Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Brain-Derived Neurotrophic Factor (BDNF) Depression and Subjective Sleep Quality in the First Trimester of Pregnancy Among Migrant Workers in Thailand
Authors Kriengtuntiwong T, Zaw YH, Taneepanichskul N ![]()
Received 28 May 2021
Accepted for publication 3 September 2021
Published 15 September 2021 Volume 2021:14 Pages 2549—2556
DOI https://doi.org/10.2147/JMDH.S322355
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Thuvachit Kriengtuntiwong,1,2 Ye Htet Zaw,3 Nutta Taneepanichskul1,4
1College of Public Health Science, Chulalongkorn University, Bangkok, Thailand; 2Department of Mental Health, Srithanya Hospital, Nonthaburi, Thailand; 3Defense Services Medical Academy, Yangon, Myanmar; 4HAUS IAQ Research Unit, Department of Pediatrics, Faculty of Medicine, Chulalongkorn University, King Chulalongkorn Memorial Hospital, Bangkok, Thailand
Correspondence: Nutta Taneepanichskul
College of Public Health Sciences, Chulalongkorn University, Bangkok, Thailand
Tel +668 9 206– 6534
Email [email protected]
Introduction: Brain-derived neurotrophic factor (BDNF) influences neurodevelopment during pregnancy. Maternal sleep quality and depression are suggested to influence BDNF levels. The objective of this study was to assess the association between depression, sleep quality, and BDNF levels among Myanmar migrant pregnancies.
Methods: A cross-sectional study was conducted at Krathum Baen Hospital, Samut Sakhon province, from June to October 2018. A total of 108 first-trimester women were recruited into our study. Maternal blood was collected to analyze BDNF. Depression levels were assessed using the Patient Health Questionnaire (PHQ-9) instrument. The Pittsburgh Sleep Quality Index (PSQI) questionnaire was applied to evaluate subjective sleep quality. Because BDNF was skewed, binary logistic regression was analyzed.
Results: We found that 28.7% of pregnant women reported poor sleep quality, and 33.4% were classified as having mild to moderate depression. After adjusting for covariate variables, pregnant women with depression had higher BDNF levels than those without depression (OR = 2.972, 95% CI = [1.111, 7.949], p = 0.030). Pregnant women with poor sleep quality had lower BDNF levels than those who had good sleep quality (OR = 0.359, 95% CI = [0.132, 0.972], p = 0.044).
Discussion: The results suggested that BDNF might be an alternative tool to assess sleep quality in pregnant women.
Keywords: brain-derived neurotrophic factor, BDNF, pregnancy, first trimester, sleep quality, depression
Introduction
During pregnancy, mothers will face many challenges because so many things will change with their health, mental health, families, and social lives. These changes lead some pregnant women to experience mental illnesses during both the antepartum and postpartum periods.1 Depression and anxiety are the most common mental illnesses that occur during these times.2 The estimated prevalence of depression during pregnancy differs between studies. In a previous study of depression during pregnancy, high-income countries were shown to have a prevalence between 7–20% while the prevalence in low- and middle-income countries was 20% or more.3 Another previous study found that the rate of depression was highest during the first trimester and lower in the second and third trimesters.4 In contrast, a different prior study found that the rates of mental illness were highest during the second and third trimesters but lowest during the first trimester.5 Depression in pregnancy is the most common cause of a mother’s incapacity to work6,7 because she may use alcohol, illicit substances, or tobacco and may not notice signs of labor.8 Finally, pregnant mothers can experience suicidal ideation if they have long-term depression.9 Their newborns will be at risk of preterm delivery and low birth weights.8
Sleep quality is another problem during pregnancy. The prevalence of insomnia varies according to study design and population. In Thailand, a previous study found that during pregnancy, 94.7% of participants had poor sleep quality.10 The meta-analysis from Sedov found that based on 24 studies, the average prevalence of poor sleep quality during pregnancy was 45.7%.11 Poor sleep quality during pregnancy will have an effect on maternal and newborn health. It can lead to longer labor times12 and depression during the antepartum and postpartum periods.13–16 Finally, it can cause suicidal ideation in the mother.17 As with maternal depression, poor sleep quality can lead to low birth weights18 and preterm births.19
Brain-derived neurotrophic factor (BDNF) has been studied in recent years to determine its association with depression20–27 and sleep quality.23,28–30 BDNF affects the hippocampus, claustrum, amygdala, bed nucleus of the stria terminalis, septum, and the nucleus of the solitary tract in the human brain.31 It is synthesized from a precursor called pro-BDNF. This precursor cleaves to generate mature BDNF (mBDNF).32,33 These two types of BDNF will have an effect on different receptors: pro-BDNF on the pan-neurotrophin receptor p75 (p75NTR) and mBDNF on the tyrosine kinase B receptor (TrkB). These two forms of BDNF and receptors work together in many ways to affect our health. BDNF serves unique functions during pregnancy. It is important for follicular development, implantation, and placentation within reproductive tissues. BDNF plays an important role in healthy placental development, and low BDNF bioavailability has been implicated in placental pathology. It also crosses the uteroplacental barrier, and animal models show that circulating maternal levels of BDNF correspond with fetal brain levels.34
Migrant people are a risk group that will have a treatment gap in Thailand’s health system. Data from the Department of Employment in Thailand show that Samut Sakhon has the second highest migrant population in Thailand.35 Therefore, this study investigated the association between depression, sleep quality, and BDNF levels among pregnant Myanmar migrants in Samut Sakhon.
Methods
Study Design
This research was a nested cross-sectional study that was part of a birth cohort study conducted between June 2018 and August 2019 among Myanmar migrants in Samut Sakhon province, Thailand.36 The province was selected because it has the second largest population of Myanmar migrants. Briefly, 108 pregnant women aged between 18 and 35 years of age at less than 14 weeks of gestation were recruited from the antenatal care clinic. Inclusion criteria were 1) being a pregnant Myanmar migrant visiting the clinic for the first time, 2) the ability to read, write, and communicate in the Myanmar language, and 3) willingness to give blood samples. Exclusion criteria were 1) having given birth more than five times, 2) an inter-pregnancy interval of less than one year, and 3) a medical history of depression. This study and the birth cohort study complied with the Declaration of Helsinki. The data collection and analysis were approved by the Research Ethics Review Committee for Research Involving Human Research Participants, Health Sciences Group, Chulalongkorn University (RECCU) (COA No.251/2018 and COA No.094/2021). Participants’ informed consent was obtained prior to participation.
Plasma BDNF Analysis
Trained nurses drew maternal blood in the laboratory department of Krathum Baen Hospital. A total of 5 mL of blood was collected and separated into two EDTA tubes; 2.5 mL of blood was used to analyze plasma BDNF. The sample tubes were properly labeled with the hospital number and name of the participant. All sample tubes were stored at 4°C before being transferred to the laboratory for BDNF analysis. The analysis of plasma BDNF was explained by Zaw and Taneepanichskul (2019).36 Briefly, maternal plasma BDNF concentrations were measured using a quantitative sandwich enzyme-linked immunosorbent assay (ELISA) kit (RayBio, USA). Sample dilutions of antibody cocktails and serial dilutions of the standard solution were prepared. The samples were assayed in duplicate. The immobilized antigen and antibody were incubated with an antibody cocktail containing biotinylated anti-human BDNF. The solutions were discarded by adding and washing them. Color development was stopped. The solution was used with an absorbance of 450 nm by a microplate reader. All incubations were performed at room temperature.
Questionnaire
Trained research assistants distributed the structured self-report questionnaires to the participants, which included questions about socio-demographic characteristics and health behaviors. Participants provided details including age (years), marital status (married or not married but living together), BMI (kg/m2), education (primary school or less, or more than primary school), occupation (employed or unemployed), monthly family income (Thai baht [THB]), smoking history (now, never, or before pregnancy), secondhand smoke exposure (now, never, or before pregnancy), alcohol consumption (now, never, or before pregnancy), regular aerobic exercise (yes or no), systolic blood pressure (sBP) (mmHg), and diastolic blood pressure (dBP) (mmHg).
Depression was assessed with the Patient Health Questionnaire 9 (PHQ-9) instrument. The PHQ-9 is a nine-item questionnaire for assessing depression module scoring of the nine Diagnostic and Statistical Manual of Mental Disorders-IV (DSM‐IV) criteria. It uses a four-point Likert score ranging from 0 to 3, where not at all = 0, several days = 1, more than half the days = 2, nearly every day = 3. The total score ranges from 0 to 27. The reliability of the PHQ-9 was quantified with Cronbach’s alpha, which was 0.89.10 The level of depression severity is classified as minimal (total PHQ-9: 1–4), mild (total PHQ-9: 5–9), moderate (total PHQ-9: 10–14), moderate to severe (total PHQ-9: 15–19), and severe (total PHQ-9: 20–27).37 In this study, each component of the PHQ-9 was classified into “yes (several days and above)” or “no (not at all).” The total PHQ-9 score was classified into binary outcomes: no or minimal depression (total PHQ-9 < 5) and mild to severe depression (total PHQ-9 ≥ 5).
Sleep quality during the previous month of pregnancy was assessed with the Pittsburgh Sleep Quality Index (PSQI) questionnaire.38 Nineteen self-rated items were classified into seven components, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medication, and daytime dysfunction. The total score for each component ranged from zero to three. Subjective sleep quality was subdivided into the following categories: very bad, fairly bad, fairly good, and very good. Sleep latency was originally subdivided into ≤ 15 minutes, 16–30 minutes, 31–60 minutes, and > 60 minutes. Sleep duration was calculated from the number of sleep hours during the nighttime and categorized into < 5 hours, 5.0–5.9 hours, 6–6.9 hours, and ≥ 7 hours. The sleep efficiency scale was calculated with the formula (hours of sleep/hours in bed) × 100 and grouped by ≥ 85%, 75% to 84%, 65% to 74%, and < 65%. Sleep disturbance was rated from nine items of trouble sleeping, which were subdivided according to whether the occurred three or more times a week, once or twice a week, less than once a week, and not during the past month. Use of sleep medication was assessed and categorized into three or more times a week, once or twice a week, less than once a week, and not during the past month. The global PSQI score was calculated from a summation of each component ranging from zero to 21. Based on previous literature, participants with scores of five or less were classified as having good sleep quality, and those with scores of six or more were classified as having poor sleep quality.38 The internal consistency and reliability coefficient was 0.83 for its seven components.
Statistical Analysis
Data analysis was done using SPSS 22.0 (SPSS for Windows, version 22.0; SPSS, Inc., Chicago, IL, USA, Chulalongkorn University license). The general characteristics of the pregnant women were reported by counts (percentages) for category data and mean (± standard deviation, SD) for continuous data. BDNF levels were categorized as high (> 6.38 μg/L) and low (≤ 6.38 μg/L) by median value because they lacked a standard cut-off point. The association between the characteristics of the participants and their BDNF levels was analyzed with binary logistic regression. A crude odds ratio (OR) with 95% confidence intervals (CI) was reported. Multiple logistic regression was performed for the associations among BDNF, sleep quality, and depression. The final model was adjusted for age (< 30 or ≥ 30 years), BMI (< 25 or ≥ 25 kg/m2), and education (primary school or less, or more than primary school). A p-value less than 0.05 was considered statistically significant.
Results
Table 1 presents the general characteristics of the participants (n = 108). The majority of participants were less than 30 years old (63.9%) and completed more than primary school (58.3%). Of the participants, 79 (73.1%) had BMIs lower than 25, and 59 (54.6%) reported secondhand smoking; 78.7% did not regularly exercise. Regarding depression status, 66.6% reported no to minimal depression and 33.4% reported mild to severe depression. The majority of the pregnant women, 71.3%, were good sleepers.
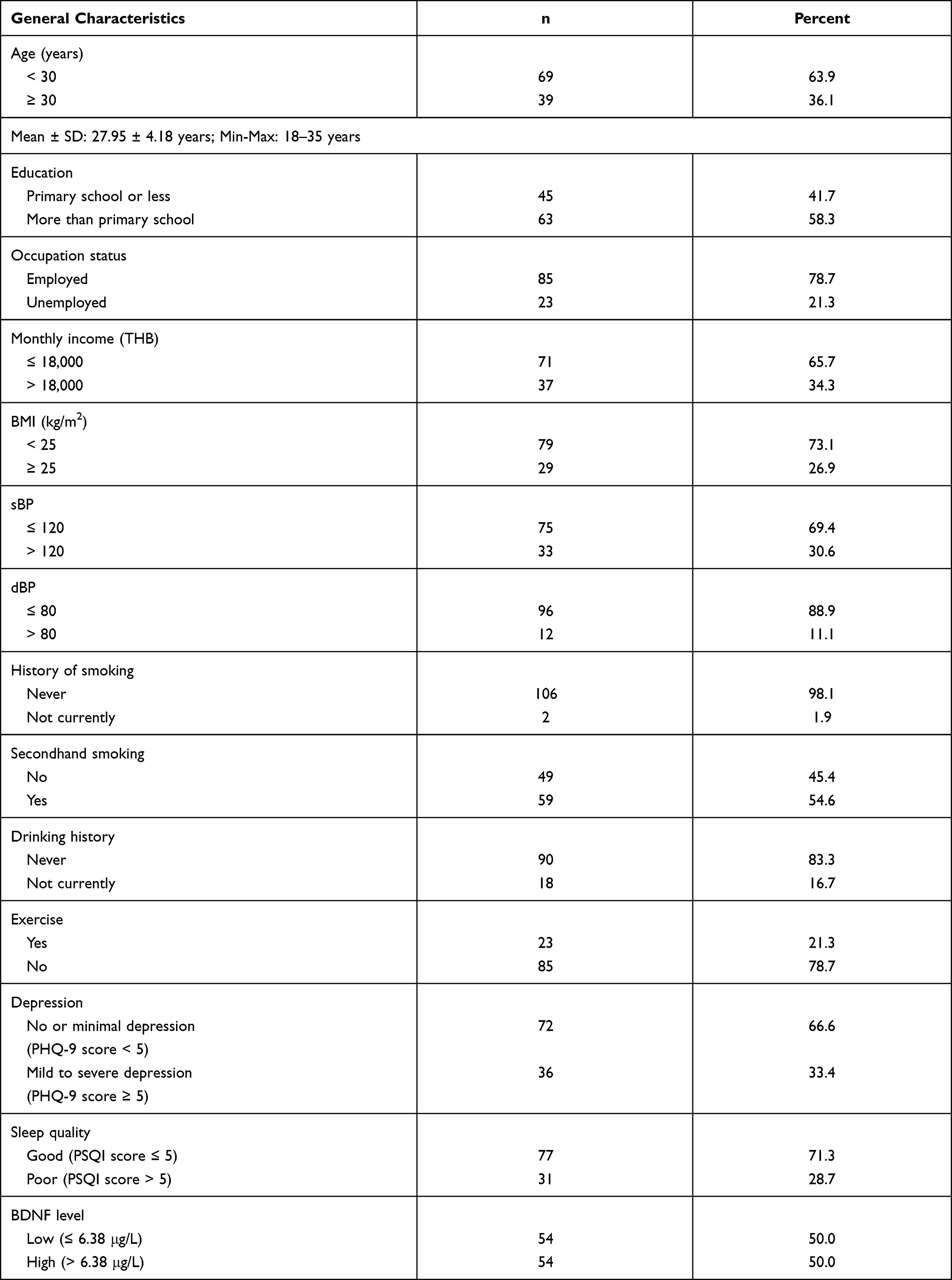 |
Table 1 General Characteristics of Participants (n = 108) |
Table 2 presents the bivariate analysis between factors related to BDNF levels. The result from binary logistic regression showed that factors associated with BDNF were not significant. Table 3 presents the final model of an association among depression, sleep quality, and BDNF. After adjusting for age, BMI, education, depression, and sleep quality, a significant association among depression, sleep quality, and BDNF levels was shown. Participants who reported mild to severe depression had higher BDNF levels (AOR = 2.972, 95% CI = [1.111, 7.949], p = 0.03) compared to no or minimal depression. Participants with poor sleep quality had lower BDNF levels (OR = 0.359, 95% CI = [0.132, 0.972], p = 0.044) compared to those with good sleep quality.
 |
Table 2 Association Between General Characteristics and BDNF Level |
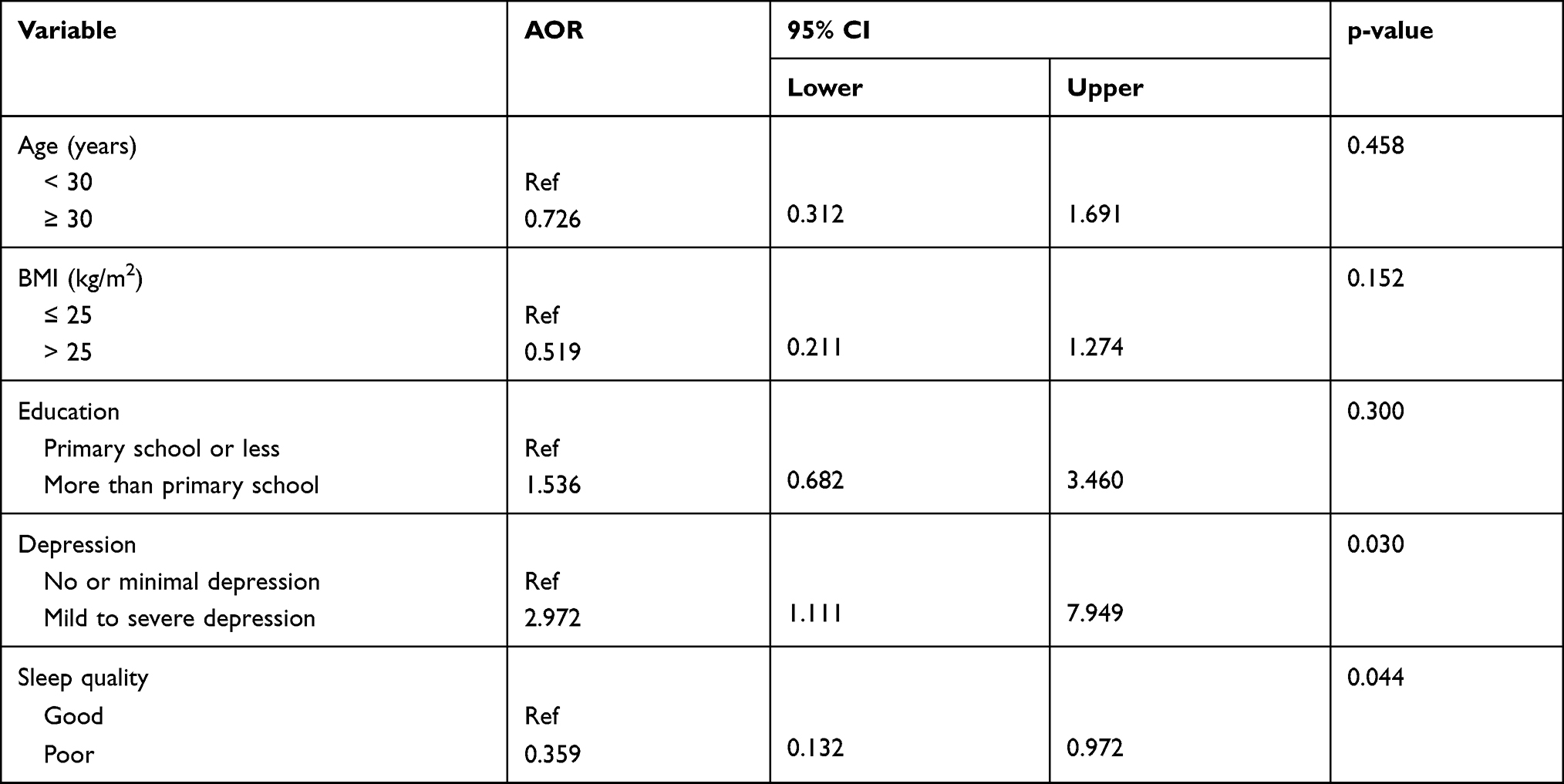 |
Table 3 Final Model of Depression, Sleep Quality, and BDNF |
Discussion
Our study investigates the relationship among depression, sleep quality, and BDNF levels. We found that 28.7% of pregnant women reported poor sleep quality, and 33.4% were classified as having mild to severe depression. Pregnant women with depression tended to have increased BDNF levels, while poor sleep quality tended to be associated with decreased BDNF levels.
The prevalence of poor sleep quality in pregnancy varies according to each study’s design and participants. In Thailand, a previous study of women in their second and third trimesters found that 94.7% had poor sleep quality.10 Regarding other locations, a study in the USA found that 39% of pregnant women in the first trimester and 53.5% in the third trimester had poor sleep quality.39 A study in Peru found that 16.9% had poor sleep quality during the second trimester.40 In Turkey, among all trimesters, 52.2% of pregnant women experienced poor sleep quality.41 In Australia, 52% of women in all trimesters had poor sleep quality.
Our study found that pregnant women with mild to severe depression had higher BDNF levels compared to those with no or minimal depression. Our findings are inconsistent with previous studies. Shimizu et al found that BDNF levels were significantly lower in people with depression who did not use antidepressants than in those who used antidepressants or did not have depression.22 A previous study by Fung et al found that BDNF levels were significantly lower in pregnant women with antepartum depression compared to those who did not have antepartum depression. Fung et al also found that women whose BDNF levels were in the lowest three quartiles (< 17.32 ng/mL) had 1.61-fold increased odds (OR = 1.61, 95% CI = [1.13, 2.30]) of antepartum depression as compared with women whose BDNF levels were in the highest quartile (> 25.31 ng/mL).20 BDNF has an effect on depression because BDNF binds to the TrkB receptor. Depression increases the expression of the bcl-2 protein in the hippocampus and regulates neuronal survival via the phosphatidylinositol 3-kinase (PI3-kinase)/Akt pathway. If people have chronic stress, it will lead to downregulation of BDNF levels and decreased bcl-2, reducing neurogenic cell survival and resulting in the development of depression symptoms.
We found that pregnant women who slept poorly had lower BDNF levels. The Giese study found that BDNF levels were significantly higher in participants with no insomnia compared to the sub-threshold insomnia and insomnia groups.28 However, this result is inconsistent with a previous study by Santiago that found no significant difference in BDNF levels between the good sleep, poor sleep, and sleep disturbance groups.42 This result is also inconsistent with the Rethorst study, which found that hypersomnia will reduce BDNF levels (p = 0.03), but BDNF levels were not associated with insomnia.29 BDNF can affect sleep quality by binding with TrkB, which sends signaling to the pedunculopontine tegmental nucleus (PPT). The PPT plays an essential role in the development of the REM sleep homeostatic drive. An animal study showed that there is a significant positive relationship between the REM sleep homeostatic drive and the level of PPT BDNF expression. In contrast, TrkB receptor inhibition reduces the REM sleep homeostatic drive.43
Several limitations of this study should be noted. First, the sample size was small. To the best of our knowledge, this is the first birth cohort study among migrant workers in Thailand. Second, the study was designed to be cross-sectional; therefore, a causal relationship cannot be proved. Reported questionnaires lead to recall bias among participants. Our study was limited to the first trimester of pregnancy. Further studies should focus on the second and third trimesters, during which maternal sleep quality worsens. In addition, the plasma BDNF measurements in this study were performed with ELISA kits that can detect both mBDNF and pro-BDNF. Therefore, it was not possible to differentiate between these two BDNF expressions. Last, our study lacks external validity, so generalizability was not possible. Finally, participants were selected from only one study area.
In conclusion, our study found that 28.7% of pregnant women were poor sleepers and 33.4% reported mild to severe depression. Pregnant women with mild to severe depression had higher BDNF levels than those with no or minimal depression. Pregnant women who were poor sleepers had lower BDNF levels than good sleepers. We suggest that BDNF may be a biomarker for assessing depression and sleep quality in pregnant women.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, agreed to the submitted journal, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Smith MV, Shao L, Howell H, Lin H, Yonkers KA. Perinatal depression and birth outcomes in a Healthy Start project. Matern Child Health J. 2011;15(3):401–409. doi:10.1007/s10995-010-0595-6
2. Alipour Z, Lamyian M, Hajizadeh E. Anxiety and fear of childbirth as predictors of postnatal depression in nulliparous women. Women Birth. 2012;25(3):e37–e43. doi:10.1016/j.wombi.2011.09.002
3. Melville JL, Gavin A, Guo Y, Fan MY, Katon WJ. Depressive disorders during pregnancy: prevalence and risk factors in a large urban sample. Obstet Gynecol. 2010;116(5):1064. doi:10.1097/AOG.0b013e3181f60b0a
4. Gavin NI, Gaynes BN, Lohr KN, Meltzer-Brody S, Gartlehner G, Swinson T. Perinatal depression: a systematic review of prevalence and incidence. Obstet Gynecol. 2005;106(5 Pt 1):1071–1083. doi:10.1097/01.AOG.0000183597.31630.db
5. Bennett HA, Einarson A, Taddio A, Koren G, Einarson TR. Prevalence of depression during pregnancy: systematic review. Obstet Gynecol. 2004;103(4):698–709. doi:10.1097/01.AOG.0000116689.75396.5f
6. Polen KN, Rasmussen SA, Riehle-Colarusso T, Reefhuis J. Association between reported venlafaxine use in early pregnancy and birth defects, national birth defects prevention study, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2013;97(1):28–35. doi:10.1002/bdra.23096
7. Penberthy JK, Hook JN, Hettema J, Farrell-Carnahan L, Ingersoll K. Depressive symptoms moderate treatment response to brief intervention for prevention of alcohol exposed pregnancy. J Subst Abuse Treat. 2013;45(4):335–342. doi:10.1016/j.jsat.2013.05.002
8. Wichman CL, Stern TA. Diagnosing and treating depression during pregnancy. Prim Care Companion CNS Disord. 2015;17(2). doi:10.4088/PCC.15f01776
9. Mikšić Š, Miškulin M, Juranić B, et al. Depression and suicidality during pregnancy. Psychiatr Danub. 2018;30(1):85–90. doi:10.24869/psyd.2018.85
10. Thakolpattanakul K, Deoisres W, Tachasuksri A. Factors related to sleep quality in pregnant women. J Faculty Nursing Burapha Univ. 2019;27(1):60–67.
11. Sedov ID, Cameron EE, Madigan S, Tomfohr-Madsen LM. Sleep quality during pregnancy: a meta-analysis. Sleep Med Rev. 2018;38:168–176. doi:10.1016/j.smrv.2017.06.005
12. Naghi I, Keypour F, Ahari SB, Tavalai SA, Khak M. Sleep disturbance in late pregnancy and type and duration of labour. J Obstet Gynaecol. 2011;31(6):489–491. doi:10.3109/01443615.2011.579196
13. Mellor R, Chua SC, Boyce P. Antenatal depression: an artefact of sleep disturbance? Arch Womens Ment Health. 2014;17(4):291–302. doi:10.1007/s00737-014-0427-6
14. Skouteris H, Wertheim EH, Germano C, Paxton SJ, Milgrom J. Assessing sleep during pregnancy: a study across two time points examining the Pittsburgh Sleep Quality Index and associations with depressive symptoms. Womens Health Issues. 2009;19(1):45–51. doi:10.1016/j.whi.2008.10.004
15. Tomfohr LM, Buliga E, Letourneau NL, Campbell TS, Giesbrecht GF. Trajectories of sleep quality and associations with mood during the perinatal period. Sleep. 2015;38(8):1237–1245. doi:10.5665/sleep.4900
16. Gao M, Hu J, Yang L, et al. Association of sleep quality during pregnancy with stress and depression: a prospective birth cohort study in China. BMC Pregnancy Childbirth. 2019;19(1):444. doi:10.1186/s12884-019-2583-1
17. Gelaye B, Barrios YV, Zhong QY, et al. Association of poor subjective sleep quality with suicidal ideation among pregnant Peruvian women. Gen Hosp Psychiatry. 2015;37(5):441–447. doi:10.1016/j.genhosppsych.2015.04.014
18. Liu H, Li H, Li C, et al. Associations between maternal sleep quality throughout pregnancy and newborn birth weight. Behav Sleep Med. 2021;19(1):57–69. doi:10.1080/15402002.2019.1702551
19. Wang L, Jin F. Association between maternal sleep duration and quality, and the risk of preterm birth: a systematic review and meta-analysis of observational studies. BMC Pregnancy Childbirth. 2020;20(1):125. doi:10.1186/s12884-020-2814-5
20. Fung J, Gelaye B, Zhong QY, et al. Association of decreased serum brain-derived neurotrophic factor (BDNF) concentrations in early pregnancy with antepartum depression. BMC Psychiatry. 2015;15:43. doi:10.1186/s12888-015-0428-7
21. Molendijk ML, Bus BA, Spinhoven P, et al. Serum levels of brain-derived neurotrophic factor in major depressive disorder: state-trait issues, clinical features and pharmacological treatment. Mol Psychiatry. 2011;16(11):1088–1095. doi:10.1038/mp.2010.98
22. Shimizu E, Hashimoto K, Okamura N, et al. Alterations of serum levels of brain-derived neurotrophic factor (BDNF) in depressed patients with or without antidepressants. Biol Psychiatry. 2003;54(1):70–75. doi:10.1016/S0006-3223(03)00181-1
23. Monteiro BC, Monteiro S, Candida M, et al. Relationship between brain-derived neurotrofic factor (BDNF) and sleep on depression: a critical review. Clin Pract Epidemiol Ment Health. 2017;13:213–219. doi:10.2174/1745017901713010213
24. Yang T, Nie Z, Shu H, et al. The role of BDNF on neural plasticity in depression. Front Cell Neurosci. 2020;14:82. doi:10.3389/fncel.2020.00082
25. Phillips C. Brain-derived neurotrophic factor, depression, and physical activity: making the neuroplastic connection. Neural Plast. 2017;2017:7260130. doi:10.1155/2017/7260130
26. Arosio B, Guerini FR, Voshaar RCO, Aprahamian I. Blood brain-derived neurotrophic factor (BDNF) and major depression: do we have a translational perspective? Front Behav Neurosci. 2021;15:626906. doi:10.3389/fnbeh.2021.626906
27. Youssef MM, Underwood MD, Huang YY, et al. Association of BDNF Val66Met polymorphism and brain BDNF levels with major depression and suicide. Int J Neuropsychopharmacol. 2018;21(6):528–538. doi:10.1093/ijnp/pyy008
28. Giese M, Unternaehrer E, Brand S, Calabrese P, Holsboer-Trachsler E, Eckert A. The interplay of stress and sleep impacts BDNF level. PLoS One. 2013;8(10):e76050. doi:10.1371/journal.pone.0076050
29. Rethorst CD, Greer TL, Toups MSP, Bernstein I, Carmody TJ, Trivedi MH. IL-1β and BDNF are associated with improvement in hypersomnia but not insomnia following exercise in major depressive disorder. Transl Psychiatry. 2015;5(8):e611. doi:10.1038/tp.2015.104
30. Fan TT, Chen WH, Shi L, et al. Objective sleep duration is associated with cognitive deficits in primary insomnia: BDNF may play a role. Sleep. 2018;42(1):zsy192.
31. Murer MG, Boissiere F, Yan Q, et al. An immunohistochemical study of the distribution of brain-derived neurotrophic factor in the adult human brain, with particular reference to Alzheimer’s disease. Neuroscience. 1999;88(4):1015–1032. doi:10.1016/S0306-4522(98)00219-X
32. Mowla SJ, Farhadi HF, Pareek S, et al. Biosynthesis and post-translational processing of the precursor to brain-derived neurotrophic factor. J Biol Chem. 2001;276(16):12660–12666. doi:10.1074/jbc.M008104200
33. Yang J, Siao CJ, Nagappan G, et al. Neuronal release of proBDNF. Nat Neurosci. 2009;12(2):113–115. doi:10.1038/nn.2244
34. Christian LM, Mitchell AM, Gillespie SL, Palettas M. Serum brain-derived neurotrophic factor (BDNF) across pregnancy and postpartum: associations with race, depressive symptoms, and low birth weight. Psychoneuroendocrinology. 2016;74:69–76. doi:10.1016/j.psyneuen.2016.08.025
35. Journal of migrant workers statistic in Thailand [Internet]; 2015 [cited May 26, 2021]. Available from: https://www.doe.go.th/prd/assets/upload/files/alien_th/cea979ea00fbb2f2ad2b6d5e53d5dde8.pdf.
36. Zaw YH, Taneepanichskul N. Blood heavy metals and brain-derived neurotrophic factor in the first trimester of pregnancy among migrant workers. PLoS One. 2019;14(6):e0218409. doi:10.1371/journal.pone.0218409
37. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
38. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
39. Facco FL, Kramer J, Ho KH, Zee PC, Grobman WA. Sleep disturbances in pregnancy. Obstet Gynecol. 2010;115(1):77–83. doi:10.1097/AOG.0b013e3181c4f8ec
40. Gelaye B, Addae G, Neway B, et al. Poor sleep quality, antepartum depression and suicidal ideation among pregnant women. J Affect Disord. 2017;209:195–200. doi:10.1016/j.jad.2016.11.020
41. Kızılırmak A, Timur S, Kartal B. Insomnia in pregnancy and factors related to insomnia. Sci World J. 2012;2012:197093. doi:10.1100/2012/197093
42. Santiago GTP, de Menezes Galvão AC, de Almeida RN, et al. Changes in cortisol but not in brain-derived neurotrophic factor modulate the association between sleep disturbances and major depression. Front Behav Neurosci. 2020;14:44. doi:10.3389/fnbeh.2020.00044
43. Barnes AK, Koul-Tiwari R, Garner JM, Geist PA, Datta S. Activation of brain-derived neurotrophic factor-tropomyosin receptor kinase B signaling in the pedunculopontine tegmental nucleus: a novel mechanism for the homeostatic regulation of rapid eye movement sleep. J Neurochem. 2017;141(1):111–123. doi:10.1111/jnc.13938
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.