacity of this target group, especially since almost all the interviewees expressed interest in this type of training, as was reported in the Dominican Republic, Nigeria and India.19,31,32 The efficiency of this type of intervention has been demonstrated and the experience is worth trying given the number of lives that could be potentially saved.35
As far as previous experience as a victim of an RC is concerned, it probably makes the PM aware of the situation for having personally experienced it and makes him/her more empathetic, which probably explains the association found with the level of practice.
Limitations
The results of this study provide an initial idea of the status of first-aid knowledge and practices of PMs in the city of Cotonou. They are of interest in the analysis of the opportunity of the integration of this socio-professional group in the RC first-aid chain. The limitations, however, lie in the fact that the first-aid practices were self-reported and the study was unable to assess by observation the real level of practice of first-aid technical procedures. A possible information bias, which may lead to a possible overestimation of the indicators, cannot be ruled out on this aspect. This does not, however, affect the conclusions for guiding strategic decisions.
Conclusion
This study showed that the level of knowledge and practices of PMs in first aid is low in the city of Cotonou. However, coherent and relevant avenues for the possible integration of this socio-professional group as a link in the first-aid chain in RCs were identified. These factors must be considered in the strategic analysis for improving the first-aid chain in RCs in Benin.
Acknowledgments
The authors are sincerely grateful to all participants and authorities.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global Status Report on Road Safety 2018. Geneve: WHO; 2018.
2. World Health Organization. Rapport mondial sur la prévention des traumatismes dus aux accidents de la circulation: Résumé. Genève: WHO; 2004.
3. Hussain LM, Redmond AD. Are pre-hospital deaths from accidental injury preventable? BMJ. 1994;308(6936):1077–1080. doi:10.1136/bmj.308.6936.1077
4. Henry JA, Reingold AL. Prehospital trauma systems reduce mortality in developing countries: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2012;73(1):261–268. doi:10.1097/TA.0b013e31824bde1e
5. Harmsen AM, Giannakopoulos GF, Moerbeek PR, Jansma EP, Bonjer HJ, Bloemers FW. The influence of prehospital time on trauma patients outcome: a systematic review. Injury. 2015;46(4):602–609. doi:10.1016/j.injury.2015.01.008
6. Mahama MN, Kenu E, Bandoh DA, Zakariah AN. Emergency response time and pre-hospital trauma survival rate of the national ambulance service, Greater Accra (January - December 2014). BMC Emerg Med. 2018;18(1):33. doi:10.1186/s12873-018-0184-3
7. Ibrahim NA, Ajani AWO, Mustafa IA, et al. Road traffic injury in Lagos, Nigeria: assessing prehospital care. Prehosp Disaster Med. 2017;32(4):424–430. doi:10.1017/S1049023X17006410
8. Adeloye D. Prehospital trauma care systems: potential role toward reducing morbidities and mortalities from road traffic injuries in Nigeria. Prehosp Disaster Med. 2012;27(6):536–542. doi:10.1017/S1049023X12001379
9. Nazif-Munoz JI, Puello A, Williams A, Nandi A. Can a new emergency response system reduce traffic fatalities? The case of the 911-emergency response system in the Dominican Republic. Accident Anal Prev. 2020;143:105513. doi:10.1016/j.aap.2020.105513
10. Lukumay GG, Ndile ML, Outwater AH, et al. Provision of post-crash first aid by traffic police in Dar es Salaam, Tanzania: a cross-sectional survey. BMC Emerg Med. 2018;18(1):45. doi:10.1186/s12873-018-0199-9
11. Oliver GJ, Walter DP, Redmond AD. Prehospital deaths from trauma: are injuries survivable and do bystanders help? Injury. 2017;48(5):985–991. doi:10.1016/j.injury.2017.02.026
12. Oliver GJ, Walter DP, Redmond AD. Are prehospital deaths from trauma and accidental injury preventable? A direct historical comparison to assess what has changed in two decades. Injury. 2017;48(5):978–984. doi:10.1016/j.injury.2017.01.039
13. Kureckova V, Gabrhel V, Zamecnik P, Rezac P, Zaoral A, Hobl J. First aid as an important traffic safety factor – evaluation of the experience–based training. Eur Transport Res Rev. 2017;9(1):5. doi:10.1007/s12544-016-0218-4
14. Larsson EM, Martensson NL, Alexanderson KA. First-aid training and bystander actions at traffic crashes–a population study. Prehosp Disaster Med. 2002;17(3):134–141. doi:10.1017/S1049023X00000352
15. Shrivastava SR, Pandian P, Shrivastava PS. Pre-hospital care among victims of road traffic accident in a rural area of Tamil Nadu: a cross-sectional descriptive study. J Neurosci Rural Pract. 2014;5(Suppl1):S33–38.
16. Balhara KS, Bustamante ND, Selvam A, et al. Bystander assistance for trauma victims in low- and middle-income countries: a systematic review of prevalence and training interventions. Prehosp Emerg Care. 2019;23(3):389–410. doi:10.1080/10903127.2018.1513104
17. Alemshet AT, Zewdie AA. Knowledge, attitude and practice of first aid and factors associated with practice among taxi drivers in Addis Ababa, Ethiopia. Ethiop J Health Dev. 2017;31(3):200–227.
18. Ndile ML, Lukumay GG, Bolenius K, Outwater AH, Saveman B-I, Backteman-Erlanson S. Impact of a postcrash first aid educational program on knowledge, perceived skills confidence, and skills utilization among traffic police officers: a single-arm before-after intervention study. BMC Emerg Med. 2020;20(1):21. doi:10.1186/s12873-020-00317-y
19. Olumide AO, Asuzu MC, Kale OO. Effect of first aid education on first aid knowledge and skills of commercial drivers in South West Nigeria. Prehosp Disaster Med. 2015;30(6):579–585. doi:10.1017/S1049023X15005282
20. Vakili MA, Mohjervatan A, Heydari ST, et al. The efficacy of a first aid training course for drivers: an experience from northern Iran. Chin J Traumatol. 2014;17(5):289–292.
21. Institut National de la Statistique et de l’Analyse Economique. Enquête Modulaire Intégrée sur les Conditions de Vie des ménages (Emicov) Bénin 2007: Rapport Général d’Analyse. Cotonou; 2009.
22. Unlocking Public and Private Finance for Poor. Les Zem, ambassadeurs du paiement mobile au Bénin. Vol. 2020. Cotonou;2017.
23. Marchais G. Règles publiques, règles privées: les taxis-motos au Bénin. L’Economie Politique. 2009;41(1):59–68. doi:10.3917/leco.041.0059
24. Centre National de Sécurité Routière. Annuaire des statistiques des accidents de la voie publique, Bénin. Cotonou: CNSR; 2013.
25. Centre National de Sécurité Routière. Annuaire des statistiques des accidents de la voie publique, Bénin. Cotonou: CNSR; 2014.
26. Centre National de Sécurité Routière. Annuaire des statistiques des accidents de la voie publique, Bénin. Cotonou: CNSR; 2015.
27. Ministère des Infrastructures et des Transports. Statistiques nationales des immatriculations de 1981 à 2018. Cotonou: MIT; 2019.
28. Ministère des Infrastructures et des Transports. Annuaire des Statistiques 2013-2016. Cotonou: MIT; 2017.
29. World Health Organization. Plan Mondial Pour La Décennie d’Action Pour La Sécurité Routière 2011-2020. Geneve: WHO; 2010.
30. Lawin H, Ayi Fanou L, Hinson V, Tollo B, Fayomi B, Ouendo EM. [Occupational risk factors and perceptions of air pollution by motorcycle taxi drivers in Cotonou, Benin]. Sante Publique (Paris). 2018;30(1):125–134. doi:10.3917/spub.181.0125
31. Arellano N, Mello MJ, Clark MA. The role of motorcycle taxi drivers in the pre-hospital care of road traffic injury victims in rural Dominican Republic. Inj Prev. 2010;16(4):272–274. doi:10.1136/ip.2009.025627
32. Awasthi S, Pamei G, Solanki HK, Kaur A, Bhatt M. Knowledge, attitude, and practice of first aid among the commercial drivers in the Kumaon region of India. J Family Med Prim Care. 2019;8(6):1994–1998. doi:10.4103/jfmpc.jfmpc_295_19
33. Arbon P, Hayes J, Woodman R. First aid and harm minimization for victims of road trauma: a population study. Prehosp Disaster Med. 2011;26(4):276–282. doi:10.1017/S1049023X11006522
34. Stromme H, Jeppesen E, Reinar LM. NIPH Systematic Reviews: executive Summaries. In: First Aid Training May Improve First Aid Skills. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2015. Available from: https://www.ncbi.nlm.nih.gov/books/NBK390580/pdf/Bookshelf_NBK390580.pdf.
35. Jayaraman S, Mabweijano JR, Lipnick MS, et al. First things first: effectiveness and scalability of a basic prehospital trauma care program for lay first-responders in Kampala, Uganda. PLoS One. 2009;4(9):e6955. doi:10.1371/journal.pone.0006955
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.