Back to Journals » Cancer Management and Research » Volume 12
Bronchial Sleeve Resection with Complete Pulmonary Preservation: A Single-Center Experience
Authors Duan J, Cai H, Huang W, Lin L, Wu L, Fan J
Received 17 October 2020
Accepted for publication 6 December 2020
Published 16 December 2020 Volume 2020:12 Pages 12975—12982
DOI https://doi.org/10.2147/CMAR.S286934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Chien-Feng Li
Jiangnan Duan,1,* Haomin Cai,1,* Wei Huang,1,* Lin Lin,2 Liang Wu,1 Jiang Fan1
1Department of Thoracic Surgery, Shanghai Pulmonary Hospital, Shanghai, People’s Republic of China; 2School of Medicine, Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liang Wu; Jiang Fan Department of Thoracic Surgery
Shanghai Pulmonary Hospital, Shanghai, People’s Republic of China
Email [email protected]; [email protected]
Purpose: Bronchial sleeve resection with complete pulmonary preservation (BSRCPP) is a classic surgical method for the treatment of benign or low-grade bronchial tumors. For elderly patients and patients with poor cardiopulmonary function, BSRCPP is particularly advantageous because some of these patients may not tolerate lobectomy or pneumonectomy. We retrospectively reviewed the clinical data of 20 patients who underwent BSRCPP during the past 7 years. This report presents the experience with BSRCPP in our department.
Patients and Methods: We collected the data of 20 patients who underwent BSRCPP. Of these 20 patients, 17 underwent thoracotomy and 3 underwent video-assisted thoracoscopic surgery (VATS). The study cohort comprised 7 male and 13 female patients with an average age of 44 years (range, 4– 71 years). All patients underwent a systematic preoperative examination to confirm the surgical indications and methods. Regular follow-up was conducted after the operation.
Results: All patients survived and remained clinically well. Two of the 20 patients (10%) were re-admitted to the hospital because of pulmonary air leakage, which was resolved after thoracic drainage. No patients developed tumor recurrence.
Conclusion: BSRCPP may be an effective treatment for selected patients with bronchial tumors. Notably, however, many technical key points require improvement, especially in VATS. Therefore, thoracoscopic minimally invasive treatment requires more practice and exploration.
Keywords: sleeve lobectomy, BSRCPP, VATS, thoracotomy
Introduction
As a special type of bronchial sleeve resection, bronchial sleeve resection with complete pulmonary preservation (BSRCPP) retains healthy lung tissue with radical tumor resection. Because of the outstanding curative effect of BSRCPP (minimal invasiveness of treatment and maximal preservation of lung function), this procedure has been applied to the treatment of both benign, indolent bronchial malignancies and bronchial stenosis.1,2 In 2019, we performed 14,465 surgical procedures for the treatment of lung cancer, and our department has become an ultra-high-volume thoracic surgery center. This situation has been reported by our counterparts.3 We reviewed the evolution of BSRCPP in our department during the past 7 years, focusing on the indications for and clinical outcomes of this special surgical technique as well as the feasibility of its application by video-assisted thoracoscopic surgery (VATS).
Patients and Methods
This retrospective analysis was performed at a single institution. The clinical data of 20 patients who underwent BSRCPP during the past 7 years were collected from the medical records. Chest computed tomography and telephone follow-ups were performed every half year in all patients to assess the prognosis and survival. This study was approved by Shanghai Pulmonary Hospital, Tongji University and was performed in accordance with the guidelines of the Helsinki Declaration of 1975, revised in 1983. All participants provided written informed consent. We confirm that a parent or legal guardian of patients under the age of 18 years provided informed consent.
Surgical Techniques
The patients were placed in the lateral decubitus position. After general anesthesia and endotracheal intubation, a posterolateral incision was made at the fourth or fifth intercostal space (ICS). Double-portal VATS involved the placement of one 1-cm camera port at the seventh ICS along the posterior axillary line and performance of one 3-cm utility incision at the fourth ICS along the anterior axillary line. First, we examined whether any adhesion was present in the thoracic cavity, loosened the inferior pulmonary ligament, and performed hilar release with a C-shaped incision in the pericardium at the bottom of the inferior pulmonary vein according to the tension of the anastomosis. The mediastinal pleura was then opened to expose the veins of the upper and lower lobes and the main trunk of the pulmonary artery. With the assistance of intraoperative bronchoscopy, we determined the boundary and scope of the tumor. After freeing the main bronchus and clearing the surrounding lymph nodes, the segments of the trachea containing tumor lesions were circularly resected. Proximal and distal margins of at least 0.5 cm were transected for frozen section examination to confirm a tumor-free status. In patients who underwent thoracotomy, end-to-end bronchial anastomosis was performed using 3–0 Vicryl interrupted sutures. In the three patients who underwent VATS, a running suture was applied using 3–0 Prolene (Figures 1–4). Finally, thoracic flushing was performed after careful hemostasis, and the lungs were pressurized to test for air leakage at the anastomosis site. We usually wrapped the bronchial anastomosis with pericardial fat, pleura, or pedicled intercostal muscles, and two chest tubes were placed for drainage. In Patient 15, because the tumor was located in the right main bronchus and was large in diameter, we performed carina reconstruction during BSRCPP. For sleeve resection of left main bronchus tumor, avoiding obstruction of aortic arch is the main problem to be solved. We fully dissociate the aortic arch and pull it up with a ribbon, leaving room for simple continuous suture, which is the main procedure and the challenging moment. As for the pairing of tracheal membrane and cartilage during the anastomosis, we believe that there is no special point. The most important thing is to ensure that there is no tension during the anastomosis and the bronchus cannot be twisted.
 |
Figure 1 The reconstruction of the left and right main bronchus: end-to-end between distal trachea and left or right distal main bronchus. |
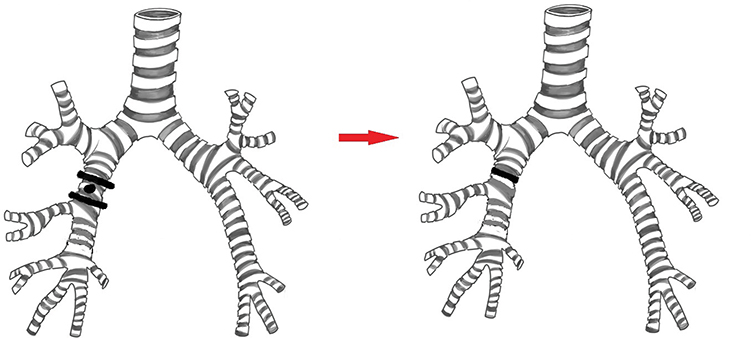 |
Figure 2 The reconstruction of the right bronchus intermedius: end-to-end anastomosis. |
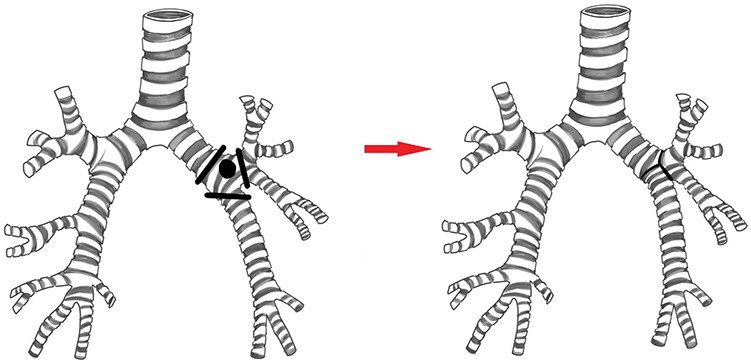 |
Figure 3 The reconstruction of the left bronchial corner: side-to-side between upper lobe and lower lobe bronchus + end-to-end insertion into the proximal left main bronchus. |
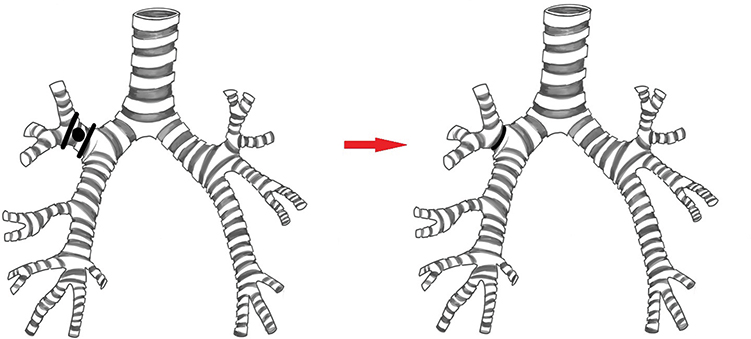 |
Figure 4 The reconstruction of the right upper lobe bronchus: end-to-end anastomosis. |
Results
Baseline Characteristics
The data of 20 patients who underwent BSRCPP from January 2013 to October 2019 were collected from the medical records. In the past 7 years, the total surgical volume in our department was 77,241, and the number of cases in this study accounted for 0.025%. Of these 20 patients, 17 underwent thoracotomy and 3 underwent VATS (Patients 4, 13, and 16). The patients’ mean age was 42.5 ± 16.0 years (range, 4–71 years). Nineteen patients had bronchial neoplasms, and one patient (Patient 5) developed a benign stricture after trauma. Fourteen patients were symptomatic, including cough in 11 patients, dyspnea in 1, fever in 1, and chest pain in 1. The neoplasms in the six asymptomatic patients were found during a routine checkup (Table 1).
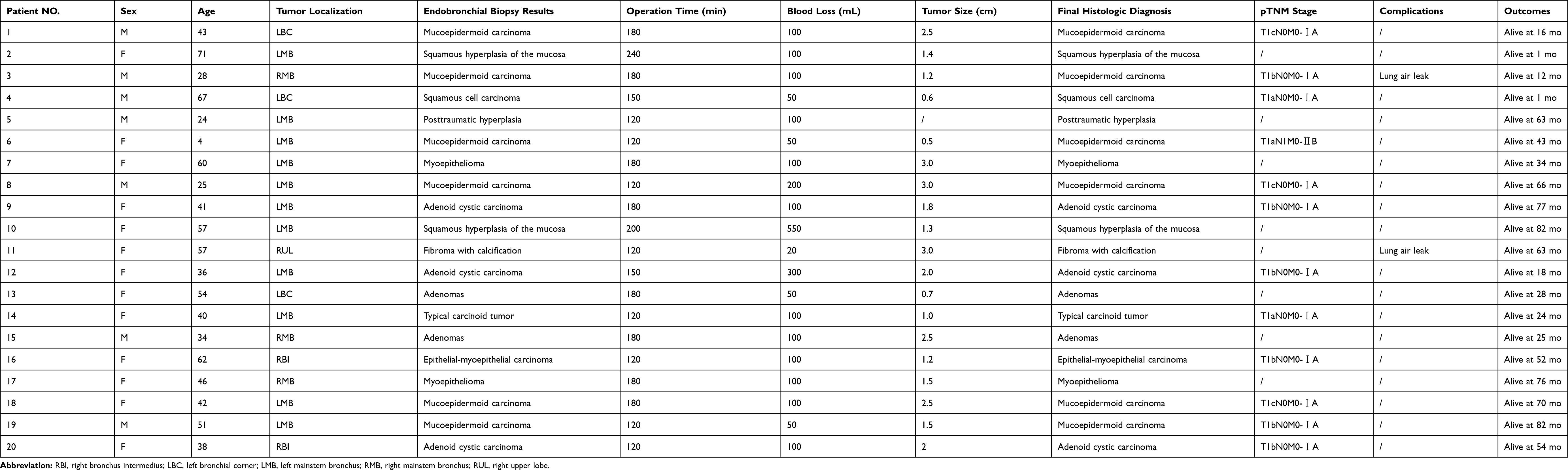 |
Table 1 Characteristics of Patients |
Preoperative Evaluations
Preoperative examinations of all patients included cardiac ultrasonography, pulmonary function tests, bronchoscopy, and chest enhanced computed tomography. Bone scans, brain magnetic resonance imaging, and positron emission tomography scans were performed to rule out metastasis in patients suspected to have malignant tumors. The preoperative evaluations were performed in an effort to confirm the following surgical indications: a benign or low-grade malignant endotracheal lesion with a small implantation base and no hilar or mediastinal lymph node metastasis. Bronchoscopic examination was a mandatory procedure for all patients before surgery because it can display clear airway conditions and is valuable for determining the location of bronchial lesions. Furthermore, a bronchoscopic biopsy was performed to confirm the presence of benign or low-grade malignant lesions. Although the biopsy result of Patient 4 was squamous cell carcinoma, the patient had an endotracheal pedicled tumor with a diameter of only 0.6 cm and a small base. Therefore, we performed BSRCPP under the assistance of VATS. On the first postoperative day, we routinely performed bedside bronchoscopy to observe the bronchial anastomosis and airway sputum accumulation and perform corresponding treatments.
Among the 20 patients who underwent bronchoscopy before surgery, the lung function tests in two patients (Patients 8 and 13) revealed pulmonary ventilation dysfunction, and the tumor occupied the tracheal cavity, leading to atelectasis. These two patients were treated with local ablation with high-frequency electrocoagulation (40 W), temporarily releasing the airway obstruction. After confirmation that the anesthetic cannula can be tolerated, we performed BSRCPP. Both of our patients underwent surgery after 7 days.
No patient died during the surgery, and the median length of hospital stay was 7.7 days (range, 4–21 days). Postoperative complications (pulmonary air leakage) occurred in two patients (Patients 3 and 11), both of whom were cured after thoracic drainage. No patients developed a bronchopleural fistula as confirmed by bronchoscopy. No patients developed atelectasis or anastomotic stenosis. All patients underwent rigorous postoperative computed tomography reviews and were still alive at the time of this writing. The postoperative pathologic examinations confirmed mucoepidermoid carcinoma (n = 6), adenoid cystic carcinoma (n = 3), squamous hyperplasia of the mucosal epithelium (n = 2), leiomyoma (n = 1), fibroid (n = 1), squamous carcinoma (n = 1), basal cell adenoma (n = 1), typical carcinoid (n = 1), pleomorphic adenoma (mixed tumor), epithelial-myoepithelial tumor (n = 1), and borderline tumor (n = 1). The median follow-up time was 44.3 months (range, 1–82 months).
Comment
In 1947, Sir Clement Price Thomas performed the first bronchial sleeve resection for a patient with a right main bronchus adenoma.4 Later, in 1959, Johnson and Jones retrospectively analyzed 98 bronchial sleeve resection procedures that were performed by their team, strongly confirming the feasibility and safety of sleeve lobectomy.5 However, few reports have described bronchial sleeve resection with pulmonary preservation. BSRCPP is used to treat central lung cancer that invades the main bronchus6–8 as well as benign or low-grade malignant bronchial lesions with normal anatomy of the bronchial tree. Surgical indications also include the absence of external bronchial dissemination, the absence of hilar mediastinal lymph node metastasis, and tumors limited to the mainstem bronchus or bronchus intermedius with negative margins.9–11 BSRCPP is especially suitable for elderly patients, patients with poor cardiopulmonary function, and patients who cannot tolerate massive resection. One of our patients had post-traumatic bronchial stenosis, and the remaining patients had bronchial benign or low-grade malignant tumors. With respect to essential surgical techniques, tension-free anastomosis is critical for a successful operation. Division of the inferior pulmonary ligament and peritracheal mobilization are common techniques used during the operation.2,12,13 Hilar release can also be conducted. In the present study, a C-shaped incision was performed in the pericardium at the bottom of the inferior pulmonary vein, which greatly reduced the anastomotic tension.
The main complications of BSRCPP, among which is bronchopleural fistula formation, will deteriorate patients’ quality of life.14–16 A negative resection margin and tension-free anastomosis are the key points for the prevention of a bronchopleural fistula. Postoperative anastomotic stenosis is also a common complication and is usually caused by twisting of the bronchus when the surgeon sutures the cutting edge. In our series, Patients 3 and 11 developed postoperative pulmonary air leakage, and both were discharged after thoracic drainage. No complications, including postoperative atelectasis and pneumonia, occurred in our patients. We performed continuous anastomosis combined with interrupted suturing. Some studies have focused on innovative techniques such as the “continuous suture dividing and equal suture tightening” method and hybrid suturing techniques.17,18
During the past 20 years, video-assisted thoracic bronchial sleeve lobectomy with bronchoplasty has undergone rapid development. This technique was historically considered a technically restricted area. It was not until 2002 that Santambrogio et al successfully performed the first VATS sleeve bronchoplasty for a low-grade mucoepidermoid carcinoma of the left lower lobar bronchus.19 VATS has the following advantages: clearer surgical vision, shared resources, decreased postoperative pain, and a shorter hospital stay.20–26 Our three patients underwent double-portal VATS, which is superior to the conventional tri-portal surgical approach. Double-portal VATS may be a minimally invasive alternative. Additionally, the creation of one utility port at the fourth ICS along the anterior axillary line can avoid interference of the pulmonary artery in the anastomosis.
This study has some limitations. Notably, it was a single-center retrospective study. The number of patients was small and the operation location was not uniform; therefore, it was impossible to design a prospective randomized study. However, increasingly more practical experiences are suggesting that patients’ quality of life is better if they are treated by BSRCPP than by standard resection. There are abundant reports on this technique and its prognosis.14,27–29 In conclusion, BSRCPP is a well-developed technology, but its operation with the assistance of VATS remains stringently demanding to surgeons.30–33
Acknowledgments
This study was supported in part by grants from the National Natural Science Foundation of China (81970092), Artificial Intelligence Research Project of Shanghai Pulmonary Hospital (fk1938). Jiangnan Duan, Haomin Cai, and Wei Huang are co-first authors for this study. The revised manuscript has been polished by Edanz Editing China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Frist WH, Mathisen DJ, Hilgenberg AD, Grillo HC. Bronchial sleeve resection with and without pulmonary resection. J Thorac Cardiovasc Surg. 1987;93(3):350–357. doi:10.1016/S0022-5223(19)36412-8
2. Rendina EA, Venuta F, de Giacomo T, Rossi M, Coloni GF. Parenchymal sparing operations for bronchogenic carcinoma. Surg Clin North Am. 2002;82(3):589–609. doi:10.1016/S0039-6109(02)00021-X
3. Sihoe ADL, Han B, Yang TY, Pan C, Jiang G, Fang VWT. The advent of ultra-high volume thoracic surgical centers in Shanghai. World J Surg. 2017;41(11):2758–2768.
4. Thomas CP. Conservative resection of the bronchial tree. J R Coll Surg Edinb. 1956;1(3):169–186.
5. Johnston JB, Jones PH. The treatment of bronchial carcinoma by lobectomy and sleeve resection of the main bronchus. Thorax. 1959;14(1):48–54. doi:10.1136/thx.14.1.48
6. Okada M, Yamagishi H, Satake S, et al. Survival related to lymph node involvement in lung cancer after sleeve lobectomy compared with pneumonectomy. J Thorac Cardiovasc Surg. 2000;119(4 Pt 1):814–819. doi:10.1016/S0022-5223(00)70018-3
7. Lausberg HF, Graeter TP, Wendler O, Demertzis S, Ukena D, Schafers HJ. Bronchial and bronchovascular sleeve resection for treatment of central lung tumors. Ann Thorac Surg. 2000;70(2):367–371. doi:10.1016/S0003-4975(00)01725-2
8. Yoshino I, Yokoyama H, Yano T, et al. Comparison of the surgical results of lobectomy with bronchoplasty and pneumonectomy for lung cancer. J Surg Oncol. 1997;64(1):32–35. doi:10.1002/(SICI)1096-9098(199701)64:1<32::AID-JSO7>3.0.CO;2-Q
9. Ragusa M, Vannucci J, Cagini L, Daddi N, Pecoriello R, Puma F. Left main bronchus resection and reconstruction. A single institution experience. J Cardiothorac Surg. 2012;7(1):29. doi:10.1186/1749-8090-7-29
10. Bolukbas S, Schirren J. Parenchyma-sparing bronchial sleeve resections in trauma, benign and malign diseases. Thorac Cardiovasc Surg. 2010;58(1):32–37. doi:10.1055/s-0029-1186241
11. Lucchi M, Melfi F, Ribechini A, et al. Sleeve and wedge parenchyma-sparing bronchial resections in low-grade neoplasms of the bronchial airway. J Thorac Cardiovasc Surg. 2007;134(2):373–377. doi:10.1016/j.jtcvs.2007.03.020
12. Xie D, Deng J, Gonzalez-Rivas D, et al. Comparison of video-assisted thoracoscopic surgery with thoracotomy in bronchial sleeve lobectomy for centrally located non-small cell lung cancer. J Thorac Cardiovasc Surg. 2020. doi:10.1016/j.jtcvs.2020.01.105
13. Cerfolio RJ, Deschamps C, Allen MS, Trastek VF, Pairolero PC. Mainstem bronchial sleeve resection with pulmonary preservation. Ann Thorac Surg. 1996;61(5):1458–1462. doi:10.1016/0003-4975(96)00078-1
14. Tronc F, Gregoire J, Rouleau J, Deslauriers J. Long-term results of sleeve lobectomy for lung cancer. Eur J Cardiothorac Surg. 2000;17(5):550–556. doi:10.1016/S1010-7940(00)00405-X
15. Yildizeli B, Fadel E, Mussot S, Fabre D, Chataigner O, Dartevelle PG. Morbidity, mortality, and long-term survival after sleeve lobectomy for non-small cell lung cancer. Eur J Cardio-Thorac. 2007;31(1):95–102. doi:10.1016/j.ejcts.2006.10.031
16. Yavuzer S, Yuksel C, Kutlay H. Segmental bronchial sleeve resection: preserving all lung parenchyma for benign/low-grade neoplasms. Ann Thorac Surg. 2010;89(6):1737–1743. doi:10.1016/j.athoracsur.2010.02.060
17. Li Y, Wang J. Video-assisted thoracoscopic surgery sleeve lobectomy with bronchoplasty: an improved operative technique. Eur J Cardiothorac Surg. 2013;44(6):1108–1112.
18. Zhang Z, Huang Q, Liao Y, Ai B, Huang Q. Application of the “continuous suture dividing and equal suture tightening” method in video-assisted thoracoscopic surgery sleeve lobectomy. J Thorac Dis. 2018;10(9):5199–5207. doi:10.21037/jtd.2018.08.42
19. Santambrogio L, Cioffi U, De Simone M, Rosso L, Ferrero S, Giunta A. Video-assisted sleeve lobectomy for mucoepidermoid carcinoma of the left lower lobar bronchus: a case report. Chest. 2002;121(2):635–636. doi:10.1378/chest.121.2.635
20. Mahtabifard A, Fuller CB, McKenna RJ
21. Loscertales J. Video-assisted thoracic surgery lobectomy: results in lung cancer. J Thorac Dis. 2010;2(1):29–35.
22. Nagahiro I, Andou A, Aoe M, Sano Y, Date H, Shimizu N. Pulmonary function, postoperative pain, and serum cytokine level after lobectomy: a comparison of VATS and conventional procedure. Ann Thorac Surg. 2001;72(2):362–365. doi:10.1016/S0003-4975(01)02804-1
23. Craig SR, Leaver HA, Yap PL, Pugh GC, Walker WS. Acute phase responses following minimal access and conventional thoracic surgery. Eur J Cardiothorac Surg. 2001;20(3):455–463. doi:10.1016/S1010-7940(01)00841-7
24. Tsubokawa N, Harada H, Takenaka C, Misumi K, Yamashita Y. Comparison of postoperative pain after different thoracic surgery approaches as measured by electrical stimulation. Thorac Cardiov Surg. 2015;63(6):519–525. doi:10.1055/s-0035-1546427
25. Ghaly G, Kamel M, Nasar A, et al. Video-assisted thoracoscopic surgery is a safe and effective alternative to thoracotomy for anatomical segmentectomy in patients with clinical stage i non-small cell lung cancer. Ann Thorac Surg. 2016;101(2):465–472. doi:10.1016/j.athoracsur.2015.06.112
26. Shimizu K, Nakazawa S, Nagashima T, Kuwano H, Mogi A. 3D-CT anatomy for VATS segmentectomy. J Vis Surg. 2017;3:88. doi:10.21037/jovs.2017.05.10
27. Terzi A, Lonardoni A, Feil B, Spilimbergo I, Falezza G, Calabro F. Bronchoplastic procedures for central carcinoid tumors: clinical experience. Eur J Cardiothorac Surg. 2004;26(6):1196–1199. doi:10.1016/j.ejcts.2004.08.026
28. Petersen RH, Hansen HJ. Learning thoracoscopic lobectomy. Eur J Cardiothorac Surg. 2010;37(3):516–520. doi:10.1016/j.ejcts.2009.09.012
29. Gaissert HA, Mathisen DJ, Moncure AC, Hilgenberg AD, Grillo HC, Wain JC. Survival and function after sleeve lobectomy for lung cancer. J Thorac Cardiovasc Surg. 1996;111(5):948–953. doi:10.1016/S0022-5223(96)70369-0
30. Ludwig C, Stoelben E, Olschewski M, Hasse J. Comparison of morbidity, 30-day mortality, and long-term survival after pneumonectomy and sleeve lobectomy for non-small cell lung carcinoma. Ann Thorac Surg. 2005;79(3):968–973. doi:10.1016/j.athoracsur.2004.08.062
31. Huang CL, Liu CC, Cheng CY, Lin CH, Wu YC, Wang BY. Learning thoracoscopic lobectomy in resident training. Thorac Cardiovasc Surg. 2014;62(8):690–695.
32. Ferguson J, Walker W. Developing a VATS lobectomy programme–can VATS lobectomy be taught? Eur J Cardiothorac Surg. 2006;29(5):806–809. doi:10.1016/j.ejcts.2006.02.012
33. Nakanishi K. Video-assisted thoracic surgery lobectomy with bronchoplasty for lung cancer: initial experience and techniques. Ann Thorac Surg. 2007;84(1):191–195. doi:10.1016/j.athoracsur.2007.03.008
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.