Back to Journals » International Journal of Women's Health » Volume 18
Breaking Barriers to Motherhood: Successful Conception and Term Delivery in Infertile Women with Hyperprolactinemia – Two Case Reports
Authors Fitriyanto IA ![]() , Rachmawati A, Juslin NP
, Rachmawati A, Juslin NP ![]()
Received 18 March 2026
Accepted for publication 11 May 2026
Published 19 May 2026 Volume 2026:18 609363
DOI https://doi.org/10.2147/IJWH.S609363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Iqbal Anugrah Fitriyanto, Anita Rachmawati, Nazhira Putri Juslin
Department of Obstetrics and Gynecology, Faculty of Medicine, Padjadjaran University/Dr Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Iqbal Anugrah Fitriyanto, Department of Obstetrics and Gynecology, Faculty of Medicine, Padjadjaran University/Dr Hasan Sadikin General Hospital, Pasteur 38, Bandung, 40161, Indonesia, Tel +6281399962004, Email [email protected]
Purpose: Hyperprolactinemia is a common cause of female infertility, and prolactin-secreting pituitary macroadenomas pose unique challenges for fertility restoration and pregnancy management. Herein, we present two cases of primary infertility due to hyperprolactinemia with distinct etiologies.
Case Presentation: Case 1: A 27-year-old woman with two years of amenorrhea and polycystic ovarian morphology did not undergo standard ovulation induction. Her serum prolactin level was 1334 ng/mL, and MRI revealed hemorrhagic pituitary macroadenoma. Dopamine agonist therapy with bromocriptine normalized prolactin to 13.09 ng/mL within six months, restored menses, and resulted in pregnancy complicated by severe preeclampsia, with successful delivery of a viable neonate requiring short-term respiratory support. Case 2: A 29-year-old woman with idiopathic hyperprolactinemia (initial prolactin 59.6 ng/mL) and a dominant right ovarian follicle received bromocriptine, achieving prolactin normalization (16.7 ng/mL) and bilateral follicular development. Adjunctive letrozole and continued dopamine agonist therapy for nine months led to conception and term vaginal delivery, without complications.
Conclusion: These cases highlight that targeted dopamine agonist therapy may effectively normalize prolactin levels, restore ovulation, and achieve healthy term pregnancies in women with hyperprolactinemia, whether macroadenoma- is driven or idiopathic. Early recognition, individualized treatment, and multidisciplinary follow-up are essential to overcome reproductive obstacles in this high-risk population.
Keywords: hyperprolactinemia, infertility, macroadenoma, prolactin
Introduction
Hyperprolactinemia is a well-recognized cause of infertility, which disrupts the hypothalamic–pituitary–ovarian axis.1,2 Hyperprolactinemia may result from structural causes such as pituitary adenomas and non-structural etiologies such as idiopathic hyperprolactinemia, medications.3,4 Prolactin-secreting pituitary adenomas (prolactinomas) are the most common functioning pituitary tumors in women of reproductive age, with an estimated prevalence of 23.9 per 100 000 and peak incidence between 25 and 34 years.5 Macroadenomas, in particular, pose a dual challenge; chronic hyperprolactinemia causes anovulation, whereas the tumor mass may enlarge further under physiological gestational changes, complicating both fertility restoration and pregnancy management. Pregnancy rates are lower in women with macroadenomas than in those with microadenomas, and the risk of symptomatic tumor growth during gestation necessitates careful monitoring and coordinated care.6
While the relationship between hyperprolactinemia and infertility is well-documented, a variety of clinical presentations and therapy strategies–particularly between severe adenoma-related and idiopathic cases remains a difficulty in practice. These cases highlight various diagnostic approaches and therapeutic outcomes, including delayed diagnosis, due to overlapping characteristics with PCOS and successful conservative care without rapid imaging.
Case Presentation
Case 1
A 27-year-old nulligravida presented with irregular menstruation and primary infertility after being married for three years. She reported resumption of menses five days before presentation following a two-year period of amenorrhea. She also had a history of galactorrhoea. She had previously undergone three cycles of clomiphene citrate (50 mg daily) combined with gonadotropin injection and sequential estrogen-progestin induction, without restoration of regular cycles or conception.
On examination, her body mass index was 28.3 kg/m2. Transvaginal ultrasonography revealed bilaterally enlarged ovaries with multiple peripherally arranged follicles, consistent with polycystic ovarian morphology (Figure 1). Hysterosalpingogram demonstrated bilateral tubal patency and a normal uterine cavity. Serum anti-Müllerian hormone (AMH), luteinizing hormone (LH), and follicle-stimulating hormone (FSH) levels were within normal reference ranges. Therefore, she was diagnosed with primary infertility attributed to polycystic ovary syndrome (PCOS) and managed with metformin and a structured weight-loss diet program from a nutritionist.
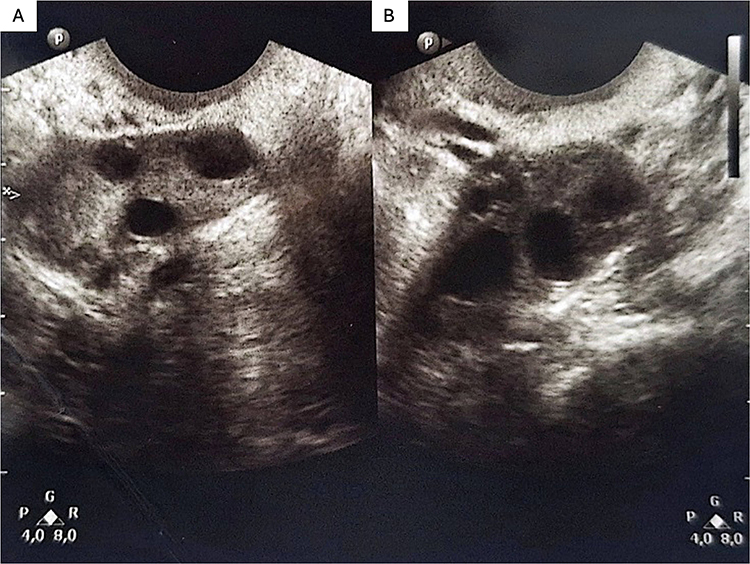 |
Figure 1 Transvaginal Ultrasound findings. (A) An ovarium showed a relative volume increase with central stroma and hyperechoic appearance with a “string of pearls” distribution suggestive of a polycystic ovarian morphology. (B) An ovarium showed a hyperechoic central stroma with small follicular distribution suggestive of a polycystic ovarian morphology. |
After two years of PCOS-directed therapy—including dietitian-supervised weight training, cardiovascular exercise (resulting in a 7 kg weight reduction), and repeat ovarian stimulation and menstrual induction therapy with co-cyprindiol, letrozole 2.5 mg, and 75 IU FSH injections—the patient continued to experience oligomenorrhea and failed to conceive. During this period, she rarely attended follow-up consultations due to limited access to care during the COVID-19 pandemic. After repeated biochemical evaluations, the results revealed a markedly elevated serum prolactin level of 1334 ng/mL (normal, < 25 ng/mL) with a normal thyroid-stimulating hormone (TSH) of 1.26 µIU/mL. Concerns regarding prolactin-secreting pituitary lesions prompted magnetic resonance imaging (MRI) of the brain. Post-contrast sequence MRI revealed heterogeneous enhancement, suggestive of hemorrhagic pituitary macroadenoma (Figure 2). The patient was diagnosed with secondary amenorrhea with hyperprolactinemia due to hemorrhagic pituitary macroadenoma. DA therapy with bromocriptine (2.5 mg) was initiated once daily. She also received folic acid 400 µg daily.
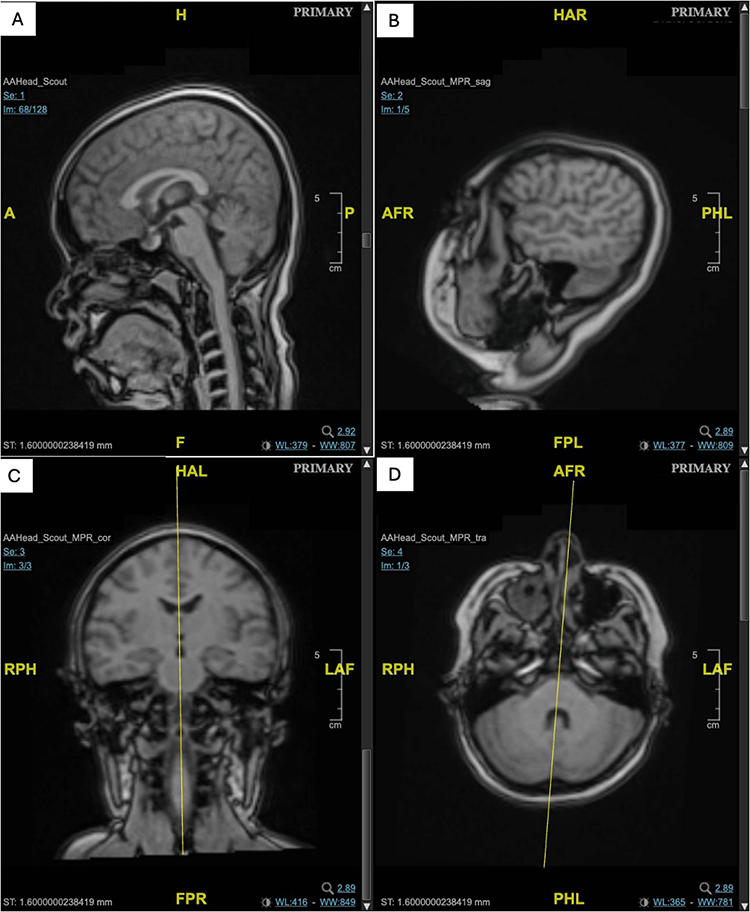 |
Figure 2 A 27-year-old nulligravida presented with irregular menstruation and primary infertility refractory to PCOS treatment and markedly elevated prolactin levels shown (A) Head MRI mid-sagittal view (B) Head MRI sagittal view (C) Head MRI coronal view (D) Head MRI transverse view. A sella turcica view demonstrated a heterogeneous, inhomogeneous solid mass with cystic degeneration and internal hemorrhage occupying the sellar and suprasellar regions (yellow arrow). The lesion extended laterally, compressing the right cavernous sinus and bulging into the left cavernous sinus, with superior displacement of the optic chiasm. |
Menstruation resumed shortly after therapy initiation. After six months, the serum prolactin normalized to 13.09 ng/mL. One month later, transvaginal ultrasound confirmed a viable intrauterine pregnancy at six weeks of gestation (the gestational sac, yolk sac, and fetal pole were visualized). The dopaminergic agonist regimen was continued throughout the pregnancy.
During the pregnancy, the patient underwent a cesarean section due to severe preeclampsia. A male neonate was delivered with a birth weight of 2580 grams and length of 46 cm. The Apgar scores were 6 at 1 min and 9 at 5 min. The newborn required transient respiratory support with continuous positive airway pressure (CPAP) and was admitted to the neonatal high care unit (NHCU) for observation. Despite these maternal and neonatal complications, a successful pregnancy outcome was achieved.
Case 2
A 29-year-old nulligravida woman was referred for primary infertility three years and seven months after marriage. She was neither using antipsychotic nor antidepressant drugs. Initial hormonal evaluation revealed the following levels: FSH 5.56 IU/L, LH 7.32 IU/L, and prolactin 59.6 ng/mL. She commenced bromocriptine (2.5 mg) twice daily, for two months, resulting in prolactin reduction to 38.2 ng/mL. Ultrasonographic evaluation revealed an anteflexed uterus and a dominant follicle in the right ovary, with the left ovary not visualized. Given the moderate prolactin elevation (59.6 ng/mL) and absence of symptoms suggestive of a pituitary mass (eg., headache or visual field disturbance), a conservative approach without immediate MRI was adopted. A diagnosis of idiopathic hyperprolactinemia was made, and bromocriptine was continued at the same dose as monthly prolactin monitoring.
One month later, serum prolactin normalized to 16.7 ng/mL, and ultrasonography revealed 13 follicles in the right ovary and 11 follicles in the left ovary. Bromocriptine was tapered to 2.5 mg once daily and letrozole (2.5 mg) was prescribed twice daily for ovulation induction.
Nine months after bromocriptine therapy and one cycle of letrozole, the patient achieved pregnancy. Transvaginal ultrasonography at 5 weeks and 5 days of gestation revealed a 1.01 cm intrauterine gestational sac. Bromocriptine was maintained throughout gestation, along with micronized progesterone 200 mg daily and folic acid 400 µg daily. The pregnancy proceeded uneventfully, culminating in a spontaneous vaginal delivery at 39 weeks of gestation.
Discussion
Both cases underscore the necessity of routine prolactin measurement in women with menstrual irregularities or infertility, even in the absence of galactorrhoea. Hyperprolactinemia accounts for approximately 15% of anovulatory infertility cases, and is found in up to 43% of women who present with both anovulation and galactorrhea. In addition to reproductive dysfunction, hyperprolactinemia manifests as amenorrhea, oligomenorrhea, and galactorrhea, which are primarily attributable to prolactin excess and its inhibitory effects on the hypothalamic-pituitary-ovarian axis. In contrast, mass effects from pituitary adenomas typically manifest as compressive symptoms, such as headaches or visual field disturbance.1,6,7
In addition to these general considerations, these cases present significant clinical insights. While the role of dopamine agonists in restoring fertility is well-established, these cases highlight variability in clinical presentation and management strategies.4 The initial case illustrates a diagnostic challenge, wherein hyperprolactinemia exhibited characteristics similar to Polycystic Ovarian Syndrome (PCOS), resulting in a delayed recognition of a pituitary macroadenoma. The second case illustrates that moderate hyperprolactinemia, in the absence of mass-related symptoms, may be effectively managed without immediate imaging, highlighting the need for an individualized diagnostic and therapeutic approach.
The pathophysiology of hyperprolactinemia-induced infertility primarily involves the disruption of the hypothalamic–pituitary–ovarian axis. Excess prolactin suppresses pulsatile gonadotropin-releasing hormone (GnRH) secretion, largely via inhibition of hypothalamic kisspeptin (Kiss1) neurons, which are key upstream regulators of GnRH dynamics. This neuroendocrine cascade produces functional hypogonadotropic hypogonadism, which is clinically characterized by impaired follicular recruitment, anovulation, and menstrual disturbances.8,9
These mechanisms were observed in our cases. In Case 1, the initial presentation of obesity, menstrual irregularity, infertility and polycystic ovarian morphology was suggestive of PCOS, a common cause of anovulatory infertility. Nonetheless, the persistence of amenorrhea despite various PCOS treatments, added with a history of galactorrhea, led to further laboratory assessment, which revealed very high prolactin levels (>1,300 ng/mL) and a pituitary adenoma. This markedly elevated prolactin levels resulted in an apparent arrested folliculogenesis (polycystic ovarian morphology), consistent with chronic suppression of GnRH to LH/FSH and the resultant functional hypogonadotropic hypogonadism. This case illustrates a diagnostic challenge, as hyperprolactinemia may present symptoms similar to those of PCOS, which may lead to delayed recognition if prolactin levels are not evaluated promptly. The prompt resumption of menses and subsequent conception after bromocriptine therapy are consistent with the reversibility of kisspeptin/GnRH suppression once prolactin is normalized.8,9
In Case 2, moderate hyperprolactinemia was linked to impaired ovulation despite otherwise acceptable baseline gonadotropin measures, and the normalization of prolactin with bromocriptine permitted restoration of bilateral follicular development (ultrasound documented) and ovulation following adjunct letrozole, again consistent with recovery of the hypothalamic-pituitary drive after correction of the hyperprolactinemic state.8
Dopamine agonists remain a cornerstone of treatment. This therapy addresses the proximate cause by activating D2 receptors on lactotrophs, lowering prolactin secretion, and often shrinking prolactinomas. Cabergoline is typically more effective and better tolerated than bromocriptine, achieving higher rates of prolactin normalization and ovulation with fewer side effects; however, bromocriptine remains widely-used due to its established safety profile in pregnancy and cost-effective option.10–12
In our two reports, bromocriptine was selected for both patients because of cost constraints and because it was well tolerated. Six months of therapy was sufficient to normalize prolactin levels, restore GnRH pulsatility and folliculogenesis (13 and 11 follicles in case 2), and permit conception. Case 1 required ongoing therapy throughout gestation because of macroadenoma risk, whereas case 2’s regimen was tapered once prolactin normalized and was supplemented with letrozole to stimulate ovulation. Both strategies culminated in healthy delivery.
Tumor size and symptomatology inform management decisions. Markedly elevated prolactin levels (often >200–250 ng/mL, as in case 1) generally warrant further evaluation with pituitary imaging. Although macroadenomas (≥10 mm) are far less common than microadenomas, they carry a higher risk of symptomatic enlargement during pregnancy versus microadenomas. By contrast, Case 2’s moderate prolactin elevation (59.6 ng/mL) and absence of mass symptoms justified a conservative approach without immediate MRI, reflecting that levels below 100 ng/mL often signify microadenomas or idiopathic hyperprolactinemia.6,13
These outcomes suggest that individualized dopamine agonist therapy guided by prolactin level, adenoma size, and clinical presentation may help restore fertility and promote favorable pregnancy outcomes.
Conclusion
Routine prolactin assessment should be considered for infertility workups. Tailored dopamine‑agonist therapy, based on prolactin levels and adenoma characteristics, may help reverse hypogonadotropic hypogonadism, restore fertility, and support successful term delivery even in high-risk macroadenoma cases. Further studies are needed to confirm these findings.
Registration of Research Studies
Registration of research is not applicable in our case.
Abbreviations
AMH, anti-Müllerian hormone; CPAP, continuous positive airway pressure; DA, dopaminergic agonist; FSH, follicle-stimulating hormone; GnRH, Gonadotropin-releasing hormone; LH, luteinizing hormone; MRI, magnetic resonance imaging; NHCU, neonatal high care unit; PCOS, polycystic ovary syndrome; TSH, thyroid-stimulating hormone.
Informed Consent Patient Statement
Written informed consent has been provided by the two patients to have the case details and any accompanying images published.
Ethical Approval
For case studies based on available clinical data, this study was exempt from ethical approval, as determined by the institutional and departmental review boards at Padjadjaran University/Dr. Hasan Sadikin General Hospital, Bandung, Indonesia. No institutional approval was required for the publication of this case.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Haidenberg-David F, Sidauy-Adissi J, Moscona-Nissan A. et al. Overview of Hyperprolactinemia: general Approach and Reproductive Health Implications. Arch Med Res. 2024;55(8):103102. doi:10.1016/j.arcmed.2024.103102
2. Fachi MM, Deus Bueno L, Oliveira DC, Silva LL, Bonetti AF. Efficacy and safety in the treatment of hyperprolactinemia: a systematic review and network meta‐analysis. J Clin Pharm Ther. 2021;46(6):1549–6. doi:10.1111/jcpt.13460
3. Sholuade O, Njoku G, Kaza S, Fatteh RA, Kollukkad M, Edwards C. Idiopathic Hyperprolactinemia: clinical Presentation, Diagnosis, Management, and Clinical Outcome. Cureus. 2025;17(12):98701. doi:10.7759/cureus.98701
4. Dehghan E, Namiranian N, Ghadiri-Anari A, Ratki SKR, Azizi R. Evaluation of hyperprolactinemia risk factors in infertile women referred to Yazd Infertility Center: a cross-sectional study. Int J Reprod Biomed. 2021;19(12):1085–1090. doi:10.18502/ijrm.v19i12.10059
5. Aldahmani K, AlMalki M, Beshyah S. A rational approach to the evaluation and management of patients with hyperprolactinemia. Ibnosina J Med Biomed Sci. 2020;12(02):90–97. doi:10.4103/ijmbs.ijmbs_38_20
6. Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and Treatment of Hyperprolactinemia: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2011;96(2):273–288. doi:10.1210/jc.2010-1692
7. Crosignani PG. Management of hyperprolactinemic infertility. Middle East Fertil Soc J. 2012;17(2):63–69. doi:10.1016/j.mefs.2012.04.003
8. Kaiser UB. Hyperprolactinemia and infertility: new insights. J Clin Investig. 2012;122(10):3467–3468. doi:10.1172/JCI64455
9. Hoskova K, Bryant NK, Chen ME, et al. Kisspeptin Overcomes GnRH Neuronal Suppression Secondary to Hyperprolactinemia in Humans. J Clin Endocrinol Metab. 2022;107(8):E3515–E3525. doi:10.1210/clinem/dgac166
10. Dos Santos Nunes V, El Dib R, Boguszewski CL, Nogueira CR. Cabergoline versus bromocriptine in the treatment of hyperprolactinemia: a systematic review of randomized controlled trials and meta-analysis. Pituitary. 2011;14(3):259–265. doi:10.1007/s11102-010-0290-z
11. Webster J, Piscitelli G, Polli A, Ferrari C, Ismail I, Scanlon MF. A Comparison of Cabergoline and Bromocriptine in the Treatment of Hyperprolactinemic Amenorrhea. N Engl J Med. 1994;331(14):904–909. doi:10.1056/NEJM199410063311403
12. Ma K, Ma L, Huang T, et al. The effectiveness and safety of aripiprazole, bromocriptine, and cabergoline in the treatment of hyperprolactinemia: a systematic review and network meta-analysis. Expert Opin Drug Saf. 2025;24(7):773–786. doi:10.1080/14740338.2024.2416918
13. Shibli-Rahhal A, Schlechte J. Hyperprolactinemia and Infertility. Endocrinol Metab Clin North Am. 2011;40(4):837–846. doi:10.1016/j.ecl.2011.08.008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Correlation Between DRD2 and COMT Gene Polymorphisms, HPT and HPG Axes Functions, and Antipsychotic Drug-Induced Hyperprolactinemia and Macroprolactinemia
Wang Z, Li J, Chen H, Jin H, Wang S, Hu X
Neuropsychiatric Disease and Treatment 2025, 21:1011-1017
Published Date: 8 May 2025