Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Bridging Nutrition and Dentistry: An Interprofessional Education (IPE) Experience Model
Authors Noorullah K, Oshita SE, McNeil AT, Ijaz A, Iqbal L, Tomar SL ![]() , Smith PD, Bilal S
, Smith PD, Bilal S
Received 16 January 2025
Accepted for publication 14 May 2025
Published 31 May 2025 Volume 2025:18 Pages 3039—3049
DOI https://doi.org/10.2147/JMDH.S514494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Khatija Noorullah,1 Shayna Emily Oshita,2 Amy T McNeil,2 Anum Ijaz,3 Laila Iqbal,1 Scott L Tomar,1 Patrick Dean Smith,1 Sobia Bilal1
1Division of Prevention and Public Health, College of Dentistry, University of Illinois Chicago, Chicago, IL, USA; 2Kinesiology and Nutrition, University of Illinois Chicago, Chicago, IL, USA; 3Division of Epidemiology and Global Health, School of Public Health, University of Illinois at Chicago, Chicago, IL, USA
Correspondence: Sobia Bilal, Division of Prevention and Public Health, College of Dentistry, University of Illinois Chicago, 801 S. Paulina St, Chicago, IL, 60612, USA, Email [email protected]
Purpose: Interprofessional Education (IPE) is essential for fostering collaborative healthcare practices. The purpose of this paper is to share a detailed description of the design, development process, implementation, and planned evaluation of an IPE model connecting Nutrition and Dentistry programs at the University of Illinois Chicago (UIC). The program sought to address educational gaps and enhance collaborative learning among healthcare students.
Methods: This IPE teaching activity was guided by the World Health Organization’s IPE guidelines and the Core Competencies for Interprofessional Collaborative Practice. The process involved the formulation of educational model, preparation of students and implementation of three IPE sessions as a collaborative effort between dental and nutrition faculty. Teaching strategies included small group discussions and case studies to foster inclusive learning. The IPE teaching activity evaluation presented in this article corresponds to traditional pretest-posttest (TPP) design, using a validated IPE tool SPICE-R2. Qualitative reflective feedback was collected to understand the program’s impact on professional confidence and holistic care delivery. Quantitative analysis was conducted using T-test for pre and post SPICE-R2 scores and thematic analysis to analyze the qualitative reflections.
Results: Pre and post SPICE-R2 scores analysis showed significant improvements in overall students’. For the domains of interprofessional teamwork, understanding of roles, and patient care outcomes, high significance was noted. Qualitative feedback highlighted the program’s success in enhancing professional confidence and promoting patient-centered care. Students valued the diverse and dynamic teaching strategies employed. Challenges included space limitations and initial role clarification difficulties.
Conclusion: This IPE model effectively improved students’ perception towards interprofessional collaborative teamwork, roles and patient outcomes. Recommendations for future iterations include expanding the program to multiple institutions, varied learning environments, and long-term assessments to ensure sustained impact. These findings underscore the importance of Interprofessional Education in preparing healthcare professionals for collaborative practice and improving patient care outcomes.
Keywords: interprofessional education, curriculum development, dietary counseling, nutrition, dentistry, undergraduate dental education
Introduction
The oral cavity plays a crucial role in maintaining overall health, functioning as both an entry point and a reflection of systemic well-being. Oral conditions such as periodontal disease, dental caries, and oral infections are increasingly recognized as being interconnected with broader systemic health issues. Studies have consistently demonstrated strong associations between oral health and systemic conditions such as cardiovascular disease, diabetes, respiratory infections, and adverse pregnancy outcomes.1–5 Among these, dental caries remains a significant global public health concern, primarily driven by excessive added sugar consumption.6 Although many diseases, such as dental caries and other diet-related noncommunicable diseases, are preventable, healthcare education remains focused on disease-centered tertiary prevention rather than primary prevention.7 Given that diet is a major contributing factor to these conditions, it is essential to incorporate nutrition education into healthcare curricula to address diet-related ailments and their broader systemic implications.8–13
Nutrition is defined as the intake of food based on the body’s dietary requirements, whereas diet is what an individual eats and drinks.14 Diet plays a direct role in the health of the oral cavity. For instance, diets high in sugar contribute to dental caries, while highly acidic diets can lead to enamel erosion.15 The connection between nutrition and oral health is well-documented, yet the collaboration between dental and nutritional professionals remains limited. This disconnect is concerning given that optimal oral health is heavily dependent on a balanced and nutritious diet, which is essential for lifelong general well-being.3
Interprofessional education (IPE) and interprofessional collaborative practice (ICP) have emerged as essential strategies to bridge the gap between different healthcare professions, including dentistry and nutrition. Institutions such as the World Health Organization (WHO), the Institute of Medicine, and the American Public Health Association strongly advocate for collaborative practice models.16–20 According to the World Health Organization (WHO), these models enable healthcare providers from different disciplines to work together with patients, their families, and the broader community to deliver comprehensive, high-quality care.21 Early exposure to IPE helps learners to grow with an attitude of adaptability and a mindset of collaborative healthcare teamwork and understanding each other’s roles.22 Research indicates that interprofessional care leads to improved patient outcomes, reduced costs, and fewer medical errors.16,23
Incorporating IPE into healthcare curricula, particularly in dentistry and nutrition, is therefore vital for fostering interdisciplinary collaboration that addresses both oral and systemic health issues. By integrating nutrition education into dental training and vice versa, healthcare providers can better address conditions that overlap between these fields. This approach is particularly relevant in the context of non-communicable diseases, where diet plays a major role in disease prevention. Early exposure to IPE can prepare healthcare students to collaborate effectively in their future careers, ensuring a more holistic, patient-centered approach to care. Khan mentioned in a review, although the importance of nutrition education in dental curricula is well established, there are gaps.24
This paper outlines the development, implementation, and evaluation of an innovative IPE model between the nutrition and dentistry programs at the University of Illinois Chicago (UIC). UIC’s IPE mission is “to create transformational change in health professions education and healthcare service delivery by delivering evidence-based learning; experiences that build collaborative competence and foster interprofessional scholarship and collaborative practice across academic programs, clinical services and community partners with focused attention to the pressing needs of underserved individuals and populations”.25 The IPE activity discussed in this paper is rooted in the World Health Organization’s (WHO) Framework for Action on Interprofessional Education & Collaborative Practice, and the Core Competencies for Interprofessional Collaborative Practice.21,26 These frameworks guide the development of a “collaboration-ready” healthcare workforce by promoting early exposure to IPE for students, which is essential for translating interprofessional learning into practice. The initiative aims to bridge the gap between the two disciplines by fostering collaboration, promoting a deep understanding of respective roles and responsibilities, and preparing students to engage in comprehensive, interdisciplinary care.
Methods
This IPE methodology involved the following key phases: first, the preparation of an educational model, followed by the preparation of students, the implementation of sessions based on the designed model and student’s perception evaluation. These details are comprehensively outlined in this section. Additionally, this project was deemed “Not Human Research” by the Office for the Protection of Research Subjects at University of Illinois Chicago (Submission ID: STUDY2024-1504) because it involved secondary analysis of de-identified data. Students completed the pre/post course evaluation survey and qualitative reflections as part of the evaluation process. Students were told verbally that the IPE activity will be used for sharing on the web. This protocol complies with the Declaration of Helsinki. The IPE teaching activity evaluation presented in this article corresponds to traditional pretest-posttest (TPP) design.
Development and Design of the Educational Model
The creation of this program was based on core principles of IPE, leveraging the established rapport between the College of Dentistry and the Department of Kinesiology and Nutrition. Faculty from both departments collaborated to design an educational experience aimed at enhancing students’ understanding of nutrition’s role in oral health. This process involved five key elements: commitment, faculty engagement, IPE design, support, and delivery. A consistent leadership approach was essential to breaking down professional silos and fostering a collaborative learning environment.27
Although the physical separation between the two disciplines remains, this activity ensured that evidence-based nutrition practices were integrated into dental education and vice versa. Nutrition students had the opportunity to educate dental students on the fundamentals of providing basic nutrition advice to patients.28 In turn, dental students gained the confidence to offer accurate and helpful nutrition information related to oral health.29 This exchange laid a strong foundation for the students’ professional growth and understanding.30
By introducing both professions early in their education, the program aimed to foster trust and collaboration. Dentistry and nutrition students not only developed their educational skills by sharing knowledge about their respective fields but also explored the intersection of their values. They learned how to collaborate in devising care plans and establishing communication strategies for their future practices. The development of these practical skills, rooted in foundational knowledge and enhanced through communication, proved vital for their professional growth. Enhancing the nutritional status of vulnerable populations is closely linked to oral health, and addressing these issues together can help prevent both medical and dental complications, reducing the need for costly interventions.31
By fostering collaboration between the fields of dentistry and nutrition, our IPE initiative aims to prevent and manage diseases more effectively, ultimately reducing complications in patient care. Grounded in the World Health Organization’s (WHO) Framework for Action on Interprofessional Education & Collaborative Practice and the Core Competencies for Interprofessional Collaborative Practice, the program was designed to cultivate a “collaboration-ready” workforce. Students from both disciplines participated in three collaborative projects, allowing them to apply their knowledge in real-world scenarios while building essential teamwork skills.32 This early exposure to interdisciplinary cooperation strengthens lifelong professional connections and enhances the likelihood of future referrals and collaboration in their respective practices, preparing them to deliver patient-centered care.33,34
The collaboration began in 2018 as standalone interprofessional experiences for second-year students in their respective programs. These experiences continued for two years until the COVID-19 pandemic disrupted the program. Despite the challenges, smaller-scale collaborative projects persisted throughout the pandemic. In 2022, the interprofessional student experience was revitalized, and full integration resumed. Over the course of six months, faculty teams from both programs designed the IPE model, selecting a cohort of approximately 130 students, defining learning outcomes, developing evidence-based content, determining the number of sessions, and planning logistics.
Students were included based on course registration in the Year 1, Dentistry DOAB 312 and HN 306 Nutrition Education. The Nutrition program integrated the IPE model into its Nutrition Education course, while the Dentistry program received approval from the College’s Curriculum Committee to incorporate the activity into its curriculum. The IPE sessions were aligned with UIC’s Core Course-Foundations of Interprofessional Collaborative Practice (FICP), a course aimed at early learners in UIC’s health science programs. The primary objective of the program was to give students a foundational understanding of interprofessional collaborative practice early in their health professions education.
Students were excluded if they could not attend the dates of the joint sessions. Students in both courses had the knowledge and experiences required to adequately prepare them for the interprofessional education session. All the students involved in the teaching and learning activity were included in the evaluation process as part of the activity. A total of 90 students participated in the first IPE session and completed the pre-test, with 54 (60%) dental students and 36 (40%) nutrition students. For the final and 3rd IPE session, 79 students completed the post-test, comprising 52 (66%) dental students and 27 (34%) nutrition students.
Preparation of Students
Nutrition students were introduced to the IPE experience on the first day of their Nutrition Education course, where the focus was on patient outcomes and understanding the roles of other healthcare providers, including the importance of cultural sensitivity in care. Dental students, on the other hand, attended a three-hour introductory session that covered the basics of nutrition, the relationship between oral health and diet, social determinants of health, and the significance of collaboration with registered dietitians.
The program was thoroughly explained to all students to ensure they had ample time to understand its objectives and expectations. The group model catered to different learning styles, allowing students to engage in ways that suited them best. Outgoing students often took on speaking roles, while more reserved students contributed by assisting with research. The program fostered an inclusive and judgment-free environment where students felt safe expressing their ideas.
The activities encouraged students to gain insights into each other’s backgrounds, current perspectives, and future career aspirations. In addition to focusing on their own professions, students were asked to consider the individuals and communities they serve. They explored the foods and traditions of various cultures, educating both themselves and each other on their discoveries. This reflection was aimed at equipping students to provide patient-centered, culturally sensitive care. By working together, students not only strengthened their support networks within their professional groups but also forged new interprofessional connections that will benefit them in their future practices.
Interprofessional Education Sessions
This activity focused on educating healthcare professionals to better serve their patients through interprofessional collaboration. The program included three sessions, each centered around key areas: roles and responsibilities, cultural sensitivity, and clinical case work, which are mostly core aspects of any healthcare profession. The exercises were designed to be versatile, making them applicable to non-clinical areas as well. For example, the model could be adapted to a business setting by focusing on client relationships and using a company project as a case study.
Group sizes ranged from 10 to 97 students, and the program structure was flexible enough to alternate between large and small groups as needed. The model’s scalability makes it easily adaptable to groups of varying sizes and applicable to other health professions. By embedding these experiences into the curriculum, we have created a sustainable model that can be replicated. If time or resources are limited, each of the sessions could be used as standalone workshops integrated into different courses. Additionally, these core sessions can be expanded to advance content over time, creating a model that supports professional development throughout the entirety of a curriculum. While in-person sessions were preferred, the model could also be transitioned to an online format with minimal adjustments, adding further flexibility.
The IPE sessions, held at the College of Dentistry, were three hours long, providing ample space to accommodate different group sizes. Figure 1 provides the flowchart of the three sessions and their objectives. The sessions included:
 |
Figure 1 Flowchart of Interprofessional Education Sessions. |
Session 1: Faculty from each discipline introduced the nutrition and dental programs, outlining their curricula, scope of practice, and patient populations. The session covered the importance of IPE, defined roles and responsibilities, discussed potential barriers, and emphasized effective communication. Students then participated in a breakout activity, creating concept maps to demonstrate how the two professions intersect.
Session 2: This session focused on cultural sensitivity, with an emphasis on understanding diverse food habits to provide culturally sensitive oral health-related nutrition recommendations. Nutrition students educated dental students on USDA (United States Department of Agriculture) MyPlate and cultural humility, while dental students taught about Stephan’s Curve and the effects of cariogenic and cariostatic foods. The breakout activity involved researching a country’s food culture, which students then presented.
Session 3: Students used case studies with student actors simulating patients presenting with oral health and nutrition concerns. The case studies incorporated elements of social determinants of health. Students worked together to interview the patient, develop comprehensive care plans, and present their findings to the class.
Evaluation
Evaluation of the IPE Experience
The effectiveness of the IPE experience was assessed through pre- and post-surveys using the validated SPICE-R2 tool, as it corresponds with the objectives of this IPE activity. The tool was developed and validated by Zorek et al in 2016.35 Validity and reliability of the tool has been previously established in several studies and is generalizable to all health-care professional students.35–37 This tool consists of 10 items that assess IPE perceptions under the subdomains of interprofessional teamwork and team-based practice (3 items), roles and responsibilities for collaborative practice (4 items), and patient outcomes (3 items). The tool is used to assess pre and post changes of student perceptions related to IPE. The responses were collected using the recommended Likert scale of one to five. A score of 1 indicated “Strongly Disagree”, 2 indicated “Disagree”, 3 indicated “Neutral”, 4 indicated “Agree”, and 5 indicated “Strongly Agree”.
The electronic surveys were self-administered using Qualtrics© software. QR code and survey link were shared with all participants during the first face-to-face session to capture the pre-test responses and later after the session three to capture the post-test responses. In addition to the quantitative data from the surveys, students provided qualitative feedback in the form of reflective experiences. At the end of the three sessions, students were asked to complete and submit their reflective questions via their learning management system. The qualitative reflective questions included: How effective did you feel after attending the IPE sessions? If you were doing these sessions again, what would you do differently? What did you learn from this experience? This combination of feedback methods, alongside the session projects, demonstrated the success of the IPE experience in meeting its objectives and fulfilling expectations.
Data Analysis
Data was analyzed using SPSS 28.0 software for descriptive and inferential statistical analysis.
T-test was used to assess the differences in overall mean scores between pre and post for the sample using the SPICE-R2 measure. Statistics were considered significant at the p <0.05.
In addition to the quantitative data, student feedback was gathered through reflections and informal communications. Faculty debriefed after each session, using the feedback to refine and adjust future sessions. The reflections highlighted an increased awareness of interprofessional collaboration and the vital connection between nutrition and dentistry in providing comprehensive patient care. Qualitative responses were analyzed thematically.
Results
Student Quantitative Pre-Post Evaluation
The comparison between pre and post-SPICE-R2 scores and sub-scores of all the participating student groups are provided in Table 1 and Figure 2. Highly significant improvement in overall SPICE-R2 scores between the pre- and post-surveys was noted (p < 0.001; 95% CI – 6.65, − 3.23) indicating that this IPE experience successfully enhanced students’ understanding and appreciation of interprofessional collaboration. Significant improvements were also observed in the sub-scales for Interprofessional Teamwork and Team-Based Practice (T) (p < 0.001; 95% CI – 2.45, − 0.89), Roles/Responsibilities for Collaborative Practice (R) (p < 0.001; 95% CI – 2.58, − 1.39) and Patient Outcomes from Collaborative Practice (O) (p < 0.001; 95% CI – 1.84, − 0.71).
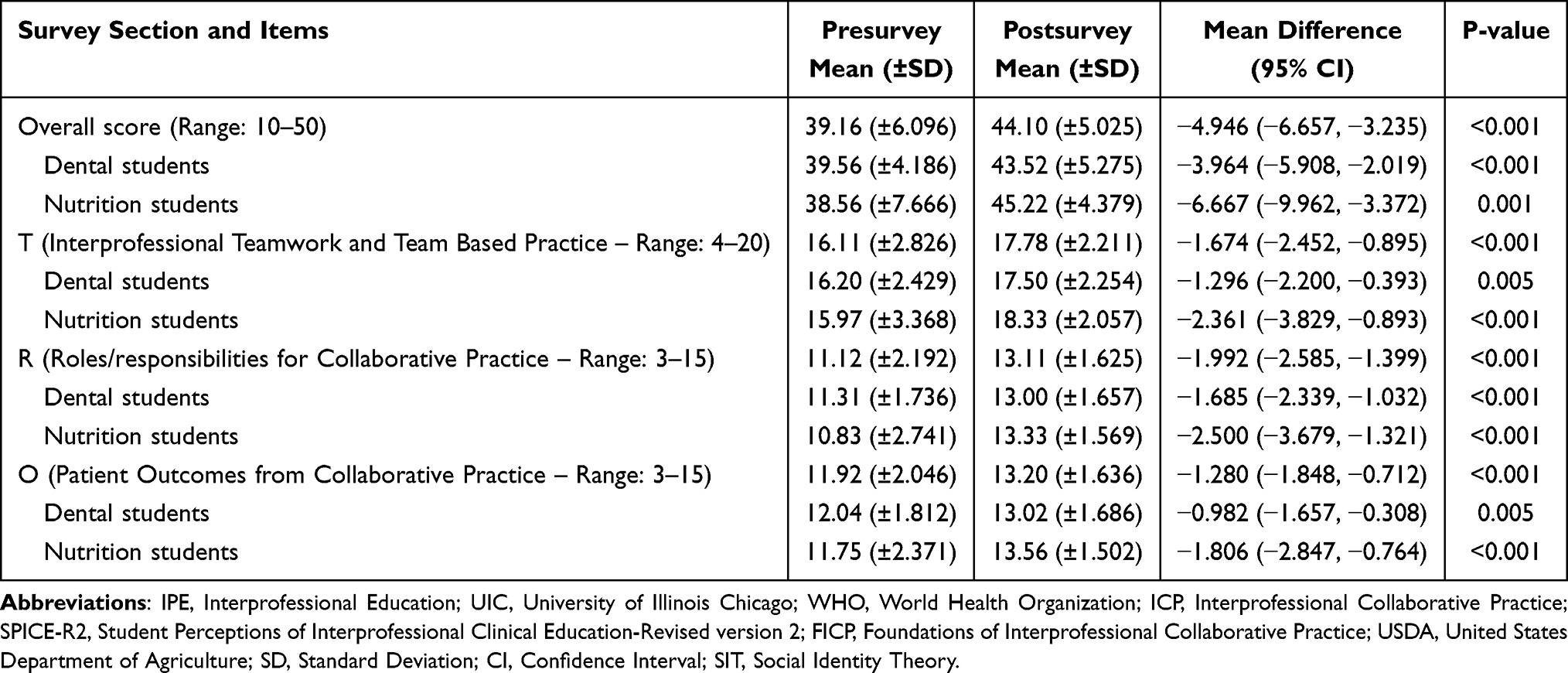 |
Table 1 Comparison of Pre- and Post-Interprofessional Education (IPE) SPICE-R2 Scores Among Dental and Nutrition Students |
 |
Figure 2 Overall SPICE-R2 scores pre- and post-intervention for both dental and nutrition students. |
Student Qualitative Reflective Feedback
Student reflections and informal communications underscored the value and effectiveness of the IPE sessions. Common themes that emerged included a deeper recognition of the importance of interprofessional collaboration, a better understanding of each other’s profession’s roles, and the significant impact of such collaboration on patient-centered care as shown in Figure 3. The following few selected quotes illustrate the students’ perspectives:
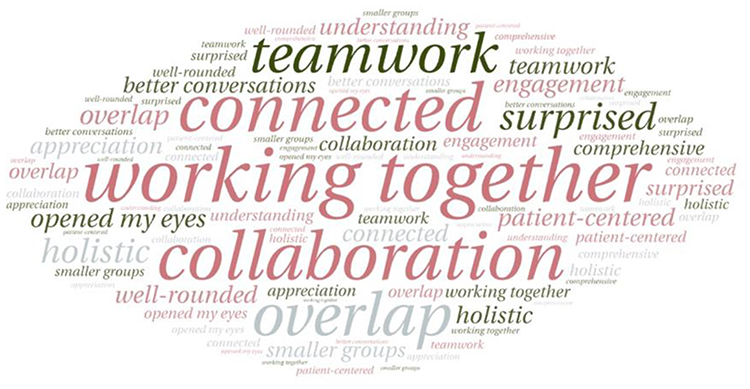 |
Figure 3 Key themes from students’ qualitative reflections. |
Nutrition Students
- “I learned that we are all working together with the goal of helping our patients and communities”.
- “This session opened my eyes to how much we can and should work together because our main goal is the patient”.
- “I was very surprised by how connected dentistry and nutrition are”.
Dental Students
- “I felt that I was very effective and learned a lot about how dentistry overlaps with nutrition”.
- “I would recommend more sessions with smaller groups to facilitate better conversations”.
- “The experience made me appreciate the importance of well-rounded, patient-centered care”.
Discussion
The integration of IPE into healthcare curricula is pivotal for improving collaborative practices and patient outcomes. This study demonstrated that an IPE model focused on interdisciplinary collaboration between Year 1 dental and nutrition students at the UIC significantly enhanced students’ perceptions by improvement in overall SPICE-R2 scores for both dental and nutrition students. This indicates that both the healthcare professional students benefited from this IPE activity. These findings are consistent with prior research indicating that early exposure to IPE can improve healthcare providers’ attitudes and perceptions towards collaborative mindset and in fostering future abilities to deliver comprehensive care and reduce medical errors.38–41
The results also indicate that this IPE learning activity significantly improved the dental and nutrition students’ attitudes across all three SPICE-R2 subdomains of interprofessional teamwork, roles and responsibilities, and patient-centered care. Previous studies are consistent with these findings, with improved scores after attending IPE course.42–44 The findings of this study suggest that early introduction of IPE learning experience in curriculum should be considered by healthcare institutions.
Tajfel and Turner in 1979 proposed Social Identity Theory (SIT),45 suggesting that people gain a part of their self-impression from their affiliation in social groups. Introducing IPE earlier in the healthcare curriculum supports students to identify their roles and responsibilities.46 The IPE activity in this study provided students identity reflection experience during case-based session, where through interdisciplinary discussion they created comprehensive patient care plan. This experience in line with SIT reflected in the findings with the highest improvement in scores seen for SPICE R2-Roles subdomain. This finding aligns with previous studies indicating that health profession students developed a deeper understanding of other healthcare professions roles and a superior gratitude for the contributions of various professionals after participating in an IPE learning activity.46–48 A core element identified in our analysis was the influence of the learning environment on fostering effective collaboration. Students benefitted most when small group settings facilitated open communication and a comfortable atmosphere, similar to earlier studies.49,50 Activities such as icebreakers at the beginning of each session helped set a positive tone, making students more comfortable and receptive to collaboration. Structured seating arrangements were also crucial, as they prevented students from grouping by discipline out of familiarity and encouraged cross-disciplinary interaction, enhancing communication and group dynamics. These strategies have been shown to improve teamwork and collaboration in other healthcare settings as well.41,51,52
Despite the overall success, challenges persisted, particularly in students’ confidence to articulate their professional roles. This issue is common in healthcare settings, as research shows that both students and professionals often struggle to clearly explain their scope of practice, which can hinder effective teamwork.39,53–55 To address this, we recommend incorporating role-playing exercises and interactive sessions, which emphasize the unique expertise of each profession. This approach has proven effective in promoting understanding and confidence among students.56–60 Additionally, using digital platforms to share collaborative work, such as case discussions or role-play outcomes, could enhance the learning experience and facilitate better feedback.
Another recommendation for improvement is to diversify the physical learning environments. Although most sessions were held in the College of Dentistry due to space limitations, providing opportunities for dental students to experience the nutrition students’ classrooms could bridge the interdisciplinary gap. This aligns with findings from other IPE studies, which suggest that varying learning environments help students better understand the contexts in which their colleagues operate.61,62 Furthermore, engaging students in these diverse settings could also highlight the unique challenges and resources of different disciplines, enhancing empathy and collaboration.
Scheduling and flexibility also emerged as critical factors. We found that integrating IPE sessions into the curriculum, rather than offering them as extracurricular activities, significantly boosted student participation and engagement. When IPE sessions were scheduled during class hours or listed in the course description, attendance and commitment were notably higher, minimizing absences and ensuring greater consistency in learning. This observation aligns with studies indicating that students engage more meaningfully in IPE when it is embedded into required coursework.50,63,64
Overall, this study underscores the positive impact of IPE on fostering collaborative practices between dental and nutrition students. However, to maximize its effectiveness, improvements in role clarification, group dynamics, and learning environments are necessary. Subsequent adaptations of this IPE model should place greater emphasis on role clarification exercises, flexible group arrangements, and the use of diverse educational settings. By refining these elements, IPE programs can better prepare healthcare students to meet the demands of patient-centered care with confidence and cohesion.
Conclusion
This study demonstrates the significant positive impact of an innovative IPE model, developed, implemented and evaluated between the Nutrition and Dentistry programs at the UIC, on students’ perceptions of teamwork, roles, responsibilities, and patient-centered care. The substantial improvements in SPICE-R2 scores and the reflective feedback from participants highlight the effectiveness of this comprehensive, collaborative interprofessional approach. By integrating a structured IPE experience into the curriculum, students were better equipped to engage in meaningful, interdisciplinary collaboration, which is essential for delivering holistic and effective patient care. Further studies are recommended using the SPICE-R2 measure with paired samples.
Despite these successes, the findings also reveal areas for improvement. Enhancing role clarification, diversifying group dynamics, and utilizing various learning environments can further elevate the impact of IPE. Addressing these elements will not only increase student confidence but also foster a deeper understanding of interprofessional collaboration. Additionally, flexible scheduling and embedding IPE within mandatory coursework were critical factors in maximizing student engagement.
Moving forward, future iterations of this model should address its limitations, such as the need for long-term follow-up assessments and expansion to multiple institutions to increase generalizability. Continued adaptation and refinement of IPE programs are vital to prepare healthcare students for the collaborative demands of their professions, ensuring they can deliver high-quality, patient-centered care. The findings contribute to the growing body of evidence supporting IPE as a transformative approach in healthcare education and advocate for its broader implementation across various disciplines.
Ethical Statement
This project was deemed “Not Human Research” by the Office for the Protection of Research Subjects at University of Illinois Chicago (Submission ID: STUDY2024-1504) because it involved secondary analysis of de-identified data. IRB review was therefore not required. All procedures followed the Declaration of Helsinki to protect privacy and confidentiality. In line with the determination letter, any publication or presentation should not describe the activity as “human research” or imply IRB approval.
Disclosure
Ms Shayna Oshita reports personal fees from Pearson Education Company, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Meurman JH, Bascones-Martinez A. Oral infections and systemic health - more than just links to cardiovascular diseases. Oral Health Prev Dent. 2021;19:441–448. doi:10.3290/j.ohpd.b1993965
2. Herrera D, Sanz M, Shapira L, et al. Association between periodontal diseases and cardiovascular diseases, diabetes and respiratory diseases: consensus report of the Joint Workshop by the European Federation of Periodontology (EFP) and the European arm of the World Organization of Family Doctors (WONCA Europe). J Clin Periodontol. 2023;50(6):819–841. doi:10.1111/jcpe.13807
3. Bui FQ, Almeida-da-Silva CLC, Huynh B, et al. Association between periodontal pathogens and systemic disease. Biomed J. 2019;42(1):27–35. doi:10.1016/j.bj.2018.12.001
4. Amar S, Han X. The impact of periodontal infection on systemic diseases. Med Sci Monit. 2003;9(12):RA291–RA299.
5. Nascimento GG, Balan P, Alves-Costa S, Bitencourt FV, Kalhan AC, Leite FRM. Oral and systemic health in Singapore: revisiting the past to define the future. Oral Epidemiol. 2024;52(3):353–363. doi:10.1111/cdoe.12913
6. Sheiham A, James WP. Diet and dental caries: the pivotal role of free sugars reemphasized. J Dent Res. 2015;94(10):1341–1347. doi:10.1177/0022034515590377
7. watt RG, Daly B, Allison P, et al. Ending the neglect of global oral health: time for radical action. Lancet. 2019;394(10194):261–272. doi:10.1016/S0140-6736(19)31133-X
8. Touger-Decker R, Mobley C. Academy of nutrition and dietetics. Position of the academy of nutrition and dietetics: oral health and nutrition. J Acad Nutr Diet. 2013;113(5):693–701. doi:10.1016/j.jand.2013.03.001
9. Kris-Etherton PM, Akabas SR, Bales CW, et al. The need to advance nutrition education in the training of health care professionals and recommended research to evaluate implementation and effectiveness. Am J Clin Nutr. 2014;99(5 Suppl):1153S–66S. doi:10.3945/ajcn.113.073502
10. Moynihan P, Makino Y, Petersen PE, Ogawa H. Implications of WHO guideline on sugars for dental health professionals. Oral Epidemiol. 2018;46(1):1–7. doi:10.1111/cdoe.12353
11. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. 2000;894:i–253.
12. World Health Organization (WHO). Diet, nutrition and the prevention of chronic diseases: report of a joint WHO/FAO expert consultation. Geneva, Switzerland: World Health Organization; 2003. WHO Technical Report Series, No. 916.
13. Glick M, Williams DM. FDI vision 2030: delivering optimal oral health for all. Int Dent J. 2021;71(1):3–4. doi:10.1016/j.identj.2020.12.026
14. World Health Organization. Nutrition. Updated December 18, 2024. Available from: https://www.who.int/health-topics/nutrition#tab=tab_1.
15. Allston A. Improving women’s health and perinatal outcomes: the impact of oral diseases. Women’s and Children’s Health Policy Center, Bloomberg School of Public Health, Johns Hopkins University; February 2002. Available from: http://www.med.jhu.edu/wchpc.
16. Buring SM, Bhushan A, Broeseker A, et al. Interprofessional education: definitions, student competencies, and guidelines for implementation. Am J Pharm Educ. 2009;73(4):59. doi:10.5688/aj730459
17. Barr H, Koppel I, Reeves S, Hammick M, Freeth D. Effective Interprofessional Education: Argument, Assumption and Evidence. Oxford: Blackwell Publishing Ltd;; 2005; doi:10.1002/9780470776445
18. Brashers VL, Curry CE, Harper DC, et al. Interprofessional health care education: recommendations of the national academies of practice expert panel on health care in the 21st century. Issues Interdisciplinary Care. 2001;3(1):21–31.
19. Freeth D, Hammick M, Reeves S, Koppel I, Barr H. Effective Interprofessional Education: Development, Delivery and Evaluation. Oxford: Blackwell Publishing Ltd; 2005; doi:10.1002/9780470776438
20. Agency for Healthcare Research and Quality. TeamSTEPPS®: strategies and tools to enhance performance and patient safety. Agency for Healthcare Research and Quality. Available from: https://www.ahrq.gov/teamstepps-program/index.html.
21. World Health Organization. Framework for action on interprofessional education and collaborative practice. World Health Organization. Available from: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice.
22. Harden RM. Interprofessional education: the magical mystery tour now less of a mystery. Anat Sci Educ. 2015;8:291–295. doi:10.1002/ase.1552
23. O’Neill B, Wyness MA. Learning about interprofessional education: student voices. J Interprof Care. 2004;18(2):198–200. doi:10.1080/13561820410001686954
24. Khan SY, Holt K, Tinanoff N. Nutrition education for oral health professionals: a must, yet still neglected. J Dent Educ. 2017;81(1):3–4. [PMID: 28049671]. doi:10.1002/j.0022-0337.2017.81.1.tb06240.x
25. UIC Center for Interprofessional Practice and Education (CAIPER). CAIPER strategic plan. University of Illinois Chicago. https://caipper.uic.edu/.
26. Interprofessional Education Collaborative. Core Competencies for Interprofessional Collaborative Practice: 2016 Update. Washington, DC: Interprofessional Education Collaborative; 2016.
27. Wong PS, Chen YS, Saw PS. Influencing factors and processes of interprofessional professional education (IPE) implementation. Med Teach. 2021;43(sup1):S39–S45. doi:10.1080/0142159X.2019.1672864
28. Hark LA, Deen D. Position of the academy of nutrition and dietetics: interprofessional education in nutrition as an essential component of medical education. J Acad Nutr Diet. 2017;117(7):1104–1113. doi:10.1016/j.jand.2017.04.019
29. Smith PD, Noorullah K, Iqbal L, Tomar SL. Dental students’ comfort discussing nutrition and obesity prevention with parents and caregivers. J Dent Educ. 2021;85(6):828–834. doi:10.1002/jdd.12575
30. DiMaria-Ghalili RA, Mirtallo JM, Tobin BW, Hark L, Van Horn L, Palmer CA. Challenges and opportunities for nutrition education and training in the health care professions: intraprofessional and interprofessional call to action. Am J Clin Nutr. 2014;99(5 Suppl):1184S–93S. doi:10.3945/ajcn.113.073536
31. Gondivkar SM, Gadbail AR, Gondivkar RS, et al. Nutrition and oral health. Dis Mon. 2019;65(6):147–154. doi:10.1016/j.disamonth.2018.09.009
32. Sangaleti C, Schveitzer MC, Peduzzi M, ELCP Z, Soares CB. Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: a systematic review. JBI Database System Rev Implement Rep. 2017;15(11):2723–2788. doi:10.11124/JBISRIR-2016-003016
33. Fernandez JB, Ahearn K, Atar M, et al. Interprofessional educational experience among dietitians after a pediatric dentistry clinical rotation. Top Clin Nutr. 2017;32(3):193–201. doi:10.1097/TIN.0000000000000112
34. Spaulding EM, Marvel FA, Jacob E, et al. Interprofessional education and collaboration among healthcare students and professionals: a systematic review and call for action. J Interprof Care. 2021;35(4):612–621. doi:10.1080/13561820.2019.1697214
35. Zorek JA, Fike DS, Eickhoff JC, et al. Refinement and validation of the student perceptions of physician-pharmacist interprofessional clinical education instrument. Am J Pharmaceut Educ. 2016;80(3):47. doi:10.5688/ajpe80347
36. Dominguez DG, Fike DS, MacLaughlin EJ, Zorek JA. A comparison of the validity of two instruments assessing health professional student perceptions of interprofessional education and practice. J Interprofessional Care. 2015;29(2):144–149. doi:10.3109/13561820.2014.947360
37. Lockeman KS, Lanning SL, Dow AW, et al. Outcomes of introducing early learners to interprofessional competencies in a classroom setting. Teaching Learning Med. 2017;29(4):433–443. doi:10.1080/10401334.2017.1296361
38. Reeves S. Why we need interprofessional education to improve the delivery of safe and effective care. Interface. 2016;20:185–197. doi:10.1590/1807-57622014.0092
39. Fernandes AR, Palombella A, Salfi J, Wainman B. Dissecting through barriers: a mixed-methods study on the effect of interprofessional education in a dissection course with healthcare professional students. Anat Sci Educ. 2015;8(4):305–316. doi:10.1002/ase.1517
40. Reeves S, Fletcher S, Barr H, et al. A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Med Teach. 2016;38(7):656–668. doi:10.3109/0142159X.2016.1173663
41. Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Rev. 2013;2013(3):CD002213. doi:10.1002/14651858.CD002213.pub3
42. Anderson OS, Hisamatsu R, Dubin LJ, Mergos J, Vordenberg SE. An asynchronous, interprofessional teams and teamwork experience for the first-exposure learner. J Interprof Educ Pract. 2019;14:47–52. doi:10.1016/j.xjep.2018.11.006
43. Heuberger R, Clark WA. Synchronous delivery of online graduate education in clinical nutrition: an inquiry into student perceptions and preferences. J Allied Health. 2019;48(1):61–66.
44. Gross MM, Phanudulkitti C, Bavireddy V, et al. Changes in student attitudes toward interprofessional education after online and in-person introductory learning activities. Health Interprofessional Pract Educ. 2022;4(3):2164. doi:10.7710/2641-1148.2164
45. Tajfel H, Turner JC, Austin WG, Worchel S. An integrative theory of intergroup conflict. Org Identity. 1979;56:9780203505984–16.
46. Roberts C, Kumar K. Student learning in interprofessional practice-based environments: what does theory say? BMC Med Educ. 2015;15:211. doi:10.1186/s12909-015-0492-1
47. Singer Z, Fung K, Lillie E, et al. Interprofessional education day – an evaluation of an introductory experience for first-year students. J Interprofessional Care. 2018;32(3):399–402. doi:10.1080/13561820.2018.1433641
48. Soubra L, Badr SBY, Zahran EM, Aboul-Seoud M. Effect of interprofessional education on role clarification and patient care planning by health professions students. Health Professions Educ. 2018;4(4):317–328. doi:10.1016/j.hpe.2017.12.005
49. Curran VR, Sharpe D, Forristall J, Flynn K. Student satisfaction and perceptions of small group process in case-based interprofessional learning. Med Teach. 2008;30(4):431–433. doi:10.1080/01421590802047323
50. Peeters MJ, Sexton M, Metz AE, Hasbrouck CS. A team-based interprofessional education course for first-year health professions students. Curr Pharm Teach Learn. 2017;9(6):1099–1110. doi:10.1016/j.cptl.2017.07.006
51. Wen A, Wong L, Ma C, et al. An interprofessional team simulation exercise about a complex geriatric patient. Gerontol Geriatr Educ. 2019;40(1):16–29. doi:10.1080/02701960.2018.1554568
52. Pettit J, Ferguson KJ. Medical emergency during flight: a team-building exercise. MedEdPORTAL. 2017;13(10530). doi:10.15766/mep_2374-8265.10530
53. Oandasan I, Reeves S. Key elements for interprofessional education. Part 1: the learner, the educator and the learning context. J Interprof Care. 2005;19 Suppl 1:21–38. doi:10.1080/13561820500083550
54. Oandasan I, Reeves S. Key elements of interprofessional education. Part 2: factors, processes and outcomes. J Interprof Care. 2005;19 Suppl 1:39–48. doi:10.1080/13561820500081703
55. McInnes S, Peters K, Bonney A, Halcomb E. A qualitative study of collaboration in general practice: understanding the general practice nurse’s role. J Clin Nurs. 2017;26(13–14):1960–1968. doi:10.1111/jocn.13598
56. Marion-Martins AD, Pinho DLM. Interprofessional simulation effects for healthcare students: a systematic review and meta-analysis. Nurse Educ Today. 2020;94:104568. doi:10.1016/j.nedt.2020.104568
57. Villadsen A, Allain L, Bell L, Hingley-Jones H. The use of role-play and drama in interprofessional education: an evaluation of a workshop with students of social work, midwifery, early years and medicine. Soc Work Educ. 2011;31(1):75–89. doi:10.1080/02615479.2010.547186
58. Mohaupt J, van Soeren M, Andrusyszyn MA, Macmillan K, Devlin-Cop S, Reeves S. Understanding interprofessional relationships by the use of contact theory. J Interprof Care. 2012;26(5):370–375. doi:10.3109/13561820.2012.673512
59. Keller KB, Eggenberger TL, Belkowitz J, Sarsekeyeva M, Zito AR. Implementing successful interprofessional communication opportunities in health care education: a qualitative analysis. Int J Med Educ. 2013;4:253–259. doi:10.5116/ijme.5290.bca6
60. Kirwin J, Greenwood KC, Rico J, Nalliah R, DiVall M. Interprofessional curbside consults to develop team communication and improve student achievement of learning outcomes. Am J Pharm Educ. 2017;81(1):15. doi:10.5688/ajpe81115
61. Hallin K, Kiessling A, Waldner A, Henriksson P. Active interprofessional education in a patient based setting increases perceived collaborative and professional competence. Med Teach. 2009;31(2):151–157. doi:10.1080/01421590802216258
62. Russell L, Nyhof-Young J, Abosh B, Robinson S. An exploratory analysis of an interprofessional learning environment in two hospital clinical teaching units. J Interprof Care. 2006;20(1):29–39. doi:10.1080/13561820500476473
63. van Diggele C, Roberts C, Burgess A, Mellis C. Interprofessional education: tips for design and implementation. BMC Med Educ. 2020;20(Suppl 2):455. doi:10.1186/s12909-020-02286-z
64. Grapczynski CA, Schuurman S, Booth AD, Bambini D, Beel-Bates C. The integrated model for interprofessional education: a design for preparing health professions’ students to work in interprofessional teams. J Allied Health. 2015;44(2):108–114.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.