Back to Journals » Open Access Journal of Contraception » Volume 14
Breaking the Binary: How Clinicians Can Ensure Everyone Receives High Quality Reproductive Health Services
Authors Jung C, Hunter A, Saleh M, Quinn GP ![]() , Nippita S
, Nippita S
Received 8 September 2022
Accepted for publication 30 January 2023
Published 15 February 2023 Volume 2023:14 Pages 23—39
DOI https://doi.org/10.2147/OAJC.S368621
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Christina Jung,1 Adam Hunter,1 Mona Saleh,2 Gwendolyn P Quinn,1 Siripanth Nippita1
1Department of Obstetrics and Gynecology, New York University Grossman School of Medicine, New York, NY, USA; 2Division of Gynecologic Oncology, Department of Obstetrics & Gynecology, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Correspondence: Gwendolyn P Quinn, Department of Obstetrics and Gynecology, New York University Grossman School of Medicine, 550 1st Ave NBV N91-F, New York, NY, 10016, USA, Tel +1-646-501-6878, Email [email protected]
Abstract: The gender binary has historically defined the study and practice of reproductive and sexual healthcare. However, the male and female binary categorization of sex does not adequately define patients seeking reproductive and sexual health. Comprehensive sexual healthcare should consider diverse gender identity and non-heteronormative sexual practices, family planning, sexually transmitted infections, cancer prevention, and sexual function. Recent research suggests clinicians do not feel prepared to provide care for sexual and gender minority (SGM) patients. In this narrative review, we focus on reproductive and sexual health within the scope of obstetric and gynecologic (OB/GYN) clinical practice. We used traditional medical subject headings to summarize data from publications in peer-reviewed journals published in the last 10 years and identified barriers, facilitators and best practices for de-gendering reproductive healthcare. Following a roughly chronological care path across the lifespan, we categorized findings into the following topics: Early Care for SGM, Sexual Health, Family Planning, and Care Later in Life for SGM. We include recommendations for creating a welcoming environment, SGM inclusive training for clinicians and staff, and best practices for individualized counseling. We review suggested practices related to service delivery and clinical considerations in the provision of sexual and reproductive health care for gender and sexual minority patients.
Keywords: gender, reproductive health, clinician, sexual and gender minorities, transgender, non-binary, LGBTQ+
Background
Reproductive healthcare includes family planning and family building; prevention and management of sexually transmitted infections; cancer screening and prevention; and sexual health and wellbeing. In medicine, biologic sex was effectively synonymous with gender, which has traditionally defined reproductive healthcare practices.1–3 Gender, if used at all, was reserved for behaviors or psychosocial demographics.4 However, gender may or may not equal sex assigned at birth, because the male and female binary categorization of sex does not adequately define all patients seeking reproductive and sexual health.
An increasing number of patients identify as transgender (not identifying with one’s sex assigned at birth), non-binary (not identifying exclusively as a man or woman), gender-fluid (with flexible gender identity), or in groups such as gender-queer, multigender, gender non-conforming, gender neutral, gender diverse, gender expansive, and two-spirit. Other nomenclatures associated with gender identity include the term agender – identifying as no gender at all. In the research literature, this group is often referred to as “gender minority”.5 All of these terms describe gender identity, which is distinct from sexual orientation.
The terms heterosexual, straight, homosexual lesbian, gay, queer, bisexual, pansexual describe sexual orientation. When a person expresses a non-heterosexual identity, the research term applied to this group is “sexual minority”.5,6 Sexual and gender minorities together may be identified using the acronym SGM, and the collection of this patient information on medical intake forms is called sexual orientation and gender identity (SOGI).6
Although we focus on the healthcare needs of gender minority people, clinicians must consider both gender identity and sexual orientation in order to provide high quality sexual and reproductive healthcare. There is inevitable overlap and intersectionality between both gender and sexual minorities. Both gender and sexual minority patients often encounter systemic prejudice when interacting with the healthcare system, and experience increased risk for gender-based violence.7 Gender identity and sexual histories can interact and affect some of the clinical details of sexual and reproductive healthcare. For instance, transgender men may desire counseling on pregnancy risk or options, depending upon sexual practices. Similarly, both cis and lesbian women may believe they do not require cervical cancer screening due to sexual orientation. The binary heteronormative framework creates stigma, discrimination, and marginalization for SGM. This can lead to missed opportunities to support early conversations for gender affirming care, as well as education regarding misperceived risk for STI prevention and screening. Disparities in access and health outcomes also fall along lines of race and class. Thus, we must consider the nuanced layering of lived experiences due to systemic marginalization.
Recent research suggests clinicians do not feel prepared to provide care for SGM patients due to lack of training.1–3 Only since 2010 has the Association of American Medical Colleges required medical school curricula to address SGM health, and the content and format of education varies.8,9 There are no specific requirements for gender or sexual health training in graduate medical education, and exposure depends on specialty and program.8
In this narrative review, we focus on reproductive and sexual health within the scope of obstetric and gynecologic (OB/GYN) clinical practice. We identify barriers, facilitators and best practices for de-gendering quality reproductive healthcare, and review suggested practices related to service delivery and clinical considerations in the provision of reproductive care for sexual and gender minority patients.
Methods
To gather a narrative review for summarizing data, we used traditional medical subject headings from publications in peer-reviewed journals published in the last 10 years. We searched Google Scholar and PubMed for the terms: “reproductive health” OR “sexual health” OR “contraception OR birth control OR family planning” OR “sexually transmitted infection prevention” OR “cervical cancer prevention” OR “HIV/AIDS prevention” OR “HPV prevention” OR “abortion or pregnancy termination” OR “fertility or family building” OR “sexual health” AND “youth” AND “aging or menopause” AND “measuring sexual function” OR “sexual function measurement” OR “sexual quality of life” AND “sexual OR gender minority” OR “transgender” OR “transman” OR “transwoman” OR “lesbian” OR “gay” OR “queer” OR “bisexual” OR “pansexual”. Following a roughly chronological order of a patient’s care path and intersection with healthcare services, we summarized the findings from each of the included publications into the following categories: Early Care for SGM, Sexual Health, Family Planning, and Care Later in Life for SGM. We have compiled practice guidelines and clinical recommendations from established clinical organizations and group consensus. We did not restrict our search to any country and therefore included all relevant publications. The majority of articles focused on both sexual and gender minorities, often without distinguishing between the two, or discussing racial/ethnic and socioeconomic minority status. We retained the nomenclature used in the original articles for terminology when referring to the SOGI status of the population.
Early Care for SGM
SGM Youth
Limited knowledge of sexual and reproductive health concerns among SGM youth contributes to their relative invisibility in the healthcare system;7 however, there has been increased research interest and evidence on sexual health and fertility among SGM adolescents in recent years. The American Academy of Pediatrics, the Society of Adolescent Health and Medicine, and the Pediatric Endocrine Society support access to developmentally appropriate gender affirming care.10 SGM youth often experience gender identity with the same level of certainty as cisgender peers,7 and gender affirming care ideally begins before the onset of puberty or Tanner stage 2.11
Youth experiencing gender dysphoria benefit from resources and referrals provided in the primary care setting.11 Many transgender youth do not disclose their gender identity to their primary care physicians or pediatricians due to concerns about stigma and confidentiality.12 Significantly, those who did feel affirmed were also more likely to receive hormones and be linked with gender affirming care, indicating the importance of clinician training and preparedness.12
At every visit, clinicians should screen for mental health concerns, bullying, substance use, school dropout, and safety.10 It is often useful to screen for eating disorders as well, as transgender youth may use food restriction to delay pubertal development.7 Clinicians should also practice the principles of trauma informed care and explain the rationale for all sensitive questions.13 Table 1 and Table 2 provide recommendations for improving the clinical environment and clinical encounter for SGM patients.
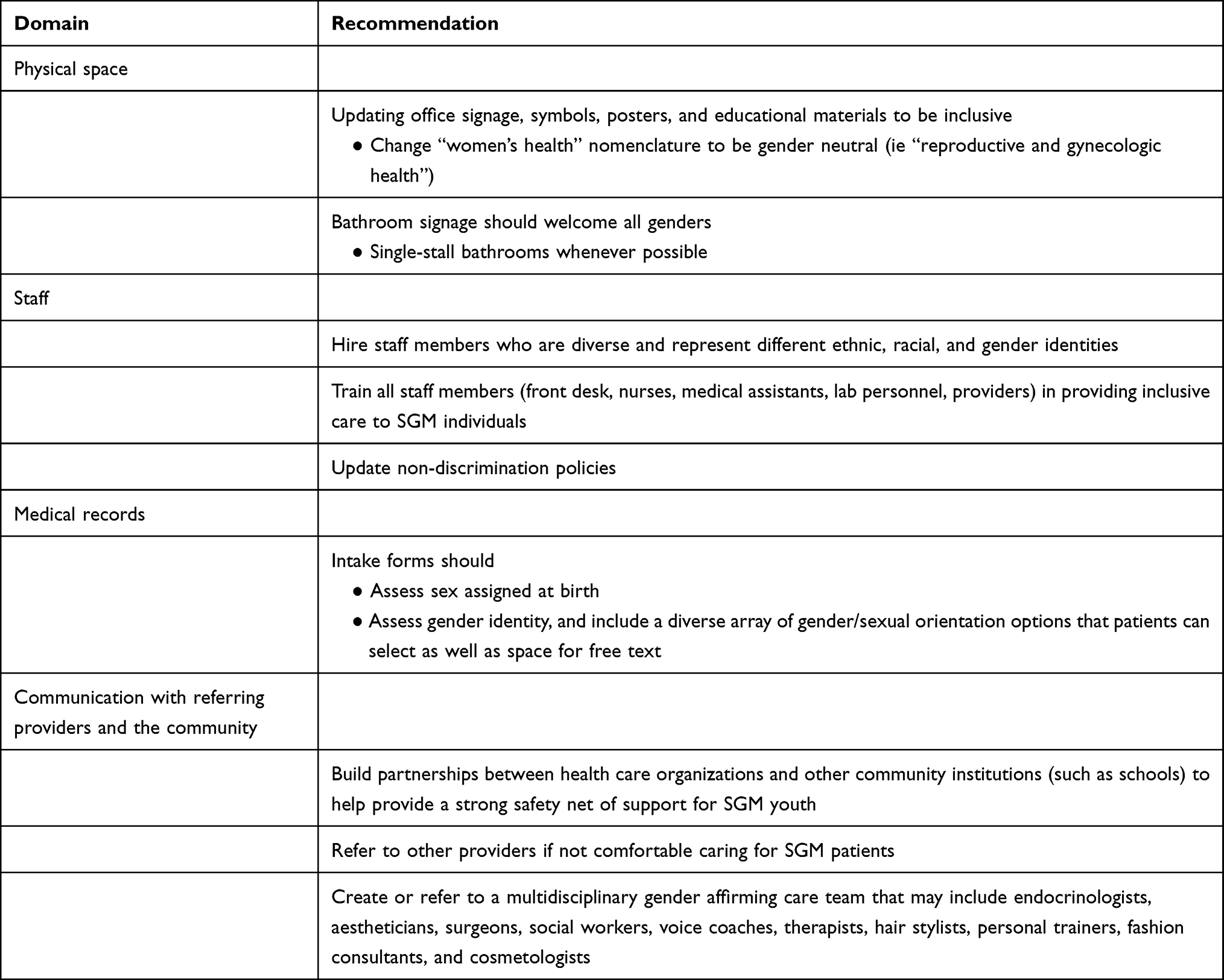 |
Table 1 Recommendations for Best Practices for Inclusive Environments and Advocacy for All SGM |
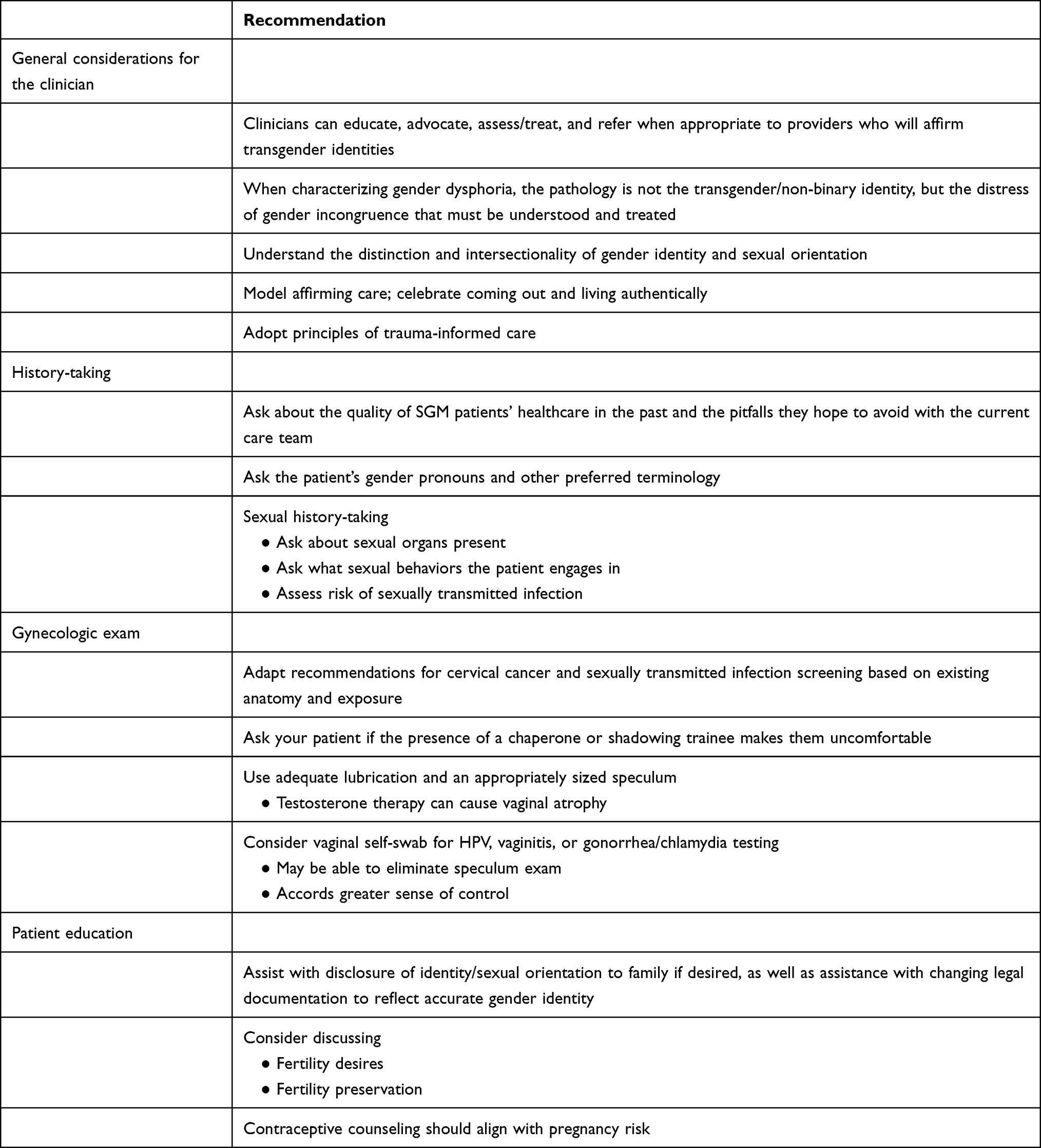 |
Table 2 Recommendations for Clinical Care for SGM |
Gender Affirming Hormone Therapy (GAHT)
Having positive self-regard is essential to SGM health and sexual function.11 At any point along the path of affirmative care, clinicians can make referrals and initiate management of dysphoria, such as providing information about safe chest binding, undergarment packing, and “stand-to-pee” devices, as well as initiating gender affirming medications. They can also refer to multidisciplinary professionals, including voice coaches, aestheticians, make-up artists, and stylists to help youth with social transition.
Prior to GAHT, gender minority adolescents had fewer sexual and romantic experiences than cisgender peers, though many reported having romantic feelings.14 Of the teens who reported sexual activity, only 50% involved their genitals due to concerns about dysphoria and poor self-image.14 After managing gender dysphoria through puberty suppression, hormones, and surgery, transgender teens had more sexual and romantic experiences within the year after surgery, improved body image and sexual satisfaction, and increased comfort with their genital anatomy.15
A survey of SGM youth showed that sexual initiation patterns were similar among SGM youths and cisgender adolescents, but SGM youth were more likely to have had multiple partners, have unprotected sex, and were slower to find romantic relationships.17 More than half (53.9%) of participants had engaged in at least one sexual behavior by age 18, and 40.8% had at least one gender minority partner.16 Social stressors – including concerns with passing as affirmed gender and body shame – tempered sexual behaviors, and many transgender youth responded that gender affirming therapy had caused changes in sexual desire.16
Sexual health education must include gender minority youth and their experiences. Inadequate and inaccurate sex education can lead to increased rates of sexually transmitted infections (STIs), unplanned pregnancy and unsafe sex. Fewer than 10% of SGM youth reported discussing such topics as STI testing; HIV stigma and pre-exposure prophylaxis (PrEP); contraception related to Lesbian, Gay, Bisexual, Transgender, Queer Plus (LGBTQ+) identity; or safe use of sex toys.17 Many reported that information about gender diversity and non-straight sexual orientation was omitted entirely, with so much emphasis on menstruation and fetal development that they felt shut out of asking questions about same-sex relationships and transgender health.18 Most gender minority youth endorsed LGBTQ+ peers as their primary source of information on sexual health and normalization of sexual behaviors, and the internet was often used as a supplementary resource, although sometimes inaccurate and poorly curated. Clinicians can become trusted resources for sexual health information by preparing to discuss these topics openly, without a heteronormative perspective, during clinic visits.17
Sexual Health
Sexually Transmitted Infections
Access to STI prevention, screening, and treatment is critically important to mitigating morbidity and promoting public health. Untreated STIs contribute significantly to sexual health related morbidity, community transmission and spread. However, access to STI testing and management is an unmet need in the SGM population, likely due to stigma and misinformation.19 A study of teens comparing sexual behaviors found that sexually active SGM teens were less likely than cisgender students to have used a condom during their most recent sexual encounter (47.3% of SGM teens versus 64.8% of cisgender teens).20 Youth report forgoing STI testing in part due to risk misperception, underestimating their vulnerability to STIs, as well as concerns about confidentiality.16
Effective STI risk assessment relies on an accurate sexual history that includes anatomy-specific exposures. Gender identity does not dictate anatomy or sexual behavior, and thus distinguishing subpopulations based on exposure is important for risk stratification.21 Clinicians should tailor STI screening and counseling for SGM individuals to their specific anatomy and sexual behaviors.
Recent data have estimated similar prevalence rates of gonorrhea and chlamydia among transgender men and cisgender men who have sex with men.22 Although the reported proportion of transmen who have undergone gender affirming surgery is low, clinicians should be mindful of anatomic diversity.23 Transmen may still have a uterus, cervix or vagina and be at risk for both bacterial and viral STIs, human papillomavirus (HPV) infections, and HPV-associated cervical cancer. All patients with a cervix should follow current screening guidelines for gonorrhea, chlamydia, and cervical cancer. Individuals should undergo syphilis as well as pharyngeal/rectal gonorrhea and chlamydia screening at least on an annual basis, based on reported sexual practices and exposure.24 Additionally, all patients should receive counseling and be offered HIV screening if desired, with frequency based on level of risk.
Epidemiological data suggest transgender people are three times more likely to contract HIV than the national average, and disparities in HIV prevalence highlight the intersectionality of gender minority, sexual minority, race and ethnicity.12,22,25 Recently estimated HIV prevalence in Black transwomen is 44–62% and in Latinx transwomen is 26–35%, whereas only 17% of white transwomen had HIV.7,19 Higher rates of HIV may be partially due to transactional high-risk sex related to homelessness, mental illness, and trafficking.13 Reduced access to medical care means transgender individuals report lower lifetime rates of HIV testing, especially compared with cisgender gay and bisexual men.12
In addition to widespread HIV screening with frequency based on level of risk, patients should be offered PrEP, approved by the FDA for all persons at risk for HIV acquisition weighing >35kg and with normal renal and hepatic function.13 The FDA also recently approved emtricitabine/tenofovir alafenamide as PrEP for sexually active cisgender men and transgender women, as well as extended release injectable cabotegravir.26 However, these medications have not yet been studied in those at risk for HIV acquisition through receptive vaginal sex.27
Barrier methods remain a mainstay of STI prevention. Clinicians should describe and teach the correct application of external and/or internal condoms as effective ways to prevent HIV and STI transmission. Using external condoms may be difficult for transgender women with reduced tumescence due to feminizing hormones.28 Transgender women may also lack agency to negotiate condom use during sex especially when engaging in transactional sex. Internal condoms may be an option for transgender men who engage in vaginal sex.28
Human Papillomavirus-Related Cancer Prevention
HPV is the most common sexually transmitted infection regardless of sexual orientation, and is the causative agent of the vast majority of cervical cancers. Cervical cancer is unique because there are methods for both primary prevention via vaccination against HPV as well as secondary prevention through well-established screening protocols with cervical cytology (Pap or Papanicolaou smear) and HPV testing. The HPV vaccine is routinely recommended as early as age 9 years (with the goal of vaccination prior to sexual debut); clinicians can offer HPV vaccination to all up to age 45. The recommendation for all individuals with a cervix is to begin screening at age 21 and undergo cytological testing every 3 years, followed by cytology and primary HPV testing every 5 years after age 30. Cancer prevention is a necessary medical service for all people, but often difficult to navigate for SGM patients.
Transgender men are 10 times less likely to have adequate cervical cancer screening compared with cisgender women.29,30 Moreover, cervicovaginal atrophy from exogenous testosterone use not only can make a speculum exam uncomfortable, limiting ability to collect a sufficient sample, but also may decrease the amount of viable cells adequate for interpretation.31 Patients with inadequate cytology then need a repeat sample to be appropriately screened.31 Transgender men are 8.3 times more likely to have inadequate cytology samples than cisgender women.29
In addition to screening for cervical cancer, clinicians should also complete anal cancer screening depending upon sexual exposures. Anal squamous cell carcinoma is similar to its cervical counterpart in that it is primarily caused by infection with HPV. The gold standard for anal cancer screening is high resolution anoscopy, but many clinicians begin screening with anal cytology – essentially a Pap test performed at the anus with a Q-tip-like collection system rather than a cytobrush. While there are no formal guidelines regarding anal cancer screening, the following groups should be screened: those who engage in penetrative anal sex, individuals with HIV, individuals with cervical/vulvar/vaginal dysplasia or cancer, those individuals on long-term immunosuppression (such as organ transplant recipients), and individuals infected with HPV 16.31
Gynecologists and other clinicians who perform Pap tests should create an environment that is inclusive of SGM patients and shows respect for privacy (Table 1).32 In many clinical practices, chaperones (often a medical assistant or nurse) are present for all pelvic exams. However, several studies found that transgender men sometimes felt uncomfortable with perceived chaperone voyeurism.33 We summarize recommendations for best practices during a clinical encounter in Table 2.
To improve the experience for SGM individuals, clinicians should use adequate lubrication and appropriately sized speculums, as they would for postmenopausal cisgender women with vaginal atrophy. Primary HPV testing via self-swabbing eliminates the speculum exam altogether. Self-collected vaginal swabs accord an increased sense of control, which many transgender men prefer. Furthermore, all office staff should be committed to ensuring an inclusive experience for all patients, including SGM individuals. All staff members (front desk staff, nurses, medical assistants, clinicians) should be trained and educated in the care of and concerns specific to SGM individuals.30,31,33
Healthcare providers should build rapport with patients such that they are comfortable reporting symptoms that may be concerning for gynecologic cancers, such as pelvic pain, abnormal uterine bleeding, or bloating. The LOvE ECHO training program, a web-based SGM cultural competency training, offers communication strategies to improve reproductive health discussions with SGM people.34
Measuring Sexual Function
Sexual function is an important component of sexual health; however, few validated instruments exist for the transgender population. Measuring sexual function should account for sexual desire/satisfaction, lubrication, orgasm, genital self-image, ease/difficulty initiating and seeking sexual contact, shame, body distortion, and other psychosocial factors.35 Accurate assessment of sexual function is essential for providing appropriate care for gender dysphoria and optimizing patient outcomes before and after gender affirming hormonal therapy and/or surgery. Recent literature attempting to characterize sexual function in transgender participants has been limited by survey tools originally designed for cisgender/heterosexual participants (Table 3).
 |
Table 3 Sample of Instruments to Measure SGM Sexual Health and Function |
Transgender individuals are more likely to have painful intercourse, poor genital self-image, and body image distortion than cisgender people.36,37 More inclusive and careful terminology with survey items – ideally defined by the transgender community – should be the standard. Such terminology recognizes that gender identity and sexual orientation are distinct, and that sexual function may depend on partner identification. In systematically describing transgender sexual function, clinician assessments should account for pharmacological treatment for depression and psychological sequelae of sexual trauma. Accurate assessment of sexual function can determine the kind of care SGM patients need to optimize sexual health and wellbeing.37 Without careful consideration of trans-specific nuances of sexual function, transgender individuals can be wrongly pathologized according to cisgender heteronormative standards.
Family Planning
Practice Setting
Historically, OB/GYNs provided the majority of reproductive health care for individuals with the capacity to become pregnant, with a smaller proportion of this care occurring in primary care settings. People may experience OB/GYN offices and freestanding abortion clinics as gendered spaces, especially given the proportion of cisgender women these practices serve. Nonetheless, SGM individuals use contraception, experience unwanted pregnancy, and have abortions, but many face barriers to seeking care for reasons such as lack of insurance/financial hardship, discrimination, mistreatment, or lack of knowledge/experience among providers and within health care settings.38,39 Several sources detail actions that health centers and clinicians can take to create and maintain an inclusive, safe environment for SGM individuals,40,41 which we have also outlined in Tables 1, 2 and 4.
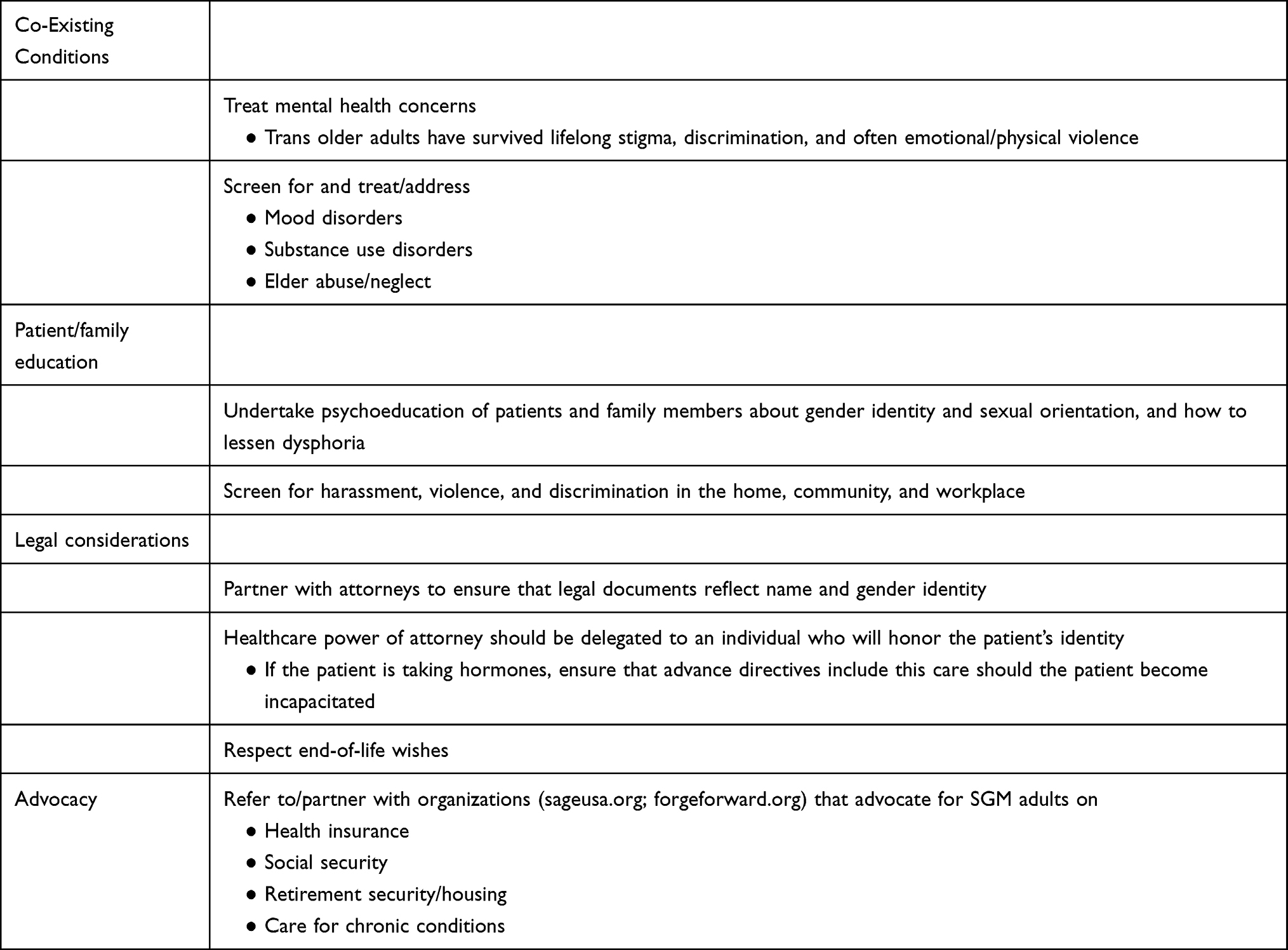 |
Table 4 Recommendations for Care for Older SGM Adults |
Contraceptive Use Among SGM Individuals
Some SGM individuals have undergone a hysterectomy or are not engaging in sexual activity that could lead to pregnancy. Clinicians should foster a safe, patient-centered environment in which pregnancy risk is assessed and contraceptive use matches that risk. Individuals wishing to avoid pregnancy may experience barriers to contraceptive use related to: accessing healthcare in safe and culturally relevant practice settings, lack of knowledge or misperceptions of pregnancy risk, clinicians’ lack of knowledge regarding risk of pregnancy and interaction of gender-affirming testosterone with hormonal contraception, and gender dysphoria with contraception use.38,42
Published studies report variable contraception use among SGM individuals, including adolescents and young adults; however, the settings from which respondents were sampled may have introduced bias. Contraceptive use was higher among cisgender/heterosexual college students,43 for example, compared with SGM individuals recruited from other settings.44 While SGM college students most often reported using the subdermal implant, intrauterine device (IUD) and condoms, respondents recruited from a LGBTQ+ health center and online reported using condoms, withdrawal or oral contraceptives.45
Testosterone and Hormonal Contraception
Some transgender men take gender-affirming testosterone, which can induce amenorrhea within months.13 Some individuals taking testosterone may equate amenorrhea with sterility. However, testosterone does not reliably inhibit ovulation and is a known teratogen.46 Endometrial proliferation also occurs in a spectrum of conditions where androgen excess is a risk factor, as with polycystic ovarian syndrome, endometrial hyperplasia, and endometrial cancer. Histologic examination of hysterectomy specimens from individuals taking testosterone frequently demonstrate proliferative endometrium.47 Breakthrough bleeding in the setting of testosterone therapy most often has no identifiable cause, but is sometimes associated with missed testosterone doses.48 Hormonal therapy may be considered to treat breakthrough bleeding, similar to its use for menstrual suppression, but no evidence exists in support of any particular approach.49
There are no data describing potential interactions between testosterone therapy and hormonal contraception. Society of Family Planning Clinical Guidelines recommend considering what is known about these therapies separately to guide clinical decision-making.40 Contraceptive methods often have specific expected bleeding profiles and side effects that individuals may find important. Two excellent guidelines consider these characteristics in greater detail, and address them from both the user’s and prescriber’s perspectives.40,48
Combined Hormonal Contraception
Combined hormonal contraception (CHC) contains estrogen and progestin, which provide excellent ovulation suppression and predictable bleeding or, if taken continuously, reliable bleeding suppression. The estrogen component (usually ethinyl estradiol or EE) suppresses follicle stimulating hormone and contributes to cycle control, whereas the progestin component suppresses the surge of luteinizing hormone (LH) needed for ovulation to occur. CHCs may be delivered in the form of pills, transdermal patches, or vaginal rings.
Although estrogen may be perceived as a feminizing hormone, CHCs are not likely to raise estrogen levels for individuals not taking testosterone or gonadotropin releasing hormone agonists.13 Most progestins used in combined pills are derived from androgens, with some notable exceptions such as drospirenone, which is derived from spironolactone and has anti-androgenic properties. In the United States (US), the two available contraceptive patches contain EE and a testosterone-derived progestin. Individuals who find a vaginal ring acceptable may opt for a monthly ring (EE/etonogestrel), which can be used continuously to suppress menses, or one that contains sufficient hormone for 13 cycles (EE/segesterone acetate). Serum EE levels are lower in vaginal ring users compared with patch users.
Progestin-Only Contraception
Progestin-only contraception may be acceptable to individuals who wish to avoid estrogen or who have a contraindication such as migraine with aura, hypertension, or who otherwise have an elevated baseline risk for venous thromboembolism.
Two progestin-only pills are available in the US. Norethindrone is taken continuously and suppresses ovulation in approximately half of people who use it. Drospirenone is also available as a progestin-only pill, with a 28-day supply containing 24 active pills and 4 inactive pills. This regimen reliably suppresses ovulation.
Depot medroxyprogesterone acetate (DMPA) is an injectable contraceptive dosed every 12–14 weeks. Users may opt for a subcutaneous formulation, which allows for self-administration and therefore, less frequent contact with health care providers. About half of users will experience amenorrhea after one year.50
The etonogestrel implant has the lowest failure rate of all contraceptive methods and does not require a pelvic exam. Bleeding is sometimes irregular in cisgender women, though expert clinicians have found that individuals taking testosterone may experience more favorable bleeding patterns.13
Four different levonorgestrel IUDs are available. Those who have IUDs with higher doses of progestin (52mg) are more likely to experience amenorrhea. Placement requires a pelvic examination.
Copper Intrauterine Device
The copper IUD does not contain hormones, and thus may be more acceptable to some individuals. However, heavier and prolonged menses occur in some copper IUD users. Limited evidence suggests that individuals on testosterone who had no bleeding at the time of copper IUD placement experienced some bleeding following the procedure, and subsequently had no further bleeding.51
Barrier Methods
Internal and external condoms are the most commonly used barrier methods, are user-controlled, and confer protection from sexually transmitted infections. They require consistent use and partner cooperation to maximize effectiveness.
Emergency Contraception
Both the copper and 52mg levonorgestrel IUDs can serve as emergency contraception when placed within 5 days of intercourse that could result in pregnancy. These options are effective regardless of body mass index (BMI), whereas levonorgestrel 1.5mg orally decreases in effectiveness with increasing BMI. Unlike levonorgestrel, ulipristal acetate (UPA) has some effectiveness in preventing or delaying ovulation after the LH surge.52 Oral levonorgestrel is available over the counter; clinicians should provide advance prescriptions for UPA if possible. For pharmacologic options, the potential benefit of pregnancy prevention far outweighs risks associated with levonorgestrel and UPA, which are small.
Permanent Contraception
Clinicians should consider any request for permanent contraception seriously. Some individuals desire gender-affirming hysterectomy, particularly if future fertility is not desired. Hysterectomy should not be a requirement for hormonal transition but is for genital surgery.48 A patient-centered discussion should explore plans and desires for future fertility, the risk of regret, and procedural risks.
Abortion Among SGM Individuals
Although a variety of state and non-governmental organizations collect demographic data on individuals who have abortions, health care facilities are not always required to report a patient’s gender or sexual orientation. The true proportion of abortions that occur in SGM individuals in the US is unknown. However, surveys of SGM people indicate that they experience both desired and undesired pregnancies.39 Discrimination, marginalization, problems with access, cost, and desire for privacy are all potential factors influencing the decision to obtain abortion care or to manage an unwanted pregnancy without medical supervision.53 Given the Supreme Court Dobbs v. Jackson Women’s Health Organization (2022) decision, access to abortion in the US will vary widely by state.54
Limited published survey data indicate that abortions mainly occur in the first trimester and are mostly procedural or completed with medications, with a small proportion of people using a different method (such as herbs, physical trauma, or substance use). Privacy concerns may drive a preference for medication abortion, in which individuals use mifepristone (a selective progesterone antagonist) and misoprostol (a prostaglandin) to stop a pregnancy’s progress and expel it. People may perceive medication abortion as more natural, less invasive, and conferring autonomy to the individual. Provision via telehealth with no-test protocols, in which ultrasound and laboratory testing are not required for individuals meeting certain criteria, further protect privacy and facilitate access.55 Alternatively, individuals may prefer to obtain medications on their own and take them without medical supervision. Self-managed medication abortion represents an option that can be more private, logistically and financially feasible, and for some, empowering. Conversely, the heavy bleeding that occurs with medication abortion may cause distress for other individuals, who might instead prefer the relative speed of a procedural abortion.
It is essential to counsel SGM patients that gender affirming hormone treatment is not contraception.40 SGM youth experience unplanned pregnancy at a rate 2–10 times higher than heterosexual youth, with a Canadian study reporting that 28% of SGM identified youth had been involved with an unplanned pregnancy compared with 7% of heterosexual teens.56 Reasons for this difference may include earlier sexual debut, sexual assault, or an overall higher number of sexual partners. SGM youth have about the same risk for unplanned pregnancy as cisgender peers.21
We are not aware of published guidelines addressing clinical aspects of abortion care specific to SGM individuals. While standards of care concerning such matters as gestational age assessment, infection prevention, and cervical preparation apply to all individuals seeking abortion, medical professionals providing this care should follow established best practices in maintaining an inclusive practice setting that respects patient privacy (Table 1). Clinicians should encourage open discussions of how aspects of medication and abortion procedures (including any pelvic exams or ultrasound evaluation, analgesia, and anesthesia) may personally affect SGM people (Table 2).
Fertility
Those who desire biological parenthood must consider potential long-term impacts of gender affirming hormonal treatment; while theoretically more easily reversed than surgery, hormonal effects on gonadal tissue and gametes are still largely unknown.57 More than 80% of transgender youth did not discuss hormonal effects on fertility with healthcare providers.13 Clinicians should discuss family planning goals and fertility preservation, if appropriate, prior to initiating GAHT.13
Recent data indicate that SGM youth have similar fertility goals to cisgender peers,58 but rates of fertility preservation prior to gender affirming hormones or surgery are low. Only 0–2% of transmasculine and 8–14% of transfeminine youth currently have preserved gametes, due in part to the dysphoria induced by gamete collection, hesitance to delay puberty suppression/GAHT while preparing for retrieval, and concern over costs of these services.13,59 About a third of transmen and half of transwomen have indicated that they would have preserved gametes if such services were available and affordable prior to transition.13
With the development of safe puberty suppression techniques, youth should consider fertility goals prior to initiation of medical management for gender dysphoria. SGM youth born with testicles can provide samples by masturbation or assisted ejaculation. Surgical sperm retrieval and cryopreservation of testicular tissue at earlier Tanner stages are currently under investigation.13 SGM youth born with ovaries can achieve fertility preservation with oocyte and/or ovarian tissue cryopreservation. Testosterone must be stopped for at least 1–3 months prior to ovarian hyperstimulation and egg retrieval. However, barriers to fertility preservation include lack of insurance coverage for these procedures as well as dysphoria. Frequent pelvic ultrasounds are required and the oocyte retrieval procedure, though usually performed with sedation, is guided by transvaginal ultrasound.13
Outside of biological parenthood and fertility preservation, adoption is a popular method of parenthood for SGM youth.44 Clinicians should counsel SGM youth and their families that there may be barriers including high costs and cis-sexism associated with the adoption process, but that adoption is a valid method of achieving parenthood when fertility preservation is undesired or untenable.44
Pregnancy in SGM
Although the prevalence of SGM patients who have achieved pregnancy is unknown, it is likely to increase in coming years.60 Person-centered and gender affirmative prenatal, intrapartum, and postpartum care for SGM patients should be within the scope of any obstetric provider.
Overall, prenatal care for SGM should follow guidelines for all pregnant patients, with a few additional considerations. Many transgender men believe testosterone to be effective birth control given its amenorrheic effect; however, testosterone is teratogenic and can cause abnormal urogenital development in biologically female fetuses.61 Patients who desire pregnancy should stop testosterone prior to conception if possible, or soon after desired positive pregnancy test.62 Similarly, lactating patients may experience diminished milk supply if taking testosterone, and options for donor milk should be considered if testosterone therapy is highly desired in the postpartum period.60 If SGM patients desire biological children but are unable to stop GAHT, they should undergo embryo or oocyte cryopreservation prior to initiating GAHT for IVF pregnancy with a carrying partner or surrogate later on.
Intrapartum or labor pain can exacerbate dysphoria some patients experience; obstetricians should offer early intrapartum pain control and/or elective cesarean delivery to mitigate the harmful effects of dysphoria.62 Clinicians should strive to avoid sensitive exams when possible for patients who do not identify with their sex organs and the traditionally gendered experience and embodiment of motherhood.
Pregnancy can be empowering but more often highly dysphoric for SGM patients. Doulas and support groups can provide patients with encouragement and an affirmative labor experience. Screening for depression, anxiety, dysphoria, and suicidality is essential as this patient population is at increased risk and may experience further isolation and loneliness from navigating the social intricacies of transmasculine pregnancy.60 Mental health providers and social workers should be brought to the prenatal care team early and frequently throughout the course of pregnancy and the postpartum period to screen for and support mental health concerns.
Care Later in Life for SGM
Older SGM adults face some of the same health concerns as older cisgender or heterosexual adults, but little health data exist on the impact of lifelong hormonal therapy and surgical gender affirmation for the SGM aging population. In general, the World Professional Association for Transgender Health (WPATH) Standards of Care indicate that transgender patients should be screened for cardiovascular disease, osteoporosis, and risk factors for cancers including breast, cervical, ovarian, uterine, and prostate.11 The US Preventive Services Task Force similarly indicates that no data suggest that screening for transgender adults should deviate from cisgender adults based on age and organs.63,64 Transgender individuals should receive the same basic health management and age-related screenings as cisgender adults.
However, systematic exclusion from employment opportunities, unstable health insurance and access to preventive health care, increased rates of smoking, risky sexual behaviors, and substance use may worsen outcomes overall.65 Transgender adults often experience more loneliness, less financial security, and worse health outcomes compared with cisgender adults.66 Transgender adults also fare worse than their cisgender counterparts with chronic health conditions like low back pain, immune compromise, heart attack, asthma, stroke, and arthritis.67
Few data exist on long-term outcomes for transgender adults on continuous hormone therapy. Many transgender adults use hormonal therapy for decades and up until the end of life.63 Hormone therapy plans should be individualized for each patient and advanced age alone is not a contraindication to its initiation. Although there are certain known risks with hormone therapy (estrogen can increase risk of deep vein thromboses, breast cancer, and pulmonary embolism; testosterone can worsen liver disease, risk for diabetes, and risk for cardiovascular disease),66 continuing hormonal therapy into old age can improve hyperlipidemia and prevent insulin resistance for those who take estrogen.63 Despite gaps in long-term data on outcomes for patients on hormonal therapy, some recommendations are standard. Transdermal estrogen is least thrombogenic and preferred over ethinyl estradiol, which should be avoided in individuals with risk factors for thrombotic events. Individuals can use lower doses of estrogen if treated concomitantly with androgen-lowering agents such as spironolactone.68
Many older adults have had or are considering gender affirming surgery, some even at retirement age.69 Discussion on maintaining sexual organ health after surgery (for example, how often and for how long one should dilate a neovagina) should be individualized as no standard protocol exists. Post-surgical patients should be aware of and screened for post-operative functional disorders including rectovaginal fistulas and urinary tract infections.11
Finally, clinicians cannot adequately address health concerns and decisions in older SGM adults without understanding the ecological systems that have affected SGM lives for decades. Years of physical, emotional, and mental trauma from stigma and discrimination yield poor self-esteem, internalized transphobia, and under- or unemployment leading to inadequate health insurance. A 2015 survey found that 25% of trans adults had suboptimal healthcare due to issues with insurance coverage (including denial of hormone therapy), and up to a third of respondents avoided healthcare because they feared stigmatization, verbal and even physical assault, and had bad experiences having to teach providers about trans health.69
Older SGM adults have survived decades of stigma and oppression. The oldest cohorts of LGBTQ+ individuals came of age hearing that homosexuality was pathologic and criminalized. In the US for example, transgender adults have dealt with “gender identity disorder and transvestic fetishism” diagnoses per the DSM-V up until 2013, and gender dysphoria – though used to justify insurance payments for gender affirming services – is still listed as a psychiatric disorder.70
Transphobia converges with ageism, heterosexism, and racism to create a multiplied oppressive effect over the years.67 Rejection and marginalization by clinicians, friends, family, and even their own children cause SGM adults to suffer from poorer physical health later in life. It cannot be overstated that according to the Care and Aging with Pride study, 71% of transgender participants endorsed lifetime suicidal ideation.69 Screening for and treating mental health concerns in the aging transgender population, as well as all SGM people, saves lives.
Conclusion
The “gendering” of health care can deter SGM people from seeking sexual healthcare; in some cases, the rigidity of a traditional binary framework can actively harm patients by creating stigma, discrimination, and “otherness.” Transgender men may find a clinic with the name Women’s Health Services unapproachable; similarly, transgender women may not engage in preventive prostate cancer care when they do not identify with traditional male anatomy. Absent training or engagement in SGM inclusive healthcare can lead to missed opportunities to support early conversations for gender affirming care and sex education, help mitigate or prevent gender-based violence or bullying, and initiate discussion of family planning goals.
In this narrative review, we began with a discussion of early SGM care. Timely identification and initiation of gender affirming care for SGM youth is crucial for consideration of GAHT and/or surgery. Since sexual orientation and gender identity can be fluid, assessing SOGI regularly at every visit is key to providing patient-centered care. SGM youth may have issues related to mental health or body image that prevent quality sexual encounters and relationships. Clinicians should offer guidance and referrals, and regularly screen for potential suicidal ideation, self-harm, abuse and bullying.
SGM inclusive care also allows for open discussion and accurate assessment of sexual function and quality of life, optimizing sexual health and wellbeing throughout the lifespan. Establishing a supportive environment allows for conversation about relevant sex education as well as STI screening and prevention. Effective STI risk assessment relies on an accurate sexual history that includes anatomy-specific exposures and sexual practices. Similarly, HPV-related cancer prevention and screening for SGM individuals should note the importance of age, anatomy, and sexual behaviors as considerations for quality care.
Concurrent discussion of family planning goals should be tailored to the SGM individual’s current anatomy, other medications, sexual behaviors and desires for future fertility. Preventing unwanted pregnancy is important for SGM people of reproductive age, particularly as GAHT is often misperceived as a form of contraception. Additionally, individuals may be reluctant to disclose sexual orientation, gender identity and sexual behaviors to clinicians due to fears of stigma and discrimination. Although abortion continues to be a volatile issue in the US, the need for compassionate care remains. SGM people of reproductive age are at increased risk for facing financial and logistic challenges, as well as discrimination, in seeking abortion services. Self-managed abortion or obtaining services within the formal healthcare system via telemedicine are two options that may expand access. Similarly, those seeking to build families should have access to honest and person-centered discussions about options for gamete preservation, pregnancy, and adoption.
Finally, we turn our attention to SGM care later in life. Clinicians should be cognizant of the historically cis- and hetero-normative healthcare systems that older SGM patients may have experienced. Internalized stigma and suspicion of the healthcare establishment can color clinical interactions. Intersectionality with systemic racism and classism further marginalize patients. Overall, transgender adults should undergo basic health management and screening as cisgender adults, based on age and anatomy. More research is needed, however, on the role of continuous GAHT on the aging process.
We provide a comprehensive assessment of the literature on considerations for improving sexual healthcare for SGM of all ages; however, our narrative review has limitations. The included studies used a variety of nomenclature, but we used the term SGM to include all people not considered cisgender or heterosexual. Some studies were exclusive to transgender identified people but did not include sexual orientation. Moreover, while our search returned over 2000 publications on this topic, it was not possible to review each publication in depth. We aimed to include citations from the most recent studies that assessed gender minorities, with some studies that assessed both gender and sexual minorities. The majority of the included literature derives from US-based and European studies, where active research on gender affirming care and surgeries have occurred. Many of the findings on practice guidelines and clinical considerations are nonetheless applicable to settings beyond the US. Finally, we are aware of our authorship biases, including caring primarily for individuals assigned female at birth, that may factor into our clinical consensus on guidelines and recommendations delineated in our narrative review.
Clinicians should strive to provide person-centered sexual and reproductive healthcare throughout the lifespan. Provision of such care includes creating a welcoming environment, SGM inclusive training for clinicians and staff, and individualized counseling based on current gender identity and sexual orientation. At each point on the path of comprehensive affirmative care, clinicians should consider diverse gender identity and non-heteronormative sexual practices, family planning, sexually transmitted infections, cancer prevention, and sexual health. As we move toward more inclusive practices in medicine, it is imperative that we no longer comply with the rigid boundaries of binary gendered language, and employ measures of sexual function and quality of life that are relevant for and respectful of SGM people, and aimed at maximizing sexual health and well-being.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mehta PK, Easter SR, Potter J, Castleberry N, Schulkin J, Robinson JN. Lesbian, gay, bisexual, and transgender health: obstetrician-gynecologists’ training, attitudes, knowledge, and practice. J Womens Health. 2018;27(12):1459–1465. doi:10.1089/jwh.2017.6912
2. Klein A, Golub SA. Enhancing gender-affirming provider communication to increase health care access and utilization among transgender men and trans-masculine non-binary individuals. LGBT Health. 2020;7(6):292–304. doi:10.1089/lgbt.2019.0294
3. Sutter ME, Bowman-Curci ML, Duarte Arevalo LF, Sutton SK, Quinn GP, Schabath MB. A survey of oncology advanced practice providers’ knowledge and attitudes towards sexual and gender minorities with cancer. J Clin Nurs. 2020;29(15–16):2953–2966. doi:10.1111/jocn.15302
4. Mulac A, Wiemann JM, Widenmann SJ, Gibson TW. Male/female language differences and effects in same‐sex and mixed‐sex dyads: the gender‐linked language effect. Commun Monogr. 1988;55(4):315–335. doi:10.1080/03637758809376175
5. Reczek C. Sexual- and gender-minority families: a 2010 to 2020 decade in review. J Marriage Family. 2020;82(1):300–325. doi:10.1111/jomf.12607
6. Alexander R, Parker K, Schwetz T. Sexual and gender minority health research at the national institutes of health. LGBT Health. 2016;3(1):7–10. doi:10.1089/lgbt.2015.0107
7. Sherer I, Hanks M. Affirming pediatric care for transgender and gender expansive youth. Pediatr Ann. 2021;50(2):e65–e71. doi:10.3928/19382359-20210115-01
8. Pregnall AM, Churchwell AL, Ehrenfeld JM. A call for LGBTQ content in graduate medical education program requirements. Acad Med. 2021;96(6):828–835. doi:10.1097/ACM.0000000000003581
9. Rubin R. Minimizing health disparities among LGBT patients. JAMA. 2015;313(1):15–17. doi:10.1001/jama.2014.17243
10. Voss RV, Simons L. Supporting the health of transgender and gender-diverse youth in primary care settings. Prim Care. 2021;48(2):259–270. doi:10.1016/j.pop.2021.02.003
11. The World Professional Association for Transgender Health. Standards of care for the health of transsexual, transgender, and gender nonconforming people; 2011. Available from: www.wpath.org.
12. Fisher CB, Fried AL, Desmond M, Macapagal K, Mustanski B. Perceived barriers to HIV prevention services for transgender youth. LGBT Health. 2018;5(6):350–358. doi:10.1089/lgbt.2017.0098
13. Mehringer J, Dowshen NL. Sexual and reproductive health considerations among transgender and gender-expansive youth. Curr Probl Pediatr Adolesc Health Care. 2019;49(9):100684. doi:10.1016/j.cppeds.2019.100684
14. Bungener SL, Steensma TD, Cohen-Kettenis PT, de Vries ALC. Sexual and romantic experiences of transgender youth before gender-affirmative treatment. Pediatrics. 2017;139(3):e20162283. doi:10.1542/peds.2016-2283
15. Bungener SL, de Vries ALC, Popma A, Steensma TD. Sexual experiences of young transgender persons during and after gender-affirmative treatment. Pediatrics. 2020;146(6):e20191411. doi:10.1542/peds.2019-1411
16. Maheux AJ, Zhou Y, Thoma BC, Salk RH, Choukas-Bradley S. Examining sexual behavior among U.S. transgender adolescents. J Sex Res. 2021;58(8):1050–1060. doi:10.1080/00224499.2020.1855408
17. Haley SG, Tordoff DM, Kantor AZ, Crouch JM, Ahrens KR. Sex education for transgender and non-binary youth: previous experiences and recommended content. J Sex Med. 2019;16(11):1834–1848. doi:10.1016/j.jsxm.2019.08.009
18. Chong LSH, Kerklaan J, Clarke S, et al. Experiences and perspectives of transgender youths in accessing health care: a systematic review. JAMA Pediatr. 2021;175(11):1159–1173. doi:10.1001/jamapediatrics.2021.2061
19. Centers for Disease Control and Prevention. HIV and transgender people: HIV prevalence. Centers for Disease Control and Prevention; 2022. Available from: https://www.cdc.gov/hiv/group/gender/transgender/hiv-prevalence.html.
20. Andrzejewski J, Pampati S, Johns M, Sheremenko G, Lesesne C, Rasberry C. Sexual behaviors, referral to sexual health services, and use of sexual health services among transgender high school students. J School Health. 2020;90:349–357. doi:10.1111/josh.12880
21. Safer JD, Tangpricha V. Care of the transgender patient. Ann Intern Med. 2019;171(1):ITC1–ITC16. doi:10.7326/AITC201907020
22. Becasen JS, Denard CL, Mullins MM, Higa DH, Sipe TA. Estimating the prevalence of HIV and sexual behaviors among the US transgender population: a systematic review and meta-analysis, 2006–2017. Am J Public Health. 2019;109(1):e1–e8. doi:10.2105/AJPH.2018.304727
23. USTS reports. 2022 U.S. trans survey. Available from: https://www.ustranssurvey.org/reports.
24. Deutsch M. Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people | Gender affirming health program. Available from: https://transcare.ucsf.edu/guidelines.
25. Tordoff DM, Dombrowski JC, Ramchandani MS, Barbee LA. Trans-inclusive sexual health questionnaire to improve HIV/STI care for transgender patients: anatomic-site specific STI prevalence & screening rates. Clin Infect Dis. 2022;ciac370. doi:10.1093/cid/ciac370
26. FDA. FDA approves first injectable treatment for HIV pre-exposure prevention; 2021. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-first-injectable-treatment-hiv-pre-exposure-prevention.
27. Mayer KH, Molina JM, Thompson MA, et al. Emtricitabine and tenofovir alafenamide vs emtricitabine and tenofovir disoproxil fumarate for HIV pre-exposure prophylaxis (DISCOVER): primary results from a randomised, double-blind, multicentre, active-controlled, Phase 3, non-inferiority trial. Lancet. 2020;396(10246):239–254. doi:10.1016/S0140-6736(20)31065-5
28. Poteat TC, Radix A. HIV antiretroviral treatment and pre-exposure prophylaxis in transgender individuals. Drugs. 2020;80(10):965–972. doi:10.1007/s40265-020-01313-z
29. Peitzmeier SM, Khullar K, Reisner SL, Potter J. Pap test use is lower among female-to-male patients than non-transgender women. Am J Prev Med. 2014;47:808–812. doi:10.1016/j.amepre.2014.07.031
30. Domogauer J, Cantor T, Quinn G, Stasenko M. Disparities in cancer screenings for sexual and gender minorities. Curr Probl Cancer. 2022;46:100858. doi:10.1016/j.currproblcancer.2022.100858
31. Nisly NL, Imborek KL, Miller ML, Kaliszewski SD, Williams RM, Krasowski MD. Unique primary care needs of transgender and gender non-binary people. Clin Obstet Gynecol. 2018;61(4):674–686. doi:10.1097/GRF.0000000000000404
32. Daly A, Champion JD. Creating inclusive health care environments: health care stories from the trans population. J Am Assoc Nurse Pract. 2020;33(6):451–458. doi:10.1097/JXX.0000000000000383
33. Dhillon N, Oliffe JL, Kelly MT, Krist J. Bridging barriers to cervical cancer screening in transgender men: a scoping review. Am J Mens Health. 2020;14(3):1557988320925691. doi:10.1177/1557988320925691
34. Block RG, Sampson A, Gagliardi J, et al. The LOvE ECHO training: developing a web-based LGBTQ cultural competency training module for oncology allied health professionals. J Adolesc Young Adult Oncol. 2022;11:556–563. doi:10.1089/jayao.2021.0159
35. Vedovo F, Di Blas L, Aretusi F, et al. Physical, mental and sexual health among transgender women: a comparative study among operated transgender and cisgender women in a national tertiary referral network. J Sex Med. 2021;18(5):982–989. doi:10.1016/j.jsxm.2021.02.006
36. Barcelos TMR, Ferreira CHJ, Lerri MR, et al. Sexual function of transgender women after gender affirming surgery: a mini review. Clin Anat. 2022;35(5):560–570. doi:10.1002/ca.23863
37. Kerckhof ME, Kreukels BPC, Nieder TO, et al. Prevalence of sexual dysfunctions in transgender persons: results from the ENIGI follow-up study. J Sex Med. 2019;16(12):2018–2029. doi:10.1016/j.jsxm.2019.09.003
38. Gomez AM, Đỗ L, Ratliff GA, Crego PI, Hastings J. Contraceptive beliefs, needs, and care experiences among transgender and nonbinary young adults. J Adolesc Health. 2020;67(4):597–602. doi:10.1016/j.jadohealth.2020.03.003
39. Moseson H, Fix L, Hastings J, et al. Pregnancy intentions and outcomes among transgender, nonbinary, and gender-expansive people assigned female or intersex at birth in the United States: results from a national, quantitative survey. Int J Transgend Health. 2021;22(1–2):30–41. doi:10.1080/26895269.2020.1841058
40. Bonnington A, Dianat S, Kerns J, et al. Society of family planning clinical recommendations: contraceptive counseling for transgender and gender diverse people who were female sex assigned at birth. Contraception. 2020;102(2):70–82. doi:10.1016/j.contraception.2020.04.001
41. Fix L, Durden M, Obedin-Maliver J, et al. Stakeholder perceptions and experiences regarding access to contraception and abortion for transgender, non-binary, and gender-expansive individuals assigned female at birth in the U.S. Arch Sex Behav. 2020;49(7):2683–2702. doi:10.1007/s10508-020-01707-w
42. Karrington B. The experiences of transmasculine people with contraception and menstruation: a literature review of qualitative and mixed method studies. Transgend Health. 2021;6(6):303–314. doi:10.1089/trgh.2020.0047
43. Reynolds CA, Charlton BM. Sexual behavior and contraceptive use among cisgender and gender minority college students who were assigned female at birth. J Pediatr Adolesc Gynecol. 2021;34(4):477–483. doi:10.1016/j.jpag.2021.03.009
44. Stark B, Hughto JMW, Charlton BM, Deutsch MB, Potter J, Reisner SL. The contraceptive and reproductive history and planning goals of trans-masculine adults: a mixed-methods study. Contraception. 2019;100(6):468–473. doi:10.1016/j.contraception.2019.07.146
45. Light A, Wang LF, Zeymo A, Gomez-Lobo V. Family planning and contraception use in transgender men. Contraception. 2018;98(4):266–269. doi:10.1016/j.contraception.2018.06.006
46. Taub RL, Ellis SA, Neal-Perry G, Magaret AS, Prager SW, Micks EA. The effect of testosterone on ovulatory function in transmasculine individuals. Am J Obstet Gynecol. 2020;223(2):229.e1–229.e8. doi:10.1016/j.ajog.2020.01.059
47. Grimstad FW, Fowler KG, New EP, et al. Uterine pathology in transmasculine persons on testosterone: a retrospective multicenter case series. Am J Obstet Gynecol. 2019;220(3):257.e1–257.e7. doi:10.1016/j.ajog.2018.12.021
48. Krempasky C, Harris M, Abern L, Grimstad F. Contraception across the transmasculine spectrum. Am J Obstet Gynecol. 2020;222(2):134–143. doi:10.1016/j.ajog.2019.07.043
49. Krempasky C, Grimstad F. Research is needed to assess breakthrough bleeding rates in transmasculine individuals utilizing hormonal contraception. Am J Obstet Gynecol. 2020;223(6):946. doi:10.1016/j.ajog.2020.06.036
50. Hubacher D, Lopez L, Steiner MJ, Dorflinger L. Menstrual pattern changes from levonorgestrel subdermal implants and DMPA: systematic review and evidence-based comparisons. Contraception. 2009;80(2):113–118. doi:10.1016/j.contraception.2009.02.008
51. Bentsianov S, Gordon L, Goldman A, Jacobs A, Steever J. Use of copper intrauterine device in transgender male adolescents. Contraception. 2018;98(1):74–75. doi:10.1016/j.contraception.2018.02.010
52. Brache V, Cochon L, Deniaud M, Croxatto HB. Ulipristal acetate prevents ovulation more effectively than levonorgestrel: analysis of pooled data from three randomized trials of emergency contraception regimens. Contraception. 2013;88(5):611–618. doi:10.1016/j.contraception.2013.05.010
53. Moseson H, Fix L, Gerdts C, et al. Abortion attempts without clinical supervision among transgender, nonbinary and gender-expansive people in the United States. BMJ Sex Reprod Health. 2022;48(e1):e22–e30. doi:10.1136/bmjsrh-2020-200966
54. Scarffe E. Dignitary harms and abortion law. Am J Bioeth. 2022;22(8):85–87. doi:10.1080/15265161.2022.2089273
55. Aiken A, Lohr PA, Lord J, Ghosh N, Starling J. Effectiveness, safety and acceptability of no-test medical abortion (termination of pregnancy) provided via telemedicine: a national cohort study. BJOG. 2021;128(9):1464–1474. doi:10.1111/1471-0528.16668
56. Leonardi M, Frecker H, Scheim A, Kives S. Reproductive health considerations in sexual and/or gender minority adolescents. J Pediatr Adolesc Gynecol. 2019;32:15–20. doi:10.1016/j.jpag.2018.09.010
57. Rew L, Young CC, Monge M, Bogucka R. Review: puberty blockers for transgender and gender diverse youth-a critical review of the literature. Child Adolesc Ment Health. 2021;26(1):3–14. doi:10.1111/camh.12437
58. Strang JF, Jarin J, Call D, et al. Transgender youth fertility attitudes questionnaire: measure development in nonautistic and autistic transgender youth and their parents. J Adolesc Health. 2018;62(2):128–135. doi:10.1016/j.jadohealth.2017.07.022
59. Nahata L, Chen D, Quinn GP, et al. Reproductive attitudes and behaviors among transgender/nonbinary adolescents. J Adolesc Health. 2020;66(3):372–374. doi:10.1016/j.jadohealth.2019.09.008
60. McCracken M, DeHaan G, Obedin-Maliver J. Perinatal considerations for care of transgender and nonbinary people: a narrative review. Curr Opin Obstet Gynecol. 2022;34(2):62–68. doi:10.1097/GCO.0000000000000771
61. Thornton KGS, Mattatall F. Pregnancy in transgender men. CMAJ. 2021;193(33):E1303. doi:10.1503/cmaj.210013
62. Obedin-Maliver J, Makadon HJ. Transgender men and pregnancy. Obstet Med. 2016;9(1):4–8. doi:10.1177/1753495X15612658
63. Slack DJ, Safer JD. Cardiovascular health maintenance in aging individuals: the implications for transgender men and women on hormone therapy. Endocr Pract. 2021;27(1):63–70. doi:10.1016/j.eprac.2020.11.001
64. Caughey AB, Krist AH, Wolff TA, et al. USPSTF approach to addressing sex and gender when making recommendations for clinical preventive services. JAMA. 2021;326(19):1953–1961. doi:10.1001/jama.2021.15731
65. Dai H, Meyer IH. A population study of health status among sexual minority older adults in select U.S. geographic regions. Health Educ Behav. 2019;46(3):426–435. doi:10.1177/1090198118818240
66. Persson DI. Unique challenges of transgender aging: implications from the literature. J Gerontol Soc Work. 2009;52(6):633–646. doi:10.1080/01634370802609056
67. Hash KM, Morrow DF. Lesbian, gay, bisexual, and transgender persons aging in rural areas. Int J Aging Hum Dev. 2020;90(2):201–208. doi:10.1177/0091415019836110
68. Maas AH, Rosano G, Cifkova R, et al. Cardiovascular health after menopause transition, pregnancy disorders, and other gynaecologic conditions: a consensus document from European cardiologists, gynaecologists, and endocrinologists. Eur Heart J. 2021;42(10):967–984. doi:10.1093/eurheartj/ehaa1044
69. Johnson K, Yarns BC, Abrams JM, Calbridge LA, Sewell DD. Gay and gray session: an interdisciplinary approach to transgender aging. Am J Geriatr Psychiatry. 2018;26(7):719–738. doi:10.1016/j.jagp.2018.01.208
70. Kohls G, Roessner V. Editorial perspective: medical body modification in youth with gender dysphoria or body dysmorphic disorder - is current practice coherent and evidence-based? J Child Psychol Psychiatry. 2022. doi:10.1111/jcpp.13717
71. Kozee HB, Tylka TL, Bauerband LA. Measuring transgender individuals’ comfort with gender identity and appearance: development and validation of the Transgender Congruence Scale. Psychol Women Q. 2012;36(2):179–196. doi:10.1177/0361684312442161
72. Rosen R, Brown C, Heiman J, Leiblum S, D’Agostino R. The female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191–208. doi:10.1080/009262300278597
73. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1960;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
74. Sjoberg MD, Walch SE, Stanny CJ. Development and initial psychometric evaluation of the transgender adaptation and integration measure (TGAIM). Int J Transgend. 2006;9(2):35–45. doi:10.1300/J485v09n02_05
75. Testa RJ, Habarth J, Peta J, Balsam K, Bockting W. Development of the gender minority stress and resilience measure. Psychol Sexual Orient Gender Diversity. 2015;2(1):65–77. doi:10.1037/sgd0000081
76. Rosen R, Riley A, Wagner G, Osterloh I, Mishra A, Mishra A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49:822–830. doi:10.1016/S0090-4295(97)00238-0
77. Spector IP, Carey MP, Steinberg L. The sexual desire inventory: development, factor structure, and evidence of reliability. J Sex Marital Ther. 1996;22(3):175–190. doi:10.1080/00926239608414655
78. The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;28:551–558. doi:10.1017/S0033291798006667
79. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
80. Vedovo F, Di Blas L, Perin C, Pavan N, Trombetta C. Operated male-to-female sexual function index: validity of the first questionnaire developed to assess sexual function after male-to-female gender affirming surgery. J Urol. 2020;204:115–120. doi:10.1097/JU.0000000000000791
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.