Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Bridging Accessibility and Precision: Evaluating the Reliability and Validity of a Smartphone-Based Skin Colorimeter
Authors Ouyang H ![]() , Yang J, Ning X
, Yang J, Ning X ![]() , Xia Q, Zuo X, Xu J, Sheng Y, Song J, Ma Z, Wu L, Song X, Cui Y
, Xia Q, Zuo X, Xu J, Sheng Y, Song J, Ma Z, Wu L, Song X, Cui Y
Received 15 December 2025
Accepted for publication 24 March 2026
Published 31 March 2026 Volume 2026:19 589014
DOI https://doi.org/10.2147/CCID.S589014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Monica K. Li
Hongfei Ouyang,1,2 Jungang Yang,2,3 Xiaoli Ning,2,4 Qingyue Xia,1,2 Xianbo Zuo,2,5,6 Jingkai Xu,2,5,6 Yujun Sheng,2 Jinyan Song,7 Zitao Ma,7 Liang Wu,7 Xuejiao Song,2,5,6 Yong Cui1,2
1China-Japan Friendship Hospital (Institute of Clinical Medical Sciences), Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Dermatology, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 3Peking University China-Japan Friendship School of Clinical Medicine, Beijing, People’s Republic of China; 4Department of Dermatology, China-Japan Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 5Big Data Center, Department of Information, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 6NHC key laboratory of Clinical Big Data Standardization & Integration, Beijing, People’s Republic of China; 7Hangzhou C2H4 Internet Technology Co., Ltd, Hangzhou, People’s Republic of China
Correspondence: Yong Cui, China-Japan Friendship Hospital (Institute of Clinical Medical Sciences), Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China, Email [email protected] Liang Wu, Hangzhou C2H4 Internet Technology Co., Ltd, Hangzhou, People’s Republic of China, Email [email protected]
Background: Accurate quantification of skin color is essential for dermatologic research and clinical practice. Conventional methods rely on specialized equipment, trained operators, and high costs. Smartphone-based technologies provide a promising alternative for accessible skin color assessment.
Objective: To evaluate the reliability and validity of the smartphone-based skin colorimeter application, You Look Good Today (YLGTD), for facial skin color assessment compared with two validated devices, VISIA and DermaLab Combo.
Methods: A total of 105 Chinese participants with healthy facial skin were enrolled. Cheek skin color measurements were obtained using YLGTD (user self-assessment and physician measurement modes), VISIA, and DermaLab Combo. Inter-rater reliability between YLGTD measurement modes was assessed using intraclass correlation coefficients (ICC) and Bland-Altman analysis. Criterion validity was evaluated using Pearson’s correlation coefficients between YLGTD measurements and the reference devices.
Results: YLGTD demonstrated excellent inter-rater reliability across all parameters (ICC: 0.85– 0.95). Bland–Altman analysis showed small biases between the two measurement modes for the L, a, and b (− 0.05, 0.18, and − 0.99, respectively). For criterion validity, YLGTD in user mode showed strong correlations with DermaLab Combo for L* (r = 0.71), individual typology angle (ITA°, r = − 0.81), and chroma (C*, r = 0.78), and moderate correlations for b* (r = 0.59) and hue (h°, r = 0.57). Correlations were consistently stronger in physician mode (L*: r = 0.77; b*: r = 0.75; C*: r = 0.84; ITA°: r = − 0.87). VISIA showed a stronger correlation for a* (r = 0.55) but weaker correlations for L* (r = 0.56) and ITA° (r = − 0.68) compared with YLGTD.
Conclusion: The smartphone-based application YLGTD demonstrated excellent reliability and acceptable validity for facial skin color assessment, particularly for pigmentation-related parameters. Its standardized measurement workflow and integrated algorithms enable consistent skin color evaluation across devices and real-world conditions, providing a convenient and cost-effective approach for objective skin color assessment.
Keywords: skin color, skin colorimetry, smartphone application, YLGTD, reliability, device validation
Introduction
Human skin color is a prominent phenotypic characteristic primarily determined by melanin, carotenoids, and hemoglobin.1 Among these, melanin plays a central role in photoprotection against ultraviolet radiation (UVR).1 Alterations in skin color are closely associated with various pathological conditions, including pigmentary disorders (eg., melasma and vitiligo), inflammatory dermatoses (eg., rosacea), and certain systemic diseases (eg., jaundice).2 Quantitative skin color measurement provides objective markers for disease diagnosis and treatment monitoring, while also supporting photodamage evaluation, skin cancer risk prediction, and surgical flap matching.3–5 Accordingly, objective skin color evaluation is integral to personalized dermatologic care, aesthetic interventions, and quantitative monitoring of treatment outcomes.
Current approaches for skin color assessment range from administered visual scales to instrument-based colorimetry.6 The Fitzpatrick Skin Type (FST), originally developed to classify UVR responses in Caucasian populations, remains widely used in clinical practice.7 However, its correlation with objective colorimetric parameters is limited.8 In contrast, instrument-based colorimetric devices provide quantitative and reproducible skin color measurements, including tristimulus colorimeters (eg., Colorimeter CL-400) and reflectance spectrophotometers (eg., DermaLab Combo).9 These instruments quantify skin color using L*a*b*and individual typology angle (ITA°) values within the CIELAB color space standardized by the Commission Internationale de l’Eclairage (CIE).9,10 Despite their accuracy, their widespread use remains limited by high costs, environmental sensitivity, and reliance on trained personnel.
Recent advances in spectral imaging and artificial intelligence (AI) have spurred innovation in dermatologic tools.11,12 The VISIA imaging system (Canfield Scientific, USA) is widely used in dermatology and cosmetic research. It enables comprehensive skin evaluation under standard white light, ultraviolet, and cross-polarized lighting conditions.13 Meanwhile, smartphone-based applications have emerged as promising tools for rapid and cost-effective skin assessment.14 However, smartphone imaging is susceptible to inter-device hardware variability and environmental influences. Differences in camera modules, sensor performance, and image signal processing algorithms across smartphone models, as well as ambient lighting conditions, may compromise imaging reproducibility, which is critical for medical image analysis.15
“You Look Good Today” (YLGTD; Hangzhou C2H4 Internet Technology Co., China) is a smartphone-based skin analysis application that integrates AI-driven image processing algorithms. The system is trained on a large-scale skin image database and incorporates neural network–based color correction and feature recognition. These techniques mitigate cross-device and environmental variability, enabling stable and quantitative assessment of skin color. However, its clinical applicability requires rigorous validation of measurement reproducibility and accuracy against established reference standards.
This study investigates the reliability and criterion validity of YLGTD for facial skin color assessment. Its performance was evaluated under two measurement modes (user self-assessment mode and physician measurement mode) and compared with two established reference systems: VISIA and DermaLab Combo. By addressing key gaps in the validation of mobile dermatologic technologies, this study aims to determine whether YLGTD can serve as a scalable, cost-effective, and user-friendly alternative to conventional colorimetric devices.
Materials and Methods
Study Design and Participants
This was a single-center, cross-sectional study conducted at China-Japan Friendship Hospital from July 2024 to September 2024. A total of 105 participants were recruited from the dermatology department. The sample size was determined based on clinical feasibility and practicality. The study was approved by the Clinical Research Ethics Committee of China-Japan Friendship Hospital (2023-KY-218) and conducted in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent and acknowledged the privacy policy of the YLGTD application. The study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.16
Only individuals with uniform cheek skin tone and without facial skin diseases, such as pigmentary disorders, rosacea, or other dermatologic diseases, were included. Participants with secondary skin pigmentation abnormalities caused by conditions such as anemia, jaundice, or renal insufficiency, or those with a history of photosensitivity, were excluded.
Instruments
YLGTD
Facial images were acquired using the smartphone-based application YLGTD (Hangzhou C2H4 Internet Technology Co., Ltd., China) in two modes: user self-assessment and physician measurement. Smartphones were required to have high-resolution rear cameras (≥2448×3264 pixels) to minimize hardware-related variability. Participants were positioned in uniformly illuminated environments without direct sunlight. Facial images were captured using the rear camera under application-guided voice instructions, with facial coverage exceeding 80% of the frame and maintained through real-time adjustments of distance and angle. The smartphone light-emitting diode (LED) flash was automatically activated to standardize illumination.
Post-acquisition processing included color restoration, facial feature localization, and quantitative analysis. A neural network–based iterative color correction algorithm incorporated device-specific parameters, including smartphone model and exposure settings, to reduce cross-device variability and reconstruct the original skin tone. After color normalization, the cheek region was automatically segmented while excluding spots, moles, and acne lesions.
Skin color analysis was performed using a three-step image-processing pipeline. First, mean pixel values within the region of interest were calculated in the red–green–blue (RGB) color space. These values were then converted into the CIELAB color space using OpenCV (version 3.4.20) and encoded in an 8-bit integer format (L: 0–255; a: 0–255; b: 0–255). Finally, a machine learning–based parameterization model derived three quantitative indices representing skin lightness, chromaticity, and hue: skin color level (0–1000), skin color temperature (0–1000), and skin color hue (0°–90°).
VISIA
Facial images were obtained using the VISIA imaging analysis system (Canfield Scientific, USA) under standardized illumination conditions. Image acquisition was conducted in a light-controlled darkroom to eliminate ambient interference. The system utilizes a 15-megapixel camera equipped with automated focusing and white-balance functions. Acquired images were subsequently processed using the YLGTD embedded algorithm for skin color quantification.
DermaLab Combo
The DermaLab Combo system (Cortex Technology, Denmark) employs reflectance spectrophotometry to quantify skin color parameters. Reflected optical signals are transformed into CIELAB parameters, including L* (lightness), a* (red-green axis), and b* (yellow-blue axis). In dermatologic research, L* reflects skin lightness, a* is associated with erythema, and b* reflects pigmentation and tanning.10 Based on these parameters, three composite indices are derived: ITA°, an objective indicator of melanin-related skin tone; chroma (C*), representing color saturation; and hue angle (h°), representing color tone.10,17 The asterisk (*) denotes parameters in the CIELAB color space.10
Measurement Protocol
Skin color measurements were performed using YLGTD, VISIA, and DermaLab Combo under controlled clinical conditions and real-world user settings. The measurement protocol comprised three stages: (1) Preprocessing: Participants underwent facial cleansing followed by a 15-minute acclimatization period under controlled environmental conditions (22 ± 2 °C; 50 ± 10% relative humidity; windowless room without daylight). (2) Professional measurements: Physicians sequentially acquired facial images using YLGTD (iPhone 15 Pro) and the VISIA system. Contact measurements were subsequently performed using the DermaLab Combo color probe at four predefined sites on each cheek. The mean value was calculated while avoiding pigmented nevi, acne lesions, scars, and uneven pigmentation. (3) User self-assessment: Participants captured facial images using YLGTD on their personal smartphones in real-world environments.
Data collection was supervised by trained researchers. FST classification was conducted through clinician-guided assessment according to the method of Eilers et al18 Demographic characteristics (age, sex, ethnicity) and smartphone models used for self-assessment were recorded.
Statistical Analysis
Statistical analyses were performed using SPSS (version 27.0) and GraphPad Prism (version 10), with p < 0.05 considered statistically significant. Reliability between the two YLGTD measurement modes (user self-assessment and physician measurement) was assessed using intraclass correlation coefficients (ICC), interpreted as > 0.75 (excellent), 0.40–0.75 (good), and < 0.40 (poor).19 Normality of paired differences was examined using the Shapiro–Wilk test. Agreement between measurement methods was evaluated using Bland–Altman analysis. Validity between devices was assessed using Pearson’s correlation coefficients (r), interpreted as |r| ≥ 0.70 (strong), 0.50–0.69 (moderate), and < 0.50 (weak).20 Subgroup analyses were performed stratified by smartphone platform (iPhone and Android).
Results
Participants and Descriptive Statistics
The demographic and clinical characteristics of the participants are summarized in Table 1. A total of 105 participants were enrolled, including 85 females (80.95%) and 20 males (19.05%), with an age range of 18–50 years (mean ± SD: 25.8 ± 3.7 years). The majority were of Han Chinese ethnicity (95.24%). Fitzpatrick skin types were distributed as follows: type II (19.05%), type III (58.10%), and type IV (22.86%). Smartphone brand distribution for self-assessment was as follows: iPhone (53.33%), Huawei (19.05%), Xiaomi (12.38%), and vivo (9.52%), with other brands comprising the remaining proportion.
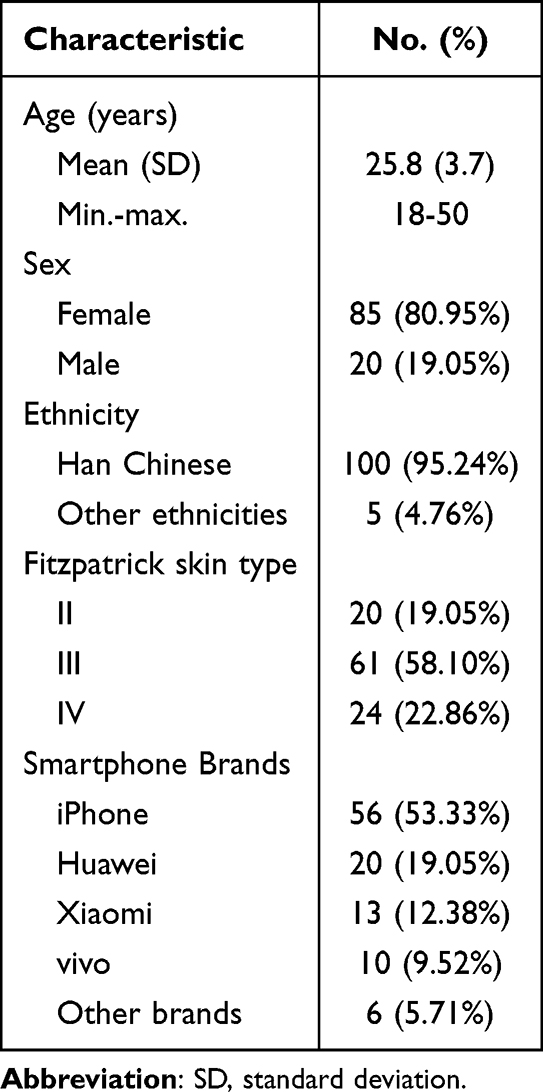 |
Table 1 Demographic and Clinical Characteristics of the Participants (n = 105) |
Inter-Rater Reliability of YLGTD: User Vs. Physician Measurements
Inter-rater reliability between YLGTD user self-assessment (user mode) and physician measurement (physician mode) was assessed (Table 2 and Figure 1). ICC values for the six skin color parameters ranged from 0.85 to 0.95, indicating excellent reliability. Bland-Altman analysis showed small biases for L, a, and b parameters (−0.05, 0.18, and −0.99, respectively), with relatively narrow 95% Limits of Agreement (LoA) (L: −5.34 to 5.24; a: −2.64 to 3.00; b: −3.95 to 1.97). Larger absolute biases were observed for skin color level and skin color temperature (−7.71 and −41.21, respectively). Across all parameters, 92.38%–97.14% of differences fell within the 95% LoA, indicating good agreement between the two measurement modes. Subgroup analyses stratified by smartphone platform showed comparable ICC values and mean biases across iPhone and Android devices (Supplementary Table S1).
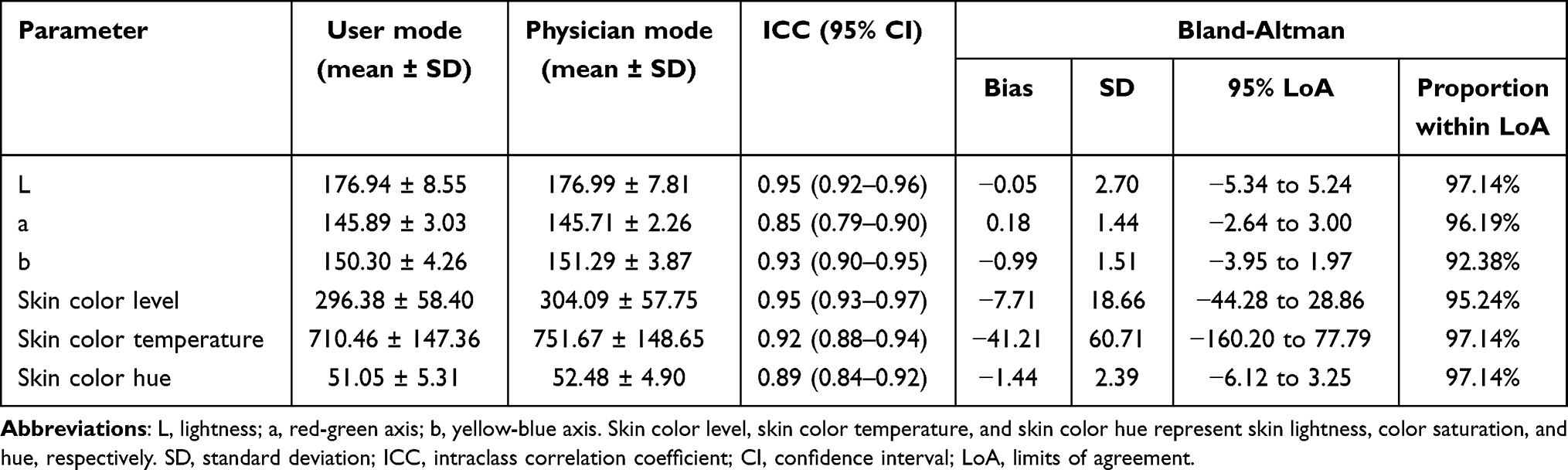 |
Table 2 Inter-Rater Reliability of YLGTD for Skin Color Assessment: User vs. Physician Measurements |
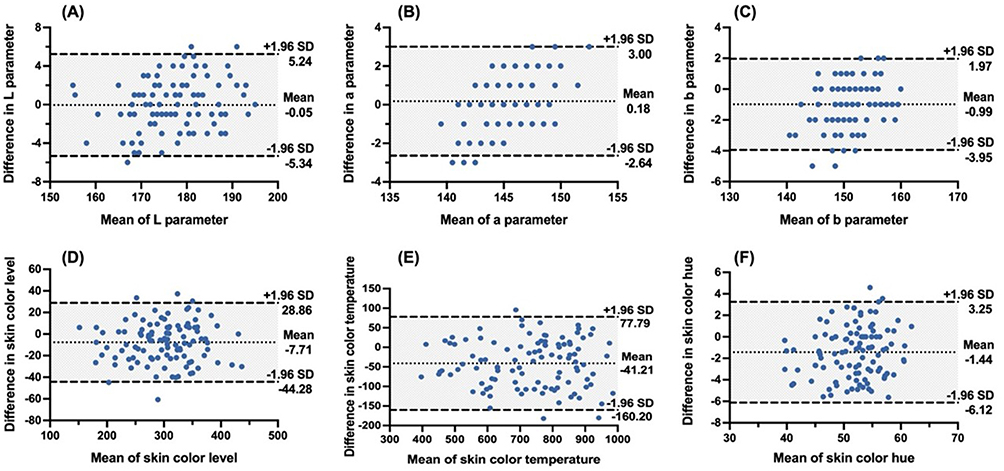 |
Figure 1 Bland–Altman plots showing agreement between YLGTD user self-assessment and physician measurements (n = 105). Panels (A–F) correspond to the parameters L, a, b, skin color level, skin color temperature, and skin color hue, respectively. The y-axis represents the difference between user and physician measurements (user − physician), and the x-axis represents their mean. The central dotted line indicates the mean bias, and the dashed lines indicate the upper and lower 95% limits of agreement. Some points overlap due to identical values. |
Agreement Between YLGTD and VISIA
Skin images were acquired using YLGTD (Figure 2A) and VISIA (Figure 2B). Agreement between the two systems is summarized in Table 3. In the user self-assessment mode, ICC values ranged from 0.15 for the a parameter (poor agreement) to 0.78 for skin color level (excellent agreement). The remaining parameters showed good agreement, including L (ICC = 0.56), b (ICC = 0.50), skin color temperature (ICC = 0.69), and skin color hue (ICC = 0.54). In the physician measurement mode, ICC values ranged from 0.24 for the a parameter (poor agreement) to 0.74 for skin color level (good agreement). Agreement improved for several parameters, including b (ICC = 0.60) and skin color hue (ICC = 0.59), while other parameters showed levels of agreement comparable to those in the user mode.
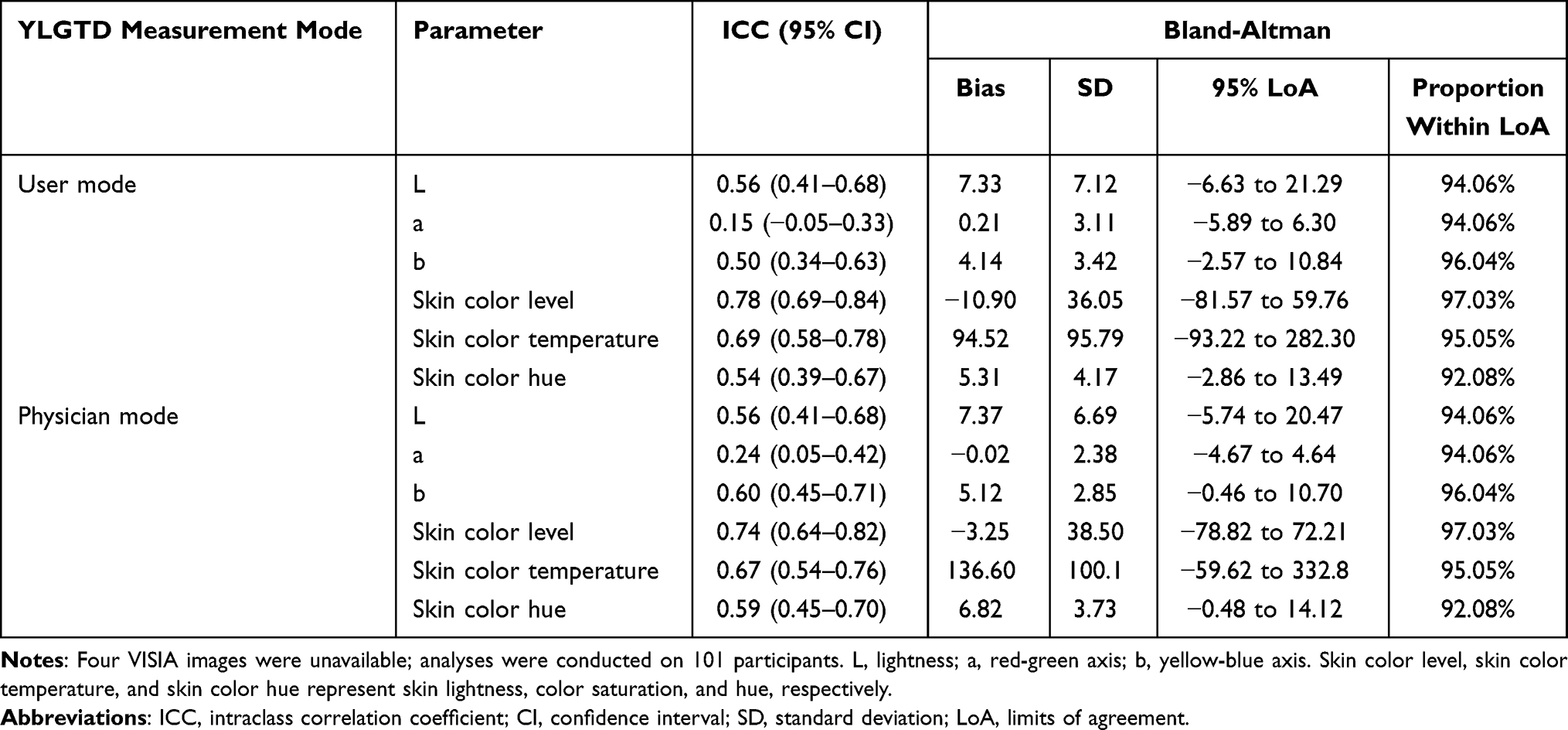 |
Table 3 Agreement Between YLGTD and VISIA for Skin Color Assessment |
 |
Figure 2 Facial images captured by YLGTD (A) and VISIA (B). |
Bland–Altman analysis showed varying mean biases across parameters. In the user mode, bias values ranged from −10.90 to 94.52, while in the physician mode they ranged from −3.25 to 136.60. Correspondingly, relatively wide 95% LoA were observed. Nevertheless, the proportions of differences within the LoA remained high, ranging from 92.08% to 97.03%.
Criterion Validity of YLGTD and VISIA Compared with DermaLab Combo
Criterion validity relative to DermaLab Combo is summarized in Table 4. In the user self-assessment mode, YLGTD showed strong correlations with DermaLab Combo for L* (r = 0.71) and chroma (C*, r = 0.78), and moderate correlations for b* (r = 0.59) and hue (h°, r = 0.57). Skin color level showed a strong negative correlation with ITA° (r = −0.81), whereas the correlation between a and a* was weak (r = 0.21). In the physician measurement mode, correlations with DermaLab Combo were generally stronger, with strong correlations for L* (r = 0.77), b* (r = 0.75), ITA° (r = −0.87), and chroma (C*, r = 0.84), moderate correlation for hue (h°, r = 0.65), and weak correlation for a* (r = 0.28). Compared with both YLGTD modes, VISIA showed a moderate correlation for a* (r = 0.55) but weaker correlations for L* (r = 0.56) and ITA° (r = −0.68).
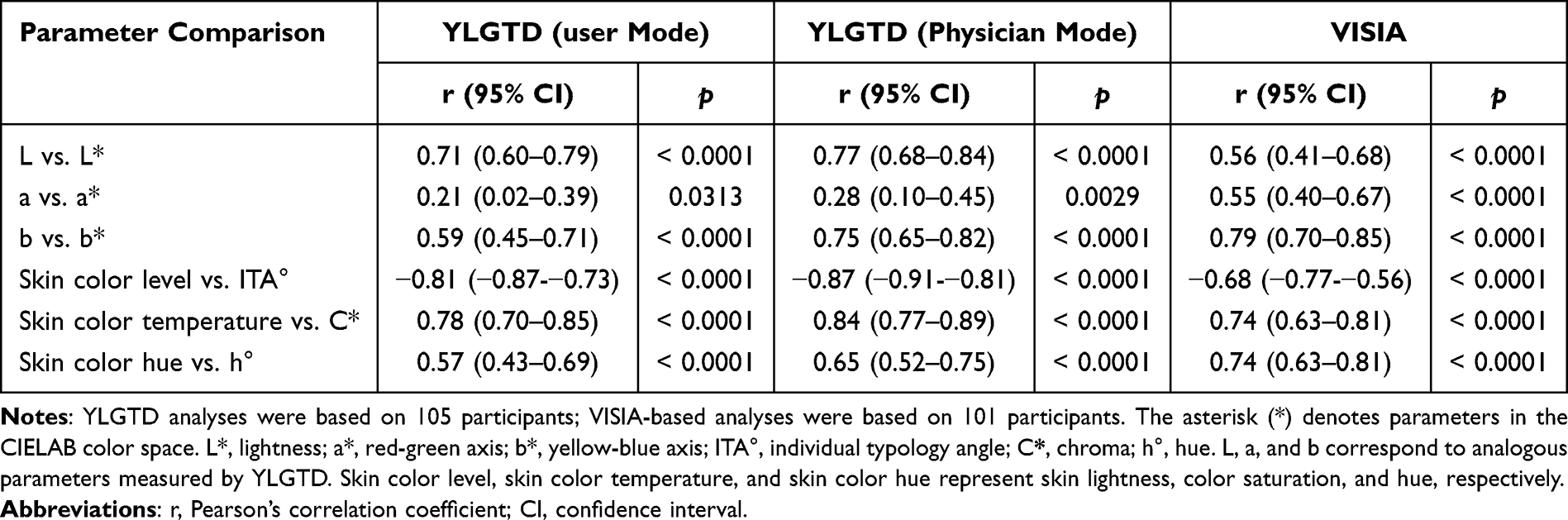 |
Table 4 Criterion Validity of YLGTD and VISIA Compared with DermaLab Combo for Skin Color Assessment |
Discussion
This study evaluated the reliability and validity of the smartphone-based application YLGTD for facial skin color assessment compared with two reference devices: the VISIA imaging system and the DermaLab Combo spectrophotometer.
Using ICC and Bland–Altman analyses, our findings indicated that YLGTD achieved excellent reliability (ICC: 0.85–0.95) in both user self-assessment and physician measurement modes, with small biases in the L, a, and b parameters. The dual-mode design allowed evaluation of measurement consistency under different usage conditions. Images in physician mode were captured using a uniform device under controlled settings, whereas participants in user mode used personal smartphones from multiple brands in everyday environments. Subgroup analyses stratified by smartphone platform also showed comparable reliability between iPhone and Android devices. Together, these results suggested that the standardized workflow and integrated correction algorithm may reduce measurement variability across devices and usage conditions. These findings were consistent with previous studies reporting reliable performance of smartphone-based dermatologic assessment tools in heterogeneous real-world settings.21
Among the evaluated parameters, the a parameter (ICC = 0.85) showed slightly lower inter-rater reliability than L (ICC = 0.95) and b (ICC = 0.93), although all parameters still demonstrated excellent reliability. Similar observations have been reported in previous DermaLab studies of erythema assessment.22 This discrepancy may reflect the greater sensitivity of erythema-related signals to subtle physiological fluctuations and environmental illumination. These findings emphasized the importance of standardized image acquisition protocols and appropriate user guidance when assessing erythema-related parameters.
In addition to the basic color parameters, the derived composite indices—skin color level, skin color temperature, and skin color hue—also exhibited excellent reliability (ICC: 0.89–0.95). Although skin color level and temperature showed relatively larger absolute biases due to their broader measurement ranges, more than 92% of observations remained within the 95% limits of agreement. By transforming conventional CIELAB metrics into more intuitive representations, these indices may enhance interpretability and improve accessibility for non-specialist users.
VISIA is a widely used facial imaging system in dermatology and cosmetic research that provides standardized images for precise skin assessment. Previous studies have shown that VISIA-derived indicators, such as brown spots, correlate with melanin levels, whereas red areas reflect erythema severity.13,23 In the present study, agreement between YLGTD and VISIA ranged from poor to excellent across parameters, with poor agreement observed for the a parameter and good-to-excellent agreement for most other skin color parameters. Systematic biases were observed, which may reflect hardware-related differences between VISIA and smartphone cameras. VISIA uses a standardized illuminant, whereas smartphone imaging relies on flash LEDs with different spectral power distributions and lower color rendering indices.24,25 Smartphone flash LEDs typically exhibit blue-dominant spectra, which may influence skin color appearance and contribute to measurement discrepancies.24,25 Despite these differences, the results suggested that smartphone-based skin tone assessment may provide comparable information for several melanin-related parameters, particularly L and chroma, which are commonly used indicators of pigmentation.
DermaLab Combo is a specialized skin analysis instrument primarily used in cosmetic research. Its color probe employs reflectance spectrophotometry to quantify melanin and erythema within the CIELAB color space, providing objective and standardized skin color measurements.26 Previous studies have reported excellent inter-rater reliability (ICC: 0.94–0.98) for DermaLab measurements, supporting its role as a reference device for quantitative skin color assessment.22
In comparison with DermaLab Combo, YLGTD demonstrated strong correlations for L* (lightness) and C* (chroma) parameters, particularly in the physician mode, indicating high consistency with spectrophotometric measurements. The pronounced negative correlation between skin color level and ITA° further supported the capability of YLGTD in characterizing pigmentation gradients. These findings suggested that smartphone-based tools may provide a practical approach for skin tone classification in non-specialized settings. However, weak correlations were observed for the erythema-related a* parameters, which also showed lower agreement in the VISIA comparison. This limitation may be partly related to spectral constraints of smartphone flash LEDs, particularly the insufficient red spectral components that are important for accurate erythema detection.27
Objective skin color assessment plays an important role in dermatologic practice, particularly for pigmentation evaluation, treatment monitoring, and photodamage assessment. As an accessible and cost-effective approach, smartphone-based skin color quantification may facilitate large-scale screening, longitudinal monitoring, teledermatology consultations, and objective evaluation of cosmetic or laser treatment outcomes. These applications may be particularly valuable in primary care settings and resource-limited regions where professional imaging devices are unavailable. Overall, YLGTD provides a practical and economical option for precision skin color assessment in real-world settings.
This study has several limitations that should be acknowledged. First, the single-center design, relatively small sample size, and recruitment of participants from a relatively homogeneous Chinese population may limit the generalizability of the findings. Second, erythema-related measurements remain more susceptible to hardware and illumination constraints. Third, only participants with normal facial skin were included, and applicability to pathological skin conditions requires further investigation. Future studies should include larger multi-center populations, optimize imaging techniques, and evaluate performance in pathological skin conditions.
Conclusion
Overall, the smartphone-based application YLGTD demonstrated excellent reliability and acceptable validity with established reference devices, particularly for pigmentation-related parameters including lightness and chroma. Through standardized image acquisition and algorithm-based color correction, YLGTD enables consistent skin color evaluation across different devices and diverse real-world conditions. As a convenient, cost-effective, and user-friendly tool, it offers an accessible approach for objective skin color assessment, with potential applications in longitudinal skin monitoring and personalized skincare evaluation. Further validation in larger multi-center populations and continued optimization of erythema-related algorithms are warranted.
Data Sharing Statement
The data are available on reasonable request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Statement
The study was approved by the Clinical Research Ethics Committee of China-Japan Friendship Hospital (2023-KY-218) and conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants, including consent for publication of identifiable images.
Acknowledgments
The authors would like to thank all the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National High Level Hospital Clinical Research Funding (No.2023-NHLHCRF-YXHZ-ZRZD-06) and the Horizontal Project of China-Japan Friendship Hospital (No.2024-HX-92).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lin JY, Fisher DE. Melanocyte biology and skin pigmentation. Nature. 2007;445(7130):843–10. doi:10.1038/nature05660
2. Burg G. Changes in color of the skin and systemic disease. Clin Dermatol. 2019;37(6):610–617. doi:10.1016/j.clindermatol.2019.07.033
3. Paulus VAA, van Raay SHC, Teunissen JS, Lese I, Ulrich DJO. Skin color match in autologous breast reconstruction: which donor site gives the best result? Plast Reconstr Surg. 2025;155(1):9–18. doi:10.1097/prs.0000000000011562
4. Sitek A, Rosset I, Żądzińska E, Kasielska-Trojan A, Neskoromna-Jędrzejczak A, Antoszewski B. Skin color parameters and Fitzpatrick phototypes in estimating the risk of skin cancer: a case-control study in the polish population. J Am Acad Dermatol. 2016;74(4):716–723. doi:10.1016/j.jaad.2015.10.022
5. Pardo LM, Hamer MA, Liu F, et al. Principal component analysis of seven skin-ageing features identifies three main types of skin ageing. Br J Dermatol. 2020;182(6):1379–1387. doi:10.1111/bjd.18523
6. Weir VR, Dempsey K, Gichoya JW, Rotemberg V, Wong AI. A survey of skin tone assessment in prospective research. NPJ Digit Med. 2024;7(1):191. doi:10.1038/s41746-024-01176-8
7. Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124(6):869–871. doi:10.1001/archderm.124.6.869
8. Leenutaphong V. Relationship between skin color and cutaneous response to ultraviolet radiation in Thai. Photodermatol Photoimmunol Photomed. 1995;11(5–6):198–203. doi:10.1111/j.1600-0781.1995.tb00169.x
9. Langeveld M, van de Lande LS, O’Sullivan E, van der Lei B, Van dongen JA. Skin measurement devices to assess skin quality: a systematic review on reliability and validity. Skin Res Technol. 2022;28(2):212–224. doi:10.1111/srt.13113
10. Ly BCK, Dyer EB, Feig JL, Chien AL, Del Bino S. Research techniques made simple: cutaneous colorimetry: a reliable technique for objective skin color measurement. J Invest Dermatol. 2020;140(1):3–12.e1. doi:10.1016/j.jid.2019.11.003
11. Kim S, Cho D, Kim J, et al. Smartphone-based multispectral imaging: system development and potential for mobile skin diagnosis. Biomed Opt Express. 2016;7(12):5294–5307. doi:10.1364/boe.7.005294
12. Fliorent R, Fardman B, Podwojniak A, et al. Artificial intelligence in dermatology: advancements and challenges in skin of color. Int J Dermatol. 2024;63(4):455–461. doi:10.1111/ijd.17076
13. Linming F, Wei H, Anqi L, et al. Comparison of two skin imaging analysis instruments: the VISIA(®) from canfield vs the ANTERA 3D(®) CS from miravex. Skin Res Technol. 2018;24(1):3–8. doi:10.1111/srt.12381
14. Raju G, Ranjan A, Banik S, Poddar A, Managuli V, Mazumder N. A commentary on the development and use of smartphone imaging devices. Biophys Rev. 2024;16(2):151–163. doi:10.1007/s12551-023-01175-1
15. Hunt B, Ruiz AJ, Pogue BW. Smartphone-based imaging systems for medical applications: a critical review. J Biomed Opt. 2021;26(4):040902. doi:10.1117/1.JBO.26.4.040902
16. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–s34. doi:10.4103/sja.SJA_543_18
17. Wu Y, Yi F, Akimoto M, Tanaka T, Meng H, Dong Y. Objective measurement and comparison of human facial skin color in East Asian females. Skin Res Technol. 2020;26(4):584–590. doi:10.1111/srt.12838
18. Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-report in assessing Fitzpatrick skin phototypes I through VI. JAMA Dermatol. 2013;149(11):1289–1294. doi:10.1001/jamadermatol.2013.6101
19. Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychologl Assess. 1994;6(4):284. doi:10.1037/1040-3590.6.4.284
20. Mukaka MM. A guide to appropriate use of correlation coefficient in medical research. Malawi Med J. 2012;24(3):69.
21. Niakan S, Safi M, Younespour S, Khoshtarkib S. Comparative analysis of smartphone colorimeter apps and spectrophotometry for measuring forehead skin color in maxillofacial prosthesis fabrication. J Prosthodont. 2024;34:602–608. doi:10.1111/jopr.13970
22. Gankande TU, Duke JM, Danielsen PL, DeJong HM, Wood FM, Wallace HJ. Reliability of scar assessments performed with an integrated skin testing device - the DermaLab Combo(®). Burns. 2014;40(8):1521–1529. doi:10.1016/j.burns.2014.01.025
23. Huang YW, Arkesteijn W, Lai YJ, Ng CY. A comparative study of an advanced skin imaging system in diagnosing facial pigmentary and inflammatory conditions. Sci Rep. 2024;14(1):14673. doi:10.1038/s41598-024-63274-7
24. Bellia L, Bisegna F, Spada G. Lighting in indoor environments: visual and non-visual effects of light sources with different spectral power distributions. Build Environ. 2011;46(10):1984–1992. doi:10.1016/j.buildenv.2011.04.007
25. Melgosa M, Richard N, Fernández-Maloigne C, et al. Colour differences in Caucasian and oriental women’s faces illuminated by white light-emitting diode sources. Int J Cosmet Sci. 2018;10. doi:10.1111/ics.12457
26. Szczepanek M, Frątczak A, Lis-święty A. Narrow-band reflectance spectrophotometry for the assessment of erythematous and hyperpigmented skin lesions in localized scleroderma: a preliminary study. Clin Cosmet Invest Dermatol. 2021;14:575–580. doi:10.2147/ccid.S312208
27. Kimme F, Brick P, Chatterjee S, Khanh TQ. Optimized flash light-emitting diode spectra for mobile phone cameras. Appl Opt. 2013;52(36):8779–8788. doi:10.1364/AO.52.008779
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.