Back to Journals » Infection and Drug Resistance » Volume 15
Campylobacter Gastroenteritis Among Under-Five Children in Southwest Ethiopia
Authors Nigusu Y ![]() , Abdissa A, Tesfaw G
, Abdissa A, Tesfaw G
Received 23 December 2021
Accepted for publication 28 May 2022
Published 9 June 2022 Volume 2022:15 Pages 2969—2979
DOI https://doi.org/10.2147/IDR.S354843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yared Nigusu,1 Alemseged Abdissa,2,3 Getnet Tesfaw3
1Department of Medical Laboratory Science, College of Health Sciences, Mettu University, Mettu, Ethiopia; 2Armauer Hansen Research Institute, Addis Ababa, Ethiopia; 3School of Medical Laboratory Science, Institute of Health, Jimma University, Jimma, Ethiopia
Correspondence: Yared Nigusu, Tel +251 921 20 46 63, Email [email protected]; [email protected]
Background: Under-five children are at an increased risk for foodborne illnesses because of the ingenuousness of their immune system. Although Campylobacter species are one of the bacterial etiologies of gastroenteritis, Campylobacter gastroenteritis among under-five children is not well considered in Ethiopia. Therefore, this study aimed at exploring the prevalence, associated risk factors, and antibiotic susceptibility patterns of Campylobacter species among under-five children with diarrhea.
Methods: The institution-based cross-sectional study was conducted among under-five children with diarrhea at Jimma Medical Center, southwestern Ethiopia from January 5 to April 21, 2020. Stool samples were collected and inoculated into Campylobacter agar medium. Isolation and identification were done using standard bacteriological techniques. Antibiotic susceptibility testing was conducted on Mueller-Hinton agar supplemented with 10% sheep blood using disk diffusion techniques. Bivariate and multivariate logistic regressions were used to assess the associated risk factors.
Results: A total of 214 under-five children were enrolled. The prevalence of Campylobacter infection was 8.9%. Absence of caretakers’ handwashing before preparation of food [AOR = 3.7, 95% CI: (1.2– 10.8)], direct contact with domestic animals [AOR = 3.6, 95% CI: (1.0– 12.7)], and consumption of raw dairy products [AOR = 4.5, 95% CI: (1.4– 13.9)] are the factors associated with Campylobacter infection. Some Campylobacter species were found to be resistant to most available antibiotics.
Conclusion: The magnitude of Campylobacter gastroenteritis indicates the need for routine isolation and identification of Campylobacter species from all under-five children clinically diagnosed with diarrhea. Species that are resistant to the drug of choice for Campylobacteriosis are also emerging. Health education on the importance of pasteurization of milk and caretakers’ handwashing can mitigate the transmission. Mechanism of handling of domestic animals should be considered to reduce transmission of zoonotic diseases like Campylobacteriosis.
Keywords: Campylobacter species, prevalence, antibiotic susceptibility pattern, Ethiopia
Introduction
Globally, under-five mortality has reduced from 51 deaths in 2010 to 39 deaths per 1000 live births in 2018. However, a significant number of under-five children are losing their lives. Sub-Saharan Africa was the region with the highest under-five mortality in the world with an average mortality rate of 78 deaths per 1000 live births in 2018.1
In 2016, 9% of all the global under-five mortality was attributed to diarrhea, of which 90% of deaths occurred in Low- and Middle-Income Countries (LMICs). Estimated 290,724 deaths in sub-Saharan Africa were attributed to diarrhea.2
Campylobacter spp. are one of the most common bacterial pathogens associated with diarrhea among under-five children along with Enterohemorrhagic Escherichia coli (EHEC), Enterotoxigenic Escherichia coli (ETEC), Salmonella spp., Shigella spp., Vibrio spp., and Yersinia spp. in different parts of the world.2,3 Most species are part of the commensal flora of a wide range of animals including food-producing animals like chickens, pigs, and ruminants (eg. sheep, goats, and cattle).4,5 Infection with Campylobacter spp. may also result in extra-gastrointestinal manifestations like Guillain-Barre Syndrome (GBS), Miller Fisher Syndrome, bacteremia/septicemia, meningitis, and reactive arthritis.6 Due to their ability to colonize most domestic and wild animals, consumption of undercooked meat/poultry, unpasteurized dairy products, contaminated drinking water, and direct contact with farm animals are found to be risk factors for infection with Campylobacter spp.7
Worldwide, Campylobacter spp. are responsible for up to 400–500 million infection cases each year.8 In 2010, Campylobacter spp. were one of the most common bacterial agents of diarrhea and were responsible for about 96 million illnesses, 21,374 deaths, and 2.1 million Disability Adjusted Life Years (DALYs) globally. The African regions bore more than half (50.6% of the total DALYs per 100,000 population) of the global Campylobacter disease burden. The global morbidity rate of 2010 caused by Campylobacter infections was relatively higher as compared with Shigella spp. (1.2 million DALYs), Vibrio cholera (1.7 million DALYs), and Enterotoxigenic Escherichia coli (2.0 million DALYs).9
In Europe, Campylobacteriosis remains the most reported gastrointestinal disease since 2005 and affected over 220,000 people in 2019.10
The global burden of Campylobacter spp. is not confined only to its ability of infecting humans, rather the emergence of drug-resistant Campylobacter spp. also became a global concern.11 Increasing trends of resistance by Campylobacter spp. against the fluoroquinolone class of antibiotics have been observed in European countries.12
The magnitude of Campylobacter infection among under-five children in developing countries is under the shadow ; as there are no surveillance systems and routine diagnostic mechanisms in line seen in many developed countries.13 The possible reasons are the absence of a well-equipped laboratory required for isolation and identification of Campylobacter spp., the absence of a national surveillance program involving Campylobacter gastroenteritis, and the bacteriological characteristics of the organism (fastidiousness).
As a result, the above challenges make the rates and burden of Campylobacter infection remain hidden and/or underestimated in Ethiopia. Therefore, this study aimed to explore the isolation rate, antibiotic resistance pattern, and associated risk factors of Campylobacter spp. among under-five children in southwestern Ethiopia.
Materials and Methods
Study Setting and Period
The study was conducted at Jimma Medical Center (JMC) from January 5 to April 27, 2020. JMC is one of the teaching and referral hospitals in the southwestern part of Ethiopia and serves a catchment population of 15–20 million. The hospital has 600 beds and about 1620 staff, providing services for more than 218,000 outpatients, 16,000 inpatients, 14,200 emergencies, and 5900 deliveries annually. The pediatric ward at the center has a bed capacity of 110, admits about 2030 children per year, and serves 4680 children per year as an outpatient. The pediatrics clinic has 78 health professionals, of which 12 are pediatricians, 21 are residents and 45 are pediatric nurses.
Study Design and Study Population
A hospital-based cross-sectional study was conducted among all under-five children presented with acute diarrhea at JMC pediatric clinic during the study period.
Sample Size and Sampling Technique
A single population proportion formula was used to calculate the minimum sample size.14 Considering a 95% confidence interval, 16.7% previous prevalence of Campylobacter spp. among under-five children in Ethiopia,15 and a 5% margin of error, the sample size was 214. A consecutive sampling technique was used to achieve the required sample size.
Eligibility Criteria
Inclusion Criteria
All under-five children who presented with acute diarrhea at JMC during the study period were included.
Exclusion Criteria
All under-five children presented with acute diarrhea who had been treated with antibiotics in the last 7 days prior to data collection.
Data Collection Procedures
Socio-demographic data of both caretakers and under-five children were collected through face-to-face interviews using a structured questionnaire. Height, weight, and age of the children were recorded to assess the nutritional status, and presented as indices of height-for-age (HFA), weight-for-age (WFA), and weight-for-height (WFH). Each index was recorded as the Z-score value of HFA, WFA, and WFH calculated from WHO-Anthro software version 3.2.2 (WHO, Geneva, Switzerland). Accordingly, the Z-score values of ˂-2 standard deviation for HFA, WFA, and WFH were considered as stunting, underweight, and wasting, respectively. Z-score values between −2 standard deviations and 2 standard deviations were considered normal, and Z-score values of ˃ 2 standard deviations for WFH were considered overweight.16
Sample Collection and Processing
Freshly passed stool specimens were collected using a swab and placed in a 6-mL Cary-Blair transport medium (HKM, Hong Kong, China) prepared in a tube. The samples were then transported to Jimma University Medical Microbiology Laboratory within 2 hours of collection. Stool samples of study participants were directly inoculated into Campylobacter agar base media (HiMedia, Mumbai, India) supplemented with Campylobacter Supplement-I/Blazer-Wang (HiMedia, Mumbai, India) (having 1.250IU Polymyxin B, 5 mg of Vancomycin, 2.500 mg of Trimethoprim, 1 mg of Amphotericin B, and 7.500 mg of Cephalothin) and 10% defibrinated sheep blood. An inoculated medium was incubated at 42°C for 48 hours using a 3.5-L anaerobic jar in a micro-aerobic atmosphere of approximately 5–10% O2, 5–10% CO2, and 85% N2 produced using gas generating sachets, CampyGen (Oxoid Ltd, Hampshire, England).17,18
Isolation and Identification of Campylobacter spp
Grayish, flat, and moistened colonies, with a tendency to spread, and having a metallic sheen on Campylobacter agar media were considered. A saline wet mount was performed and microscopically examined for the characteristic darting/corkscrew motility. Gram staining was also performed, and Gram-negative rod, curved, or spiral bacteria having sea-gull wing appearance were considered. Catalase and oxidase-positive organisms were sub-cultured on blood agar and incubated at 42°C for 48 hours. Colonies having characteristics of non-hemolytic, shiny, and colorless to grayish with irregular or round-edged nature were confirmed as Campylobacter spp.17 The isolated strains were differentiated to the species level based on phenotypic classification methods, which depend on the hydrogen sulfide production in triple sugar iron agar and susceptibility to nalidixic acid (30 μg) and cephalothin (30 μg).19
Antimicrobial Susceptibility Testing
The antimicrobial susceptibility patterns of the isolated strains were determined using Kirby-Bauer disk diffusion technique. Mueller-Hinton agar (HiMedia, Mumbai, India) supplemented with 5% defibrinated sheep blood was prepared on a 90 mm petri dish. The isolated Campylobacter spp. were mixed into sterile normal saline and bacterial suspension having turbidity equivalent to 0.5 McFarland standards was prepared. Using a sterile cotton swab, a bacterial suspension was streaked all over the surface of the prepared Mueller-Hinton agar (HiMedia, Mumbai, India) supplemented with 5% defibrinated sheep blood. Antimicrobial disks of ampicillin (AMP) (10μg), amoxicillin with clavulanic acid (AUG) (30μg), gentamicin (GEN) (10μg), ciprofloxacin (CIP) (5μg), ceftriaxone (CTX) (30μg), erythromycin (E) (15μg), chloramphenicol (C) (30μg), meropenem (MEM) (10μg), trimethoprim-sulfamethoxazole (SXT) (25μg) and azithromycin (AZM) (15) (all Liofilchem, Abruzzo, Italy) was applied over the inoculated plates and incubated micro-aerobically at 42°C for 24 hours. Susceptibility patterns toward nalidixic acid (NA) (30μg) and cephalothin (CEF) (30 μg) were additionally used for species-level identification. The panel of antibiotics was chosen following Clinical and Laboratory Standards Institute (CLSI) guidelines from the previous studies and recent reports of resistance to Campylobacter spp.20,21 Analysis of the diameter of zones of inhibition for erythromycin (E), ampicillin (AMP), ciprofloxacin (CIP), and nalidixic acid (NA) was performed according to the CLSI guideline for Campylobacter spp. from the previous studies.21,22 The rest were done according to CLSI guideline breakpoints for Enterobacteriaceae and were interpreted as susceptible (S), intermediate (I), and resistant (R).23
Data Processing and Statistical Analysis
Data were entered into Epi-data version 3.1 and exported to IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, NY, USA) for statistical analysis. Descriptive statistics were computed to determine the prevalence of Campylobacter infections and the frequencies of other variables. The bivariate logistic regression was conducted and all independent variables with a p-value ≤0.25 in a bivariate logistic regression analysis were taken as candidate variables for possible associated factors. Multivariable logistic regression analyses were computed to identify factors associated with Campylobacter infection. The strength of the association was indicated by the odds ratio (OR) at a 95% confidence interval (CI). A p-value of ≤0.05 was considered indicative of a statistically significant association.
Quality Control
A dummy medium of Campylobacter agar was incubated at 42°C for 48 hours for sterility checking. The sterile Campylobacter agar media and Campylobacter supplement were checked using control strains of Campylobacter jejuni (ATCC 33560) and Escherichia coli (ATCC 25922) for growth and partial or complete inhibition characteristics, respectively. All antibiotic disks and Mueller-Hinton agar medium were checked for correct functionality by control strain of Escherichia coli (ATCC 25922).24
Results
Socio-Demographic Characteristics of the Study Participants
A total of 214 under-five children with diarrhea were enrolled. More than half, 109 (50.9) were males and about 54% were living in rural areas. The age of study participants ranged from 1 to 56 months, with a mean age of 15.78 months (±11.8 SD). Most of the children, 79 (36.9%) were between 12 and 24 months of age. Majority of the children’s caretakers, 75 (35%) had no level of education and about 76.6% had latrine at the household level (Table 1).
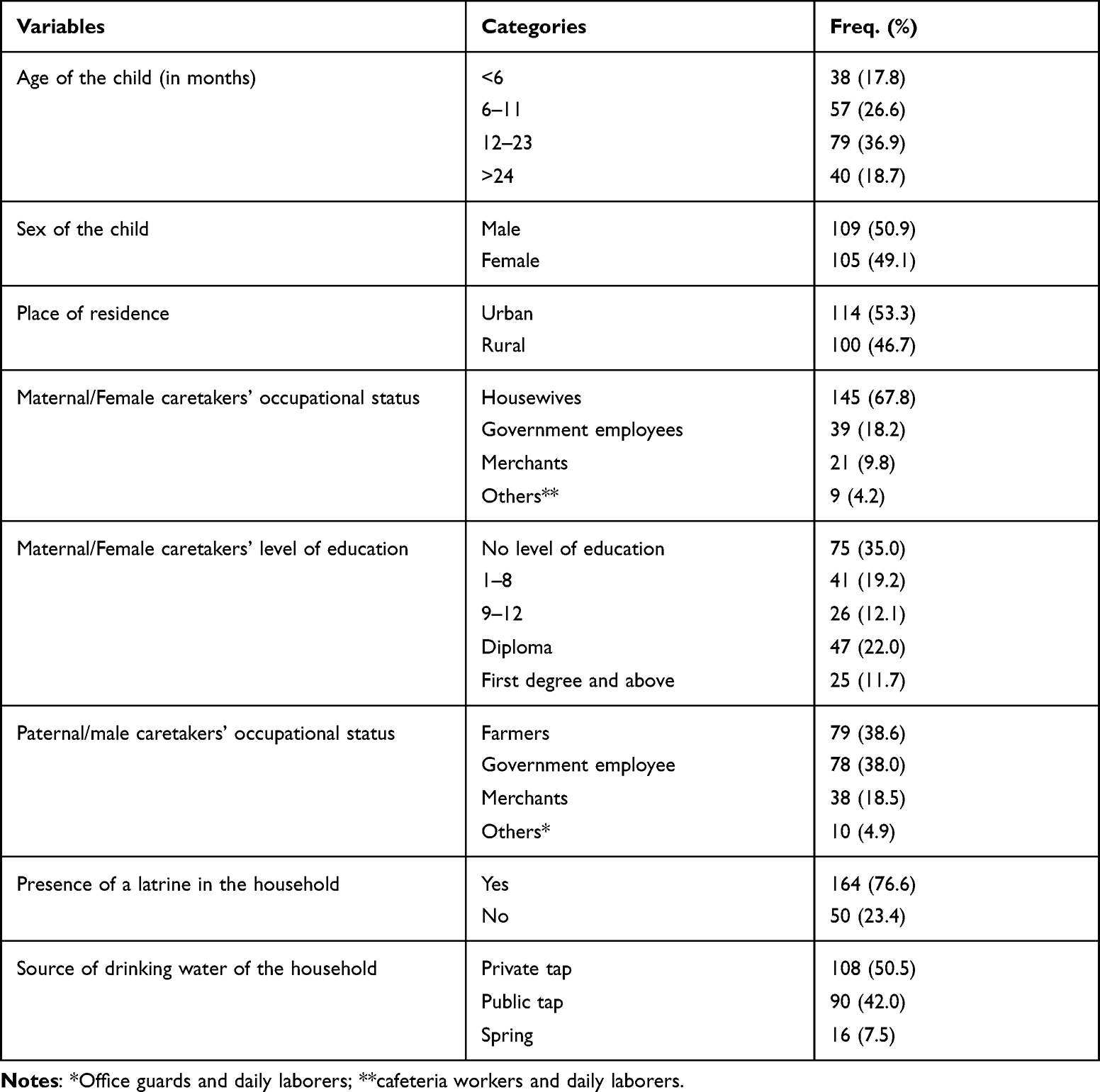 |
Table 1 Socio-Demographic Characteristics of the Study Participants at Jimma Medical Center, Southwest Ethiopia (N = 214) |
Behavioral and Clinical Characteristics of the Study Participants
Most of the caretakers, 172 (80.4%) had a habit of handwashing after using the toilet. The highest number of caretakers, 147 (68.7%) had a habit of handwashing before preparing food for their children. More than half, 143 (66.8%) used treated water for drinking. Only 9 (4.2%) of the children had a chance of eating raw/undercooked meat and about one-fourth of the children, 52 (24.3%) had a habit of eating raw dairy products. Three fourth of the under-five children had vomiting (Table 2).
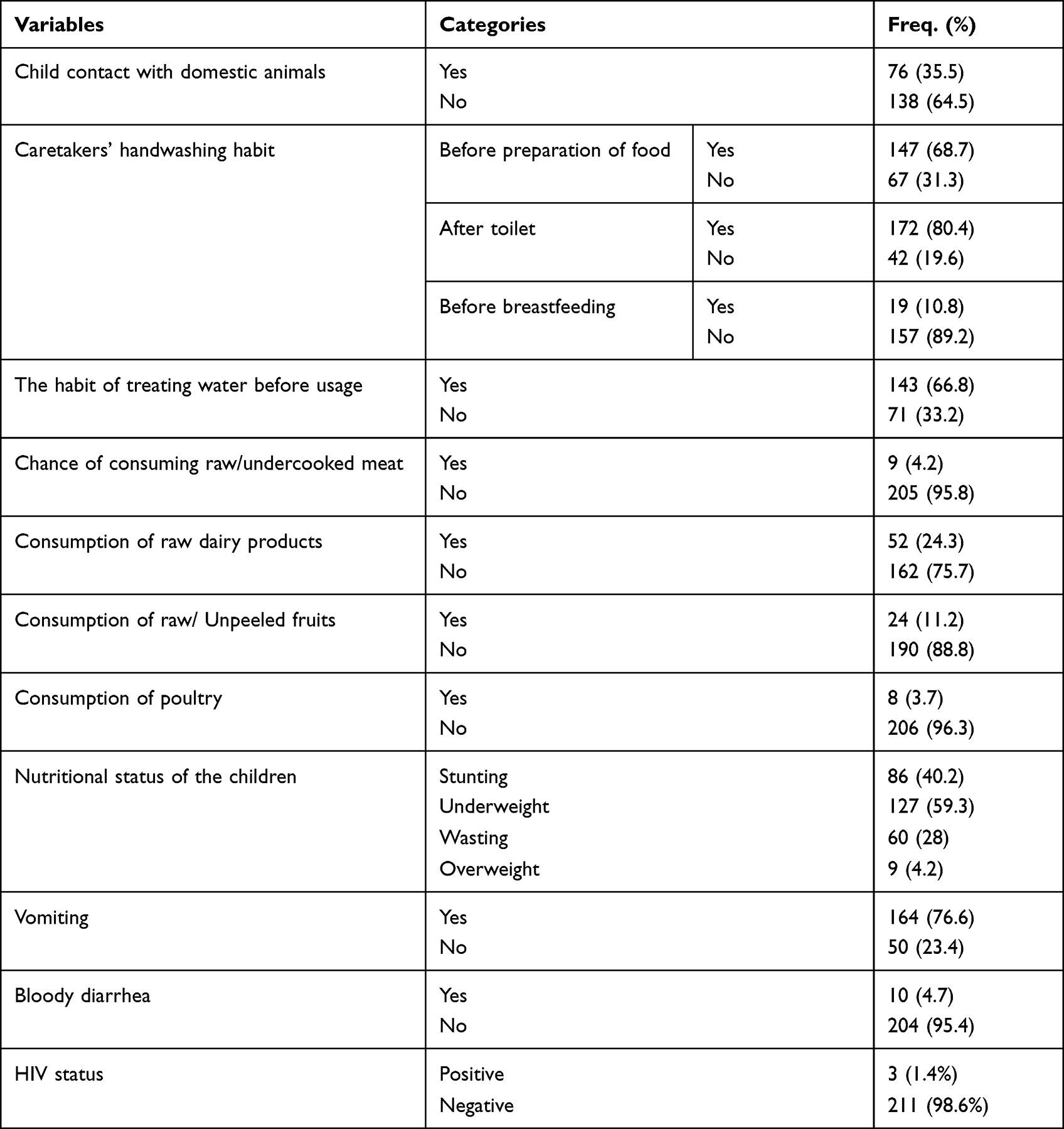 |
Table 2 Behavioral and Clinical Characteristics of the Study Participants at Jimma Medical Center, Southwest Ethiopia (N = 214) |
Prevalence of Campylobacter spp
Campylobacter spp. were isolated from 19 under-five children with diarrhea, with a prevalence of 8.9% [CI: (5.76, 13.4)]. All isolated spp. were C. jejuni and/or C. coli. The majority, 16 (84.2%) of the isolated Campylobacter spp. were among children aged 6–23 months. About 79% of the spp. were isolated from children living in rural areas.
Factors Associated with Campylobacter Infection
In the final logistic regression analysis, the absence of caretakers’ hand washing before preparation of food, child contact with domestic animals, and child consumption of raw dairy products were independent predictors of Campylobacter infection among under-five children.
Accordingly, the odds of Campylobacter infection among under-five children whose mothers/caretakers do not wash their hands before preparing food were 3.7 times [AOR = 3.7, 95% CI: (1.2, 10.8)] higher compared to their counterparts. Likewise, under-five children who had contact with domestic animals were 3.6 times [AOR = 3.6, 95% CI: (1.0, 12.7)] more likely to be infected by Campylobacter spp. On the other hand, the odds of Campylobacter infection were 4.5 times higher among under-five children who consumed raw dairy products [AOR = 4.5, 95% CI: (1.4, 13.9)] compared to those who did not consume raw dairy products (Table 3).
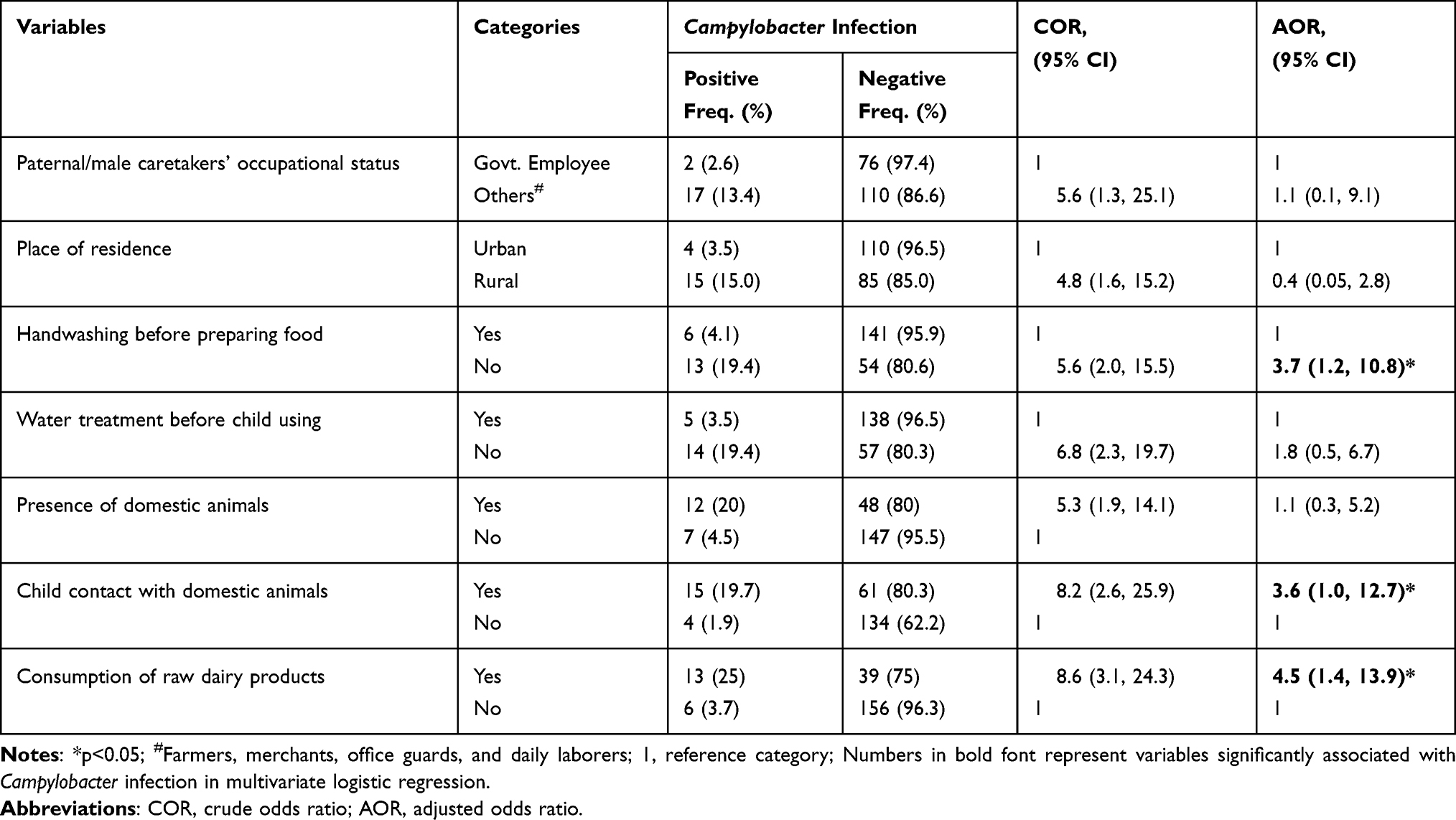 |
Table 3 Bivariate and Multivariable Logistic Regression Analysis Between Candidate Variables and Campylobacter Infection Among Under-Five Children at Jimma Medical Center, Southwest Ethiopia (N = 214) |
Antimicrobial Susceptibility Pattern of the Isolates
All isolated Campylobacter spp. (100%) were susceptible to gentamicin and azithromycin. Nearly 95% of the isolates were susceptible to ciprofloxacin and about 79% were susceptible to erythromycin. Of all Campylobacter spp., 94.7% were resistant to ceftriaxone and trimethoprim-sulfamethoxazole. About one-fourth (22%) of the isolated strains were resistant to ampicillin. More than half (57.9) were resistant to chloramphenicol. About 79% of the isolated strains were non-susceptible to at least one agent in three or more antimicrobial categories (MDR). However, neither XDR nor PDR strains were isolated according to the definitions of MDR, XDR, and PDR given through the initiatives of the European Centre for Disease Prevention and Control (ECDC), and the Centers for Disease Control and Prevention (CDC)25 (Table 4).
 |
Table 4 Antimicrobial Susceptibility Pattern of Campylobacter spp. Isolated from Under-Five Children at Jimma Medical Center, Southwest Ethiopia (N = 19) |
Discussion
The principal aim of the study was to assess the burden of Campylobacter infection among under-five children. Our study showed that the prevalence of Campylobacter spp. among under-five children was 8.9%. This finding is inline with studies conducted in Poland (9.3%),26 Egypt (9.37%),27 Tanzania (9.7%),28 and Uganda (9.3%).29 However, a higher prevalence of Campylobacter infections among under-five children was reported in South Africa (25%),30 India (17.35%),31 and Kenya (16%).32 The variation in the isolation rates of Campylobacter spp. could be due to differences in socio-demographic characteristics, study subjects, study periods, and methods employed. However, the finding of this study was lower than the studies conducted in other parts of Ethiopia, where the isolation rates were 15.4%, and 16.7% in Gondar33 and Jimma,15 respectively. The major variation observed between this study and the previous studies conducted in Ethiopia could be due to variation in study periods, as seasonality is one of the factors that affect the prevalence of Campylobacteriosis.34 Additionally, previous studies were conducted on samples taken from health centers where acute diarrhea could be found common.
The odds of Campylobacter infection were higher among under-five children who had contact with domestic animals. This finding is consistent with studies conducted in California,35 Sweden,36 Norway,37 and Jordan.38 A similar study conducted in Ethiopia also agrees with the finding of an association between Campylobacter infections and the presence and contact of domestic animals in the household.39 This could be due to the fact that Campylobacter spp. are harbored by most domestic animals as normal gut microbiota. Therefore, the presence and contact with domestic animals increases the possibility of contamination of food and hence increases the rate of infection.
This study has also identified under-five children who did not consume raw dairy products had low odds of infection with Campylobacter spp. This finding agrees with the findings of the study conducted in Sweden,36 Norway,37 and New Zealand.40 The possible reason for this finding is due to the probability of contamination of dairy products, mainly raw milk with animals manure.
Campylobacter infection was higher among under-five children whose mothers/caretakers do not wash their hands before preparing food. This result is consistent with a study conducted in 8 selected low-income countries.41 The absence of routine handwashing practices could be the cause of Campylobacter infection in the presence of maternal contact with domestic animals.
On the other hand, all isolated strains of Campylobacter spp. were found to be susceptible to gentamicin and azithromycin. This finding is supported by studies conducted in Macedonia42 and Korea.43 However, it was found to be higher as compared to the previous study conducted in Ethiopia where nearly 87% of the isolates were susceptible to gentamicin.15 This could be due to the difference in the Campylobacter spp. isolated from the participants, where the isolated strains of Campylobacter were all C. jejuni and/or C. coli.
Moreover, nearly 95% of the isolates were susceptible to ciprofloxacin, which is consistent with another study conducted in Ethiopia.44 Our study also revealed the rate of resistance to erythromycin is comparable with findings from South Africa20 and other parts of Ethiopia.15,33 This study also indicates a high rate of resistance to ceftriaxone (94.7%), trimethoprim-sulfamethoxazole (94.7%), ampicillin (78.5%), and chloramphenicol (42.1%).
However, lower rates of resistance were recorded in Macedonia42 and Korea,43 Pakistan21 Bangladesh.45 The main reason could be due to inappropriate use of antibiotics in Ethiopia.46
Limitation of the Study
This study has a limitation as it could not differentiate between C. jejuni and C. coli due to the absence of hippurate hydrolysis test used for this purpose. The limited sample size could also be a reason for which additional risk factors of infections were not identified.
Conclusion and Recommendation
The rate of isolation of Campylobacter spp. among under-five children in the study area was noticeable. The magnitude of Campylobacter gastroenteritis indicates the need for routine isolation and identification of Campylobacter spp. from every under-five child clinically diagnosed with diarrhea. Although appreciable susceptibility was recorded for azithromycin and gentamicin, resistance to the drug of choice for Campylobacter infection is also emerging. Health education on the importance of pasteurization of milk and caretakers’ hand washing can mitigate the transmission. The mechanism of handling domestic animals should also be considered to reduce the transmission of zoonotic diseases like Campylobacteriosis. Moreover, having these baseline data, researchers and concerned bodies should undergo further studies to disclose the burden of Campylobacter infection in developing countries, which in turn points out the mechanism of dwarfing the burden among under-five children.
Abbreviations
DALYs, Disability-Adjusted Life Years; HFA, height-for-age; MDR, multi-drug resistant; XDR, extensively-drug resistant; PDR, pan-drug resistant; JMC, Jimma Medical Center; WFA, Weight-for-Age; WFH, Weight-for-Height.
Data Sharing Statement
Data used in the findings of this study are included in the manuscript.
Ethics Approval and Consent to Participate
The study was approved and ethical clearance was obtained from the Institutional Review Board of the Institute of Health, Jimma University (Ref. No: IHRPGD/581/18). The study protocol was performed following the Declaration of Helsinki. Overviews of the study were explained for families/caretakers of under-five children. Then, informed consent was obtained from families/caretakers of under-five children regarding socio-demographic and clinical data collection including sample collection.
Consent for Publication
Not applicable – this manuscript does not contain any individual data.
Acknowledgments
We would like to gratefully thank Jimma University and the African Center of Excellence in Materials, Product Development and Nanotechnology (MAPRONANO), Makerere University, for funding this study. Data collectors and study participants also owed a debt of gratitude for their participation in this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This project was funded by the Research and Post Graduate office of the Institute of Health, Jimma University, Ethiopia, and the African Center of Excellence in Materials, Product Development and Nanotechnology (MAPRONANO), Makerere University, Uganda.
Disclosure
All the authors declare no conflicts of interest in this work.
References
1. UNICEF, WHO, World Bank Group, United Nations. Levels and trends in child mortality 2019, Estimates developed by the UN inter-agency group for child mortality estimation. Lancet Glob Health. 2019;7(6):e710–e720.
2. Troeger C, Blacker BF, Khalil IA, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhea in 195 countries: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1211–1228. doi:10.1016/S1473-3099(18)30362-1
3. Zhu X-H, Tian L, Cheng Z-J, et al. Viral and bacterial etiology of acute diarrhea among children under 5 years of age in Wuhan, China. Chin Med J. 2016;129(16):1939. doi:10.4103/0366-6999.187852
4. Kassa T, Gebre-selassie S, Asrat D. The prevalence of thermotolerant Campylobacter spp. in food animals in Jimma Zone, southwest Ethiopia. Ethiop J Health Dev. 2005;19(3):225–229.
5. Sheppard SK, Dallas JF, Strachan NJ, et al. Campylobacter genotyping to determine the source of human infection. Clin Infect Dis. 2009;48(8):1072–1078. doi:10.1086/597402
6. Kaakoush NO, Castaño-Rodríguez N, Mitchell HM, Man SM. Global epidemiology of Campylobacter infection. Clin Microbiol Rev. 2015;28(3):687–720. doi:10.1128/CMR.00006-15
7. Ravel A, Hurst M, Petrica N, et al. Source attribution of human Campylobacteriosis at the point of exposure by combining comparative exposure assessment and subtype comparison based on comparative genomic fingerprinting. PLoS One. 2017;12(8):e0183790. doi:10.1371/journal.pone.0183790
8. Igwaran A, Okoh AI. Human Campylobacteriosis: a public health concern of global importance. Heliyon. 2019;5(11):e02814. doi:10.1016/j.heliyon.2019.e02814
9. Havelaar AH, Kirk MD, Torgerson PR, et al. World Health Organization global estimates and regional comparisons of the burden of foodborne disease in 2010. PLoS Med. 2015;12(12):e1001923. doi:10.1371/journal.pmed.1001923
10. European Food Safety Authority and European Centre for Disease Prevention and Control. The European Union one health 2019 zoonoses report. Efsa J. 2021;19(2):e06406.
11. Koluman A, Dikici A. Antimicrobial resistance of emerging foodborne pathogens: status quo and global trends. Crit Rev Microbiol. 2013;39(1):57–69. doi:10.3109/1040841X.2012.691458
12. European Food Safety Authority and European Centre for Disease Prevention and Control. The European Union Summary Report on antimicrobial resistance in zoonotic and indicator bacteria from humans, animals, and food in 2019–2020. EFSA J. 2022;20(3):e06490.
13. Mughal MH. Campylobacteriosis-A global threat. Biomed J Sci Tech Res. 2018;11(5):8804–8808. doi:10.26717/BJSTR.2018.11.002165
14. Fosgate GT. Practical sample size calculations for surveillance and diagnostic investigations. J Vet Diagn Invest. 2009;21(1):3–14. doi:10.1177/104063870902100102
15. Tafa B, Sewunet T, Tassew H, Asrat D. Isolation and antimicrobial susceptibility patterns of campylobacter species among diarrheic children at Jimma, Ethiopia. Int J Bacteriol. 2014;2014:1–7. doi:10.1155/2014/560617
16. World Health Organization. Guideline: assessing and managing children at primary health-care facilities to prevent overweight and obesity in the context of the double burden of malnutrition; 2017.
17. Public Health England. UK Standards for Microbiology Investigations; Identification of Campylobacter Spp. Bacteriology. Public Health England; 2018.
18. Vandepitte J, Verhaegen J, Engbaek K, et al. Basic Laboratory Procedures in Clinical Bacteriology. World Health Organization; 2003.
19. Barrett TJ, Patton CM, Morris GK. Differentiation of Campylobacter spp. using phenotypic characterization. Lab Med. 1988;19(2):96–102. doi:10.1093/labmed/19.2.96
20. Chukwu MO, Abia ALK, Ubomba-Jaswa E, Obi L, Dewar JB. Characterization and phylogenetic analysis of Campylobacter spp. isolated from pediatric stool and water samples in the Northwest province, South Africa. Int J Environ Res Public Health. 2019;16(12):2205. doi:10.3390/ijerph16122205
21. Noreen Z, Siddiqui F, Javed S, Wren BW, Bokhari H. Transmission of multidrug-resistant Campylobacter jejuni to children from different sources in Pakistan. J Glob Antimicrob Resist. 2020;20:219–224. doi:10.1016/j.jgar.2019.07.018
22. Luangtongkum T, Morishita TY, El-Tayeb AB, Ison AJ, Zhang Q. Comparison of antimicrobial susceptibility testing of Campylobacter spp. by the agar dilution and the agar disk diffusion methods. J Clin Microbiol. 2007;45(2):590–594. doi:10.1128/JCM.00986-06
23. Patel JB, Cockerill F, Bradford PA. Performance standards for antimicrobial susceptibility testing: twenty-fifth informational supplement; 2015.
24. European Committee on Antimicrobial Susceptibility Testing. Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST; 2019.
25. Magiorakos A-P, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
26. Szczepanska B, Andrzejewska M, Spica D, Klawe JJ. Prevalence and antimicrobial resistance of Campylobacter jejuni and Campylobacter coli isolated from children and environmental sources in urban and suburban areas. BMC Microbiol. 2017;17(1):1–9. doi:10.1186/s12866-017-0991-9
27. Sainato R, ElGendy A, Poly F, et al. Epidemiology of Campylobacter infections among children in Egypt. Am J Trop Med Hyg. 2018;98(2):581. doi:10.4269/ajtmh.17-0469
28. Deogratias A-P, Mushi MF, Paterno L, et al. Prevalence and determinants of Campylobacter infection among under-five children with acute watery diarrhea in Mwanza, North Tanzania. Archives of Public Health. 2014;72(1):1–6. doi:10.1186/2049-3258-72-17
29. Mshana S, Joloba M, Kakooza A, Kaddu-Mulindwa D. Campylobacter spp. among children with acute diarrhea attending Mulago hospital in Kampala-Uganda. Afr Health Sci. 2009;9(3):201.
30. Samie A, Ramalivhana J, Igumbor E, Obi CL. Prevalence, hemolytic and haemagglutination activities, and antibiotic susceptibility profiles of Campylobacter spp. isolated from human diarrhoeal stools in Vhembe District, South Africa. J Health Popul Nutr. 2007;25(4):406.
31. Mohakud NK, Patra SD, Kumar S, Sahu PS, Misra N, Shrivastava AK. Detection and molecular typing of Campylobacter isolates from human and animal feces in the coastal belt of Odisha, India. Indian J Med Microbiol. 2019;37(3):345–350. doi:10.4103/ijmm.IJMM_19_394
32. Beatty M, Ochieng J, Chege W, et al. Sporadic pediatric diarrhoeal illness in urban and rural sites in Nyanza Province, Kenya. East Afr Med J. 2009;86(8):387–398. doi:10.4314/eamj.v86i8.54159
33. Lengerh A, Moges F, Unakal C, Anagaw B. Prevalence, associated risk factors and antimicrobial susceptibility pattern of Campylobacter spp. among under-five diarrheic children at Gondar University Hospital, Northwest Ethiopia. BMC Pediatr. 2013;13(1):1–9. doi:10.1186/1471-2431-13-82
34. Lake I, Colon-Gonzalez FJ, Takkinen J, et al. exploring Campylobacter seasonality across Europe using the European surveillance system (TESSy), 2008 to 2016. Eurosurveillance. 2019;24(13):1800028. doi:10.2807/1560-7917.ES.2019.24.13.180028
35. Pires A, Patterson L, Kukielka E, Aminabadi P, Navarro-Gonzalez N, Jay-Russell M. Prevalence and risk factors associated with Campylobacter spp. and Salmonella enterica in livestock raised on diversified small-scale farms in California. Epidemiol Infect. 2019;147. doi:10.1017/S095026881900205X
36. Studahl A, Andersson Y. Risk factors for indigenous Campylobacter infection: a Swedish case-control study. Epidemiol Infect. 2000;125(2):269–275. doi:10.1017/S0950268899004562
37. Kapperud G, Espeland G, Wahl E, et al. Factors associated with increased and decreased risk of Campylobacter infection: a prospective case-control study in Norway. Am J Epidemiol. 2003;158(3):234–242. doi:10.1093/aje/kwg139
38. Obaidat MM. Seroprevalence and risk factors for Campylobacter jejuni seropositivity in Jordan. Infect Dis. 2019;51(2):140–146. doi:10.1080/23744235.2018.1540883
39. Budge S, Barnett M, Hutchings P, et al. Risk factors and transmission pathways associated with infant Campylobacter spp. prevalence and malnutrition: a formative study in rural Ethiopia. PLoS One. 2020;15(5):e0232541. doi:10.1371/journal.pone.0232541
40. Davys G, Marshall J, Fayaz A, Weir R, Benschop J. Campylobacteriosis associated with the consumption of unpasteurized milk: findings from a sentinel surveillance site. Epidemiol Infect. 2020;148. doi:10.1017/S0950268819002292
41. Amour C, Gratz J, Mduma E, et al. Epidemiology and impact of Campylobacter infection in children in 8 low-resource settings: results from the MAL-ED study. Clin Infect Dis. 2016;63(9):1171–1179. doi:10.1093/cid/ciw542
42. Trajkovska-Dokic E, Mihajlov K, Mirchevska G, Kostovski M, Blazevska A, Stojkovska S. Antimicrobial susceptibility of Campylobacter isolates in the capital of North Macedonia. Prilozi. 2019;2019:0017.
43. Park SH, Kim BJ, Kwon YH, et al. Antimicrobial susceptibility and genetic analysis of Campylobacter jejuni isolated from diarrhea patients in Busan. Ann Clin Microbiol. 2019;22(2):42–49. doi:10.5145/ACM.2019.22.2.42
44. Mulatu G, Beyene G, Zeynudin A. Prevalence of Shigella, Salmonella and Campylobacter spp. and their susceptibility patterns among under-five children with diarrhea in Hawassa town, South Ethiopia. Ethiop J Health Sci. 2014;24(2):101. doi:10.4314/ejhs.v24i2.1
45. Pervin MK, Jhora ST, Paul S, Naher A. Antibiotic susceptibility pattern of diarrhoeal pathogens in under-five children. Bangladesh Medl J Khulna. 2019;52(1–2):35–39. doi:10.3329/bmjk.v52i1-2.46148
46. Muhie OA. Antibiotic use and resistance pattern in Ethiopia: systematic review and meta-analysis. Int J Microbiol. 2019;2019:1–8. doi:10.1155/2019/2489063
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.