Back to Journals » Therapeutics and Clinical Risk Management » Volume 19
Bridging the Gap in Traditional PIVC Placement: An Evaluation of Operation STICK Vascular Access Outcomes
Authors Mielke N ![]() , Xing Y, Gibson SM, DiLoreto E, Bahl A
, Xing Y, Gibson SM, DiLoreto E, Bahl A
Received 7 September 2023
Accepted for publication 4 November 2023
Published 21 November 2023 Volume 2023:19 Pages 937—948
DOI https://doi.org/10.2147/TCRM.S435628
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor De Yun Wang
Nicholas Mielke,1 Yuying Xing,2 Steven Matthew Gibson,3 Emily DiLoreto,4 Amit Bahl4
1Department of Medicine, Creighton University School of Medicine, Omaha, NE, USA; 2Corewell Health Research Institute, Royal Oak, MI, USA; 3Vascular Access Consulting, Henderson, KY, USA; 4Department of Emergency Medicine, Corewell Health William Beaumont University Hospital, Royal Oak, MI, USA
Correspondence: Amit Bahl, Department of Emergency Medicine, Corewell Health William Beaumont University Hospital, 3601 13 Mile Road, Royal Oak, MI, 48073, USA, Email [email protected]
Objective: Education and training is core to improving peripheral intravenous access outcomes. This study aimed to show that a vascular access training program (Operation STICK) in the emergency department (ED) improves the outcomes of traditionally placed peripheral intravenous catheters (PIVC).
Methods: This was a pre-post quasi-experimental study of traditionally placed PIVCs at a large ED in southeastern Michigan, United States. A control group (non-OSTICK) was compared to an experimental group (OSTICK) using a 3:1 propensity score matched analysis. Groups were comprised of ED patients with traditional PIVC placements in two separate six-month periods: non-OSTICK PIVCs from April to September 2021 and OSTICK PIVCs (placed by an OSTICK graduate) from October 2022 to March 2023. The primary outcome was PIVC functionality. The secondary outcome was adherence to best practices.
Results: A total of 6512 PIVCs were included in the study; 4884 (75.0%) were in the non-OSTICK group, while 1628 (25.0%) were in the OSTICK group. 68.1% of OSTICK PIVCs and 59.7% of non-OSTICK PIVCs were placed by ED technicians (p < 0.001). 91.3% of OSTICK PIVCs were placed on the first attempt, and 98.5% were placed within two attempts. A subgroup analysis of admitted patients (2540 PIVCs; 553 (21.8%) OSTICK-trained and 1987 (78.2%) non-OSTICK-trained) revealed 87.6% of OSTICK PIVCs and 80.3% of non-OSTICK PIVCs were 20 gauge (p < 0.001). The median proportion of dwell time to hospital length of stay was 94% for OSTICK PIVCs, compared to 88% for non-OSTICK PIVCs (p < 0.001).
Conclusion: This study underscores the value of education and training in enhancing vascular access outcomes. Implementing Operation STICK, a comprehensive vascular access training program, at a large ED has led to high first-stick success, adherence to best practice recommendations for site and device selection, and improved PIVC functionality for traditionally placed catheters.
Keywords: peripheral intravenous catheter, venous access, vascular access score, traditional insertion, operation stick, palpation method
Introduction
Among the 100 million emergency department (ED) visits in the United States annually, an estimated 60% of the patients will require peripheral intravenous catheter (PIVC) placement.1–3 For patients admitted to the hospital for further care, this number approaches nearly 90%.2,4 Given the vast need for this technology in the hospital setting, PIVC placement is the most frequently conducted invasive procedure globally.2,4,5
PIVC placement by threading a plastic cannula over a needle was first introduced nearly 100 years ago.6 Over time, despite some enhancements to this technology, such as safety features, catheter composition, and variety of sizes and lengths,7 PIVC outcomes have remained consistently poor with high complication and failure rates.5 In fact, up to 63% of PIVCs fail prior to the completion of their intended therapy, with complications including phlebitis, infiltration, extravasation, and bloodstream infections being common occurrences.5 While these complications will trigger a simple re-insertion in most cases, some will require more aggressive measures such as intensive care admission or operative intervention.8,9 Ultimately, PIVC shortfalls may also lead to patient care delays and operational inefficiencies characterized by longer hospitalizations.10 Given the vast use of PIVCs and the frequency of complications, there are heavy costs to poor PIVC outcomes, and the economic burden in the United States is conservatively estimated to be $1.5 billion annually.11
Despite best practice guidelines for vascular access being readily available, there is limited compliance with recommendations and a lack of uniformity in PIVC placement among clinicians.12 As this procedure is foundational to delivering most therapies in hospitalized patients, such as medications, fluids, and blood products, strategies must be explored to reduce complications and improve functionality. One critical gap that likely has substantially influenced PIVC outcomes is the paucity of investment in education and training programs in vascular access. Only two-thirds of healthcare institutions reported delivering PIVC education to their staff, according to one survey of 611 institutions.13 This is a common theme as many emergency medical services (EMS) training programs, nursing schools, and hospitals provide very little education and training regarding PIVC insertion, with the predominant method being the “see one, do one, teach one” approach.14
This “accepted but unacceptable” culture5 of PIVC inadequacy led the authors, a multidisciplinary group of clinicians, to create Operation STICK in the Fall of 2021. The aim of this comprehensive program is to overhaul the approach to PIVC insertion, including incorporating best practice guidelines, infection prevention practices, venous assessment methodologies, administrative oversight and surveillance, and best-in-class education and training for both traditional and advanced access techniques. The program includes a self-paced video series, interactive lectures, simulation, and supervised one-on-one training with live patients. Since the program’s inception, over 164 ED technicians, nurses, physicians, and students have participated in the training program. This study aimed to demonstrate the improved PIVC outcomes of traditionally placed PIVCs after implementing a vascular access educational and training program in the ED setting.
Methods
Study Setting
This study was conducted at a large, 1100 beds, tertiary care center located 20 miles (32.2 km) north of Detroit, Michigan, United States. The 160+ bed ED has level one trauma status and serves as the training ground for emergency medicine residents and fellows. These clinicians serve a diverse metropolitan community that encapsulates over two million people.
Operation STICK Overview
ED-based clinicians (nurses, ED technicians, physicians, advanced practice providers, and select medical students) were invited to enhance their PIVC placement skills by participating in additional PIVC training through the Operation STICK program. Participation was optional and not a condition of employment. This program began in October 2021 and has been ongoing. Typically, 6–8 new trainees enroll in the program every month and graduate once they show proficiency in both traditional and ultrasound-guided insertions. This generally takes between 5 and 12 PIVC placements on live patients.
Operation STICK Training Pathway
Operation STICK is a comprehensive PIVC training curriculum that consists of three main components: educational video series, didactic and simulation training, and supervised one-on-one training sessions with live patients. The online, self-paced modules feature interactive videos, quizzes, and case-based learning to establish a foundation for the learner. These modules serve as an introduction to venous access, offering a comprehensive review of assessment strategies with special attention to site, vein, and device selection, infection prevention measures, fundamental and advanced insertion methodologies, relevant equipment and supplies, and necessary documentation protocols. This is followed by a supplemental, in-person lecture and simulation training in a small group environment. During this component, trainees become familiarized with advanced visualization technologies (eg, ultrasound and near-infrared) and practice the mechanics of traditional and ultrasound-guided PIVC placement. Lastly, a specially trained advanced preceptor meets with the trainee individually and assesses their skill level. The advanced preceptor supervises the trainee to place PIVCs on ED patients that require venous access. Each PIVC placement is carefully monitored by the advanced preceptor through an evidence-based checklist that details every component of PIVC insertion. Once the trainee can confidently place the PIVC while meeting all checklist criteria, they are deemed “competent” by the advanced preceptor and may place PIVCs (both traditional and ultrasound-guided techniques) independently. At six months post competency, graduates are required to demonstrate continued proficiency via a competency audit. This audit includes traditional and advanced placements. These audits are then conducted annually.
Operation STICK Vascular Access Score
One of the key goals of the OSTICK program is to standardize the process of the assessment to benefit the masses rather than applauding the outlier who can skillfully establish access in a suboptimal location and poor quality vein. Instead of focusing on the skillset of the individual inserter, this program highlights the needs of the patient by teaching the skills and knowledge to elevate all clinicians to make better choices consistently. The OSTICK program prioritizes patient needs by equipping all clinicians with the necessary skills and knowledge for this approach. To accomplish this, one innovative aspect of OSTICK is the incorporation of an evidence-based venous scoring system,15–17 which the program refers to as the “vascular access score”. For each potential venous target, OSTICK-trained clinicians evaluate the palpability, visibility, and distension of the vein by assigning a score. This scoring system aids clinicians in efficiently assessing the vasculature, helping distinguish between patients suitable for conventional venipuncture and those who may require an escalated approach involving advanced visualization technologies such as ultrasound guidance. As OSTICK training equips clinicians with expertise in both traditional and advanced techniques, they develop the full skillset to effectively address each patient’s individual needs.
Study Design and Participants
Two groups comprised this pre-post quasi-experimental observational study: non-OSTICK and OSTICK. Propensity score matching was implemented to create a non-OSTICK group, where each OSTICK PIVC was matched with three non-OSTICK PIVCs. Both groups consisted of ED patients who >18 years of age that underwent traditional PIVC placement during separate six-month time periods; non-OSTICK PIVCs were placed between April 1st, 2021, and September 30th, 2021 (prior to the inception of Operation STICK), while OSTICK PIVCs were placed between October 1st, 2022, and March 31st, 2023, by a graduate of Operation STICK. The period of time between the two groups serves as a time in which the program could grow and mature. All patient data was collected retrospectively via data queries from the electronic health record (EHR) system. The local institutional review board (IRB) approved the study. A waiver of informed consent was granted by the IRB as the study meets exemption based on design and objectives.
Data Sources/Measurement
The data retrieval process involved querying electronic health records using EPIC (Verona, Wisconsin, USA). Among the collected data, two specific elements, namely the number of attempts and vascular access score, were exclusively reported for the OSTICK group. These variables were not recorded during the non-OSTICK period.
Study Definitions
The comorbidity burden was assessed via the Charlson Comorbidity Index.18 Furthermore, the selection of vesicant and irritant intravenous medications was guided by the standards delineated in the Infusion Nurses Society Standards of Practice.12,19 The term “PIVC dwell time” refers specifically to the interval from PIVC placement to its eventual removal. Concurrently, “hospital length of stay” is defined as the period commencing from the patient’s arrival at the ED to either their discharge from the ED or the hospital entirely. The vascular access score is an evidence-based venous scoring system specifically designed to aid graduates of the OSTICK program in objectively determining an optimal target for PIVC placement.15–17 Lastly, “number of attempts” is a term designated to quantify the instances where a clinician punctures the patient’s skin, with the count including both successful and unsuccessful PIVC placements.
Outcomes and Measurements
The primary outcome was functionality of the PIVC. This was measured as the proportion of dwell time to hospital length of stay. The secondary outcome was adherence to best practices in site and device selection as defined by the Infusion Nursing Society.12 Specifically, the green zone of the forearm is the optimal site and 20 gauge is the best catheter size that reduces complication risk and improves functionality.
Statistical Analysis
Descriptive analysis was conducted to provide an overview of the clinical characteristics. Continuous variables were summarized using means and standard deviations, as well as medians and interquartile ranges. Categorical variables were presented as frequencies and percentages. The Kruskal–Wallis test was used to compare continuous variables between groups, while the Chi-square test was employed for categorical variables.
Propensity score matching was implemented to create a non-OSTICK PIVC group, where each OSTICK PIVC was matched with three non-OSTICK PIVCs. Matching was based on patients’ age, sex, race, and Charlson Comorbidity Index. This approach aimed to establish comparable groups for assessing the impact of the OSTICK program.
Linear mixed-effects regression analysis was utilized to evaluate the effect of the OSTICK program on the proportion of PIVC dwell time to hospital length of stay. The analysis incorporated patients’ age, sex, race, and Charlson Comorbidity Index as fixed effects. Additionally, the propensity score matching grouping factor was included as a random effect to account for any inherent clustering or variability within the matched groups.
The estimated results were reported with corresponding 95% confidence intervals (CIs) and p-values for the linear regression analysis. All statistical tests were two-sided, and statistical significance was determined using a p-value threshold of less than 0.05. The analysis was conducted using R-4.2.1, provided by the R Foundation for Statistical Computing.
Results
A total of 6512 PIVCs met inclusion criteria, of which 4884 (75.0%) were placed by non-OSTICK trained clinicians and 1628 (25.0%) were OSTICK trained. The majority of the population was female (58.4%), the average age was 53.85 years, and 45.1% of the population had a Charlson Comorbidity Index of 0. There was no difference in the use of irritant/vesicant administration between the two groups (all p > 0.05). Regarding PIVC placement location, 39.1% of OSTICK PIVCs were placed in the forearm, compared to 19.9% of non-OSTICK PIVCs (p < 0.001). The most common inserter type was an ED technician in both groups. 68.1% of OSTICK PIVCs were placed by ED technicians, compared to 59.7% of non-OSTICK PIVCs (p < 0.001). First stick success was 91.3% and 98.5% were placed within two attempts of the OSTICK PIVCs (Table 1).
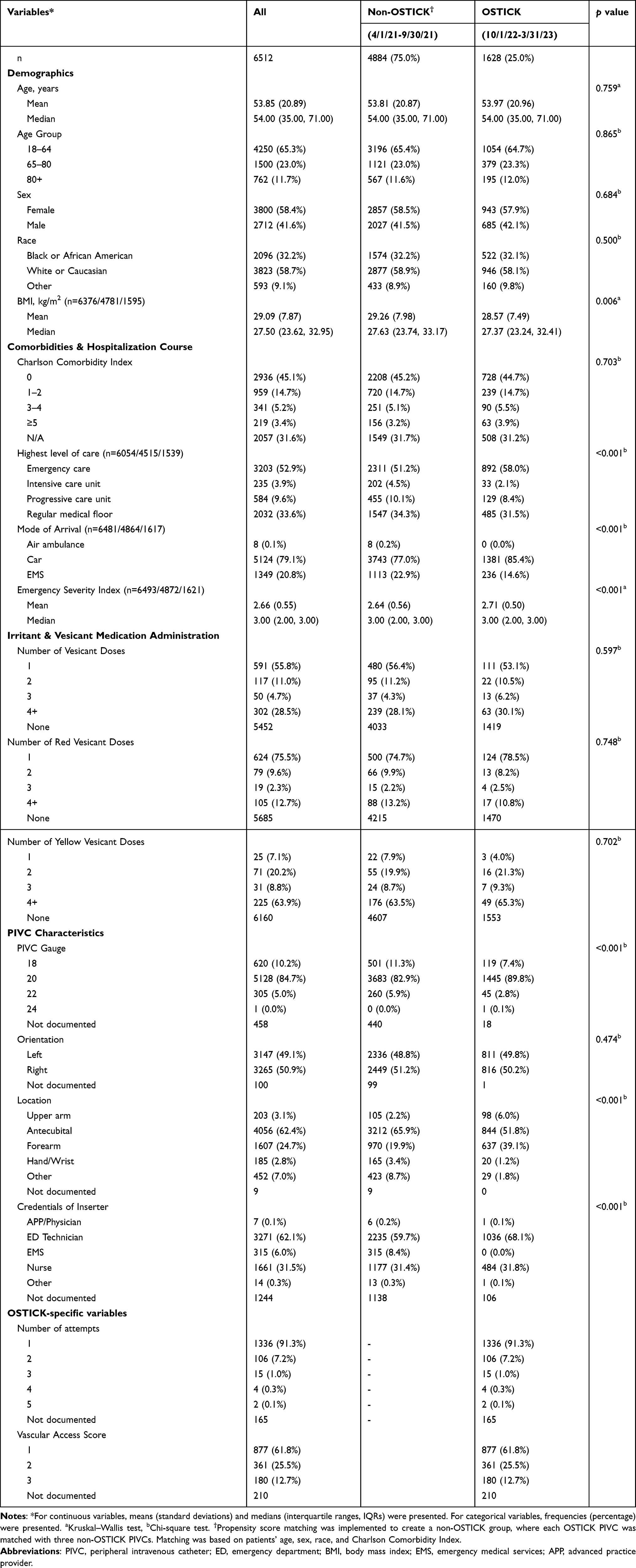 |
Table 1 Demographics, Comorbidities, Hospitalization Course, Medication Administration, PIVC Characteristics, and OSTICK-Specific Variables for All ED Patients with Traditional PIVC Placement |
The subgroup analysis of admitted patients included 2540 PIVCs, with 553 (21.8%) placed by OSTICK-trained and 1987 (78.2%) placed by non-OSTICK-trained clinicians. The average age was 63.52 years and 50.4% were female. 10.7% of the population required intensive care unit (ICU)-level care, while 62.3% remained on the regular medical floor. 87.6% of OSTICK PIVCs were 20 gauge, compared to 80.3% of non-OSTICK PIVCs (p < 0.001). OSTICK PIVCs were predominantly placed in the forearm (46.3%) and antecubital fossa (43.4%), while 59.2% of non-OSTICK PIVCs were placed in the antecubital fossa and 24.6% were in the forearm (p < 0.001). The median proportion of dwell time to hospital length of stay was 94% for OSTICK PIVCs, compared to 88% for non-OSTICK PIVCs (p < 0.001) (Table 2).
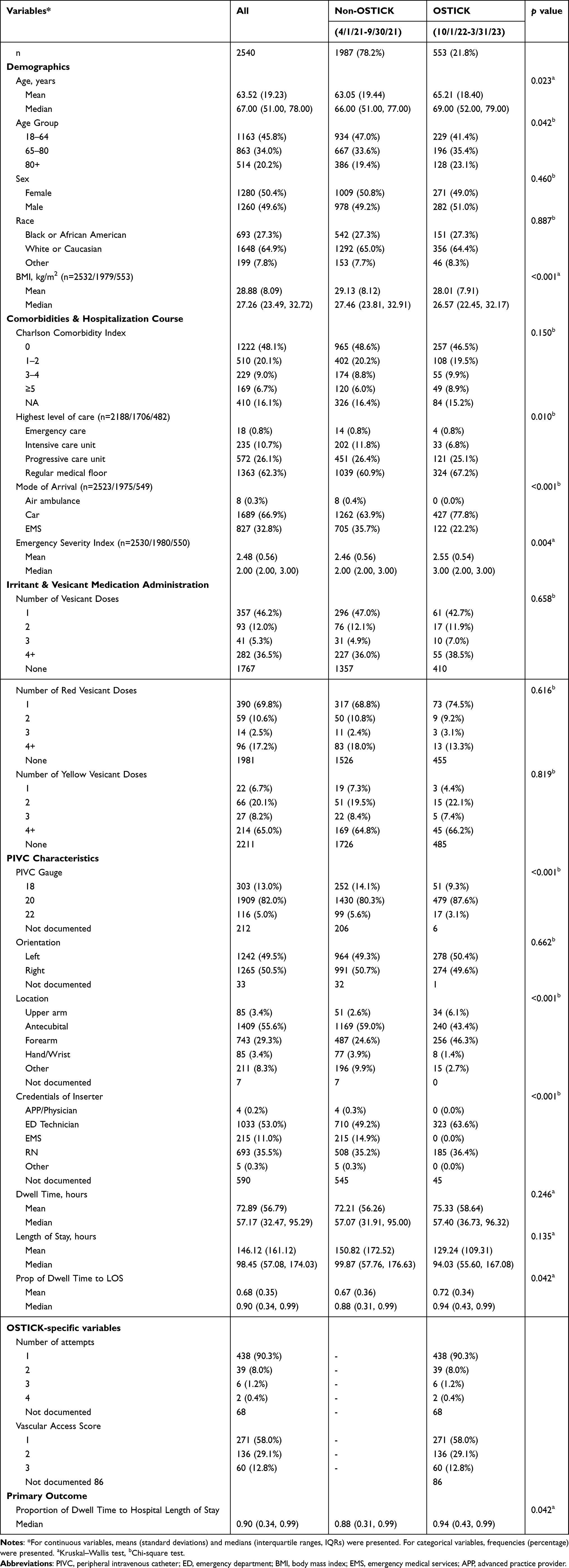 |
Table 2 Demographics, Comorbidities, Hospitalization Course, Medication Administration, PIVC Characteristics, and OSTICK-Specific Variables for Admitted Patients with Traditional PIVC Placement |
The proportion of PIVC dwell time to hospital length of stay was further analyzed via a linear mixed effects regression analysis of the admitted patient subpopulation. When compared PIVCs placed by non-OSTICK clinicians, PIVCs placed by OSTICK clinicians exhibited a statistically significant increase in the proportion of catheter dwell time relative to hospital length of stay, with an estimate of 0.0431 (95% confidence interval (CI): 0.0105, 0.0758; p = 0.0096). An increase in age was associated with an estimate of −0.0013 (95% CI −0.0021, −0.0006; p = 0.0004). The male population, compared to the female population, had an estimate of 0.0526 (95% CI 0.0246, 0.0806; p = 0.0002) (Table 3).
 |
Table 3 Linear-Mixed Effects Regression Analysis of the Proportion of PIVC Dwell Time to Hospital Length of Stay for Admitted Patients |
Discussion
This paper provides an exploration of Operation STICK’s impact on patient vascular access outcomes. After rigorous technical training and gaining knowledge of best practices, OSTICK clinicians followed a standardized method of insertion that led to improved vascular access outcomes. The combination of optimal site of PIVC placement, use of the suitable device, and a proficiently trained OSTICK clinician all enhanced the chances of first stick success and the probability of a functioning, complication-free PIVC throughout its needed duration. In this study, the first stick success rate was 91.3%, and nearly 99% within two attempts by OSTICK-trained clinicians. This stands as a significant achievement among published training programs, aiming to reduce trauma and unnecessary needlesticks in emergency care patients.20 Published evidence illustrates that first-stick success in adults has been reported to be much lower, ranging from 65% to 86%.21,22 While other interventional studies primarily focus on success rates during the insertion phase, most do not demonstrate the impact of initial vascular access care throughout hospitalization.11,23,24 This research suggests that a single PIVC can be achievable for the majority of hospitalized patients, as indicated by the 94% catheter dwell to duration of stay rate. These results are in contrast to other reports in which dwell times for traditionally placed PIVCs are substantially shorter. For instance, in a prospective analysis, only 79% of PIVCs achieved survival at 72 hours post insertion.25 Additionally, across eight prospective randomized controlled studies, the median incidence of PIVC failure was an alarming 43%.5 In contrast, the strong results of this study emphasized the vital importance of proper education and training in shaping frontline ED clinicians to deliver the best vascular access outcomes for patients throughout their hospital stay.
This study illustrated the importance of comprehensive and systematic vasculature assessments prior to venipuncture which is responsible for the high first stick success. The program challenges the conventional standard and culture that allows clinicians two attempts at placement before escalating to advanced visualization technologies.26 Instead, OSTICK uses the objective vascular access scoring system to guide decision-making. Rather than rigidly requiring two placement attempts before considering other options, the OSTICK method incorporates the vascular access score to determine if a site is appropriate to attempt. If no optimal site is present for traditional placement, the scoring system calls for immediate escalation to an ultrasound-guided approach and prevents unnecessary, and likely unsuccessful, punctures. A comprehensive assessment before any needle insertion ensures optimal placement from the beginning, reducing the need for additional needlesticks and mitigating the risk of complications. Additionally, this removes the need for specialty services or other resources, which could lead to delays in care, prolonged ED stays, and higher costs.
Effective and efficient healthcare delivery, which is paramount for patient safety, hinges on proper education and training. Having knowledge of optimal care and its application to patient treatment is critical. Yet, the current state of education around PIVC placement is inadequate, as indicated by the high failure rate of up to 63%.5 This shortfall in PIVC education was highlighted in a survey conducted by Hunter et al, involving over 600 healthcare institutions. The findings showed that 92% of the trained staff had received five hours or less of instruction in PIVC insertion and care management.13
A majority of the inserters relied primarily on on-the-job training with little or no didactic content to provide an in-depth understanding of the core principles. The common approach of “see one, do one, teach one”, where a preceptor demonstrates a procedure before the novice attempts the next insertion, contributes to significant practice variability and less-than-ideal outcomes.27 Instead, OSTICK uses a robust, standardized, and comprehensive education and training curriculum to ensure that clinicians have the knowledge, tools, and skills to treat the vascular access needs of all ED patients.
An important strength of the OSTICK program is that it has trained healthcare providers at all levels, including ED technicians, nurses, medical students, resident and attending physicians, physician assistants, and nurse practitioners. As the ED is plagued with nursing shortages and nearly all ED patients have vascular access needs, strategically shifting some of the vascular access responsibilities to non-nurse ED clinicians can better streamline ED operations in a cost-effective manner. Training ED technicians has proven successful in achieving the desired outcomes while managing resources effectively. In this study, approximately 68% of OSTICK insertions were performed by ED technicians, with a success rate of nearly 99% within two attempts. As they are often the first point of contact for ED patients, ED technicians represent a largely untapped resource. They are fully capable of initiating vascular access in urgent and emergent settings, which can prevent delays in diagnostic and therapeutic interventions. By leveraging this larger pool of potential staff, ED technicians can help mitigate staffing shortages while maintaining a high level of skill.
Limitations
This study has some limitations. Despite being a quasi-experimental investigation, the study design is limited in that randomization was not possible. However, the use of advanced statistics with propensity score matching approach allowed for adjusting of confounders to more precisely compare the interventional (OSTICK) group to a very large “control” (non-OSTICK) group. Another limitation is reliance on the medical record for data. While capturing electronic health data allows for the evaluation of very large datasets, it is limited due to incomplete or missing data. For instance, over half the patients were missing data on removal assessment. Thus, using endpoints of failure or completion of therapy for PIVC functionality was not a robust and appropriate approach. Instead, the authors used a novel measure of dwell time relative to hospital length of stay to report on PIVC functionality. This approach accounts for data that is typically censored in survival analyses and gives a more accurate depiction of functionality. Further, individual inserter data was not captured during the study period. As this was a pre-post study design, it is possible that some of the same individuals inserted PIVCs in both phases of the study introducing a confounder. Also, individual experience data was not collected and this may have influenced the results. However, as nearly 400 clinical staff place PIVCs in our large department, the impact of the individual on influencing the global improvements in outcomes is unlikely. Lastly, it is not possible to show comparative data for some variables, such as the number of attempts or the vascular access score, as these variables were not part of the documentation worksheet prior to the implementation of OSTICK. Thus, comparisons for these elements were limited to the existing published evidence.
Conclusions
This study underscores the critical value of education and training in enhancing vascular access outcomes. Implementing Operation STICK, a comprehensive vascular access training program, at a large ED has led to high first-stick success, adherence to best practice recommendations for site and device selection, and improved PIVC functionality for traditionally placed catheters. Future research on dissemination of the Operation STICK model to other EDs and clinical settings is warranted.
Data Sharing Statement
The data that support the findings of this study are available via a data access agreement. Please contact the corresponding author (AB) for this request.
Ethics Committee Approval
This study was approved by the Corewell Health Institutional Review Board. A waiver of informed consent was granted by the IRB as the study meets exemption based on design and objectives.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
AB, NM, ED, and SMG are founders of the Operation STICK vascular access program and are voting members of Operation STICK, LLC. Additionally, AB has research grant support from B. Braun Medical, Becton-Dickinson, Teleflex, Adhezion, Medline Industries, Moderna, and Access Vascular. AB is a paid consultant for B. Braun Medical, Teleflex, Lineus Medical and Interrad Medical. SMG is a paid consultant for Lineus Medical, Nexus Medical, PICC Excellence, and Fujifilm Sonosite. The authors report no other conflicts of interest in this work.
References
1. FastStats - Emergency Department Visits [Internet]; 2023. Available from: https://www.cdc.gov/nchs/fastats/emergency-department.htm.
2. Alexandrou E, Ray-Barruel G, Carr PJ, et al. International prevalence of the use of peripheral intravenous catheters. J Hosp Med. 2015;10(8):530–533. PMID: 26041384. doi:10.1002/jhm.2389
3. Hawkins T, Greenslade JH, Suna J, et al. Peripheral intravenous cannula insertion and use in the emergency department: an intervention study. Acad Emerg Med. 2018;25(1):26–32. PMID: 29044739. doi:10.1111/acem.13335
4. Alexandrou E, Ray-Barruel G, Carr PJ, et al. Use of short peripheral intravenous catheters: characteristics, management, and outcomes worldwide. J Hosp Med. 2018;13(5):1–7. doi:10.12788/jhm.3039
5. Helm RE, Klausner JD, Klemperer JD, Flint LM, Huang E. Accepted but unacceptable: peripheral IV Catheter failure. J Inf Nur. 2015;38(3):189–203. PMID: 25871866. doi:10.1097/NAN.0000000000000100
6. Southorn PA, Narr BJ. The Massa or Rochester plastic needle. Mayo Clin Proc. 2008;83(10):1165–1167. PMID: 18828978. doi:10.4065/83.10.1165
7. Rivera AM, Strauss KW, Van Zundert A, Mortier E. The history of peripheral intravenous catheters: how little plastic tubes revolutionized medicine. Acta Anaesthesiol Belg. 2005;56(3):271–282.
8. Bahl A, Haddad L, Hoerauf K, Mares A, Alsbrooks K. The clinical and economic burdens of infiltration and extravasation with peripheral intravenous catheters: a contemporary narrative review. Int J Nur Health Care Res. 2023;6(6):1436.
9. Drugeon B, Guenezan J, Pichon M, et al. Incidence, complications and costs of peripheral venous catheter-related bacteraemia: a retrospective, single centre study. J Hosp Infect. 2023;135:67–73. PMID: 36918069. doi:10.1016/j.jhin.2023.02.012
10. Lim S, Gangoli G, Adams E, et al. Increased clinical and economic burden associated with peripheral intravenous catheter–related complications: analysis of a US hospital discharge database. Inquiry. 2019;56:0046958019875562.
11. Keleekai NL, Schuster CA, Murray CL, et al. Improving nurses’ peripheral intravenous catheter insertion knowledge, confidence, and skills using a simulation-based blended learning program: a randomized trial. Simul Healthcare. 2016;11(6):376. PMID: 27504890. doi:10.1097/SIH.0000000000000186
12. Gorski LA, Hadaway L, Hagle ME, et al. Infusion therapy standards of practice. J Inf Nur. 2021;44(1S):S1–S224. PMID: 33394637. doi:10.1097/NAN.0000000000000396
13. Hunter MR, Vandenhouten C, Raynak A, Owens AK, Thompson J. Addressing the silence: a need for peripheral intravenous education in North America. J Assoc Vascul Pub. 2018;23(3):157–165. doi:10.1016/j.java.2018.06.001
14. Vandenhouten CL, Owens AK, Hunter MR, Raynak A. Peripheral intravenous education in north American nursing schools: a call to action. J Nurs Educ. 2020;59(9):493–500. PMID: 32865581. doi:10.3928/01484834-20200817-03
15. van Loon FHJ, van Hooff LWE, de Boer HD, et al. The modified A-DIVA scale as a predictive tool for prospective identification of adult patients at risk of a difficult intravenous access: a multicenter validation study. J Clin Med. 2019;8(2). PMID: 30691137. doi:10.3390/jcm8020144
16. Civetta G, Cortesi S, Mancardi M, et al. EA-DIVA score (Enhanced Adult DIVA score): a new scale to predict difficult preoperative venous cannulation in adult surgical patients. J Vasc Access. 2019;20(3):281–289. PMID: 30324841. doi:10.1177/1129729818804994
17. Van Loon FHJ, Lapm P, Houterman S, Bouwman ARA. Development of the A-DIVA scale: a clinical predictive scale to identify difficult intravenous access in adult patients based on clinical observations. Medicine. 2016;95(16). PMID: 27100437.
18. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 2021;40(5):373–383. PMID: 3558716. doi:10.1016/0021-9681(87)90171-8
19. Gorski LA, Stranz M, Cook LS, et al. Development of an evidence-based list of noncytotoxic vesicant medications and solutions. J Inf Nur. 2017;40(1):26–40. doi:10.1097/NAN.0000000000000202
20. van Loon FHJ, Buise MP, Claassen JJF, Dierick-van Daele ATM. Comparison of ultrasound guidance with palpation and direct visualisation for peripheral vein cannulation in adult patients: a systematic review and meta-analysis. Br J Anaesth. 2023;121(2):358–366. PMID: 30032874. doi:10.1016/j.bja.2018.04.047
21. Carr PJ, Rippey JCR, Cooke ML, et al. Development of a clinical prediction rule to improve peripheral intravenous cannulae first attempt success in the emergency department and reduce post insertion failure rates: the Vascular Access Decisions in the Emergency Room (VADER) study protocol. BMJ Open. 2016;6(2):e009196. PMID: 26868942. doi:10.1136/bmjopen-2015-009196
22. Carr PJ, Rippey JCR, Cooke ML, et al. Factors associated with peripheral intravenous cannulation first-Time insertion success in the emergency department. A multicentre prospective cohort analysis of patient, clinician and product characteristics. BMJ Open. 2019;9(4):e022278. doi:10.1136/bmjopen-2018-022278
23. Archer-Jones A, Sweeny A, Schults JA, et al. Evaluating an ultrasound-guided peripheral intravenous cannulation training program for emergency clinicians: an Australian perspective. Aust Emerg Care. 2020;23(3):151–156. PMID: 31926958. doi:10.1016/j.auec.2019.12.008
24. Hassanein SMA, Tantawi HR, Sadek BN, Hendy A, Awad HA. Impact of structured simulation-based and on-job training program on nurses’ competency in pediatric peripheral intravenous cannulation: children’s hospital experience. Nurse Educ Today. 2021;98:104776.
25. Shokoohi H, Boniface KS, Kulie P, Long A, McCarthy M. The utility and survivorship of peripheral intravenous catheters inserted in the emergency department. Ann Emerg Med. 2019;74(3):381–390. PMID: 30926188. doi:10.1016/j.annemergmed.2019.02.003
26. Schults JA, Calleja P, Slaughter E, et al. Peripheral intravenous catheter insertion and use of ultrasound in patients with difficult intravenous access: Australian patient and practitioner perspectives to inform future implementation strategies. PLoS One. 2022;17(6):e0269788. doi:10.1371/journal.pone.0269788
27. Ayub SM. “See one, do one, teach one”: balancing patient care and surgical training in an emergency trauma department. J Glob Health. 2022;12:03051. PMID: 35787589. doi:10.7189/jogh.12.03051
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.