Back to Journals » Advances in Medical Education and Practice » Volume 17
Building Professional Competence in Autism Care: Results From a Pilot Continuing Education Program in Kazakhstan
Authors Sarbassova Z, Seyduanova L, Yelzhanova Z, Kosherbayeva L, Zhylkybayev G ![]() , Akhmetzhanova Z, Kurmanalina S, Kozhageldiyeva L
, Akhmetzhanova Z, Kurmanalina S, Kozhageldiyeva L
Received 23 February 2026
Accepted for publication 1 May 2026
Published 10 June 2026 Volume 2026:17 602638
DOI https://doi.org/10.2147/AMEP.S602638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Zhanna Sarbassova,1 Laura Seyduanova,2 Zulfiya Yelzhanova,3 Lyazzat Kosherbayeva,2,4 Galymzhan Zhylkybayev,5 Zulfiya Akhmetzhanova,5 Sandugash Kurmanalina,2 Laura Kozhageldiyeva6
1Pediatrician School, Kazakh-Russian Medical University, Almaty, Kazakhstan; 2Health Policy and Management department, Asfendiyarov Kazakh National Medical University, Almaty, Kazakhstan; 3Department of Dentistry, Kazakh-Russian Medical University, Almaty, Kazakhstan; 4Health Policy and Organization department, Al-Farabi Kazakh National University, Almaty, Kazakhstan; 5Psychoneurological Department №6 “kamkor”, National Center for Children’s Rehabilitation, Astana, Kazakhstan; 6School of Medicine, Nazarbayev University, Astana, Kazakhstan
Correspondence: Laura Seyduanova, Asfendiyarov Kazakh National Medical University, 94 Tole Bi Street, Almaty, 050000, Kazakhstan, Email [email protected] Sandugash Kurmanalina, Health policy and management department, Asfendiyarov Kazakh National Medical University, Almaty, Kazakhstan, Email [email protected]
Background: Children with autism spectrum disorders (ASD) require coordinated, multidisciplinary care, yet professional training for healthcare providers in Kazakhstan remains limited. We aimed to develop, pilot, and evaluate a continuing education program to enhance knowledge and skills in ASD detection, management, rehabilitation, and family support.
Methods: A multidisciplinary team, including public health specialists, neurologists-rehabilitologists, a general practitioner, a psychologist, and parents of children with ASD, designed the program based on a review of national and international continuing education curricula. The program was aligned with Kazakhstan’s postgraduate medical education framework and received ethical approval. Pilot training was conducted in Astana with 49 healthcare professionals across two cohorts. Participants’ knowledge and skills were assessed before and after training using structured questionnaires measuring diagnostic classification knowledge, understanding of ASD subtypes, multidisciplinary care roles, referral pathways, and family support competencies.
Results: The 60-hour program effectively improved participants’ knowledge and clinical understanding. Correct identification of ASD in ICD-10 increased from 87.8% to 92.7%, while correct identification in ICD-11 increased from 73.5% to 87.8%; uncertainty regarding ICD-11 classification decreased from 24.5% to 0%. Knowledge of ASD subtypes increased, and recognition of multidisciplinary care leadership rose from 28.6% to 46.3%. Participants also reported enhanced understanding of team roles, referral pathways, and tools for providing psychological support to families, facilitating more effective and timelier ASD care.
Conclusion: The pilot program demonstrates that structured, multidisciplinary training can significantly improve healthcare professionals’ knowledge and preparedness for managing children with ASD and supporting their families. This approach provides a scalable model for continuing professional development in Kazakhstan and similar settings.
Keywords: autism spectrum disorders, multidisciplinary teamwork, general practitioners, neurologist, nurse, education
Introduction
Autism spectrum disorders (ASD) represent a range of neuropsychological differences that are considered as psychomotor impairments. These disorders arise from early neurodevelopmental processes and affect personal, social, academic, and/or professional functioning.1 They are commonly associated with difficulties in acquiring, retaining, and applying specific skills or knowledge. Neurodevelopmental disorders may involve impairments in attention, memory, perception, speech, problem-solving abilities, or social interaction. ASD is increasingly understood as a multifactorial and heterogeneous condition with no single established etiology, arising from complex interactions among genetic susceptibility, environmental exposures, epigenetic mechanisms, and immunological factors that influence early brain development. Evidence suggests contributions from rare and common genetic variants, prenatal and perinatal risk factors, maternal infection and immune activation during pregnancy, neuroinflammatory processes, and other environmental exposures, although the relative contribution of these factors remains incompletely understood. This broader understanding reinforces the need for multidisciplinary approaches to diagnosis, management, and family support.
Globally, ASD affects an estimated 61.8 million individuals, with higher prevalence among boys and certain racial and ethnic groups, substantial lifelong disability burden, and increasing early identification in children over recent years.2,3 The prevalence of ASD among children increased from 14 to 59 per 100,000 children, whereas atypical autism increased six times between 2016 and 2022 in Kazakhstan. Similarly, the overall prevalence of neurodevelopmental disorders rose from 116.8 to 149.2 per 100,000 children in Kazakhstan.4
Prevention measures and health care services in Kazakhstan, medical and preventive are provided at the level of the primary health care (PHC) system. The PHC structured by governing the attached area into the catchment areas of 1800–2000 mixed population (children and adults). Regulatory the care in each catchment area is provided by a general practitioner (GP), pediatrician or internal medicine specialist and three nurses, as well as other specialists of multidisciplinary team such as a neurologist, ophthalmologist, endocrinologist, psychologist, and others. Thus, PHC is responsible for the primary prevention, management and rehabilitation of patients with various conditions, as well as for supporting family members through educational activities and psychological support. However, one of the main challenges faced by PHC system is a shortage of health professionals, particularly in rural areas, and the need for Continuous Professional Development (CPD) and training. Previous research has shown that families of children with ASD in Kazakhstan face significant financial, social, and medical care access challenges in obtaining adequate care and support for their children.5 Parental well-being was the highest in areas related to enjoyment in caring for the child and overall quality of life, while lower well-being was associated with the child’s disability diagnosis. The study also revealed insufficient knowledge among psychologists of PHC, emphasizing the need for specialized training to better support parents of children with ASD.6 Participants, including psychiatrists, pediatric neurologists, GPs, and other specialists demonstrated a range of beliefs about ASD, many of which reflected common misconceptions regarding its etiology and manifestation. These misconceptions were found to persist across medical disciplines and regions, indicating a widespread need for improved education and awareness among healthcare professionals.7
In Kazakhstan, postgraduate medical education is delivered through medical universities within the framework of CPD and aligned with Kazakhstan’s regulatory framework for postgraduate medical education, where 1 ECTS credit equals 30 academic hours.Training programs are credit-based, with a minimum duration of 60 hours (2 credits), while extended programs may include more credits depending on their objectives and scope. Given that our program was specifically designed for primary health care professionals and focused on strengthening multidisciplinary teamwork in ASD care, a 60-hour (2-credit) format was selected by expert consensus as appropriate to meet both national educational standards and the practical learning needs of the target audience.
The main purpose of the CPD on ASD was to pilot the designed program and strengthen the capacity of PHC medical specialists, particularly in multidisciplinary care. This program for was developed to demonstrate practical tools and methods through the entire care pathway – from PHC level to rehabilitation. The program included topics related to identifying the first signs of ASD, national and local care-pathways based on regulatory system in the country, family members psychological and social support. This study describes our approaches and experiences in piloting and implementing the program, presents the outcomes of the pilot initiative, and discusses the challenges encountered, with the aim of contributing to the future improvement of care programs for children with ASD and their families.
Methods
To achieve the major research goal, this study was conducted in three stages.
Stage 1. Program Development Process
At the initial stage, the team conducted a comprehensive review of existing CPD programs for health professionals, both in Kazakhstan and internationally. Available programs from medical universities and open sources were analyzed to identify best practices.
The CPD program for healthcare professionals on the management of children with ASD had a multidisciplinary approach including lead practicing pediatrician, 2 neurologists-rehabilitation specialists from National Center for Pediatric Rehabilitation of the Ministry of Health of the Republic of Kazakhstan, 1 psychologist and 2 public health specialists. To facilitate translation of knowledge into practice, the program included real case studies involving invited parents seeking consultation for their children.
Ethical Considerations: Ethical approval for the study was obtained from the Local Ethics Committee of Kazakh National Medical University (Protocol No. 13 (149), March 29, 2024).
Stage 2. Pilot Implementation
The pilot training was conducted in Astana, Kazakhstan, at two lead city polyclinics. Two healthworker cohorts participated: the first with 25 participants and the second with 24 participants, totaling 49 health professionals. Participants represented multidisciplinary teams involved in the rehabilitation of children with ASD, including GPs, neurologists, rehabilitation specialists, chief and general nurses, child development nurses, home-visit nurses, psychologists, and social workers.
As a practical part of the training, seven supervised clinical consultations were conducted with children: four diagnosed with ASD and three with suspected ASD. All consultations were performed with informed consent from parents or legally authorized caregivers.
Participants’ knowledge and skills were assessed using a structured study-specific paper-based questionnaire administered before and after training and collected by the researchers. As no standardized instrument fully aligned with the objectives of this pilot program was identified, the questionnaire was developed by the multidisciplinary study team based on program learning objectives and expert consensus. The questionnaire assessed the following domains: (1) knowledge of ASD diagnostic classification (ICD-10/ICD-11); (2) understanding of ASD subtypes and early signs; (3) knowledge of multidisciplinary roles and referral pathways; (4) competencies related to family psychological support; and (5) self-reported confidence in applying knowledge in practice. The questionnaire was developed specifically for this pilot study and was not a previously validated instrument.
Given the pilot nature of the study and small sample size, quantitative analyzes were limited to descriptive statistics. The absence of inferential testing is acknowledged as a study limitation.
Stage 3. Interview-Based Assessment of Program Effectiveness
Following the pilot training, semi-structured interviews were conducted with both program participants and developers (lecturers) to explore their perceptions of the program’s relevance, effectiveness, practical applicability and identify the facilitators and barriers to implement this CPD into practice. The interviews aimed to evaluate the effectiveness and relevance of the training program, identify areas for improvement, and assess future capacity-building training needs for PHC professionals. Total 15 respondents agreed to participate of which 8 were lecturers and 7 were participants of the CPD. The interviews focused on three key questions:
- To what extent were the expected learning outcomes of the program achieved?
- Which aspects of the program could benefit from refinement or further development?
- What knowledge, skills, or competencies are needed from PHC professionals to enhance the management and support of children with ASD and their families?
Interviews were audio-recorded, transcribed verbatim, and analyzed using thematic analysis. Initial coding was conducted independently by SK and LK using a deductive approach, combining codes informed by the interview guide with emergent themes arising from the data. Codes were reviewed, refined, and grouped into broader themes through iterative discussion. Dedoose software (version 8.3.45) was used to support data organization, coding, and theme development.
Results
Program Structure and Content
The pilot program consisted of 2 ECTS credits (60 hours), including 4 hours of lectures, 26 hours of practical training, and 30 hours of self-study. The goal of the program was to strengthen and systematize advanced knowledge and skills in the diagnosis, management, and rehabilitation of children with ASD.
Program outcome included enabling participants to:
● Acquire knowledge of ASD management at outpatient and other levels of healthcare;
● Understand key legal and regulatory documents governing care for children in Kazakhstan;
● Apply modern methods for early diagnosis and screening of ASD;
● Provide psychological support to parents and caregivers;
● Identify developmental risks and develop individualized care pathways;
● Monitor child progress and adjust individual care plans;
● Correctly document medical and rehabilitation measures in compliance with national standards;
● Evaluate the effectiveness of interventions and make evidence-based adjustments;
● Effectively collaborate with parents and legal guardians, ensuring a partnership approach.
● The content of the program presented in Table 1.
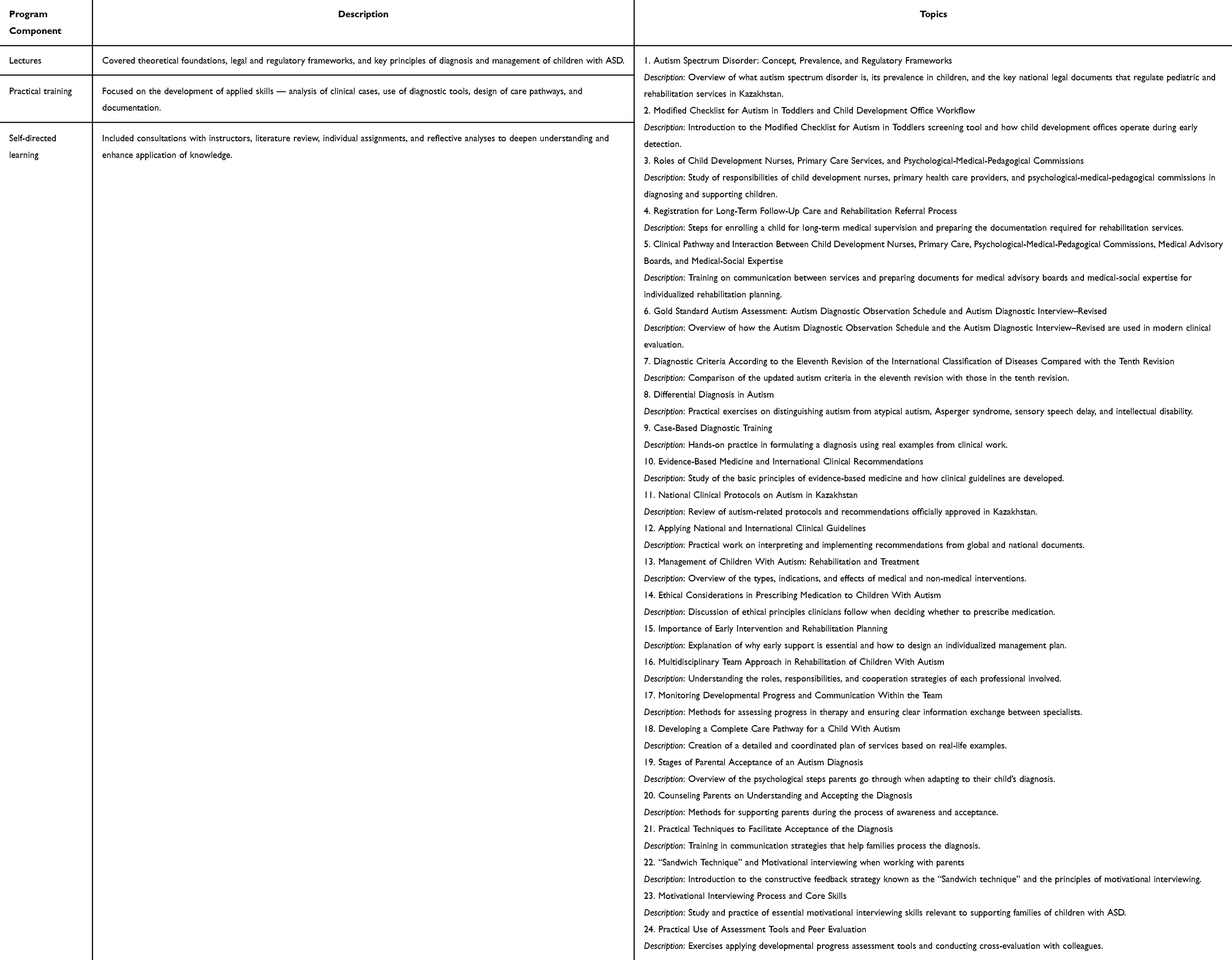 |
Table 1 Structure and Content of the Training Program |
Pilot Training Outcomes
A total of 49 participants before and 41 after training completed the questionnaire. Most had 6–10 years (36.7% and 36.6%) or over 10 years (34.7% and 39.0%) of professional experience, indicating that the majority were experienced healthcare providers.
Before the program, 87.8% of respondents correctly identified that ASD is classified in ICD-10 as “Mental and behavioral disorders (code F)”; this figure increased to 92.7% after training. Awareness of ICD-11 classifications was also improved: 73.5% initially selected the correct category “Mental, behavioral or neurodevelopmental disorders (code 06)”, compared with 87.8% post-training. The proportion of participants unsure about this topic decreased from 24.5% to 0%. Knowledge of ASD subtypes under ICD-11 increased after training. The proportion of participants selecting “all of the above” as correct rose from 42.9% to 46.3%, while the number of those unfamiliar with the classification decreased sharply from 26.5% to 2.4%.
Referral Pathways and Clinical Understanding
When asked which specialist should first assess a child with suspected ASD, most respondents selected a psychiatrist (53.1%) or neurologist (38.8%) before the course, and 46.3% and 41.5% respectively afterward. New responses appeared after the training — referral to a pediatrician (2.4%), speech therapist (2.4%), and psychologist (7.3%) — indicating an expanded understanding of multidisciplinary involvement in the diagnostic process.
Understanding of the multidisciplinary model of care improved notably. Before the training, only 28.6% of respondents recognized that children with ASD should be managed by a multidisciplinary team led by a GP or pediatrician; after training, this rose to 46.3%. Moreover, 61.2% (before) and 56.1% (after) correctly identified the key members of the care team — GP, nurse, neurologist, psychologist, and psychiatrist (Table 2).
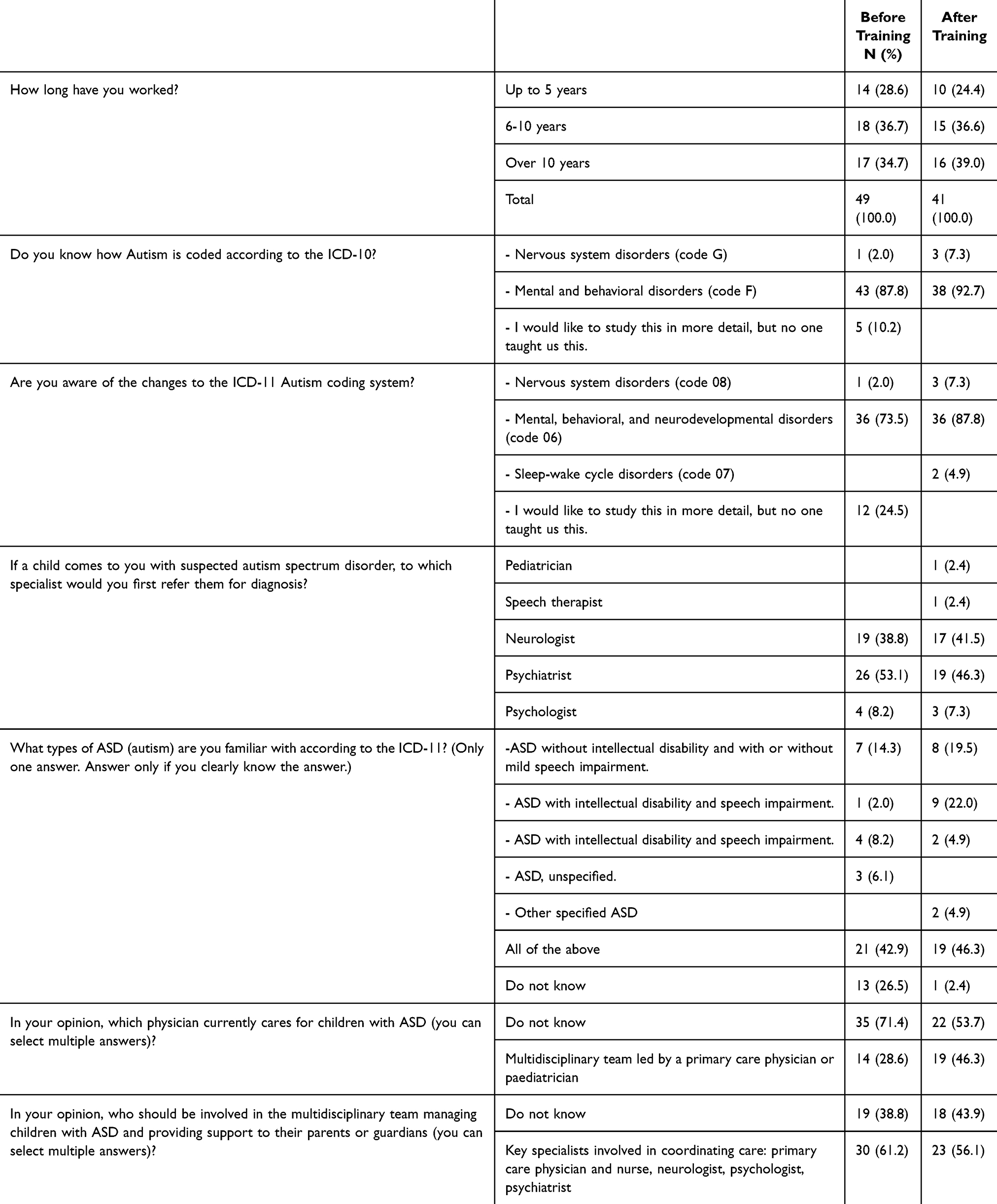 |
Table 2 Pre- and Post-Training Survey Results of Healthcare Professionals on ASD Management |
Participants reported that the program helped them understand better the roles of team members and the steps caregivers should follow to access timely medical and prevention care. The program included information on national rehabilitation care services and clinical protocols, as well as tools for psychological support for families, facilitating faster diagnosis acceptance and collaboration with specialists.
Interview Findings
1. To what extent were the expected learning outcomes of the program achieved?
Lecturers noted that while certain outcomes were achieved, some areas required further strengthening, particularly regarding the role of the multidisciplinary team. Pre- and post-training assessments indicated that overall expectations were not fully met. Lecturers highlighted that in many PHC settings, qualified specialists are not always available—for example, «the absence of a psychologist in PHC can disrupt the support pathway for individuals with ASD». One lecturer emphasized the importance of including «case scenarios addressing the absence of certain specialists in PHC and strategies to maintain continuity of care».
Participants reported that they gained in-depth understanding, especially regarding the care algorithm and its accompanying regulatory guidance.
2. Which aspects of the program could benefit from refinement or further development?
Lecturers suggested including more case studies focused on multidisciplinary care, although the program as a whole was considered feasible. Participants highlighted that, due to the shortage of clinical psychologists in PHC, additional training for nurses in providing psychological support to caregivers may be necessary—for instance, guidance on communicating a diagnosis, understanding caregiver responses, and strategies to motivate parents or guardians to engage collaboratively in care.
- What knowledge, skills, or competencies are needed from PHC professionals to enhance the management and support of children with ASD and their families?
All interviewees emphasized the importance of strengthening the workforce and ensuring that PHC facilities are equipped with necessary resources. Capacity building, adequate staffing, and access to relevant tools were consistently mentioned as critical for improving care delivery and supporting families of children with ASD.
Discussion
The CPD in Kazakhstan is provided by only accredited medical universities and the search of specific CPD courses focusing on primary care level ASD management showed the absence of such a training. Consequently, our major aim was to pilot the developed program and receive the feedback from the users and providers. Overall, the pilot program demonstrated a positive impact on healthcare professionals’ knowledge and awareness regarding the classification, diagnosis, and management of children with ASD. A notable increase in the proportion of respondents correctly identifying ASD types according to ICD-11 confirms the effectiveness of educational activities designed to familiarize specialists with the new classification structure. Similarly, a decrease in the number of respondents who were unable to answer indicates that the training not only improved knowledge but also strengthened confidence in professional competence. An increase in correct responses on questions related to autism coding according to ICD-10 and ICD-11 shows that including targeted modules on international disease classifications effectively addresses identified knowledge gaps. This improvement in awareness is particularly important in the context of Kazakhstan’s transition to ICD-11, where autism is considered within a broader neurodevelopmental continuum.8 Feedback from participants also highlighted high satisfaction with practical exercises, case discussions, and the overall relevance of the program.
Changes in responses regarding the referral of children with suspected ASD reflect a gradual shift among specialists from a narrow, single-discipline approach toward a more comprehensive understanding of the roles of various professionals, including pediatricians, speech therapists, and psychologists. This indicates the development of a foundational multidisciplinary perspective on the diagnosis and management of children with ASD, in line with contemporary international approaches. These findings are broadly consistent with international studies demonstrating that multidisciplinary ASD training can improve provider knowledge, referral practices, and confidence, while also highlighting persistent implementation barriers related to workforce capacity and interdisciplinary coordination. Multidisciplinary teamwork plays a critical role in the care of children with ASD by integrating the expertise of various specialists to comprehensively assess functional deficits and develop individualized, multimodal intervention plans. Such collaboration ensures that medical, behavioral, and developmental needs are addressed systematically, improving the effectiveness of diagnosis, treatment, and family support.9–12 In our case changes in understanding the composition and role of the multidisciplinary team also suggest that specialists recognize the need for comprehensive interprofessional collaboration. Nevertheless, the continued presence of respondents who lack a clear understanding of team composition indicates that there remains a strong need for further development of practical skills and opportunities for experience sharing. This is likely related to the limited practical implementation of multidisciplinary ASD management models in the national healthcare system and insufficient experience in interagency collaboration.
All training participants most frequently identified the shortage of psychologists in PHC as a major barrier to providing a continuous care pathway for children with ASD. In Kazakhstan, clinical psychology began to be formally integrated into PHC in 2013, when psychologists were first included as staff positions within these services. However, in the absence of clinical psychologists, professionals from the educational sector were often involved to fill this gap. Clinical psychology remains a relatively new and developing field in Kazakhstan, making this issue particularly acute not only in large cities but especially in rural areas, where access to qualified specialists is limited. This is also reflected in the expressed interest of nurses to improve their knowledge and skills in providing psychological support to caregivers of children with ASD, particularly in areas such as communicating a diagnosis and motivating caregivers to engage collaboratively in the child’s care.
Eventually, the results of the pilot phase confirm the effectiveness of the professional development program, but emphasize the need to continue educational work aimed at strengthening knowledge, developing practical competencies, and establishing sustainable professional relationships between specialists from various fields involved in providing assistance to children with autism spectrum disorders and their families.
As a pilot study, this work did not include a comparison group or controlled design, limiting causal inference regarding the effectiveness of the training relative to existing programs or standard practice. Future studies should consider controlled comparative designs and more robust inferential statistical analyses.
Emerging technologies for early ASD detection, including digital screening tools, machine learning-assisted behavioral analysis, and biomarker-based approaches, may have future relevance for professional training. However, these technologies remain variably validated, resource-dependent, and not yet widely integrated into routine primary care practice, particularly in resource-constrained settings.
Strengths and Limitations
This study has several strengths. It provides a comprehensive evaluation of a multidisciplinary continuing education program for healthcare professionals managing children with ASD by integrating quantitative assessments with qualitative feedback. Participants demonstrated improved knowledge of ASD classification (ICD-10 and ICD-11), referral pathways, multidisciplinary care, and family-centered approaches. Practical exercises, case discussions, and supervised clinical consultations strengthened participants’ confidence and ability to apply skills in real-world PHC settings. Inclusion of parents in development program provided valuable perspectives and helped ensure that the program addressed family needs and care coordination.
Several limitations should be acknowledged. The pilot was conducted in urban PHC settings, which may limit generalizability to rural areas where workforce shortages and resource constraints are more pronounced. The sample size was relatively small, and data saturation in qualitative interviews was not fully achieved. Some expected learning outcomes, particularly related to practical implementation of multidisciplinary care, were not fully achieved. In addition, shortages of clinical psychologists in PHC and limited prior experience with multidisciplinary models may have constrained the effectiveness of certain program components. As a pilot study, this work did not include a randomized or comparative control group, limiting conclusions regarding effectiveness relative to existing training approaches. Furthermore, quantitative analyzes were limited to descriptive methods, and more robust inferential statistical analyzes were beyond the scope of this pilot.
Future research should include controlled comparative designs, larger-scale implementation studies, and more robust statistical evaluation. Future program development should also consider expansion to rural and regional PHC centers through innovative delivery models, including telehealth-supported training, community-based outreach, and context-appropriate public health education strategies to address workforce and resource disparities. Additional assessment tools, including adaptive behavior scales (eg., Vineland) and cognitive or executive function assessments, may also strengthen participants’ competencies in comprehensive ASD evaluation.
Longitudinal follow-up studies are needed to evaluate the long-term impact of the training on clinical practice, as well as its potential influence on patient outcomes and family satisfaction. Additionally, national strategies to strengthen multidisciplinary collaboration and expand integration of clinical psychology within PHC should be further supported.
Conclusion
The pilot program enhanced healthcare professionals’ knowledge, skills, and confidence in managing children with ASD, particularly in classification, referral pathways, and multidisciplinary, family-centered care. Remaining challenges include limited staff availability, especially clinical psychologists, and resource disparities in rural PHC. Future implications include scaling the program to underserved regions, integrating targeted psychological support training for PHC staff, and promoting multidisciplinary collaboration with the goal of supporting improved long-term outcomes for children with ASD and their families, although the current study assessed provider knowledge and preparedness rather than patient-level outcomes.
Data Sharing Statement
Materials and these articles are with the correspondence authors.
Ethical Approval
The study was approved by the Local Ethics Committee of Kazakh National Medical University, Kazakhstan (Protocol No. 13 (149), 29 March 2024). All study procedures were conducted in accordance with the ethical standards of the institutional research committee and with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to study commencement. Participants were fully informed about the study objectives, procedures, potential risks and benefits, confidentiality of data, and their right to withdraw from the study at any time without any consequences. Personal data were anonymized to ensure confidentiality and privacy protection.
Funding
There is no funding to report.
Disclosure
The authors declare they have no competing interests in this work.
References
1. Braconnier ML, Siper PM. Neuropsychological assessment in autism spectrum disorder. Curr Psychiatry Rep. 2021;23(10):63. doi:10.1007/s11920-021-01277-1
2. Santomauro DF, Erskine HE, Mantilla Herrera AM; Global Burden of Disease Study. Autism spectrum collaborators. The global epidemiology and health burden of the autism spectrum: findings from the Global Burden of Disease Study 2021. Lancet Psychiatry. 2025;12(2):111–10. doi:10.1016/S2215-0366(24)00363-8
3. Shaw KA, Williams S, Patrick ME, et al. Prevalence and early identification of autism spectrum disorder among children aged 4 and 8 years — autism and developmental disabilities monitoring network, 16 Sites, United States, 2022. MMWR Surveill Summ. 2025;74(2):1–22. doi:10.15585/mmwr.ss7402a1
4. Nukeshtayeva K, Bolatova Z, Galayeva A, Shintayeva N, Zhanalina G. Epidemiological trends in autism and other neurodevelopmental disorders in Kazakhstan (2016–2022): a regional and national perspective. Front Psychiatry. 2025;16:1520460. doi:10.3389/fpsyt.2025.1520460
5. Imamatdinova A, Samambayeva A, Akhtaeva N, et al. Autism spectrum disorders: experience of parents in Kazakhstan. BMC Public Health. 2025;25(1):2676. doi:10.1186/s12889-025-23764-3
6. Akhtayeva N, Kosherbayeva L, Imamatdinova A, Šmigelskas K. Wellbeing of parents raising children with autism spectrum disorder and the role of psychologists. Arch Med Sci. 2025;21(3):858–867. doi:10.5114/aoms/190772
7. Somerton M, Stolyarova V, Khanin S. Autism and the Knowledge and Beliefs of specialists in Kazakhstan. J Autism Dev Disord. 2022;52(3):1156–1168. doi:10.1007/s10803-021-05021-9
8. The international classification of diseases, 11th revision, was presented in the Kazakh language for the first time. News of the Ministry of Health in Kazakhstan. 2025. Available from: https://www.gov.kz/memleket/entities/dsm/press/news/details/938338?lang=ru.
9. Frye RE. A personalized multidisciplinary approach to evaluating and treating autism spectrum disorder. J Pers Med. 2022;12(3):464. doi:10.3390/jpm12030464
10. Penner M, Senman L, Andoni L, et al. Concordance of diagnosis of autism spectrum disorder made by pediatricians vs a multidisciplinary specialist team. JAMA Netw Open. 2023;6(1):e2252879. doi:10.1001/jamanetworkopen.2022.52879
11. Huber JF, Loh A, Monga S, Esufali J, Shouldice M. Development of a novel multi-disciplinary specialized care service for children and adolescents with autism spectrum disorder and/or intellectual/developmental disability in a tertiary children’s hospital setting. Children. 2022;10(1):57. doi:10.3390/children10010057
12. Alenezi S, Alkhiri A, Hassanin W, et al. Findings of a multidisciplinary assessment of children referred for possible neurodevelopmental disorders: insights from a retrospective chart review study. Behav Sci. 2022;12(12):509. doi:10.3390/bs12120509
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Disparate Digital Literacy Levels of Nursing Manager and Staff, Specifically in Nursing Informatics Competencies and Their Causes: A Cross-Sectional Study
Hariyati RTS, Handiyani H, Wildani AA, Afriani T, Nuraini T, Amiruddin MH
Journal of Healthcare Leadership 2024, 16:415-425
Published Date: 25 October 2024
Development and Effectiveness of a Central Venous Catheter Management Education Program for Nurses in Hematology-Oncology Wards
Park S, Kim J
Nursing: Research and Reviews 2026, 16:546043
Published Date: 5 February 2026