Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Budget Impact Analysis of Botulinum Toxin Type A for Patients with Severe Blepharospasm in Thailand
Authors Hirunwiwatkul P ![]() , Permsuwan U
, Permsuwan U ![]() , Ngamkiatphaisan S, Chirapapaisan N
, Ngamkiatphaisan S, Chirapapaisan N ![]() , Sriratanaban J
, Sriratanaban J ![]()
Received 16 May 2025
Accepted for publication 29 September 2025
Published 11 October 2025 Volume 2025:17 Pages 717—728
DOI https://doi.org/10.2147/CEOR.S540982
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Parima Hirunwiwatkul,1,2 Unchalee Permsuwan,3,4 Sureerat Ngamkiatphaisan,5 Niphon Chirapapaisan,6 Jiruth Sriratanaban7
1Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 2Department of Ophthalmology, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand; 3Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand; 4Center for Medical and Health Technology Assessment (CM-HTA), Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand; 5Research Center of Health Systems and Services, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 6Department of Ophthalmology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 7Preventive and Social Medicine Department, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Correspondence: Unchalee Permsuwan, Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, 239 Huaykaew Road, Suthep, Chiang Mai, 50200, Thailand, Tel +665-394-4334, Fax +665-322-2741, Email [email protected]
Objective: Severe blepharospasm is a disabling neurological condition that significantly affects patients’ quality of life. Botulinum toxin type A (BoNT-A) is considered the standard treatment due to its targeted therapeutic effect and fewer systemic side effects compared to oral medications. However, its high cost poses a barrier to access within Thailand’s healthcare system. This study aimed to assess the budget impact of introducing BoNT-A treatment (Onabotulinumtoxin A and Abobotulinumtoxin A) compared with current oral medications for severe blepharospasm in Thailand.
Methods: A budget impact model was developed from the perspective of Thailand’s healthcare system over a 5-year time horizon. The current scenario (oral medications use) was compared with a new scenario involving BoNT-A treatment. The costs considered included drug acquisition, outpatient visits, and accident-related injuries. The base-case assumed gradual uptake of BoNT-A (30% in year 1, 50% in year 2, and 100% from year 3). Sensitivity analyses explored full uptake from year 1, no dose sharing, and inclusion of injury-related costs.
Results: Excluding injury-related costs, the 5-year net budget impact (NBI) was 7.91 million THB (223,040 USD) for onabotulinumtoxin A and 7.27 million THB (205,064 USD) for abobotulinumtoxin A. Including injury-related costs reduced the NBI to 4.20 million THB (118,564 USD) and 3.57 million THB (100,588 USD), respectively. Without dose sharing, the NBI rose significantly, reaching 40.5 million THB (1.14 million USD) for abobotulinumtoxin A.
Conclusion: BoNT-A treatment increases healthcare costs, primarily due to drug costs. However, reduced injury costs and dose-sharing strategies may enhance affordability and support BoNT-A’s inclusion in Thailand’s National List of Essential Medicine.
Keywords: blepharospasm, onabotulinumtoxin A, abobotulinumtoxin A, botulinum toxin, budget impact, Thailand
Introduction
Severe blepharospasm is a debilitating neurological condition characterized by involuntary eyelid spasms. This disorder significantly impacts patients’ daily activities and quality of life. The standard treatments for blepharospasm include oral medications such as clonazepam, trihexyphenidyl, and baclofen. However, these drugs are often associated with adverse effects, including sleepiness and drowsiness, which limit patient adherence and the overall effectiveness of treatment.1–3
Botulinum toxin type A (BoNT-A) treatment is considered the standard treatment for blepharospasm, with the evidence supporting its ability to effectively reduce disease severity and improve patients’ quality of life. BoNT-A works by temporarily blocking the release of acetylcholine at neuromuscular junctions, leading to a reduction in involuntary muscle spasms. Unlike oral medications, BoNT-A offers a more targeted approach, providing relief from symptoms without the common side effects of drowsiness or sleepiness.2
However, despite its clinical benefits, the high acquisition cost of BoNT-A compared to oral medications presents significant challenges for widespread adoption of patients under three healthcare schemes (Civil Servant Health Benefit Scheme, Social Security Scheme, and Universal Healthcare Coverage Scheme) in Thailand. One potential solution to this issue is the inclusion of BoNT-A with the indication of severe blepharospasm in Thailand’s National List of Essential Medicines (NLEM). This would allow patients covered under these healthcare schemes to access BoNT-A without facing substantial financial barriers, thereby increasing treatment accessibility for a larger population of patients with severe blepharospasm. The decision-making process for such a policy relies on economic evidence, with budget impact analysis (BIA) playing a crucial role in addressing the affordability issue for the government. Hence, this study was requested by the Health Economic Working Group under the Sub-Committee for the development of the NLEM in Thailand to assess the financial implications of introducing BoNT-A for the treatment of severe blepharospasm by substituting current oral medication treatments.
Methods
Budget Impact Model Overview
A budget impact model was developed using Microsoft Excel for Microsoft 365 (Microsoft Corporation, Redmond, WA, USA) to compare the costs associated with treating severe blepharospasm using BoNT-A (new scenario) versus current oral medications (current scenario). The model was designed to estimate the financial impact on Thailand’s healthcare system over a 5-year time horizon following the Thai Health Technology Assessment (HTA) Guideline.4
Estimation of Target Population
Thai patients diagnosed with severe blepharospasm had an average age of 61 years.3 The target population in this study included patients aged ≥61 years who were diagnosed with severe blepharospasm using the Jankovic Rating Scale (JRS). Eligible patients had a total JRS score, considering both severity and frequency, ≥6, indicating severe symptoms affecting their daily lives. Based on available epidemiological data, the prevalence of blepharospasm was estimated to be 2.59 per 100,000 people.5 Due to a lack of incidence data, we assumed that the incidence of blepharospasm was equal to the lower bound of 95% confidence interval for prevalence, which was 1.19 per 100,000 people. Of those with blepharospasm, 36% had a JRS score ≥6.6–9 Based on the Thai population of 11,818,211 people aged ≥61 years, the number of individuals with severe blepharospasm was estimated to be 110, and the number of new cases (incidence) was estimated to be 51.
The proportion of blepharospasm patients with JRS ≥ 6 reported in the literature is mainly derived from studies published between 1983 and 2008. Since then, there has been no further publication specifically reporting this distribution using the JRS. A more recent study from Japan described the clinical characteristics of blepharospasm patients; however, the JRS was not employed as the severity grading tool.10 Instead, clinical findings and functional impact were used for assessment, which are not standardized for international comparisons. For this reason, our analysis relied only on the available JRS-based literature, despite its publication period being relatively older.6–9
Treatment Scenarios
The current scenario, no BoNT-A treatment, involved the target population being treated with oral medications. Based on our unpublished survey of 35 Thai neuro-ophthalmologists and neurologists treating patients with blepharospasm (Table S1), oral medications included clonazepam (75%), trihexyphenidyl (23%), and others, such as nortriptyline and baclofen (2%).
The new scenario involved introducing BoNT-A, specifically onabotulinumtoxin A at 30 units (100 units per vial) and abobotulinum A at 90 units (500 units per vial), administered for a duration of approximately 12 to 16 weeks, depending on the patient’s individual response. It was assumed that the efficacy and safety of two products were not significantly different.
Healthcare Costs
In accordance with the Thai HTA Guideline,4 this study adopted a healthcare system perspective. Therefore, only undiscounted direct medical costs were included in the analysis. These costs comprised expenditures for medications, outpatient visits, and treatments related to injuries resulting from accidents attributable to vision impairment. Annual costs for each item were derived from a previous economic evaluation.11
For the BoNT-A treatment scenario, both onabotulinumtoxin A and abobotulinumtoxin A were assumed to be dose-shared among patients. The unit cost per injection was calculated by the required dosage per administration by the cost per vial, then divided by the total units per vial. Unit costs were based on 100 units per vial for onabotulinumtoxin A (7,312 THB or 206.27 USD) and 500 units per vial for abobotulinumtoxin A (11,209 THB or 316.18 USD), sourced from the Drug and Medical Supply Information Center, Ministry of Public Health.12 Out-patient visit costs were obtained from the multicenter study hospitals, which were in accordance with the service rate set by the Thailand Comptroller General’s department.
This analysis incorporated costs related to four types of accident-related injuries: cervical spine (C-spine) fractures, limb fractures, blunt abdominal injuries, and non-incapacitating injuries. The category of “non-incapacitating injuries”, as defined in the published literature, refers to minor injuries that do not require hospitalization. These include bruises, abrasions, and minor lacerations, requiring only simple sutures, which can be managed in an outpatient setting.13 These accident-related injuries were included to reflect the increased risk of accidents due to vision impairment in patients with severe blepharospasm. The probabilities of these injuries occurring in patients receiving BoNT-A treatment versus those not receiving BoNT-A treatment were obtained from literature review.13 The cost data were collected from medical records and face-to-face interviews with patients and their families. The injuries are caused by accidents such as falls, tripping, or bumping into objects, resulting from sudden, unpredictable, and uncontrollable bilateral eyelid closure. This mechanism produces temporary functional blindness and directly increases the risk of minor but clinically relevant injuries in affected patients.
To estimate the total cost of accident-related injuries, the probability of each type of injury was multiplied by its respective treatment cost. Treatment costs were based on the average medical expenses for complications from the joint diagnosis group at King Chulalongkorn Memorial Hospital, a major university affiliated hospital in Bangkok. The resulting individual injury costs were then summed up to derive the total cost of accident-related treatments.
All costs were adjusted to 2024 values using the medical care component of the Thai consumer price index.14 Costs were then converted to US dollars using an exchange rate of 35.45 THB/USD.15 The cost inputs are shown in Table 1.
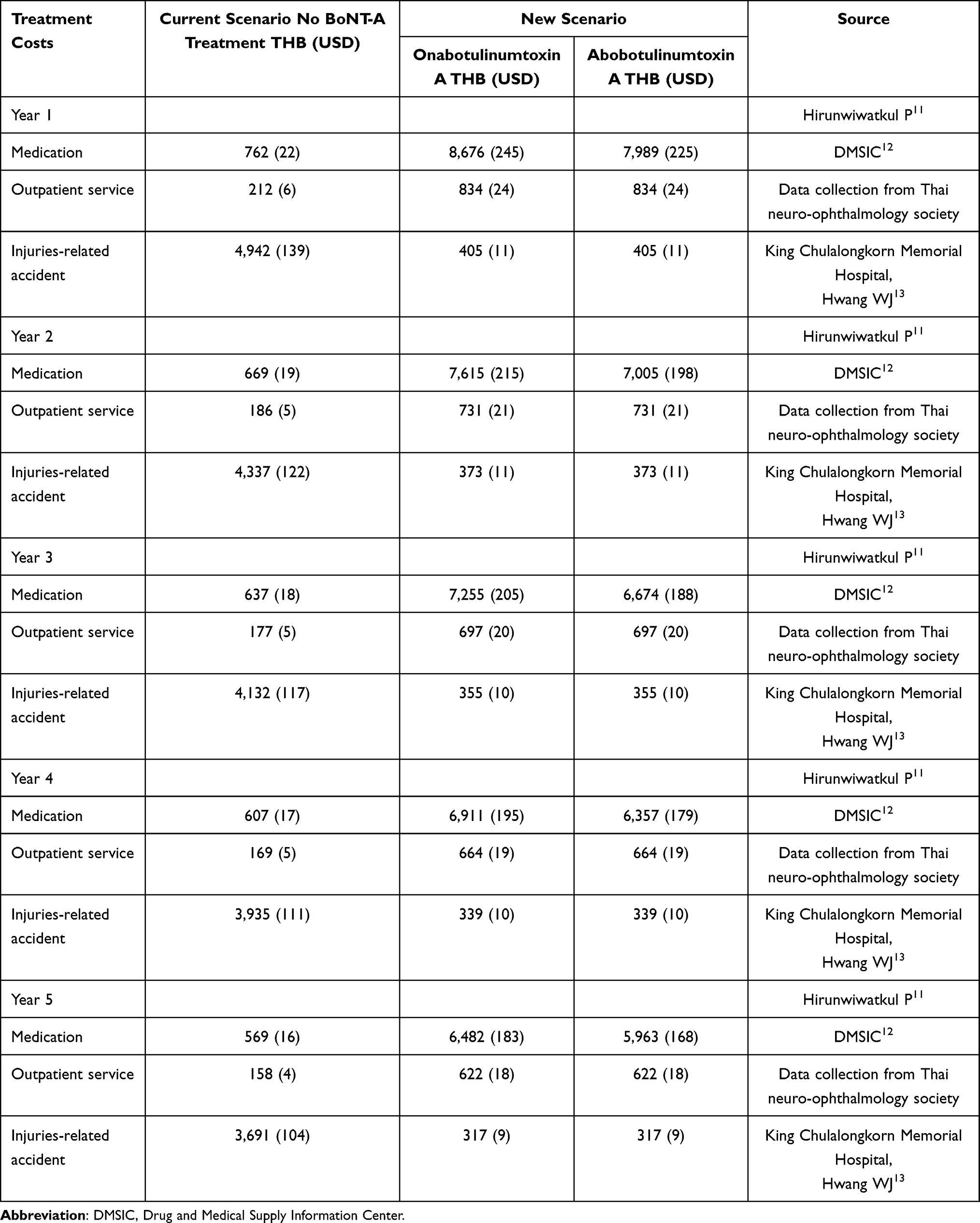 |
Table 1 Annual Cost Inputs |
Base-Case Analysis and Sensitivity Analysis
The BIA was performed over a 5-year time horizon. The total budgets of the current scenario (no BoNT-A treatment) and new scenario (BoNT-A treatment) were calculated. The base-case analysis excluded accident-related costs. The BoNT-A uptake assumptions were based on the current Thai healthcare setting, where eligible patients are treated at tertiary hospitals. Listing BoNT-A in the NLEM would improve access through government subsidies, but wider adoption requires training programs at regional hospitals. Accordingly, uptake was assumed to increase gradually: 30% in year 1, 50% in year 2, and 100% from year 3 onward, reflecting growing provider capacity and patient acceptance.
The net budget impact (NBI) was calculated as the difference in total expenditure between each BoNT-A treatment scenario and the no BoNT-A treatment scenario. Results were reported as annual NBI, 5-year cumulative costs and average annual costs. Deterministic sensitivity analysis was carried out to assess the impact of key parameter uncertainties. In this analysis, the BoNT-A uptake rate was assumed to be 100% from year 1 through year 5, and BoNT-A treatment costs were calculated without assuming dose sharing. In addition, a scenario analysis was conducted in which costs associated with accident-related injuries were included. The net budget impact was further assessed under alternative scenarios with reductions in drug acquisition costs per injection ranging from 10% to 50%.
Ethics Approval
The Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand, has exempted this study from compliance with the international guidelines for human research protection as Declaration of Helsinki, The Belmont Report, CIOMS Guidelines, International Conference on Harmonization in Good Clinical Practice (ICH-GCP) and 45CFR 46.101(b). The COE No. 030/2023.
Results
In the base-case analysis (excluding accident-related costs), introducing BoNT-A treatment at 30% uptake in year 1, 50% in year 2, and 100% from year 3 and onward, both BoNT-A treatment led to higher expenditures compared to the current scenario in all years. Over five years, the NBI was 7,906,753 THB (223,040 USD) for onabotulinumtoxin A and 7,269,507 THB (205,064 USD) for abobotulinumtoxin A (Table 2). The cost of BoNT-A itself contributed the largest share of the total NBI (Figure 1).
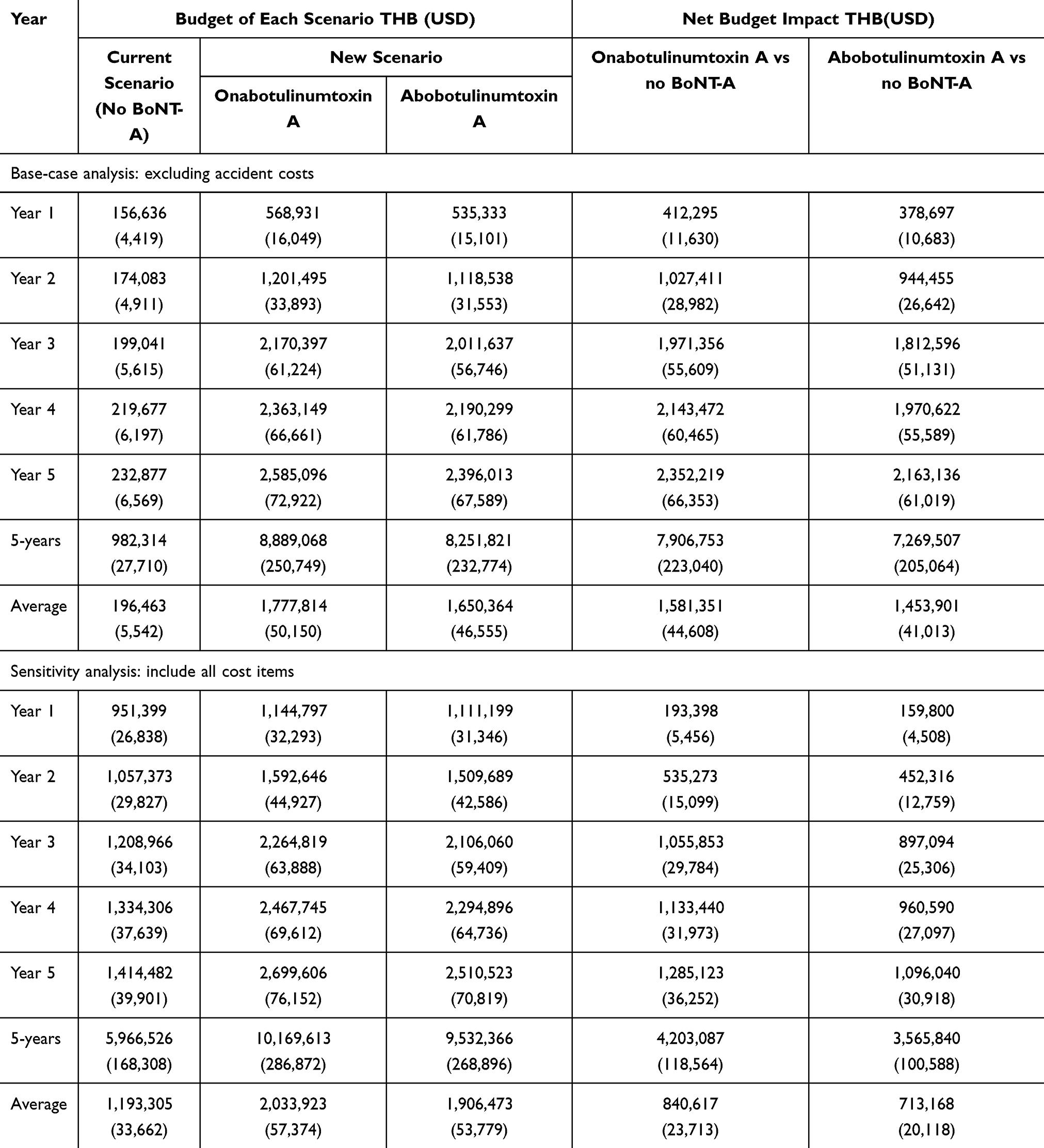 |
Table 2 Results of Base-Case Analysis and Scenario Analysis |
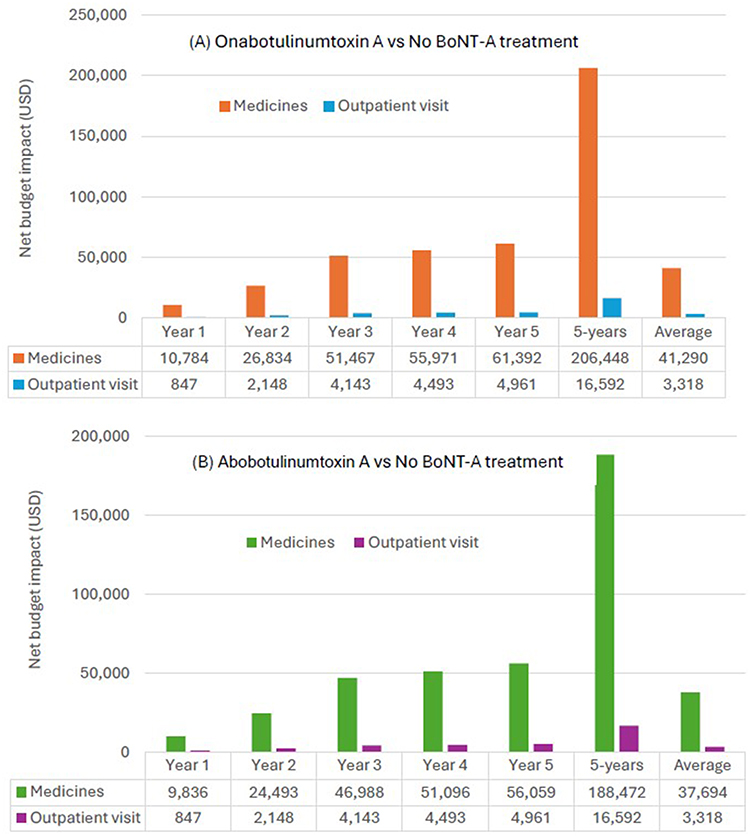 |
Figure 1 The component of net budget impact. (A) Onabotulinumtoxin A vs No BoNT-A treatment. (B) Abobotulinumtoxin A vs No BoNT-A treatment). |
When injury-related costs were included, the overall budgets for both scenarios increased. However, the increase was more pronounced in the current scenario (no BoNT-A treatment), leading to a smaller NBI in every year compared to the base-case analysis that excluded injury costs (Table 1).
When 100% uptake of BoNT-A treatment was introduced, the NBI increased compared to the base-case analysis, regardless of whether accident-related costs were included. Over the 5-year period, the NBI for both BoNT-A treatment remained higher than the current scenario (no BoNT-A treatment) in all years. Excluding accident-related costs, the 5-year NBI was 9.16 million THB (258,520 USD) for onabotulinumtoxin A and 8.42 million THB (237,583 USD) for abobotulinumtoxin A. Including accident-related costs, the NBI decreased to 4.63 million THB (130,504 USD) for onabotulinumtoxin A and 3.88 million THB (109,934 USD) for abobotulinumtoxin A, due to higher injury-related expenditures in the no-treatment scenario (Table 3 and Figure 2).
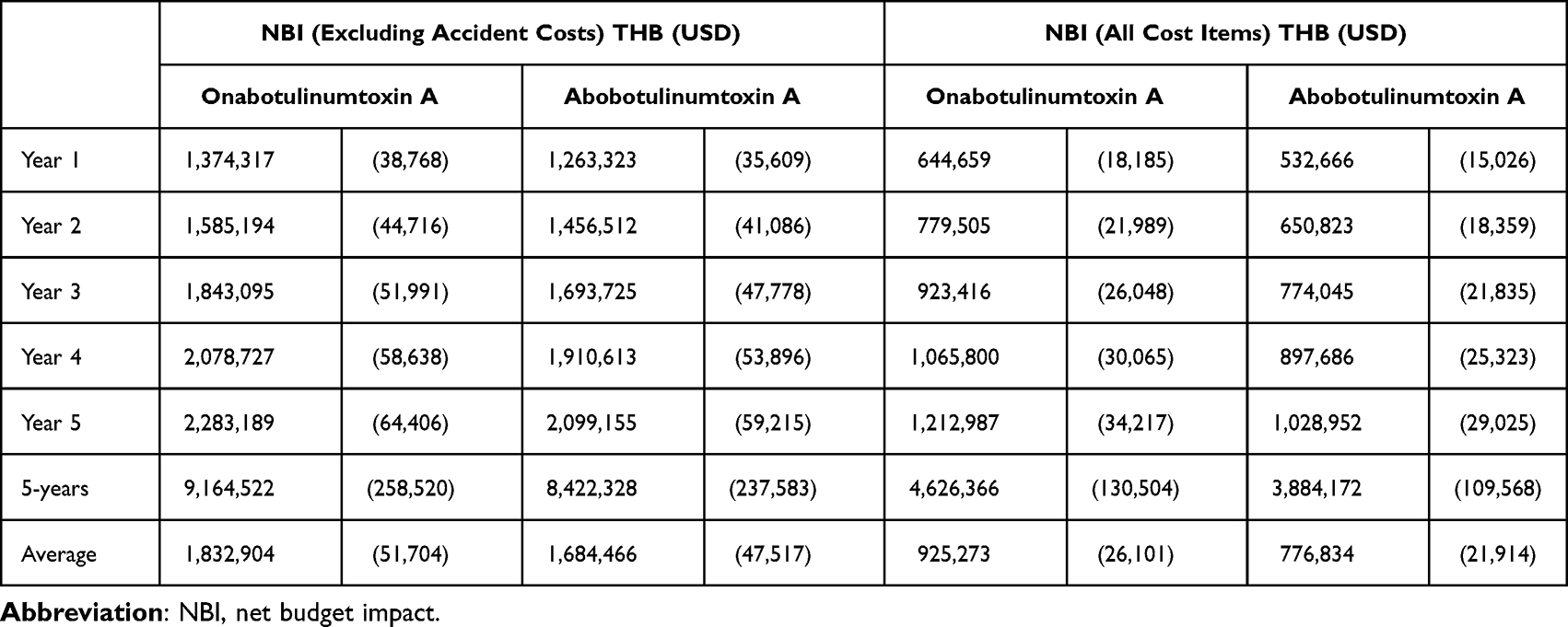 |
Table 3 Net Budget Impact for 100% Uptake of BoNT-A Treatment for year 1 Onward |
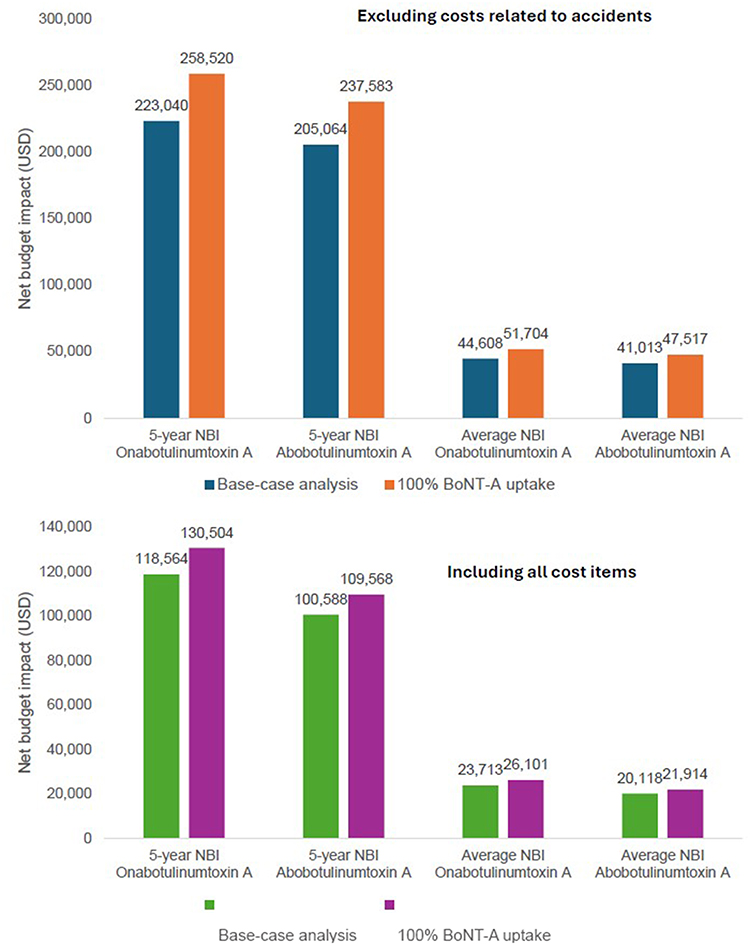 |
Figure 2 Net budget impact comparison between base-case and 100% BoNT-A uptake. |
When using either onabotulinumtoxin A or abobotulinumtoxin A at one vial per patient without dose sharing, the budget for BoNT-A treatment increased significantly, leading to a high NBI. Over five years, the NBI was 26.4 million THB (745,390 USD) for onabotulinumtoxin A and 40.5 million THB (1.14 million USD) for abobotulinumtoxin A, excluding accident-related costs. When accident-related costs were included, the NBI decreased slightly. The higher NBI associated with abobotulinumtoxin A was primarily due to its higher unit cost per vial compared to onabotulinumtoxin A (Table 4 and Figure 3).
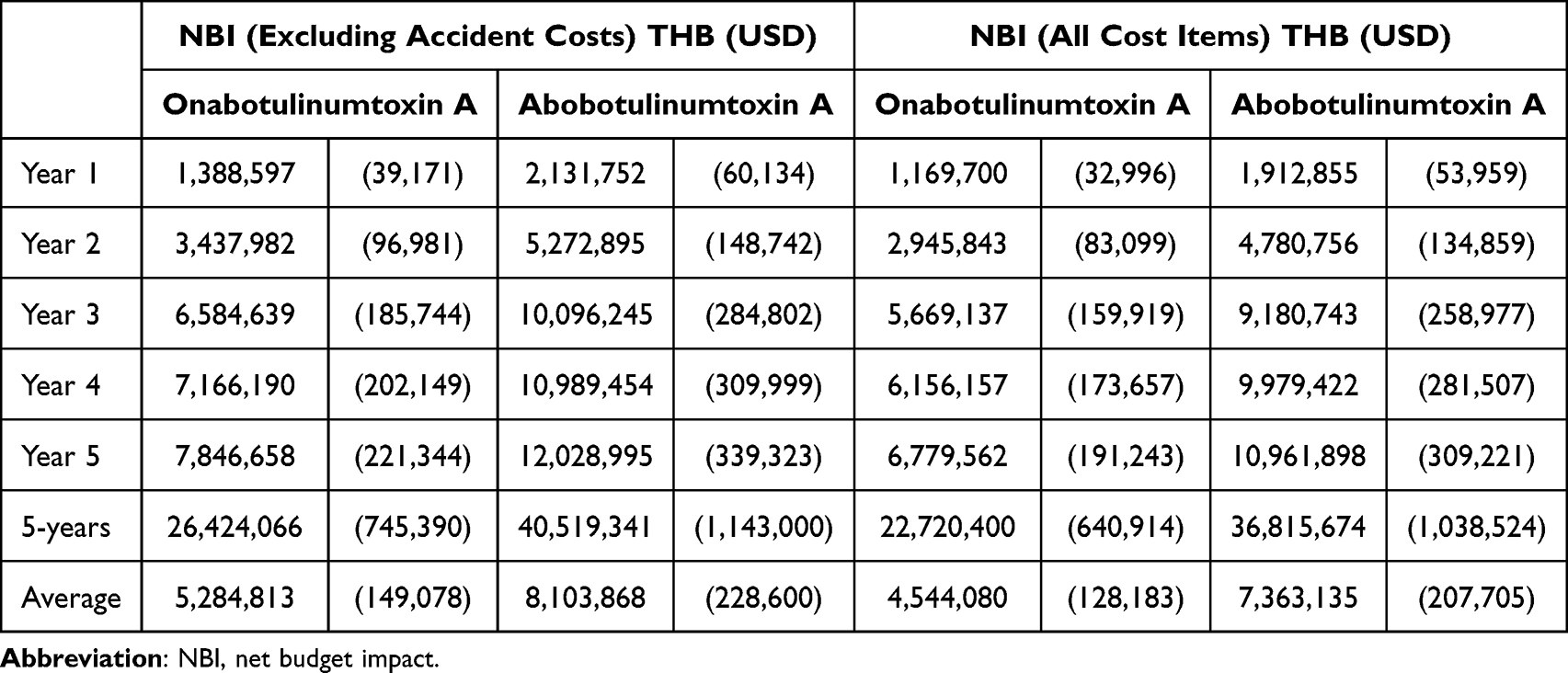 |
Table 4 Net Budget Impact Without Dose Sharing |
 |
Figure 3 Net budget impact comparison between base-case and no dose sharing. |
In addition, the NBI decreased as drug acquisition costs per injection were reduced for both onabotulinumtoxin A and abobotulinumtoxin A (Figure 4). At approximately a 50% reduction from the base-case cost, the NBI of abobotulinumtoxin A turned negative, indicating a cost-saving scenario.
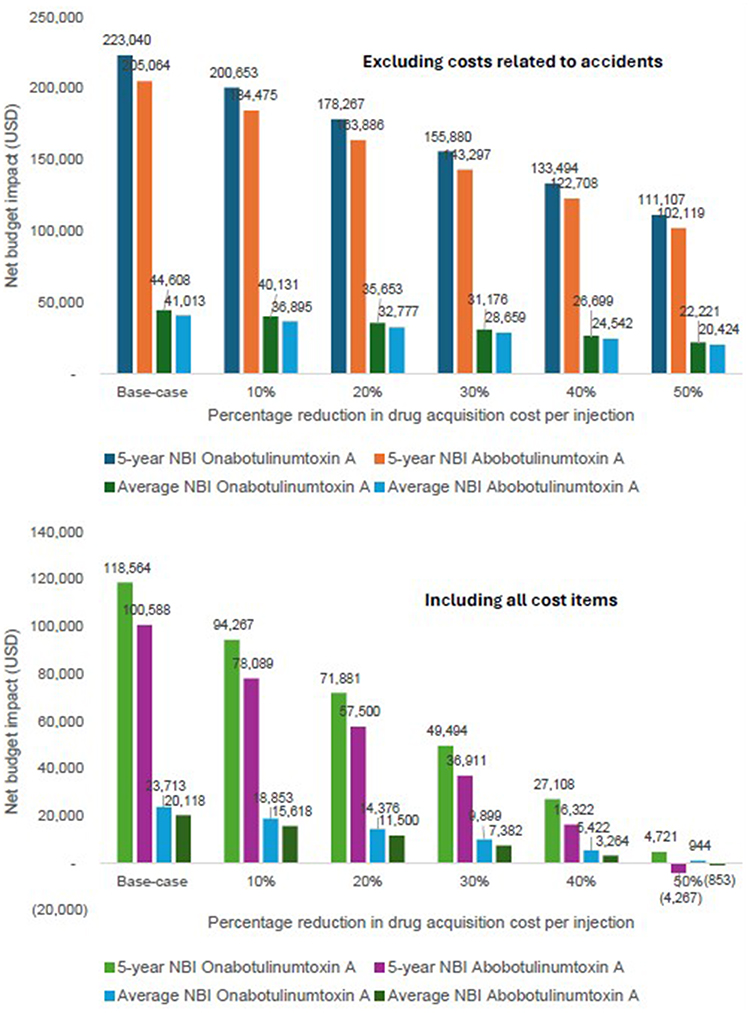 |
Figure 4 Net budget impact with 10%-50% reductions in drug acquisition costs. |
Discussion
Budget impact is an essential component of economic evidence to support decision-making. In Thailand, the inclusion of a medicine in the National List of Essential Medicines (NLEM) is guided by a multicriteria decision-making process. Safety and efficacy are the primary criteria considered for all purposed medicines. However, for high-cost medicines or those expected to impose a substantial budget impact, both economic evaluation and budget impact analysis information is required for the Subcommittee for the development of the NLEM to be conducted to consider in decision-making. Beyond these, additional factors such as healthcare system capacity, equity, and ethical considerations are also taken into account in the final decision-making process.16
This budget impact analysis evaluated the financial implications of introducing BoNT-A treatments (onabotulinumtoxin A and abobotulinumtoxin A) for patients with severe blepharospasm in Thailand, across various uptake scenarios and cost assumptions.
In the base-case analysis, where accident-related costs were excluded and BoNT-A uptake gradually increased (30% in year 1, 50% in year 2, and 100% from year 3 onward), both BoNT-A treatment resulted in higher annual and cumulative expenditures compared to the current scenario with no BoNT-A treatment. Over five years, the NBI was 7.91 million THB (223,040 USD) for onabotulinumtoxin A and 7.27 million THB (205,064 USD) for abobotulinumtoxin A. The cost of the BoNT-A drug itself was the main driver of the increased expenditure. However, when accounting for accident-related injury costs, which are more common in untreated patients, the NBI decreased across all years, particularly under full BoNT-A uptake. This reduction occurred because the lower incidence of injuries among BoNT-A treated patients partly offset the high acquisition cost of BoNT-A.
The size of the eligible population influenced the NBI. In base-case analysis, eligibility was defined as patients with severe blepharospasm aged 61 years and older. When the starting age was lowered to 50 years, the estimated 5-year NBI increased from 118,564 USD to 227,773 USD for onabotulinumtoxin A, and from 100,588 USD to 193,240 USA for abobotulinumtoxin A. When accident-related costs were excluded, the corresponding 5-year NBI rose from 223,040 USD to 428,482 USD for onabotulinumtoxin A, and from 205,064 USD to 393,949 USD for abobotulinumtoxin A.
Among the treatment options, abobotulinumtoxin A generally showed a lower budget impact than onabotulinumtoxin A under dose-sharing conditions, but this was reversed in scenarios without dose sharing due to abobotulinumtoxin A’s higher unit cost. The analysis highlights the importance of efficient administration practices, such as vial sharing, and underscores potential cost offsets from reducing vision-related injuries. However, in real-world clinical settings, the implementation of dose-sharing may be limited by challenges such as coordinating patient schedules, ensuring sterility and stability of opened vials, regulatory restrictions, increased staff workload, and potential patient inconvenience.
The study conducted in Thailand reported that integrating BoNT-A treatment into the Thai healthcare system for patients with post-stroke spasticity would require a budget outlay of approximately 15–35 million THB (413,246 USD – 966,103 USD).17 The estimated budget impact is approximately 3–5 times higher than the budget impact found in the present study for BoNT-A treatment in patients with severe blepharospasm. One possible reason is the higher number of patients with post-stroke spasticity compared to those with blepharospasm in Thailand. Inclusion of BoNT-A treatment for blepharospasm in the NLEM may therefore be affordable within the country’s resource constraints. However, effective administrative strategies, such as a dose sharing policy, should be implemented to manage costs efficiently.
Thailand relies heavily on imported medicines, with around 74% of total expenditure from multinational companies. To ensure equitable access, all three public insurance schemes cover only medicines listed on the NLEM.16 Inclusion of BoNT-A in the NLEM would therefore improve access for all patients, regardless of their insurance scheme.
Blepharospasm negatively affects mental health and socializing, as reported in previous studies. Beyond budget consideration, a prospective multicenter, observational study in Thailand found that BoNT-A treatment not only reduces physical severity but also improves quality of life, including non-physical aspects. Greater baseline severity was associated with larger quality of life improvements following BoNT-A treatment.3
This study has several limitations. First, the epidemiological estimates are constrained by a lack of local prevalence and incidence data, relying instead on data from other countries. Second, the model assumes constant treatment efficacy and injury risk reduction over the 5-year horizon, which may not fully reflect all clinical realities. Nonetheless, we attempted to address these uncertainties through multiple sensitivity analyses. Third, the costs of injury-related accidents were obtained from a single-hospital. Data from one center may not be representative of the broader Thai healthcare system. Future study should therefore collect cost data on injury-related accidents from hospitals at different levels of care across Thailand to strengthen the evidence on the benefit of BoNT-A treatment.
Conclusions
Introducing BoNT-A treatment for severe blepharospasm in Thailand increases healthcare expenditures, primarily due to the high cost of the drug. This impact is especially pronounced under full uptake and no dose-sharing conditions. However, when accounting for the potential reduction in accident-related injury costs and applying the use of dose-sharing strategies, the NBI is notably reduced. These findings suggest that BoNT-A treatment could be a financially viable option for inclusion in Thailand’s National List of Essential Medicines, particularly when combined with efficient administrative practices to manage costs and improve access. Inclusion of BoNT-A in the NLEM would therefore improve access for all patients, regardless of their insurance scheme.
Acknowledgments
This paper represents the views of the authors. This study was conducted at the request of the National List of Essential Medicine (NLEM). This manuscript is a part of the project “The health economic analysis of botulinum toxin type A for daily-life affected blepharospasm treatment” which was used to support the policy-making process under the Subcommittee for the Development of the NLEM in Thailand through the Health Economic Working Group (HEWG) but the HEWG is not responsible for the study findings and the dissemination of the fundings. The study was funded by the Food and Drug Administration, Ministry of Public Health, Thailand. We would like to acknowledge the assistance of OpenAI’s ChatGPT-4 architecture in refining the language and grammar of this document.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Woo KA, Kim HJ, Yoo D, et al. Patient-reported responses to medical treatment in primary dystonia. J Clin Neurosci. 2020;75:242–244. doi:10.1016/j.jocn.2020.03.025
2. Boghen DR, Lesser RL. Blepharospasm and hemifacial spasm. Curr Treat Options Neurol. 2000;2(5):393–400. doi:10.1007/s11940-000-0037-7
3. Hirunwiwatkul P, Supawatjariyakul W, Jariyakosol S, et al. Health-related quality of life of daily-life-affected benign essential blepharospasm: multi-center observational study. PLoS One. 2023;18(3):e0283111. doi:10.1371/journal.pone.0283111
4. Leelahavarong P. Budget impact analysis. In: Chaikledkaew U, Teerawattananon Y, editors. Guidelines for Health Technology Assessment in Thailand.
5. Medina Escobar A, Pringsheim T, Goodarzi Z, Martino D. The prevalence of depression in adult onset idiopathic dystonia: systematic review and metaanalysis. Neurosci Biobehav Rev. 2021;125:221–230. doi:10.1016/j.neubiorev.2021.02.036
6. Jankovic J, Ford J. Blepharospasm and orofacial-cervical dystonia: clinical and pharmacological findings in 100 patients. Ann Neurol. 1983;13(4):275–283. doi:10.1080/01658107.2017.1409770
7. Evatt ML, Freeman A, Factor S. Chapter 37 - Adult-onset dystonia. In: Weiner WJ, Tolosa E, editors. Handbook of Clinical Neurology. Elsevier; 2011:481–511.
8. Grandas F, Elston J, Quinn N, Marsden CD. Blepharospasm: a review of 264 patients. J Neurol Neurosurg Psychiatry. 1988;51(6):767–772. doi:10.1136/jnnp.51.6.767
9. Tolosa E, Marti MJ. Blepharospasm-oromandibular dystonia syndrome (Meige’s syndrome): clinical aspects. Adv Neurol. 1988;49:73–84.
10. Wakakura M, Yamagami A, Iwasa M. Blepharospasm in Japan: a clinical observational study from a large referral hospital in Tokyo. Neuroophthalmology. 2018;42(5):275–283. doi:10.1080/01658107.2017.1409770
11. Hirunwiwatkul P, Permsuwan U, Ngamkiatphaisan S, Chirapapaisan N, Sriratanaban J. Cost-utility analysis of botulinum toxin type A versus oral drug treatment in patients with severe blepharospasm in Thailand. PLoS One. 2025;20(4):e0319926. doi:10.1371/journal.pone.0319926
12. Drug and Medical Supply Information Center. Available from: http://dmsic.moph.go.th.
13. Hwang WJ, Tsai CF. Motor vehicle accidents and injuries in patients with idiopathic blepharospasm. J Neurol Sci. 2014;339(1–2):217–219. doi:10.1016/j.jns.2014.01.028
14. Bureau of Trade and Economics Indices, Ministry of Commerce. CPI. 2024. Available from: https://www.price.moc.go.th/en/content1.aspx?cid=1.
15. Bank of Thailand. Foreign exchange rates. Available from: https://www.bot.or.th/App/BTWS_STAT/statistics/ReportPage.aspx?reportID=123&language=th.
16. Teerawattananon Y, Tritasavit N, Suchonwanich N, Kingkaew P. The use of economic evaluation for guiding the pharmaceutical reimbursement list in Thailand. Z Evid Fortbild Qual Gesundhwes. 2014;108(7):397–404. doi:10.1016/j.zefq.2014.06.017
17. Hadnorntun P, Prawjaeng J, Kongmalai T, et al. Botulinum toxin type A for the treatment of patients with post-stroke spasticity in Thailand: cost-utility and budget impact analysis. BMJ Open. 2025;15(1):e090701. doi:10.1136/bmjopen-2024-090701
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preseptal and Pretarsal Botulinum Toxin Injection in Hemifacial Spasm and Blepharospasm: A 10-Year Comparative Study
Teekaput C, Teekaput K, Thiankhaw K
Therapeutics and Clinical Risk Management 2023, 19:35-42
Published Date: 13 January 2023