")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Bowen’s Disease of the Nipple and Areola: Case Report and Literature Review
Authors Zhang G, Lu Y, Liu B, Wang Y, Li W, Xu Y
Received 27 April 2023
Accepted for publication 4 July 2023
Published 9 August 2023 Volume 2023:16 Pages 2113—2118
DOI https://doi.org/10.2147/CCID.S419059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Guiyun Zhang,1 Yufeng Lu,2 Bin Liu,3 Yanmei Wang,4 Wenyi Li,1 Yangchun Xu1
1Department of Dermatology, The Second Hospital of Jilin University, Changchun, 130041, People’s Republic of China; 2Department of Thoracic Surgery, China-Japan Union Hospital of Jilin University, Changchun, 130000, People’s Republic of China; 3Department of Breast Surgery, The Second Hospital of Jilin University, Changchun, 130041, People’s Republic of China; 4Department of Clinical Nutrition, Jilin Province People’s Hospital, Changchun, 130021, People’s Republic of China
Correspondence: Yangchun Xu, Department of Dermatology, The Second Hospital of Jilin University, No. 218 Ziqiang Street, Nanguan District, Changchun, 130041, People’s Republic of China, Tel +86-431-8113-6244, Email [email protected]
Introduction: Bowen’s disease (BD) commonly occurs in sites of chronic sunlight exposure such as head, neck and extremities. It rarely distributes on the nipple and areola.
Case Presentation: A 59-year-old female presented with crusted plaque on the right breast for over 1 month. Physical examination found an asymptomatic plaque (5 cm × 5 cm) with irregular shape on the right breast. Histopathological examination suggested irregularly acanthotic epidermis and atypical epidermal cells. Dermis showed inflammatory cell infiltration. Immunohistochemical staining showed negative staining for cytokeratin 7 and cytokeratin 20, and positive staining for Ki67 (60%). The mass was excised and no recurrence occurred in the follow-up. Additionally, we reviewed the literature about BD of the breast and summarized the clinical manifestations, histological features, and treatment options.
Conclusion: We reported a rare BD case involving nipple and areola. Wide local excision and complete nipple excision are effective for patients with BD of the nipple and areola.
Keywords: Bowen’s disease, breast, nipple, case report
Introduction
Bowen’s disease (BD) is a type of non-melanocytic intraepidermal malignancy,1 firstly described by John Templeton Bowen in 1912.2 It usually presents as a gradually enlarging well-demarcated erythematous plaque with an irregular border and crusting or scaling surface.3 To our best knowledge, BD usually develops on sun-exposed areas such as head, neck and extremities, with rare cases showed lesions involving palms, soles or breast.4–6 In this study, we reported a rare BD case involving nipple and areola.
Case Report
A 59-year-old female was referred to our department with crusted plaque on the right breast for over 1 month. Before presenting to our department, she was treated with compound dexamethasone acetate, but the symptoms did not resolve. Physical examination showed normal right breast. There were no axillary lymphadenopathy, edema, orange peel-like lesion or varicose veins in the bilateral breasts. An irregular asymptomatic plaque with a size of 5 cm × 5 cm was seen on the right breast (Figure 1). The plaque showed an unsmooth, scaly, and scarred surface with local ulceration. Ultrasound examination showed no occupying lesions in both breasts, and there were no abnormally enlarged lymph node echoes in bilateral axillae and supraclavicular fossae. Histopathological examination showed hyperkeratosis, parakeratosis, and epidermal pustules (Figure 2A). The epidermis was irregularly acanthotic and epidermal atypia was noted. Inflammatory cell infiltration was presented within the dermis. Immunohistochemical staining indicated negativity for cytokeratin 7 (Figure 2B) and cytokeratin 20 (Figure 2C), and positivity for Ki67 (60%) (Figure 2D). Finally, the patient was diagnosed with BD of the breast. The tumor mass was dissected under general anesthesia, and no recurrence was reported by the patient during the 6-month follow-up.
 |
Figure 1 Large scaly erythematous plaque on the right breast. |
 |
Figure 2 Histological pathogenesis of the resected specimen. (A) H&E staining. (B) Immunohistochemical staining of cytokeratin 7, (C) cytokeratin 20, and (D) Ki67. Scale bar: 100 μm. |
Discussion
BD is firstly recognized as an intraepidermal or in situ malignant neoplasm precursor in 1912.2 Most cases of BD present with lesions on body parts that have been exposed to ultraviolet light, such as hand, head, and neck, with a few cases presenting with lesions on the nipples. A case of BD involved the nipple was first described by Cremer et al in 1982.7 Since then, rare studies have reported BD patients with lesions on the nipple. Through a comprehensive literature search from Medline, PubMed, and Em-BASE databases, we obtained 12 BD cases (2 males and 10 females) with breast involvement (Table 1) using the following keywords: “extensive Bowen’s disease”, “huge Bowen’s disease”, “large Bowen’s disease”, “squamous cell carcinoma in situ”, and “nipple” and “areola”.6–15 In this case report, we reported a BD patient with the involvement of the nipple and areola, and summarized the clinical manifestations, histological features, and treatment options for BD patients, aiming to enhance our understanding of BD of the breast.
 |
Table 1 Summary of Case Reports of Bowen’s Disease in the Nipple and Areola |
Patients with BD are typically asymptomatic in terms of clinical manifestations. The condition is characterized by a single, well-demarcated, solitary, erythematous, and scaly patch that corresponds to the non-pigmented subtype. The surface may be hyperkeratotic, dry, or fissured with irregular borders or uniform roundness.16 A pigmented variant typically appears on areas of the skin that are not exposed to the sun in patients, and it manifests as a scaly plaque with pigmentation. Once skin that has been exposed to the sun is involved by BD, other lesions indicative of chronic sun damage may also appear, such as discoloration, basal cell carcinoma, dermatophytosis, and solar keratosis.16 The majority of patients with BD exhibit a peculiar dermoscopic pattern characterized by a scaly surface and glomerular vessels.17 Mammography revealed nodular thickening of the soft tissue in the right areolar skin, which was associated with a mass shadow located beneath the areola.12 The lesion grows slowly and centripetally, typically reaching a diameter of 10–26 mm.11 In an 82-year-old female patient with BD, a long-standing lesion may grow laterally to a size exceeding 3.5 cm.18 BD of the breast is clinically manifested as a pruritic and scaly lesion over the unilateral nipple.14 In addition, patients may present with scaling, crusting, pruritus, swelling, occasional bleeding, and inflammation of the nipple.9,10,13,15
The histological characteristics included thickening of the epithelium, parakeratosis, epithelial mitoses, pleomorphic nuclei with full-thickness epidermal atypia, and sparing of the basal layer. The other histological features included abnormal keratinocytes throughout a thickened epidermis, as well as involvement of acrotrichia, with or without hyperpigmentation of basal keratinocytes and/or melanophages in the dermis.11,14,15,19 Atypical cells of the epidermis often have large, and hyperchromatic nuclei, which commonly show keratinization of individual cells.16 Many anaplastic keratinocytes were noted in the epidermis, with nuclei of irregular size and form.11 Although the plaque in our patient occurred over sun-unexposed breast, increased amount of melanin pigment was not observed in stratum basale, dermal melanophages, or melanocytes. Patients with BD of the nipple exhibit epidermal changes characterized by acanthosis, elongation of rete pegs due to large atypical cells with loss of polarity, and a parakeratotic layer on the surface.8 Biopsy specimens from patients with BD display irregular epidermal hyperplasia and diffuse interstitial infiltration at the papillary dermis, and the majority of the inflammatory cells were lymphocytes.7,10,11 Immuno-histological staining revealed that cases with BD were negative for cytokeratin 7, cytokeratin 20, and positive for cytokeratin 5, cytokeratin 6, and p63.11,14,15
Although BD is typically limited to the epidermis, the distinctive anatomy of the nipple allows the disease to spread deeply through the lactiferous ducts, which are a continuation of the nipple’s epidermal layer.10 The differential diagnosis for this disease includes Paget’s disease and seborrheic keratosis due to their similar clinical and dermoscopic features. Superficial basal cell carcinoma, melanoma, and solar keratosis should be considered in the differential diagnosis of BD.20 The atypical cells in BD are characterized by the involvement of the outer root sheath of the hair follicle, which could differentiate BD from solar keratosis.16 Despite certain similarities between Bowen’s disease and Paget’s disease,6,8 there are differences in the clinical presentation, disease progression, distribution, and histopathological characteristics between the two conditions (Table 2). It is crucial to differentiate BD and Paget’s disease using immuno-histological staining. Cytokeratin 7 is negative in BD cases, while it is positive in those with Paget’s disease. Cytokeratin 5 and cytokeratin 6 are positive in BD patients, but negative in patients with Paget’s disease.14
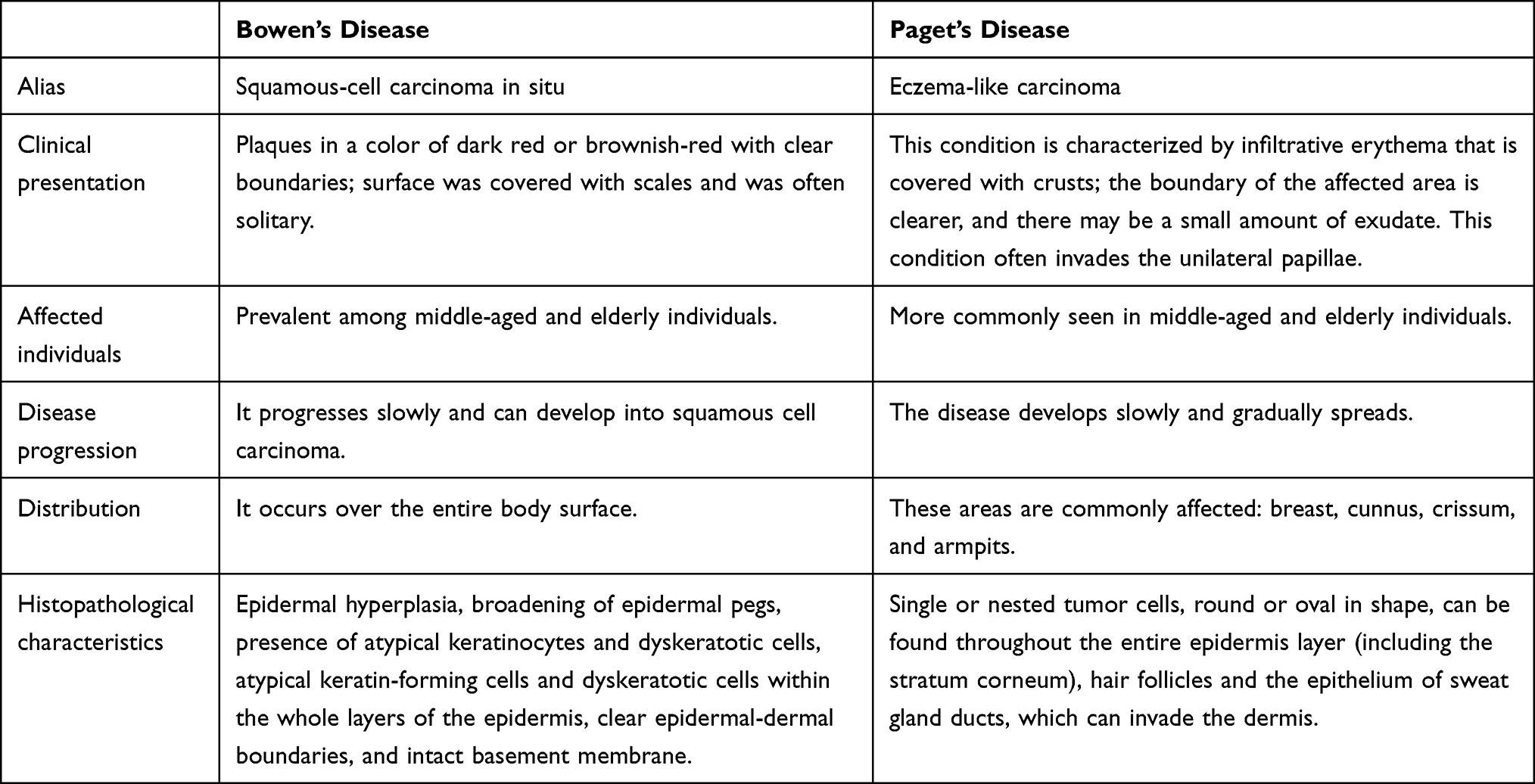 |
Table 2 Summary of Differences Between Bowen’s Disease and Paget’s Disease |
BD can progress into invasive squamous cell carcinoma after several years if left untreated.16 The treatment options for BD are extensive and have shown favorable therapeutic effects. These options include cryotherapy, curettage with cautery, topical fluorouracil, radiotherapy, excision, imiquimod, photodynamic therapy, and topical diclofenac.4,21 The choice of therapy can be influenced by various factors, including the patient’s age, number, size and localization of the lesion, patient’s preferences and comfort level, and the affordability of different therapeutic modalities. There is currently no widely accepted management protocol for BD of the nipple due to its rarity. For these patients, treatment modalities include photodynamic therapy, cryotherapy, simple mastectomy, and sentinel lymph node biopsy.6 In clinical practice, steroid-based treatments are not commonly used because most patients do not respond to topical creams containing steroids.8,9,15 Furthermore, performing a wide local excision with immediate full-thickness skin graft reconstruction can aid in rehabilitation without leaving any underlying abnormalities.8,14
Conclusion
In conclusion, BD involving the nipple and areola is rarely reported. Here, we diagnosed a patient with BD on the nipple and areola. Furthermore, we have provided a summary of the clinical manifestations, histological features, and available treatment options for patients diagnosed with BD. Wide local excision and complete nipple excision are effective treatments for patients with BD involving the nipple and areola.
Ethics Approval and Informed Consent
This study was performed according to the convention of the Declaration of Helsinki. This study protocol was reviewed and approved by the Ethics Committee of the Second Hospital of Jilin University [Approval No.: 2022-117]. Written informed consent was obtained from the patient.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Jilin Provincial Science and Technology Development Project [Grant No.: 20200201577JC].
Disclosure
The authors declare that they have no competing interests.
References
1. Palaniappan V, Karthikeyan K. Bowen’s disease. Indian Dermatol Online J. 2022;13:177. doi:10.4103/idoj.idoj_257_21
2. Bowen JT. Precancerous dermatoses: a study of two cases of chronic atypical epithelial proliferation. Arch Dermatol. 1983;119(3):243–260. doi:10.1001/archderm.1983.01650270061020
3. Mohandas P, Lowden M, Varma S. Bowen’s disease. BMJ. 2020;368. doi:10.1136/bmj.m813
4. Cox NH, Eedy DJ, Morton CA. Guidelines for management of Bowen’s disease: 2006 update. Br J Dermatol. 2007;156:11–21. doi:10.1111/j.1365-2133.2006.07610.x
5. Yamaguchi K, Matsunuma R, Kumeta T, et al. Concurrent Bowen’s disease of the nipple and breast cancer. Case Rep Oncol. 2020;13:1410–1414. doi:10.1159/000511565
6. Brookes PT, Jhawar S, Hinton CP, Murdoch S, Usman T. Bowen’s disease of the nipple-a new method of treatment. Breast. 2005;14:65–67. doi:10.1016/j.breast.2004.05.001
7. Cremer H, Paulussen F. Die Bowensche Erkrankung der Mamille [Bowen’s disease of the nipple]. Geburtshilfe Frauenheilkd. 1982;42:590–592. German. doi:10.1055/s-2008-1036926
8. Venkataseshan VS, Budd DC, Un Kim D, Hutter RV. Enfermedad de Bowen en la epidermis de la mama Intraepidermal squamous carcinoma (Bowen’s disease) of the nipple. Hum Pathol. 1994;25:1371–1374. Spanish. doi:10.1016/0046-8177(94)90100-7
9. Sharma R, Iyer M. Bowen’s disease of the nipple in a young man with AIDS: a case report. Clin Breast Cancer. 2009;9:53–55. doi:10.3816/CBC.2009.n.010
10. Yazicioglu MB, Tokyol C, Keskin AI, Aktepe F. A rare disease of the breast: bowen’s disease. Nat J Med Res. 2014;4:168–169.
11. Ishikawa M, Ohtsuka M, Yamamoto T. Bowen’s Disease of the nipple and areola in an old man. Indian J Dermatol. 2015;60:424. doi:10.4103/0019-5154.160543
12. Huang -C-C, Chang Y-C, Tzen C-Y, Liu C-L, Liu T-P. Bowen’s Disease of the nipple in a woman with tongue cancer. J Cancer Res Pract. 2015;2:168–171.
13. Kitahara M, Hozumi Y, Watanabe A, Iijima T. Bowen’s disease of the nipple. Case Rep Oncol. 2018;11:609–614. doi:10.1159/000492382
14. Liang DG, Soliman B, Cha J. A rare case of Bowen’s disease of the nipple: literature review and management pathway. Breast J. 2020;26:1234–1238. doi:10.1111/tbj.13824
15. Torabi M, Onyemkpa CJ, Samat S, et al. Bowen’s disease of the nipple: a case report. Ann Breast Surg. 2021;5:41. doi:10.21037/abs-20-154
16. Rickert RR, Brodkin RH, Hutter RV. Bowen’s disease. CA Cancer J Clin. 1977;27(3):160–166. doi:10.3322/canjclin.27.3.160
17. Behera B, Kumari R, Thappa DM, et al. Dermoscopy of Bowen’s disease: a case series of five patients. Indian J Dermatol Venereol Leprol. 2021;87:576–580. doi:10.25259/IJDVL_987_20
18. Ortiz-Mendoza CM, Acosta-Sánchez NA, Catarino-Dircio A. [Bowen’s disease of the breast]. Cir Cir. 2005;73:379–381. Spanish.
19. Stewart TJ, Farrell J, Crainic O, Rosen RH. A large series of pigmented Bowen’s disease. Int J Dermatol. 2020;59:e316–e317. doi:10.1111/ijd.14977
20. Lacarrubba F, Verzì AE, Caltabiano R, Micali G. Bowen’s disease of the penile shaft presenting as a pigmented macule: dermoscopy, reflectance confocal microscopy and histopathological correlation. An Bras Dermatol. 2021;96(5):609–612. doi:10.1016/j.abd.2020.10.009
21. Calin MA, Diaconeasa A, Savastru D, Tautan M. Photosensitizers and light sources for photodynamic therapy of the Bowen’s disease. Arch Dermatol Res. 2011;303(3):145–151. doi:10.1007/s00403-011-1122-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.