Back to Journals » Infection and Drug Resistance » Volume 19
Brucellosis Complicated by Thyroid Abscess and Life-Threatening Hemophagocytic Syndrome: A Case Report
Authors Wang Z, Ma R ![]() , Ding Z, Ma L, Liu X, Wang Y
, Ding Z, Ma L, Liu X, Wang Y
Received 21 November 2025
Accepted for publication 10 March 2026
Published 17 March 2026 Volume 2026:19 583365
DOI https://doi.org/10.2147/IDR.S583365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Zhiwei Wang,1,2 Ru Ma,1,2 Zihui Ding,1,2 Li Ma,1,2 Xiaoxuan Liu,1,2 Yan Wang1,2
1Department of Infection, Third Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 2Department of Infection, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, Shanxi, People’s Republic of China
Correspondence: Yan Wang, Department of Infection, Third Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China, Tel +8613513635015, Email [email protected]
Introduction: Brucella infections can affect various systems in the body, such as the osteoarticular and genitourinary systems; however, cases involving the thyroid gland are rare. This case report describes the clinical management of a thyroid abscess associated with brucellosis in a farmer.
Case Presentation: A 67-year-old male farmer presented to Shanxi Bethune Hospital on 17 March 2024 with a chief complaint of “intermittent fever with fatigue for over 3 months and neck swelling and pain for 2 months”. Upon admission, his serum Brucella tube agglutination test titre was 1:200, Rose Bengal plate agglutination test was positive, and blood culture was negative for Brucella. Neck computed tomography revealed a low-density nodular shadow in the right thyroid lobe measuring approximately 4.79× 4.45 cm. Coffee-coloured pus was aspirated during thyroid puncture. Pathogenic metagenomic next-generation sequencing and pus culture confirmed Brucella infection as the cause of the thyroid abscess. During treatment, the patient developed hemophagocytic syndrome. The patient’s condition was controlled with aggressive anti-infective therapy and glucocorticoid treatment. However, because of symptom recurrence, the patient ultimately underwent surgical intervention, comprising partial thyroidectomy, abscess incision and drainage, and thyroid injection, following which he recovered fully.
Conclusion: This article reports an extremely rare case of brucellosis leading to a thyroid abscess. Physicians should consider the possibility of brucellosis when encountering patients with thyroid abscesses and be vigilant of other potential complications.
Keywords: brucellosis, thyroid abscess, hemophagocytic syndrome, metagenomic next-generation sequencing, mNGS
Key Take-Aways
The key take-aways are as follows: (1) despite the low incidence of thyroid abscess, it should be considered in immunocompromised patients presenting with fever and neck pain. Furthermore, in patients whose symptoms persist despite initial management, thyroid abscess should also be included in the differential diagnosis, regardless of their immune status; (2) ultrasound-guided puncture for pus culture can aid in diagnosis, but if traditional culture is negative, novel techniques such as mNGS can assist in clinical diagnosis; (3) monitoring complete blood count, NK cell activity, and ferritin and soluble CD25 levels and bone marrow examination in patients with severe infection can facilitate early detection of concurrent HLH, enabling effective treatment; and (4) surgical intervention should be considered when combined antibiotic therapy and puncture drainage fail to control the condition.
Introduction
Brucellosis is a zoonotic disease caused by various Brucella species, and its main clinical manifestations include fever, chills, fatigue, sweating, weight loss, and arthralgia. It can affect multiple systems including the osteoarticular and genitourinary systems;1 however, cases involving the thyroid gland are rare. Of all the complications, the incidence of thyroid abscess is less than 1%.2 A thyroid abscess carries a risk of mortality and severe complications, including thyrotoxicosis, airway obstruction, internal jugular vein thrombosis, recurrent laryngeal nerve injury, and sepsis.3
Hemophagocytic lymphohistiocytosis (HLH) is a rare, life-threatening immune disorder characterised by the uncontrolled activation of cytotoxic lymphocytes and macrophages, leading to tissue damage and multi-organ dysfunction.4 HLH can be classified as primary or secondary. Primary HLH is caused by genetic mutations inherited in a homozygous or compound heterozygous manner. Secondary HLH is triggered by external factors such as infection, malignancy, rheumatological diseases, or other underlying causes.5 The clinical manifestations include persistent fever, hepatosplenomegaly, cytopenia (affecting two or more lineages), coagulopathy, hyperferritinaemia, and central nervous system involvement. Patient condition can rapidly deteriorate to multi-organ failure and death. Therefore, timely diagnosis and treatment are crucial for patient survival.6 To facilitate rapid clinical recognition, the core clinical features of HLH are summarized in Table 1.7 This case report details the diagnosis and treatment of a patient with brucellosis involving the thyroid, leading to a thyroid abscess complicated by HLH. The patient eventually recovered through anti-infective, anti-inflammatory, and surgical treatments.
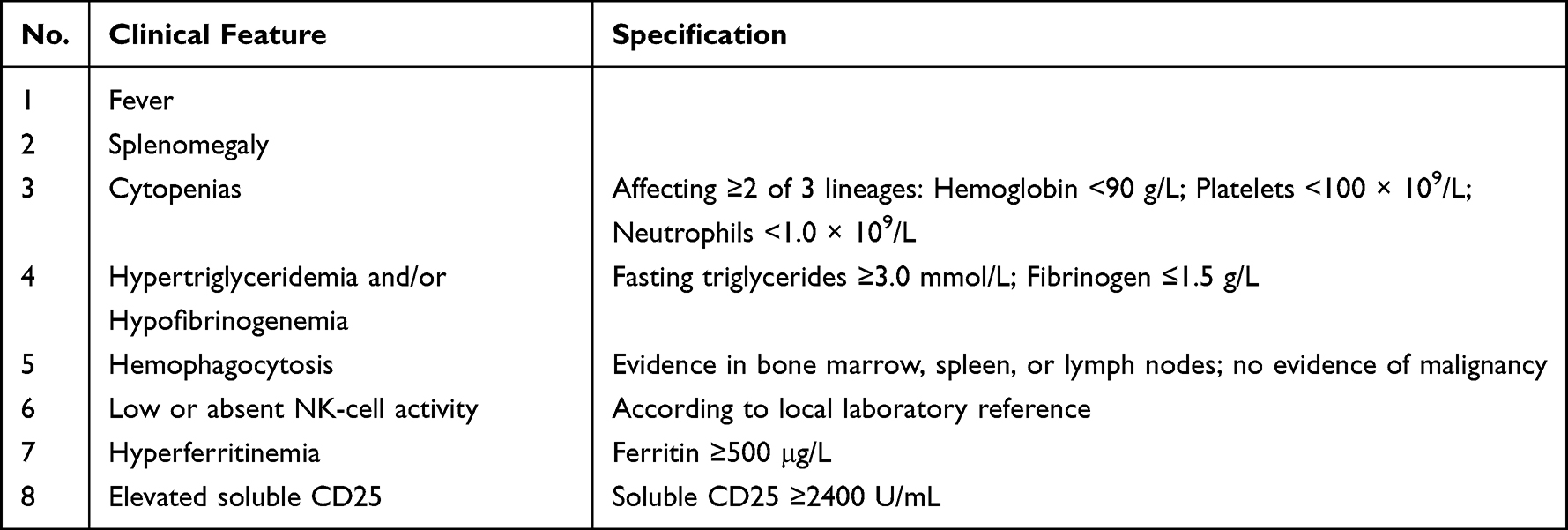 |
Table 1 Core Clinical Features of HLH |
Case Presentation
A 67-year-old male farmer engaged in animal husbandry presented with intermittent fever, with a maximum temperature of 38.8°C, and fatigue of unknown cause in December 2023. The patient did not seek immediate medical care. One month later, the patient developed neck swelling and pain. Thyroid ultrasonography, performed at a local hospital, revealed a heterogeneous nodule in the right thyroid lobe. Non-steroidal anti-inflammatory drug treatment provided no significant improvement, with recurrent fever and persistent enlargement of the thyroid nodule accompanied by swelling and pain. The patient was admitted to a local hospital on 15 March 2024. During hospitalisation, his temperature repeatedly spiked to a maximum of 39.6°C, and symptomatic treatment was ineffective. On 17 March 2024, he was transferred to the Department of Infectious Diseases at Shanxi Bethune Hospital with clinical signs of “intermittent fever with fatigue for 3 months and neck swelling and pain for 2 months”. Upon admission, the patient exhibited fever, fatigue, chills, and sweating. The neck pain was significant and severely affected swallowing and eating. Physical examination findings were as follows: temperature, 38.1°C; pulse, 89 beats/min; respiration rate, 21 breaths/min; and blood pressure, 123/76 mmHg. Significant swelling and tenderness were observed on the right side of the neck. Superficial lymph nodes in the neck were palpable, enlarged, and tender. All other physical signs were negative.
Laboratory results upon admission were as follows: white blood cell count, 5.7 × 109/L; neutrophil count, 3.93 × 109/L; lymphocyte count, 1.17 × 109/L; red blood cell count, 4.35 × 1012/L, haemoglobin level, 118 g/L; platelet count, 162 × 109/L; C-reactive protein level, >200 mg/L; erythrocyte sedimentation rate, 66 mm/h; interleukin-6 level, 97.3 pg/mL; and ferritin level, 483.2 ng/mL. Thyroid functional assessment revealed free T3 and T4 levels of 2.92 pg/mL and 1.39 ng/dL, respectively, and thyroid-stimulating hormone level of 0.92 μIU/mL. On 19 March 2024, the Brucella tube agglutination test showed a titre of 1:200, the Rose Bengal plate test was positive, and blood culture was negative.
On thyroid ultrasound, a cystic nodule (sized 6.7×4.6 × 4.0 cm) was observed in the right thyroid lobe, with multiple enlarged lymph nodes in the right supraclavicular region. On abdominal ultrasound, hepatomegaly (right lobe maximum oblique diameter, 15.9 cm), homogeneous parenchymal echo, and splenomegaly (length, 11.6 cm; intercostal thickness, 5.44 cm; anatomical length, 13.79 cm) were observed. Neck computed tomography (CT; plain and contrast) revealed a low-density nodular shadow (4.79 × 4.45 cm) in the right thyroid lobe. Soft tissue swelling was observed in the retropharyngeal space (Figure 1). The initial diagnoses were brucellosis, a thyroid nodule of unknown nature, infection, or tumour. The initial anti-brucellosis regimen was rifampin (0.6 g, once daily, oral) and doxycycline (0.1 g, twice daily, oral) combined with ceftriaxone (2 g, once daily, intravenously) for anti-brucellosis treatment. Further investigations of the thyroid were performed.
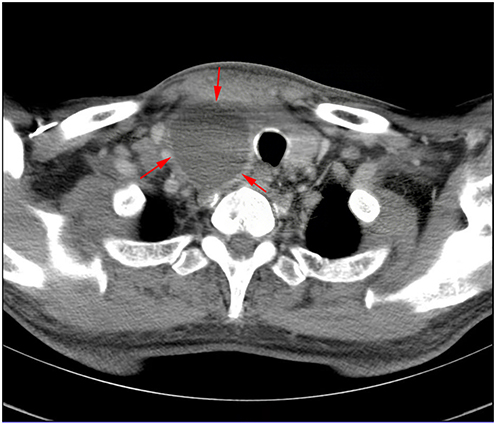 |
Figure 1 Neck computed tomography (CT) images, plain and contrast-enhanced, reveal a low-density nodular shadow (4.79 × 4.45 cm) in the right thyroid lobe. The arrow indicates the area of the thyroid abscess. |
On 21 March 2024, 50 mL of coffee-coloured pus was aspirated from the nodule in the right thyroid lobe under ultrasound guidance and sent for routine testing, bacterial culture, and pathogenic metagenomic next-generation sequencing (mNGS). On the day of puncture, the patient developed chills and high fever; therefore, levofloxacin was added to the anti-infective regimen (0.5 g once daily from 23 March, 2024). After the puncture, neck swelling and tenderness improved. However, owing to the small size of the liquefied abscess, drainage could not be performed.
On 24 March 2024, the pus test results returned. Microscopically, white blood cells (pus cells) covered the entire field of view/high power field. Bacterial culture was positive for Brucella spp., and pus mNGS detected 3,524,110 genus-specific alignment sequences for Brucella, confirming the diagnosis of brucellosis complicated by a thyroid abscess.
During subsequent treatment monitoring, progressive decreases in white blood cells, platelets, and haemoglobin were observed (minimums of 2.4 × 109/L, 49 × 109/L, and 117 g/L, respectively). Meanwhile, procalcitonin and ferritin levels showed continuous elevation (peaks of 5.68 and 898.3 ng/mL, respectively). Further tests showed NK cell activity of 10.98% and soluble CD25 level of 34943 pg/mL. Bone marrow aspiration results indicated hyperplastic marrow with hemophagocytic cells in the marrow smear (Figure 2). The patient met the following criteria: fever, hyperferritinaemia, pancytopenia, lymphadenopathy, splenomegaly, and presence of hemophagocytic cells in the bone marrow. A comprehensive diagnosis of brucellosis complicated by HLH was made. Treatment with dexamethasone (starting dose of 10 mg/m2, gradually tapered) was initiated and anti-infective therapy continued.
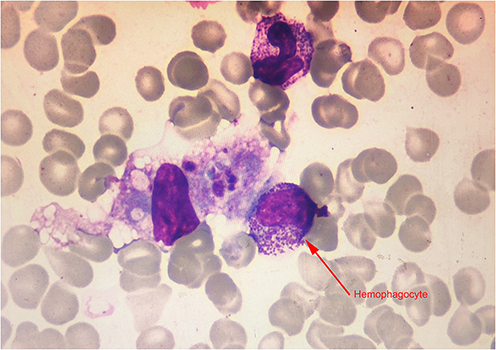 |
Figure 2 The myelogram shows hemophagocytosis. The arrow indicates a hemophagocyte containing phagocytosed granulocytes, erythrocytes, and platelets. |
Following active anti-infective and steroid treatments, patient indicators gradually improved (Table 2). After the patient’s condition stabilised, he was transferred to a local hospital for continued treatment with ceftriaxone (4 g once daily, intravenously for 10 days), rifampin (0.6 g once daily, oral), doxycycline (0.1 g twice daily, oral), and levofloxacin (0.5 g once daily, oral).
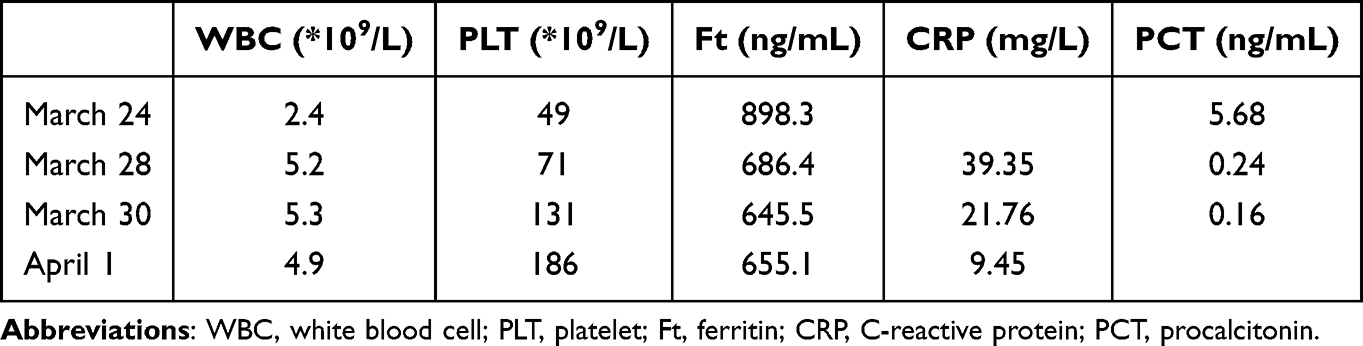 |
Table 2 Changes in Laboratory Indicators During the Treatment of Hemophagocytic Syndrome |
On 29 April 2024, during ongoing anti-brucellosis treatment, the patient experienced recurrent neck swelling and pain and returned to the Department of Infectious Diseases at Shanxi Bethune Hospital. Repeat neck CT revealed a liquid area within the cystic lesion in the right thyroid lobe, indicating a persistent thyroid abscess with progression compared to the scan from 20 March 2024. Considering the poor response of the thyroid abscess to medical anti-infective therapy and the small size of the liquefied area precluding drainage, surgical intervention was decided upon. After preoperative preparation, the patient underwent partial thyroidectomy, abscess incision, drainage, and thyroid injection. The resected specimens were sent for frozen section pathology. Thyroid follicles were observed within the hyperplastic fibrous tissue, with stromal haemorrhage accompanied by abundant acute and chronic inflammatory cell infiltration and lymphoid follicle formation. Numerous eosinophils were observed in some areas (Figure 3). Postoperatively, the patient continued anti-infective treatment without surgical complications and was discharged after 1 week of observation. Post-discharge, he continued oral anti-infective therapy with rifampin (0.6 g once daily), doxycycline (0.1 g twice daily), and levofloxacin (0.5 g once daily) (Figure 4).
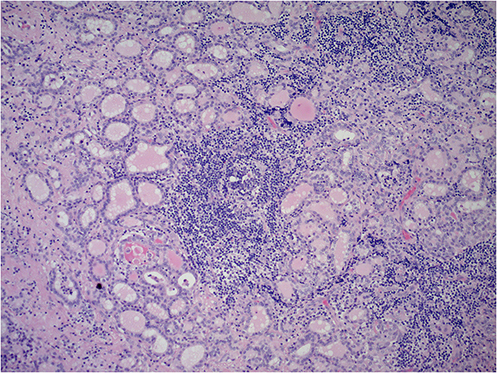 |
Figure 3 The resected specimens were sent for frozen section pathology. Thyroid follicles were observed within the hyperplastic fibrous tissue, with stromal haemorrhage accompanied by abundant acute and chronic inflammatory cell infiltration and lymphoid follicle formation. Numerous eosinophils were observed in some areas. |
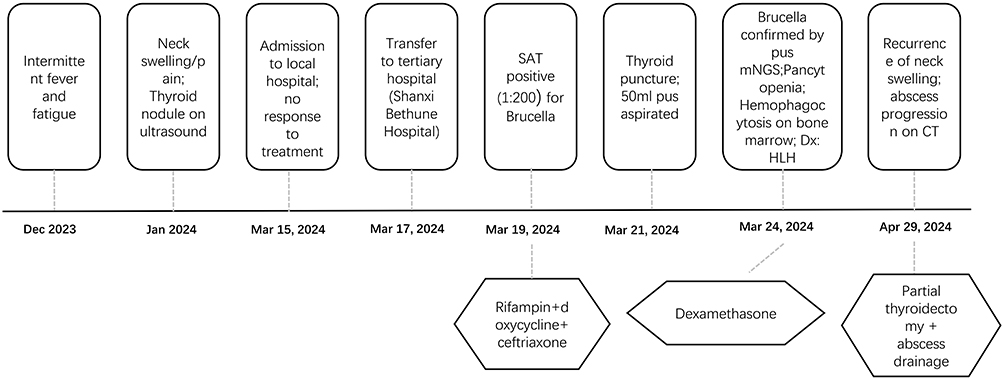 |
Figure 4 Timeline of diagnosis and management for brucellosis with thyroid abscess and secondary HLH. |
Six weeks post-surgery, follow-up neck CT revealed that the cystic lesion (1.41 × 2.04 cm) in the right thyroid lobe had significantly reduced in size compared to that in previous imaging. The patient was instructed to continue the anti-infective regimen until 12 weeks postoperatively. Telephone follow-up after 1 year indicated stable condition without recurrence of fever, fatigue, or neck pain.
Discussion
Brucella infections can affect various systems in the body, leading to diverse complications. Brucellosis, a zoonotic disease caused by Brucella species, is primarily transmitted to humans through ingestion of contaminated animal products or direct contact with infected animals. Only a small number of cases occur via aerosol, respiratory, or intrauterine transmission.8 The symptoms of brucellosis include fever, chills, fatigue, sweating, weight loss, and arthralgia. It can affect any organ or tissue, but most commonly affects the osteoarticular, digestive, genitourinary, or hematopoietic systems.1 Glandular involvement often affects the testes, epididymis, and prostate,9 with thyroid abscesses being an extremely rare clinical manifestation.
Akdemir reported a 25-year-old female patient who developed postpartum thyroid abscess 1 month after delivery and presented with tracheal compression. Aspiration of the thyroid abscess was performed, and the bacterial culture of the pus was positive for Brucella. The patient underwent left thyroid lobe, isthmus, and pyramidal lobe and abscess resection.10
Dastjerdi reported a 47-year-old female patient who presented with a progressively swollen neck mass. Based on neck CT findings, routine biochemical test results, a pus bacterial culture positive for Brucella ovis, and a single specific anti-Brucella o antiserum, a diagnosis of thyroid abscess was made. Treatment by surgical abscess drainage and antibiotic therapy resolved the condition.11
Harman reported a 20-year-old patient who was initially diagnosed with brucellar sacroiliitis and presented with neck pain during the course of anti-Brucella therapy. Brucella was detected on bacterial culture of the specimen obtained by fine needle aspiration biopsy. The patient did not undergo surgery, and the anti-Brucella therapy was extended to 11 weeks.12
Starakis reported an 87-year-old female patient who presented with fever and neck pain and had a 2-year history of glucocorticoid use. The patient was diagnosed with a thyroid abscess, and fine needle aspiration biopsy culture was positive for Brucella. Initially, the patient was administered only anti-Brucella therapy, but later underwent thyroidectomy due to disease progression.13
Sunnetcioglu reported a 22-year-old female patient who presented with fever, neck pain, and swelling and had a 4-year history of goitre. Aspiration of a thyroid cyst revealed Brucella on bacterial culture. The patient underwent thyroidectomy, and the condition was resolved following anti-Brucella therapy.14
Kazaz reported a 45-year-old female patient who presented with neck pain and was diagnosed with thyroid abscess. Bacterial culture of the thyroid abscess drainage was positive for Brucella, and the condition was resolved with anti-Brucella therapy.2
Zhou reported a 61-year-old male patient who presented with a progressively enlarged neck mass. The patient was initially diagnosed with intracystic haemorrhage of thyroid cystadenoma and was scheduled for thyroidectomy, but was diagnosed with a thyroid abscess intraoperatively and underwent thyroid abscess drainage surgery. Brucella was cultured from the pus, and the patient’s condition resolved following postoperative anti-Brucella therapy.15
A synthesis of these reported cases reveals several common features: the majority occurred in female patients (7/8), often with predisposing factors such as postpartum status, glucocorticoid use, or pre-existing thyroid conditions. Surgical intervention (abscess drainage or thyroidectomy) was required in most cases, highlighting the limitations of antibiotic therapy alone in managing localized infections. Compared with these previously reported cases, the present case is unique in two significant aspects. First, the patient developed HLH during the disease course, a complication not documented in any of the prior thyroid abscess cases. Second, the clinical course was characterized by initial improvement followed by relapse after discharge, ultimately requiring surgical intervention—a pattern that underscores the importance of close monitoring and consideration of surgical drainage even in apparently stable patients.
Normally, the thyroid gland is highly resistant to infections, and the incidence of thyroid infections and abscesses is low. This is primarily due to its protective fibrous capsule, rich blood supply, lymphatic drainage, and the inhibitory effect of high iodine content on bacteria.16
Thyroid abscesses are more likely to occur in two groups: (1) immunocompromised individuals, such as those with human immunodeficiency virus infection, those receiving chemotherapy or steroid therapy, and post-transplant patients;17 and (2) individuals with pre-existing thyroid diseases, such as goitre, pyriform sinus fistula, or thyroid cancer.18 In the present case, the patient had no identified immunodeficiency but had a pre-existing thyroid nodule, which might have been a contributing factor.
The most common pathogens causing thyroid abscesses are Staphylococcus aureus and Streptococcus species, followed by Gram-negative bacilli,19 including Salmonella,20 Escherichia coli,21 Klebsiella pneumoniae,22 and Brucella.2 Overall, this case of thyroid abscess caused by Brucella is exceedingly rare. Other bacteria were not detected in the purulent sample.
Ultrasonography is the preferred method for diagnosing thyroid abscesses and can guide puncture for further diagnosis.19 In the present case, ultrasound-guided puncture yielded purulent fluid. Bacterial culture and mNGS testing of the pus led to the definitive diagnosis of brucellosis with a thyroid abscess. Compared with traditional bacterial culture, mNGS offers advantages such as a broad scope, rapid turnaround time, and no need for incubation. Although mNGS cannot replace traditional culture methods, its rapid and accurate diagnostic value can significantly aid patient diagnosis and treatment. The combined use of mNGS and traditional culture methods can further improve the pathogen detection rate.23,24 In the present case, both bacterial culture and mNGS were performed on the pus from the thyroid abscess, allowing timely and accurate identification of the pathogen and facilitating the development of a more comprehensive anti-infective regimen. Although species-level identification of Brucella was not performed in this case, this did not compromise patient management. Currently, no distinct treatment regimens have been established for different Brucella species.25 Therefore, while species-level identification holds significant value for epidemiological surveillance and source tracing,26 the lack of species differentiation was not a critical limitation in the urgent clinical decision-making process for this thyroid abscess case.
Doxycycline and rifampin are first-line therapeutic agents. Quinolones and aminoglycosides are also effective against brucellosis. The current practice typically involves combination therapy with two or more antibiotics. For specific patients such as those with abscesses, combination antibiotic therapy may be supplemented with puncture and pus drainage. Surgical intervention should also be considered.8,27 In this case, after diagnosis, combined antibiotic therapy was promptly initiated. Due to the small abscess size, puncture drainage was initially not feasible, but the condition was initially controlled. However, the patient’s symptoms recurred after discharge, necessitating surgery.
Brucella can promote macrophage activation through pathways such as TLR4, potentially triggering an excessive inflammatory response that may lead to HLH.28–31 For the diagnosis of HLH, the HLH-2004 criteria remain the current standard, requiring the presence of at least five of the eight core clinical features summarized in Table 1 to establish a definitive diagnosis. In this case, the decrease in blood cell count and rising ferritin levels during treatment indicated the possibility of HLH, allowing for timely intervention. Controlling the underlying infection is key. The concurrent use of medications such as dexamethasone, etoposide, or cyclosporine may be necessary to control excessive inflammatory responses.32 Notably, while the thyroid abscess was ultimately managed with surgical resection due to recurrence after initial medical therapy, the patient’s HLH had already been controlled through pharmacologic intervention prior to surgery. This suggests that in brucellosis-associated HLH, controlling the systemic inflammatory response with medical therapy can be achieved even when the local infectious focus requires subsequent surgical management.
Limitations
As this is a single case report, there are inherent limitations. The diagnostic approaches and therapeutic strategies discussed herein may serve as a reference for clinical practice. However, the management of other patients should be individualized based on their specific clinical circumstances.
Conclusions
In summary, this report presents a rare case of thyroid abscess caused by Brucella infection, complicated by the development of HLH. Future multicenter collaboration is warranted to accumulate more cases and further elucidate the disease characteristics and optimal treatment strategies.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study complies with the requirements of the Declaration “Helsinki Declaration”, and was approved by the Ethics Committee of Shanxi Bethune Hospital (No. YXLL-2025-238). Written informed consent was obtained from the patient. Written informed consent was obtained from the patient for publication of this case report and images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Buzgan T, Karahocagil MK, Irmak H, et al. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature. Inter J Infect Dis. 2010;14(6):e469–9. doi:10.1016/j.ijid.2009.06.031
2. Kazaz I, Yazici E, Aygar İS, HoŞBul T. Brucella melitensis’in Neden Olduğu Bir Tiroid Bezi Apsesi Olgusu. Mikrobiyoloji Bulteni. 2024;58(2):217–223. doi:10.5578/mb.20249810
3. AlYousef MK, Al-Sayed AA, Al Afif A, Alamoudi U, LeBlanc JM, LeBlanc R. A pain in the neck: Salmonella spp. as an unusual cause of a thyroid abscess. A case report and review of the literature. BMC Infect Dis. 2020;20(1). doi:10.1186/s12879-020-05161-w
4. Griffin G, Shenoi S, Hughes GC. Hemophagocytic lymphohistiocytosis: an update on pathogenesis, diagnosis, and therapy. Best Pract Res. 2020;34(4):101515. doi:10.1016/j.berh.2020.101515
5. Ponnatt TS, Lilley CM, Mirza KM. Hemophagocytic Lymphohistiocytosis. Arch Pathol Lab Med. 2022;146(4):507–519. doi:10.5858/arpa.2020-0802-RA
6. Chinnici A, Beneforti L, Pegoraro F, et al. Approaching hemophagocytic lymphohistiocytosis. Front Immunol. 2023;14. doi:10.3389/fimmu.2023.1210041
7. Henter JI, Horne A, Aricó M, et al. HLH‐2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2006;48(2):124–131. doi:10.1002/pbc.21039
8. Qureshi KA, Parvez A, Fahmy NA, et al. Brucellosis: epidemiology, pathogenesis, diagnosis and treatment–a comprehensive review. Ann Med. 2024;55(2). doi:10.1080/07853890.2023.2295398
9. Jin M, Fan Z, Gao R, Li X, Gao Z, Wang Z. Research progress on complications of brucellosis. Front Cell Infect Microbiol. 2023;13. doi:10.3389/fcimb.2023.1136674
10. Akdemir Z, Karaman E, Akdeniz H, Alptekin C, Arslan H. Giant thyroid abscess related to postpartum brucella infection. Case Reports Infect Dis. 2015;2015:1–3. doi:10.1155/2015/646209
11. Moradi Dastjerdi S, Karimi Ghahderijani F, Sajad RS, Sen K. Acute granulomatous thyroiditis with abscess formation due to brucellosis: a case report. Case Reports Endocrinol. 2025;2025(1). doi:10.1155/crie/9644135
12. Harman R, Aşık Z, Inan D, Turhan Ö, Baysan B, Gunseren F. Thyroid abscess due to brucellosis: case report. Trakya Universitesi Tip Fakultesi Dergisi. 2010;27(4).
13. Starakis I, Stoubou V, Siagris D, Alexandridis T, Petrochilos I, Karatza C. Brucellar thyroid abscess: case report and review of the causes and management of this rare medical entity. Infect Dis Clin Pract. 2007;15(1):70–73. doi:10.1097/01.idc.0000236981.35194.45
14. Sunnetcioglu M, Ceylan MR, Atmaca M, Baran Aİ, Mentes O, Ücler R. Rare brucellosis involvement: thyroid gland abscess. East J Med. 2015;20(1):62.
15. Zhou T, Wang G, Luo X, et al. Clinical features of a case of brucellosis complicated with thyroid abscess. Chin J Endemiol. 2024;133–136.
16. Falhammar H, Wallin G, Calissendorff J. Acute suppurative thyroiditis with thyroid abscess in adults: clinical presentation, treatment and outcomes. BMC Endocr Disord. 2019;19(1). doi:10.1186/s12902-019-0458-0
17. Damoune I, Akioud F, Cherrabi K, Benhommad O, Ajdi F. Thyroid abscess in a human immunodeficiency virus-infected patient. Egyptian J Otolaryngol. 2022;38(1). doi:10.1186/s43163-022-00307-w
18. Khoo KS, Koh PS, Ng KL. Salmonella thyroid abscess—two case reports. Gland Surg. 2020;9(6):2198–2203. doi:10.21037/gs-20-474
19. Yedla N, Pirela D, Manzano A, Tuda C, Lo Presti S. Thyroid abscess: challenges in diagnosis and management. J Investigative Med High Impact Case Reports. 2018;6. doi:10.1177/2324709618778709
20. Sahli M, Hemmaoui B, Errami N, Benariba F. Salmonella thyroid abscess. European Ann Otorhinolaryngol Head Neck Dis. 2022;139(1):51–52. doi:10.1016/j.anorl.2021.05.004
21. Urbón‑sánchez P, Mendoza‑Moreno F, Sánchez De Toca‑Gómez S, et al. Thyroid abscess, an uncommon diagnosis: a case report and mini‑review of the literature. Med Int. 2024;4(3). doi:10.3892/mi.2024.153
22. Sanker V, Mohamed A, Jadhav C. Acute suppurative thyroiditis (AST) with thyroid abscess: a rare and potentially fatal neck infection. Cureus. 2022. doi:10.7759/cureus.29062
23. Hilt EE, Ferrieri P. Next generation and other sequencing technologies in diagnostic microbiology and infectious diseases. Genes. 2022;13(9):1566. doi:10.3390/genes13091566
24. Zhou Y, Shi W, Wen Y, Mao E, Ni T. Comparison of pathogen detection consistency between metagenomic next-generation sequencing and blood culture in patients with suspected bloodstream infection. Sci Rep. 2023;13(1):9460. doi:10.1038/s41598-023-36681-5
25. National Health Commission of the People’s Republic of China. Bulushi junbing zhenliao fang’an (2023 nian ban) [Diagnosis and treatment scheme for Brucellosis (2023 Edition)]. Chin J Infect Control. 2024;23(5):663–664. doi:10.12138/j.issn.1671-9638.20245123
26. De Massis F, Ali RM, Serrani S, et al. Genetic diversity of Brucella melitensis isolated from domestic ruminants in Iraq. Microorganisms. 2024;12(3):475. doi:10.3390/microorganisms12030475
27. Lafontaine N, Learoyd D, Farrell S, Wong R. Suppurative thyroiditis: systematic review and clinical guidance. Clin Endocrinol. 2021;95(2):253–264. doi:10.1111/cen.14440
28. Yu H, Bai L, Zhang Y, Wang Z, Yu Y. Repetitive extragenic palindromic DNA sequences from Brucella melitensis stimulate Toll-like receptor 9 signaling in macrophages. Mol Med Reports. 2017;15(1):271–276. doi:10.3892/mmr.2016.5990
29. Hao M, Zhao D, Liu W, et al. Deletion of the alr gene in Brucella suis S2 attenuates virulence by enhancing TLR4-NF-κB-NLRP3- mediated host inflammatory responses. Int Immunopharmacol. 2024;137:112443. doi:10.1016/j.intimp.2024.112443
30. Wang Y, Li Y, Li H, et al. Brucella dysregulates monocytes and inhibits macrophage polarization through LC3-dependent autophagy. Front Immunol. 2017;8. doi:10.3389/fimmu.2017.00691
31. Jarvis BW, Harris TH, Qureshi N, Splitter GA. Rough lipopolysaccharide from Brucella abortus and Escherichia coli differentially activates the same mitogen-activated protein kinase signaling pathways for tumor necrosis factor alpha in RAW 264.7 macrophage-like cells. Infect Immun. 2002;70(12):7165–7168. doi:10.1128/iai.70.12.7165-7168.2002
32. Park D, Yoon K, Lo A, Bolos D. Hemophagocytic lymphohistiocytosis induced by brucellosis: a case report. Cureus. 2024;16(7). doi:10.7759/cureus.64287
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.