")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Can Pharmacists’ Counseling Improve the Use of Inhalers and Quality of Life? A Prospective “Pre” and “Post” Education Analysis in Mardan, Pakistan
Authors Gul S, Rehman IU, Goh KW, Ali Z, Rahman AU, Khalil A, Shah I, Khan TM, Ming LC
Received 25 January 2023
Accepted for publication 5 May 2023
Published 6 July 2023 Volume 2023:16 Pages 679—687
DOI https://doi.org/10.2147/JAA.S405943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Luis Garcia-Marcos
Sumaira Gul,1 Inayat Ur Rehman,1 Khang Wen Goh,2 Zahid Ali,3 Aziz Ur Rahman,4 Asad Khalil,5 Ismail Shah,1 Tahir Mehmood Khan,6 Long Chiau Ming7,8
1Department of Pharmacy, Garden Campus, Abdul Wali Khan University Mardan, Khyber Pakhtunkhwa, Pakistan; 2Faculty of Data Science and Information Technology, INTI International University, Nilai, Malaysia; 3Department of Pharmacy, University of Peshawar, Peshawar, Pakistan; 4Department of Urology, North West General Hospital and Research Center Peshawar, Peshawar, Pakistan; 5Department of Medicine, Lady Reading Hospital, Peshawar, Pakistan; 6Institute of Pharmaceutical Sciences, University of Veterinary and Animal Sciences Lahore, Lahore, Pakistan; 7PAP Rashidah Sa’adatul Bolkiah Institute of Health Sciences, Universiti Brunei Darussalam, Gadong, Brunei Darussalam; 8School of Medical and Life Sciences, Sunway University, Sunway City, Malaysia
Correspondence: Inayat Ur Rehman, Department of Pharmacy, Garden Campus, Abdul Wali Khan University Mardan, Khyber Pakhtunkhwa, 23200, Pakistan, Email [email protected] Long Chiau Ming, School of Medical and Life Sciences, Sunway University, Sunway City, Selangor, 47500, Malaysia, Email [email protected]
Introduction: Asthma is one of the common major non-communicable respiratory diseases, and is associated with a lower health-related quality of life (QOL). Poor inhalation is a significant contributing factor to poor control of asthma. Community pharmacist has a vital role to play in assisting patients and ultimately improving their asthma conditions through the use of inhalers.
Aim: This study aimed to assess the effectiveness of “pre” and “post” educational intervention by a community pharmacist within a community pharmacy on asthma patients’ QOL, inhaler technique, and adherence to therapy during the endemic phase of COVID-19.
Methods: A “pre” and “post” interventional study was performed at a community pharmacy in the city of Mardan, Pakistan, in 2022 during the COVID-19 pandemic. Patients were divided into two groups, ie control and pharmacist-led education groups. After assigning patients to both groups, the baseline data were collected and followed for one month to compare the reduction in errors in the use of inhalers, QOL, and adherence to therapy. A paired sample t-test was performed, keeping a p-value < 0.05 as statistical significance.
Results: A total of 60 patients were recruited, majority (58.3%) were females, and 28.3% were from the age group of 46– 55 years old. A statistically significant difference was observed in the pre- and post-education QOL score among patients in the pharmacist-led education group, from a mean ± SD at pre-education of 40.23± 10.03 to a mean±SD at post-education of 48.10± 5.68. Similarly, a statistically significant difference was observed for the correct use of inhalers, ie MDIs and DPIs. Similarly, a statistically significant difference was observed in the adherence status between pre-education and post-education by pharmacists.
Conclusion: The findings of the study revealed a positive impact of community pharmacist-led education on QOL, inhaler technique, and adherence to therapy among patients with asthma.
Keywords: adherence, asthma, community pharmacist, pharmacist-led education, quality of life, Pakistan
Corrigendum for this paper has been published.
Introduction
Chronic respiratory diseases such as asthma are the biggest threat to health worldwide, especially in developing countries.1 The prevalence of asthma is increasing at a very alarming rate due to rapid urbanization, lifestyle modification, and industrialization.2 Globally, there are approximately 334 million asthma cases, and its prevalence is increasing year by year.3 Prevalence and mortality of asthma vary geographically with higher cases observed in developed countries; however high mortality is observed in developing countries too.4 Asthma is among the most common major non-communicable respiratory diseases which are associated with poor health-related quality of life (QOL).5,6
Among patients with asthma, poor inhalation is a significant contributing factor toward poor control of the disease because of inadequate dosing of the prescribed medication.7 Asthma has a great impact on the population, socially as well as economically, and when asthma is poorly controlled it may lead to considerable economic impact with frequent hospital admissions, poor QOL, and ultimately death.8 Adherence to therapy plays an important role in the overall health of the patient. 24% of exacerbations and almost 60% of hospitalizations resulting from asthma-related issues are due to poor adherence to therapy.9 Adherence to controller medication for the management of asthma is critical. The literature revealed medication adherence toward the controller medication is constantly low,10–14 and poor medication adherence is a major challenge for asthma resulting from complex therapeutic regimens.15 Various reasons contribute to non-adherence to therapy, including poor knowledge of the proper and appropriate use of inhalers, forgetfulness, and misconceptions about asthma’s long-term impacts on health.13,16,17 Other than these, several other factors also play a contributing role in the non-adherence to therapy including complex regimens, side effects associated with therapy, high cost of medication, in some cases dislike of medication, and distant pharmacies.13,18,19 It is extremely important to counsel patients through video instruction programs or lecturing on proper techniques for inhaler use to optimize their treatment.20
Pharmacists have a very important role in delivering both the initial training to asthma patients regarding the first-time use of an inhaler, and the subsequent regular follow-up retraining of patients.21,22 Community pharmacists can play a significant, positive role in the health of patients who live in rural areas and are isolated because of limited access to primary health-care facilities.23,24 More particularly, in some countries community pharmacists are specifically placed for the regular checking of inhaler techniques in case of new inhaler prescriptions or refills; pharmacist interventions significantly assist in improving the inhaler technique of asthma patients.25–27 Pharmacist-led interventions among patients with asthma enable these patients to enhance their inhaler technique, thus contributing to improved medication adherence, asthma control and QOL.28,29 Furthermore, the pharmacist’s education and counseling role can lead to improved asthma control and, overall, enable asthma patients to have a fully active and productive life.30 Poor asthma control results from delivery of sub-therapeutic doses due to improper inhalation techniques.31
Various studies in Pakistan documented that in patients with asthma an improper inhalation technique persisted, leading to poor compliance and uncontrolled asthma status.6,32–35 Consultants and physicians are overburdened in Pakistan, so a community pharmacist’s role is vital to assist patients and ultimately improve the asthma conditions of patients using inhalers. This study aimed to assess the effectiveness of a pharmacist-led education intervention by a community pharmacist on QOL, inhaler technique, and adherence to therapy among patients with asthma during the endemic phase of COVID-19.
Method
Study Design
This study had a pre–post study design, in order to assess the effectiveness of a pharmacist-led education intervention by a community pharmacist in a community pharmacy setting on QOL, inhaler technique, and adherence to therapy among patients with asthma. The study was performed in 2022 during the endemic phase of COVID-19, when a surge of respiratory-related diseases was observed. The counseling was performed by a registered pharmacist working in a community pharmacy in the city of Mardan, Pakistan.
Eligibility Criteria
Patients who were aged 18 years or above, of both genders (male and female), clinically diagnosed with asthma, and prescribed inhalers for managing their asthma were included in the study. Patients not willing to participate in this study were excluded.
Study Procedure
The study’s purpose was explained, and patients’ consent was obtained before enrolment in the study. After consent, the patients were screened for eligibility criteria. For those who met the inclusion criteria, all the parameter data were recorded, ie age, gender, education status, marital status, socio-economic status, the severity of disease, and QOL. Patients were randomly assigned into one of two groups, ie control group and a pharmacist-led education group. After assigning patients, the baseline data were collected and one month’s follow-up was performed to compare patients’ reduction in inhaler use error, adherence to therapy and ultimately their QOL.
Ethics and Dissemination
The study was approved by the Ethical and Research Committee of Abdul Wali Khan University Mardan, Pakistan. All procedures performed in this study involved human participants following the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration. Informed written consent was obtained from all the patients who were willing to participate in this study. Furthermore, the patients were informed that they could leave the study at any time. For future reference, proper patient identity numbers were assigned to each patient. To avoid and minimize any bias in the study all the data were kept highly confidential.
Measurement Tools
Demographics data: A demographic data sheet was designed to collect data on patients related to age, gender, education status, weight, employment status, marital status, socioeconomic status, and severity of asthma disease.
Quality of life (QOL): To evaluate the aspects of QOL, a validated tool named Functional Assessment for Non-Life-Threatening Conditions (FANLTC) was used. The FANLTC assesses 4 domains, namely physical well-being, social/family well-being, emotional well-being, and functional well-being. Each item of these 4 domains of FANLTC is scored from 0 to 4, where 0 is considered as “not at all” while 4 is considered as “very much”. The QOL score on the FANLTC tool ranges from 0 to 104, in which a lower score represents a poor QOL while a higher one represents a better QOL.36
Metered Dose Inhalers (MDIs) and Dry Powder Inhalers (DPIs): To assess the correct and appropriate use of either MDIs or DPIs among patients with asthma, a checklist was adopted from previous literature.37 For MDIs the checklist was comprised of 8 questions, while for DPIs it was comprised of 11 questions. For each correct step, a score of 1 was awarded, while for an incorrect step a score of zero was given. To assess the correct use of inhalers among patients, the checklist used depended on whether patients were using an MDIs or DPI. The questionnaire was administered to patients in both the pharmacist-led education group and in the control group. After one month of pharmacist-led education and counseling, the checklist was administered to the same patients in both groups to assess any improvement in the correct use of inhalers.
Adherence to Inhaler Treatment
The adherence to the inhaler treatment was assessed on a ten-item questionnaire “Test of Adherence to Inhalers (TAI)”.38 The score for each item of the questionnaire ranged from 1 to 5, “where 1 was considered as the worst possible score while 5 as the greatest possible score”, thus 10 points represent a minimum score whereas 50 points a maximum score. Three stages for adherence were established along this continuum: ≤45 graded as poor, 46–49 graded as intermediate, and 50 graded as good. The scores for adherence to inhaler treatment were assessed for the two groups of patients, both at the start of the study (pre-education for the non-control group) and after one month, at the endpoint of the study (post-education).
Education/Intervention Tool
Pharmacist-led education was performed by using a leaflet as a counseling aid as well as verbal counseling about the proper use of inhalers. The counseling material was designed according to the standard reference and approved after consultation with a practicing respiratory consultant and a registered pharmacist.
Sample Size and Data Analysis
The study was a pilot study designed to assess the effectiveness of pharmacist-led education by a community pharmacist on QOL, inhaler technique, and adherence to therapy among patients with asthma in Pakistan. Therefore, no formal sample size calculation was conducted. The study aimed to recruit at least 60 patients, with 30 patients in each group, ie the control group and the pharmacist-led education group. All the data collected through the questionnaires were entered and analyzed using Software Package for Statistical Sciences (SPSS) version 21. For categorical variables, numbers and frequencies were used. Quantitative variables were represented as mean ± standard deviation and a paired sample t-test was used for comparisons between the pre- and post-data, with a p-value of <0.05 being considered statistically significant.
Results
Demographic Characteristics of Patients
A total of 60 patients with asthma were included in this study, with 30 patients in each group. The majority of the patients, n=35 (58.3%), were females, n=17 (28.3%) were from the age group of 46–55 years, and half of the patients, n=30 (50%), were uneducated. Regarding marital status, n=48 (88%) were married and n=25 (41.7%) were housewives/stay-at-home moms. About the severity status of asthma, n=35 (58.3%) of the patients were categorized as having persistent-moderate asthma (See Table 1 for details).
 |
Table 1 Demographic Characteristic of Included Patients |
Assessment of QOL of Patients with Asthma
The quality of life of patients with asthma was assessed by using a validated tool named FANLTC. In the pharmacist-led education group, the mean ± standard deviation at pre-education was 40.23 ± 10.03 and at post-education was 48.10 ± 5.68. A statistically significant difference was observed in the mean scores of the patients between pre- and post-education, with p=<0.001, while no statistically significant difference was observed between pre- and post-education for the control group of patients (See Table 2 for details).
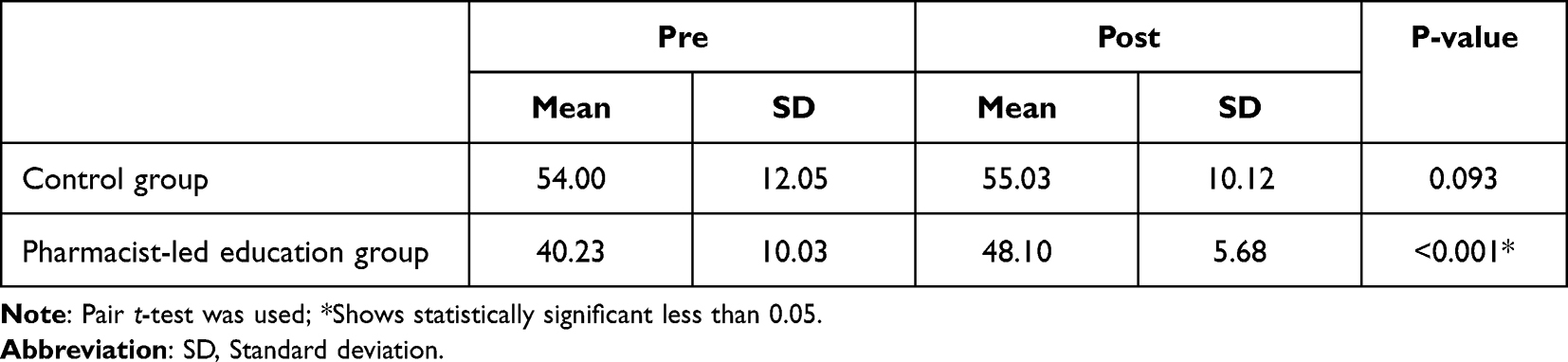 |
Table 2 Pre and Post Comparison of Quality of Life Score in Both Groups |
Assessment of Inhalation Technique at Pre- and Post-Education
Among n=30 patients with asthma in the pharmacist-led education group, n=17 were using MDIs and n=13 were using DPIs. In this group, the patients were given counseling and education about the correct use of inhalers prescribed to them. A statistically significant difference was observed in the correct use of inhalers for both MDIs (from mean ± standard deviation of 4.65 ± 0.70 to 5.65 ± 1.54) and DPIs (from 6.00 ± 1.00 to 6.85 ± 10.7), with p=0.003 and p=0.002, respectively. In the control group, no statistically significant difference was observed (see Table 3 for details).
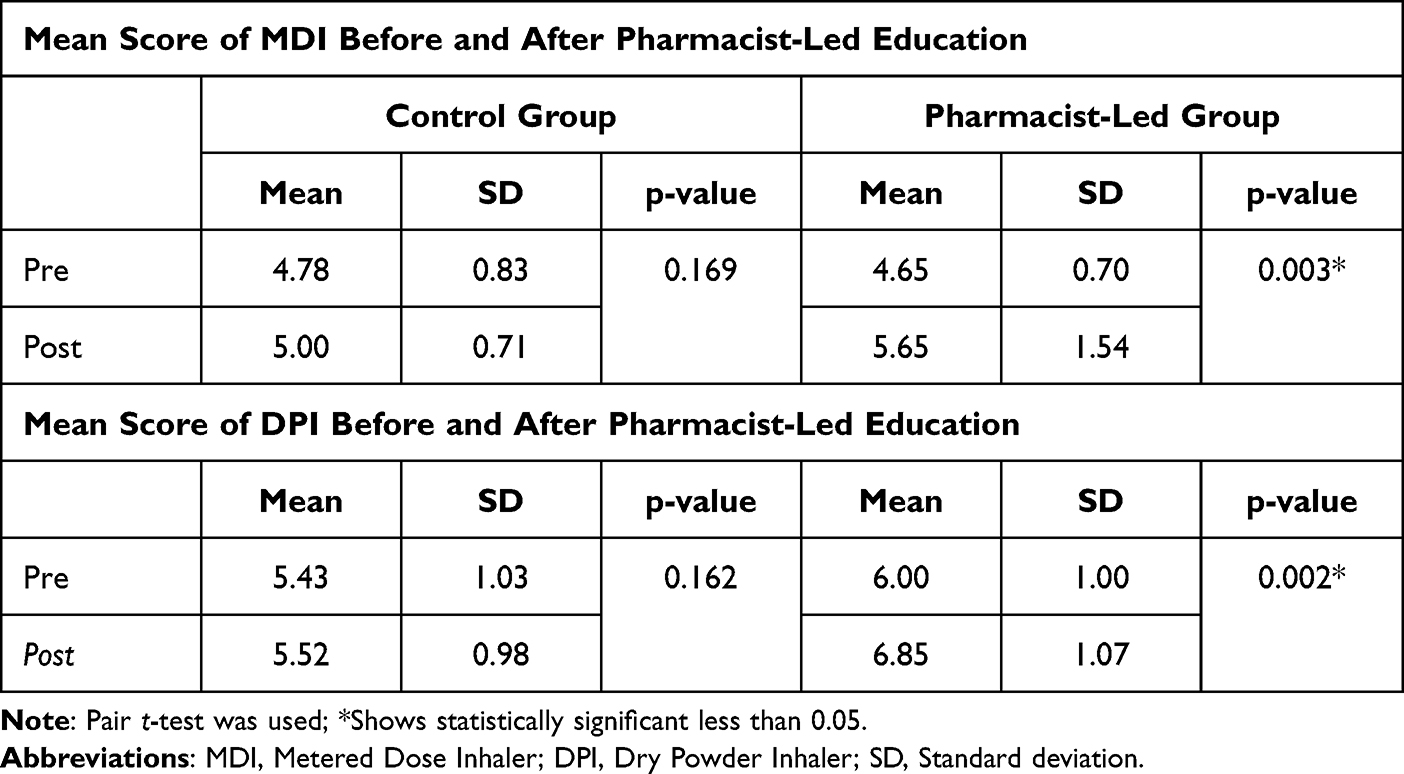 |
Table 3 Pre and Post Comparison for the Mean Score of MDI and DPI in Both Groups |
Adherence to Inhaler Treatment
The adherence to inhaler treatment was assessed by using the ten-item questionnaire “Test of Adherence to Inhalers” (TAI). The pharmacist-led education and counseling showed that a good number of patients shifted from poor adherence to intermediate or good adherence, thus showing an improvement in the adherence status of patients toward their medication. Also, a statistically significant difference was observed in the adherence status between pre- and post-education by pharmacists, namely p=0.003, while no statistically significant difference was observed in patients of the control group (see Table 4 for details).
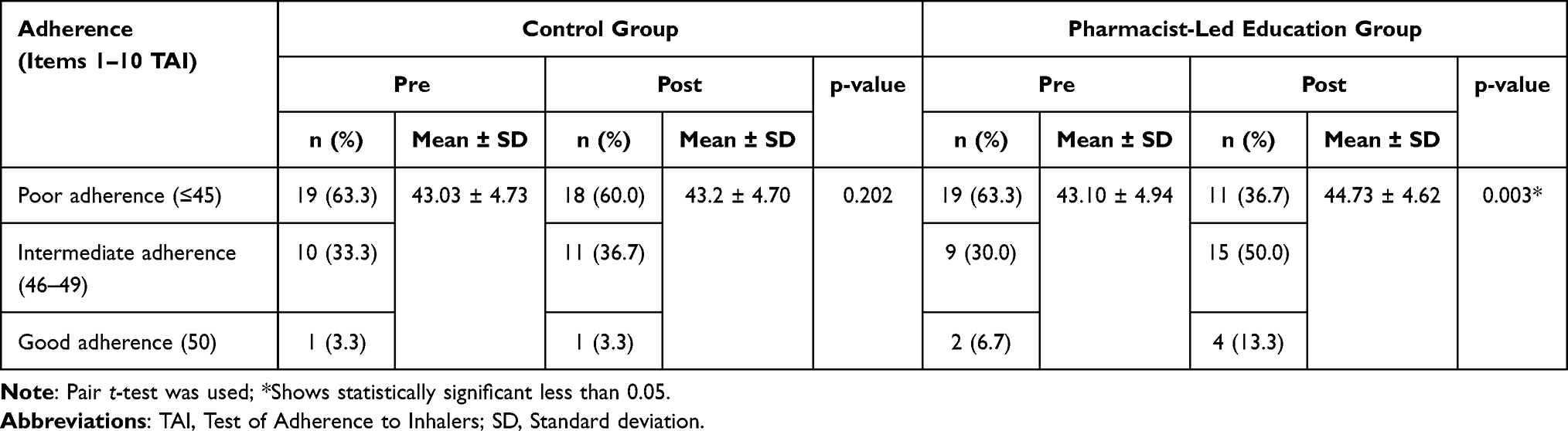 |
Table 4 Pre and Post Comparison for Adherence to Inhaler Use in Both Groups |
Discussion
Asthma is a common major non-communicable respiratory disease leading to compromised health-related quality of life. Among patients with asthma, inadequate use of prescribed inhaler medication contributes significantly to inadequate dosing of these medications, and ultimately leads to poor control of asthma.
To the best of our knowledge, the current study is the first of its kind to evaluate the impact of pharmacist-led education by a community pharmacist on QOL, inhaler technique, and adherence to therapy among patients with asthma in a community pharmacy in Pakistan. Despite the availability of various drug therapies for asthma, symptoms in the majority of patients are uncontrolled, and they present with poor QOL, mainly due to the incorrect use of inhalational techniques. A study conducted in Pakistan reported that the majority of patients with asthma have compromised QOL due to incorrect inhaler technique.6 Studies have also shown that patients having improper inhaler techniques are more prone to frequent hospitalizations and have poorly controlled asthma.39 Another study conducted in Pakistan reported poor health-related QOL among patients with asthma.40 In the present study, we found significant improvement in patients’ QOL in the pharmacist-led education group compared to the control group. Similar results are also reported by a study conducted in Nepal which found significant improvement in QOL of asthma patients as a result of pharmacist-led intervention.41 Other studies also reported that pharmacist-led intervention can improve patients’ QOL.28,42 However, one study reported no improvement in QOL of patients with asthma following pharmacist-led intervention.43 The difference in results may be attributed to the nature of the education/intervention provided by the pharmacists.
Our study findings showed statistically significant improvement regarding the correct use of inhalers, in terms of mean scores for both MDIs and DPIs, which is in agreement with other studies which also reported significant improvement in patients’ proper use of inhalers after following pharmacist instructions.28,44–46
Adherence to asthma medication is crucial for its optimum outcomes. Our findings also showed a statistically significant difference in the adherence status between pre- and post-education by the pharmacist. A decent number of patients shifted from poor adherence to intermediate adherence and good adherence, thus showing an improvement in the adherence status of patients toward medication. Similar results were reported by Yadav et al,41 where pharmacist-led intervention resulted in patients’ significantly improved adherence to therapy and proper inhalation technique. Another study by Mehuys et al reported similar results.45 A recent study, conducted in 2022, concluded that an individualized educational intervention can improve adherence to therapy among patients with asthma.47 Furthermore, a systematic review and meta-analysis conducted in 2020 compared the impact of the pharmacist-led intervention on adherence to therapy in asthma/COPD patients between the pharmacist-led intervention group and control group, and concluded that adherence to therapy is significantly increased in the pharmacist-led intervention group vs control group.48
Strengths and Limitations
Our study showed a positive impact of community pharmacist-led education on QOL, inhaler technique, and adherence to therapy among patients with asthma. Therefore, it demonstrated the value of a community pharmacist working with patients with asthma in a community pharmacy to improve inhalation techniques and adherence to therapy, reducing hospitalizations and frequent visits to the emergency department associated with improper inhaler use and poor adherence to therapy, and thus leading to an improved QOL. However, the results of this study should be confirmed through larger studies.
Conclusion
Our study demonstrated a positive impact of pharmacist-led education intervention on quality of life, inhaler techniques, and adherence to therapy in a community pharmacy among patients with asthma. Therefore, community pharmacists could play an important role in reducing frequent hospitalizations by improving quality of life, adherence to therapy, and inhalation techniques among patients with asthma.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach. World Health Organization; 2007. Available from: https://apps.who.int/iris/bitstream/handle/10665/43776/9789241563468_eng.pdf?sequence=1.
2. Rashmi R, Kumar P, Srivastava S, Muhammad T. Understanding socio-economic inequalities in the prevalence of asthma in India: an evidence from national sample survey 2017–18. BMC Pulm Med. 2021;21(1):1–12. doi:10.1186/s12890-021-01742-w
3. Enilari O, Sinha S. The global impact of asthma in adult populations. Ann Glob Health. 2019;85(1). doi:10.5334/aogh.2412
4. To T, Stanojevic S, Moores G, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health. 2012;12(1):1–8. doi:10.1186/1471-2458-12-204
5. Dharmage SC, Perret JL, Custovic A. Epidemiology of asthma in children and adults. Front Pediatr. 2019;7:246. doi:10.3389/fped.2019.00246
6. Hashmi A, Soomro JA, Memon A, Soomro TK. Incorrect inhaler technique compromising quality of life of asthmatic patients. J Med. 2012;13(1):16–21. doi:10.3329/jom.v13i1.7980
7. Basheti IA, Armour CL, Reddel HK, Bosnic-Anticevich SZ. Long-term maintenance of pharmacists’ inhaler technique demonstration skills. Am J Pharm Educ. 2009;73(2):32. doi:10.5688/aj730232
8. Rasheed W, Khan RN. Assessment of factors affecting symptom control in asthmatic patients. J Dow Univ Health Sci. 2020;14(3):126–132. doi:10.36570/jduhs.2020.3.1028
9. Bårnes CB, Ulrik CS. Asthma and adherence to inhaled corticosteroids: current status and future perspectives. Respir Care. 2015;60(3):455–468. doi:10.4187/respcare.03200
10. Gamble J, Stevenson M, McClean E, Heaney LG. The prevalence of nonadherence in difficult asthma. Am J Respir Crit Care Med. 2009;180(9):817–822. doi:10.1164/rccm.200902-0166OC
11. Desai M, Oppenheimer JJ. Medication adherence in the asthmatic child and adolescent. Curr Allergy Asthma Rep. 2011;11(6):454–464. doi:10.1007/s11882-011-0227-2
12. Jentzsch N, Camargos P, Colosimo E, Bousquet J. Monitoring adherence to beclomethasone in asthmatic children and adolescents through four different methods. Allergy. 2009;64(10):1458–1462. doi:10.1111/j.1398-9995.2009.02037.x
13. Bender BG, Bender SE. Patient-identified barriers to asthma treatment adherence: responses to interviews, focus groups, and questionnaires. Immunol Allergy Clin. 2005;25(1):107–130.
14. Jácome C, Almeida R, Pereira AM, et al. Monitoring adherence to asthma inhalers using the InspirerMundi app: analysis of real-world, medium-term feasibility studies. Front Med Technol. 2021;32:154.
15. Jácome C, Almeida R, Pereira AM, et al. Monitoring adherence to asthma inhalers using the InspirerMundi app: analysis of real-world, medium-term feasibility studies. Front Med Technol. 2021;3:649506. doi:10.3389/fmedt.2021.649506
16. Howell G. Nonadherence to medical therapy in asthma: risk factors, barriers, and strategies for improving. J Asthma. 2008;45(9):723–729. doi:10.1080/02770900802395512
17. Ponieman D, Wisnivesky JP, Leventhal H, Musumeci-Szabó TJ, Halm EA. Impact of positive and negative beliefs about inhaled corticosteroids on adherence in inner-city asthmatic patients. Annals Allergy Asthma Immunol. 2009;103(1):38–42. doi:10.1016/S1081-1206(10)60141-X
18. Dima AL, Hernandez G, Cunillera O, Ferrer M, de Bruin M. Asthma inhaler adherence determinants in adults: systematic review of observational data. Eur Respir J. 2015;45(4):994–1018. doi:10.1183/09031936.00172114
19. Aberhe W, Hailay A, Zereabruk K, Mebrahtom G, Haile T. Non-adherence to inhaled medications among adult asthmatic patients in Ethiopia: a systematic review and meta-analysis. Asthma Res Pract. 2020;6(1):1–8. doi:10.1186/s40733-020-00065-7
20. Von Schantz S, Katajavuori N, Juppo AM. The use of video instructions in patient education promoting correct technique for dry powder inhalers: an Investigation on Inhaler-Naïve Individuals. Pharmacy. 2018;6(4):106. doi:10.3390/pharmacy6040106
21. Basheti IA, Reddel HK, Armour CL, Bosnic-Anticevich SZ. Improved asthma outcomes with a simple inhaler technique intervention by community pharmacists. J Allergy Clin Immunol. 2007;119(6):1537–1538. doi:10.1016/j.jaci.2007.02.037
22. Basheti IA, Salhi YB, Basheti MM, Hamadi SA, Al-Qerem W. Role of the pharmacist in improving inhaler technique and asthma management in rural areas in Jordan. Clin Pharmacol. 2019;11:103. doi:10.2147/CPAA.S213271
23. Wibowo Y, Berbatis C, Joyce A, Sunderland VB. Analysis of enhanced pharmacy services in rural community pharmacies in Western Australia. Rural Remote Health. 2010;10(3):1–9.
24. Saini B, Filipovska J, Bosnic‐Anticevich S, Taylor S, Krass I, Armour C. An evaluation of a community pharmacy‐based rural asthma management service. Austral J Rural Health. 2008;16(2):100–108. doi:10.1111/j.1440-1584.2008.00975.x
25. Ruud KW, Rønningen SW, Faksvåg PK, Ariansen H, Hovland R. Evaluation of a structured pharmacist-led inhalation technique assessment service for patients with asthma and COPD in Norwegian pharmacies. Patient Educ Couns. 2018;101(10):1828–1837. doi:10.1016/j.pec.2018.05.018
26. Makhinova T, Walker BL, Gukert M, Kalvi L, Guirguis LM. Checking inhaler technique in the community pharmacy: predictors of critical errors. Pharmacy. 2020;8(1):6. doi:10.3390/pharmacy8010006
27. Hasan S, Al Oum L, Hassan NA. A simulated patient study to evaluate community pharmacist assessment, management and advice giving to patients with asthma. J Pharma Policy Pract. 2021;14(1):1–10. doi:10.1186/s40545-020-00294-4
28. Petkova VB. Pharmaceutical care for asthma patients: a community pharmacy-based pilot project.
29. Poudel RS, Piryani RM, Shrestha S, Prajapati A. Benefit of hospital pharmacy intervention on the current status of dry powder inhaler technique in patients with asthma and COPD: a study from the Central Development Region, Nepal. Integr Pharm Res Pract. 2017;6:7. doi:10.2147/IPRP.S119202
30. Bousquet J, Clark T, Hurd S, et al. GINA guidelines on asthma and beyond. Allergy. 2007;62(2):102–112. doi:10.1111/j.1398-9995.2006.01305.x
31. Osman A, Hassan ISA, Ibrahim MIM. Are Sudanese community pharmacists capable to prescribe and demonstrate asthma inhaler devices to patrons? A mystery patient study. Pharm Pract (Granada). 2012;10(2):110. doi:10.4321/S1886-36552012000200008
32. Farooq MZ, Farooq MS, Waqar W, Mustaqeem M, Khan JA, Saadullah S. Assessment of inhalation technique among patients of chronic respiratory disorders in Civil Hospital Karachi: a cross sectional study. J Pak Med Assoc. 2016;66(11):1502.
33. Baqai HZ, Saleem MA, Abair-ul-Haq M. Assessment of metered dose inhaler technique in patients with chronic lung disease at government hospitals of Rawalpindi. J Ayub Med Coll Abbottabad. 2011;23(1):37–39.
34. Ahmad H, Farooqi R, Ashraf S, Afridi MZ. Assessment of inhaler technique of patients admitted with acute exacerbation of chronic obstructive pulmonary disease at pulmonology unit Khyber Teaching Hospital Peshawar. KJMS. 2013;6(2):231.
35. Ahmed M, Munir M, Sufyan A, et al. Metered dose inhaler technique: a priority catch for physicians. Cureus. 2020;12(10):25.
36. Rehman IU, Chan KG, Munib S, Lee LH, Khan TM. The association between CKD-associated pruritus and quality of life in patients undergoing hemodialysis in Pakistan: a STROBE complaint cross-sectional study. Medicine. 2019;98(36):e16812. doi:10.1097/MD.0000000000016812
37. Sodhi M. Incorrect inhaler techniques in Western India: still a common problem. Int J Res Med Sci. 2017;5(8):3461–3465. doi:10.18203/2320-6012.ijrms20173541
38. Plaza V, Fernández-Rodríguez C, Melero C, et al. Validation of the “Test of the Adherence to Inhalers”(TAI) for asthma and COPD patients. J Aerosol Med Pulm Drug Deliv. 2016;29(2):142–152. doi:10.1089/jamp.2015.1212
39. Al-Jahdali H, Ahmed A, Al-Harbi A, et al. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Allergy Asthma Clinl Immunol. 2013;9(1):1–7. doi:10.1186/1710-1492-9-8
40. Malik M, Khan A, Hussain A, Hashmi A. Assessment of health-related quality of life among Asthmatic patients: the need for structured pharmaceutical care delivery system in Pakistan. J Pharm Bioallied Sci. 2017;9(4):272. doi:10.4103/JPBS.JPBS_185_17
41. Yadav A, Thapa P. Pharmacist led intervention on inhalation technique among asthmatic patients for improving quality of life in a private hospital of Nepal. Pulm Med. 2019;2019:1–9. doi:10.1155/2019/8217901
42. Mustafa M, Mustafa R, Asif R, Mazhar M, Munir N, Mahmood Z. Pharmaceutical monitoring and care for asthmatic patients management from Lahore city of Pakistan. Natl J Med Health Sci. 2020;3(2):49–58.
43. Bender BG, Apter A, Bogen DK, et al. Test of an interactive voice response intervention to improve adherence to controller medications in adults with asthma. J Am Board Fam Med. 2010;23(2):159–165. doi:10.3122/jabfm.2010.02.090112
44. Tommelein E, Mehuys E, Van Hees T, et al. Effectiveness of pharmaceutical care for patients with chronic obstructive pulmonary disease (PHARMACOP): a randomized controlled trial. Br J Clin Pharmacol. 2014;77(5):756–766. doi:10.1111/bcp.12242
45. Mehuys E, Van Bortel L, De Bolle L, et al. Effectiveness of pharmacist intervention for asthma control improvement. Eur Respir J. 2008;31(4):790–799. doi:10.1183/09031936.00112007
46. Almomani BA, Mokhemer E, Al-Sawalha NA, Momany SM. A novel approach of using educational pharmaceutical pictogram for improving inhaler techniques in patients with asthma. Respir Med. 2018;143:103–108. doi:10.1016/j.rmed.2018.09.004
47. Sánchez-Nieto JM, Bernabeu-Mora R, Fernández-Muñoz I, et al. Effectiveness of individualized inhaler technique training on low adherence (LowAd) in ambulatory patients with COPD and asthma. NPJ Prim Care Respir Med. 2022;32(1):1–9. doi:10.1038/s41533-021-00262-8
48. Jia X, Zhou S, Luo D, Zhao X, Zhou Y, Cui Y-M. Effect of pharmacist-led interventions on medication adherence and inhalation technique in adult patients with asthma or COPD: a systematic review and meta-analysis. J Clin Pharm Ther. 2020;45(5):904–917. doi:10.1111/jcpt.13126
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.