")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Budget Impact of Early Introduction of Amino Acid Formula in Managing Infants with Cow Milk Protein Allergy: Arabian Gulf Countries’ Experience
Authors Miqdady M, AlMutaeri S, Alsawi N, Goronfolah L, Tzivinikos C, Al Hameli H , Cremonesini D, Al-Enezi M, Hussain A, Al Damerdash Z, Al-Biltagi M
Received 18 September 2022
Accepted for publication 21 December 2022
Published 5 January 2023 Volume 2023:16 Pages 73—82
DOI https://doi.org/10.2147/JAA.S390352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Mohamad Miqdady,1,2 Saif AlMutaeri,3 Najwa Alsawi,4 Loie Goronfolah,5 Christos Tzivinikos,6 Hamad Al Hameli,7 David Cremonesini,8 Mohammed Al-Enezi,9 Ahmad Hussain,10 Zainab Al Damerdash,11 Mohammed Al-Biltagi12,13
1American Board of Pediatrics Gastroenterology, Hepatology & Nutrition, Chief Pediatric Gastroenterologist, Hepatology & Nutrition Division, Sheikh Khalifa Medical City, Abu Dhabi, United Arab Emirates; 2College of Medicine & Health Sciences, Khalifa University, Abu Dhabi, United Arab Emirates; 3King Faisal Specialist Hospital & Research Centre, Riyadh, Kingdom of Saudi Arabia; 4Sulaiman Al Habib Private Sector Hospital, Riyadh, Kingdom of Saudi Arabia; 5National Guard Jeddah Government Hospital, Jeddah, Kingdom of Saudi Arabia; 6Al Jalila Children’s Specialty Hospital, Dubai, United Arab Emirates; 7Cleveland Clinic, Abu Dhabi, United Arab Emirates; 8Al Ain Hospital, Al Ain, Abu Dhabi, United Arab Emirates; 9Dar Al-Shefa Hospital, Hawally, Kuwait; 10Amiri Hospital/Salam Hospital, Kuwait City, Kuwait; 11Amiri Hospital, Kuwait City, Kuwait; 12Faculty of Medicine, Tanta University, Tanta, Egypt; 13King Abdullah Medical City, Arabian Gulf University, Dr. Sulaiman Al Habib Medical Group, Manama, Kingdom of Bahrain
Correspondence: Mohammed Al-Biltagi, Faculty of Medicine, Tanta University, Tanta, Egypt, Tel +97339545472, Email [email protected]
Objective: This study estimates the budgetary impact of the introduction of amino-acid formula (AAF) as first-line management in the elimination diet of infants with suspected cow milk protein allergy (CMPA) in the Kingdom of Saudi Arabia (KSA), Kuwait, and the United Arab Emirates (UAE) from a health-care payer’s perspective.
Methods: A global decision tree model was adapted to compare estimated costs in current practice (extensively hydrolyzed formula [eHF] or soy formula [SF] with the proposed approach of early introduction of AAF as first-line treatment of CMPA in non-breast-fed infants). Model inputs were derived from explorative literature reviews and medical experts’ opinions. All costs were reported in local currency, ie, Saudi Riyal (SAR) for KSA, Kuwaiti Dinar (KWD) for Kuwait, and United Arab Emirates Dirham (AED) for the UAE.
Results: Cost savings with the early introduction of AAF were 10% (SAR 15102542) in KSA, 10% (KWD 306565) in Kuwait, 17% (AED 1842018) in the UAE government sector and 13% (AED 4232932) in the UAE private sector. The highest cost reduction was observed in the cost of soy formula (SF), with a 58% reduction both in KSA (SAR 4204540) and UAE public sector (AED 110331). A significant cost reduction in medication costs in Kuwait (37%; KWD 5630) and medical examination costs in the UAE private sector (50%; AED 1508918) was observed.
Conclusion: Results indicated that the introduction of AAF as the first line in the management of CMPA is a cost-saving strategy for the Gulf Cooperation Council (GCC) countries—KSA, Kuwait, and UAE— from a health-care payer’s perspective.
Keywords: cow’s milk protein allergy, amino acid formula, infants, Kingdom of Saudi Arabia, Kuwait, United Arab Emirates, Arabian Gulf
Plain Language Summary
- Early introduction of AAF (Neocate®) for CMPA management can effectively reduce the symptomatic period for infants suspected of CMPA.
- The early introduction of AAF is cost-saving from the health-care payer’s perspective for the Kingdom of Saudi Arabia, Kuwait, and the United Arab Emirates.
Introduction
Food allergy has emerged as a significant public health concern among infants and children with its recent rise in prevalence.1 Cow’s milk protein allergy (CMPA) is the most prevalent food allergy in young children and often the first to develop among infants.2 CMPA occurs due to an immunological reaction to cow’s milk proteins affecting several body organs; the most common manifestations include atopic skin diseases, respiratory involvement, allergic rhinitis, or gastrointestinal reactions.3–5 The immunoglobulin (Ig) E mediated form can cause severe systemic allergic reactions and may lead to anaphylaxis and be a life-threatening condition.6 Diverse dietary habits and variation in diagnostic criteria across the globe result in a varying range of prevalence of CMPA from 2% to 7.5%.7
The diagnostic approach to CMPA includes the evaluation of the medical history of the patient, focusing on atopic manifestations and family history of allergies, and a subsequent physical examination.2 Skin prick and patch tests are the standard diagnostic tools for CMPA.8 A radioallergosorbent test (RAST) is conducted to confirm the presence of IgE antibodies in patients with type-I allergic reactions. However, these tests are unreliable and have a potential risk of misclassifying patients with CMPA.8 Moreover, it has no value in confirming the diagnosis of non-IgE mediated CMPA. The signs and symptoms of non-IgE-mediated CMPA can mimic other conditions common in infants, such as infantile colic, gastroesophageal reflux, lactose intolerance, infantile eczema, etc. The diagnosis of CMPA is typically confirmed through an oral food challenge (OFC) by establishing a causal relationship between the symptoms and the allergen.2,7,9
Consequently, the dietary elimination of cow’s milk protein is the key precept in diagnosing and treating CMPA.2,7,9 However, introducing an elimination diet in non-breast-fed infants without adequate substitutions fosters potential nutritional deficiencies.10,11 Hence, a substitute formula is needed in non-breast-fed infants <24 months of age. Available substitute formulas include extensively hydrolyzed formula (eHF), soy formula (SF), and amino acid formula (AAF).2,7 Alternative animal milk as a substitute formula is unacceptable because of potential cross reactivity.12 Therefore, an infant formula with an appropriate composition is recommended to achieve nutritional adequacy. eHF has demonstrated high efficacy and tolerance in infants with CMPA and is recommended as the first treatment choice by most scientific societies.13 According to the latest ESPGHAN committee practical guidelines, AAF use is recommended if the infant does not show symptomatic improvement within two to four weeks of eHF, considering that the infant might be allergic to eHF peptides.9 Soy-based formulae have few limitations; they can be used for full-term infants older than six months only, as soy contains isoflavones and phytoestrogens that are unsuitable for infants below six months or pre-term infants.14 There is a potential cross-reactivity between soy and CMP as The American Academy of Pediatrics statement established that 10–14% of infants with CMPA also had a soy protein allergy.15 In comparison, AAF contains constituent amino acids that are non-allergic and well tolerated in infants with CMPA, and the risk of allergy is almost non-existent. As per ESPGHAN guidelines, AAF is recommended as the primary option for infants with anaphylaxis (IgE mediated) and other life-threatening symptoms and in those who have failed to respond to eHF.7,9,16 In clinical practice, an alternative formula is recommended if the initial formula proves ineffective after two to four weeks of treatment.2,9,17 Hence, this practice makes the current approach of selecting appropriate formula time-consuming and may increase the symptomatic period for infants and initiate unnecessary investigations and medications.
Moreover, it may induce uncertainty about the accuracy of the diagnosis. This practice may also result in a significant economic impact on CMPA management. To date, only limited studies are available that focus on the financial aspect of appropriate substitute formula selection in non-breast-fed infants with CMPA in the region. The objective of the current study is to adapt the decision tree model to estimate the budgetary impact of using AAF (Neocate®) as first-line management for the treatment of non-breast-fed infants with suspected CMPA in Gulf Cooperation Council (GCC) countries, ie, the Kingdom of Saudi Arabia (KSA), Kuwait, and the United Arab Emirates (UAE) from the health-care payer’s perspective.
Methods
The adaptation of the decision tree model was performed from the health-care payer’s perspective for the three countries—KSA, Kuwait, and the UAE. All costs were reported in local currency, ie, Saudi Riyal (SAR) for KSA, Kuwaiti Dinar (KWD) for Kuwait, and United Arab Emirates Dirham (AED) for UAE.
Model Structure
A global decision tree model was adapted to evaluate the estimated costs of introducing AAF (Neocate®) as the primary elimination diet in three GCC countries—KSA, Kuwait, and the UAE— in infants under two age groups (0–6 months and 6–24 months). The estimated cost of infant formula in current practice with AAF use after lack of response or intolerance to eHF and SF was also assessed.2,9
In the current practice, open oral food challenge (OFC) is recommended after eight weeks for infants who show improvement in CMPA to confirm the diagnosis.18 The proposed practice suggests using AAF four weeks before an OFC test.
An explorative literature review was conducted to retrieve robust data on disease epidemiology and the characteristics of the CMPA population in KSA, Kuwait, and the UAE. The literature review also included an evaluation of local CMPA management and treatment pathways across the three countries and any variations from the global disease model. A questionnaire was developed to gather insights from a total of 18 key medical experts (including pediatricians, pediatric gastroenterologists, pediatric allergists, and dieticians) and payers in the region engaged in CMPA management. These inputs from key medical experts were utilized to narrow data gaps and validate data retrieved from literature prior to local adaptation of the model. A visual representation of the decision tree model as current practice and proposed practice is shown in Supplementary Figure 1A and Supplementary Figure 1B, respectively. The study was conducted per the Declaration of Helsinki’s ethical principles and good clinical practices.
Model Inputs
Population Inputs
The model population included non-breastfeeding infants (0–2 years) with suspected CMPA. The population statistics were obtained from local reports – General Authority for Statistics (GaStat), Saudi population 2018 data for KSA,19 Kuwait 2018 population statistics for Kuwait,20 and Dubai Statistics Center 2018 for the UAE.21 The eligible population was included in the study based on key medical experts’ inputs on the percentage of breastfed infants and CMPA prevalence (Supplementary Figure 2).
Cost Inputs
The analysis included cost inputs that were drug acquisition costs, drug administration costs, monitoring, and associated adverse event management costs. The costs were assumed to be borne for the duration while the infant was on substitution therapy. All costs were reported in Saudi Riyal (SAR) for KSA, Kuwaiti Dinar (KWD) for Kuwait, and UAE Dirham (AED) for the UAE.
Unit cost inputs for substitute formulas used for CMPA management, ie, SF, eHF, and AAF, were obtained from retail pharmacies’ prices for KSA and Kuwait. For the UAE government sector, the cost of eHF and AAF was based on inputs from key medical experts, while for the UAE private sector, the cost of eHF and AAF was obtained collectively from key medical experts’ opinions and the Dubai Health Authority (DHA) claims database. The cost of SF for the UAE governmental and private sectors was obtained from the literature. The weekly consumption of eHF and AAF for KSA, Kuwait, the UAE governmental sector, and the UAE private sector was calculated based on key medical experts’ opinions. At the same time, the weekly consumption of SF was derived as an average of eHF and AAF for KSA and the UAE government sector. SF was not used in Kuwait and the UAE private sector as per the key medical experts’ opinion (Supplementary Table 1).
The costs of other medications such as domperidone, ranitidine, hydroxyzine, topical hydrocortisone, simethicone, and probiotics used for CMPA management in non-breast-fed infants under age group <6 months and >6 months were obtained from the National Unified Procurement Company (NUPCO)22 and Saudi Food and Drug Authority (SFDA)23 for KSA, Kuwait Ministry of Health (MOH)24 for Kuwait, DHA25 and Abu Dhabi Health Services Company (SEHA)26 for the UAE Government sector and the UAE private sector model, respectively (Supplementary Tables 2 and 3). The administration and monitoring costs include the associated procedures and costs for medical staff such as doctors, nurses, dieticians, and allied health-care professionals. The procedure costs included in the analysis covered oral provocation test, RAST for cow’s milk, endoscopy, radiographic imaging, or other diagnostic tests (patch test, skin prick test, serological test). Other medical examination costs and allied health-care professional costs were also analyzed for all three GCC countries and are represented in Supplementary Table 4. The health-care utilization costs were obtained from the MOH list for KSA, while they were based on key medical experts’ opinions for Kuwait and the UAE government sector. For the UAE’s private sector, the health-care utilization costs were obtained collectively from key medical experts’ opinions and the DHA claims database.
Model Assumptions
The key model assumptions were: a) the eligible study population for infants under two years of age was calculated as an average of the population data for children (0–4 years) for all the three GCC countries; b) the price of Lactobacillus Reuteri (BioGaia) used as a probiotic supplement for infants was obtained from literature, as the prices were not available in NUPCO/SFDA/UAE MOH; and c) the weekly consumption of SF was derived as an average of eHF and AAF for KSA and the UAE government sector.
Statistical Methods
Univariate sensitivity analysis was performed to clarify the inherent uncertainty in the model parameters, by mostly varying each parameter at value of ± 25% while keeping other parameters constant. The single clinical and cost variables associated with the new diagnostic strategy (using the amino acid formula) were remodeled based on minimum and maximum estimated values.
Results
Budget Impact and Cost Breakdown
The early introduction of AAF in the management of non-breast-fed infants suspected with CMPA exhibited cost savings of 10% (SAR 15102542) in KSA, 10% (KWD 306565) in Kuwait, 17% (AED 1842018) in the UAE government sector and 13% (AED 4232932) in the UAE private sector. Table 1 shows the net budget impact of current and proposed practices for the three GCC countries—KSA, Kuwait, and the UAE. With the early introduction of AAF, the major cost reduction was attributed to the decrease in the cost of SF use, with a 58% reduction in KSA (SAR 4204540) and a 58% reduction in the UAE government sector (AED 110331). In Kuwait, the major cost reduction was attributed to medication costs with a 37% (KWD 5630) reduction in total costs, while in the UAE private sector, the major cost reduction was attributed to medical test costs with a 50% (AED 1508918) reduction in total costs. Table 2 shows the health-care utilization cost for KSA, Kuwait and the UAE (Government and Private sector).
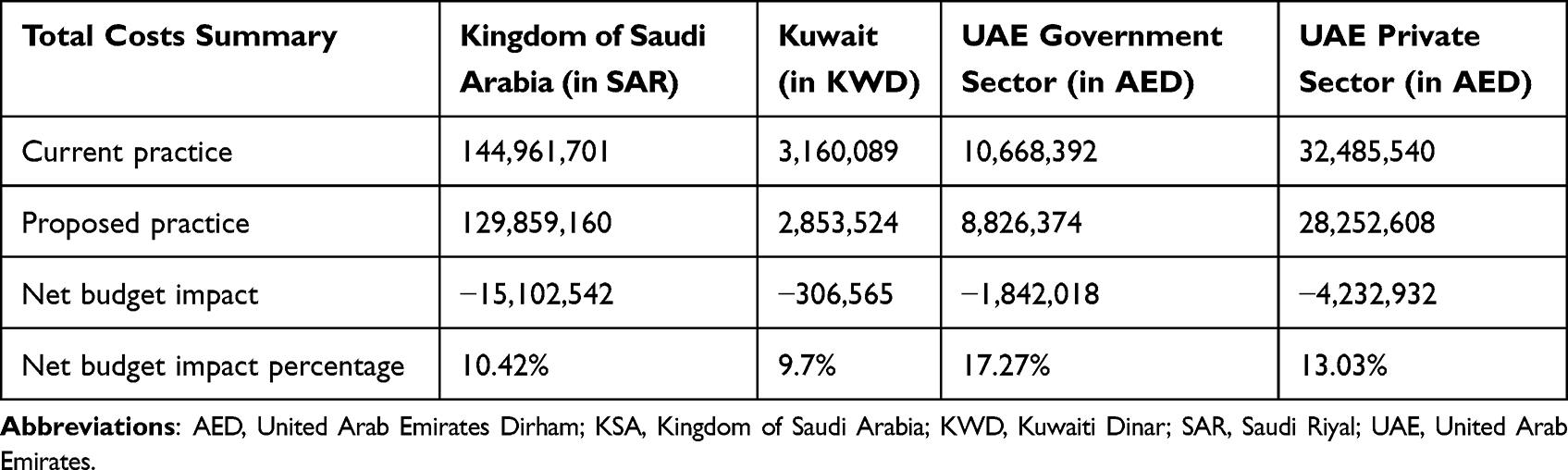 |
Table 1 Net Budget Impact in the Three GCC Countries – KSA, Kuwait and UAE |
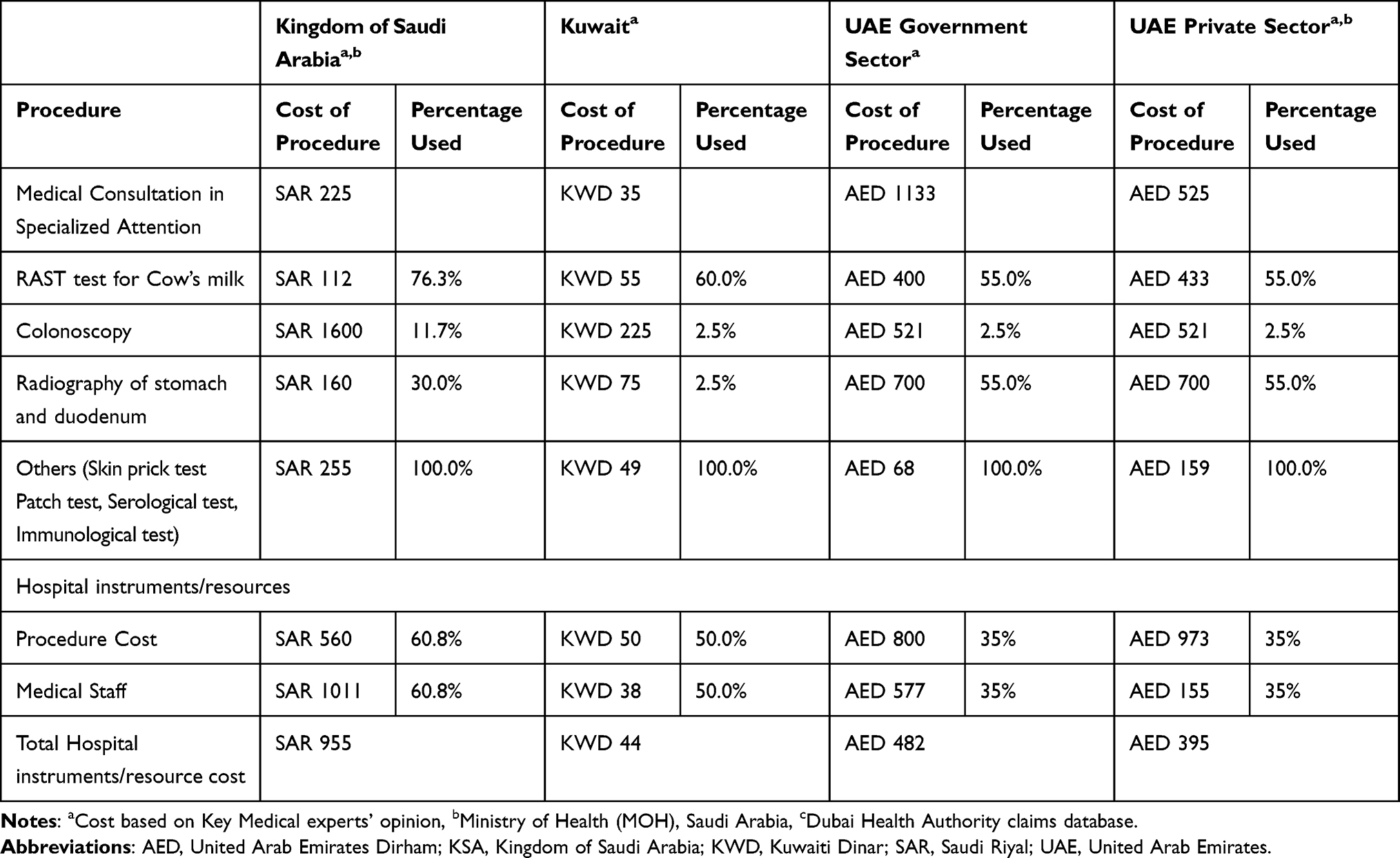 |
Table 2 Health-care Utilization Cost for KSA, Kuwait and the UAE (Government and Private Sector) |
Kingdom of Saudi Arabia
From the proposed practice, the early use of AAF in infants with suspected CMPA in the KSA showed a decrease of SAR 15102542 in the total budget from the KSA payer’s perspective, ie, a reduction of 10%. The significant cost-saving observed was attributed to a reduction in the cost of use of SF by 58% (SAR 4204540), followed by a 41% (SAR 3427266) reduction in medical examination costs and a 39% (SAR 956457) reduction in the cost of medications (Figure 1). In the proposed practice, the cost of the AAF formula increased by 57% (SAR 14086709).
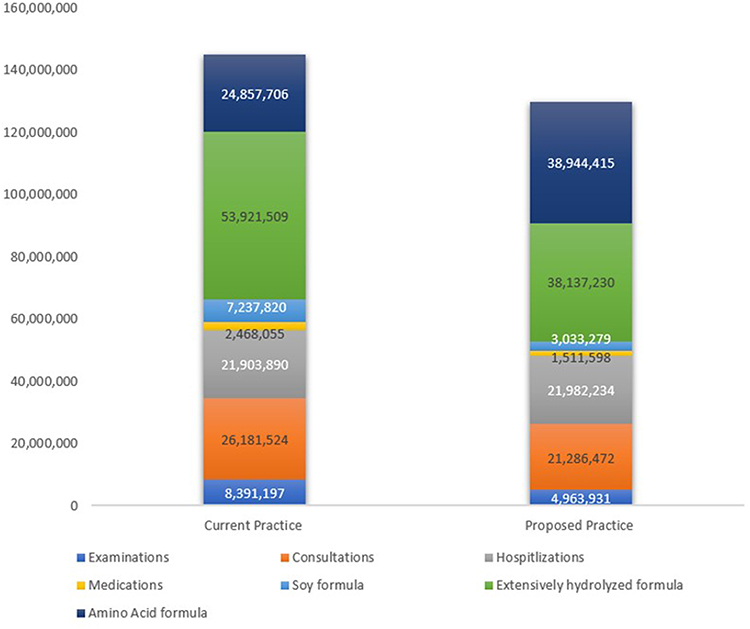 |
Figure 1 Cost breakdown of AAF use in current and proposed practice in KSA. Abbreviations: AAF, Amino Acid Formula; KSA, Kingdom of Saudi Arabia; SAR, Saudi Riyal. |
Kuwait
In Kuwait, the early use of AAF in the proposed practice in infants with suspected CMPA exhibited a reduction in the overall budget of KWD 306565, ie, about 10% from the Kuwait payer’s perspective. The significant cost-saving observed was attributed to a reduction in medication costs by 37% (KWD 5630), followed by a reduction in the cost of eHF by 28% (KWD 290583) and physician consultations by 19% (KWD 204644) (Figure 2). The significant cost offset in the proposed practice was due to an increase in the cost of AAF by 57% (KWD 222993).
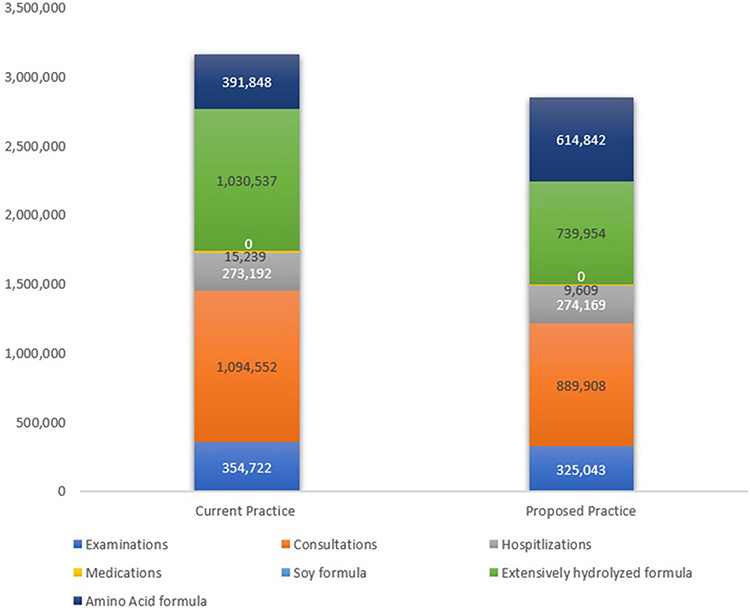 |
Figure 2 Cost breakdown of AAF use in current and proposed practice in Kuwait. Abbreviations: AAF, Amino acid formula; KWD, Kuwaiti Dinar. |
UAE Government Sector
From the proposed practice, the early use of AAF formula in infants with suspected CMPA in the UAE (government sector) resulted in a decrease of AED 1842018, ie, over 17% reduction in the total budget from the UAE payer’s perspective. The major cost-saving was attributed to a reduction in SF costs by 58% (AED 110331), with a similar reduction in medical examination costs by 58% (AED 307929) and a reduction of 37% (AED 4237) in the cost of the medications. The cost of AAF increased by 57% (AED 378741) in the proposed practice.
UAE Private Sector
From the UAE payer’s perspective, the early use of AAF in infants with suspected CMPA who were managed in the private sectors, in the proposed practice, showed a decrease of 13% (AED 4232932) in the total budget. The significant cost-saving observed was attributed to a reduction in medical examination costs by 50% (AED 1508918), followed by a reduction in the cost of medications by 35% (AED 72290) and the cost of eHF by 29% (AED 2027154).
The cost of AAF increased by 57% (AED 2331787) in the proposed practice. Figure 3 demonstrates the cost breakdown of the use of AAF in proposed practice in the UAE government and private sectors.
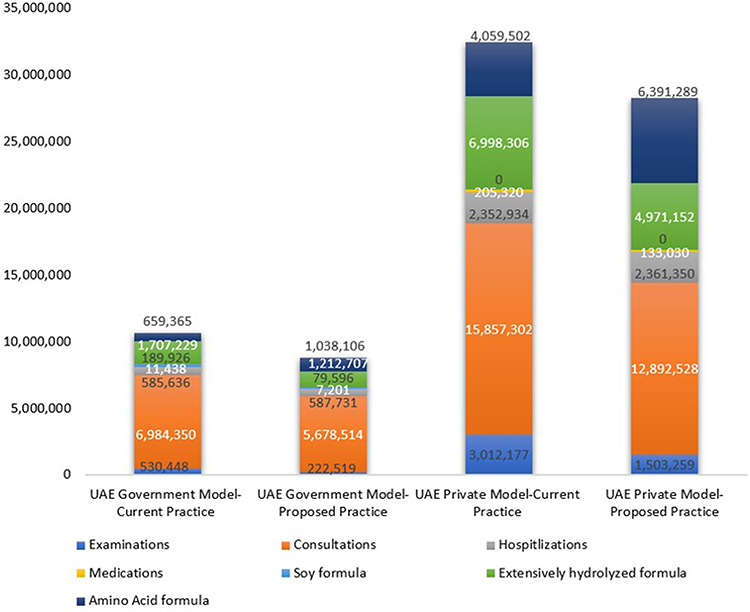 |
Figure 3 Cost breakdown of AAF in current and proposed practice in the UAE (Government sector and Private sector). Abbreviations: AAF, Amino Acid Formula; AED, United Arab Emirates Dirham; UAE, United Arab Emirates. |
Discussion
The current practice of CMPA diagnosis and management for infants involves serological diagnostic tests followed by continuous re-evaluation with an oral challenge test for symptomatic assessment by adjusting the ongoing treatment formula, starting with eHF formula followed by SF and AAF.9 This increases the time of diagnosis of CMPA and extends the symptomatic period. The proposed practice in the current study minimizes the OFC cycles, leading to early diagnosis of CMPA and the early introduction of effective infant formula as a substitute. This study is the first to estimate the budgetary impact of the early introduction of AAF in the diet of non-breast-fed infants suspected of CMPA in GCC countries—KSA, Kuwait, and the UAE.
Early introduction of AAF for the management of CMPA in the proposed practice exhibited the highest cost savings of 17% in the UAE government sector, followed by 13% in the UAE private sector and 10% in KSA, while Kuwait had cost savings of about 10%. Overall, the early introduction of AAF in the treatment pathway proves to be cost-saving from a health-care payer’s perspective for all three GCC countries—KSA, Kuwait, and the UAE.
Overall, the cost of medical examinations was the highest contributor to the cost savings, with a 58% (AED 307929) reduction in the UAE governmental sector; a 50% (AED 1508918) reduction in the UAE private sector; and a 41% (SAR 3427266) reduction in KSA. The reduction in the cost of SF largely impacted the cost savings in the UAE government sector by 58% (AED 110331) and in KSA by 58% (SAR 4204540). Another significant difference was the reduction in the medication cost in Kuwait by 37% (KWD 5630) and in the UAE private sector by 35% (AED 72290). However, the cost of AAF increased across all countries. This increase in cost could be because AAF was considered the primary infant formula in the proposed practice with a reduced intake of other substitute formulas.
The AAF-based infant formulas are non-allergic, well tolerated, and effective in symptomatic improvement in infants suspected of CMPA.27 They are recommended as the first choice for infants with severe complex gastrointestinal food allergies or life-threatening symptoms.7,9,28 Previous studies have established that the AAF formula is effective in symptomatic resolution in infants intolerant to eHF.29 Nevertheless, AAF is introduced as an ultimate treatment measure due to its high cost.
A pharmacoeconomic study from the perspective of the Brazilian public healthcare system proved that the early introduction of AAF in diagnosis is cost-saving and enhances symptom-free days compared to current treatment recommendations.30 In addition, the first-line use of AAF was associated with lower costs than eHF in infants with suspected CMPA presenting with proctocolitis or eczema in an economic burden of disease study in Turkey.31 The current study results also ascertain that the direct introduction of AAF is cost-saving and can reduce the overall cost of medication and the cost of medical examination associated with CMPA management. A limitation of the current study is that some inputs were derived from key medical experts from each country due to the unavailability of published data.
Limitations of the study: Considering being conducted in three Arabian gulf countries, the results of this study can be applied in countries with similar economic and financial status. Countries with less economic abilities may need to conduct their own studies to find what is more compatible to their financial status. In addition, as the study was conducted by explorative literature reviews and medical experts’ opinions, we did not directly assess the effects of AAF use on the duration of the symptomatic period of CMPA as well as including the variation of breastfeeding practice among the three including countries on the cost reduction as the main aim of the study was on non-breastfed infants with CMPA. We also did not analyze the effects of early using AAF according to CMPA subtypes.
Conclusion
We expect that early introduction of AAF for CMPA management can effectively reduce the symptomatic period for infants suspected of CMPA, which will be reflected on the cost of CMPA management. The current study results demonstrate that the early introduction of AAF is cost-saving from the health-care payer’s perspective for all three GCC countries—KSA, Kuwait, and the UAE. Hence, the early introduction of AAF could be clinically and economically significant in the GCC countries.
Abbreviations
AAF, Amino acid formula; AED, United Arab Emirates Dirham; CMPA, Cow Milk Protein Allergy; eHF, Extensively Hydrolyzed Formula; ESPGHAN, The European Society for Paediatric Gastroenterology Hepatology and Nutrition; GCC, The Gulf Cooperation Council; Ig, Immunoglobulin; KSA, The Kingdom of Saudi Arabia; KWD, Kuwaiti Dinar; OFC, Oral Food Challenge; RAST, Radioallergosorbent test; SAR, Saudi Riyal; SF, Soy Formula; UAE, The United Arab Emirates.
Data Sharing Statement
Data are available upon valid request by contacting the corresponding author by email.
Acknowledgments
The authors would like to thank Koshu Mahajan and Vibha Dhamija from IQVIA for their medical writing and editing support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation. All the authors took part in drafting, revising and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work, according to ICMJE authorship criteria. All authors ensured that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
Funding for the study was provided by Nutricia Middle East DMCC. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
Prof. Mohamed Miqdady received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events and consulting fees from Nutricia, Nestle, Novalac. Prof. Mohamed Miqdady received support from Nutricia for the manuscript. Dr. Christos Tzivinkos received Speaker Honoraria from Nutricia, Abbvie, Takeda and Nestle. Dr. Christos Tzivinkos received travel support from Nutricia and Nestle. The authors report no other conflicts of interest in this work.
References
1. Savage J, Johns CB. Food allergy: epidemiology and natural history. Immunol Allergy Clin North Am. 2015;35(1):45–59. doi:10.1016/j.iac.2014.09.004
2. Fiocchi A, Brozek J, Schünemann H, et al. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) Guidelines. Pediatr Allergy Immunol. 2010;21(Suppl 21):1–125.
3. Høst A, Halken S, Jacobsen HP, Christensen AE, Herskind AM, Plesner K. Clinical course of cow’s milk protein allergy/intolerance and atopic diseases in childhood. Pediatr Allergy Immunol. 2002;13(s15):23–28. doi:10.1034/j.1399-3038.13.s.15.7.x
4. Suh J, Lee H, Lee JH, et al. Natural course of cow’s milk allergy in children with atopic dermatitis. J Korean Med Sci. 2011;26(9):1152–1158. doi:10.3346/jkms.2011.26.9.1152
5. Tătăranu E, Diaconescu S, Ivănescu CG, Sârbu I, Stamatin M. Clinical, immunological and pathological profile of infants suffering from cow’s milk protein allergy. Romanian j Morphol Embryology. 2016;57(3):1031–1035.
6. Grabenhenrich LB, Dölle S, Moneret-Vautrin A, et al. Anaphylaxis in children and adolescents: the European Anaphylaxis Registry. J Allergy Clin Immunol. 2016;137(4):1128–1137.e1121. doi:10.1016/j.jaci.2015.11.015
7. Vandenplas Y, Koletzko S, Isolauri E, et al. Guidelines for the diagnosis and management of cow’s milk protein allergy in infants. Arch Dis Child. 2007;92(10):902–908. doi:10.1136/adc.2006.110999
8. Fiocchi A, Bouygue GR, Restani P, Bonvini G, Startari R, Terracciano L. Accuracy of skin prick tests in IgE-mediated adverse reactions to bovine proteins. Ann Allergy Asthma Immunol. 2002;89(6 Suppl 1):26–32. doi:10.1016/S1081-1206(10)62119-9
9. Koletzko S, Niggemann B, Arato A, et al. Diagnostic approach and management of cow’s-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. J Pediatr Gastroenterol Nutr. 2012;55(2):221–229. doi:10.1097/MPG.0b013e31825c9482
10. Mehta H, Groetch M, Wang J. Growth and nutritional concerns in children with food allergy. Curr Opin Allergy Clin Immunol. 2013;13(3):275–279. doi:10.1097/ACI.0b013e328360949d
11. Mailhot G, Perrone V, Alos N, et al. Cow’s milk allergy and bone mineral density in prepubertal children. Pediatrics. 2016;137:5.
12. Ehlayel M, Bener A. Camel’s milk allergy. Allergy Asthma Proce. 2018;39(5):384–388. doi:10.2500/aap.2018.39.4150
13. Terheggen-Lagro SW, Khouw IM, Schaafsma A, Wauters EA. Safety of a new extensively hydrolysed formula in children with cow’s milk protein allergy: a double blind crossover study. BMC Pediatr. 2002;2:10. doi:10.1186/1471-2431-2-10
14. Agostoni C, Axelsson I, Goulet O, et al. Soy protein infant formulae and follow-on formulae: a commentary by the ESPGHAN Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2006;42(4):352–361. doi:10.1097/01.mpg.0000189358.38427.cd
15. Bhatia J, Greer F. Use of soy protein-based formulas in infant feeding. Pediatrics. 2008;121(5):1062–1068. doi:10.1542/peds.2008-0564
16. Dupont C, Kalach N, Soulaines P, et al. Safety of a New Amino Acid Formula in Infants Allergic to Cow’s Milk and Intolerant to Hydrolysates. J Pediatr Gastroenterol Nutr. 2015;61(4):456–463. doi:10.1097/MPG.0000000000000803
17. Luyt D, Ball H, Makwana N, et al. BSACI guideline for the diagnosis and management of cow’s milk allergy. Clin Exp Allergy. 2014;44(5):642–672. doi:10.1111/cea.12302
18. Solé D, Silva LR, Rosário Filho NA, et al. Consenso Brasileiro sobre alergia alimentar: 2007. Rev Bras Alergia Imunopatol. 2008;31(2):64–89.
19. General Authority for statistics, Kingdom of Saudi Arabia, Saudi population 2018. Available from: https://www.stats.gov.sa/en/indicators/10.
20. Public Authority For Civil Information, Population statistics, Kuwait; 2018. Available from: http://stat.paci.gov.kw/englishreports/.
21. Dubai Statistics Center - Government of Dubai; 2018. Available from: https://www.dsc.gov.ae/en-us.
22. National Unified Procurement Company for Medical Supplies (NUPCO), Saudi Arabia. Available from: http://www.nupco.com.
23. Saudi Food and Drug Authority (SFDA), The Kingdom of Saudi Arabia. Available from: www.sfda.gov.sa.
24. Ministry of Health (MOH), Kuwait. Available from: https://www.moh.gov.kw/en/Pages/default.aspx.
25. Dubai Health Authority (DHA), Government of Dubai. Available from: https://services.dha.gov.ae/eservices/dhaweb/default.aspx.
26. Abu Dhabi Health Services Company (SEHA). Available from: www.seha.ae.
27. Hill DJ, Murch SH, Rafferty K, Wallis P, Green CJ. The efficacy of amino acid-based formulas in relieving the symptoms of cow’s milk allergy: a systematic review. Clin Exp Allergy. 2007;37(6):808–822. doi:10.1111/j.1365-2222.2007.02724.x
28. Meyer R, Groetch M, Venter C. When Should Infants with Cow’s Milk Protein Allergy Use an Amino Acid Formula? A Practical Guide. J Allergy Clin Immunol Pract. 2018;6(2):383–399. doi:10.1016/j.jaip.2017.09.003
29. Dupont C, Kalach N, Soulaines P, et al. A thickened amino-acid formula in infants with cow’s milk allergy failing to respond to protein hydrolysate formulas: a randomized double-blind trial. Paediatr Drugs. 2014;16(6):513–522. doi:10.1007/s40272-014-0097-x
30. Morais MB, Spolidoro JV, Vieira MC, et al. Amino acid formula as a new strategy for diagnosing cow’s milk allergy in infants: is it cost-effective? J Med Econ. 2016;19(12):1207–1214. doi:10.1080/13696998.2016.1211390
31. Sekerel BE, Seyhun O. Expert panel on practice patterns in the management of cow’s milk protein allergy and associated economic burden of disease on health service in Turkey. J Med Econ. 2017;20(9):923–930. doi:10.1080/13696998.2017.1342171
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.