Back to Journals » International Journal of Women's Health » Volume 13
Calcium Consumption During Pregnancy: A Multicenter Study in a Middle-Income Country in Southeast Asia
Authors Panburana P ![]() , Komwilaisak R
, Komwilaisak R ![]() , Tongprasert F
, Tongprasert F ![]() , Phadungkiatwattana P, Kor-anantakul O, Lumbiganon P
, Phadungkiatwattana P, Kor-anantakul O, Lumbiganon P ![]()
Received 7 October 2020
Accepted for publication 28 December 2020
Published 6 January 2021 Volume 2021:13 Pages 31—38
DOI https://doi.org/10.2147/IJWH.S285516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Panyu Panburana,1 Ratana Komwilaisak,2 Fuanglada Tongprasert,3 Podjanee Phadungkiatwattana,4 Ounjai Kor-anantakul,5 Pisake Lumbiganon2
1Department of Obstetrics & Gynecology, Faculty of Medicine, Ramathibodi University Hospital, Mahidol University, Bangkok, Thailand; 2Department of Obstetrics & Gynecology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 3Department of Obstetrics & Gynecology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 4Rajavithi Hospital, Ministry of Public Health, Bangkok, Thailand; 5Department of Obstetrics & Gynecology, Faculty of Medicine, Songklanagarind Hospital, Prince of Songkla University, Hat Yai, Songkhla, Thailand
Correspondence: Panyu Panburana
Department of Obstetrics & Gynecology, Faculty of Medicine, Ramathibodi University Hospital, Mahidol University, Bangkok, Thailand
Email [email protected]
Objective: To perform a cross-sectional observational study of calcium consumption among pregnant women from multicenter tertiary care hospitals in the middle-income country in Southeast Asia.
Study Design: A cross-sectional observational study.
Setting: The study was conducted in four geographical regions (northern, northeastern, southern, and central) of Thailand. Five participating hospitals consisted of one university hospital in each region and one additional tertiary care hospital in the central region.
Materials and Methods: A cross-sectional study was performed nationwide from 1st November 2017 to 31st January 2019. All singleton aged 19– 40 years were included. Exclusion criteria were any conditions that influenced calcium-containing food consumption. Dietary intake self-records immediately after eating for two working days and one holiday were analyzed via INMUCAL-NV3.0 dietary program.
Results: The 1549 records were obtained. The mean age was 29 ± 5.7 years. Most participants were primigravida (48.6%). The average gestational age was 20.6 ± 8.8 weeks. Mean calcium consumption was 602.4 mg/day (95% CI; 589.2615.6 mg/day) mg/dL. Inadequate calcium consumption prevalence based on the Thai dietary reference intake (less than 800 mg/day) and US Institute of Medicine (less than 1000 mg/day) were 82.0% and 93.4%, respectively.
Conclusion: The mean calcium consumption among pregnant women in the middle-income country in Southeast Asia was 602.4 mg/day (95% CI 589.2– 615.6 mg/day). Inadequate calcium consumption of Thai pregnant women prevalence was 82.0% and 93.4% according to Thai dietary reference intake in pregnancy and the US Institute of Medicine.
Keywords: calcium consumption, pregnancy, a middle-income country, Southeast Asia
Introduction
Calcium is an indispensable element for normal physiologic function, especially during pregnancy for both mothers and fetuses.1 The high fetal demand for calcium during pregnancy results not only in increasing maternal bone turnover but also in impacting on infants’ bone density.2 There are pieces of evidence of the inverse relationship between calcium consumption and preeclampsia.3–5 Increased parathyroid hormone and 1,25-hydroxyvitamin D levels in low calcium-consumption mothers may come with intracellular calcium elevation that causes high blood pressure due to increased vascular muscle tone.6,7 Hypertensive disorder in pregnancy is one of the leading causes of maternal death, with a Maternal Mortality Ratio (MMR) of 3.5 per 100,000 live births in Thailand in 2018.8 The analysis of the world health organization’s multicountry survey on maternal and newborn health revealed preeclampsia incidence worldwide, and Thailand was 2.16% and 2.22%, respectively, in 2013.9 World Health Organization recommended routine calcium supplementation from 20 weeks of pregnancy at doses of 1.5–2.0 g per day, particularly in a population with low calcium consumption to prevent preeclampsia.3 A recent systematic review and meta-analysis summarized that the mean calcium consumption in pregnancy in high-income countries (HICs) and low-and middle-income countries (LMICs) were 948.3 mg/day (95% CI 872.1–1024.4 mg/day) and 647.6 mg/day (95% CI 568.7–726.5 mg/day), respectively. This paper also reported that the incidences of calcium consumption below 800.0 mg/day in HICs and LMICs were 29% and 82%, respectively.6 Unfortunately, the data on calcium consumption in pregnant women across Thailand, which is now one of the middle-income countries in Southeast Asia, are still lacking. Only two studies reported calcium consumption incidence in some local areas of Thailand.10,11 The comprehensive information about calcium consumption in pregnancy is very important for policymakers to decide whether routine calcium supplementation during pregnancy is necessary or not. The National Health Security Office of Thailand is considering implementing calcium supplementation as a beneficial package for all Thai pregnant women. This study aimed to evaluate the calcium consumption of Thai pregnant women in four different regions of Thailand, which are different in geography and in culture and ways of life, especially in dietary intake.
Materials and Methods
Study Design
A multicenter hospital-based, cross-sectional study from four geographical regions of Thailand was performed from 1st November 2017 to 31st January 2019. This study was approved by the central research ethics committee (ref. no. CREC008/60BRm) and endorsed by each study site’s hospital ethics committee. Written informed consent records were obtained from all participants. This study was conducted in accordance with the declaration of Helsinki.
Setting
The study was conducted in four geographical regions (northern, northeastern, southern, and central) of Thailand. Five participating hospitals consisted of one university hospital in each region and one additional tertiary care hospital in the central region.
Participants
Participants were pregnant women who attended the antenatal care at the five participating hospitals from four geographic regions of Thailand during the study period. The study included pregnant women at the age of 19–40 years and all pregnancies of any ethnic groups, parities, education levels, and socio-economic statuses. Exclusion criteria were as follows: any conditions that hampered the calcium intake, history of calcium allergy, sarcoidosis, increased parathyroid gland activity, kidney stones, and decreased kidney function. Vegetarians were also excluded. We planned to recruit participants by trimester, 25%, 50%, and 25% in the first, second, and third trimesters.
Data Sources and Measurement
Data collection was performed at the antenatal clinic by using a standardized dietary chart record. Prospective self-written dietary records of types and amount of raw material, ingredients, seasoning, as well as the names of a ready-to-eat dietary menu in two weekdays and one holiday, were performed. Trained research nurses identified eligible participants among women who attended antenatal care clinic using inclusion and exclusion criteria described above. They then explained to eligible participants on how to record the dietary charts correctly. Diaries of what, when, and how much food was eaten were demonstrated via food illustration and quantity measurement. With an accurate summary of food record, error associated with memory was minimized by the immediate record after eating each day. The research nurses checked for the completeness of the data record. After knowing the quantity of calcium consumption, the result was informed back to each participant. The food composition information for each participant was analyzed by the INMUCAL-Nutrients program of the Institute of Nutrition, Mahidol University, Bangkok, Thailand.12,13 This INMUCAL-Nutrients program is an automatic program for calculating or transferring the weight of cooked food to raw food ingredients and according to the cooking method using cooking conversion factor.14
Sample Size and Statistical Analysis
When the prevalence of inadequate calcium consumption during pregnancy of 55% from the previous study10 with an acceptable error of 5% and an alpha error of 5% was taken into account, at least 381 participants were required for each region. The descriptive statistics were used to describe demographic characteristics, presented as mean, standard error (SE) or 95% confidence interval (CI), median, and range for describing continuous data. Frequency and percentage were used to describe categorical data. Linear regression analysis was used to assess the association between demographic factors and the amount of calcium intake. All data processing was performed using Stata V15·0 Stata Corp LLC 4905 Lakeway Drive College Station, Texas 77,845–4512 USA. The p-value of less than 0.05 was considered statistically significant.
Results
There were 1549 participants recruited for this study; 404, 404, 415, and 326 participants from central, northern, northeastern, and southern regions, respectively (Figure 1). The main characteristics of all participants are revealed in Table 1. The mean age was 29 ± 5.7 years. Most participants were primigravida (48.6%). The average gestational age was 20.6 ± 8.8 weeks. The mean prepregnant BMI was 21.8± 3.3 kg/m2. The median income was 18,000 (1000–250,000) Baht* [$562.5 (31.0–7812.5)]* (one Dollar = 32.0 Baht). About half of the participants’ educational level was a Bachelor’s degree (53.1%). Participants from the four regions were quite comparable in maternal age, gestational age, gravidity, prepregnant BMI, education level, and income. Table 2 demonstrates the mean calcium consumption across the country was 602.4 mg/day (95% CI 589.2–615.6 mg/day). Pregnant women in the northern region had the highest calcium consumption/day at 625.1 mg/day (95% CI 600.0–650.2 mg/day), while the central region had the second-highest calcium consumption/day at 621.2 mg/day (95% CI 593.9–648.5 mg/day). The calcium consumption/day in the northeastern region was 602.1 mg/day (95% CI 576.6–627.6 mg/day). While the pregnant women in the southern region had the lowest calcium consumption/day (551.3 mg/day; 95% CI 524.3–578.3 mg/day) (Table 2). The prevalence of total calcium consumption less than 500 mg/day, less than 800 mg/day, and less than 1000 mg/day was 37.7%, 82.0%, and 93.4%, respectively. The average calorie intake was 1448.8 kcal/day (95% CI 1429.4–1468.2 kcal/day) (Table 2).
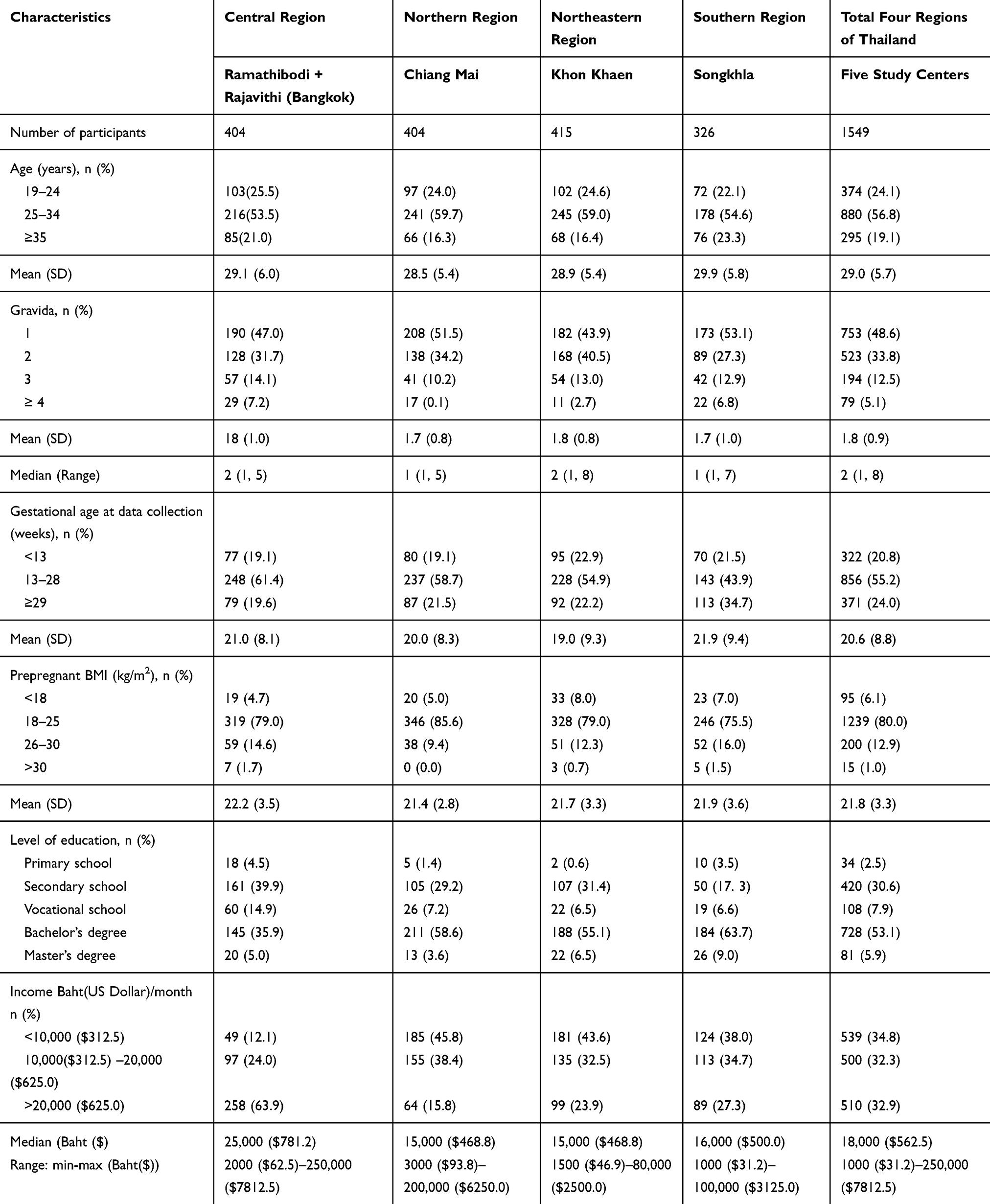 |
Table 1 Demographic Profile |
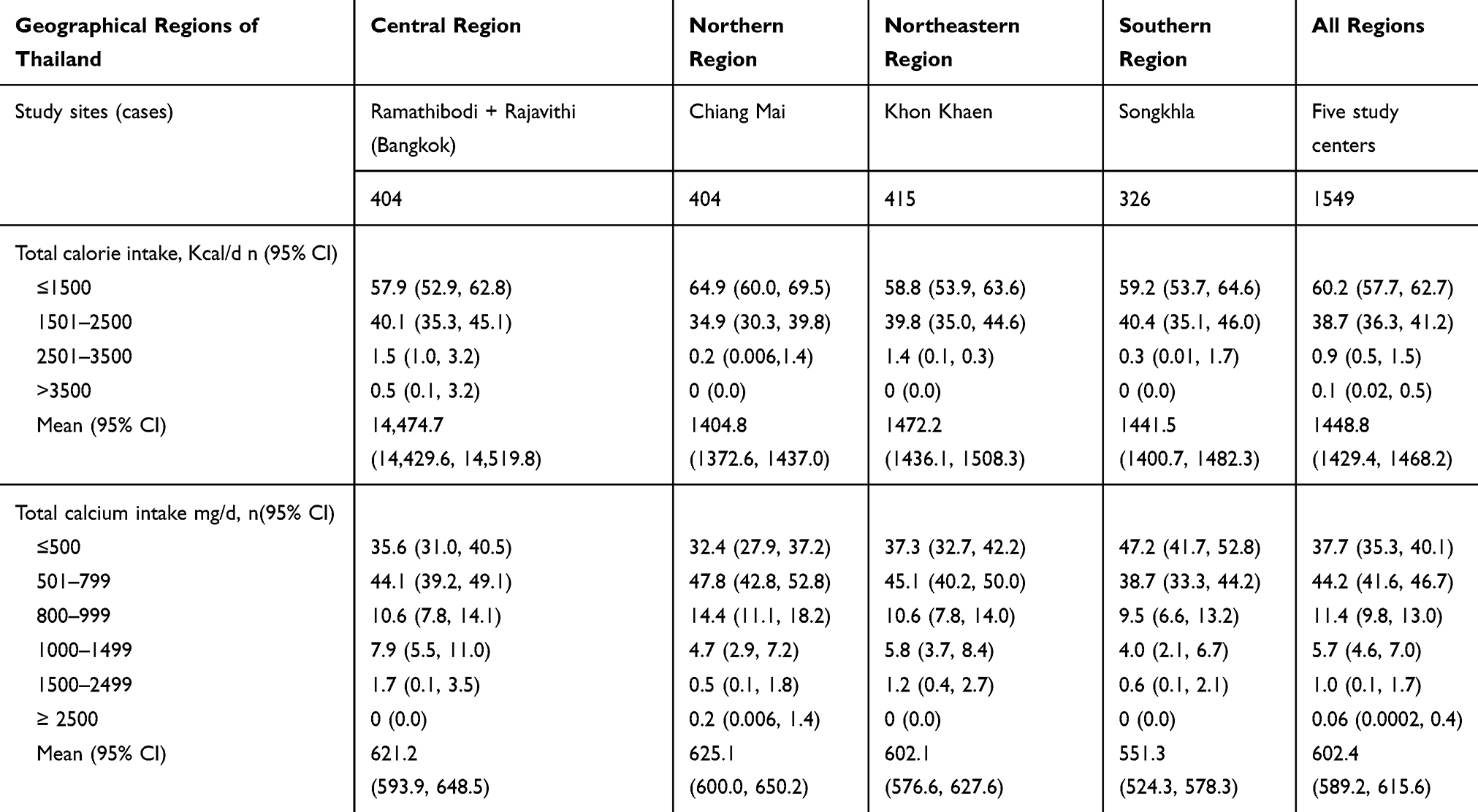 |
Table 2 Regional Total Calorie and Calcium Intake Distribution Across the Country |
 |
Figure 1 Flow diagram of study participants. |
The association between daily calcium consumption and maternal age, gestational age (GA), prepregnant BMI, educational levels, calorie intake, income are demonstrated in Table 3. In the 2nd trimester and 3rd trimester, pregnant women had calcium consumption higher than those in the 1st trimester, 61.4 and 66.2 mg/day, respectively. Participants with pre-pregnant BMI between 26–30 kg/m2 and >30 kg/m2 had mean calcium consumption less than participants with pre-pregnant BMI less than 18 kg/m2 85 and 110.4 mg/day, respectively. Participants with a calorie intake of more than 1500 Kcal/day had significantly higher calcium consumption than those with calorie intake ≤1500 kcal/day. There was no significant difference in calcium consumption across all levels of participants’ income. Interestingly, when milk or soybean consumption units/day in term of bottles/boxes/glasses taken into account, the incidences of no consumption, one-unit/day consumption, and more-than-one unit/day consumption were detected 85%, 14%, and 1%, respectively, in low calcium consumption (<800 mg/day) group. Regarding adequate calcium consumption (≥800 mg/day) group, there were the incidences of 5%, 60%, 35% of no consumption, one-unit/day consumption, and more-than-one unit/day consumption, respectively.
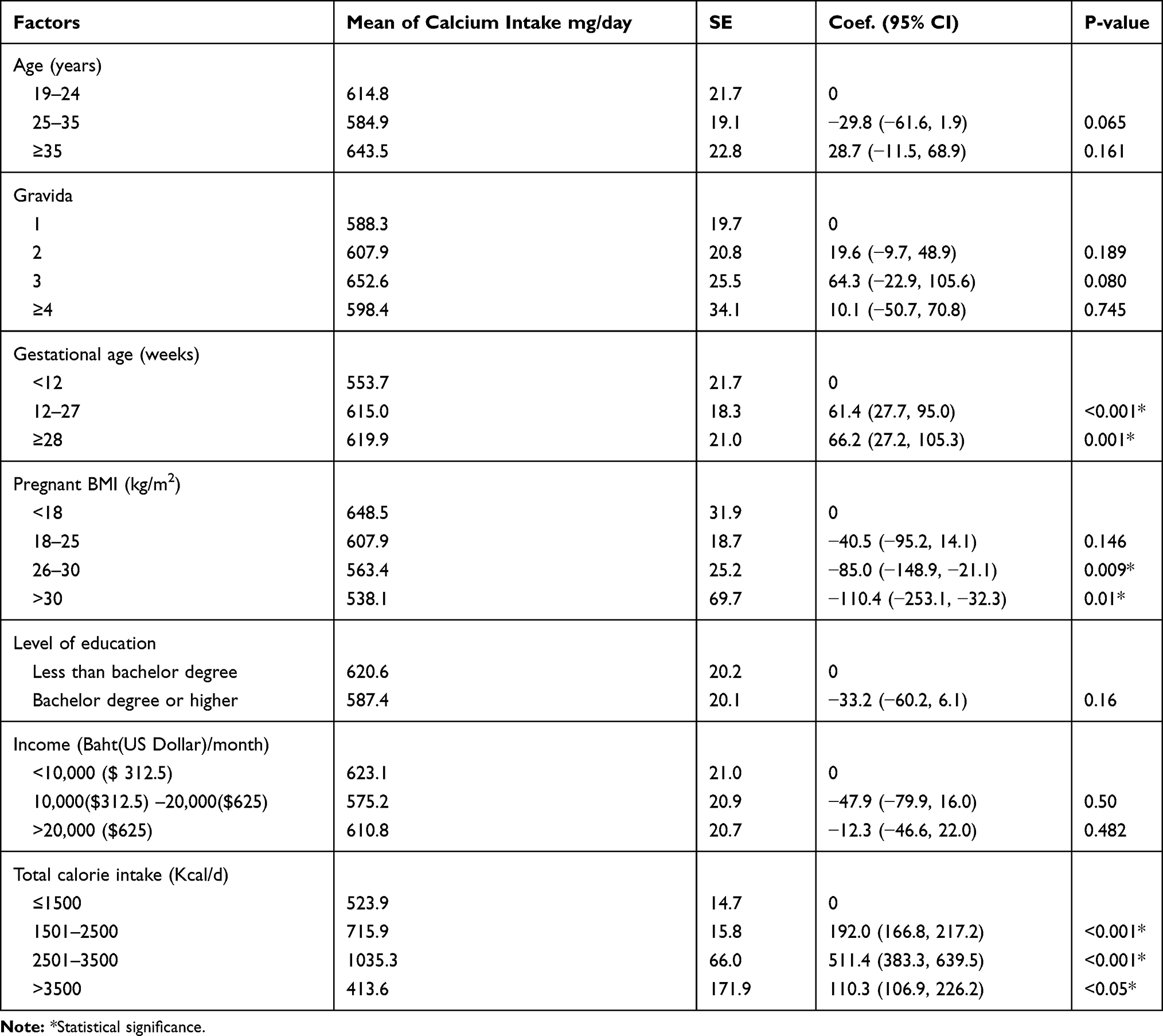 |
Table 3 Association Between Calcium Intake and Some Maternal Characteristics |
Discussion
Our data from all regions across Thailand elucidated the high prevalence of low calcium consumption. It is the level that calcium supplements should be beneficial in reducing the risk of preeclampsia.
The result from Songklanagarind Hospital, Prince of Songkla University in the southern part of Thailand, showed the lowest calcium consumption. The previous study in the deep south of Thailand also revealed the low calcium consumption in pregnant women.10 On the contrary, our result from Srinagarind Hospital, Khon Kaen University in the northeastern part of Thailand revealed the inadequacy of calcium consumption, which had an opposite result from the previous study.11 This discrepancy result from this center might be due to the different methods used for assessing calcium consumption. According to the World Bank Classification of country income, the United Nations region, Thailand is one of the middle-income countries. The mean calcium consumption during pregnancy of low-and middle-income countries was 647.64 mg/day (95% CI 568.71–726.57 mg/day) while that of high-income countries was 948.28 mg/day (95% CI 872.10–1024.57 mg/day).6 Our data demonstrated that the daily calcium consumption of Thai pregnant women was 602.4 mg/day (95% CI 589.2–615.6 mg/day), which was lower than the mean calcium consumption of low-and middle-income countries around 7.51% and lower than the mean calcium consumption of high-income countries 57.42%. When comparing with calcium consumption of pregnant women in our middle-income neighboring countries such as Malaysia, Thailand had a lower amount of calcium consumption by 3.98%.15
Strength
This study was conducted in all major geographical regions of Thailand to assess the regional variation. The results from all regions were the same (low mean calcium consumption and high inadequate intake rates). These indicate the results’ robustness. Evaluating the calcium consumption by the 3-day dietary intake immediate records (2 weekdays and 1 holiday) is also our study strength. We used the guidance of food records monitored by well-trained research nurses to ensure an accurate result. Once obtaining dietary information, the data were analyzed by experienced nutritionists using INMUCAL-NV3·0 program from the nutritional Institute, Mahidol University, Thailand. This program is suitable for Thai-style food as it was developed by collecting nutritive database values of Thai food consumption and recipes and can be compared with Thai Dietary Reference Intake (DRI).14 This program provides the accurate evaluation of many sorts of nutrients, especially from regional Thai food and recipe and the user-friendly program, which is approved to be one of the standard programs in a multicenter study in Thailand.16
Limitation
The university and tertiary care hospital study centers mostly covered the well-developed areas of the country in this study. Therefore, the result might not represent the whole actual prevalence of low calcium consumption across the country. However, even the well- to -do group of pregnant women still have low calcium consumption. We suspect that the figure must be even worse for the general population. In the southern region, we could not recruit participants according to the target sample size because there were not enough women at the antenatal care clinic of the university hospital. Gestational age, prepregnant BMI, and calorie intake were the main maternal characteristics of calcium consumption inadequacy. Nausea & vomiting during early pregnancy and calorie intake restriction in pregnancy with obesity influenced calcium consumption during gestation. The further study should focus on the amount of vitamin D consumption, parathyroid hormone, and the 1.25 – hydroxy vitamin D levels in the low calcium consumption mothers and the incidence of preeclampsia after calcium supplementation across the country.
These research findings strongly encourage not only pregnant women and medical personnel but also the national policymakers to realize the dietary low calcium consumption situation in Thailand. Our study demonstrated a high prevalence of low calcium consumption among all income levels. A recent systematic review and meta-analysis also indicated the high prevalence of low-calcium consumption in pregnancy in LMICs and HICs. Regarding the mean calcium consumption/day in LMICs (600 mg/day), the increase in calcium consumption around 400–500 mg/day might help to attain values close to current calcium consumption recommendations for pregnancy. There are three broad approaches to improve dietary intake: one is behavioral interventions that, although ideal, rely on personal habits and ability; the second is a supplementation that targets individuals; and the third is a fortification, which aims to improve the dietary intake of the whole population.17
Lifestyle interventions during antenatal care improve gestational weight, calorie, mineral, vitamins, trace elements, and calcium consumption, especially in middle- and low-income countries.18,19 According to our study, at least one unit/day of milk/soybean consumption should be encouraged in pregnancy to meet the adequate calcium requirement. The pregnant women’s attitude should also be the critical factor that can be adjusted to realize the importance of calcium consumption during pregnancy and the source of calcium in food. Therefore, health literacy about adequate perinatal nutrition, especially calcium, is very important for good antenatal care. The healthcare team should emphasize and embed this knowledge into daily practice. A pragmatic approach to dietary calcium management needs to be considered and implemented among the middle-income countries in Southeast Asia.
In conclusion, the mean calcium consumption among pregnant women in Thailand, which is considered one of the middle-income countries in Southeast Asia, was 602.4 mg/day (95% CI 589.2–615.6 mg/day). According to Thai dietary reference intake in pregnancy and the international recommendation, the prevalence of inadequate calcium consumption of Thai pregnant women was 82.0% and 93.4%.
Author contributions: All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Data Sharing Statement
All the data are held at Ramathibodi University Hospital, Mahidol University. The data sharing can be allowed by contacting the coordinating author with the relevant ethics committee approval.
Acknowledgments
We sincerely thank all the participants and staffs from all study sites. We should also owe Professor Pisake Lumbiganon for his encouragement and advice with an outstanding debt of gratitude. Sincere thanks also go to Thailand Research Fund (Distinguished Research Professor Award) for financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Guideline: Calcium Supplementation in Pregnancy Women. 2013:1–30
2. Zeni SN, Oretela SCR, Lazzari A, et al. Interrelationship between bone turnover markers and dietary calcium intake in pregnant women: a longitudinal study. Bone. 2003;33(4):606–613. doi:10.1016/S8756-3282(03)00203-5
3. WHO. Recommendations on Antenatal Care for a Positive Pregnancy Experience. Luxembourg: WHO Press; 2016:152.
4. Hofmeyr GJ, Lawrie TA, Atallah AN, Torloni MR. Calcium Supplementation During Pregnancy for Preventing Hypertensive Disorders and Related Problems (Review). 2018:1–121.
5. Omotayo MO, Dickin KL, O’Brien KO, Neufeld LM, De Regil LM, Stoltzfus RJ. Calcium supplementation to prevent preeclampsia: translating guidelines into practice in low-income countries. Adv Nutr. 2016;7(2):275–278. doi:10.3945/an.115.010736
6. Cormick G, Betrán AP, Romero IB. Global inequities in dietary calcium intake during pregnancy: a systematic review and meta-analysis. BJOG. 2019;126(4):444–456. doi:10.1111/1471-0528.15512
7. Repke JT, Villar J, Anderson C, Pareja G, Dubin N, Belizan JM. Biochemical changes associated with blood pressure reduction induced by calcium supplementation during pregnancy. Am J Obstet Gynecol. 1989;160(3):684–690. doi:10.1016/S0002-9378(89)80059-6
8. Ministry of Public Health. Public Health Statistics A.D.2018. Bangkok, Thailand;2018:142.
9. Abalos E, Cuesta C, Carroli G. Preeclampsia, eclampsia and adverse maternal and perinatal outcomes: a secondary analysis of the World Health Organization multicountry survey on maternal and newborn health. BJOG. 2014;121:14–24. doi:10.1111/1471-0528.12629
10. Sukchan P, Liabsuetrakul T, Chongsuvivatwong V, Songwathana P, Sornsrivichai V, Kuning M. Inadequacy of nutrients intake among pregnant women in the deep south of Thailand. BMC Public Health. 2010;10(572):1–8. doi:10.1186/1471-2458-10-572
11. Chotboon C, Soontrapa S, Buppasiri P, Muktabhant B, Kongwattanakul Kiattisak TJ, Thinkhamrop J. Adequacy of calcium intake during pregnancy in a tertiary care center. Int J Women’s Health. 2018;10:523–527. doi:10.2147/IJWH.S167980
12. INMUCAL. Nutrient calculation software institute of nutrition. Mahidol University. Available from: http://www.inmu.mahidol.ac.th/inmucal/.
13. Institute of Nutrition, Mahidol University. Nutrient Calcula- Tion Computer Software INMUCAL-Nutrients V.3 Database NB.2 Nakornpathom. 2013.
14. Ponprachanuvut P, Keeratichamroen A, Chammari K, Srisangwan N. Manual of INMUCAL-Nutrients V.4.0. Salaya. Nakhon Pathom: Institute of Nutrition, Mahidol University; 2019:154.
15. Loy SL, Marhazilina M, Nor Azwany Y, Hamid JJM. Development validity and reproducibility of a food frequency questionnaire in pregnancy for the Universiti Sains Malaysia birth cohort study. Malays J Nutr. 2011;17(1):1–18.
16. Schaafsma A, Deurenberg P, Calame W, et al. Design of the South East Asian nutrition survey (SEANUTS): a four-country multistage cluster design study. Br J Nutr. 2013;110(S3):S2–S10. doi:10.1017/S0007114513002067
17. WHO. E-Library of Evidence for Nutrition Actions (Elena). Department of Nutrition for Health and Development (NHD); 2011.
18. Aci O, Rathfisch G, García-Miranda R, Moreno-Altamirano L, Solís-Hernández R, Molina-Salazar R. Effect of lifestyle interventions of pregnant women on their dietary habits. lifestyle behaviors and weight gain: a randomized controlled trial. JHPN. 2016;35(7):1–9. doi:10.1186/s41043-015-0038-5
19. Ghosh-Jeruath S, Devasenapathy N, Singh A, Shankar A, Zodpey S. Ante natal care (ANC) utilization, dietary practices and nutritional outcomes in pregnant an recently delivered women in urban sums of Delhi, India: exploratory cross-sectional study. Reprod Health. 2015;12(20):1–11. doi:10.1186/1742-4755-12-1
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.