")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Campaign Governance and Partnerships: Unraveling COVID-19 Vaccine Promotion Efforts in China’s Neighborhoods
Received 18 October 2023
Accepted for publication 15 December 2023
Published 28 December 2023 Volume 2023:16 Pages 2915—2929
DOI https://doi.org/10.2147/RMHP.S441874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Ronghui Yang, Sirui Sun
Department of Public Administration, College of Humanities, Donghua University, Shanghai, 200051, People’s Republic of China
Correspondence: Sirui Sun, Department of Public Administration, College of Humanities, Donghua University, 1882 West Yan’an Road, Shanghai, 200051, People’s Republic of China, Tel +8618521057816, Email [email protected]
Background: COVID-19 vaccine promotion helps counter vaccine hesitancy and raise vaccine acceptance. Therefore, the Chinese state created collaborative infrastructures of COVID-19 vaccine promotion programs to promote stakeholder engagement and unload the burden of policy practitioners. However, partnerships in COVID-19 vaccine promotion programs have been underrepresented.
Methods: To address this lacuna, we qualitatively explored how partnerships in the COVID-19 vaccine promotion campaign (CVPC) were organized in China’s neighborhoods. Specifically, we recruited participants via personal networks, referrals from acquaintances, and snowballing approaches, and conducted the qualitative thematic analysis following interviews with 62 Chinese stakeholders.
Results: This study indicates that to promote partnerships in CVPCs, neighborhood managers formed leadership in CVPCs, expanded the collaborative network, trained Health Promotion Practitioners (HPPs), and coordinated with HPPs to shape partnership agreements, produced COVID-19 vaccine promotional materials and advertised COVID-19 vaccines via diverse media tools. Although coproduction of CVPCs to a certain extent promoted state-society interaction in neighborhoods and state responsiveness to public demands, partners’ disagreements on strategies applied by states for promoting COVID-19 vaccines eroded partnerships in CVPCs.
Conclusion: To construct a robust partnership in CVPCs, depoliticizing CVPCs and creating shared values among stakeholders in CVPCs are expected. Our study will not only deepen global audiences’ understanding of CVCPs in China but also offer potential neighborhood-level solutions for implementing local and global health promotion efforts.
Keywords: campaign governance, partnerships, COVID-19 vaccine promotion, neighborhood, China
Introduction
COVID-19 vaccine promotion helps enhance vaccine acceptance, reach herd immunity swiftly and contain virus spread. Countries around the world, therefore, competitively implemented the COVID-19 Vaccine Promotion Program (CVPP) within their territories during the COVID-19 pandemic in pursuit of high vaccination rates.1 In China, states created a series of policies, such as “Technical Guidelines for COVID-19 Vaccination” issued in March 2021,2 “Notice on COVID-19 Vaccine Science Popularization” issued in April 2022, and “Implementation Plan for Second Dose of COVID-19 Vaccine” issued in December 2022,3 to offer institutional, financial and technical support for CVPPs at a local level.
In academia, mainstream scholarship related to Chinese COVID-19 vaccination centers on the attitudes, beliefs and acceptance of COVID vaccines among different population groups and their determinants.4,5 In addition, several scholars mentioned strategies for marketing COVID-19 vaccines, such as inviting patients to convey the severity of contracting COVID-19,5 involving physicians in promoting the immunization,6 improving the perceived efficacy of vaccines, suggesting campaign-style governance and agile promotion approaches tailored to different population groups,7 promoting hope to return to normalcy and elicit anticipated guilt for refusing vaccination.8 However, the COVID-19 vaccine promotion program in China has been less systematically presented. Informed by these analyses above, we explored how COID-19 vaccine promotion activities were organized in China. This study will not only deepen our understanding of COVID-19 vaccine promotion efforts in an authoritarian regime but also offer potential neighborhood-level solutions for implementing local and global public health promotion programs. In the following sections, we first introduced academic debates about campaign strategies for promoting vaccines and partnerships in vaccination promotion activities. Subsequently, we presented the methods through which we achieved this and their results, and finally we discussed the findings and our contributions to academic debates about COVID-19 vaccine marketing.
Unraveling Partnerships in Vaccine Promotion Campaigns
In this section, we traced academic debates on partnerships in vaccine promotion campaigns, to favor readers’ understanding of the development and patterns of Chinese vaccine promotion activities, and on this basis, confirm the research lacuna.
Campaign Strategies for Advertising Vaccines
According to Moran et al, vaccine promotion refers to various activities involved in transmitting vaccine-related information to target audiences via media tools to alter their beliefs and behaviors toward vaccines in a desirable way.9 In the context of public health emergencies like epidemics, and widespread vaccine hesitancy, conventional means fail to effectively promote public acceptance of vaccines. Deploying an immunization campaign helps create a favorable information environment, reach a wide audience, boost vaccine acceptance, and swiftly achieve vaccination goals. The mobilization campaign, originated from the military affairs, refers to that a series of actions or events are launched to gain public support and achieve a particular goal.10 The elements of a marketing campaign involve creating campaign goals, defining and engaging with target audiences, offering key information that induces changes and distributing campaigns via multiple media.11
Prior studies center on various avenues for implementing vaccine promotion campaigns, such as social media campaigns,12 partnering with social influencers to steer public opinions and advocate vaccines,13 creating public demands for vaccination via gain-loss framing,14,15 enhancing the vaccination experience via optimizing service provision, monetary incentives,16 empowering health promotion practitioners (HPPs), standardizing immunization programs, diffusing information via social networks,17,18 and creating collaborative networks. Among them, partnerships in vaccine promotion campaigns have gained widespread attention in academia.
Partnerships in Vaccine Promotion Campaigns in Different Political Settings
Partnerships in immunization promotion campaigns refer to that diverse stakeholder, such as governments, private companies, religious groups, experts and societal actors’ band together, leveraging their respective knowledge, expertise and resources to advertise vaccines tailored to specific target audiences’ beliefs, needs and prior vaccination experience in vaccines to boost vaccine acceptance. Creating partnerships in vaccine promotion campaigns not only helps promote diverse stakeholder engagement and unload the burden of vaccine program managers but also forges a participatory and democratic governance infrastructure.19 In the West, the mainstream scholarship illustrates the content of vaccine promotions and strategies and risks of implementing vaccine promotion campaigns. Vaccine promotions include advertising the safety, efficacy, benefits, precautions, potential side effects of vaccinations, and responding to vaccine misinformation.20
Collaborative vaccine promotion campaigns involve expanding the collaborative network, creating leadership, constructing mutual trust, affirming shared visions among partners, and shaping partnership contracts. Implementing vaccine promotion campaigns necessitates connecting with various stakeholders. Therefore, scholars suggested engaging social media influencers, representatives of marginalized groups, and peers of target audiences in the collaborative network to reach wide audiences and enhance the credibility of vaccine promotion campaigns. Specifically, Lutkenhaus et al proposed identifying potential social media influencers using big data analytics such as social media network and degree centrality.21 Metcalfe and Sexton suggested incorporating various representatives of marginalized populations, such as, homeless persons, refugees and migrants whose demands and perspectives on vaccinations are easily ignored HPPs to reach their counterparts.22 Volpp et al recommended partnering with peers of target audiences to advertise vaccines given that peers may share similar values, experiences and needs on vaccinations.23 Shaping leadership in vaccine promotion campaigns helps strengthen organizational cohesion, reduce internal conflicts, favors rational decision-making, and boosts the productivity of teamwork. Therefore, Wang et al suggested conducting specialized training for vaccine promotion managers and integrating local influencers such as role models, political leaders and public figures, into the collaborative network to create leadership in vaccine promotion activities.24 Creating shared visions and common goals helps eliminate disputes and reach agreements among partners, thereby enhancing the efficiency of collaborative vaccine promotion efforts. Steffens et al thus advocated open dialogues among partners to enhance mutual trust, reach consensuses on vaccine promotion strategies, improve collective agreements on immunization programs, and identify shared interests and values.25 Forming partnership agreements helps standardize vaccination promotion programs and promote efficient collaboration efforts. Therefore, Dhama et al suggested creating partnership agreements to define the missions, goals, schemes, and responsibilities of all parties involved in vaccine promotion programs.26
In addition, prior studies also identified vulnerabilities in coordinated vaccine promotion campaigns, such as disproportionate resource input and benefit gaining among partners decreasing their motivation to collaborate,26 and lacking consensuses among partners on strategies for advertising vaccines decreasing coproduction of vaccine promotion activities.27 Many floating HPPs existing in the cooperative network are not conducive to mutual trust.28
In authoritarian China, states also placed the vaccine promotion program in a critical position and issued a series of policies to implement vaccine promotion efforts. For instance, the central state enacted “Notice on Promoting National Vaccination Popularization” issued in March 2015, “Regulations on Vaccine Circulation and Vaccination Programs” issued in April 2016,29 “The Vaccine Administration Law in China” issued in July 2019, and updated “Regulations on Vaccination Programs” issued in May 2021,30 to require local health authorities to implement vaccine-related science popularization, create intragovernmental partnerships, train HPPs, and offer policy and financial support for vaccine promotion programs. Extant academic research mainly explored partnered approaches to advertising vaccines. For instance, Zhao and Sun advocated state-driven vaccine promotion programs, favoring quickly shaping the leadership and mobilizing other stakeholder engagement.31 Therefore, Yu et al proposed empowering local officials via specialized training and ideological and political education to improve their vaccine promotion capacity and boost their internal cohesion, political loyalty, and sense of serving the people to ensure the pivotal role of the party-state in vaccine promotion programs.32 Strengthening intragovernmental partnerships helps improve the institutional efficiency of vaccine promotion programs.33 As such, senior states clearly defined the responsibility boundaries of each health department to favor collaborative vaccine promotion.33 Diverse stakeholder engagement in vaccine promotion programs helps connect with their expertise and resources and create co-production of vaccine promotion programs. Therefore, Du et al suggested advertising collectivism and volunteerism to raise individuals’ sense of social responsibility and forging diverse participatory mechanisms to support stakeholder engagement.34 The application of media tools helps stakeholder collaboration and accurately confirming public demands on vaccination. As such, Lin et al suggested leveraging social media to promote information sharing and reciprocal communication between partners and utilizing big data analytics to identify public demands and advertising vaccines in line with these public demands.35 Additionally, Li indicated that the implementation of coordinated vaccine promotion campaigns was driven by top-down political pressure, and it is unlikely to be sustained without the institutional pressure in China.36
In summary, extant research theoretically illustrated the pivotal role of states, diverse stakeholder engagements and media tool application in vaccine promotion campaigns in China. Nonetheless, collaborative vaccine promotion campaigns in the Chinese grassroots society have been underrepresented in the literature. To address this lacuna, we explored how partnerships in COVID-19 vaccine promotion campaigns (CVPCs) were organized in Chinese neighborhoods. Specifically, this study interrogated the dynamics and components of coordinated CVPCs and their impact on China’s neighborhood governance structure.
Materials and Methods
Research Design
In this study, we adopted qualitative methods to gain insight into the scenario and elements of the coordinated CVPC in communities and its implications for Chinese neighborhood governance structure. Two authors with expertise in semi-structured interviews and immunization promotion conducted interviews with Chinese stakeholders to gather data in an exploratory way. We interviewed respondents via face-to-face interaction, telephone and video calls on WeChat (akin to WhatsApp) between July 2022 and December 2022. Prior to the interviews, we obtained oral informed consent from participants after sharing with them the research goals, methods, expected outcomes, anticipated impacts, and the rights and responsibilities of participants and after ensuring their anonymity.
Data Collection and Analysis
The data collection involved identifying, recruiting, and investigating respondents and creating an interview transcript. We first confirmed potential interviewees based on their knowledge and experiences with CVPCs. Specifically, we identified respondents based on whether their work involved COVID-19 vaccine promotion. To this end, we confirmed multiple stakeholders interviewed based on literature review, pre-screening interviews and interviewers’ expertise in qualitative research and immunization promotion. We then recruited participants via snowballing approaches in line with the specific Chinese context: selection started through informal, personal networks and continued through snowballing to include participants’ colleagues. For instance, we first interviewed staff of the resident’s committee we were familiar with and recruited more participants via referrals from acquaintances. Subsequently, we identified other potential subjects via these enrolled participants. These sampling methods generated enough data for analysis. In this way, we interviewed 62 respondents in Beijing, Guangzhou, Shanghai, Wuhan and Changsha to reach the data saturation.37 The research population included 5 directors, 5 secretaries and 10 staff of the neighborhood committee, 6 doctors in the community public healthcare center, 5 staff of the property company, 4 public health experts in the Center for Disease Control (CDC), 4 experts in the Volunteer Association for Science and Technology Promotion (VASTP), 17 community volunteers, and 6 members of the homeowner’s association. As requested by the respondents, the interviews were not recorded. During the interviews, we avoided taking notes in front of participants to mitigate their guardedness and encourage them to express their opinions freely. We created detailed transcriptions from memory immediately afterwards. To ensure that we would do justice to original intentions and connotations and the correctness of quotes, in some cases we verified these via WeChat.38 Finally, we collated the interview data and created an interview transcript using Microsoft Word for qualitative analysis.
Thematic analysis was conducted to inductively analyze the interview transcript. Specifically, Coder 1, served by the first author, manually coded the interview transcript using NVivo 12 to gain a condensed overview of main points that recur throughout the data. Coder 1 shaped a tree node to visualize the relationship between codes and developed Codebook_1 on the basis of this. Coder 2, served by an external researcher with expertise in qualitative data coding and health promotion, coded the interview transcript in the same way as Coder 1 and developed Codebook_2. Subsequently, we evaluated the inter-coder reliability using the Kappa Coefficient in NVivo 12 to confirm coding discrepancies. The second author was then invited to discuss and resolve coding discrepancies. Finally, we evaluated and confirmed the final codebook (see Figure 1). In that way, sub-themes we identified in this study include the scenario, actors and dynamics of coordinated CVPCs, shaping leadership, expanding the collaborative network of CVPCs, training HPPs, creating partnership agreements, producing COVID-19 vaccine promotional materials, and advertising COVID-19 vaccines, state responsiveness to public demands, and HPPs’ disagreements on strategies for implementing CVPCs. Important themes identified were coordinated CVPCs in communities, organizations of coordinated CVPCs and the implications of CVPCs for Chinese neighborhood governance structure. In the Results section, we selected exemplary data from the interview transcript as quotes (Appendix 1).39
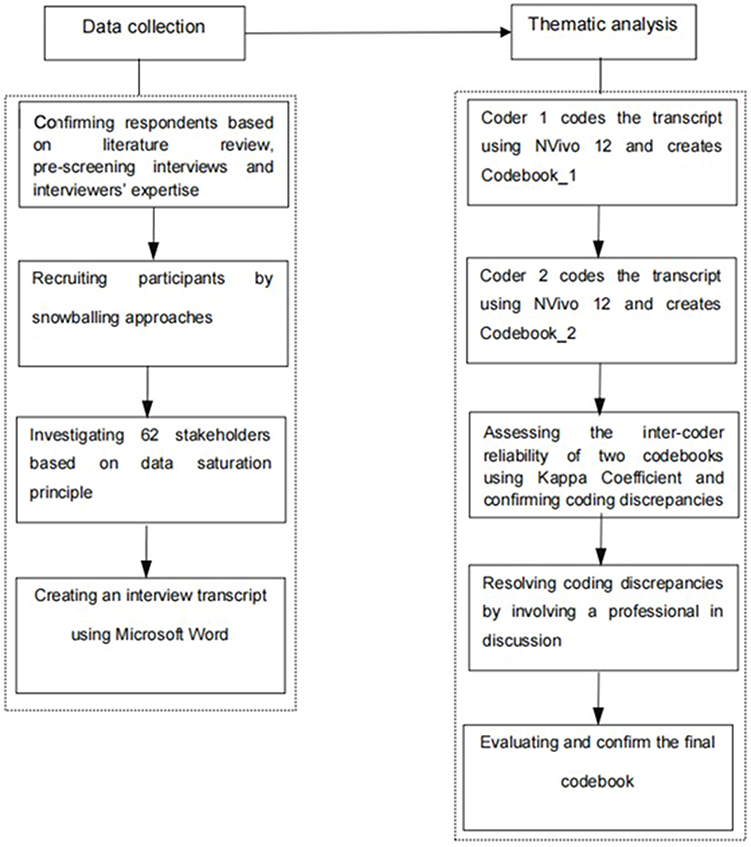 |
Figure 1 Procedures of qualitative data collection and analysis. |
Results
In this chapter, we illustrated the scenario of and partnerships in CVPCs, the dynamics and organizations of coordinated CVPCs, and the impact of CVPCs on Chinese neighborhood governance structure.
Coordinated CVPCs in Communities
COVID-19 vaccines help contain virus spread and protect personal health.40–47 However, affected by the voluntary COVID-19 vaccine policy created by the central state in 2022, many citizens chose not to be vaccinated or not to be fully vaccinated. Therefore, the state launched COVID-19 vaccine promotion campaigns (CVPCs) across the country to raise vaccine acceptance. In this context, in November 2022, we observed that a group of HPPs, wearing uniform red jackets and holding COVID-19 vaccination brochures, were bustling with promoting COVID-19 vaccines to passing residents in a community in Shanghai. A cluster of HPPs were posting on community bulletin boards and hanging up banners at the entrance of the community to advertise the importance and urgency of COVID-19 vaccination. Meanwhile, a neighborhood manager, leading several volunteers, was advertising COVID-19 vaccines to residents face-to-face at their homes. The foregoing scenario reflects a typical Chinese CVPCs in a neighborhood. These campaigns were not exclusive to certain communities. Instead, they occurred in most urban communities in China. COVID-19 vaccination has been treated as a crucial matter of Chinese neighborhood governance in 2022 and sparked massive media coverage.
In CVPCs, HPPs included members of the neighborhood committee, homeowner’s association, property managers and the community healthcare service center, building directors who are elected by residents of this building and are responsible for implementing tasks assigned by the neighborhood committee, conveying government policies to residents and maintaining the environmental sanitation and security in the building, volunteers, CDC experts, experts in VASTPs and et cetera. Among them, neighborhood committees, functioning as an extension of the government apparatus in communities to deliver public services and implement administrative tasks, led community CVPCs, and other members were responsible for assisting neighborhood committees in implementing CVPCs (ID 1–5).
The dynamics of applying coordinated approaches to implementing CVPCs were to unload the burden of neighborhood managers and support public engagement in neighborhood governance. Deficits in resources, manpower and expertise disabled neighborhood committees to solely implement CVPCs, thereby necessitating partnering with other stakeholders and connecting with their resources and expertise (ID 10–13). One of our respondents argued that, senior governments exerted pressure on policy practitioners to attain vaccination goals. In this case, neighborhood committees unable to complete vaccination tasks had to collaborate with multiple stakeholders to jointly implement CVPCs in communities (ID 8). In addition, residents with volunteerism and community spirit desired to involve in CVPCs, to enhance vaccine acceptance among their neighbors, reach herd immunity and prevent virus spread in communities. The construction of the collaborative system of CVPCs offered channels for public participation in neighborhood governance (ID 6–7).
Organization of Partnerships in CVPCs
Coordinated approaches to implementing CVPCs involve shaping leadership in CVPCs, expanding collaborative networks of COVID-19 vaccine promotion, training HPPs, creating partnership agreements, producing promotional materials of COVID-19 vaccines, and marketing COVID-19 vaccines.
Shaping Leadership in CVPCs
Forming leadership in collective actions helps manage intra-organizational conflicts, intensify internal cohesion, connect with members’ expertise and resources and achieve goals efficiently.48 However, leadership in CVPCs was initially absent, as neighborhood committees, serving as managers of community COVID-19 vaccine programs, failed to integrate community recourse, resolve internal conflicts, and properly implement CVPCs (ID 9, 19–22). That greatly decreased public trust and eroded neighborhood committees’ initiatives in CVPCs. One volunteer we interviewed argued that,
In CVPCs, conflicts between members often occurred. However, neighborhood committee leaders failed to resolve these disputes, damaging organizational ties and eroding their leadership in CVPCs. Meanwhile, improperly implementing CVPCs triggered volunteers’ dissatisfaction with neighborhood committees. (ID 24)
Senior states conducted professional training and ideological and political education on neighborhood committee members and mobilized administrative officials to sink to communities to strengthen the leadership of neighborhood committees and manage conflicts in community CVPCs. Specifically, the sub-district office commissioned local CDC experts and experts in VASTPs to train HPPs in communities to improve their knowledge and marketing skills of COVID-19 vaccinations (ID 9, 14–17). State agencies conducted ideological and political education on neighborhood committee members via holding mobilization meetings and Chinese Communist Party (CCP) meetings to enhance their political loyalty and their compliance with government policies. These approaches helped achieve agreements among members of the neighborhood committees on strategies for implementing CVPCs, and construct neighborhood committees’ leadership in CVPCs. Additionally, the party-state also required governmental actors and CCP members to sink to communities to assist neighborhood committees in implementing CVPCs, which has also reinforced neighborhood committees’ leadership in CVPCs (ID 18, 1–4).
Expanding Collaborative Networks of CVPCs
The failure of neighborhood committees to independently implement CVPCs necessitated partnering with other stakeholders to unload their burdens. Strategies for expanding collaborative networks of CVPCs involved recruiting volunteers and collaborating with members of grid-based management system. In communities, many residents with volunteerism and CCP members and grassroots cadres with sense of serving the people proactively engaged in community-based COVID-19 vaccine promotion activities. However, these individuals who voluntarily advertised COVID-19 vaccines have not yet been organized officially. Recruiting these volunteers in the collaborative network of CVPCs helps integrate community resources (ID 57–61). One of our respondents argued that,
Organized by the Community Corrections Administration, offenders who serve penalities in communities actively participated in community vaccination programs, publicizing COVID-19 vaccines to residents, and raising funds to purchase necessities for vaccine promotion. Incorporating these individuals into the cooperative network helps optimize resource allocation and expand networks of HPPs. (ID 58)
Neighborhood committees also mobilized public engagement in CVPCs via propagandizing collectivism, altruism, and community spirit. For instance, banners hung up in communities claimed: promoting the spirit of Lei Feng (who was characterised as selfless and modest person devoted to the communist party) and assisting elders in vaccination; contributing to your efforts, caring for the weak and serving the society; promoting volunteerism and strengthening vaccine cooperation to build a great wall against the COVID-19 pandemic (ID 5–9, 62). Additionally, neighborhood committees partnered with members of the grid-based governance system. The grid management model has been widely deployed by the government to optimize community public service. As members of the grid-based governance system, property managers, homeowners’ committees, community public health service centers, and building directors are responsible for assisting neighborhood committees in delivering public services. Therefore, neighborhood committees can easily engage these stakeholders in the collaborative network of CVPCs (ID 7–19).
Training HPPs
Training HPPs helps them acquire skills of leveraging multiple media tools to advertise vaccines, and skills of managing their partnerships with others, and ensure vaccine promotion aligning with moral norms, individual rights and public demands.49 However, in practice, numerous HPPs lacked these skills, preventing them from sustaining successful partnerships with other members and advertising COVID-19 vaccines tailored to public needs and values. Specialized training on community HPPs is thus needed to boost their abilities to promote vaccines and to collaborate with others (ID 4–8). A secretary of the neighborhood committee argued that,
Conflicts often occurred between HPPs. Failure to resolve these disputes frustrated HPPs’ desire to collaborate. Therefore, they would rather clarify their respective responsibilities to favor independent work than cooperate with other members. (ID 8)
In response, the sub-district office and the neighborhood committee trained HPPs via conducting community-based learning activities, e-learning seminars, and practical guidance. Specifically, the sub-district office commissioned local CDC experts to conduct routine COVID-19 vaccination education seminars in communities to ensure that HPPs acquire adequate knowledge of COVID-19 vaccinations (ID 53–55). The sub-district office and neighborhood managers also connected with experts in VASTPs to conduct practical guidance and learning activities in communities to develop HPPs’ skills in immunization promotion (eg, utilizing various media tools, promoting vaccines from the public perspective and fitting community cultures, and in an easy-to-understand way) (ID 49–51). In addition, neighborhood committees also organized HPPs to participate in COVID-19 vaccination online learning seminars held by local states to favor their deep understanding of the laws, regulations, and professional knowledge of COVID-19 immunization, and vaccine promotion strategies (ID 23, 25–27).
Creating Partnership Agreements
A partnership agreement refers to a contract between all parties involved in starting a partnership, and this contract defines the rights and responsibilities of each partner to reduce potential conflicts, tighten up the teamwork, and improve productivity.50 In CVPCs, HPPs created partnership agreements to favor co-production of COVID-19 vaccine promotion. The neighborhood committee primarily drafted the formulation of a partnership agreement, and other partners were responsible for evaluating and confirming the final cooperation agreement.
Partnership agreements involve several matters. First, partnership agreements help identify partners, including the neighborhood committee, the community healthcare service center, property managers, homeowner’s association, volunteers, community polices, building directors, CDC experts, experts in the VASTP and et cetera (ID 3–19). Second, partnership agreements set schedules for implementing CVPCs. Timetabling CVPCs facilitates routine CVPC implementation and enhances their efficiency. Therefore, HPPs primarily scheduled CVPCs via open interaction and based on their availability (ID 28–31). Third, partnership agreements form personal code of conduct. Creating personal code of conduct favors friendly interaction and forming a tight partnership among members. Personal code of conduct in the partnership agreement includes, such as be kind to others, prohibiting any forms of abuse and violence against others, upholding CCP’s leadership, and practicing core socialist values (eg, harmony, friendship, integrity, and equality) (ID 32–35). Fourth, partnership agreements help manage conflicts involving disputes between HPPs and between HPPs and residents. They help tighten ties among HPPs and create public trust in CVPCs. To manage conflicts in CVPCs, the partnership agreement defines the conflict managers and conflict resolution principles. Conflict managers include leaders of neighborhood committees, of property companies, and of homeowner’s associations, community celebrities and community police, given their social influences in communities and interpersonal conflict management capacity. Conflict resolution principles involve such as respecting others, interacting openly, empathy, fairness, and handling conflicts in a timely manner (ID 36–41). Fifth, partnership agreements help develop schemes of CVPCs. Planning activities help identify required resources, expertise and potential risks in advance, thereby improving the efficiency of CVPCs. Designing schemes of CVPCs involves confirming specific affairs of CVPCs, and key organizers. Affairs of COVID-19 vaccine promotion activities generally include producing promotional materials about COVID-19 vaccines and advertising COVID-19 vaccines via various media tools. Meanwhile, neighborhood committees also identified key organizers for each activity based on the expertise and resources required for this activity and the organizers’ schedules. For instance, clinicians in the public healthcare service center led the implementation of vaccination science popularization activities; property companies were responsible for holding entertainment activities of vaccine promotion (ID 36–43).
Producing COVID-19 Vaccine Promotional Materials
Before advertising COVID-19 vaccines, HPPs need to produce promotional materials of COVID-19 vaccines. Promotional genres of COVID-19 vaccines involve creating popular science short videos and articles, brochures, banners, posters, and display boards.
In the era of social media, popular science short videos and articles exert a key role in delivering scientific knowledge and advertising vaccines. Short video marketing is an easy way to evoke public emotion and cater to public preferences. Marketing via popular science articles facilitates comprehensively responding to public concerns and vaccine misinformation.51 Therefore, HPPs jointly created popular science articles of COVID-19 vaccines based on scientific evidence, experts’ opinions and clinical trial data to address COVID-19 vaccine misinformation in online communities. Meanwhile, HPPs were involved in creating popular science short videos to ensure short video marketing tailored to community cultures and norms (36–40). Creating popular science short videos involved copywriting, video recording, and editing, necessitating engaging with media professionals. To this end, neighborhood committees recruited media professionals to steer the creation of popular science short videos. Specifically, HPPs and media professionals first gained insight into residents’ concerns and needs via empirical investigation to facilitate copywriting. Subsequently, influential community figures and residents supporting vaccination were invited to appear on camera to publicize the safety, effectiveness, and importance, urgency and precautions of COVID-19 vaccines. Finally, media professionals edited these videos to enhance their viewing experience (ID 2–5, 41–45). A director of the neighborhood committee argued that,
Led by media professionals, community HPPs distributed their responsibilities in popular science short video creating: some members wrote copies, some members reached influential figures to appear on camera and some involved in video editing. (ID 5)
Traditional media such as banners, brochures and posters also play a critical role in promoting vaccines. Banner advertising adopts concise and easy-to-understand expression and integrates slogans and socialist values, encouraging public obedience to social morality. Marketing brochures offer a wealth of information and facilitate audiences’ reading at their leisure.52 Marketing posters are a medium of bright colors, bold fonts, and striking images. They use visual aesthetics to vividly convey key information, catch target audiences’ eyes, and generate a lasting impression. As such, HPPs conducted brainstorming sessions to promote creative thinking, create banner slogans, and designed posters and brochures based on pop culture, core socialist values and public preferences (ID 46–48).
Marketing COVID-19 Vaccines
HPPs advertised COVID-19 vaccines via social media, official websites, digital tools, traditional media, and community-based activities. In Chinese semi-acquaintance structured societies, high trust in acquaintances enables acquaintances to exert a positive influence in persuading target audiences to get vaccinated. Social media, such as Sina Weibo, TikTok and WeChat, supports HPPs advertising COVID-19 vaccines to people they are acquainted with. Promoting vaccines via official media, such as official websites of and official WeChat accounts of the neighborhood committee, helps increase the reliability of information sources and public acceptance of vaccines. The application of digital media, such as broadcast and outdoor digital screen, can also reach a wide audience and increase the efficiency of vaccine promotion.53 Traditional media, such as banners, posters and loudspeakers, once viewed as the mouthpiece of the government in the Maoist era, was employed to propagandize public affairs and implement mass mobilization campaigns in the neighborhood. Traditional media marketing portrayed vaccine promotion activities as political campaigns, aiming to intensify the public’s obedience to government authorities and boost vaccine acceptance. Performing community-based activities, involving informative and entertaining events, not only increases the interestingness of vaccine promotion but also positions target audiences in a virtual theater, stimulating them to perceive the benefits of vaccination and the risks of non-vaccination, thereby eliciting their vaccine acceptance.54 In practice, HPPs flexibly leveraged diverse mediums to promote COVID-19 vaccines. Specifically, they forwarded popular science short videos and articles of COVID-19 vaccines using personal social media accounts to facilitate their acquaintances access to these messages. Neighborhood committees delivered real-time COVID-19 vaccine news, policies, knowledge and schedules of comm, unity COVID-19 vaccination programs to residents via their official websites, WeChat public accounts and the smart community application to ensure that residents gained authoritative information. Neighborhood committees also advertised COVID-19 vaccines in communities via traditional media tools, such as banners, posters, brochures, and loudspeakers (ID 27–33). One of our respondents indicated that,
Banners hung up in communities claimed that: To protect your family members, please get fully vaccinated; COVID-19 vaccination benefits both oneself and others; COVID-19 vaccination helps reach herd immunity. (ID 28)
CVPCs also emphasized multistakeholder collaboration to persuade vaccine refusers to get vaccinated. For instance, medical professionals, neighborhood committee leaders, and acquaintances of target audiences visited residents’ home to market COVID-19 vaccines tailored to their concerns and needs. Additionally, HPPs also promoted COVID-19 vaccines via science popularization and entertaining activities. Science popularization aims to convey scientific knowledge to citizens to foster them to rationally think about vaccinations. In communities, HPPs primarily conducted science popularization seminars and COVID-19 vaccine knowledge contests by partnering with clinicians and CDC experts.38 Entertaining marketing refers to promoting a brand or an idea through a series of entertainment activities to elicit audiences’ emotions and create last impression on audiences.55 In communities, HPPs organized diverse recreational activities, such as poem recitation, situational performance and parent–child interaction therapies, where residents can engage, to increase the interactivity of vaccine promotion activities and the attractiveness of vaccine promotion to residents (ID 5–8, 52, 56, 33–35).
Implications of Coordinated CVPCs for China’s Neighborhood Governance
Co-production of CVPCs has exerted subtle impact on China’s neighborhood governance structure. On the one hand, co-production of CVPCs stimulated citizens to actively engage in neighborhood governance, favored reciprocal interaction of and mutual trust between states and society, and enhanced state responsiveness to public demands. On the other hand, in CVPCs, multiple sub-cooperative networks led by various stakeholders arose and functioned independently, which helps curb partners’ disagreements on government strategies to implement CVPCs, enable the flexible implementation of coproduction of CVPC, and create polycentric governance structure in the neighborhood. However, weak ties and the lack of resource and information sharing between these sub-cooperative systems to some extent eroded partnerships in neighborhood governance.
Partnerships in CVPCs imply nuances in state-society relationships in Chinese neighborhood governance. States’ failure to implement CVPCs solely necessitates partnering with societal forces. Meanwhile, engaging the public in neighborhood governance helps expand grassroots autonomy and democracy and construct a robust neighborhood governance infrastructure in an authoritarian context. To stimulate public participation in CVPCs, community HPPs advertised volunteerism, altruism, and civic awareness to elicit the public’s awareness of social responsibility and collective spirit and encourage public engagement in scrutinizing political affairs to maintain public interests. They also advertised a cooperative spirit to bolster neighborhood ties in response to threats. In the coordinated CVPCs, frequent state-society interaction supported neighborhood committees discerning public demands and values, increased neighborhood committees’ awareness of serving the people, and enhanced public trust in states (ID 7–11). Meanwhile, COVID-19 vaccine promotion practice has constructed a public sphere that facilitated a reciprocal dialogue between the state and the public and increased the responsiveness of state agencies to public demands at the grassroots level (ID 27–32). To implement CVPCs, HPPs leveraged social media to create online communities where grassroots-level officials and neighborhood managers engaged to favor interaction between partners and promote vaccines to residents. In online communities, citizens could reach state actors directly to express their needs and opinions. The inadequate response of state actors to public demands would spur public expressing their negative sentiments in virtual communities. Therefore, state actors and neighborhood managers must actively respond and address public needs and incorporate feasible public opinions into their decisions (ID 13–15). One of our respondents argued that,
Neighborhood committee members can swiftly respond to public needs in WeChat groups. That is not only attributed to the neighborhood committee’s concern that negative public sentiment expression in virtual communities may damage their reputation but also to their increasing awareness of serving the people. (ID 13)
Multiple leadership structures have been formed in the collaborative network of CVPCs. The vaccination promotion cooperative network involves not only the sub-collaborative network led by the government but also multiple sub-networks oriented by other stakeholders, such as property managers, volunteers, and clinicians. The emergence of these sub-collaborative networks can be ascribed to HPPs’ disagreements on the schedule and strategies for implementing CVPCs. On the one hand, HPPs’ failure to reach agreements on the CVPV implementation schedule led to a rise in multiple sub-cooperative networks favoring HPPs that flexibly implemented CVPCs based on availability (ID 11–14). On the other hand, some HPPs advocated for CVPCs, but did not endorse strategies employed by states to implement CVPCs, such as stigmatizing unvaccinated people, advertising COVID-19 vaccines underpinned by collectivism and political authority, and neglecting individualism. Therefore, these HPPs conducted CVPCs independently of the government (ID 28–32). A volunteer we interviewed argued that,
We perceived the importance of COVID-19 vaccines in curbing virus spread. Nonetheless, I am dissatisfied with strategies used by neighborhood committees to promote vaccines. To enhance vaccine rates, they stigmatized non-vaccinators as immoral, unpatriotic, selfish, and violating community conventions. These strategies are less inclusive and fail to reconcile collective and individual interests. Therefore, we prefer to conduct CVPCs independently of the neighborhood committee. (ID 31)
However, the independent function of multiple sub-cooperative systems of COVID-19 vaccine promotion substantially eroded partnerships in neighborhood governance. In CVPCs, value conflicts between governments and citizens damaged state-civil society partnerships in the neighborhood. Meanwhile, interaction and information and resource sharing among these sub-collaborative networks of COVID-19 vaccine promotion led by multiple stakeholders are weak, decreasing co-production of neighborhood governance (ID 3–5, 35–37). Therefore, community immunization program managers should construct shared values among HPPs via reciprocal interactions to promote the latter’s agreements on strategies for implementing CVPVs. Furthermore, community immunization program managers must consolidate partnerships between sub-collaborative networks of COVID-19 vaccine promotion oriented by multiple stakeholders via resource and information sharing to construct robust collaborative infrastructures of COVID-19 vaccine promotion (ID 4, 35–37).
Discussion
Our analysis shows that co-production of CVPCs was launched to unload the burden of neighborhood managers and promote public engagement in neighborhood governance. The components of collaborative CCPVs involve shaping leadership in CVPCs, expanding the collaborative network, training HPPs, creating partnership agreements, producing COVID-19 vaccine promotional materials, and advertising COVID-19 vaccines via multiple media. The implications of the CVPC co-production for Chinese neighborhood governance exhibit dual tendencies. On the one hand, coordinated CVPCs supported reciprocal interaction between states and society and state responsiveness to public demands at the neighborhood level. On the other hand, HPPs’ disagreements on strategies employed by states for promoting COVID-19 vaccines and the independent function of multiple sub-cooperative systems of COVID-19 vaccine promotion eroded partnerships in neighborhood governance. Therefore, neighbourhood immunization program managers should create shared values among HPPs, and intensify partnerships between multiple sub-collaborative networks of COVID-19 vaccine promotion to forge robust collaboration infrastructures of COVID-19 vaccine promotion.
The implementation of global CVPCs has raised scholarly attention to partnerships in CVPCs. Extant research centers on strategies for constructing collaborative networks of CVPCs and vulnerabilities of coordinated CVPCs in countries other than China. Strategies to construct collaborative networks of CVPCs involve partnering with influential figures, constructing participatory vaccine promotion programs, empowering HPPs and forming leadership in CVPCs. Influential figures serving as COVID-19 vaccine ambassadors help reach a wider audience and enhance public trust in COVID-19 vaccine programs and vaccine acceptance. As such, several scholars suggested connecting with social media influencers to deter online misinformation and create an information environment conducive to COVID-19 vaccinations,56 partnerships with community celebrities and trusted individuals to promote vaccine acceptance in the US,57 and coordination with religious leaders to advertise COVID-19 vaccines among their followers based on religious beliefs and moral obligations.58,59 Nguyen and Catalan proposed creating participatory mechanisms to engage more volunteers in immunization programs to ensure vaccine promotion aligned with genuine public demands and values in the West.60 Afolabi and Ilesanmi suggested empowering HPPs via specialized training to enhance their ability to handle conflicts in teams and implement inclusive vaccine promotion activities in Europe.54 Tahir et al highlighted the pivotal role of states in implementing CVPCs, given their prominent competence to mobilize social engagement and integrate social resources in Pakistan.61 Additionally, Quinn et al indicated challenges of collaborative CVPCs, including weak ties, a lack of mutually beneficial and trusted partnerships, and poor information and resource sharing among partners in the US.62 Similar to previous studies, our study also highlighted state-led CVPCs, partnerships with diverse stakeholders, empowering HPPs, and identified the vulnerabilities of collaborative COVID-19 vaccine promotion approaches. Building upon previous studies, this research revealed specific strategies for implementing collaborative CVPCs in communities and the dual implications of the coordinated CVPC for Chinese neighborhood governance. Interestingly, our analysis indicates that coordinated CVPCs exhibited a stress-response pattern in China. The lack of common interests and shared values among HPPs and HPPs’ disagreements on strategies employed by states for implementing CVPCs weakened partnerships in CVPCs. In response, senior states conventionally tweaked grassroots-level states and mobilized public participation to ensure the active performance of policy practitioners and maintain multistakeholder collaboration to carry out CVPCs. However, when political pressure subsides, ties between stakeholders in communities are weak. Therefore, senior governments had to persistently exert political pressure on policy practitioners to sustain co-production of CVPCs in neighborhoods.
Tweaking the institution has to a certain extent politicized COVID-19 vaccine promotion programs in neighborhoods. To ensure the political loyalty of policy practitioners and their active performance, senior states tightened the rein on grassroots-level states by conducting top-down inspections, political mobilization, and ideological and political education, and steer the bureaucracy by leveraging carrots and sticks.63 They also created political discourses and moral norms underpinned by collectivism, altruism, and patriotism related to COVID-19 vaccinations to ensure public compliance with states and elicit vaccine acceptance. While the political tendency of vaccine promotion programs has enhanced the institutional efficiency of Chinese CVPCs, it triggered value conflicts between states and citizens, decreased public trust, and eroded partnerships in neighborhood governance. At the same time, citizens considered promoting collectivism and patriotism that encourages public compliance with state authorities to be moral hijacking, sparking public opposition to campaign-style governance in China. Therefore, creating shared values among multistakeholders in co-production of neighborhood governance warrants further research.
Limitation of the Research
This qualitative study deepened our understanding of partnerships in CVPCs in Chinese communities. Nonetheless, this research must be considered against the backgrounds of its limitations. First, we accessed participants in an informal and snowballing approach instead of a scientific sampling method to align with China’s highly relationship-oriented society.64 However, data gleaning by snowballing in this study has conformed to the principle of data saturation. Second, although we approached diverse stakeholders, collected data based upon the data saturation principle and evaluated inter-coder reliability to increase the validity of data collection and coding, a more rigorous thematic analysis, such as researcher triangulation, description of audit trails, peer debriefing and member checking, should be conducted to establish trustworthiness in qualitative research. Finally, this study centers on CVPCs in urban communities, but not yet on COVID-19 vaccine promotion in rural China. According to Li et al, China’s urban-rural divide with a focus on constraining rural-to-urban mobilization by a household registration system instituted by the government in 1958 and differentiated resource input between rural and urban areas caused urban-rural differences in the contexts, strategies and risks of COVID-19 vaccination promotion activities.65 Future research is thus expected to explore coordinated CVPCs in rural China.
Conclusion
COVID-19 vaccine promotion helps counter vaccine hesitancy and raise vaccine acceptance. Therefore, the Chinese state implemented coordinated CVPCs in communities to unload the burden of neighborhood managers and facilitate stakeholder engagement. To favor co-production of CVPCs, neighborhood managers created leadership in CVPCs, expanded cooperative networks of CVPCs and trained HPPs, and partnered with other HPPs to shape partnership agreements, produce promotional materials and advertise COVID-19 vaccines. Although coordinated COVID-19 vaccine marketing efforts have promoted state-society interaction in neighborhoods and state responsiveness to public demands, excessive political intervention induced citizens’ disagreements on strategies for implementing CVPCs and eroded partnerships in neighborhood governance. Depoliticizing CVPVs and implementing a social marketing campaign led by diverse stakeholders to encourage COVID-19 vaccination in China are therefore needed.
Abbreviations
CVPC, COVID-19 Vaccine Promotion Campaign; HPP, Health Promotion Practitioner; CDC, Center for Disease Control; VASTP, Volunteer Association for Science and Technology Promotion; CVP, COVID-19 Vaccine Programs, Chinese Communist Party.
Data Sharing Statement
All data and materials were included in this paper. We can provide all data upon reasonable request after all studies and sub-studies have been completed.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki. Informed consent was obtained from the investigated participants, and all participants were fully anonymized before further analysis. The University Research Ethics Committee at the College of Humanities of Donghua University (URECFHDU) approved this study and offered a waiver of consent for analysis, as this study presents no more than minimal risks to participants and does not require ethical approval according to Chinese law.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Fundamental Research Funds for the Central Universities (No. 2232023E-05), the Shanghai Committee of Science and Technology (No. 23YF1425200), Soft Science Key Program Fund from Shanghai 2022 “Action Plan of Technological Innovation” (No.22692199300) and the Fundamental Research Funds for the Central Universities (No.2232022E-13).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Okan O, Messer M, Levin-Zamir D, Paakkari L, Sørensen K. Health literacy as a social vaccine in the COVID-19 pandemic. Health Promotion Int. 2022;38(4):daab197. doi:10.1093/heapro/daab197
2. Group C 19 VTW. Technical vaccination recommendations for COVID-19 vaccines in China. China CDC Weekly. 2021;3(21):459. doi:10.46234/ccdcw2021.083
3. The state council. China releases measures to optimize COVID-19 response. Xinhua; 2022. Available from: https://english.www.gov.cn/news/topnews/202211/11/content_WS636e31efc6d0a757729e2e63.html.
4. Yin F, Wu Z, Xia X, Ji M, Wang Y, Hu Z. Unfolding the determinants of COVID-19 vaccine acceptance in China. J Med Int Res. 2021;23(1):e26089. doi:10.2196/26089
5. Wang J, Yuan B, Lu X, et al. Willingness to accept COVID-19 vaccine among the elderly and the chronic disease population in China. Hum Vaccines Immunother. 2021;17(12):4873–4888. doi:10.1080/21645515.2021.2009290
6. Wong M, Wong EL, Cheung AW, et al. COVID-19 vaccine hesitancy in a city with free choice and sufficient doses. Vaccines. 2021;9(11):1250. doi:10.3390/vaccines9111250
7. Tong KK, He M, Wu A, Dang L, Chen JH. Cognitive factors influencing COVID-19 vaccination intentions: an application of the protection motivation theory using a probability community sample. Vaccines. 2021;9(10):1170. doi:10.3390/vaccines9101170
8. Wang X. Putting emotions in the health belief model: the role of hope and anticipated guilt on the Chinese’s intentions to get COVID-19 vaccination. Health Communication. 2023;38(11):2491–2500. doi:10.1080/10410236.2022.2078925
9. Moran MB, Lucas M, Everhart K, Morgan A, Prickett E. What makes anti-vaccine websites persuasive? A content analysis of techniques used by anti-vaccine websites to engender anti-vaccine sentiment. J Commun Healthcare. 2016;9(3):151–163. doi:10.1080/17538068.2016.1235531
10. Bueno de Mesquita E, Dickson ES. The propaganda of the deed: terrorism, counterterrorism, and mobilization. Am J Political Sci. 2007;51(2):364–381. doi:10.1111/j.1540-5907.2007.00256.x
11. Denton RE Jr, Trent JS, Friedenberg RV. Political Campaign Communication: Principles and Practices. Rowman & Littlefield; 2019.
12. Shropshire AM, Brent-Hotchkiss R, Andrews UK. Mass media campaign impacts influenza vaccine obtainment of university students. J Am College Health. 2013;61(8):435–443. doi:10.1080/07448481.2013.830619
13. Bonnevie E, Rosenberg SD, Kummeth C, Goldbarg J, Wartella E, Smyser J. Using social media influencers to increase knowledge and positive attitudes toward the flu vaccine. PLoS One. 2020;15(10):e0240828. doi:10.1371/journal.pone.0240828
14. Park SY. The effects of message framing and risk perceptions for HPV vaccine campaigns: focus on the role of regulatory fit. Health Mark Q. 2012;29(4):283–302. doi:10.1080/07359683.2012.732847
15. Wood S, Schulman K. When vaccine apathy, not hesitancy, drives vaccine disinterest. JAMA. 2021;325(24):2435–2436. doi:10.1001/jama.2021.7707
16. Feng L, Mounts AW, Feng Y, et al. Seasonal influenza vaccine supply and target vaccinated population in China, 2004–2009. Vaccine. 2010;28(41):6778–6782. doi:10.1016/j.vaccine.2010.07.064
17. Dhama K, Sharun K, Tiwari R, et al. COVID-19 vaccine hesitancy–reasons and solutions to achieve a successful global vaccination campaign to tackle the ongoing pandemic. Hum Vaccines Immunother. 2021;17(10):3495–3499. doi:10.1080/21645515.2021.1926183
18. Latkin C, Dayton LA, Yi G, et al. COVID-19 vaccine intentions in the United States, a social-ecological framework. Vaccine. 2021;39(16):2288–2294. doi:10.1016/j.vaccine.2021.02.058
19. Decouttere C, De Boeck K, Vandaele N. Advancing sustainable development goals through immunization: a literature review. Globalization Health. 2021;17(1):95. doi:10.1186/s12992-021-00745-w
20. Steffens MS, Dunn AG, Leask J, Wiley KE. Using social media for vaccination promotion: practices and challenges. Digital Health. 2020;6:2055207620970785. doi:10.1177/2055207620970785
21. Lutkenhaus RO, Jansz J, Bouman MP. Tailoring in the digital era: stimulating dialogues on health topics in collaboration with social media influencers. Digital Health. 2019;5:2055207618821521. doi:10.1177/2055207618821521
22. Metcalfe SE, Sexton EH. An academic‐community partnership to address the flu vaccination rates of the homeless. Public Health Nurs. 2014;31(2):175–182. doi:10.1111/phn.12088
23. Volpp KG, Loewenstein G, Buttenheim AM. Behaviorally informed strategies for a national COVID-19 vaccine promotion program. JAMA. 2021;325(2):125–126. doi:10.1001/jama.2020.24036
24. Wang TL, Jing L, Bocchini JA Jr. Mandatory influenza vaccination for all healthcare personnel: a review on justification, implementation and effectiveness. Curr Opin Pediatr. 2017;29(5):606–615. doi:10.1097/MOP.0000000000000527
25. Steffens MS, Dunn AG, Wiley KE, Leask J. How organisations promoting vaccination respond to misinformation on social media: a qualitative investigation. BMC Public Health. 2019;19(1):1–12. doi:10.1186/s12889-019-7659-3
26. Hedt-Gauthier B, Airhihenbuwa CO, Bawah AA, et al. Academic promotion policies and equity in global health collaborations. Lancet. 2018;392(10158):1607–1609. doi:10.1016/S0140-6736(18)32345-6
27. Seaton CL, Holm N, Bottorff JL, et al. Factors that impact the success of interorganizational health promotion collaborations: a scoping review. Am J Health Promotion. 2018;32(4):1095–1109. doi:10.1177/0890117117710875
28. Merzel C, D’Afflitti J. Reconsidering community-based health promotion: promise, performance, and potential. Am J Public Health. 2003;93(4):557–574. doi:10.2105/AJPH.93.4.557
29. Feng J, Qin LI. How to ensure vaccine safety: an evaluation of China’s vaccine regulation system. Vaccine. 2021;39(37):5285–5294. doi:10.1016/j.vaccine.2021.07.081
30. He H, Wang L, Li J. The impact of emergencies on vaccination services, risk assessment and response suggestions. Chin J Prevent Med. 2021;55:10.
31. Zhao H, Sun P. Research on negotiation and public rationality in internet public opinion events. J Northeast Univ. 2019;21:2.
32. Yu J, Zhu X, Gao X. Co-evolution logic of government function transformation and market supervision and governance system construction. Manage World. 2020;36:2.
33. Wang Y, Zhang L. Status of public–private partnership recognition and willingness to pay for private health care in China. Int J Health Plann Manag. 2019;34(2). doi:10.1002/hpm.2757
34. Du Z, Luo X, Su L. Collective action under social expectations: a study on the cognitive construction of media exposure on the public’s willingness to be vaccinated against the new coronavirus. Int Journalism. 2022;44(4):53–77.
35. Lin S, Liu Q, Zhang S, Pate RR. Evaluation of the effectiveness of vaccination management model for migrant children using big data platform. Mod Preventive Med. 2007;44(3):153–159. doi:10.1016/j.ypmed.2006.10.001
36. Lin Y. Investigation and research on the vaccination rate of 7 kinds of vaccines in the immunization program of migrant children in Rudong County. Syst Med. 2018;3:17.
37. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quantity. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
38. Yang R, Penders B, Horstman K. Vaccine hesitancy in China: a qualitative study of stakeholders’ perspectives. Vaccines. 2020;8(4):650. doi:10.3390/vaccines8040650
39. Yang R, Penders B, Horstman K. Addressing vaccine hesitancy in China: a scoping review of Chinese scholarship. Vaccines. 2019;8(1):2. doi:10.3390/vaccines8010002
40. Notarte KI, Guerrero‐Arguero I, Velasco JV, et al. Characterization of the significant decline in humoral immune response six months post‐SARS‐CoV‐2 mRNA vaccination: a systematic review. J med virol. 2022;94(7):2939–2961. doi:10.1002/jmv.27688
41. Notarte KI, Ver AT, Velasco JV, et al. Effects of age, sex, serostatus, and underlying comorbidities on humoral response post-SARS-CoV-2 Pfizer-BioNTech mRNA vaccination: a systematic review. Crit Rev Clin Lab Sci. 2022;59(6):373–390. doi:10.1080/10408363.2022.2038539
42. Notarte KI, Catahay JA, Peligro PJ, et al. Humoral response in hemodialysis patients post-SARS-CoV-2 mRNA vaccination: a systematic review of literature. Vaccines. 2023;11(4):724. doi:10.3390/vaccines11040724
43. Notarte KI, Catahay JA, Velasco JV, et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: a systematic review. E Clin Med. 2022;3:53.
44. Chopra H, Choudhary OP, Choudhary OP. mRNA vaccines as an armor to combat the infectious diseases. Travel Med Infectious Dis. 2023;52:102550. doi:10.1016/j.tmaid.2023.102550
45. Choudhary OP, Choudhary P, Singh I. India’s COVID-19 vaccination drive: key challenges and resolutions. Lancet Infect Dis. 2021;21(11):1483–1484. doi:10.1016/S1473-3099(21)00567-3
46. Abusalah MAH, Chopra H, Sharma A, et al. Nanovaccines: a game changing approach in the fight against infectious diseases. Biomed Pharmacother. 2023;167:115597.
47. Choudhary OP, Singh I, Singh I. Protective immunity against COVID-19: unravelling the evidences for humoral vs. cellular components. Travel Med Infectious Dis. 2021;39:101911. doi:10.1016/j.tmaid.2020.101911
48. Yang R, Qi Y. Neighbourhood governance, citizen initiatives and media application: investigating community group buying during Shanghai’s COVID lockdown. Int J Disaster Risk Reduct. 2023;93:103793. doi:10.1016/j.ijdrr.2023.103793
49. Nyhan B, Reifler J, Richey S, Freed GL. Effective messages in vaccine promotion: a randomized trial. Pediatrics. 2014;133(4):e835–e842. doi:10.1542/peds.2013-2365
50. Wallerstein N, Duran B, Oetzel JG, Minkler M. Community-Based Participatory Research for Health: Advancing Social and Health Equity. John Wiley & Sons; 2017.
51. Puri N, Coomes EA, Haghbayan H, Gunaratne K. Social media and vaccine hesitancy: new updates for the era of COVID-19 and globalized infectious diseases. Hum Vaccines Immunother. 2020;16(11):2586–2593. doi:10.1080/21645515.2020.1780846
52. Desai V, Vidyapeeth B. Digital marketing: a review. Int J Trend Sci Res Dev. 2019;5(5):196–200. doi:10.31142/ijtsrd23100
53. Lamberton C, Stephen AT. A thematic exploration of digital, social media, and mobile marketing: research evolution from 2000 to 2015 and an agenda for future inquiry. J Marketing. 2016;80(6):146–172. doi:10.1509/jm.15.0415
54. Afolabi AA, Ilesanmi OS. Addressing COVID-19 vaccine hesitancy: lessons from the role of community participation in previous vaccination programs. Health Promotion Perspect. 2021;11(4):434. doi:10.34172/hpp.2021.54
55. Peddecord KM, Jacobson IG, Engelberg M, Kwizera L, Macias V, Gustafson KW. Can movie theater advertisements promote health behaviors? Evaluation of a flu vaccination pilot campaign. J Health Commun. 2008;13(6):596–613. doi:10.1080/10810730802285149
56. Hernandez RG, Hagen L, Walker K, O’Leary H, Lengacher C. The COVID-19 vaccine social media infodemic: healthcare providers’ missed dose in addressing misinformation and vaccine hesitancy. Hum Vaccines Immunother. 2021;17(9):2962–2964. doi:10.1080/21645515.2021.1912551
57. Bogart LM, Dong L, Gandhi P, et al. What Contributes to COVID-19 Vaccine Hesitancy in Black Communities, and How Can It Be Addressed? RAND Santa Monica;2021.
58. Achrekar GC, Batra K, Urankar Y, et al. Assessing COVID-19 booster hesitancy and its correlates: an early evidence from India. Vaccines. 2022;10(7):1048. doi:10.3390/vaccines10071048
59. Galang JRF. Science and religion for COVID-19 vaccine promotion. J Public Health. 2021;43(3):e513–e514. doi:10.1093/pubmed/fdab128
60. Nguyen A, Catalan D. Digital mis/disinformation and public engagement with health and science controversies: fresh perspectives from Covid-19. Media and Communication. 2020;8(2):323–328. doi:10.17645/mac.v8i2.3352
61. Tahir MJ, Saqlain M, Tariq W, et al. Population preferences and attitudes towards COVID-19 vaccination: a cross-sectional study from Pakistan. BMC Public Health. 2021;21(1):1–12. doi:10.1186/s12889-021-11814-5
62. Quinn A, White A, Abbatangelo-Gray J, McCarron S, Schub T, Ratzan SC. COVID-19 communication campaigns for vaccination: an assessment with perspectives for future equity-centered public health efforts. J Health Commun. 2023;28(sup1):54–66. doi:10.1080/10810730.2023.2208529
63. He AJ, Shi Y, Liu H. Crisis governance, Chinese style: distinctive features of China’s response to the Covid-19 pandemic. Policy Design Pract. 2020;3(3):242–258. doi:10.1080/25741292.2020.1799911
64. Yang MM. Gifts, Favors, and Banquets: The Art of Social Relationships in China. Cornell University Press; 2016.
65. Li X, Deng Y, Tang W, et al. Urban-rural disparity in cancer incidence, mortality, and survivals in Shanghai, China, during 2002 and 2015. Front Oncol. 2018;8:579. doi:10.3389/fonc.2018.00579
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.